a historic case of visual agnosia revisited after 40 years
TRANSCRIPT

Brain (1991), 114, 789-800
A HISTORIC CASE OF VISUAL AGNOSIAREVISITED AFTER 40 YEARS
by STEVEN A. SPARR,1 MILTON JAY,2 FRANK W. DRISLANE3 and
NAGAGOPAL VENNA2
(From the Departments of Neurology, 'Albert Einstein College of Medicine, Bronx, New York,2Boston City Hospital and ^Beth Israel Hospital, Boston, Mass., USA)
SUMMARY
In one of the seminal works on visual agnosia, Adler (1944, 1950) presented the case of a 22-yr-old womanwho sustained carbon monoxide cerebral toxicity in the Cocoanut Grove nightclub disaster of 1942. Welocated this patient 40 yrs after injury and performed a detailed reevaluation. The patient demonstratedpersistent deficits in visual recognition, characterized most prominently by defective recognition of elementalshape and form, associated with alexia, prosopagnosia, visuospatial disorientation and impaired visualimagery. Visual acuity, colour recognition, writing ability and verbal intelligence were relatively preserved.Isolated bilateral occipital injury was demonstrated by CT and MRI scanning. On comparison with previouslyreported cases, our results support the hypodiesis that carbon monoxide toxicity can induce a visual agnosiaof the apperceptive type with well defined characteristics, seldom seen with other types of cerebral injury.Prognosis for long-term recovery is poor.
INTRODUCTION
The acquired disorders of visual recognition include visual agnosias of several formsand alexia without agraphia occurring in isolation ('pure alexia'). These syndromes arerare and elucidation of their clinical and pathogenetic features has been dependent uponrelatively few well described case reports.
In one of the seminal works on visual agnosia, Alexandra Adler (1944, 1950) describeda 22-yr-old woman who developed a profound disorder of visual recognition as the resultof injury sustained in the Cocoanut Grove nightclub disaster of 1942. Unusual featuresreported by Adler include the aetiology, carbon monoxide toxicity, which may beresponsible for a unique form of visual agnosia (Benson and Greenberg, 1969); thepresence of alexia without agraphia with preserved visual fields, rarely encounteredin cases of pure alexia (Greenblatt, 1973); and the lack of confounding aphasia ordementia, allowing for detailed analysis of a visual integrative disturbance in a relativelypure form. As one of the earliest and most meticulously documented studies of a visualagnosia of the apperceptive type, Adler's work has had significant influence on subsequentinvestigators of disorders of complex visual processing.
As the long-term natural history of visual agnosia has not been well characterized,and the localization and neuropsychological mechanism of the apperceptive form remainincompletely understood, we located Adler's patient 40 yrs after injury, replicatedmany of the studies that had been previously performed and performed additional
Correspondence to: Dr Steven A. Sparr, Department of Neurology, Albert Einstein College of Medicine, 1300 MorrisPark Avenue, Bronx, New York 10461, USA.
© Oxford University Press 1991
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

790 S. A. SPARR AND OTHERS
neuropsychometric, radiological and electrophysiological testing unavailable at the timeof her earlier evaluations. Our results demonstrate continued fixed deficits in visuospatialperception and, despite normal intelligence and high motivation, minimal improvementin her alexia in the intervening years. We describe unique aspects of carbon monoxide-induced visual agnosia in comparison with other previously reported cases.
CASE HISTORY
H.C. was a healthy, right-handed 22-yr-old woman, a high school graduate employed as a comptometeroperator, when she attended the Cocoanut Grove nightclub on the evening in November 1942, when atragic fire claimed 491 lives. She lost consciousness while trying to escape and was rescued by firemenafter at least 20 min of exposure to fumes. On arrival at Boston City Hospital she was conscious, butwas agitated, confused, and apparently blind. She had mild respiratory difficulty, hoarseness, and a minorburn on the right shoulder. She remained confused for several days with flight of ideas and inappropriateelation. Her speech remained fluent throughout. She had poor memory, including amnesia for the fire.
