a nabh accredited hospital care plus · from max super speciality hospital, phase vi, mohali a nabh...
TRANSCRIPT

Dr. N M Gupta• Former HOD, Dept. of General Surgery,
PGI, Chandigarh
• Pioneer in developing Transhiatal Esophagectoym in India
• Gastro Intestinal Surgery & Oncology
Dr. M S Bedi• Hepato-pancreatic-biliary surgery
• Gastro Intestinal Oncology
• Bariatric & Metabolic Surgery
• Advanced laparoscopic Surgery-colorectal, upper GI and biliary surgery
• Thoracoscopic Surgery for esophagus
Dr. K S Dhillon• Bariatric surgery
• Basic and advanced laparoscopic surgery
• Single incision/scar less laparoscopic surgery
• Day care laparoscopic surgery for Hernia, GB, Appendix, Gynaecologic surgery
• Pioneer in 1cm incision Laparoscopic surgery for Ulterus, GB & appendix
Area ofSpecialization
Vol. I Issue 3
SPECIAL ISSUE ON GENERAL SURGERY
Care PlusA Monthly New
From Max Super Speciality Hospital, Phase VI, Mohali
A NABH Accredited Hospital
sletter
Dr. N M GuptaPrincipal Consultant-SurgeonGeneral Surgery & Academic Coordinator
DYSPHAGIADysphagia is a greek word, meaning disordered or difficult (dys) eating (phagiein) and refers to the sensation of food being hindered in its normal passage from mouth to the stomach. The symptom is usually described as a sensation in which the food “sticks, get caught, hung up, does not go down or even feel funny going down.”
Dysphagia is classically divided into two syndromes. 1. Oropharyngeal dysphagia – It is described as an inability to initiate the act of swallowing and is due to impaired ability to transfer the bolus from the mouth to the upper esopahgus. 2. Esophageal dysphagia- refers to difficulty with the transport of ingested material down the
esophagus.
The second type of dysphagia will be the main focus of discussion.
ETIOLOGY OF DYSPHAGIA A. Motility disorders a. Achlasia b. Diverticulum c. Scleroderma d. Diffuse spasm e. Chaga’s diseases B. Mechanical disorders a. Intrinsic i. Carcinomacii. Corrosive iii. Foreign body iv. Peptic stricture v. Rings /webs b. Extrinsic i. Vascular ii. Mediastinal tumor iii. Cervical osteoarthritis
DIAGNOSIS The old axiom that most diagnosis can be made on the basis of good history is nowhere more true than in the evaluation of esophageal diseases.
The following vital questions should be ascertained initially A. History of corrosive intake?B. History of FB ingestion?C. What kind of food (liquid or solid) produce symptoms?D. Is dysphagia intermittent or progressive?E. Is there associated heartburn?
On the basis of answers to these questions, the diagnosis can be made in the large majority of cases.Upper GI endoscopy and biopsy can confirm the diagnosis. Various radiological investigations e.g, CECT with oral contrast and EUS helps in delineating the extent of the tumor. Barium swallow ( esp. Double contrast) is useful for benign lesion.

STITCHLESS SINGLE INCISION LAPAROSCOPICHYSTERECTOMY (UTERUS REMOVAL)
The newest advancement in Gyane Surgery is single port hysterectomy SILS(single incision/cut laparoscopic surgery). It
replaces the three to four port/incision made in standard laparoscopy with just one incision of less than 1cm in
belly button. It leads to no scar – SCARLESS\STITCHLESS HYSTERECTOMY.
It has high cosmetic score and minimal pain. It is a daycare procedure-Patient can be discharged same day. There is a less risk of port site infection and injury to abdominal wall nerves and blood vessels. It is scarless, no Keloid formation and reduced risk of hernia. Post operative requirement for antibiotics and pain killers is reduced so that their side effects are avoided. Patient can quickly resume the work. All this leads to cost
reduction and in total it is more cost effective.Nowdays well aware ,NRI patients ,models and
film stars are opting for this particular type of operation. Stitchless Single Incision laparoscopic
Hysterectomy is a better and safe procedure for uterus removal but can only be done by very experienced team
of Surgeons. It can be combined with other surgeries like Gallbladder, Appendix etc.
it is becoming pandemic involving substantial population in developing world. Obesity brings with it many diseases that decrease life span and also quality of life thus increasing economic burden of healthcare system. The annual cost of managing obesity in United States is around $100 billion, out of which around $52billion is direct cost to healthcare system.
