a nursing informatics leadership role - himss.org20clin... · of quality informatics roles, lyda...
TRANSCRIPT

A Nursing Informatics
Leadership Role
Improving Clinical Quality
Outcomes through EHR Design,
Development, and Utilization

Lyda Gardiner – B.Sc., B.Ed., M.Ed., BSN, RN Practice Director – Quality and Performance Innovation - Jacobus Consulting
Lyda is a respected quality and clinical informatics leader, with a proven track record of spearheading strategic change to realize the full benefits of EHR enabled systems. Employing proven methodologies such as Continuous Quality Improvement, and innovative approaches such as the development of Quality Informatics roles, Lyda empowers leaders and teams to utilize their EHRs to meet Meaningful Use, Value Based Purchasing, and Accountable Care. Drawing on a strong clinical nursing foundation, deep knowledge of healthcare systems and quality methodologies, Lyda effectively creates solutions that combine operational effectiveness with knowledge and information to ensure effective outcomes and realization of strategic goals and objectives.
2

3
New workflows and documentation
requirements can be difficult for
clinicians to adopt and for EHR
vendors to support well.
Focus on Value Based
& P4P payment models
& other Quality
Outcomes programs
will increase the need
to extract actionable
data from EHRs & other
systems &
reimbursement of
organizations will be
based on data
submitted from the EHR
Incentive program goal: EHRs that
support high quality care through
new EHR-enabled workflows,
ensuring accurate, reproducible,
high quality data at individual and
aggregate level are necessary to
measure OUTCOMES OF CARE
Emerging new payment models
for health care will require “value”
over volume. Examples of such
payment models include:
•Health homes
•Accountable care organizations
•Medicare’s value-based
purchasing (pay for
performance) programs
•Core Measures
•Meaningful Use
•Inpatient/Outpatient Quality
Reporting
Accurate
patient care
documentation
across the
continuum of
care is
necessary for
reporting
OUTCOMES of
evidence
based care

4
• NI Leaders must develop & use skills in ALL informatics domains to help their organizations successfully implement & manage Quality Outcomes Programs (QOPs)
• EHR is foundational to successful QOPs which drive healthcare forward through provision of data, information & knowledge
• Design, Build & Maintenance of HCIS MUST ensure effective data/analytics
• NI competencies need to develop through all layers of the organization
Objectives
for
Today
Safe,
Timely
Equitable,
Effective,
Efficient,
Patient-
Centered
Data,
Information,
Knowledge,
Wisdom

Current Health Care Environment
2009 ARRA (American
Recovery & Reinvestment
Act) : Meaningful Use EHR
Incentives Program
Foundational to PPACA
Improve quality, safety, efficiency
Reduce health disparities
Engage patients, families in their care
Improve Care Coordination
Improve Population and Public Health
Ensure Privacy/Protection of PHI
2010 PPACA ( Patient
Protection and Affordable Care
Act) :
Accountable Care
Organizations (ACO), Value
Based Purchasing (P4P)
Provide Value
Improve Quality, control cost/efficiency
Protect Patients
Improve Safety, involve patients &
families, ensure privacy of PHI
Ensure Affordable Care
Reduce disparity, improve care
coordination, improve pop/public health 5

AHRQ: “Health IT & EHR are the Foundations
for Value & Quality” EHR Supports:
1. Quality measurement and improvement based on data from EHR
2. Optimized data collection from the EHR
3. Care coordination–EHR provides information across care continuum
4. Provides clinicians & patients with necessary info to optimize care
5. Provides timely feedback to care providers about care
6. Facilitates provision of right care & time, based on most current info
7. Allows for the comparative evaluation of treatments and interventions
8. Allows for the collection of data and information at a population level
– allowing for effective management of high-impact conditions
9. Data provides information about regional and other disparities in care
10. Value of care measurement provided by an organization, or its
component departments, or measure the value of care provided by AC0

