a look into the determination of cell morphology in...
TRANSCRIPT

A Look Into the Determination of Cell Morphology in Hematology in the 21st Century
Ramon Simon-Lopez, MD Global Scientific Director Beckman Coulter

Is cell morphology important?

AML t(15,17) AML M7
Plasma cell Leukemia
CLL CD5 CD19
NHL Mantle cell CD5 CD19
NHL Villous S L M Zone
AML t(8;21)(q22;q22) AML M2

Normal human blood cells

Normal Cells

Normal cells as seen in peripheral blood
Erythrocyte
B Cell Platelets
T Cell T Cell CD1C +
NK Cell
Monocyte Eosinophil Basophil Neutrophil

Normal cells as seen in peripheral blood
VCS Technology

Newly described/classified blood cells

Newly described normal cells: Subtypes of dendritic cells
Human blood DCs
plasmacytoid CD303+
myeloid CD1c+
myeloid CD141+
=CD303, =CD1c, =CD141
CD16+ Dendritic Cell
Myeloid Related Dendritic Cell
Lymphoid Related Dendritic Cell
Human blood DCs

Immature and abnormal cells

Neutrophil maturation

M0
M1
M2
Abnormal neutrophils

Abnormal monocytes
Mono-Histocyte
M5a M5b
A, B Monoblasts
C, D Promoncytes
E, F Abnormal Monocytes

Abnormal Lymphocytes


How can we detect abnormal or immature cells in an automated complete blood count (CBC)?

Parameters and Reference Values Reference Range Studies A Normal Range study was con ducted to assess the Reference Ranges for the DxH 800. Whole-blood samples were collected from approximated 240 donors (males and females). The selection of donors was consistent with the guidelines stated in CLSI C28-A2. These ranges are used as the System manager default normal range flags. Your patient population ranges may be different. Parameter Units Overall
Mean 95% Confidence Low Limit
95% Confidence High Limit
WBC x103/µl 6.3 3.6 11.2
RBC x106/µl 4.52 3.73 5.50
HGB g/dl 13.4 11.4 15.9
HCT % 39.0 33.3 45.7
MCV fL 86.4 73.7 95.5
MCH pg 29.6 24.3 33.2
MCHC g/dl 34.2 32.5 35.8
From the DxH 800 operators manual

Parameters and Reference Values cont. Parameter Units Overall
Mean 95% Confidence Low Limit
95% Confidence High Limit
RDW % 13.8 12.3 17.0 RDW-‐SD fL 41.4 37.1 47.8 PLT x103/µl 257 159 386 MPV fL 9.2 7.5 11.2
NE % 58.5 43.3 76.6
LY % 29.6 16.0 43.5
MO % 8.3 4.5 12.5
EO % 2.8 0.6 7.9
BA % 0.7 0.2 1.4
NE# x103/µl 3.7 1.8 7.8
LY# x103/µl 1.8 1.0 3.0
MO# x103/µl 0.5 0.3 1.0
EO# x103/µl 0.2 0.0 0.5 BA# x103/µl 0.0 0.0 0.1 NRBC /100 WBC 0.1 0.0 0.4 NRBC# x103/µl 0.01 0.00 0.02
From the DxH 800 operators manual
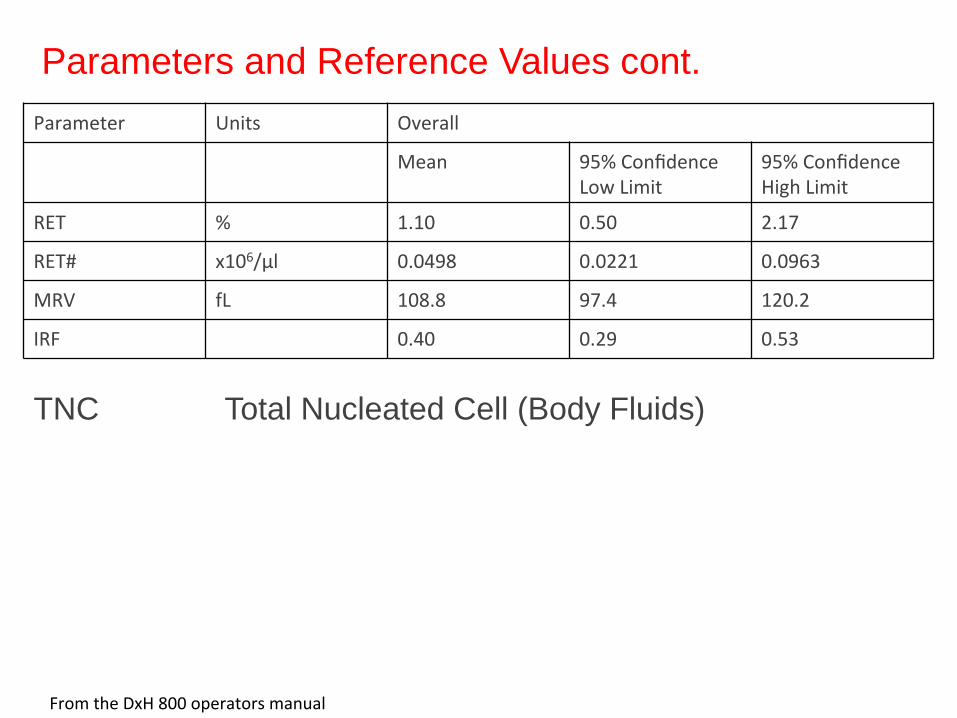
TNC Total Nucleated Cell (Body Fluids)
Parameter Units Overall
Mean 95% Confidence Low Limit
95% Confidence High Limit
RET % 1.10 0.50 2.17
RET# x106/µl 0.0498 0.0221 0.0963
MRV fL 108.8 97.4 120.2
IRF 0.40 0.29 0.53
Parameters and Reference Values cont.
From the DxH 800 operators manual

