a memorable cup of tea - newcastle university€¦ · · 2017-08-08a memorable cup of tea aruk...
TRANSCRIPT

A memorable cup of tea ARUK 14th September 2016
Dr Ed Okello
Newcastle University - AFRD
1

2
“WHAT IS THE POINT of a long life if you can’t remember it – and what is more tragic than losing your mind before you lose the use of your body?”
Holford 2005

3
Current treatments for AD
No cure for AD: irreversible, progressive
brain disease
Treat symptoms
Slow progression
Prevent?

Alzheimer
disease
A ‘magic bullet’ for dementia?
ACh
degeneration
abnormal
amyloid
processing
plaques
and
tangles
inflammation
viral
exposure
free radical
damage
compromised
glucose
metabolism
brain
atrophy
nicotine
intake
alcohol
consumption
diet
socio-
economic
status
toxin
exposure
head
trauma
hormonal
status
ApoE
phenotype
ageing
RISK
FACTORS
DISEASE
PROCESSES

Quote from Thomas A. Edison (1847-1931): Inventor, Scientist and businessman
“The doctor of the future will
give no medication, but will
interest his patients in the care
of the human frame, diet and in
the cause and prevention of
disease.”

Alzheimer
disease
head
trauma
aluminium
exposure
ACh
degeneration
compromised
glucose
metabolism
ageing
ApoE
phenotype
nicotine
intake
socio-
economic
status
diet
alcohol
consumption
hormonal
status
inflammation
free radical
damage
abnormal
amyloid
processing
brain
atrophy
plaques
and
tangles
viral
exposure
Potential Natural products/nutritional targets
RISK
FACTORS
DISEASE
PROCESSES
PREVENTION TREATMENT?

7
Plant derived drugs
• During the last 30 years- up to 50% of approved drugs are either directly or indirectly from natural products (food or none food sources) (Newman and Cragg, 2012 – J Nat Prod 75:311-335.
Medicinal Foods
• Research in to chemistry and biochemistry of bioactive compounds in food substances
• Their safety and efficacy
• Potential uses against a range of indications
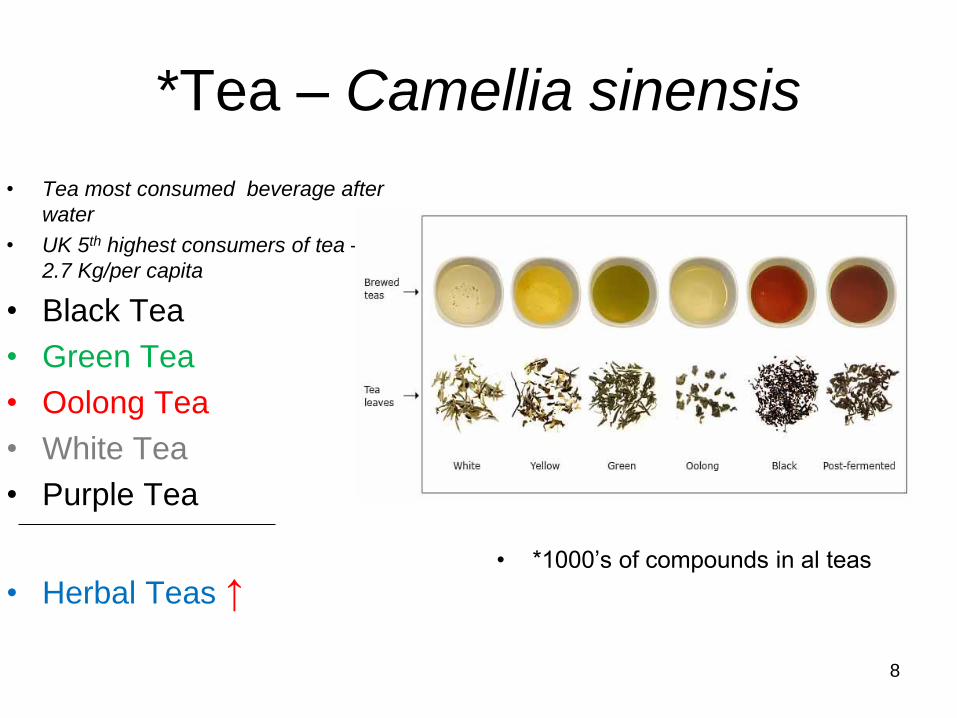
*Tea – Camellia sinensis
• Tea most consumed beverage after
water
• UK 5th highest consumers of tea – ca
2.7 Kg/per capita
• Black Tea
• Green Tea
• Oolong Tea
• White Tea
• Purple Tea
• Herbal Teas ↑
• *1000’s of compounds in al teas
8