Value Based & P4P Reimbursement
7
Payment reform that rewards
Value rather than
Volume of patient care is
a primary goal, if not THE
primary goal, of today’s
healthcare reform
How is VALUE defined?
QUALITY
OUTCOMES
+ = VALUE COST
EHR IS FOUNDATIONAL TO ACHIEVE
VALUE IN HEALTH CARE
8

Definition of Value
Value may be defined as the health
outcomes achieved per dollar spent
OR:
The Intersection of Quality & Cost
9
Quality
Cost
Value
Equilibrium
(optimal)

Relationship Between
Quality and Value…
Achieving high value for patients MUST
become the overarching goal of improved
health care delivery
Value — should define the framework for performance
improvement in health care. Rigorous, disciplined
measurement and improvement of value is the best way
to drive system progress.
10
- The New England Journal of
Medicine Michael E. Porter, Ph.D.

11
Outcomes
QUALITY
Quality Programs are Focused on Outcomes: Getting the right care
To the right patient
At the right time – Every time
to ensure the BEST Outcomes Possible
Quality Care
The IOM
Dimensions of
Quality Care are:
Safe
Timely
Effective
Efficient
Equitable
Patient Centered
12
The ability to effectively
improve Quality requires:
Ability to measure & evaluate
Structure, Processes, & Outcomes
against Quality Dimensions (use
data)
Ability to impact outcomes through
the use of Evidence
Commitment to change when a
better way is reliably identified-
Continuous Quality Improvement

Quality Department
Functions
Measure/evaluate/improve structure & process
Measure/evaluate and improve Outcomes and
the 6 Dimensions of Quality. Provide data &
improvement strategies to nursing,
physicians, & other clinical practice areas
Report data to population/condition data bases to
provide information for condition management
Report outcomes for Pay for Performance, and
other reimbursement
Provide physicians with credentialing and
performance data
Ensure continuous quality improvement –
through practice change based on evidence
(data, clinical research)
13
Methodology
Abstract Information from records
Performance Improvement (PDCA, six
sigma, lean – etc.)
Meet Evidence Based Standards for
structure, process and outcomes
(EBM/P)
Support the implementation of new
evidence for improved quality
Change Management
NEED:
Effective data gathering mechanism –
reliable EHR

14
Information &
Communications
Technology
Information
Sciences
•Codification & Taxonomy
•Collection, Organization,
Storage & retrieval of
Information, knowledge
•Interpretation
•Transmission of
information
•Human-Computer
Interaction
•Iterative design
processes
•Ways people generate,
use & find information
•Storage & Dissemination of
data
•Design and build of
systems such as HCIS,
Clinical (Business)
Intelligence & other systems
•Data Storage & Retrieval
•Focus on tools that enable
efficient: Capture, Delivery,
Transmission, & Use of data,
information, & knowledge
•Effective application of
those tools
Informatics

Nursing Informatics
15
NURSING
PRACTICE INFORMATION
TECHNOLOGY
INFORMATION
SCIENCE
•Full Scope & Practice of
Nursing, as defined by
ANA
• NI competencies for
bedside nurses, Nurse
Informaticians, & Nurse
Informatics Specialists
(graduate level education)
•Scope of NI is
commensurate with
scope of nursing practice
& nursing science with a
concentration on data,
information, & knowledge

Clinical Care (Nursing)
The Health System
Information & Communications
Technology
EXTERNAL FACTORS Value (quality + cost)
Focus on QOPs
Evidence Based Practice
Value Based Payment
New models of
reimbursement – ACO,
Medical home
Regulatory environment
ARRA/MU
INTERNAL FACTORS Increased interdisciplinary practice and patient centric processes
Coordination of Care
People, Processes, & Technology
Culture
Practice Goals for each discipline
Practice Based Evidence
Slide 16
Clinical Informatics

