a medical crisis management simulation activity for ... · a medical crisis management simulation...
TRANSCRIPT

782 Journal of Dental Education ■ Volume 75, Number 6
A Medical Crisis Management Simulation Activity for Pediatric Dental Residents and AssistantsGee Mei Tan, M.M.E.D.Abstract: Dentists are expected to deliver safe and pain-free dental procedures after they graduate from dental school. This in-cludes using local anesthetics and sedative drugs that may be associated with side effects and complications that can lead to crisis situations. This study postulated that teaching medical crisis management to dental residents and assistants using human patient simulation (HPS) would improve their confidence in managing crisis situations in the real world. Four medical crisis scenarios were designed and programmed into a pediatric simulator. The scenarios included anaphylaxis, laryngospasm during procedural sedation, sedative medication overdose, and multiple drug interaction with cardiac arrhythmia. The simulation room was outfitted with an authentic dental operatory and emergency equipment to enhance the realism. One first- or second-year pediatric dentistry resident and a staff dental assistant were assigned as a team to participate in each ten-minute scenario followed by a debriefing session. At the end of the sessions, the participants completed an anonymous survey regarding the simulation experience. There were a total of twenty-four participants, 91.7 percent of whom felt that HPS was a good tool for learning medical crisis and that they will be more confident in managing a similar situation in the dental office after this experience. A majority of the participants felt that using HPS as a tool to teach crisis management is an acceptable and valuable technique to help improve their confidence in managing crisis situations that may occur in dental offices.
Prof. Tan is Assistant Professor, Department of Anesthesiology, The Children’s Hospital, University of Colorado Denver. Direct correspondence and requests for reprints to him at The Children’s Hospital, Department of Anesthesiology, 13123 East 16th Avenue, B090, Aurora, CO 80045; 720-777-4826 phone; 720-777-7266 fax; [email protected].
Keywords: patient safety, medical emergencies, teaching methods, dental curriculum, patient simulation, dental education, pediatric dentistry
Submitted for publication 6/20/10; accepted 8/26/10
Dental residents and assistants are expected to deliver safe and pain-free dental procedures when they graduate from dental school. This
would not only include competent dentistry skills but also the use of drugs like local anesthetics, ketamine, benzodiazepines, and opioids for sedation and anal-gesic purposes. These drugs have inherent risks of cardiovascular and respiratory complications, which may be more evident with the current complexity of medical problems in patients at the extremes of age.1-4 Medical emergencies in a dental practice are not common. However, without proper training of dental personnel in appropriate resuscitation and management skills, an emergency situation may have devastating consequences.
Medical crisis management education is a small component of the dental curriculum. Clark et al. surveyed all dental schools in the United States in 1983 and conducted follow-up surveys nine and twenty years later.5-7 They found that, in those three years, schools dedicated means of 17.4 hours, nine-teen hours, and twenty-two hours, respectively, to medical emergency training in their dental curricula.
They also found that not all schools required a medi-cal emergency training course in their curriculum.
In 2006, the American Academy of Pediatric Dentistry and American Academy of Pediatrics adopted guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures.8 This guide-line states that the practitioner responsible for the administration of sedative drugs must be competent to use such techniques and be able to manage the complications of these techniques. It also states that support personnel must be trained in and be capable of providing pediatric basic life support. In pediat-ric versus adult dental office procedures, there is a higher proportion of patients who are more anxious and less cooperative; hence, there is a greater need for sedation and anxiolysis. This would mean that the dentists and the dental assistants would need to be competent in managing any inadvertent crisis that develops during these procedures.
Simulation has been used extensively in teach-ing specific technical skills, for example, bronchos-copy9 and fiberoptic intubation.10 It has also been

June 2011 ■ Journal of Dental Education 783
used to teach and assess performance in medical crisis situations.11,12 The Anesthesiology Department at The Children’s Hospital (TCH) of the University of Colorado Denver is active in medical simulation and, in collaboration with the Dentistry Department, piloted an innovative simulation course as part of the pediatric dental residency curriculum. This study postulated that teaching medical crisis management to dental residents and dental assistants using human patient simulation would improve their confidence in managing crisis situations in the real world.
Materials and Methods The Colorado Multiple Institutional Review
Board approval for the publication of the curriculum and the post simulation experience survey results was obtained for this study. The study had been approved by the hospital’s Institutional Review Board prior to implementing any study-related interventions.
Four pediatric dental faculty members on staff in the Pediatric Dentistry Department of TCH decided among themselves which dental office-based crisis scenarios they would like to simulate, and each dentist was assigned to write one of the four scenarios. These scenarios were then enhanced and programmed into PediaSim Emergency Care Simulator (Medical Education Technologies, Inc., Sarasota, Florida). The PediaSim is an adolescent human simulator that can be manipulated by a computer system to reflect normal and abnormal human anatomy and physiology. It is able to blink, has breath sounds with chest wall movements and heart sounds with central and peripheral pulses, and is able to communicate via a microphone-speaker system controlled by an operator behind the scenes. It can also exhibit physiological reactions to drugs administered including oxygen, epinephrine, atro-pine, and muscle relaxants.
