a psychiatrist's guide to sleep disorder screening - the lung
TRANSCRIPT

Treatment of Insomnia for
Clinicians
Larry Pawluk, M.D., FRCPC
Diplomate, American Board of Sleep Medicine
Clinical Professor of Psychiatry,
Sleep Medicine Program, University of Alberta

What is Insomnia?
A complaint of:
• Difficulty falling asleep
• Difficulty staying asleep
• Poor quality sleep
Associated with:
• Distress
• Impaired function

Insomnia
And finally there was the sleepless night
When I decided to explore and fight
The foul, the inadmissible abyss,
Devoting all my twisted life to this
One task.
- Vladimir Nabokov (from Pale Fire)

Insomnia: Daytime Complaints
Fatigue, sluggishness
Sleepiness
Somatic complaints (aches & pains)
Stress about poor sleep
Mood disturbances
Poor concentration
Impaired performance

Insomnia: Consequences
Decreased quality of life
Increased healthcare costs
Increased absenteeism
Decreased productivity
Increased risk for developing psychiatric disorders
Increased accident risk
Chesson A Jr. et al. SLEEP 2000;23.
Sateia MJ et al. SLEEP 2000;23.
Insomnia: Prevalence
Insomnia is the most
common sleep complaint
in the industrialized
world
Complaints in 30% to
40%
Complaint with distress
or impairment: 8% to
19%
Sateia MJ et al. SLEEP 2000;23.
Major Risk Factors
Previous history of insomnia
Increasing age
Female gender
Psychiatric symptoms and disorders
Medical symptoms and disorders

Management of Insomnia
Insomnia
History
– Initiation vs. Maintenance vs. Early Morning
Awakening
– Description Speed of onset and precipitant
Temporal relationship to other symptoms
Course and duration
Exacerbating/alleviating factors

Insomnia
History
– Typical Night Pre-bed routine and bedtime
Sleep onset
Number of awakenings and duration
Final awakening
Variation in schedule on weekends/vacations
Daytime Naps
– Daytime Consequences
– Sleep Log/Diary
– Interview with bed partner

Insomnia
Common Causes
– Most often there is more than one cause.
– Insomnia related to a psychiatric disorder
makes up > 75% of primary or secondary
diagnoses in insomniacs presenting to sleep
centres (APA/NIMH DSM IV Field Trial).

Insomnia
Common Causes
– Poor sleep hygiene
– Alcohol, nicotine, caffeine, substances
– Medications
– Psychiatric disorders
– Medical disorders
– Psychophysiological (Conditioned) insomnia
– Restless Legs Syndrome and Periodic Limb
Movements
– Delayed Sleep Phase Syndrome
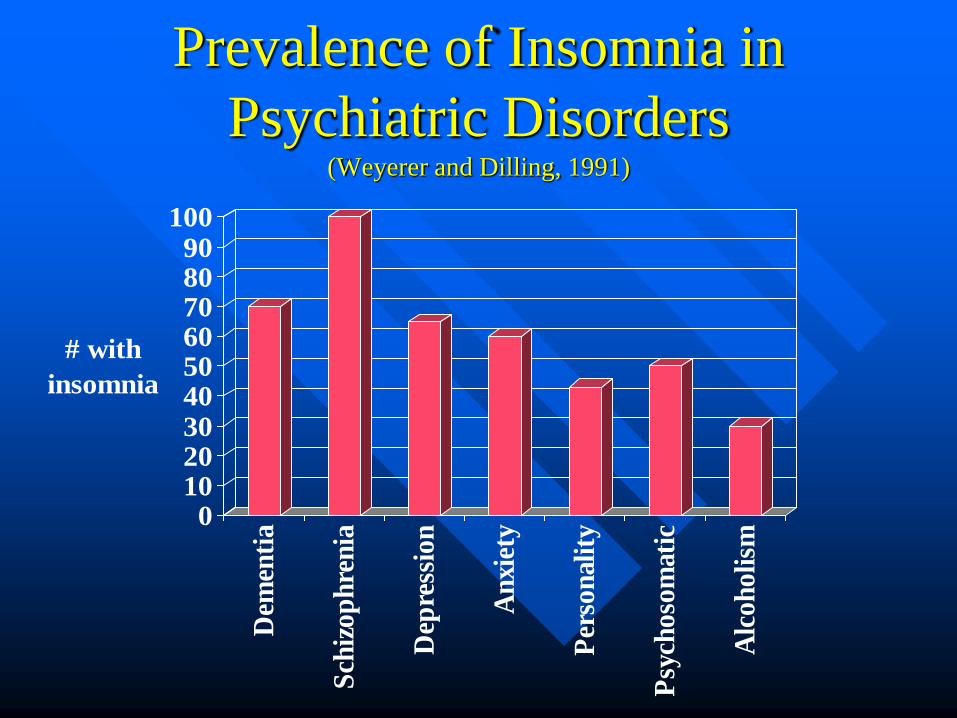
Prevalence of Insomnia in
Psychiatric Disorders (Weyerer and Dilling, 1991)
0102030405060708090
100
# with
insomnia
Dem
enti
a
Sch
izop
hre
nia
Dep
ress
ion
An
xiet
y
Per
son
alit
y
Psy
choso
mat
ic
Alc
oh
oli
sm