17
QUALITY
INFORMATICS (The study of) information use in
understanding and improving health care
quality and safety
Expert knowledge of all quality and patient
safety initiatives
Measures, regulatory expert – ensures
consistency between modules
Assists with design/development of EHR
Ensures streamlined build to facilitate
reporting
Works with end-users to ensure accurate,
reliable entry of data/information
Works with Data Architect – build, data
marts, reporting/data mining, BI solutions
Facilitates BI Maturity
Supports Quality department
transformation to HCIS
Supports Organizational transformation to
data driven/Quality Driven Organization
Practice of
Quality
Sciences
Computer
Science
Information
Science

Evidence
2 Perspectives – Both Critical for
Successful Healthcare
Transformation
18

What is Evidence Based Practice?
19
The conscientious, explicit, and
judicious practice of integrating
individual clinical expertise with the best
available clinical evidence from
systematic research in making
decisions about the care of individual
patients. DL Sackett
The integration of best-
researched evidence and
clinical expertise with patient
values Institute of Medicine Committee on Quality of
Health Care in America

20
What is Practice Based Evidence?
Applies scientific method
to the gathering and
utilization of organization
specific data
Aligns data and measurement with
organizational strategies and
performance improvement goals to
result in data driven decision
making
A structured, systematic
approach to utilizing data
obtained from your EHR to drive
decision making

Evidence Based Practice &
Practice Based Evidence
Quality Outcomes Programs (QOPs) are structured
programs of data collection with defined measures
targeted to provide data, information & knowledge
about diseases & populations that account for big
populations and/or high cost
Provide data, information & knowledge for Clinical
Decision Making, which must be coupled with Expert
Knowledge & Experience (Wisdom)
When practiced together,
form the basis of Continuous
Quality Improvement
21

Nursing Informatics & Coordination of Care
• Nurses – Most qualified, well positioned, & largest group of contributors to
healthcare services
– Best positioned to support essential clinical transformation efforts through automated clinical tools (EHRs) which will result in new care delivery models
• As nurses coordinate care – HCIS will become THE tool that facilitates effective and efficient
coordination through communication
– Real-time availability of information in the form of CDS (clinical decision support,) all of which will facilitate the real-time coordination of care (CDS combines EBP & PBE)
• Design and flow of data and information will be critical
• Build MUST – Begin with the end(s) in mind
– Be well defined and clear as to the outcomes needed – both for the patients, and for the system (remember – there is EBP with regard to HCIS systems as well as for patient care)
22

Coordination of Care (cont.) NI practitioners are
– Leaders - Designers - Facilitators - Educators -
They will help nurses gain competencies necessary to
utilize EHR at the bedside to provide the knowledge,
information, & communication needed
Nurses & the nursing profession are positioned as the most
qualified to respond to the current health system changes &
meet eHealth transformational agendas…Amara (2000)
They are the leaders who will help Nurse Executives move the
nursing agenda forward with regard to QOPs and delivery of
VALUE to all patients
23

Key Consideration
• If reimbursement is now based on VALUE, how do you know it has been delivered? – Measure of cost & other financial measures –
Finance Teams
– Measure care and treatment OUTCOMES– CLINICAL AND QUALITY PROGRAMS & DEPARTMENTS (QOPs)
• Measure – interventions, actions, treatments
• Rigorously define the way outcome is measured, controlling as many variables as possible to allow the data to be comparable and inferences to be accurate
24
Outcomes
• Are evaluated through measurements designed to
– provide actionable data
– measure the impact of a treatment, action or intervention
• Measures
– provide data & information
– Expand knowledge
– allow quantification, comparisons between organizations & practices
25
• There are hundreds of
measures, developed by
many agencies – two
examples are
• NQF – over 600 endorsed
measures
• PQRI – 153 Quality
measures

Outcomes (cont.)
• Must be measureable using EHR data
• Data and information provided must be
accurate
• Must be able to report large volumes of data
• Data fields MUST be well defined, multiple
fields must be captured, specific criteria
included or excluded
26

Quality Outcomes Programs (QOPs)
Measure sets
Are used to provide information regarding quality of care provided by an
organization
May include measures of intervention, treatment, specific practices or other
action or activity depending how they are built and utilized
Are generally a group of measures related to a specific topic, i.e. AMI,
SCIP, etc.
Along the 6 dimensions of quality
Safe
Timely
Effective
Efficient
Equitable
Patient Centered
The Quality “Measures” in
QOPs measure
Structure
Process
Outcomes
21%
30% 24%
25%
30