She did not fix her eyes on any target and gazed straight ahead for prolonged periods. She was able,however, to recognize objects and people by tactile, auditory and olfactory sensations (e.g., she distinguishedphysicians from nurses by the smell of tobacco on the physicians' clothing). A neuropsychologist foundnormal optic fundi, reactive pupils, and normal sensory and motor examinations. His initial impressionwas that the patient's 'blindness' was a form of hysteria.
On the fifth hospital day the patient was examined by Dr Alexandra Adler of the Boston City HospitalNeurological Unit. Adler concluded that her symptoms were due to brain injury, and began a series ofinvestigations that were to span 5 yrs. On her initial evaluation Adler found that she could distinguishlight from dark, but could not recognize form or colour. After 2 wks she could name and match coloursby intensity and hue, and visual acuity was normal.
With return of normal visual acuity the patient exhibited a profound alexia, initially unable to identifyany word or single letter. On the 17th hospital day she recognized the letter H, but no others, and inferredher name, HELEN, from the first letter and length of the word. She subsequently discerned other lettersby recognition parts, frequently confusing letters of similar form. After 6 months she was able to readprinted words, but not handwriting, even her own. Five years after injury she was able to read a novel,but found reading to be a slow laborious process, devoid of pleasure. Her ability to read handwriting remainedunpaired.
In addition to this alexia, Adler documented a pervasive underlying visual agnosia. For the first 2 wksshe was unable to recognize any object presented visually. Over the next month she began to perceivethe outer contours of objects and, ultimately, began to discern internal detail. By 6 months visual objectagnosia could be demonstrated only tachistoscopically. She experienced difficulty in recognizing facesof well-known acquaintances on first encounter after injury, and devised a system for recalling faces bymemorizing salient features. She was unable to copy simple geometric figures, reproduce Koh's blocksdesigns, or separate visually embedded figures. When presented with a complex scene, she described onlyindividual isolated features and was unable to give an overview of the interaction between components.Similarly, she lost track of the action when watching a movie when too many characters appeared in ascene. She no longer dreamed in visual images, but rather, described vague emotional experiences(e.g., 'suffocation') during sleep.
H.C. experienced topographical disorientation, and found it necessary to establish a system of markersto find her way around her own neighbourhood. Her ability to calculate was severely impaired, with lossof ability to perform arithmetical operations more complex than simple addition and subtraction. She showedno evidence of aphasia or disturbance of logical thought processes. An EEG and visual field examinationby Goldmann perimetry (1° test object) were normal.
Interim history
Since her last evaluation by Adler in 1947, H.C. has remained in excellent general health. There havebeen no subsequent hospitalizations except for childbirth. She has remained physically and socially active,caring for her home and family, and retaining a particular fondness for ballroom dancing.
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from
VISUAL AGNOSIA REVISITED 791
Through the years, however, she has frequently been frustrated by her inability to perform a wide varietyof simple tasks. For example, she is unable to follow a recipe when cooking due to inability to discerndemarcations on a measuring cup. She has difficulty finding her way in unfamiliar places and rarely reads,as this is no longer pleasurable. She feels that her deficits have prevented her from reaching her full potentialin life and feels particularly deprived by her inability to work or to drive an automobile.
Until we located the patient in 1983, she had had no formal neurological revaluation since leaving Adler'scare. In the interim, she had consulted opticians and ophthalmologists in the hope that her visual difficultiescould be corrected by proper refraction.
REEXAMINATION OF THE PATIENT
H.C., now 62-yrs-old, appeared younger than her stated age. General physical examination wasunremarkable. She was socially appropriate and cooperative, with normal speech and affect. Recent andremote memory were excellent. Detailed cognitive testing is described below.
Corrected visual acuity was 20/30 bilaterally by Snellen chart. Visual fields were full to bedside testingwith a 4 mm test object. She did not extinguish simultaneously-presented visual stimuli; she exhibited normalopticokinetic nystagmus. Fundoscopy by a consultant ophthalmologist was normal. Extraocular movementswere full with smooth pursuits; the remainder of cranial nerve, motor and sensory examinations were normal.
