a multidisciplinary approach to full mouth rehabilitation...
TRANSCRIPT
Case Report
Full mouth rehabilitation & Dilemma of Wriggling Dentures...Nidawani P et al Journal of International Oral Health 2014; 6(2):136-140
Received: 15th August 2013 Accepted: 21st February 2014 Conflict of Interest: None
Source of Support: Nil
A Multidisciplinary Approach to Full Mouth Rehabilitation and Solving the Dilemma ofWriggling Dentures- A Case ReportPrakash Nidawani1, Girish Galagali2, E Srinivas Reddy1, Sidhartha S P Behera3
136
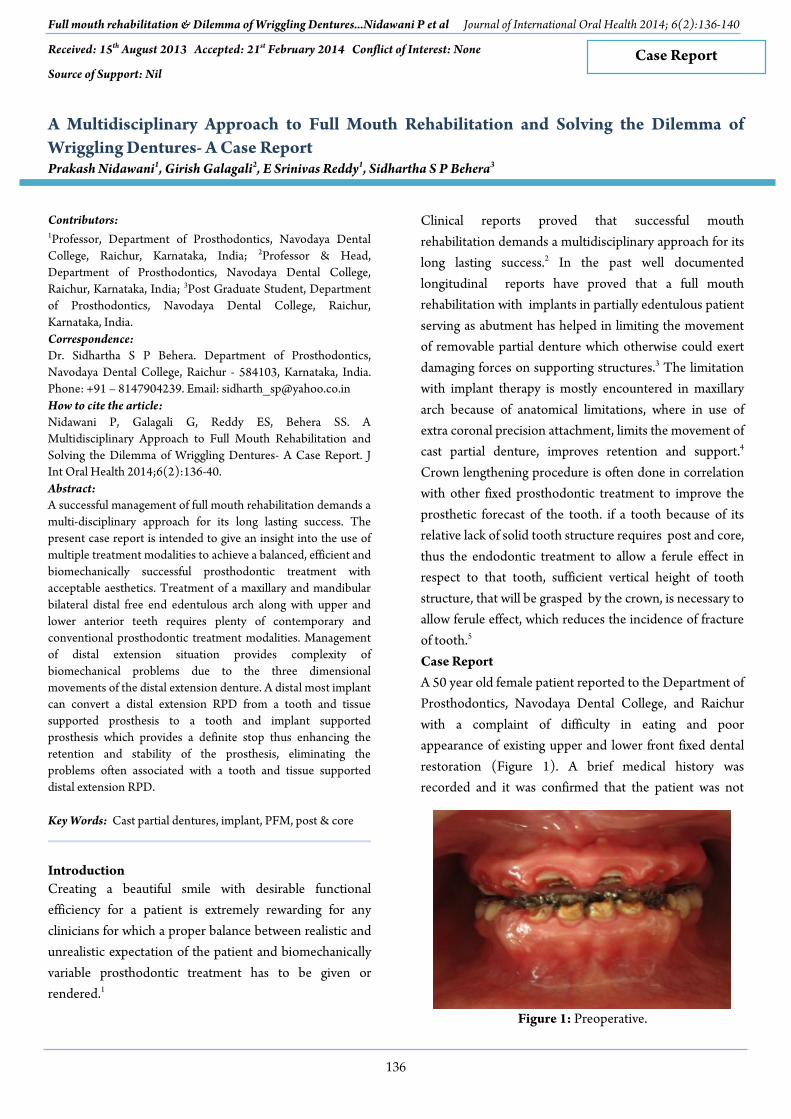
Figure 1: Preoperative.