Quality Outcomes Programs (cont.)
Built based on evidence ranging from double-blind
clinical trials to expert consensus; provides information
on population, disease, interventions, treatments, etc.
Organizations may build Practice Based Measures;
e.g. measuring fall rates in inpatient medicated
populations over age 65
Measures form the basis for reports that are fed to
dashboard for PI, Surveillance, QOPs, upload to
national databases, & other mandatory reporting
28

Outcomes Programs are based on Measures
Formal Measures Development
Ensures
– Consistent measurement
– Defined measurements to allow comparison
of data
– Structured
Examples of Measures (see next slides)
29

Core Measures
30
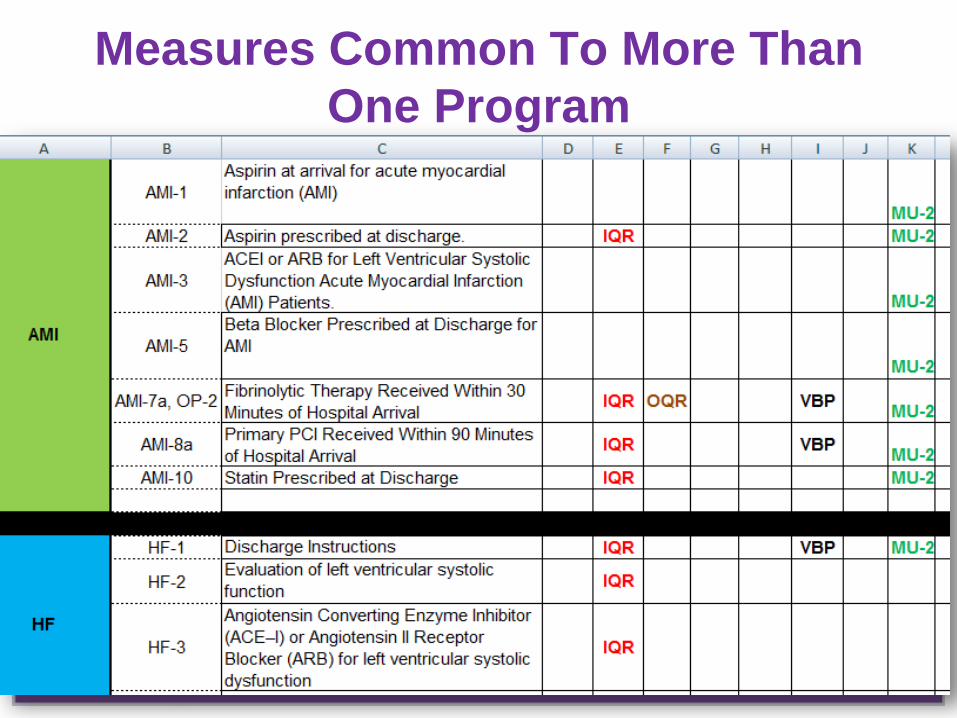
Measures Common To More Than
One Program
31

VBP Measures
32

Quality Outcomes Programs Joint Commission
In-pt/Out-pt Quality Reporting
Value Based Purchasing
AHRQ – In-pt Quality- Pt.
Safety & Pediatric Indicators
Hospital Quality Association –
In-pt indicators
Hospital Acquired Conditions
Long Term Care Hospital
Quality Indicators
Inpatient Psychiatric Facility
Quality Indicators
Meaningful Use – Stage I, II, & III –
Core, Menu & Quality Measures
National Database of Nurse
Quality Indicators
Medications
Mortality – 30
National Quality Forum – Clinical
Quality Measures
OASIS (Home Health Data Set)
Hospice Quality Measures
Inpatient Rehabilitation Quality
Indicators
33

