a novel colorectal and cervical cancer education program: findings from the community network for...
TRANSCRIPT
A Novel Colorectal and Cervical Cancer Education Program:Findings from the Community Network for CancerPrevention Forum Theater Program
Luis O. Rustveld & Ivan Valverde & Roshanda S. Chenier &
Robert J. McLaughlin & Vicki S. Waters & John Sullivan &
Maria L. Jibaja-Weiss
Published online: 14 August 2013# Springer Science+Business Media New York 2013
Abstract Medically underserved populations continue to bedisproportionatelyburdenedbycancer.Theexact reasonfor thisdisparity has not been fully elucidated, but likely involvesmul-tiple factors. We explored the potential utility of a novelcommunity-based cancer education program called ForumTheater (FT), aimed at raising awareness about colorectal(CRC) and cervical cancer (CxC) screening among African–
American, Hispanic, and Vietnamese populations.We also de-termined audience likelihood of obtaining CRC and CxCscreening in the 6 months following performances. Thirty FTperformances were held between September 2011 and July2012. A brief survey was administered at each performance,elicitingresponsesonkeyCRCandCxCscreeningquestions.Atotal of 662 community residents (316 Hispanic, 165 African–American, and 181 Vietnamese; overall mean age 50.3±16.4)participated in performances. The survey response rate was71.1%.After seeing FT performances, the majority respondedcorrectly (>70 %) on CRC and CxC screening questions. Incomparison toHispanic andVietnamese participants, African–Americans were less likely to report that CRC and CxC arepreventable (p <0.05), that timely and regular screening saveslives (p =0.05), and that CxC screening should begin at age 21formostwomen(p <0.05).Our findingssuggest thatFTmaybean effective strategy to disseminate cancer screening informa-tion. Lack of awareness that CRC/CxC screening saveslives and that CRC/CxC is preventable, as reported byAfrican–Americans, may not stem from lack of knowledgeor misconceptions alone, but may be influenced by a senseof fatalism regarding cancer outcomes in this population.
Keywords Colorectal cancer screening . Cervical cancerscreening . Forum Theater . Medically underserved . Cancerprevention and education
Introduction
Burden of Colorectal and Cervical Cancer in Houston’s HarrisHealth System
Life expectancy and overall health have improved for thegeneral US population, including those with cancer [1].However, sectors of the population, including racial/ethnic
L. O. Rustveld (*)Department of Family and Community Medicine, Baylor CollegeofMedicine, 3701Kirby Drive, Suite 600, Houston, TX 77098, USAe-mail: [email protected]
I. Valverde : R. S. ChenierOffice of Outreach and Health Disparities, Dan L. Duncan CancerCenter, Baylor College of Medicine, One Baylor Plaza,Suite 710D, Houston, TX 77030, USA
I. Valverdee-mail: [email protected]
R. S. Cheniere-mail: [email protected]
R. J. McLaughlin :V. S. WatersSchool of Allied Health Sciences, Baylor College of Medicine,One Baylor Plaza, Suite MS: BCM115, Houston, TX 77030, USA
R. J. McLaughline-mail: [email protected]
V. S. Waterse-mail: [email protected]
J. SullivanNational Institute of Environmental Health Sciences inEnvironmental Toxicology, COEC, University of Texas MedicalBranch, 301 University Blvd, Galveston, TX 77555-1311, USAe-mail: [email protected]
M. L. Jibaja-WeissOffice of Outreach and Health Disparities, Dan L. Duncan CancerCenter, Baylor College of Medicine, One Baylor Plaza, Suite 710D,Houston, TX 77030, USAe-mail: [email protected]
J Canc Educ (2013) 28:684–689DOI 10.1007/s13187-013-0530-9

minorities, are still disproportionately burdened by cancer. Forexample, advanced colorectal cancer (CRC) stage diagnosis atHouston’s Harris Health System (HHS) accounts for approx-imately 70 % of new diagnoses, which is considerably higherthan the national proportion of 60 % [2]. African–Americanscarry a disproportionate burden of late-stage CRC seen in theHHS compared to other racial/ethnic groups; 52.9 % of HHSpatients with late-stage CRC are African–American versus23.5 % Hispanic, 14.7 % White, and 8.8 % Asian.