Contributors:1Professor, Department of Prosthodontics, Navodaya DentalCollege, Raichur, Karnataka, India; 2Professor & Head,Department of Prosthodontics, Navodaya Dental College,Raichur, Karnataka, India; 3Post Graduate Student, Departmentof Prosthodontics, Navodaya Dental College, Raichur,Karnataka, India.Correspondence:Dr. Sidhartha S P Behera. Department of Prosthodontics,Navodaya Dental College, Raichur - 584103, Karnataka, India.Phone: +91 – 8147904239. Email: [email protected] to cite the article:Nidawani P, Galagali G, Reddy ES, Behera SS. AMultidisciplinary Approach to Full Mouth Rehabilitation andSolving the Dilemma of Wriggling Dentures- A Case Report. JInt Oral Health 2014;6(2):136-40.Abstract:A successful management of full mouth rehabilitation demands amulti-disciplinary approach for its long lasting success. Thepresent case report is intended to give an insight into the use ofmultiple treatment modalities to achieve a balanced, efficient andbiomechanically successful prosthodontic treatment withacceptable aesthetics. Treatment of a maxillary and mandibularbilateral distal free end edentulous arch along with upper andlower anterior teeth requires plenty of contemporary andconventional prosthodontic treatment modalities. Managementof distal extension situation provides complexity ofbiomechanical problems due to the three dimensionalmovements of the distal extension denture. A distal most implantcan convert a distal extension RPD from a tooth and tissuesupported prosthesis to a tooth and implant supportedprosthesis which provides a definite stop thus enhancing theretention and stability of the prosthesis, eliminating theproblems often associated with a tooth and tissue supporteddistal extension RPD.
Key Words: Cast partial dentures, implant, PFM, post & core
IntroductionCreating a beautiful smile with desirable functionalefficiency for a patient is extremely rewarding for anyclinicians for which a proper balance between realistic andunrealistic expectation of the patient and biomechanicallyvariable prosthodontic treatment has to be given orrendered.1
Clinical reports proved that successful mouthrehabilitation demands a multidisciplinary approach for itslong lasting success.2 In the past well documentedlongitudinal reports have proved that a full mouthrehabilitation with implants in partially edentulous patientserving as abutment has helped in limiting the movementof removable partial denture which otherwise could exertdamaging forces on supporting structures.3 The limitationwith implant therapy is mostly encountered in maxillaryarch because of anatomical limitations, where in use ofextra coronal precision attachment, limits the movement ofcast partial denture, improves retention and support.4
Crown lengthening procedure is often done in correlationwith other fixed prosthodontic treatment to improve theprosthetic forecast of the tooth. if a tooth because of itsrelative lack of solid tooth structure requires post and core,thus the endodontic treatment to allow a ferule effect inrespect to that tooth, sufficient vertical height of toothstructure, that will be grasped by the crown, is necessary toallow ferule effect, which reduces the incidence of fractureof tooth.5
Case ReportA 50 year old female patient reported to the Department ofProsthodontics, Navodaya Dental College, and Raichurwith a complaint of difficulty in eating and poorappearance of existing upper and lower front fixed dentalrestoration (Figure 1). A brief medical history wasrecorded and it was confirmed that the patient was not

Full mouth rehabilitation & Dilemma of Wriggling Dentures...Nidawani P et al Journal of International Oral Health 2014; 6(2):136-140
137
Figure 2: Crown Lengthening Post and Core,ToothPreparation.
Figure 3: Temporisation.
Figure 4: Opgafter Implant Placement.
Figure 5: Ball Abutments in Lower Molar Region.
Figure 6: Upper Cpd.
Figure 7: Nylon Housings in Upper Cpd.
under any medical supervision.After clinical examination and definitive radiologicalexamination a comphrensive treatment plan wasformulated. The same was explained to the patient in detailalong with duration of the treatment and anticipatedoutcome of the treatment. After a thorough oralprophylactic procedure, diagnostic impressions were madeand casts obtained diagnostic mounting was done on asemi adjustable articulator at an established vertical height.