Quality Reporting Timeline – QOPs
34

Quality Outcomes Programs
QOPs require organizations to apply a basic CQI approach to systematic change, founded on:
–Identifying a problem & Determining a measure
–Collecting Data & Reporting actual results
–Comparing actual outcomes against goal
–Comparing goal against benchmark
–Applying interventions (based on evidence) designed to improve outcomes
Legislation and national/state initiatives are requiring CQI & associated methodology through QOPs
35

Implementing Automated, Large-Scale
Quality Outcomes Programs (QOPs)
Current QOPs are frequently managed with manual data
extraction from electronic record (NDNQI, CORE Measures,
IQR, BH, ARU, etc.)
Quality team members manually extract data for representative
samples and submit to national databases
To effectively implement QOPs and the volumes of data they
require, automated data extraction from the EHR is essential
How can this be automated from the EHR?
Nursing Informatics can lead the way

Types of Issues Impacting
Automated Data Extraction
from EHR for QOPs
Key Areas Requiring Nursing
Informatics Expertise
Data Input Issues
Inconsistent build, hybrid records, multiple locations
to document the same information
Lack of awareness of where reportable data is
captured (ALL locations) so changes made accurately
Lack of knowledge of which data MUST be captured
for QOPs, regulatory, Nursing Initiatives & Nursing
Quality Improvement programs – therefore needed
fields do not exist
Lack of effective change control – fields providing
report data changed by user groups (break reports)

Data Input Issues (cont.)
• Validity – data captured in measures reports provides the correct data for
the measure
• Narrative data – reduces ability to report discrete, comparable data
• Hybrid record – data captured on paper must be manually abstracted –
cannot be automatically reported
• Reliability – Information to be documented is captured as expected
• Lack of information about data quality in the EHR
Accurate documentation capture (frequency) rates
Optimized system build opportunities
Recognized source of truth (required fields for data capture)
Related to end-user documentation reliability
To be sure information is pulled correctly & accurately for reports
Data quality assurance

Ensure EHR build supports automated QOPs
consistently
Effective data extraction begins with EHR DESIGN & BUILD
Sophisticated tools & software for data extraction / reporting will not work if data fields are
–Not present
–Not used or inconsistently used
–Too many places data can be entered into the system (documented)
–Data is captured in narrative or other formats that cannot be reported
NI Leaders MUST be PROACTIVE in their knowledge and anticipation of required data for
–QOPs such as MU, VBP, etc.
–PBE data fields for nursing or organization’s CQI programs
–Anticipation of future data needs
–Ensure optimization or other efforts don’t negatively impact automated QOP date reporting
NI leaders MUST coordinate with all experts throughout the system to ensure
–System design & build reflect the MOST EFFICIENT way to gather actionable, reportable
data for QOPs
–Synchronization with clinical workflow, data collection does not cause artificial or
extra work for clinicians in the form of data collection

Reportable Data
Identify data needed
from the system prior
to build if possible in
order to measure
outcomes
Build and develop the
EHR knowing new
requirements for
reporting will
continuously occur
MU criteria including Quality
Measures
Quality Indicators – CORE Measures,
other data sets
NDNQI measures – nurse sensitive
indicators
Other patient care indicators – defined
by external agencies or your
organization for
Performance Improvement purposes
(Quality Dept, Clinical Outcomes Dept)
TJC measures of success
Measures identified for any type of audit
Content of future QOPs (future
requirements) already available
– NI should already be working
w clinical leaders to implement &
have in place prior to required
reporting

Design and Build
NI Practitioner MUST have a much broader focus
and greater knowledge of where
All data is housed
How it is developed
Accuracy, reliability & validity (does it capture data
needed for reporting quality measures)
42
Design EHR to capture data currently available OR
needed to meet QOPs, other legislated requirements
Facilitate Performance Improvement as part of
Nursing’s CQI Methodology