Insomnia
Common Causes
– Clues suggestive of a psychiatric diagnosis Other psychiatric symptoms began in proximity to
insomnia.
Early morning awakening.
Non-restorative sleep.
Daytime fatigue/anergia.
Feelings of hopelessness, helplessness; anhedonia.
Agitation, worrying.
Overwhelmed by or excessively focused on insomnia.

Insomnia
Common Causes
– Medical disorders
» Neurological
Seizures, headache, Parkinsons, dementia, tumors, movement disorders.
» Endocrinopathies
Diabetes, hyperthyroidism, Addisons, Cushings.
» Respiratory
Obstructive Sleep Apnea, COPD, asthma, CF.
» Pain
Arthritis, various other.
» GI
GERD, PUD, inflammatory bowel disease.
» Renal, Cardiac, IDs, Dermatological
Insomnia
Common Causes
– Psychophysiological (Conditioned) insomnia
» Largest category of “non-psychiatric” chronic insomnia.
» May have obsessional or somatoform traits.
» Features:
Initiating factor= stressor in light sleeper.
Insomnia develops “life of its own” after stressor diminishes.
Excessive focus on poor sleep results in maladaptive associations promoting further wakefulness eg. clockwatching, ruminating, catastrophizing.
Occasionally sleeps better away from home.

Insomnia
Common Causes
– Restless Legs Syndrome and Periodic Limb
Movements
» Cardinal symptoms
Unusual sensations exclusively in lower legs typically at
bedtime often preventing sleep initiation.
Accompanied by strong urge to move legs which
alleviates the uncomfortable sensation.
Once asleep, bed partner may notice lower leg
jerking/kicking which may or may not be associated with
brief cortical arousals.

Insomnia
Common Causes
– Delayed Sleep Phase Syndrome
» Shift of entire sleep period in a phase delayed direction.
» Sleep initiation insomnia with difficulty awakening in the
morning – at times with morning daytime sleepiness.
» Usually adolescents and young adults.
» Disorder “disappears” when allowed to follow their preferred
sleep schedule.
» DDx includes mood disorders, substance abuse, poor sleep
hygiene.

Clinical Presentation
Predisposing, Precipitating and Perpetuating Factors

Assessment: Sleep/wake Diary

Assessment: Polysomnography
Indications
– Suspect other sleep disorder
– Poor treatment response
– Atypical clinical presentation
Not routinely indicated for the evaluation of insomnia
Practice parameters for the evaluation of chronic insomnia. SLEEP 2000;23.