With Suspect Flags
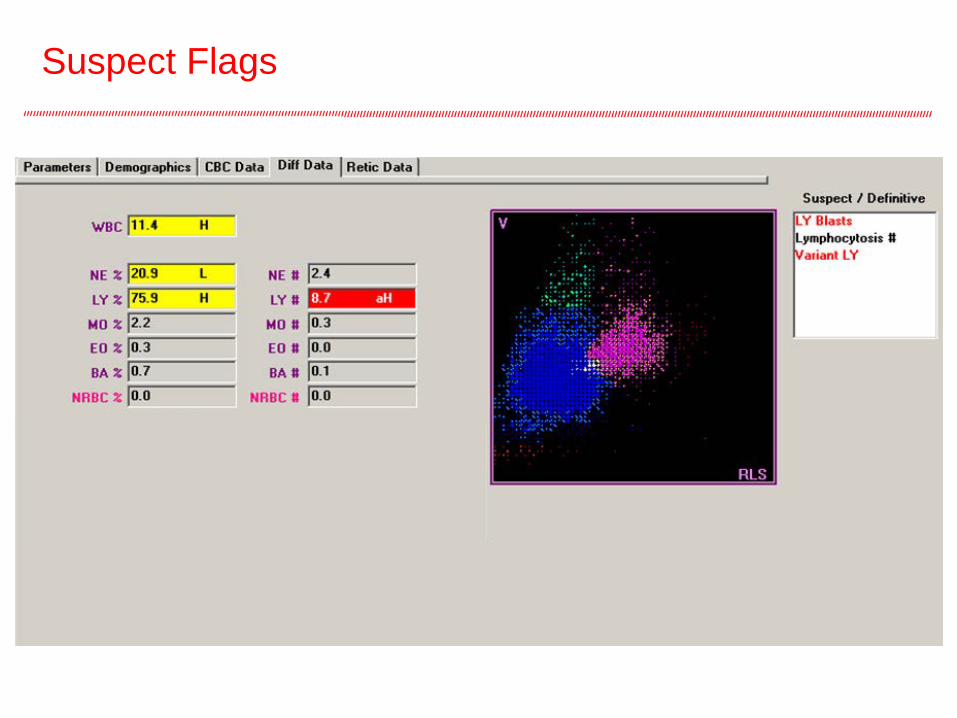
Suspect Flags

Case with Blasts (Acute Lymphoblastic Leukemia)
Lymphoblast

Are suspect flags and reference values enough?

Intended Use, Clinical Sensitivity of the DxH 800/600
Intended Use The UniCel DxH 800 Analyzer is a quantitative multi-parameter, automated hematology analyzer for in vitro diagnostic use in screening patient populations found in clinical laboratories. The UniCel& DxH 800 Analyzer identifies and enumerates the parameters indicated below on the following sample types:
• Whole Blood (Venous and Capillary) − WBC, RBC, HGB, UCT, MCV, MCII, MCHC, RDW, RDW-SD,PLT, MPV, NE%, NE#, LY%, LY#, MO%, MOlt, EO
%, EOD#,%, BA#l, NRBC%, NRBC#l, RET0/, RET#, MRV, IRF
• Pre-Diluted Whole Blood (Venous and Capillary) − WvBC, RBC, HGB, HCT, MCV, MCH, MCI-C, RDW, RDW-SD, PLT, MPV
• Body Fluids (cerebrospinal, serous and synovial) − TNC and RBC
Clinical Sensitivity and Specificity Performance Characteristics Clinical sensitivity and specificity of WBC differential flagging performance can be influenced by a number of factors relating to instrument technology, cellular frequency, uncertainty in the reference determination of a “positive” and the sample population evaluated. The DxH 800 provides the ability to set the levels and sensitivities of a variety of Flags and Messages to meet individual laboratory requirements. Beckman Coulter, Inc. recommends completion of sensitivity and specificity studies using your sample population to establish these settings.


TABLE 2. Truth Table Summary
Is 2.9% false negatives acceptable? 2.9% of 300 samples x day Everyday 8 or 9 patients with a disease that will be reported as normal. Is this acceptable?
Number % True positive 1483 11.20 False positive 2476 18.60 True negative 8953 67.30 False negative 386 2.90 Total number of samples 13298
Barnes PW, McFadden SL, Machin SJ, Simson E. The interna^onal consensus for hematology review: suggested criteria for ac^on following automated CBC and WBC differen^al analysis. Laboratory Hematology. 2005.

Think about the faces of these people

How we can tailor or adapt the instrument sensitivity
to our needs?

Decision Rules allow for user-defined flags, system messages and actions to be written

• If a pathologist or a technologist identifies certain morphologic findings in a sample, he will take in consideration information about the patient to determine its significance.
• The DxH 800 does just that, automatically, for every single CBC-diff run in a lab.
• Users just have to have the decision rule of their interest. • The end result:
• Optimal patient care with review of significant morphologic abnormalities.
• Minimized unnecessary manual reviews (false positives)
DxH 800/600 – an automated hematological consult for every sample

Lymphoid
Reactive, HIV
Monocytes
Normal low B12 or Folate
Lymphoproliferative Disorders
Myeloid

Conclusion
Beckman Coulter’s user-defined decision rules allow each lab the ability to activate,
modify and adjust them according to individual lab requirements.