Periodontally compromised 16, 35 were surgicallyextracted. The remaining upper and lower teeth wereendodontically treated. After due observation to facilitatethe crown retention a crown lengthening procedure wascarried out for all endodontically treated teeth and theywere prepared to receive threaded metal post of desired
length and crown build up was done with resin based corebuild up material (Figure 2).l The appropriate shade wasselected and biomechanical preparation of the teeth wasdone. The final impression in relation to upper and lowerarches was made with addition silicone elastomericimpression material followed by temporisation (Figure 3).The upper posterior bilateral edentulous space wasrestored with a distal extension cast partial dentureretained by precision attachments. Open horse shoe major
connector was designed for the maxillary arch keeping inmind the patient’s complaint of gag reflex. The two extracoronal precision attachments were placed bilaterally distalto the second premolars (Figure 6 and 7). The lowerposterior bilateral edentulous space was restored with animplant retained distal extension cast partial denture, a
Full mouth rehabilitation & Dilemma of Wriggling Dentures...Nidawani P et al Journal of International Oral Health 2014; 6(2):136-140
138
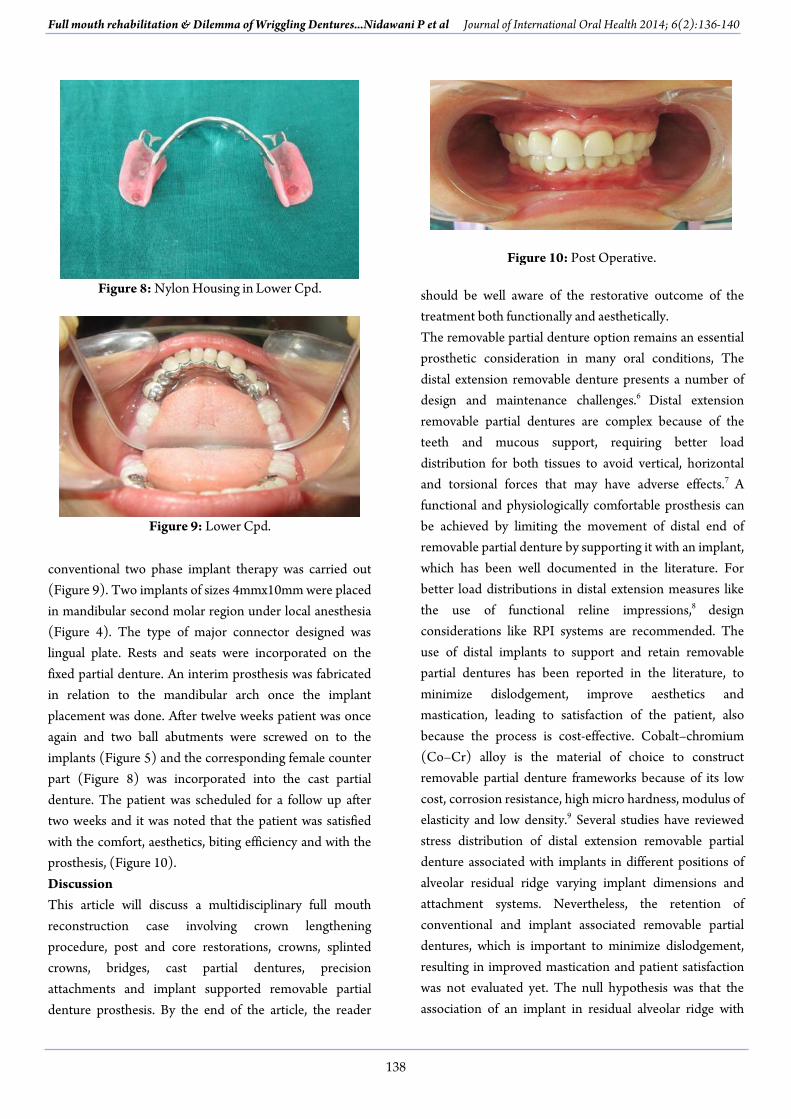
Figure 8: Nylon Housing in Lower Cpd.
