a preliminary clinical study using implantable...
TRANSCRIPT

11th Annual Conference of the International FES SocietySeptember 2006 – Zao, Japan
A preliminary clinical study using implantable microstimulators to facilitate recovery of upper limb function in hemiplegia
Burridge JH 1, Turk R 1, Davis R2, Cosendai G2, Sparrow O3, Roberts H3, Schulman J 1
1 University of Southampton, Southampton, SO17 1BJ, UK 2 Alfred Mann Foundation, 25134 Rye Canyon Loop #200, Santa Clarita, CA 91355 USA 3 Southampton University Hospitals NHS Trust, Southampton, SO16 6YD
AbstractThis paper presents an overview of the design of a preliminary clinical study to develop and test the feasibility of a triggered open-loop system using radio frequency controlled microstimulators. The study is in upper limb rehabilitation following stroke.
1. INTRODUCTION Approximately 75% of middle cerebral artery infarcts result in a motor deficit, particularly of the upper limb (1) and 24% of patients have residual upper limb motor loss at three months post-stroke (2). Various longitudinal studies have investigated the long-term outcome following stroke: Kwakkel in his review quotes that for 30 to 60% of patients the paretic arm remains without function (3) and Wade that half of all acute stroke patients starting rehabilitation will have a marked impairment of function of one arm of whom only about 14% will regain useful upper limb function (4). Upper limb function is clearly a major problem and the objective of this project is to develop a system that allows voluntary activation and responsive control over stimulation during functional upper limb tasks and to test the feasibility of using radio frequency controlled microstimulators (RFM)s to improve motor re-learning and recovery of arm and hand function following stroke.
De Kroon’s review (5) examined the relationship between stimulation parameters and methods of application, and improvement in upper limb function in post stroke hemiplegia. Her review found that the only factor that made a significant difference was voluntary activation of stimulation. The finding of this review supports motor learning theory which states that for motor learning to occur
activities must be repetitive, goal orientated and at the limit of performance (6). It is also supported by recent translation of animal based findings showing that enriched environments may equate with augmented therapy and relate to cortical changes associated with improved motor function (7).
Studies using voluntary activated electrical stimulation have shown improved function (8-10) but surface stimulation has usability problems. Firstly the inconvenience and accurate placement of surface electrodes and secondly the inability to selectively activate wrist extensors and the muscles controlling finger and thumb extension and thumb abduction. Implanted neuroprosthetic systems such as the freehand have effectively achieved selective activation of different muscles and muscle groups, but such systems require invasive surgery and are not intended for relatively short term therapeutic use as part of a rehabilitation programme.
This paper describes the design of a study in which we have explored the feasibility of using implantable microstimulators for recovery of upper limb function following stroke. The safety of the system(Cosendai), surgical procedure (Davis) and preliminary results of changes in function and impairment over the first 12 weeks of the study (Turk) are presented elsewhere at the conference.
2. METHODS 1.1 DesignThe study is in three phases: during the first phase we have implanted between six and seven devices in the arms of seven post-stroke hemiplegic participants to facilitate elbow, wrist, and finger and thumb extension and thumb abduction. We have designed open-loop function-based programmes that participants
– 16 –
11th Annual Conference of the International FES SocietySeptember 2006 – Zao, Japan
were able to use at home for approximately two hours per day. During this phase we developedexternal sensors, interface, control system andprogramming software to provide a responsive triggered open loop system to enable participants to perform functional arm and handmovement. During phase 2 of the study we are designing participant specific programmes - each comprising a series of activity sequencesthat enable each participant to use the system to practice functional activities. During Phase 3 participants will use the system for 12 weeks at home without further input from the research team to test the reliability and usability of the system and therapeutic effect. Participants will then discontinue using the system for 12 weeks and be re-assessed to measure long-term carry-over effect.
1.2.The microstimulatorThe RF microstimulators (RFMs), (Figure 1)used in the study have been developed by theAlfred Mann Foundation. They are injectablecylindrical microstimulators. RFMs are implanted through a small incision (5mm)under local anaesthesia using specially designedinsertion tools. Devices are positioned either adjacent to a peripheral nerve or close to amotor point within a muscle. Risks associatedwith invasive surgical procedure and the presence of leads within the body is thusreduced. Each device is individually addressed, allowing control over timing, rise and fall times, amplitude and pulse width ofstimulation. RFMs receive power supply andcontrol signals from a control unit via an inductance coil. Stimulation parameters, set by a PC based fitting system respond to triggersissued by sensors.