Similarly, African–American and Hispanic women in theHHS are more likely to ultimately die of cervical cancer (CxC)due to advanced disease stage, comorbid conditions, andinsufficient education and awareness about CxC screening.This is especially tragic since CxC is largely preventable withtimely screening. Several factors, including lack of access tocare, misconceptions, and lack of trust in health-care institu-tions, have been traditionally explored as potential contribu-tors, but do not fully explain cancer screening disparitiesobserved in this population, as Harris county residents areeligible for subsidized cancer screening and medical servicesthrough the HHS Gold Card program, regardless of income.The barriers to CxC for the majority of eligible high-riskwomen in Harris County are similar to those for CRC screen-ing—lack of awareness of risk factors and available screeningprograms in the population, and health system constraints onthe volume of services that can be delivered.
Addressing CRC and CxC Disparities in Harris CountyMedically Underserved Residents
In 2010, the Dan L. Duncan Cancer Center (DLDCC) Officeof Outreach and Health Disparities at Baylor College ofMedicine (BCM) was awarded a prevention grant from theCancer Prevention Research Institute of Texas. This project iscalled the Community Network for Cancer Prevention, whichincludes the BCM/DLDCC, BCM’s Department of Familyand Community Medicine, BCM’s Physician AssistantProgram, The University of Texas MD Anderson CancerCenter, and HHS’s Community Health Program, includingthe community health centers and three public hospitals.Other community service organizations, including HopeThrough Grace, Hope Clinic, the American Cancer Society,and Neighborhood Centers, Inc., also form part of this net-work. The purpose of this joint collaboration is to reachmedically underserved Harris County residents with CRCand CxC screening information, assist eligible residents ingaining access to HHS to receive cancer screening services,and improve follow-up appointment rates for those already inthe system. Our strategy is to develop population-specificoutreach utilizing Geographic Information Systems mappingand other methods (i.e., specific cancer indicators) to identifyhigh-risk and underserved areas in Harris County for outreachand education.
In an attempt to provide culturally and linguistically appro-priate CRC and CxC prevention education to medically un-derserved Harris County residents, it was important to takeinto consideration prevalent community attitudes and culturalbeliefs about cancer screening and prevention. In this context,we developed an interactive cancer prevention education pro-gram called the Forum Theater (FT) to stimulate communityinvolvement in problem solving around issues related to CRCand CxC screening. At the very core, FT program wasdesigned to present to the audience how demographic, psy-chosocial, cultural, and structural barriers can prevent individ-uals and families from accessing available cancer preventionand treatment services. The expectation was that dramaticrepresentation of these barriers would offer opportunities forfrank dialogue that proposed solutions.
The Origins of FT
FT originated with Brazilian playwright and director AugustoBoal. FT, an applied theater model for dialogue and problemsolving, is a component of a larger, more comprehensivedramatic system that Boal called Theater of the Oppressed[3]. The driving force behind this theater model is continueddialogue and communication between actors and audiencemembers throughout performances, thereby stimulating learn-ing about barriers to health, as well as identifying possiblesolutions.
The objectives of the current analysis are to (1) explore thepotential utility of the FT as a novel cancer prevention educa-tion tool for disseminating CRC and CxC prevention mes-sages targeted at Hispanic, African–American, andVietnamese populations residing in Harris County, Texas;(2) report on findings from postperformance surveys to assessCRC and CxC screening awareness; and (3) determine audi-ence likelihood of obtaining CRC and CxC screening in thenext 6 months following performances.
Methods
Our Approach to FT
We adapted Boal’s applied theater model to cancer preventioneducation. A principal component of our approach involvedinclusion of community health workers (CHWs) to engage theHispanic, African–American, and Vietnamese communitiesaround issues related to CRC and CxC prevention, risk man-agement, and screening. Scenes that are part of each perfor-mance use a combination of comedy and drama to engageaudience members and invite them to propose solutions as thestory unfolds. FT performances present a core conflict (i.e.,the person who does not want to get screened facing offagainst those who want him or her to get screened) and allow
J Canc Educ (2013) 28:684–689 685

audience members to actively intervene and propose solutions(i.e., presenting the information differently, correctingmiscon-ceptions, and presenting additional information) [4]. The un-derlying theory is that by incorporating physicality, commu-nication occurs nonverbally, and there is opportunity for par-ticipants to become more fully engaged.