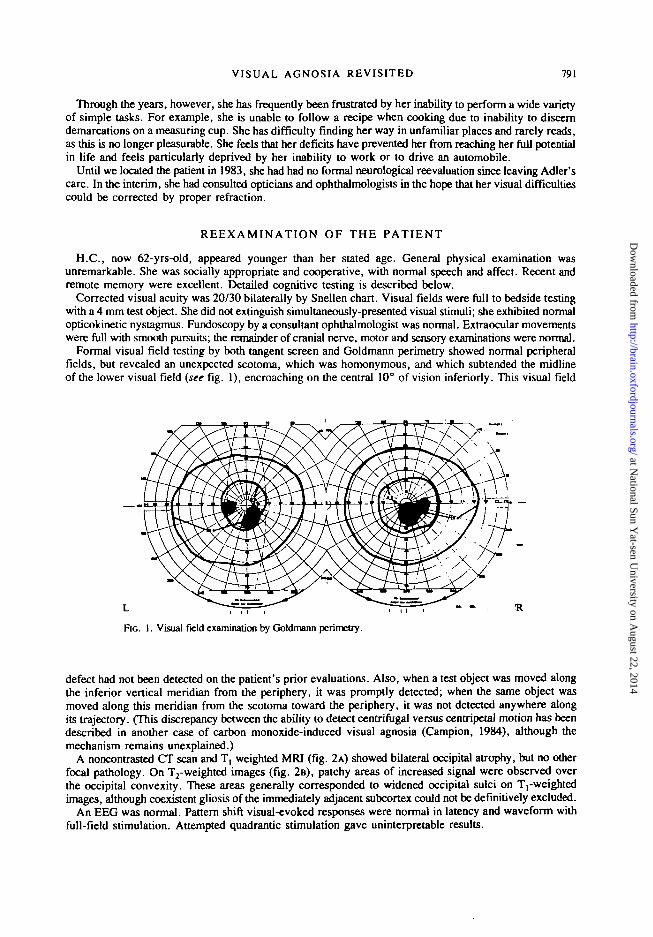
Formal visual field testing by both tangent screen and Goldmann perimetry showed normal peripheralfields, but revealed an unexpected scotoma, which was homonymous, and which subtended the midlineof the lower visual field (see fig. 1), encroaching on the central 10° of vision inferiorly. This visual field
FIG. 1. Visual field examination by Goldmann perimetry.
defect had not been detected on the patient's prior evaluations. Also, when a test object was moved alongthe inferior vertical meridian from the periphery, it was promptly detected; when the same object wasmoved along this meridian from the scotoma toward the periphery, it was not detected anywhere alongits trajectory. (This discrepancy between the ability to detect centrifugal versus centripetal motion has beendescribed in another case of carbon monoxide-induced visual agnosia (Campion, 1984), although themechanism remains unexplained.)
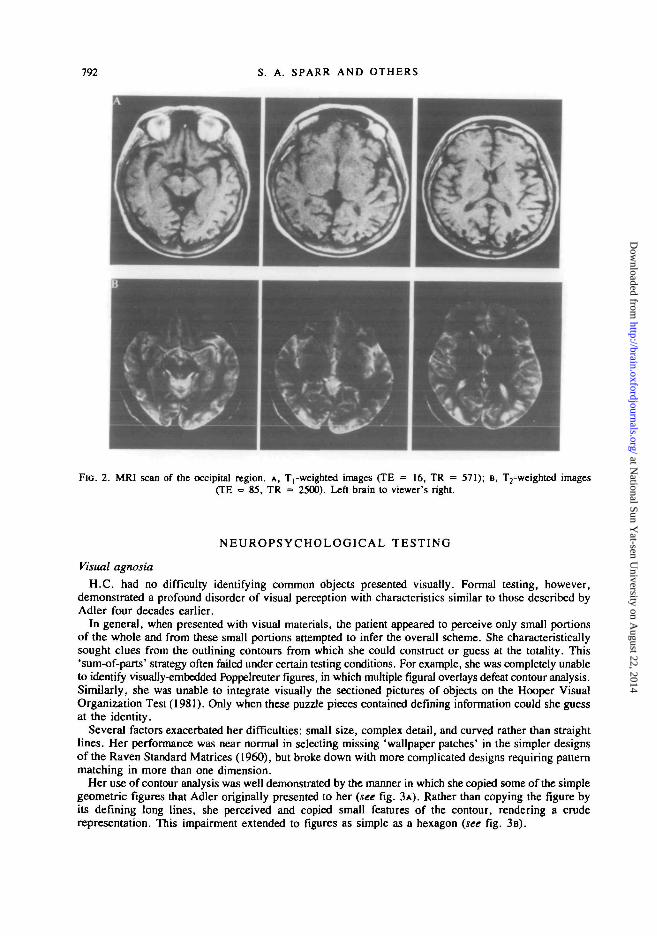
A noncontrasted CT scan and T, weighted MRI (fig. 2A) showed bilateral occipital atrophy, but no otherfocal pathology. On T2-weighted images (fig. 2B), patchy areas of increased signal were observed overthe occipital convexity. These areas generally corresponded to widened occipital sulci on T,-weightedimages, although coexistent gliosis of the immediately adjacent subcortex could not be definitively excluded.