Figure 9: Lower Cpd.
Figure 10: Post Operative.
conventional two phase implant therapy was carried out(Figure 9). Two implants of sizes 4mmx10mm were placedin mandibular second molar region under local anesthesia(Figure 4). The type of major connector designed waslingual plate. Rests and seats were incorporated on thefixed partial denture. An interim prosthesis was fabricatedin relation to the mandibular arch once the implantplacement was done. After twelve weeks patient was onceagain and two ball abutments were screwed on to theimplants (Figure 5) and the corresponding female counterpart (Figure 8) was incorporated into the cast partialdenture. The patient was scheduled for a follow up aftertwo weeks and it was noted that the patient was satisfiedwith the comfort, aesthetics, biting efficiency and with theprosthesis, (Figure 10).DiscussionThis article will discuss a multidisciplinary full mouthreconstruction case involving crown lengtheningprocedure, post and core restorations, crowns, splintedcrowns, bridges, cast partial dentures, precisionattachments and implant supported removable partialdenture prosthesis. By the end of the article, the reader
should be well aware of the restorative outcome of thetreatment both functionally and aesthetically.The removable partial denture option remains an essentialprosthetic consideration in many oral conditions, Thedistal extension removable denture presents a number ofdesign and maintenance challenges.6 Distal extensionremovable partial dentures are complex because of theteeth and mucous support, requiring better loaddistribution for both tissues to avoid vertical, horizontaland torsional forces that may have adverse effects.7 Afunctional and physiologically comfortable prosthesis canbe achieved by limiting the movement of distal end ofremovable partial denture by supporting it with an implant,which has been well documented in the literature. Forbetter load distributions in distal extension measures likethe use of functional reline impressions,8 designconsiderations like RPI systems are recommended. Theuse of distal implants to support and retain removablepartial dentures has been reported in the literature, tominimize dislodgement, improve aesthetics andmastication, leading to satisfaction of the patient, alsobecause the process is cost-effective. Cobalt–chromium(Co–Cr) alloy is the material of choice to constructremovable partial denture frameworks because of its lowcost, corrosion resistance, high micro hardness, modulus ofelasticity and low density.9 Several studies have reviewedstress distribution of distal extension removable partialdenture associated with implants in different positions ofalveolar residual ridge varying implant dimensions andattachment systems. Nevertheless, the retention ofconventional and implant associated removable partialdentures, which is important to minimize dislodgement,resulting in improved mastication and patient satisfactionwas not evaluated yet. The null hypothesis was that theassociation of an implant in residual alveolar ridge with

Full mouth rehabilitation & Dilemma of Wriggling Dentures...Nidawani P et al Journal of International Oral Health 2014; 6(2):136-140
139
removable partial dentures improves retention and stressdistribution. The main objective of placing implant in theposterior region is to stabilize the removable partialdenture and provide additional retention, reduce theresidual ridge resorption. A tooth and tissue supportedprosthesis could be changed to implant supportedprosthesis.10 Posterior occlusion in tissue supported distalextension is unstable but with implant supported at distalregion, a stable bilateral occlusal contact is established.Keltjens et al.11 also stated that the fitting of implants underthe distal extension of the base of the removable partialdentures results in better occlusal stability. Two clinicalcases were reported combining the use of implants withremovable partial dentures providing occlusal stability andcomfort to the patient. Planning of the oral rehabilitationof partially edentulate arches with free ends, it is notedthat, compared with the other treatment options theremovable partial dentures supported and retained bydistal implants, provides adequate retention, stability andsupport which provides comfort, allowing the patient toperform the functions of the stomatognathic system. It isalso found that, when compared with the denture fixed ontop of implants, the removable partial denture and implantcombination is less expensive, with a shorter treatmenttime and there is the possibility of fitting shorter implants,since there will be no lever arm in the crown portion.12