Treatment of Insomnia

Nonpharmacologic Therapy: Sleep Hygiene and Cognitive Behavioral
Therapy (CBTI)

Cognitive Behavioral Therapy
Reset or reinforce biological rhythm with light
therapy and/or melatonin.
Circadian rhythm
entrainment
Reduce arousal & decrease anxiety Relaxation training
Address maladaptive thoughts and beliefs that
interfere with sleep.
Cognitive therapy
Restrict time in bed to improve sleep depth &
consolidation
Sleep restriction
Strengthen bed & bedroom as sleep stimulus Stimulus control
Promote habits that help sleep; provide rationale
for instructions.
Sleep hygiene
AIM TECHNIQUE
Behavioral Treatment: Sleep Hygiene
Regularize sleep / wake schedule
Avoid stimulants and stimulating behavior
Establish relaxing bedtime routine
Provide conducive sleep environment
Limit daytime naps
Reduce or eliminate alcohol, caffeine and
nicotine
Obtain regular exercise
Avoid clock watching

Behavioral Treatment:
Stimulus Control
Use bed for sleep (and sex)
Go to bed only when sleepy
Get out of bed when unable to sleep
Wake up at a consistent time (including weekends)
Do not take daytime naps

Behavioral Treatment: Sleep Restriction (Consolidation)
Determine average time asleep
Set time in bed = time asleep
Consistent wake-up time
No daytime naps
If time asleep > 90% of time in bed then increase time in bed (15-30 minutes)
If time asleep < 80% of time in bed then decrease time in bed (15-30 minutes)
Spielman AJ et al. SLEEP 1987;10.

Nonpharmacologic Treatment Efficacy
90
0
10
20
30
40
50
60
70
80
Stimulus
Control
Sleep
Restriction Relaxation Sleep
Hygiene Multi-component
Sle
ep L
aten
cy (
Min
ute
s)
Pre-treatment
Post-treatment
Adapted from Morin CM et al. Am J Psychiatry 1994;151.
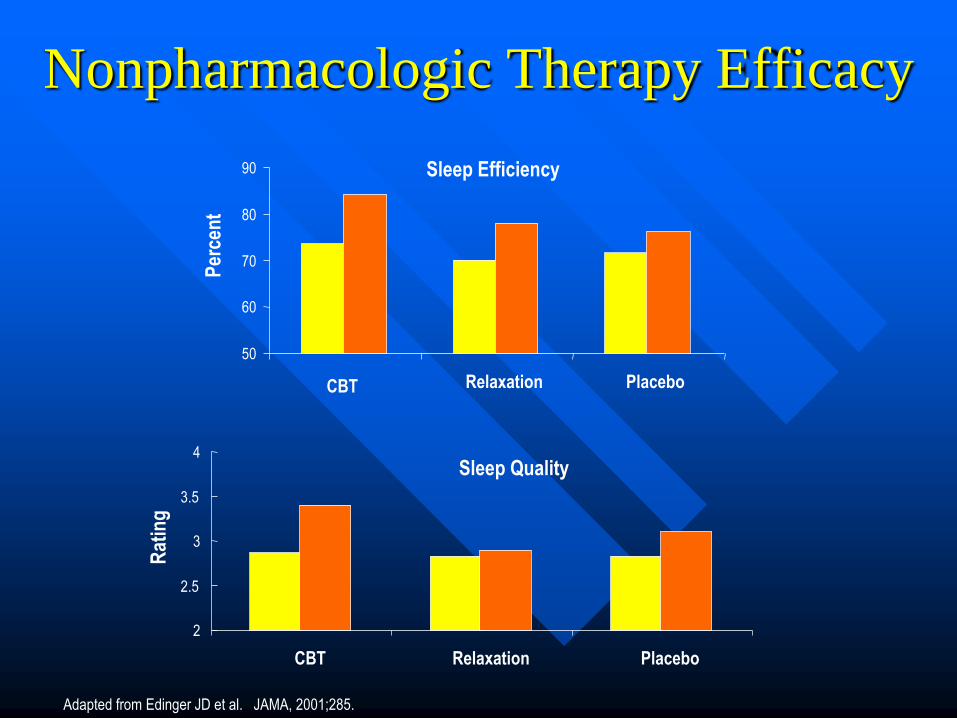
Nonpharmacologic Therapy Efficacy
Sleep Efficiency
50
60
70
80
90
CBT Relaxation Placebo
Per
cen
t
Adapted from Edinger JD et al. JAMA, 2001;285.
Sleep Quality
2
2.5
3
3.5
4
CBT Relaxation Placebo
Rat
ing