O2-03-05 PROTECTIVE EFFECT OF JAPANESE GREEN TEA
AGAINST COGNITIVE IMPAIRMENT IN
THE ELDERLY, A TWO-YEAR FOLLOW-UP OBSERVATION
Tohru Hasegawa1, Edward Okello2, Tatsuo Yamada3;
1Saga Woman Junior College, Saga, Japan; 2University of Newcastle upon Tyne, Tyne,
United Kingdom; 3Fukuoka University, Medical School, Fukuoka, Japan
Background: Association between -
• Daily intake of polyphenols (Green tea)
• Cognitive Function (MMSE)
• Total plasma Homocysteine levels
Findings (published JAD – supplement 2005)
• ≤ 0.3 g/day tea polyphenol ↓ MMSE score
• ≥ 0.8 g/day or > no sig. change in MMSE
• ↑Thcy in cognitively impaired but ↓ with higher tea polyphenol intake
9

Green tea consumption and cognitive function: a cross-sectional study
from the Tsurugaya project
Shinichi Kuriyama, et al., Amer J Clin Nutr 2006; 83:355-61
• Comprehensive Geriatric Assessment (CGA) conducted among elderly
Japanese, July and October 2002 (CGA – Physical, mental and social
functioning status):- Cross sectional data in 2002
• Subjects: 1003 Japanese subjects aged ≥70 y.
• Data: frequency of consumption of green tea, black or oolong tea, and
coffee and cognitive function.
• Mini-Mental State Examination with cut-offs of ≤ 28,≤ 26, and ≤ 24 and
calculated multivariate-adjusted odds ratios (ORs) of cognitive impairment.
• Results: ORs decreased with frequency of green tea consumption ORs: 1 ≤
3 cups/week (reference) to 0.46 for 2 cups/day
• Conclusion: A higher consumption of green tea is associated with a lower
prevalence of cognitive impairment in humans.
10

Tea consumption and cognitive impairment and decline in older
Chinese adults.
Tze-Pin Ng, et al., 2008. Am J Clin Nutr 88: 224 –31.
Study:
• Cross-sectional analysis of MMSE at baseline and 1-2 years later.
• 2501 participants aged ≥55 years (baseline) and longitudinal
analysis of data from 1438 cognitively intact participants of Chinese
adults (Singapore)
• Cognitive impairment was defined as an MMSE score ≤ 23 and
cognitive decline as a drop in MMSE score of ≥1 point.
Conclusion:
• Regular tea consumption was associated with lower risks of
cognitive impairment and decline independent of other risk factors.
• These effects were most evident for Black (fermented) and Oolong
(semi-fermented) teas, the predominant types in Singapore
• In contrast, no association between coffee intake and cognitive
status was found.
• Contrast with Green tea: genetic polymorphisms or chemistry?
11

Scientific Evidence for
Biological activities of Tea
relevant to AD?
12

13

14


Nutrition and Cognition
Research • We measure effects on
brain wave (electrical activities) using a simplified portable electroencephalograms (EEG).
• We measure effects on mood, anxiety, attention/ concentration and memory using an on-line battery of validated psychological/cognitive tests