An EEG was normal. Pattern shift visual-evoked responses were normal in latency and waveform withfull-field stimulation. Attempted quadrantic stimulation gave uninterpretable results.
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from
792 S. A. SPARR AND OTHERS
FIG. 2. MRI scan of the occipital region, A, Trweighted images (TE = 16, TR = 571); B, T2-weighted images(TE = 85, TR = 2500). Left brain to viewer's right.
NEUROPSYCHOLOGICAL TESTING
Visual agnosia
H.C. had no difficulty identifying common objects presented visually. Formal testing, however,demonstrated a profound disorder of visual perception with characteristics similar to those described byAdler four decades earlier.
In general, when presented with visual materials, the patient appeared to perceive only small portionsof the whole and from these small portions attempted to infer the overall scheme. She characteristicallysought clues from the outlining contours from which she could construct or guess at the totality. This'sum-of-parts' strategy often failed under certain testing conditions. For example, she was completely unableto identify visually-embedded Poppelreuter figures, in which multiple figural overlays defeat contour analysis.Similarly, she was unable to integrate visually the sectioned pictures of objects on the Hooper VisualOrganization Test (1981). Only when these puzzle pieces contained defining information could she guessat the identity.
Several factors exacerbated her difficulties: small size, complex detail, and curved rather than straightlines. Her performance was near normal in selecting missing 'wallpaper patches' in the simpler designsof the Raven Standard Matrices (1960), but broke down with more complicated designs requiring patternmatching in more than one dimension.
Her use of contour analysis was well demonstrated by the manner in which she copied some of the simplegeometric figures that Adler originally presented to her (see fig. 3A). Rather than copying the figure byits defining long lines, she perceived and copied small features of the contour, rendering a cruderepresentation. This impairment extended to figures as simple as a hexagon (see fig. 3B).
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

VISUAL AGNOSIA REVISITED 793
0FIG. 3. Patient's attempt at copying (A) a simple geometric figure
at various angles of rotation and (B) a hexagon. Stimulus on left,H.C.'s copy on right.
She demonstrated impaired constructions in replicating Kohs block designs, which she did slowly andwith poor strategy. She was able to reproduce items 1—5 of the Block Design Subtest of the WAIS-R(Wechsler, 1981), but designs of the 9 block level were quite beyond her capabilities.
Additional visuospatial deficits included some degree of inattention to the right side of space when bisectinglines or attempting to locate the centre of a square. She showed poor topographical orientation and couldnot properly orientate to compass directions.
Colour naming and matching tasks were performed normally; she was able to identify colours presentedto each hemifield without any sign of hemiachromatopsia.
Reading
The patient's alexia was essentially unchanged from that detailed by Adler in 1950. Although she isa high school graduate and formerly an avid reader, she now avoids reading as it has become so arduous.Formal assessment with the Durrell Analysis of Reading Difficulty (1955), Gilmore Oral Reading Test(1968) and the Woodcock Word Identification Test (1973) indicated that she read at approximately a thirdgrade level of overall achievement.
At the single word level, she regularly misidentified individual letters, particularly in the interiors ofwords. For example, she read front as first, soapy as sorry, farm as from, and smolder as smaller. Atthe same time she was able to read and comprehend much more sophisticated words such as jeopardize,physician, and sapphire, although her overall abilities at this level were quite abnormal. Occasionally whenshe experienced difficulty discerning a word, she used her right index finger to trace one or more letters;this technique appeared to improve her performance.