Kuzmanovic and colleagues treated a 66-year-old partiallyedentulous patient with an implant-supported RPD. In thispatient, the mandibular premolars and molars weremissing on both sides, and the anterior teeth were worn.They placed bilateral single molar implants to eliminatedisplacement of the distal extensions, a common problemwith conventional RPDs. At the 2-year recall appointment,no prosthodontic maintenance was needed, except forsimple activation of the gold matrices of the mandibularRPD to re-establish retention on the patrices.13 Brudvikreported that when the implants are connected with otherattachments, including conventional clasping on the otherteeth (or precision crowns), lateral stability and retentioncould be enhanced. Extracoronal attachments such as anO-ring should be utilized when a single implant abutmentis used on an RPD.14
ConclusionBenefits of implant supported RPD have been welldocumented, this clinical case demonstrates fabrication ofa cast partial denture with an implant as anchorage in the
distal extension. The goal of restoring the partiallyedentulous patient with cast partial denture is to improvethe masticatory function, establish stable posteriorocclusion with established vertical dimension.References1. Le TR. Multidisciplinary Approach to a Full Mouth
Reconstruction. Contemp Esthet 2007;5:40-5.2. Nam J, Raigrodski AJ, Heindl H. Utilization of
Multiple Restorative Materials in Full MouthRehabilitation: A Clinical Report. J Esthet RestorDent 2008;20:251-65.
3. Keltjens HM, Kayser AF, Hertel R, Battistuzzi PG.Distal Extension Removable Partial DenturesSupported By Implants and Residual Teeth:Considerations and Case Reports. Int J OralMaxillofac Implants 1993;2:208-13.
4. Amit K. Full Mouth Rehabilitation With Fixed AndRemovable Prosthesis Using Extra coronalAttachments: A Clinical Report. Peoples J Sci Res2011;2:47-52.
5. Shillingburg Jr HT, Hobo S, Whitsett LD, Jacobi R,Brackett S. Fundamentals Of Fixed Prosthodontics,3rd ed. USA: Quintessence; 1996.
6. Starr NL. The distal extension case: an alternativerestorative design for implant prosthetics. Int JPeriodontics Restorative Dent 2001;1:61-7.
7. Rodrigues RC, Faria AC, Macedo AP, de MattosMdaG, Ribeiro RF. Retention and stress distribution indistal extension removable partial dentures with andwithout implant association. J Prosthodont Res2012;57:14-9.
8. Soni P. A Modified Treatment Approach ForFabricating A Mandibular Distal Extension PartialDenture A Clinical Report. Quintessence Int2010;41:185-9.
9. Souza JE. Retention strength of cobalt-chromium vs.nickel-chromium titanium vs. CP titanium in a castframework association of removable partialoverdenture. J Contemp Dent Pract 2011;13:179-86.
10. Grossmann Y. Clinical effectiveness of implant-supported removable partial dentures: a review of theliterature and retrospective case evaluation. J OralMaxillofac Surg 2009;9:1941-6.
11. Keltjens HM, Kayser AF, Hertel R, Battistuzzi PG.Distal extension removable partial dentures

Full mouth rehabilitation & Dilemma of Wriggling Dentures...Nidawani P et al Journal of International Oral Health 2014; 6(2):136-140
140
supported by implants and residual teeth:considerations and case reports. Int J Oral MaxillofacImplants 1993;8(2):208-13.
12. Asvanud C, Morgano SM. Restoration of unfavorablypositioned implants for a partially edentulous patientby using an overdenture retained with a milled barand attachments: a clinical report. J Prosthet Dent2004;1:6-10.
13. Kuzmanovic DV, Payne AG, Purton DG. Distalimplants to modify the Kennedy classification of aremovable partial denture: a clinical report. J ProsthetDent 2004;1:8-11.
14. Brudvik JS. Advanced Removable Partial Dentures.Hanover Park, Illinios: Quintessence Publishing;1999. p. 153-9.