The use of CHWs was a natural choice for this type ofoutreach as they are already fully engaged with the medicallyunderserved on a day-to-day basis and are trained to addressboth psychosocial and cultural barriers that may hinder pa-tients’ ability to obtain recommended CRC and CxC screen-ing. Three FT troupes were formed, with the troupe membersrepresenting their respective communities (Hispanic, African–American, and Vietnamese). Each troupe was led by a CHWspecifically trained to be a FT facilitator. Troupe memberswere largely volunteers from the community and were fluentin Spanish, English, or Vietnamese. They were familiar withorganizations in their communities such as churches, busi-nesses, neighborhood centers, and other organizations thatprovided services to the medically underserved on a dailybasis. Troupe members were in charge of contacting organi-zations to inquire about potential venues for FT performances.Once suitable venues were identified, venue representativeswere given flyers that advertised upcoming FT performances.Several weeks before FT performances, troupe memberscontacted venues again to get an estimate of the number ofcommunity members that expressed interest in attending FTperformances. We did not collect screening behavior datafrom participants prior to FT performances.
FT Curriculum
The FT curriculum content was guided by a comprehensivereview of the literature on CRC and CxC etiology, risk, andtreatment experience among medically underserved patients,as well as information obtained from the HHS on how theyoutreach to Harris County residents with cancer preventioneducation information. We enlisted faculty with expertise inCRC and CxC at BCM to create the CRC and CxC preventioneducation content to be disseminated at FT performances.Each FT performance included CRC and CxC preventioneducation content in the same performance. Aided byCHWs’ input, all cancer screening and prevention mes-sages were standardized across the different target popula-tions (Hispanic, African–American, and Vietnamese) toensure that the content was accurate, up to date, relevant,and culturally and linguistically appropriate. Key messagesemphasized at performances were (1) CRC and CxCscreening tests can detect cancer early, and (2) early detec-tion of cancer can result in lower morbidity and mortalitytypically associated with late-stage diagnosis. The follow-ing key barriers to CRC and CxC screening were alsoaddressed at each FT performance: (1) talking about CRC
and CxC is difficult; (2) misconceptions regarding basicprevention messages are prevalent, despite long-term ef-forts at education using other methods; and (3) mistrust ofmedical establishment and systemic barriers to care preventmany people from seeking screening.
FT Training
Training took place once a week for 7 weeks, with 16 peoplein attendance. The first training session included evidence-based CRC and CxC content education. The remaining6 weeks focused on FT methods from a recognized localexpert on the FT process, which consisted of techniques suchas trust exercises, improvisation, scene building and flow, andencouraging audience participation [5]. Throughout the train-ing, participants developed skills for addressing barriers andmyths related to cancer screening and prevention, as well ashow to address these issues with community members. Aftercompleting training sessions, CHWs became involved inidentifying and coordinating locations for performances. TheFT troupes then assemble in these communities which aredisproportionately affected by CRC and CxC in HarrisCounty.
FT Performances
A total of 30 FT performances were held between September2011 and July 2012 in our three target populations. In order tomaximize outreach to those most affected by CRC and CxC,all venues for the FT performances were chosen using a prioridefined criteria (local sociodemographic characteristics andlevel of cancer burden in that community). Venues includedchurches, community centers, and schools. All performanceswere conducted in the language spoken by the targeted com-munities (English, Spanish, and Vietnamese). A brief post-FTsurvey consisting of ten questions, excluding demographics,was administered to assess participants’ knowledge andawareness about key CRC and CxC screening facts. Thissurvey was administered once after each performance. Forexample, “Colon and cervical cancer are preventable.”Participants rated the cancer knowledge questions as 1 (Yes),2 (No), and 3 (Not sure). Likelihood of future screening wasassessed retrospectively after FT performances with two ques-tions: (1) “Before seeing the play, how likely were you to havea colon (FIT or colonoscopy) or cervical cancer screening(PAP) test in the next 6 months?” and (2) “After seeing theplay, how likely are you to have a colon or cervical cancerscreening test in the next 6 months?” These questions wererated from 1 (Definitely) to 3 (Not at all). Age- and gender-specific CRC and CxC screening questions were added to thesame questionnaire. All participants who filled out surveysanswered all questions, regardless of age or gender eligibilityfor CRC and CxC screening.
686 J Canc Educ (2013) 28:684–689
Data Analysis
All survey data were entered into Excel spreadsheets and laterformatted as SPSS files in preparation for analysis. Categoricalvariables were summarized by frequencies, and continuousvariables, by means and standard deviations; statistically sig-nificant differences were determined by Chi square analysisand Student’s t test. We obtained age- and gender-specificresponses to CRC and CxC screening questions by performingcrosstabs between age group, gender, and each cancer screen-ing question. Differences in means for continuous variablesacross the three target populations (Hispanic, African–American, and Vietnamese) were determined with the use ofanalysis of variance.