Nonpharmacologic Treatment:
“The Minimum”
Review sleep hygiene
Limit time in bed
Establish regular wake-up time
Go to bed only when sleepy
Get out of bed if unable to sleep

Pharmacotherapy: Indications
Acute Stress
Shift Work
Jet Lag
Predictable Stress
Chronic Insomnia

Pharmacotherapy
Benzodiazepines
Newer GABA receptor agonists
Antidepressants
Antihistamines
Melatonin
Others
Benzodiazepines
temazepam (Restoril)
triazolam (Halcion)
clonazepam (Rivotril)
lorazepam (Ativan)
diazepam (Valium)
flurazepam (Dalmane)
Pharmacotherapy:
Benzodiazepine/GABA Receptor
Agonists
Non-benzodiazepines
zopiclone (Imovane)
zolpidem SL (Sublinox)
zaleplon (Starnoc)

Drug Onset of
Action
Elimination
Half-Life (h)
Typical Adult
Dose
Triazolam 10-20 min 1.5-5 0.125-0.25 mg
Temazepam 45-60 min 8-20 15-30 mg
Zaleplon 10-20 min 1.0 5-20 mg
Zopiclone 20-30 min 5 3.75-7.5 mg
Zolpidem SL 15-20 min 2.6 10 mg
Hypnotic Pharmacokinetics

Pharmacotherapy: Benzodiazepines
Actions
Hypnotic
Anxiolytic
Myorelaxant
Anticonvulsant
Side effects
Sedation
Anterograde amnesia
Ataxia, falls
Respiratory depression
Tolerance, dependence,
abuse

Benzodiazepine/GABA Receptor
Agonists: Effects on Sleep
Sleep continuity
– Sleep latency
– Awakenings
– Sleep Duration
Slow Wave Sleep (BZs only)
REM (BZs only)
Duration and number of sleep spindles
Periodic limb movements and associated arousals
Benzodiazepines: Rebound
Insomnia
Is related to dose and half-life
Can be prevented by tapering dose
Cannot easily be distinguished from return of
original symptoms
Does not predict future pill-taking behavior
Varies among drugs
May not be seen with some agents
Benzodiazepine/GABA Receptor
Agonists: Clinical Approach
Establish correct diagnosis
Evaluate carefully for apnea, respiratory impairment, organic
mental disorders, substance abuse history
Choose drug with desired pharmacokinetic profile
Use lowest effective dose
Monitor side effects (e.g. fall risk, sedation)
Aim for short-term, intermittent use
Consider long-term use in carefully selected patients

Sublinox® (zolpidem tartrate ODT):
Product Profile Product
Fast disintegrating, sublingual zolpidem tablet
Characteristics
Fast sublingual disintegration (≤ 2 minutes)
For patients with difficulty swallowing or those who don’t like to swallow pills or don’t have access to water
Ideal product profile for “on demand” treatment
Next day residual effects comparable to oral formulation
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.
Mechanism of Action • Subunit modulation of the GABAA receptor chloride channel macromolecular complex is
hypothesized to be responsible for sedative, anticonvulsant, anxioytic, and myorelexant drug
properties.
• The major modulatory site of the GABAA receptor complex is located on its alpha () subunit
and is referred to as the benzodiazepine (BZ) or omega () receptor.
• Zolpidem has a chemical structure unrelated to benzodiazepines, barbiturates, or other drugs
with known hypnotic properties
• It interacts with the GABA-BZ receptor complex and shares some of the pharmacological
properties of the benzodiazepines.
• In contrast to the benzodiazepines, zolpidem in vitro binds the (ω1) receptor preferentially with
a high affinity ratio of the alpha1/alpha5 subunits.
• Selective binding of zolpidem on the (ω1) receptor may explain:
- the relative absence of myorelaxant and anticonvulsant effects in animal studies
- the preservation of deep sleep (stages 3 and 4) in human studies of zolpidem at
hypnotic doses (vs. benzodiazepines)
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.