• Multiple documentation locations to find the same information
• Lack of designated source of truth
• Insufficient knowledge of measurement & evaluation (data &
information needed for data to wisdom continuum) & CQI techniques
• Lack of change control - user group makes changes w/out
evaluation by team with ability to evaluate impact at all levels of the
EHR, including disabling reporting
• No records of what and when changes were made (these can
impact how far back certain types of data can be extracted)
• How / where data is stored, how long it is available for reporting
Data Output (Extraction) Issues

Ensure the EHR supports QOPs with automation
(Roadmap for QOPs)
1. Develop coordinated reporting plan Organizational Reporting & Data Access
Develop leadership dashboard
Develop department specific reporting & dashboards (PBE)
Build reports for critical/repetitively needed data/information – Quality abstracted data, Case Management data, NDNQI etc.
Start with small projects: facts, data, and information
2. Change Control
3. Coordinate like groups with regard to reports
4. NI or other informatics practitioners learn about reporting & data storage, formats of data entry to support large scale reporting
5. Determine/anticipate additional reporting needs and work with IT to meet needs (may be over time)

LOBI – Ladder of Business (Clinical)
Intelligence:
Closely parallels the Blum Model – and
makes the case for PBE/C(B)I
Enabled Intuition
Understanding
Knowledge
Information
Data
Facts
Roadmap for QOPs (cont.)
Data Plan/Program
–Data Structure and Repository Assessment
Adequate for high volume reporting
Organized approach for high volume reporting
Management, storage & retrieval mechanisms in place
–Develop Data Strategic Plan – 1, 3, 5 years
–Develop necessary expertise
•Data Architect
•Quality Informatics
Data Management Plan:
must align w/
financial/operational goals:
start small if necessary
– Data infrastructure prepared for
expanding data needs
•Data repository/Data warehouse
•Availability of data, purging, other
storage activities
•CI/BI
•Quality Informatician – Data quality
– entry to storage, to retrieval

CI - Clinical (Business) Intelligence
• CI/BI system purchase is unnecessary in the beginning
• Can grow one from SQL/data repository & other tools
• Need to develop expertise within the organization
• Need nursing/quality informatics expertise
• Eventually Data Architect, Data Strategy & Plan
• Most EHRs can report big volume data as needed for successful PBE, QOPs, Financial metrics, etc.
• CI/BI system may be added later, generally ROI is realized from organized data management & reporting for QOPs, CQI etc. & facilitates CI/BI development
Develop Methodologies To
Ensure Safe Succession
48
Safeguard knowledge about how the system
was developed, decisions made, build
strategies
Keep records of
changes and iterations
Document required
quality measures and
other quality
information in a
spreadsheet record –
such as core measures

Outpatient Quality Reporting Program
(OQR)
49
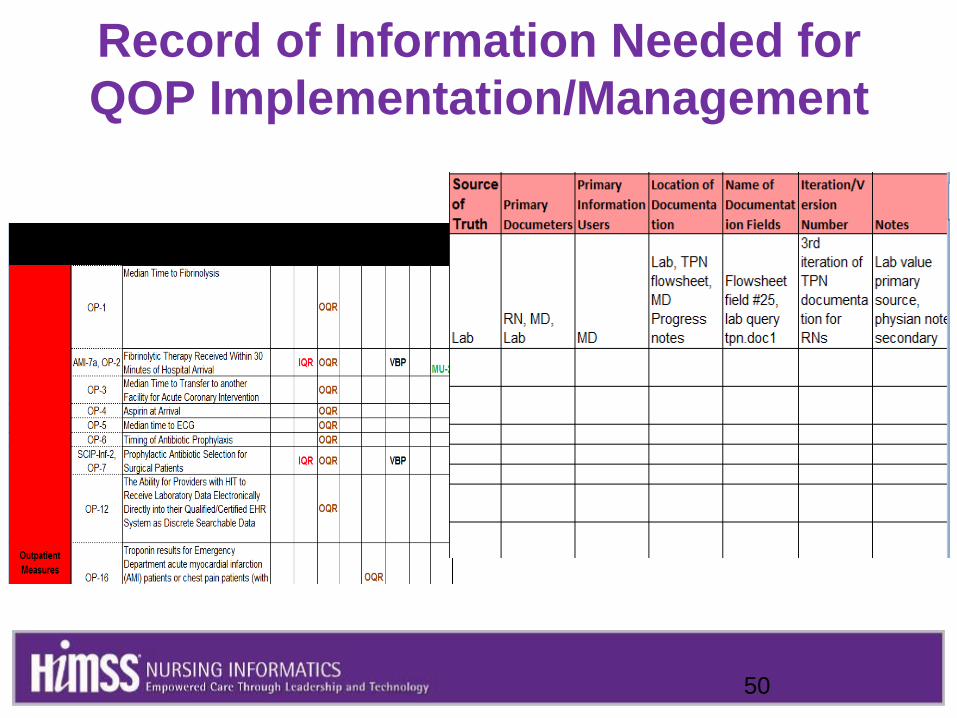
Record of Information Needed for
QOP Implementation/Management
50