Results
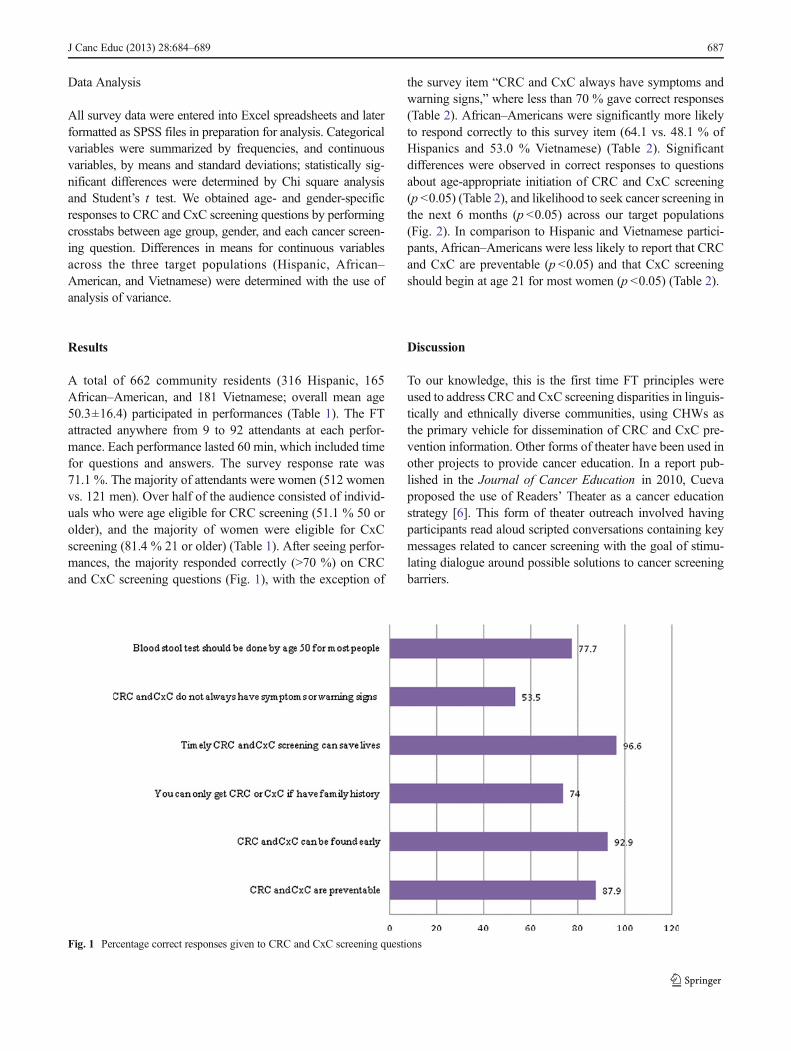
A total of 662 community residents (316 Hispanic, 165African–American, and 181 Vietnamese; overall mean age50.3±16.4) participated in performances (Table 1). The FTattracted anywhere from 9 to 92 attendants at each perfor-mance. Each performance lasted 60 min, which included timefor questions and answers. The survey response rate was71.1 %. The majority of attendants were women (512 womenvs. 121 men). Over half of the audience consisted of individ-uals who were age eligible for CRC screening (51.1 % 50 orolder), and the majority of women were eligible for CxCscreening (81.4 % 21 or older) (Table 1). After seeing perfor-mances, the majority responded correctly (>70 %) on CRCand CxC screening questions (Fig. 1), with the exception of
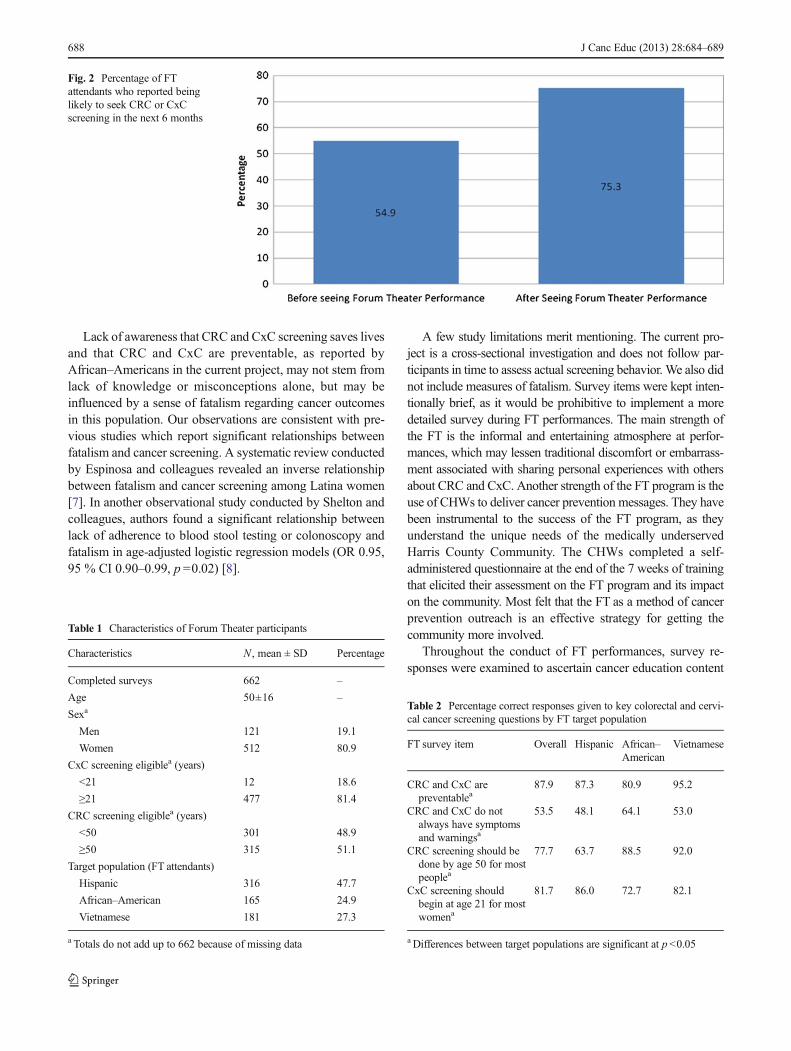
the survey item “CRC and CxC always have symptoms andwarning signs,” where less than 70 % gave correct responses(Table 2). African–Americans were significantly more likelyto respond correctly to this survey item (64.1 vs. 48.1 % ofHispanics and 53.0 % Vietnamese) (Table 2). Significantdifferences were observed in correct responses to questionsabout age-appropriate initiation of CRC and CxC screening(p <0.05) (Table 2), and likelihood to seek cancer screening inthe next 6 months (p <0.05) across our target populations(Fig. 2). In comparison to Hispanic and Vietnamese partici-pants, African–Americans were less likely to report that CRCand CxC are preventable (p <0.05) and that CxC screeningshould begin at age 21 for most women (p <0.05) (Table 2).
Discussion