Incidence of Treatment-Emergent Adverse Experiences in Placebo-
Controlled Clinical Trials with zolpidem tartrate lasting up to 35 nights (Percentage of patients reporting)
Body System/
Adverse Event*
Zolpidem tartrate (≤ 10 mg)
(N=152)
Placebo
(N=161)
Central and Peripheral Nervous System
Drowsiness 8 5
Dizziness 5 1
Lethargy 3 1
Drugged feeling 3 -
Lightheadedness 2 1
Depression 2 1
Abnormal dreams 1 -
Amnesia 1 -
Sleep disorder 1 -
Gastrointestinal System
Diarrhea 3 2
Abdominal pain 2 2
Constipation 2 1
Respiratory System
Sinusitis 4 2
Pharyngitis 3 1
Skin and Appendages
Rash 2 1
*Reactions
reported by at
least 1% of
patients treated
with oral
zolpidem and at a
greater frequency
than placebo.
Only dizziness
and drugged
feeling were
reported with
statistically
significant
differences
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.

Sublingual zolpidem in early onset of sleep
compared to oral zolpidem: polysomnographic study
in patients with primary insomnia
Staner L, et al. Curr Med Res Opin. 2010;26(6):1423-1431.

Study Design
Randomized, double-blind, two-period, cross-over multi-centre study
Polysomnographic study in patients with DSM-IV primary insomnia
Powered to test for superiority of sublingual oral zolpidem compared to oral zolpidem on latency to persistent sleep
Powered for “at least as good as” total sleep time and duration of wake after sleep onset
Staner L et al. Curr Med Res Opin. 2010;26(6):1423-1431.

Results – Sleep Initiation
Baseline Sublingual
zolpidem
Oral
zolpidem
Treatment
differences
Latency to persistent
sleep (min)
84.54±40.35 19.76±15.55 30.06±23.48 -
10.28(p=0.0
01)
Sleep onset latency
(min)
72.30±39.32 17.66±13.37 26.31±22.72 -8.63
(p<0.01)
Latency to stage 1 (min) 61.07±34.64 13.94±12.67 21.35±20.30 -7.43
(p<0.01)
Staner L, et al. Curr Med Res Opin. 2010;26(6):1423-1431.

Results – Sleep Continuity
and Architecture
Baseline Sublingual
zolpidem
Oral zolpidem Treatment
differences
SEI (%) 67.47±6.95 89.9±6.09 83.33±6.98 1.56 (p<0.05)
TTA (min) 153.94±46.43 45.80±29.23 53.41±33.57 -7.52 (p<0.05)
ST1 (min) 22.08±8.81 23.06±8.50 23.15±8.18 -0.06 (p=NS)
ST2 (min) 182.56±46.04 253.09±35.98 242.38±34.09 10.54 (p<0.05)
SWS (min) 51.65±25.19 71.91±32.69 73.60±29.96 -1.51 (p=NS)
REM (min) 70.44±19.64 86.74±24.72 88.31±20.64 -1.73 (p=NS)
RSL (min) 81.81±40.77 95.34±40.70 87.98±40.78 7.38 (p=NS)
• Sleep efficiency index and time spent in stage 2 were
significantly higher with sublingual zolpidem
• Patients receiving oral zolpidem demonstrated significantly
higher total time awake
Staner L et al. Curr Med Res Opin. 2010;26(6):1423-1431.