At the sentence and paragraphic levels of reading, these letter and word misidentifications interferedwith oral and silent decoding and comprehension.
Her difficulties were exacerbated by small print size, closely spaced lines, and highly stylized typeface.For example, she read the title of The New York Times Magazine as a 'Chinese Magazine' due to the highlystylized curvature of the letter T. Later, she identified the word York, but not the word New, which wassuperimposed on the boundary of light and dark of the cover photograph, suggesting difficulty in separatingfigure from ground.
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

794 S. A. SPARR AND OTHERS
Handwritten materials were particularly troublesome and she could not read a passage in her ownhandwriting shortly after writing it. Oral spelling, however, remained normal.
Writing
In her 5 yr follow-up study, Adler (1950) documented a deterioration in the patient's handwriting, withnew distortions in letter formation, most notably the addition of extra loops to the letters n, m, u, andy. Adler speculated that this deterioration was the result of faulty visual feedback-correction, which ultimatelyaltered internal percepts of letter formation.
Forty years later the patient's handwriting appeared to have stabilized at the 1947 level (fig. 4), withno further deterioration, but with persistence of the previously noted distortions.
>
FIG. 4. Writing to dictation: prcinjury (top);5 yrs after injury (after Adler, 1950) (middle);40 yrs after injury (bottom).
Facial recognition
H.C. showed no difficulty in recognizing faces in a small group setting during examination, and readilyrecognized one of the examiners before he spoke on a chance meeting in the hospital elevator.
She showed poor performance, however, in recognizing photographs of well-known people, achievingonly approximately 50% correct. Her performance improved with cuing (e.g., 'this is a world leader'),and with colour rather than black and white materials.
She often used contextual clues to help her guess at the identity. For example, when presented witha photograph of ex-President Carter shaking hands with a woman she stated, 'I don't recognize him toowell . . . That's Carter. And that looks like his wife.'
Her piecemeal approach to analysing visual information was again apparent in her handling of caricaturesand cartoons. For example, she correctly distinguished Bush from Reagan in a political cartoon stating,"This one is Bush—he has a high forehead and not much hair'. She was unable to recognize a torso-onlydrawing of Mickey Mouse, but when told the correct identity said, 'Oh yes, I can see his eyes', pointingto two large buttons on his shorts.
Her ability to recognize faces markedly deteriorated when many people appeared in a photograph. Evenwith real faces she reported difficulty picking familiar faces out of a crowd. She stated, 'I never leavemy seat on a plane trip because I'm afraid that I won't be able to find my husband again. You know howall people on a plane look the same . . . and they dress the same'.
Visual imagery
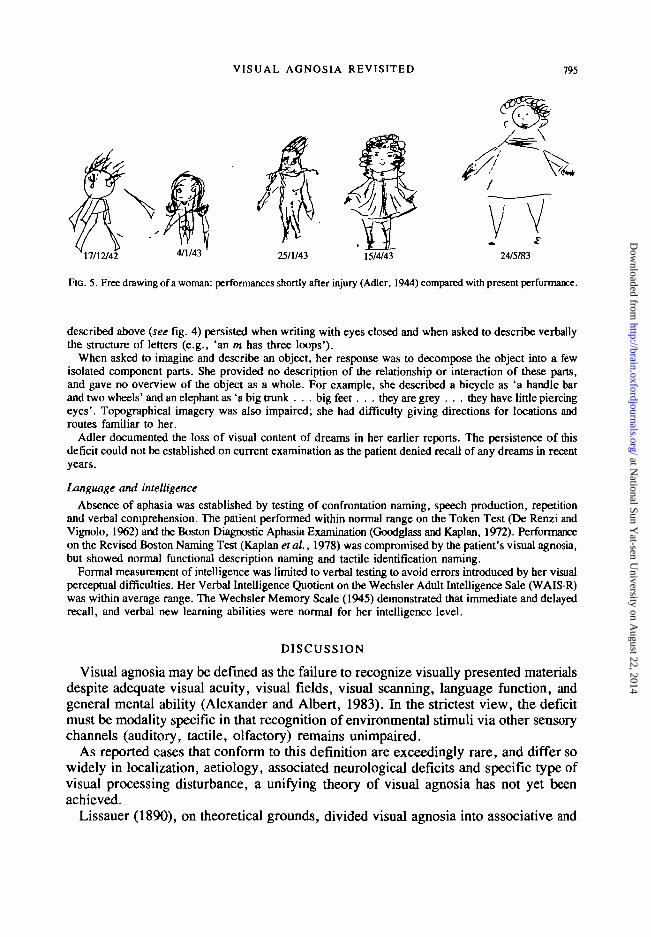
Disturbance of visual imagery was suggested by her poor performance on a number of tasks. Her freedrawings were crude and similar in quality to efforts made in 1943 (fig. 5). The distortions in letter formation
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from
VISUAL AGNOSIA REVISITED 795
17/12/42 4 / 1 / 4 3 25/1/43 15/4/43
FIG. 5. Free drawing of a woman: performances shortly after injury (Adler, 1944) compared with present performance.