To our knowledge, this is the first time FT principles wereused to address CRC and CxC screening disparities in linguis-tically and ethnically diverse communities, using CHWs asthe primary vehicle for dissemination of CRC and CxC pre-vention information. Other forms of theater have been used inother projects to provide cancer education. In a report pub-lished in the Journal of Cancer Education in 2010, Cuevaproposed the use of Readers’ Theater as a cancer educationstrategy [6]. This form of theater outreach involved havingparticipants read aloud scripted conversations containing keymessages related to cancer screening with the goal of stimu-lating dialogue around possible solutions to cancer screeningbarriers.
Fig. 1 Percentage correct responses given to CRC and CxC screening questions
J Canc Educ (2013) 28:684–689 687
Lack of awareness that CRC and CxC screening saves livesand that CRC and CxC are preventable, as reported byAfrican–Americans in the current project, may not stem fromlack of knowledge or misconceptions alone, but may beinfluenced by a sense of fatalism regarding cancer outcomesin this population. Our observations are consistent with pre-vious studies which report significant relationships betweenfatalism and cancer screening. A systematic review conductedby Espinosa and colleagues revealed an inverse relationshipbetween fatalism and cancer screening among Latina women[7]. In another observational study conducted by Shelton andcolleagues, authors found a significant relationship betweenlack of adherence to blood stool testing or colonoscopy andfatalism in age-adjusted logistic regression models (OR 0.95,95 % CI 0.90–0.99, p =0.02) [8].