Sublinox® Contraindications Known hypersensitivity to zolpidem tartarte or to any of the
inactive ingredients in the formulation
Patients with significant obstructive sleep apnea syndrome
and acute and/or severe impairment of respiratory function.
Sublinox should not be given to patients with myasthenia
gravis and in patients with severe hepatic impairment.
Patients with a personal or family history of sleepwalking
Elderly (longer half life)
Not to be taken with alcohol
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.
COMPLEX SLEEP-RELATED BEHAVIOURS: Warning
Complex sleep-related behaviours such as “sleep-driving” (i.e., driving
while not fully awake after ingestion of a sedative-hypnotic, with amnesia
for the event) have been reported in patients who have taken Sublinox.
Other potentially dangerous behaviours have been reported in patients who
got out of bed after taking a sedative-hypnotic and were not fully awake,
including preparing and eating food, making phone calls, leaving the house,
etc. As with “sleep-driving”, patients usually do not remember these events.
Although complex sleep-related behaviours may occur with Sublinox alone
at therapeutic doses, the use of alcohol and other CNS-depressants with
Sublinox appears to increase the risk of such behaviours, as does the use of
Sublinox at doses exceeding the maximum recommended dose.
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.

The Right Dose of Sublinox®
Sublinox® recommended dose is 10 mg immediately before bedtime for adults
Sublinox® effect may be slowed by ingestion with food
Dose adjustment needed when used with other CNS depressants
The potential for drug interactions must always be considered.
Sublinox® course of treatment should not exceed 4 wks
Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.
Administration Instructions
• Should be taken right before bed time.
• Should not be taken with or immediately after a meal.
• Should not be taken when drinking alcohol, or with other CNS
depressants.
• Should be placed under the tongue, where it will disintegrate.
• Should not be chewed or swallowed and should not be taken with
water.
• Maximum recommended dose of 10mg should not be exceeded.
1. Product Monograph, Sublinox, Zolpidem tartrate orally disintegrating tablets. Montreal, Canada: MEDA Valeant Pharma Canada Inc.; 2011.

Antidepressants: Rationale
No antidepressant is FDA/HPB-approved for
treatment of insomnia
Some antidepressants have sedative, sleep-
promoting effects
Some insomnia patients have symptoms of
depression or anxiety
Low risk of abuse, but psychological dependence
occurs
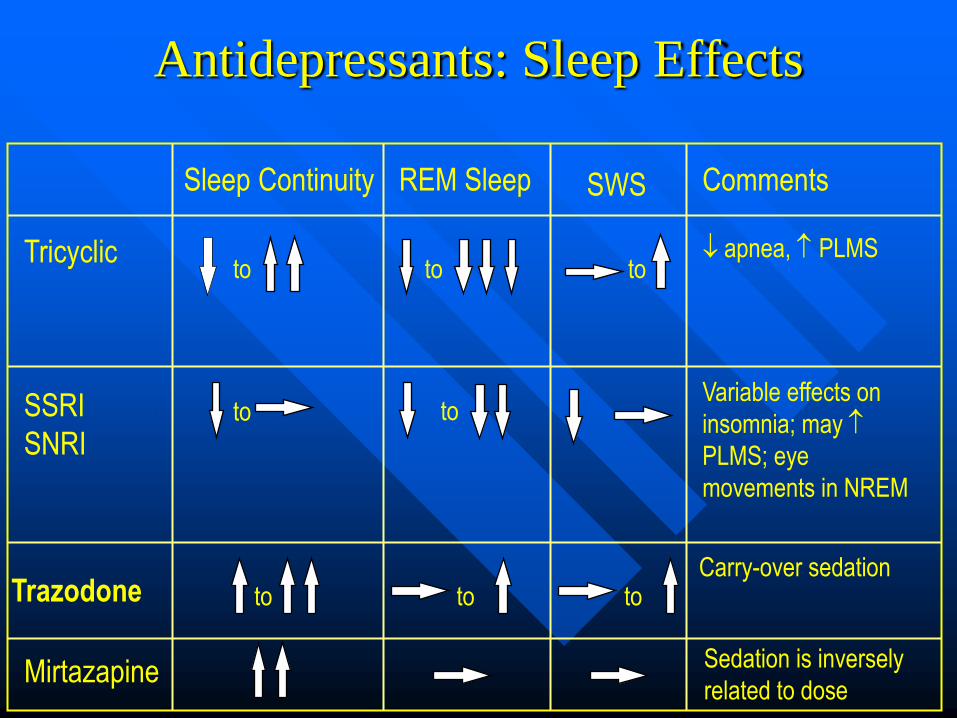
Antidepressants: Sleep Effects
Sleep Continuity REM Sleep SWS Comments
Tricyclic
apnea, PLMS
SSRI
SNRI
Variable effects on
insomnia; may
PLMS; eye
movements in NREM
to
to
to to
to to
Trazodone Carry-over sedation
Mirtazapine
to
Sedation is inversely
related to dose
to