Figure 1. The RFM
3. RESULTS Two devices were implanted close to radial nerve branches to the medial and lateral headsof triceps (MHT and LHT) for elbow extensionand either one or two devices close to theposterior interosseous nerve (PIN) to open thethumb and fingers. Wrist extension was activated by two devices close to the motorpoints of extensor carpi ulnaris and extensor carpi radialis (ECR and ECU).
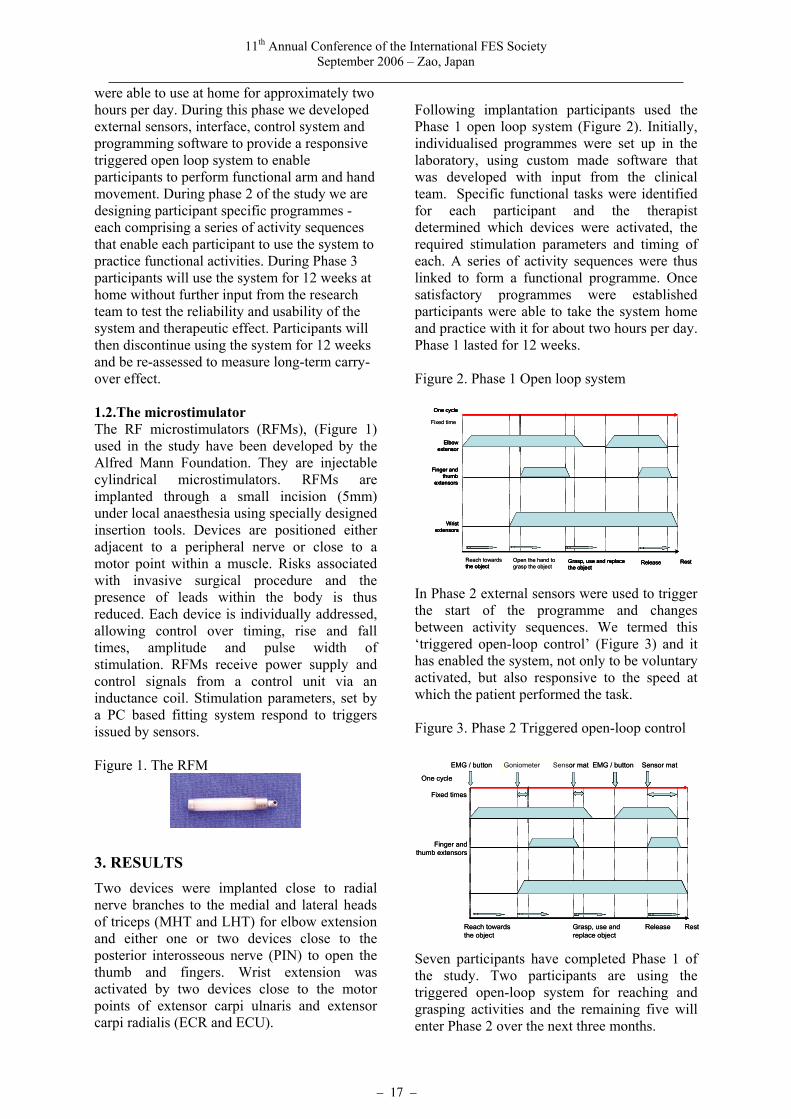
Following implantation participants used thePhase 1 open loop system (Figure 2). Initially,individualised programmes were set up in thelaboratory, using custom made software that was developed with input from the clinical team. Specific functional tasks were identified for each participant and the therapistdetermined which devices were activated, the required stimulation parameters and timing ofeach. A series of activity sequences were thus linked to form a functional programme. Once satisfactory programmes were establishedparticipants were able to take the system homeand practice with it for about two hours per day.Phase 1 lasted for 12 weeks.
Figure 2. Phase 1 Open loop system
Grasp, use and replacethe object
Release Rest
Wristextensors
One cycle
Finger andthumb
extensors
Reach towardsthe object
Open the hand tograsp the object
Elbowextensor
Fixed time
Grasp, use and replacethe object
Release Rest
Wristextensors
One cycle
Finger andthumb
extensors
the object
Elbowextensor
Grasp, use and replacethe object
Release Rest
Wristextensors
One cycle
Finger andthumb
extensors
Reach towardsthe object
Open the hand tograsp the object
Elbowextensor
Fixed time
Grasp, use and replacethe object
Release Rest
Wristextensors
One cycle
Finger andthumb
extensors
the object
Elbowextensor
In Phase 2 external sensors were used to trigger the start of the programme and changesbetween activity sequences. We termed this‘triggered open-loop control’ (Figure 3) and ithas enabled the system, not only to be voluntaryactivated, but also responsive to the speed at which the patient performed the task.