MEASUREMENT OF OBESITY Obesity represents a state of excessive storage of fat. In healthy
individuals, fat composes around 15-20% of body weight in
males and 25-30% in females. Because the difference in body
weight is only partly due to body fat variations, body weight is a
limited although easily obtained index of obesity. In general Body
mass index is used commonly to quantify obesity as it correlates
closely to body fat in most settings. It is calculated as
BMI ( Body Mass Index)= weight in kilograms/ (height in meters)²
Although BMI is closely related to body fat but there exist
caveats that preclude its use in accurate measurement of body
fat. There are many other methods of accurately measuring body
fat but are cumbersome hence BMI is most commonly being
taken as index of total body fat.
Classification of obesity
World health organization has classified obesity with risk
quantification of co morbidities as follows
Dr. M S BediSenior Consultant,MAMBS & GI Surgery
Dr. K S DhillonSenior Consultant,Advanced Laparoscopic & Bariatric Surgery
Dr. Divya AwasthiAssociate Consultant Gynae Laparoscopy & Hysteroscopy
OPEN 3-5 INCISIONLAPAROSCOPY
OPENSURGERY
SINGLE INCISIONLAPAROSCOPY
LARGE(8-10CM)
1. INCISION /CUT SIZE3-4 PUNCTURES OF
5-10MMSINGLE<1CM
2-3 WEEKS2. RECOVERY TIME 5-10 DAYS 1-2DAYS
MORE3. BLOOD LOSS/BLOOD VESSEL INJURY
LESS MINIMAL
UGLY4. SCAR/COSMESISPRESENT, MAY BE
UGLYSCARLESS EXCELLENT
COSMESIS
COMMON5. HERNIA AND INFECTION
LESS VERY MINIMAL
SEVERE ANDCOMMON
6. PAIN / NERVE DAMAGE
MODERATE ANDCOMMON
VERY MINIMAL
Single incision lap surgery
ACHLASIA Achlasia cardia is a motor disorder of the esophagus characterised by the loss of esophageal peristalsis and high pressure incompletely relaxing lower esophageal sphincter. The major histologic changes are loss of ganglion cells within the myenteric plexus and degeneration of vagus nerve. The most common initial complaint is progressive dysphagia to liquids. The solid food travels down by gravity. Regurgitation of undigested food especially at night is a common complaint. Barium swallow and endoscopic examination can confirm the diagnosis.
Achalsia can be treated 1. Medically by endoscopic balloon dilatation but it carries the risk
of esophageal disruption. Moreover risk of recurrence is high. Botulinum injection in LES has been given up due to high rates of recurrence.
2. Surgery - Cardiomyotomy ( heller’s myotomy) performed by open or laparoscopy (MAS) is the treatment of choice. In advanced cases massive oesophageal dilatation (megaesophagus), oesophageal resection is the treatment of choice.
CARCINOMAIt is quite prevalent in this country. Painless progressive dysphagia in the absence of any history of ingestion of foreign body or corrosive agent is almost diagnostic. Unfortunantely, the onset of dysphagia is also indicative of advanced disease as it initiate only if the blockage is more than 80% of lumen. UGIE and biopsy can confirm the diagnosis. CECT, PET and EUS help in delineating the extent and spread of the disease.
Despite various advances in surgery, chemo and radiotherapy, the prognosis of cancer esophagus still remains dismal. Surgical resection (esophagectomy) still carries a high morbidity and mortality at the centres where this surgery is carried out less frequently. Oesophageal resection provides the best palliation and restoration of lasting deglutition. Neo adjuvant (pre- operative) chemoradiotherapy has been found to be useful for the increased number of resection and better median survival. Newer modalities of chemoradiaotherapy combined with minimally invasive surgery for carcinoma esophagus has improved survival world over with decrease in morbidity and mortality.
Surgery for uterus has evolved from traditional abdominal /vaginal hysterectomy to LAVH(LAPAROSCOPIC ASSISTED VAGINAL HYSTERECTOMY) to TLH (TOTAL LAPAROSCOPIC HYSTERECTOMY). And now with ongoing refinement of surgical techniques and instrumentation begins the era of single port scarless hysterectomy.Minimally invasive Gyane surgery has become a standard of care for the treatment of many benign
and cancerous gynecological conditions. This has improved the complication rate and cosmesis and surgical technique as compared to the traditional open abdominal surgeries. Post surgery adhesions(no direct handling of intra abdominal organs)are less hence lower complications and if any other surgery is required later in life and it is much easier. There are innumerable advantages of laparoscopic surgery and it is safe in experienced hands. The major benefits are reduced post operative pain, decreased hospital stay , quicker recovery and return to normal physical activities, reduced blood loss, improved cosmesis (no large scar) and less wound complications . The advantage of magnification and to be able to reach deep in pelvis helps immensely in cancer surgery which is now routinely being done laparoscopically.