Design/Develop – Structured Data Cont’d
51

Change Control Process • Effective process MUST be in place to ensure the overall integrity and
continuity of the EHR
• Generally a committee – collectively the members hold the total
knowledge about the EHR
• Changes formally presented to committee – required information about
the change documented and archived (may be several processes)
• Change evaluated against Quality, PI, Financial and other reporting to
ensure appropriate changes made to system, reporting if necessary
• Changes approved
• Changes trained, competencies documented if necessary
• Changes moved from test to live

QOPs & Nursing Informatics: Goals are Aligned
• QUALITY OUTCOMES PROGRAMS inherently move across the data-wisdom continuum (can be structure, process, outcome)
• QOPs provide PBE (practice based evidence) & are based on EBP & provide information on 2 levels
– Improve practice at the organizational level
– Provide data for future research studies on the EBP level
• Together the data and information from both PBE and EBP, when combined with other data create information and knowledge which coupled with the wisdom of nursing, or when appropriate - of interdisciplinary teams forms the basis for decision making about the care provided by the organization

QOPs & Nursing Informatics: Goals are Aligned
(cont.) Create an EHR that facilitates movement along the Data-Wisdom
Continuum fluidly and continuously
The EHR provides data, information, and knowledge of your
– Organization
– Patient populations
– Clinical practices
– QOPs
QOPs, NI Practice, Wisdom, & Experience of organizational and clinical leaders facilitates highest quality patient outcomes, and results in:
– Provision of healthcare VALUE to patients
DOMAIN of Informatics to ensure the system is designed and developed to ensure these goals can be achieved - because
The DATA to WISDOM continuum is the heart of Informatics

Proprietary & Confidential
– Jacobus Consulting
55
Data are discrete
entities that are
described objectively
without interpretations –
e.g. Vital Signs in a
single moment of time
Information is data
that are interpreted,
organized or structured –
e.g. Chronological Set of
Vital Signs
Knowledge is
information that is
synthesized so that
relationships are
identified and formalized
– e.g. synthesis of the
observed trend with
nursing knowledge
Wisdom is the appropriate use of knowledge to manage and solve human problems.
It is knowing when and how to apply knowledge to deal with complex problems or specific human needs (Nelson, 1989, 2002)
Blum, in Nelson 2002 Added by
Gardiner 2011
NI Leadership – Improving QOPs through EHR
Design & Development
Nursing Informatics can lead the way
• Nursing Informatics Leaders Must – Have a good understanding of healthcare and its impact on nursing
– Understand flow of information across the EHR and how it can support coordination of care
– Have a good understanding of measures, reporting, data quality assurance, data storage, and management
– Have a good understanding of Nursing across its breadth and depth – needs, opportunities for EBP & PBE to improve care, the organization, and nursing as a profession
• Nursing Informatics Leaders must consistently employ Quality/CQI methodologies
• Nursing Informatics Leaders must have all the skills in every Informatics domain