A few study limitations merit mentioning. The current pro-ject is a cross-sectional investigation and does not follow par-ticipants in time to assess actual screening behavior. We also didnot include measures of fatalism. Survey items were kept inten-tionally brief, as it would be prohibitive to implement a moredetailed survey during FT performances. The main strength ofthe FT is the informal and entertaining atmosphere at perfor-mances, which may lessen traditional discomfort or embarrass-ment associated with sharing personal experiences with othersabout CRC and CxC. Another strength of the FT program is theuse of CHWs to deliver cancer prevention messages. They havebeen instrumental to the success of the FT program, as theyunderstand the unique needs of the medically underservedHarris County Community. The CHWs completed a self-administered questionnaire at the end of the 7 weeks of trainingthat elicited their assessment on the FT program and its impacton the community. Most felt that the FT as a method of cancerprevention outreach is an effective strategy for getting thecommunity more involved.
Throughout the conduct of FT performances, survey re-sponses were examined to ascertain cancer education content
Fig. 2 Percentage of FTattendants who reported beinglikely to seek CRC or CxCscreening in the next 6 months
Table 1 Characteristics of Forum Theater participants
Characteristics N , mean ± SD Percentage
Completed surveys 662 –
Age 50±16 –
Sexa
Men 121 19.1
Women 512 80.9
CxC screening eligiblea (years)
<21 12 18.6
≥21 477 81.4
CRC screening eligiblea (years)
<50 301 48.9
≥50 315 51.1
Target population (FT attendants)
Hispanic 316 47.7
African–American 165 24.9
Vietnamese 181 27.3
a Totals do not add up to 662 because of missing data
Table 2 Percentage correct responses given to key colorectal and cervi-cal cancer screening questions by FT target population
FT survey item Overall Hispanic African–American
Vietnamese
CRC and CxC arepreventablea
87.9 87.3 80.9 95.2
CRC and CxC do notalways have symptomsand warningsa
53.5 48.1 64.1 53.0
CRC screening should bedone by age 50 for mostpeoplea
77.7 63.7 88.5 92.0
CxC screening shouldbegin at age 21 for mostwomena
81.7 86.0 72.7 82.1
a Differences between target populations are significant at p <0.05
688 J Canc Educ (2013) 28:684–689

needing reinforcement. For example, less than 70 % of the FTaudience gave correct responses to the survey item “CRC andCxC always have symptoms and warning signs.” Since then,each FT troupe attended retraining sessions in which CRC andCxC education content were reviewed, and particular empha-sis was placed on conveying to the FTaudience that CRC andCxC do not always exhibit symptoms and warning signs.
In conclusion, our findings suggest that FT may be aneffective strategy to disseminate cancer screening informationto ethnically and linguistically diverse populations. However,further studies that include a true pre–posttest design areneeded to measure changes in knowledge, as well as theinclusion of a formal follow-up period to determine whetherFT participants actually seek and obtain CRC and CxCscreening after seeing a performance.
Acknowledgments This project was funded by the Cancer Preventionand Research Institute of Texas (CPRITAward PP100201).
References
1. US Department of Health and Human Resources (2006) US Depart-ment of Health and Human Resources fact sheet. http://www.hhs.gov/news/factsheet/minorityhealth.html. Accessed on October 29, 2012
2. Rim SH, Seeff L, Ahmed F, King JB, Coughlin SS (2009) Colorectalcancer incidence in the United States, 1999–2004. Cancer 115(9):1967–1976
3. Boal A (1993) Theater of the oppressed. Theatre CommunicationsGroup, New York. ISBN 0-930452-49-6
4. Boal A (1995) The rainbow of desire: the Boal method of theatre andtherapy, 2nd edn. Routledge, New York, 336 p
5. Boal A (1992) Games for actors and non-actors, 2nd edn. Routledge,New York, 336 p
6. Cueva M, Kuhnley R, Lanier A et al (2005) Using theater to promotecancer education in Alaska. J Cancer Educ 20:45–48
7. Espinosa de los Monteros K, Gallo LC (2010) The relevance offatalism in the study of Latinas’ cancer screening behavior: a system-atic review of the literature. Int J Behav Med 18:310–318
8. Shelton RC, Jandorf L, Ellison J, Villagra C, DuHamel KN (2011) Theinfluence of sociocultural factors on colonoscopy and FOBTscreeningadherence among low-income Hispanics. J Health Care Poor Under-served 22(3):925–944
J Canc Educ (2013) 28:684–689 689