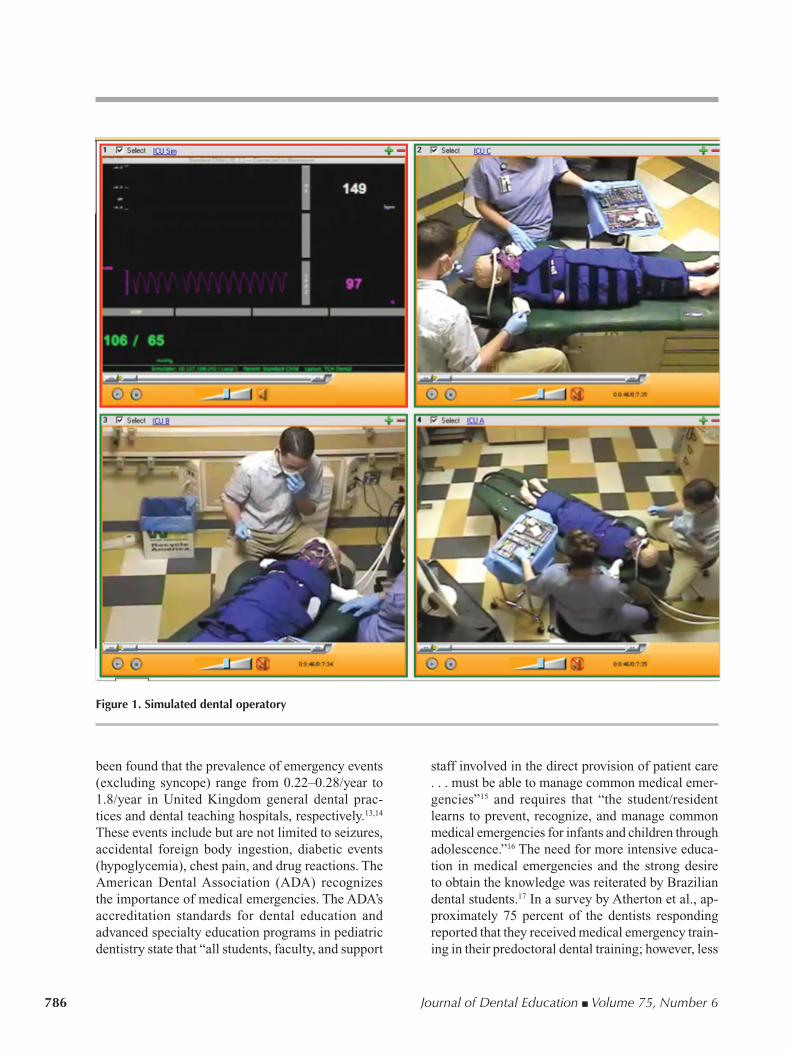
The four scenarios were anaphylaxis, la-ryngospasm during procedural sedation, sedative medication overdose, and multiple drug interaction with cardiac arrhythmia. Each scenario was writ-ten with different stages starting with a baseline or early stage, followed by deteriorating stages and a recovery stage (see example in Table 1). Each stage consists of patient vital signs and responses with the health professional’s expected actions or reactions to the patient. The simulation room at the Center for Advancing Professional Excellence (CAPE), University of Colorado Denver, was outfitted with an
authentic dental operatory and emergency equipment to enhance realism for the participants (Figure 1).
Each of the four faculty members participated in a four-hour faculty development course a month before the simulation curriculum started. None of the four had facilitated a medical crisis simulation before. The objective of the faculty development course was to allow each faculty member to experience being in the hot seat of a simulation scenario and debriefing session. The faculty development course included a one-on-one lecture on adult learning theories and debriefing techniques. This was followed by partici-pation in two of the programmed dental scenarios, with an actor portraying the role of a dental assistant, and a debriefing session for the faculty member. A checklist of expected actions (see example in Figure 2) was also created for each scenario to aid in the facilitation and debriefing of the dental residents and assistants. Each faculty member would only facilitate the learners in the same scenarios they had partici-pated in during the faculty development.
Pediatric dental residents at the University of Colorado Denver are all certified in Pediatric Advanced Life Support (PALS). Any other medical emergency-related education is taught using didactic lectures. In 2008, all dental residents and dental assis-tants participated in this new curriculum. Each dental resident and assistant participated in four scenarios over two days—that is, two scenarios per day. One dental resident was paired with a dental assistant, and the two worked as a team in each scenario on each day; thus, the team on the second day may be different from that of the first day. A facilitator was assigned to each team. Each team was given a ten-minute ac-climation to the simulation room and the manikin. They were oriented to the equipment in the room and the physiology and anatomy of the manikin. This was followed by a preparatory briefing by a facilitator that included the objectives of the event and the storyline of the simulation scenario. The participating team was brought back into the simulation room for a ten-minute scenario experience. During the simulation session, the facilitator would be watching the scenario unfold behind a one-way glass wall. During the ses-sion, the participating team would interact with the facilitator via a phone conversation if they needed or called for help. The facilitator would only enter the simulation room at the end of the ten-minute session or earlier if the team successfully completed the crisis scenario. A fifteen-minute debrief session between the team and the facilitator in a separate private room completed the session.