described above (see fig. 4) persisted when writing with eyes closed and when asked to describe verballythe structure of letters (e.g., 'an m has three loops').
When asked to imagine and describe an object, her response was to decompose the object into a fewisolated component parts. She provided no description of the relationship or interaction of these parts,and gave no overview of the object as a whole. For example, she described a bicycle as 'a handle barand two wheels' and an elephant as 'a big trunk . . . big feet . . . they are grey . . . they have little piercingeyes'. Topographical imagery was also impaired; she had difficulty giving directions for locations androutes familiar to her.
Adler documented the loss of visual content of dreams in her earlier reports. The persistence of thisdeficit could not be established on current examination as the patient denied recall of any dreams in recentyears.
Language and intelligence
Absence of aphasia was established by testing of confrontation naming, speech production, repetitionand verbal comprehension. The patient performed within normal range on the Token Test (De Renzi andVignolo, 1962) and the Boston Diagnostic Aphasia Examination (Goodglass and Kaplan, 1972). Performanceon the Revised Boston Naming Test (Kaplan et al., 1978) was compromised by the patient's visual agnosia,but showed normal functional description naming and tactile identification naming.
Formal measurement of intelligence was limited to verbal testing to avoid errors introduced by her visualperceptual difficulties. Her Verbal Intelligence Quotient on the Wechsler Adult Intelligence Sale (WAIS-R)was within average range. The Wechsler Memory Scale (1945) demonstrated that immediate and delayedrecall, and verbal new learning abilities were normal for her intelligence level.
DISCUSSION
Visual agnosia may be defined as the failure to recognize visually presented materialsdespite adequate visual acuity, visual fields, visual scanning, language function, andgeneral mental ability (Alexander and Albert, 1983). In the strictest view, the deficitmust be modality specific in that recognition of environmental stimuli via other sensorychannels (auditory, tactile, olfactory) remains unimpaired.
As reported cases that conform to this definition are exceedingly rare, and differ sowidely in localization, aetiology, associated neurological deficits and specific type ofvisual processing disturbance, a unifying theory of visual agnosia has not yet beenachieved.
Lissauer (1890), on theoretical grounds, divided visual agnosia into associative and
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

796 S. A. SPARR AND OTHERS
apperceptive varieties. Associative agnosics retain the ability to copy, match, or in someway indicate 'primary reception' of visual stimuli. Apperceptive agnosics fail at an earlierlevel of visual processing in that they are unable to demonstrate even primary reception.This classification has been criticized as over-simplistic and is unable to account forcases with mixed associative-apperceptive features (Kertesz, 1979; Riddoch andHumphreys, 1987). Nevertheless, the Lissauer classification continues to serve as aclinically useful starting point for analysing visual agnosias as the two variants appearto differ in localization and neuropsychological mechanism.
The associative form has been more thoroughly studied and is generally accepted toresult from functional disconnection of visual centres from semantic stores ('visuolimbicdisconnection', Alexander and Albert, 1983) due to lesions in connecting white matterpathways. Pathologically this disconnection arises from bilateral occipital injuries or,in a fashion analogous to the Dejerine (1892)-Geschwind (1965) hypothesis for purealexia, can arise from unilateral dominant occipital injury with involvement of the corpuscallosum (Bauer and Rubens, 1985).