EEG data acquisition

Nutritional Neuroscience
Volume 19, 2016 - Issue 5
Research article
• Effects of green and black tea consumption on brain wave
activities in healthy volunteers as measured by a simplified
Electroencephalogram (EEG): A feasibility study
Edward J. Okello et al.
18
Unconscious Conscious
Delta (Δ) Theta (θ) Alpha(α) Beta (β)
0 – 4 Hz 4 – 8 Hz 8 – 12 Hz 12 – 30 Hz
Instinct Emotion Consciousness Thought
associated with deep
sleep, coma or
hypnosis
associated with
drowsiness,
meditation, feelings or
early sleeping states (
dreams)
Awareness of the body
and relaxation state/
calm feeling
alert, such as during
deep thinking and
concentration ( mental
activity)

EEG data after Green tea consumption
• Alpha and Theta
• Beta
19

• 300 mg EGCG
• Theta (θ) ↑
• Alpha (α) ↑
• Beta (β) ↑
20
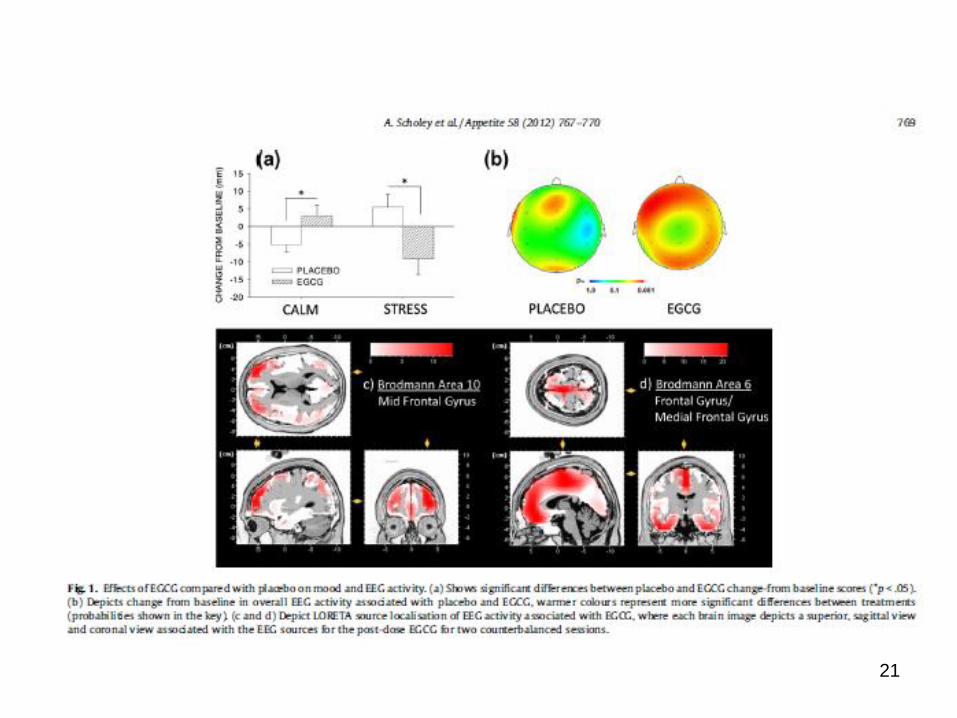
21