All such modern amenities such as surgical facilities, chemotherapy, radiotherapy and ICU facilities are available at the MAX Hospital, Mohali.
Many patients have benefitted from this approach at our centre and there are many cases that have shown complete regression of cancer after neoadjuvant chemo radiotherapy in specimens resected by minimally invasive way.
DividedOesophageal muscle
Oesphageal Lining
Laparoscopic cardiomyotomy with or without antireflux measures forms the
gold standard for the treatment of achlasia today. At Max Hospital, Mohali we have expertise to perform every kind
of treatment deemed fit for patient.Lap. Cardiomyotomy
Thoracoscopic ports Abdominal ports
Intrathoracic anastomosis Encircling esophagus
OBESITY – THE FUTURE DISASTER
Classification
Underweight
Normal range
Overweight
Pre-obesecreased
Obese class 1
Obese class 2
Obese class 3
Comorbidity risk
Above action level 1
Above action level 2
BMI (kg/m2)
< 18.5\
18.5 to 24.9
25
25.0 to 29.9
30.0 to 34.9
35.0 to 39.9
40.0
Women
80
88
Men
94
102
Risk of comorbidities
Low (but risk of other
clinical problems increased)
Average
Increased
Moderate
Severe
Very severe
Waist circumference (cm)
Obesity is a substantial health crisis is emerging all over the world. Initially it was mainly confined to developed nations but now
All the surgical procedures are performed by minimally invasive procedures thoracoscopic and laparoscopic). It entails less surgical trauma resulting in early recovery with less chances of postoperative infection. Excellent ICU facilities and minimal access approach are a boon for rapid recovery in such cases.
Open Surgery scar Single incision surgery using SILS Port
Max Super Speciality Hospital, Mohali is empanelled by ECHS, ESIC,Haryana Govt and all Major TPA’s & Corporates.
For any query please contact us at: [email protected]
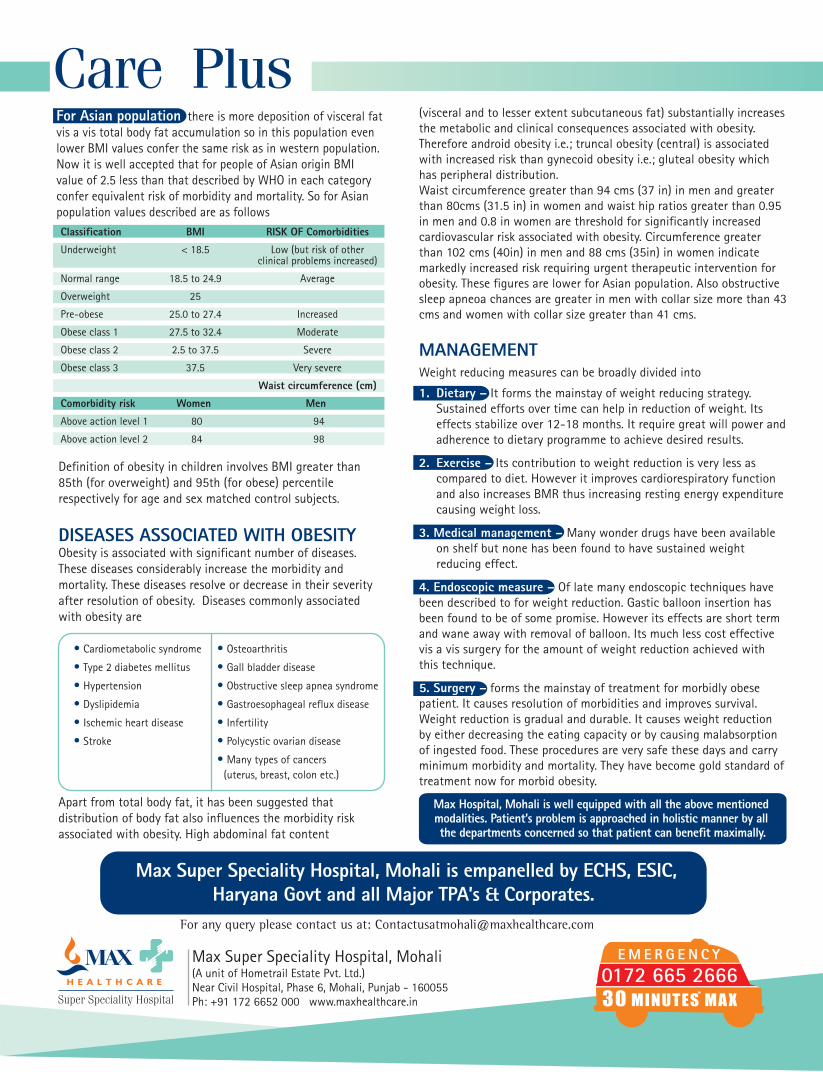
For Asian population there is more deposition of visceral fat vis a vis total body fat accumulation so in this population even lower BMI values confer the same risk as in western population. Now it is well accepted that for people of Asian origin BMI value of 2.5 less than that described by WHO in each category confer equivalent risk of morbidity and mortality. So for Asian population values described are as followsClassification BMI RISK OF Comorbidities
Underweight < 18.5 Low (but risk of other clinical problems increased)
Normal range 18.5 to 24.9 Average
Overweight 25
Pre-obese 25.0 to 27.4 Increased
Obese class 1 27.5 to 32.4 Moderate
Obese class 2 2.5 to 37.5 Severe
Obese class 3 37.5 Very severe
Waist circumference (cm)
Comorbidity risk Women Men
Above action level 1 80 94
Above action level 2 84 98
Definition of obesity in children involves BMI greater than 85th (for overweight) and 95th (for obese) percentile respectively for age and sex matched control subjects.
DISEASES ASSOCIATED WITH OBESITY Obesity is associated with significant number of diseases. These diseases considerably increase the morbidity and mortality. These diseases resolve or decrease in their severity after resolution of obesity. Diseases commonly associated with obesity are