The mechanism of apperceptive forms of visual agnosia remain less completelyunderstood. Visual agnosia with apperceptive features has been described in cases ofclosed head trauma (Goldstein and Gelb, 1918), mercury poisoning (Landis et al., 1982),and bilateral occipital infarctions (Riddoch and Humphreys, 1987), although, as willbe discussed, it occurs most commonly and in purest form as the result of carbonmonoxide toxicity.
Adler's report on her patient with visual agnosia in 1944 was an important milestonein the elucidation of the neuropsychological features of apperceptive visual agnosia,and has been acknowledged by subsequent investigators. Kurt Goldstein (1948) referredto Adler's work prominently in his exposition on disorders of gestalt formation; Bensonand Geschwind (1969) cited this work in their review of alexia without agraphia andcommented on the unusual deterioration of writing exhibited by this patient; Vincentet al. (1977) alluded to this case as a rare example of alexia without agraphia occurringwithout hemianopia or colour naming deficit; Ajax (1967) noted Adler's work as oneof the few reports to document long-term prognosis in alexia; recent major review articleson visual agnosia by Alexander and Albert (1983) and Bauer and Rubens (1985) includereference to Adler's patient as a classic example of visual agnosia of the apperceptive type.
Observation of Adler's patient over a 40 yr period reveals that she evolved from astate of global visual impairment to a specific syndrome in which recognition of formis selectively impaired. She fails to recognize a shape as simple as a hexagon {see fig. 3)and yet readily recognizes real objects where size and colour clues help compensatefor defective perception of form. Analysis of her performance on a wide variety of visualtasks indicates that she approaches complex visual material in a piecemeal fashion. Sheappears to reduce complex wholes into more manageable small components, but failsto recognize even these elemental components and thus does not succeed in reintegratingthe parts into a coherent whole.
Many of the other features of her visuospatial disorder may, in fact, be consequencesof this impaired recognition of form. These include simultanagnosia, that is, the tendencyto focus attention of a small portion of the visual scene with failure to achieve an overview,inability to separate figure from ground, and impaired constructions.
The major functional consequences of her visual agnosia have been alexia and
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

VISUAL AGNOSIA REVISITED 797
prosopagnosia. Although she has become quite adept at using compensatory strategiesin reading and facial recognition, these strategies break down when she is faced withnonstandardized materials (e.g., stylized typeface) or with masking by a complexbackground.
In addition to her visual agnosia for the external environment, H.C. demonstratesfaulty visual imagery and loss of visual content of dreams. These disturbances of internalvisual representations were first reported a century ago by Charcot and by Wilbrand(see Nielsen, 1946) and have been described in scattered case reports since (see reviewby Farah, 1984). In these reports, as in the present case, disorders of visual imageryhave been almost invariably associated with disorders of visual perception. These findingssuggest that the neural networks used for visual perception and those for visual imagerymay share at least some common elements (Levine et al., 1985).
'Primary' visual testing showed normal visual acuity, visual tracking, and peripheralfields. A small inferior paracentral scotoma (see fig. 1) and inability to detect centrifugalmotion along the inferior vertical meridian were noted, but cannot account for her complexvisuospatial disorder.
Carbon monoxide-induced visual agnosiaWith the exception of a few isolated cases with diffuse bioccipital injuries, apperceptive
visual agnosia has been reported almost exclusively as the result of carbon monoxidecerebral toxicity. Adler noted 3 previous cases of visual agnosia induced by carbonmonoxide (Schilder and Isakower, 1928; Solomon, 1932; von Hagen, 1941), andsubsequently several more have been reported (Garland and Pearce, 1967; Benson andGreenberg, 1969; Abadi et al. 1981; Alexander and Albert, 1983; Campion, 1984),including the suggestive case of Cobb and Lindemann (1943) involving another victimof the Cocoanut Grove nightclub disaster.