Figure 3. Phase 2 Triggered open-loop control
Grasp, use andreplace object
One cycle
Finger andthumb extensors
Reach towardsthe object
Fixed times
GoniometerEMG / button EMG / button
Release Rest
Goniometer Sensor mat Sensor mat
Grasp, use andreplace object
One cycle
Finger andthumb extensors
Reach towardsthe object
Fixed times
GoniometerEMG / button EMG / button
Release Rest
Goniometer Sensor mat Sensor mat
Seven participants have completed Phase 1 ofthe study. Two participants are using the triggered open-loop system for reaching andgrasping activities and the remaining five willenter Phase 2 over the next three months.
– 17 –

11th Annual Conference of the International FES SocietySeptember 2006 – Zao, Japan
4. DISCUSSION AND CONCLUSIONS The potential advantage of this system is that it not only allows voluntary activation of stimulation, so that it is activated on demand by the user, but also allows a greater functionality by responding without further intervention by the user to the speed of the activity.
Problems that will need to be addressed include designing a system which is quick and easy to programme so that it can be used in used by therapists in a clinical setting. If the system is shown to be feasible however it will provide exciting opportunities for employing other sensors such as EMG and for using implanted sensors that have the capability of communicating with the RFMs.
References
[1] Feys HM, De Weerdt WJ, Selz BE, Cox Steck GA, Spichiger R, Vereeck LE, et al. Effect of a therapeutic intervention for the hemiplegic upper limb in the acute phase after stroke: a single-blind, randomized, controlled multicenter trial. Stroke 1998 Apr;29(4):785-92.
[2] Parker VM, Wade DT, Langton HR. Loss of arm function after stroke: measurement, frequency, and recovery. Int Rehabil Med 1986;8(2):69-73.
[3] Kwakkel G, Kollen BJ, Wagenaar RC. Therapy impact on functional recovery in stroke rehabilitation: a critical review of the literature. Physiotherapy 1999 Jul;85(7):377-91 1999.
[4] Wade DT, Langton-Hewer R, Wood VA, Skilbeck CE, Ismail HM. The hemiplegic arm after stroke: measurement and recovery. J Neurol Neurosurg Psychiatry 1983 Jun;46(6):521-4.
[5] De Kroon JR, IJzerman MJ, Chae J, Lankhorst GJ, Zilvold G. Relation between stimulation characteristics and clinical outcome in studies using electrical stimulation to improve motor control of the upper extremity in stroke. [Review] [45 refs]. J Rehabil Med 2005 Mar;37(2):65-74.
[6] Schmidt RA, Lee TD. Motor control and learning a behavioural emphasis. 3rd Edition. 261-285. 1999. Human Kinetics Part 3 Motor Learning. Ref Type: Generic
[7] Nudo RJ. Adaptive plasticity in motor cortex: implications for rehabilitation after brain injury. J Rehabil Med 2003 May;(41 Suppl):7-10.
[8] Chae J, Fang ZP, Walker M, Pourmehdi S. Intramuscular electromyographically controlled neuromuscular electrical stimulation for upper limb recovery in chronic hemiplegia. Am J Phys Med Rehabil 2001 Dec;80(12):935-41.
[9] Francisco G, Chae J, Chawla H, Kirshblum S, Zorowitz R, Lewis G, et al. Electromyogram-triggered neuromuscular stimulation for improving the arm function of acute stroke survivors: a randomized pilot study. Arch Phys Med Rehabil 1998 May;79(5):570-5.
[10] Popovic DB, Popovic MB, Sinkjaer T, Stefanovic A, Schwirtlich L. Therapy of paretic arm in hemiplegic subjects augmented with a neural prosthesis: a cross-over study. Can J Physiol Pharmacol 2004 Aug;82(8-9):749-56.
Acknowledgements The Alfred Mann Foundation who supported this work, the patients who are involved in the study and colleagues at the University of Southampton who have provided engineering and technical support, especially Martin Warner and Dr Scott Notley.
– 18 –