• Cardiometabolic syndrome
• Type 2 diabetes mellitus
• Hypertension
• Dyslipidemia
• Ischemic heart disease
• Stroke
• Osteoarthritis
• Gall bladder disease
• Obstructive sleep apnea syndrome
• Gastroesophageal reflux disease
• Infertility
• Polycystic ovarian disease
• Many types of cancers (uterus, breast, colon etc.)
Apart from total body fat, it has been suggested that distribution of body fat also influences the morbidity risk associated with obesity. High abdominal fat content
(visceral and to lesser extent subcutaneous fat) substantially increases the metabolic and clinical consequences associated with obesity. Therefore android obesity i.e.; truncal obesity (central) is associated with increased risk than gynecoid obesity i.e.; gluteal obesity which has peripheral distribution. Waist circumference greater than 94 cms (37 in) in men and greater than 80cms (31.5 in) in women and waist hip ratios greater than 0.95 in men and 0.8 in women are threshold for significantly increased cardiovascular risk associated with obesity. Circumference greater than 102 cms (40in) in men and 88 cms (35in) in women indicate markedly increased risk requiring urgent therapeutic intervention for obesity. These figures are lower for Asian population. Also obstructive sleep apneoa chances are greater in men with collar size more than 43 cms and women with collar size greater than 41 cms.
MANAGEMENT Weight reducing measures can be broadly divided into
1. Dietary – It forms the mainstay of weight reducing strategy. Sustained efforts over time can help in reduction of weight. Its effects stabilize over 12-18 months. It require great will power and adherence to dietary programme to achieve desired results.
2. Exercise – Its contribution to weight reduction is very less as compared to diet. However it improves cardiorespiratory function and also increases BMR thus increasing resting energy expenditure causing weight loss.
3. Medical management – Many wonder drugs have been available on shelf but none has been found to have sustained weight reducing effect.
4. Endoscopic measure – Of late many endoscopic techniques have been described to for weight reduction. Gastic balloon insertion has been found to be of some promise. However its effects are short term and wane away with removal of balloon. Its much less cost effective vis a vis surgery for the amount of weight reduction achieved with this technique.
5. Surgery – forms the mainstay of treatment for morbidly obese patient. It causes resolution of morbidities and improves survival. Weight reduction is gradual and durable. It causes weight reduction by either decreasing the eating capacity or by causing malabsorption of ingested food. These procedures are very safe these days and carry minimum morbidity and mortality. They have become gold standard of treatment now for morbid obesity.
Max Hospital, Mohali is well equipped with all the above mentioned modalities. Patient’s problem is approached in holistic manner by all the departments concerned so that patient can benefit maximally.