784 Journal of Dental Education ■ Volume 75, Number 6
Tabl
e 1.
Sce
nari
o on
ana
phyl
axis
in t
he d
enta
l offi
ce
Scen
ario
Obj
ecti
ves:
R
ecog
nitio
nof
cri
sis
situ
atio
n
Dia
gnos
iso
fana
phyl
axis
A
dmin
istr
atio
nof
gen
eral
res
usci
tatio
nsk
ills,
i.e.
,air
way
,bre
athi
ng,c
ircu
latio
n,a
ndc
allf
orh
elp
A
dmin
istr
atio
nof
spe
cific
man
agem
entf
ora
naph
ylax
is
The
Pati
ent:
6-
year
-old
boy
20
kg
11
5cm
tall
H
asm
ilda
sthm
a;o
nal
bute
roli
nhal
era
sne
eded
Had
tons
illec
tom
yan
dad
enoi
dect
omy
done
at4
yea
rso
ld
Alle
rgic
toio
dine
and
asp
irin
→h
ives
Pa
tient
live
sw
ithm
othe
ran
dol
der
sist
erin
an
apar
tmen
t
Scen
ario
:Pa
tient
has
mul
tiple
den
talc
aviti
esa
ndis
her
efo
rde
ntal
res
tora
tions
.He
has
been
inth
ede
ntal
ope
rato
ryfo
rap
prox
imat
ely
15m
inut
es.T
hed
entis
thas
suc
cess
fully
ad-
min
iste
red
the
loca
lane
sthe
tic(1
.8m
lofL
idoc
aine
with
1:1
00,0
00e
pine
phri
ne),
plac
edth
eru
bber
dam
,pre
pare
dtw
ofil
lings
inth
elo
wer
left
quad
rant
,and
isa
bout
to
plac
eth
em
atri
xba
ndto
pre
pare
for
fillin
gth
eca
vitie
s.
Stag
eV
italS
igns
Patie
nt’s
Res
pons
eR
equi
red
Part
icip
antA
ctio
nN
otes
toO
pera
tor
Earl
yre
actio
nB
P10
4/64
to1
07/6
6m
mH
g
HR
105
/min
RR
25-
27/m
in
Satu
ratio
n95
%
Aw
ake
Hoa
rse
voic
e
Spea
kso
nly
afe
ww
ords
“Ic
an’t
brea
the.
”
“My
thro
atfe
els
full.
”
“Iit
cha
lot.”
Ass
ess
vita
lsig
ns(V
S)
Puto
nm
onito
rsfo
rVS:
BP
&H
R&
pul
se
oxim
etry
Look
for:
Ext
ento
fras
h
Ext
ento
fint
ra-
and
e
xtra
oral
sw
ellin
g
Cal
lfor
hel
p;c
all9
11
Adm
inis
ter
Ben
adry
lsub
lingu
ally
1m
g/kg
BP,
pul
seo
xim
etry
,and
HR
sho
wn
on
scre
enw
hen
aske
dfo
ran
dap
plie
d.
Tran
sitio
nto
late
rea
ctio
nin
3m
inut
es.
Late
rea
ctio
nH
R1
20to
140
/min
in
2m
inut
es
BP
drop
sto
75/
45m
mH
g
in2
min
utes
Satu
ratio
n88
%in
2m
inut
es
RR
35/
min
Puls
epr
esen
t
Whe
ezin
g
Swol
len
tong
ue
Res
pira
tory
dis
tres
s:
E
xagg
erat
edc
hest
mov
emen
t
Hig
hpi
tche
dst
rido
r
W
heez
ing
B
ronc
hosp
asm
“Ife
elit
chy.
”
Eyes
clo
sed
2m
inut
esin
tos
tate
.
Patie
ntis
min
imal
lyr
espo
nsiv
e.
Rea
sses
sVS
Che
ckfo
rAB
Cs
Adm
inis
ter
oxyg
en
Dia
gnos
ean
aphy
laxi
s
Ifhe
lpa
rriv
es,g
ive
abr
iefr
epor
tofs
ituat
ion
Cal
lfor
cra
shc
arta
ndh
elp
Adm
inis
ter
IMe
pine
phri
ne0
.2m
lof
1:
1,00
0so
lutio
nw
ithE
pipe
n
Con
side
rIM
hyd
roco
rtis
one
100m
g
Patie
ntb
ecom
esw
orse
in3
min
utes
.
Ifep
inep
hrin
eis
giv
en,g
oto
rec
over
y.
Ifep
inep
hrin
eno
tgiv
enin
4m
inut
es
into
sta
te,g
oto
ven
tric
ular
tach
ycar
dia.