Current Trends & Practices
NI Practitioners Are:
• Becoming highly competent / knowledgeable of global healthcare issues, reform, EBP/PBE & making sure nursing leaders have broad perspective to effectively lead nursing both primary nursing & care coordination roles
• Excelling in CQI & PI methodologies & applying to their practice regularly
• Helping bedside RNs become aware of information / knowledge availability & utilization of PI e.g. Kaiser UBTs (PDC/SA from an older era), Cleveland Clinic etc.
• Leading the way in providing tools and systems that enable nurses as knowledge workers
NI – in large IDNs lead or participate in QOPs, PBEs, especially
related to nursing & teach NI competencies in these areas to
bedside caregivers

Needed for Care Coordination & Transformation
More than ever, NI leaders must support the transformation of nurses & their leaders into Information Users:
– Sophisticated in their desire for data, information & knowledge
– Able to apply their wisdom and experience, making the best decisions for
Their Patients
Nursing
Their Organization

Critical Success Factors For NI To Lead Quality
Outcomes Improvement
• Clear Knowledge and Understanding of all aspects of Healthcare
Informatics
• Clearly Defined Informatics Program - System-wide and interdisciplinary
• Recognize EHR as foundational for healthcare into the foreseeable future
• Ability to perform in all 3 domains of informatics in BOTH Nursing &
Clinical Informatics
• Ability to translate data & information into knowledge & supply it to the
disciplines & organizational leadership for application of wisdom &
attainment/improvement of outcomes
• Ability to apply Informatics wisdom to data, information and knowledge to
drive informatics outcomes
• Quality team - partner and support
59

Critical Success Factors For NI To Lead Quality
Outcomes Improvement (cont.)
• Clear Understanding of Healthcare – beyond department specific
understanding
– New healthcare environment
• Changes to Payment Models
• ARRA and other EHR incentives
• Advances in technology – SMART rooms and other tools
• Advances in social media and other uses of information in healthcare
– Regulatory impact and requirements
– Issues in Professional Practice
• Clearly defined job expectations
• Clearly defined and practiced accountability
• Clear understanding of the roles of care coordination & nursing in this
critical healthcare function
60

Needed for Success:
Better Understanding
of the Role of the EHR
New ways of thinking
and doing
(Innovation)
61
KNOWLEDGE – especially
about the EHR
New Roles & Practice Models
Evidence to guide practice
Understanding that change is
needed to incorporate new
and better knowledge into
practice
IMPROVE CLINICAL
QUALITY
OUTCOMES…
62
…THROUGH NURSING
INFORMATICS
LEADERSHIP OF EHR
DESIGN, DEVELOPMENT &
UTILIZATION

Questions?
63

Proprietary & Confidential
– Jacobus Consulting
64
References: •Amara, 2000 in Remus and Kennedy.. Nursing Leadership Vol 25, #4, 2012
•Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National
Academic Press
•Englebardt, Sheila PhD RN CAN; Nelson, Ramona PhD RN BC. Healthcare Informatics: An
Interdisciplinary approach. Philadelphia, PA: Elsevier Health Sciences, 2001. Print.
•Gartner, 17 September 2010. ITScore Overview for Business Intelligence and Performance
Management. Analysts: Bill Hostman,m John Hagerty
•§ Institute of Medicine Committee on Quality of Health Care in America (Sackett, D L, Straus SE,
Richardson WS, Rosenberg W, Haynes RB. Evidence-Based Medicine: How to Practice and Teach
EBM. London: Churchill Livingstone; 2000, 2001).
Quality Informatics* Wikipedia
•Nursing Informatics – The intersection of Nursing Science, Information Science, and Computer
Science – ANA (American Nurse’s Association) AHRQ – http://www.ahrq.gov/news/test031809.htm
•Quality Informatics* Wikipedia
•The New England Journal of Medicine: Perspective: What Is Value in Health Care? Michael E.
Porter, Ph.D.N Engl. J Med 2010; 363:2477-2481December 23, 2010
•White, Kenneth R., and John R. Griffith. The Well-managed Healthcare Organization. Chicago, IL:
Health Administration, 2010. Print.