Pharmacotherapy: Antihistamines
Mechanism of action
– H1 receptor antagonism
– Variable antagonism of cholinergic,
serotonergic, adrenergic receptors
Adverse effects
– Sedation, grogginess
– Dry mouth
– Psychomotor impairment
– Delirium

Antihistamines: Sleep Efficacy
Diphenhydramine 50mg Placebo
Ord
inal
Rat
ing
Sca
le
0
0.5
1
1.5
2
2.5
3
3.5
Sleep
Latency
Number of
Awakenings
Sleep
Duration
Sleep
Quality
p<.01
Adapted from Rickels K et al. J Clin Pharmacol 1983;23.
p<.01 p<.001 p<.001

Pharmacotherapy: Melatonin
Naturally occurring hormone secreted during darkness at night
Broad range of physiological effects
Inconclusive findings concerning sleep promotion in insomnia
May be most useful in shifting circadian phase e.g. delayed sleep phase syndrome

Other Pharmacologic Agents
Tryptophan
Valerian
HRT

Pharmacologic Treatment: Approach
Select appropriate medication
Use lowest effective dose
Use at bedtime
Duration of therapy
– Use as needed for 2 to 4 weeks
– Reduce dose as tolerated
– Intermittent use suggested
– Reassess and adjust approach
Combine with behavioral strategies


Insomnia Case 1
40 year old female teacher
Unable to sleep for 5 years with worsening
over 3 months
Appears anxious
Worries she will lose job due to lack of
sleep

Insomnia Case 1
Evaluation
– 1. Description
» Initiation insomnia for 5 yrs; abrupt worsening X 3
months with EMW
» Typical noc:
» BT 10 pm, sleep onset 3 hrs (toss and turn, check
clock, ruminates, ++ focussing on need to sleep),
EMW ~ 5 am
» Sleep diary confirms

Insomnia Case 1
Evaluation
– 2. Common Causes
» Sleep hygiene incl. EtOH caffeine, substances: marks late
» Meds: occas. Antihistamine to sleep
» Medical: nil reported
» Psychiatric: sx of depression and anxiety, a few neuroveg. features, no suicidal ideation
» Psychophysiol: 5 yr hx of ++focus on sleep, check clock, ruminating
» RLS: no Circadian: no
Insomnia Case 1
Diagnoses:
– Major Depression with anxiety component
– Sleep hygiene factor: works til bedtime
– Psychophysiological insomnia component

Insomnia Case 1
Treatment
– Treat mood/anxiety disorder first:
» Antidepressant with anxiolytic properties
» Supportive therapy
» Review sleep hygiene principles eg. wind down
before bed

Insomnia Case 1
Treatment (cont.)
– After 2 months EMW and most
depressive/anxiety symptoms improve but sleep
initiation problem continues:
– Address conditioned component:
» Behavioral strategies: hide clock, stimulus control,
sleep consolidation
» Cognitive restructuring: address maladaptive
assumptions

Insomnia Case 1
Treatment (cont.)
– If required:
» Use short acting hypnotic for agreed upon period to
“help break cycle”
» If subsequent use required, use intermittently

Insomnia Case 1
40 year old female teacher
Unable to sleep for 5 years with worsening
over 3 months
Appears anxious
Worries she will lose job due to lack of
sleep