Ven
tric
ular
ta
chyc
ardi
aV
entr
icul
arta
chyc
ardi
a
No
puls
e
Unr
espo
nsiv
eN
otic
eV
T
Star
tCPR
Ask
for
defib
rilla
tor
Prep
are
tos
hock
pat
ient
Adm
inis
ter
1std
ose
IMe
pine
phri
ne0
.2m
lof
1:1
,000
sol
utio
nw
ithE
pipe
n
Go
tor
ecov
ery
if:
E
pine
phri
neg
iven
and
Defi
brill
ated
and
Com
pres
sion
sdo
ne.
End
scen
ario
at1
0m
inut
esto
tal.
EMS
arriv
es.
Rec
over
ySi
nus
tach
ycar
dia
RR
20-
25/m
Eyes
ope
n
Nor
mal
bre
ath
soun
ds
(no
whe
ezin
g,n
ost
rido
r)
Patie
ntis
exh
aust
eda
ndc
ryin
gA
dmin
iste
rox
ygen
top
atie
ntEn
dsc
enar
io.

June 2011 ■ Journal of Dental Education 785
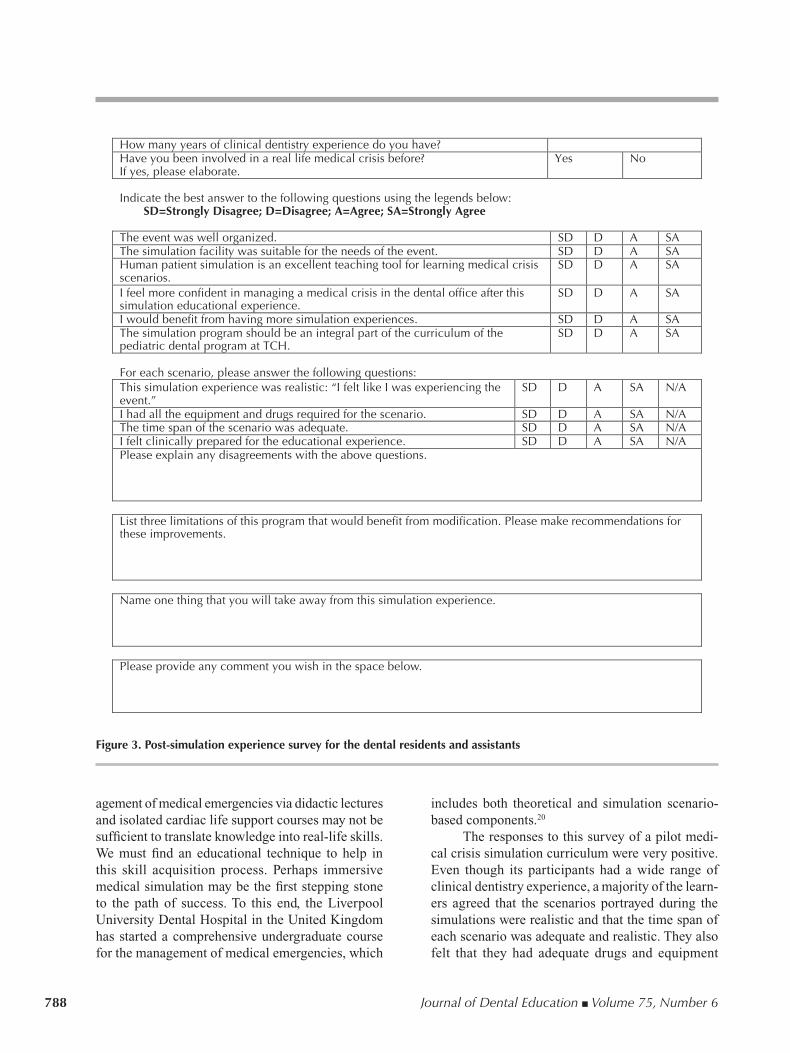
At the end of the sessions, each participant was asked to complete a voluntary anonymous survey (see survey questions in Figure 3) on a website (www.zoomerang.com) about their simulation experience. There was a post-simulation session held at the end of each day among the facilitators and this investigator to discuss the lessons learned from that day.
ResultsThere were a total of twenty-four participants
in the study: six first-year dental residents, six second-year dental residents, and twelve dental as-sistants. The results were obtained from the voluntary anonymous survey after all teams finished all four scenarios. However, not all twenty-four participants completed all the survey questions: some questions had twenty-two responses, while others had twenty-four responses. The participants had a wide range of clinical dentistry experience (range one to twenty years; median four years; average 4.85 years). Only 29 percent of the survey respondents had been in-volved in a real-life medical crisis before the simula-tion experience.
Of the participants 91.7 percent felt that human patient simulation (HPS) was a good tool for learning about medical crises and that they would be more confident in managing a similar situation in the dental office after this experience. In addition, 79.2 percent agreed that this program should be an integral part of the dental curriculum, and 87.5 percent felt that they would benefit from more simulation experience. The results of questions pertaining to each crisis scenario are shown in Table 2. About 80 percent of the respondents felt that the scenarios were realistic and that they had adequate time and equipment for the management of the crises. Not all respondents (approximately 80 percent) felt that they were clini-cally prepared for the various crisis scenarios. The post-simulation debriefing session with the facilita-tors revealed that a majority of the dental residents and assistants felt that they were unfamiliar with and had difficulty using the equipment (oxygen tank, bag and mask, defibrillator, syringes, and needles) in the room and that they were not familiar with the drug box or the drugs.