22
GREEN TEA Camellia sinensis the ultimate NEUROPROTECTIVE?
• Antioxidant (Lee et al 2000)
• Anti-AChE (Okello et al 2004) and facilitates cholinergic transmission in vivo (Katayama et al 2002)
• Activates cell survival genes and PKC signalling [Mandel et al 2005].
• Neurite outgrowth enhanced [Reznichenko et al 2005]
• Anti amyloid -reduces abeta in models [ Rezai- Zadeh et al 2005, Lee SY et al 2005] , reduces toxicity a beta [ Levites Y et al 2003, chai YT et al 2001], inhibits beta secretase [Okello et al 2004]
• Proteasome inhibitor ( Arbiser et al, 2005; Wan et al, 2005 and 2004) -low doses of proteasome inhibitors improve proteasome function with anti alpha synuclein potential
active chemicals catechins eg (-)-epigallocatechin
not caffeine or theobromine
23
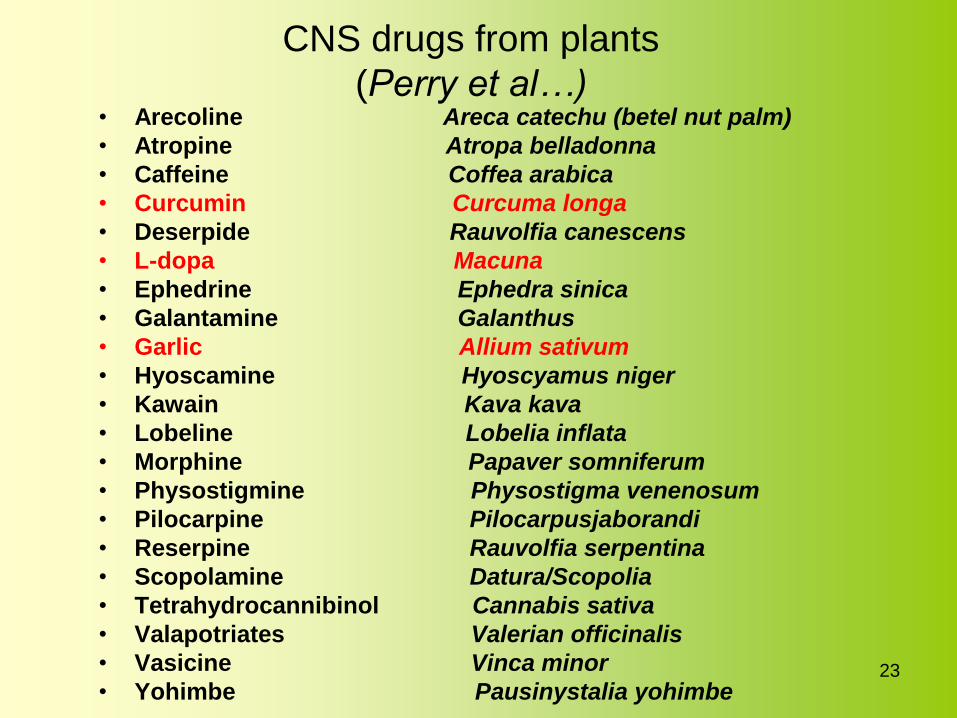
CNS drugs from plants
(Perry et al…) • Arecoline Areca catechu (betel nut palm)
• Atropine Atropa belladonna
• Caffeine Coffea arabica
• Curcumin Curcuma longa
• Deserpide Rauvolfia canescens
• L-dopa Macuna
• Ephedrine Ephedra sinica
• Galantamine Galanthus
• Garlic Allium sativum
• Hyoscamine Hyoscyamus niger
• Kawain Kava kava
• Lobeline Lobelia inflata
• Morphine Papaver somniferum
• Physostigmine Physostigma venenosum
• Pilocarpine Pilocarpusjaborandi
• Reserpine Rauvolfia serpentina
• Scopolamine Datura/Scopolia
• Tetrahydrocannibinol Cannabis sativa
• Valapotriates Valerian officinalis
• Vasicine Vinca minor
• Yohimbe Pausinystalia yohimbe

Garlic
• Allicin
24
0
0.1
0.2
0.3
0.4
0.5
0.6
B C 0.0375 0.075 0.15 0.3
“Alternative” medicines in the
management of dementia
• curcumin
– yellow pigment in turmeric (curry)
– anti-oxidant, anti-inflammatory, cholesterol
lowering
– reduces accumulation of amyloid in mice
brains
– in Phase II trials in US

CURCUMIN
Tentative evidence of better cognitive performance from curry consumption in non demented elderly Asians
Epidemiological study 1010 60-90 year olds
Frequent/ occasional curry consumers sig higher MMSEs cp non/ rare consumers
Curry consumption improves cognitive function in the elderly Ng et al. Am J Epidemiol. 2006;164:898-906
some reports lower prevalence AD
in India
27
Nutritional interventions and
Dementia:
Back to the future for new leads