DiscussionMedical emergencies in the dental office may
not be common, but they are definitely not rare. It has Tabl
e 1.
Sce
nari
o on
ana
phyl
axis
in t
he d
enta
l offi
ce
Scen
ario
Obj
ecti
ves:
R
ecog
nitio
nof
cri
sis
situ
atio
n
Dia
gnos
iso
fana
phyl
axis
A
dmin
istr
atio
nof
gen
eral
res
usci
tatio
nsk
ills,
i.e.
,air
way
,bre
athi
ng,c
ircu
latio
n,a
ndc
allf
orh
elp
A
dmin
istr
atio
nof
spe
cific
man
agem
entf
ora
naph
ylax
is
The
Pati
ent:
6-
year
-old
boy
20
kg
11
5cm
tall
H
asm
ilda
sthm
a;o
nal
bute
roli
nhal
era
sne
eded
Had
tons
illec
tom
yan
dad
enoi
dect
omy
done
at4
yea
rso
ld
Alle
rgic
toio
dine
and
asp
irin
→h
ives
Pa
tient
live
sw
ithm
othe
ran
dol
der
sist
erin
an
apar
tmen
t
Scen
ario
:Pa
tient
has
mul
tiple
den
talc
aviti
esa
ndis
her
efo
rde
ntal
res
tora
tions
.He
has
been
inth
ede
ntal
ope
rato
ryfo
rap
prox
imat
ely
15m
inut
es.T
hed
entis
thas
suc
cess
fully
ad-
min
iste
red
the
loca
lane
sthe
tic(1
.8m
lofL
idoc
aine
with
1:1
00,0
00e
pine
phri
ne),
plac
edth
eru
bber
dam
,pre
pare
dtw
ofil
lings
inth
elo
wer
left
quad
rant
,and
isa
bout
to
plac
eth
em
atri
xba
ndto
pre
pare
for
fillin
gth
eca
vitie
s.
Stag
eV
italS
igns
Patie
nt’s
Res
pons
eR
equi
red
Part
icip
antA
ctio
nN
otes
toO
pera
tor
Earl
yre
actio
nB
P10
4/64
to1
07/6
6m
mH
g
HR
105
/min
RR
25-
27/m
in
Satu
ratio
n95
%
Aw
ake
Hoa
rse
voic
e
Spea
kso
nly
afe
ww
ords
“Ic
an’t
brea
the.
”
“My
thro
atfe
els
full.
”
“Iit
cha
lot.”
Ass
ess
vita
lsig
ns(V
S)
Puto
nm
onito
rsfo
rVS:
BP
&H
R&
pul
se
oxim
etry
Look
for:
Ext
ento
fras
h
Ext
ento
fint
ra-
and
e
xtra
oral
sw
ellin
g
Cal
lfor
hel
p;c
all9
11
Adm
inis
ter
Ben
adry
lsub
lingu
ally
1m
g/kg
BP,
pul
seo
xim
etry
,and
HR
sho
wn
on
scre
enw
hen
aske
dfo
ran
dap
plie
d.
Tran
sitio
nto
late
rea
ctio
nin
3m
inut
es.
Late
rea
ctio
nH
R1
20to
140
/min
in
2m
inut
es
BP
drop
sto
75/
45m
mH
g
in2
min
utes
Satu
ratio
n88
%in
2m
inut
es
RR
35/
min
Puls
epr
esen
t
Whe
ezin
g
Swol
len
tong
ue
Res
pira
tory
dis
tres
s:
E
xagg
erat
edc
hest
mov
emen
t
Hig
hpi
tche
dst
rido
r
W
heez
ing
B
ronc
hosp
asm
“Ife
elit
chy.
”
Eyes
clo
sed
2m
inut
esin
tos
tate
.
Patie
ntis
min
imal
lyr
espo
nsiv
e.
Rea
sses
sVS
Che
ckfo
rAB
Cs
Adm
inis
ter
oxyg
en
Dia
gnos
ean
aphy
laxi
s
Ifhe
lpa
rriv
es,g
ive
abr
iefr
epor
tofs
ituat
ion
Cal
lfor
cra
shc
arta
ndh
elp
Adm
inis
ter
IMe
pine
phri
ne0
.2m
lof
1:
1,00
0so
lutio
nw
ithE
pipe
n
Con
side
rIM
hyd
roco
rtis
one
100m
g
Patie
ntb
ecom
esw
orse
in3
min
utes
.
Ifep
inep
hrin
eis
giv
en,g
oto
rec
over
y.
Ifep
inep
hrin
eno
tgiv
enin
4m
inut
es
into
sta
te,g
oto
ven
tric
ular
tach
ycar
dia.
Ven
tric
ular
ta
chyc
ardi
aV
entr
icul
arta
chyc
ardi
a
No
puls
e
Unr
espo
nsiv
eN
otic
eV
T
Star
tCPR
Ask
for
defib
rilla
tor
Prep
are
tos
hock
pat
ient
Adm
inis
ter
1std
ose
IMe
pine
phri
ne0
.2m
lof
1:1
,000
sol
utio
nw
ithE
pipe
n
Go
tor
ecov
ery
if:
E
pine
phri
neg
iven
and
Defi
brill
ated
and
Com
pres
sion
sdo
ne.
End
scen
ario
at1
0m
inut
esto
tal.
EMS
arriv
es.
Rec
over
ySi
nus
tach
ycar
dia
RR
20-
25/m
Eyes
ope
n
Nor
mal
bre
ath
soun
ds
(no
whe
ezin
g,n
ost
rido
r)
Patie
ntis
exh
aust
eda
ndc
ryin
gA
dmin
iste
rox
ygen
top
atie
ntEn
dsc
enar
io.
786 Journal of Dental Education ■ Volume 75, Number 6
been found that the prevalence of emergency events (excluding syncope) range from 0.22–0.28/year to 1.8/year in United Kingdom general dental prac-tices and dental teaching hospitals, respectively.13,14 These events include but are not limited to seizures, accidental foreign body ingestion, diabetic events (hypoglycemia), chest pain, and drug reactions. The American Dental Association (ADA) recognizes the importance of medical emergencies. The ADA’s accreditation standards for dental education and advanced specialty education programs in pediatric dentistry state that “all students, faculty, and support
staff involved in the direct provision of patient care . . . must be able to manage common medical emer-gencies”15 and requires that “the student/resident learns to prevent, recognize, and manage common medical emergencies for infants and children through adolescence.”16 The need for more intensive educa-tion in medical emergencies and the strong desire to obtain the knowledge was reiterated by Brazilian dental students.17 In a survey by Atherton et al., ap-proximately 75 percent of the dentists responding reported that they received medical emergency train-ing in their predoctoral dental training; however, less
Figure 1. Simulated dental operatory

June 2011 ■ Journal of Dental Education 787
than 30 percent of them felt that they were “well” or “fairly well” prepared to handle an emergency situ-ation at graduation.13 More than 90 percent of these dentists had sought extra medical emergency training after they graduated, but only 75 percent of them felt that they were “well” or “fairly well” prepared at the time of survey.
A recent study by Le et al.18 found that when faced with a patient with a history of angina pectoris complaining of burning and pressing sensation over the chest, only 68 percent of a group of forty third-
and fourth-year dental students identified the need to administer supplemental oxygen to the patient. Of these, only 50 percent successfully administered the oxygen. In their study, Laurent et al.19 suggested that although more than half of the final-year dental students surveyed felt that they were totally or suf-ficiently capable of performing cardiopulmonary resuscitation, none of them were capable of com-petently managing a cardiac arrest when a random sample of these students were put into a simulated scenario. These findings suggest that learning man-
Participant’s Actions Done ( ) Assess vital signs Reassess vital signs Check airway Check breathing Check circulation Apply non-invasive blood pressure cuffs and ask to check BP Apply pulse oximetry probe and ask for saturation monitoring Ask for heart rate monitoring
Look for signs of allergic reaction: extent of rash extent of intra and extraoral swelling
Call for help: attending, another assistant, or residentdial 911 crash cart
Communicate that “patient is having an allergic reaction or anaphylaxis” Give a brief summary/report of current situation to arriving help
Administer oxygen via: nasal cannula simple facemask non re-breathing mask bag and mask
Administer intralingual Benadryl @ 1mg/kg Administer nebulized albuterol Administer im epinephrine 0.2 ml of 1:1000 via epipen X 1st dose Administer im epinephrine 0.2 ml of 1:1000 via epipen X 2nd dose Consider im hydrocortisone 100 mg Notice ventricular tachycardia or pulseless patient Start cardiac compression Continue cardiac compression for __________ minutes Call for defibrillator Prepare to shock patient Continue oxygen in recovery phase Continue monitoring of vital signs in recovery phase
Figure 2. Checklist for anaphylaxis in the dental office
788 Journal of Dental Education ■ Volume 75, Number 6
agement of medical emergencies via didactic lectures and isolated cardiac life support courses may not be sufficient to translate knowledge into real-life skills. We must find an educational technique to help in this skill acquisition process. Perhaps immersive medical simulation may be the first stepping stone to the path of success. To this end, the Liverpool University Dental Hospital in the United Kingdom has started a comprehensive undergraduate course for the management of medical emergencies, which
includes both theoretical and simulation scenario-based components.20
The responses to this survey of a pilot medi-cal crisis simulation curriculum were very positive. Even though its participants had a wide range of clinical dentistry experience, a majority of the learn-ers agreed that the scenarios portrayed during the simulations were realistic and that the time span of each scenario was adequate and realistic. They also felt that they had adequate drugs and equipment
How many years of clinical dentistry experience do you have? Have you been involved in a real life medical crisis before? If yes, please elaborate.
Yes No
Indicate the best answer to the following questions using the legends below:
SD=Strongly Disagree; D=Disagree; A=Agree; SA=Strongly Agree
The event was well organized. SD D A SA The simulation facility was suitable for the needs of the event. SD D A SA Human patient simulation is an excellent teaching tool for learning medical crisis scenarios.
SD D A SA
I feel more confident in managing a medical crisis in the dental office after this simulation educational experience.
SD D A SA
I would benefit from having more simulation experiences. SD D A SA The simulation program should be an integral part of the curriculum of the pediatric dental program at TCH.
SD D A SA
For each scenario, please answer the following questions: This simulation experience was realistic: “I felt like I was experiencing the event.”
SD D A SA N/A
I had all the equipment and drugs required for the scenario. SD D A SA N/A The time span of the scenario was adequate. SD D A SA N/A I felt clinically prepared for the educational experience. SD D A SA N/A Please explain any disagreements with the above questions.
List three limitations of this program that would benefit from modification. Please make recommendations for these improvements.
Name one thing that you will take away from this simulation experience.
Please provide any comment you wish in the space below.
Figure 3. Post-simulation experience survey for the dental residents and assistants

June 2011 ■ Journal of Dental Education 789
available to manage the scenarios. Although only about a quarter of the learners felt that they were not clinically prepared for these simulation scenarios, a majority (91.7 percent) of them felt that Human Pa-tient Simulation would be a good tool for enhancing their clinical skills for managing crisis situation in their real work-life.
There were several limitations in the survey results. The sample size for the survey was small (n=22 to 24) and may not be generalizable to all dental residency programs. The results could not be distinguished according to the different roles (resi-dents versus assistants) or years of clinical experience of the learners. Thus, the distribution of these results is unknown. This is a limitation of the study, and we are looking into improving future post-simulation surveys to include a question that will enable us to distinguish the results between dental residents and assistants. However, since more than 70 percent of the results were positive, it can be postulated that this simulation program was well received by both the dental residents and assistants. The scenario checklists were not used as an evaluation tool and thus do not offer any objective results regarding the participants’ knowledge and performance during the simulations. This is therefore only a descriptive report of the curriculum and cannot be used to relate clinical performance by the dental residents or as-sistants. The post-simulation survey was designed to be anonymous and voluntary in order to obtain unbiased and uncoerced opinions about the program from the participants. However, this led to incomplete data collection due to participants who chose to skip some questions.
From the organization and execution of the simulation together with the feedback during the debriefing sessions and the survey, several important lessons emerged. First, despite being PALS certified, dental residents are still apprehensive at using resus-
citation algorithms, drawing up drugs, and “firing” up and using the defibrillator. However, since the dental offices at TCH have Automated Electronic Defibrillators (AEDs), the dental residents and as-sistants felt that it may be less of a stumbling block to use an AED instead of a traditional defibrillator. Second, neither the dental residents or assistants are familiar with the resuscitation bag and mask equipment (hyperinflation bag with manometer by Ventlab) or the oxygen tank, and they are not able to use it effectively during the simulated resuscitation despite having the exact same equipment available at the dental offices. Third, dental residents are not familiar with drawing up drug dosages using syringes and needles out of drug ampoules/bottles. They have all been taught this via didactic lessons regarding the indications and dosages of the drugs, but not many have had the opportunity to physically perform the task. This simulation was the first time many of them had a hands-on experience with using this equipment and hence realized their lack of these technical skills.
With the experience and lessons learned from this pilot simulation event, the TCH Dentistry Depart-ment changed some of its procedures/equipment to enhance patient safety at the dental offices. Another in-service for the use of the oxygen delivery system and AED was planned for all the staff of the Dentist Office. A separate resuscitation drug box was as-sembled and placed in each of the dental operatories where sedation cases are managed. This box contains syringes and needles and the following drugs: suc-cinylcholine, epinephrine pens, atropine, diphenhydr-amine, albuterol inhaler, flumazenil, naloxone, and hydrocortisone. Even though these drugs are also available in the crash cart outside the Dental Opera-tory within the dental office, the crash cart is usually locked and would have a bigger financial impact each time it was opened. It is therefore more feasible to have the drug box in the room and handy at all
Table 2. Survey results for each scenario
Anaphylaxis Laryngospasm Oversedation Cardiac Responses Responses Responses Arrhythmia (%) (%) (%) Responses(%)
Thesimulationscenariowasrealistic. 20/22(90.9%) 21/22(95.5%) 21/24(87.5%) 20/24(83.3%)Ihadallthedrugsandequipmentavailableforthescenario. 19/22(86.4%) 20/22(90.9%) 20/24(83.3%) 20/24(83.3%)Thetimespanforthescenariowasadequateandrealistic. 19/22(86.4%) 21/22(95.5%) 19/24(79.2%) 20/24(83.3%)Ifeltclinicallypreparedforthisexperience. 17/22(77.3%) 17/22(77.3%) 17/24(70.8%) 19/24(79.2%)

790 Journal of Dental Education ■ Volume 75, Number 6
times. The simulation program was so well received by the participants that the department decided to fully implement it into its residency curriculum and continue it for subsequent years. The AED was also incorporated into the simulation scenarios instead of the traditional defibrillator in the following years.
Although crisis management simulation activi-ties have been very popular in the medical world, they are still in their infancy in the world of dentistry. This qualitative study described the innovative use of a medical simulation to teach medical crisis manage-ment to dental residents and assistants. Future quali-tative studies that include pre- and post-intervention tests and correlation to real-life events would be needed to promote its use in dentistry.
ConclusionsThe feedback to this pilot simulation shows that
a majority of the participants felt that using Human Patient Simulation as a tool to teach crisis manage-ment is an acceptable and valuable technique to help improve dental provider and assistant confidence in managing crisis situations that may occur in dental offices. Some participants agreed that this simula-tion should be incorporated into the pediatric dental residency program.
AcknowledgmentsI would like to thank the pediatric dentistry
faculty members—Dr. Ulrich Klein, Dr. Irwin Co-hen, Dr. Mark Koch, and Dr. Linda Murzyn—for their permission to use the data collected from the dental residency program. I would also like to thank the Center for Advancing Professional Excellence, School of Medicine Colorado, especially Mr. Joey Failma, for their help and expertise in the simulation.
REFERENCES1. Jastak JT, Peskin RM. Major morbidity or mortality from
office anesthetic procedures: a closed-claim analysis of 13 cases. Anesth Prog 1991;38(2):39–44.
2. Krippaehne JA, Montgomery MT. Morbidity and mortal-ity from pharmacosedation and general anesthesia in the dental office. J Oral Maxillofac Surg 1992;50(7):691–8; discussion 8–9.
3. Cote CJ, Notterman DA, Karl HW, Weinberg JA, Mc-Closkey C. Adverse sedation events in pediatrics: a critical incident analysis of contributing factors. Pediatrics 2000;105(4 Pt 1):805–14.
4. Dionne RA, Yagiela JA, Cote CJ, Donaldson M, Edwards M, Greenblatt DJ, et al. Balancing efficacy and safety in
the use of oral sedation in dental outpatients. J Am Dent Assoc 2006;137(4):502–13.
5. Clark MS, Heine CS, Fryer GE Jr. Medical emergency education in American dental schools. J Dent Educ 1985;49(3):179–81.
6. Clark MS, Fryer GE Jr. A nine-year follow-up survey of medical emergency education in dental schools. J Dent Educ 1993;57(5):363–5.
7. Clark MS, Wall BE, Tholstrom TC, Christensen EH, Payne BC. A twenty-year follow-up survey of medical emergency education in U.S. dental schools. J Dent Educ 2006;70(12):1316–9.
8. Cote CJ, Wilson S. Guidelines for monitoring and man-agement of pediatric patients during and after sedation for diagnostic and therapeutic procedures: an update. Pediatrics 2006;118(6):2587–602.
9. Blum MG, Powers TW, Sundaresan S. Bronchoscopy simulator effectively prepares junior residents to compe-tently perform basic clinical bronchoscopy. Ann Thorac Surg 2004;78(1):287–91.
10. Binstadt E, Donner S, Nelson J, Flottemesch T, Hegarty C. Simulator training improves fiber-optic intubation proficiency among emergency medicine residents. Acad Emerg Med 2008;15(11):1211–4.
11. Kim J, Neilipovitz D, Cardinal P, Chiu M, Clinch J. A pilot study using high-fidelity simulation to formally evaluate performance in the resuscitation of critically ill patients: the University of Ottawa critical care medicine, high-fidelity simulation, and crisis resource management I study. Crit Care Med 2006;34(8):2167–74.
12. Wayne DB, Butter J, Siddall VJ, Fudala MJ, Linquist LA, Feinglass J, et al. Simulation-based training of internal medicine residents in advanced cardiac life support pro-tocols: a randomized trial. Teach Learn Med 2005;17(3): 202–8.
13. Atherton GJ, McCaul JA, Williams SA. Medical emer-gencies in general dental practice in Great Britain. Part 1: their prevalence over a 10-year period. Br Dent J 1999;186(2):72–9.
14. Atherton GJ, Pemberton MN, Thornhill MH. Medical emergencies: the experience of staff of a UK dental teach-ing hospital. Br Dent J 2000;188(6):320–4.
15. Accreditation standards for dental education programs. Chicago: American Dental Association, 2010.
16. Accreditation standards for advanced specialty education programs in pediatric dentistry. Chicago: American Dental Association, 1998.
17. Carvalho RM, Costa LR, Marcelo VC. Brazilian dental students’ perceptions about medical emergencies: a quali-tative exploratory study. J Dent Educ 2008;72(11):1343–9.
18. Le TT, Scheller EL, Pinsky HM, Stefanac SJ, Taichman RS. Ability of dental students to deliver oxygen in a medi-cal emergency. J Dent Educ 2009;73(4):499–508.
19. Laurent F, Augustin P, Nabet C, Ackers S, Zamaroczy D, Maman L. Managing a cardiac arrest: evaluation of final-year predoctoral dental students. J Dent Educ 2009;73(2):211–7.
20. Balmer MC. A dental undergraduate course for the man-agement of medical emergencies in dental practice. Eur J Dent Educ 2008;12(4):239–46.