These cases demonstrate a striking similarity. In general, after carbon monoxideexposure sufficient to induce loss of consciousness, the patient regains consciousness,is transiently in a confusional state, and ultimately becomes lucid. Memory disturbancesand extrapyramidal signs are variably seen, and are consistent with the well-knowntoxicity of carbon monoxide on the hippocampus and basal ganglia (Lapresle and Fardeau,1967; Ginsberg, 1980; Brierley and Graham, 1984). Initially the patient is corticallyblind, then clears to a state of impaired visual perception with intact visual fields (orminor field defects) and normal visual acuity. The patient is unable to name accurately,copy or match visual stimuli (apperceptive visual agnosia). Frequently associated is thedistortion of internal visual imagery and loss of visual content of dreams, the Charcot-Wilbrand syndrome (Nielsen, 1946). Some improvement may be seen early in the course,with nearly complete recovery reported in one case (Schilder and Isakower, 1928). Morecommonly, however, some degree of visual impairment persists and, as suggested bythe present study, may become permanent.
In their detailed study of one such case, Benson and Greenberg (1969) found thattheir patient was able to detect subtle differences in luminescence, wavelength and area,but failed to distinguish differences in shape. They noted the similarity between theircase and Adler's and suggested that this was a unique syndrome which they proposedbe called visual form agnosia.
The anatomical locus of pathology in carbon monoxide-induced visual agnosia is
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

798 S. A. SPARR AND OTHERS
unknown; there have been no postmortem studies. Benson and Greenberg proposed anintracortical localization, due either to laminar necrosis or patchy 'salt and pepper' corticalinfarctions of the primary visual cortex, both of which are known consequences of carbonmonoxide toxicity. This localization is appealing from a theoretical point of view asit places the lesion at an early stage of visual processing. On the other hand, carbonmonoxide characteristically causes subcortical white matter degeneration, with occipitaland splenial fibres frequently affected (Hsu and Ch'eng, 1938; Schwedenberg, 1959;Lacey, 1981). Subcortical localization would parallel the accepted pathogeneticmechanisms of other forms of disturbed visual recognition (associative visual agnosiaand pure alexia), and would account for the relative specificity of carbon monoxidefor this syndrome, as white matter degeneration is less frequently observed in hypoxicbrain injury of other aetiologies.
In the absence of pathologically studied material, attempts have been made to distinguishbetween these proposed localizations by in vivo techniques: detailed visual fieldexamination, neuroimaging studies, and visual-evoked potentials. Campion (1984)performed detailed mapping of the central visual field of a patient with carbon monoxide-induced visual agnosia and demonstrated multiple minute scotomata. He suggested thatthese arose due to patchy cortical infarctions, although scattered subcortical lesions couldproduce a similar clinical picture. Indeed, bilateral subcalcarine infarctions were visualizedby CT scanning in Campion's patient. No such lesions, however, were evident oncomputerized tomography of our patient or a similar patient reported by Alexander andAlbert (1983). MRI scanning performed in our patient demonstrated focal occipitalatrophy bilaterally. There were no discrete lesions visible in the deep white matteralthough injury to immediately subcortical white matter could not be excluded withcertainty.
Pattern reversal visual-evoked responses were absent in the patient of Alexander andAlbert, which they felt was indicative of extensive damage to occipital cortex. Normalresponses were elicited in our patient. These normal responses, however, do not excludelaminar necrosis of the occipital cortex as recent studies in primates suggest generationof most components of the VEP in lamina IV (Kraut et al., 1985), which is highly resistantto laminar necrosis. Thus the question of localization of carbon monoxide-induced visualagnosia to cortical versus subcortical structures remains unresolved and may ultimatelyrequire pathological examination for resolution.
In summary, carbon monoxide toxicity can induce a visual agnosia with apperceptivefeatures, seldom seen with other types of cerebral injury. This syndrome occurs afterrecovery from cortical blindness and is a characterized misperception of elemental shapeand form, alexia, and impairment of visual imagery. Pathology is localized to bilateraloccipital lesions. Long-term prognosis for recovery of visual function is poor.
ACKNOWLEDGEMENTS
The authors wish to thank DT Joseph Rizzo, Department of Ophthalmology, Boston City Hospital, forperforming detailed ophthalmological and visual field testing. We especially wish to convey our gratitudeto Dr Alexandra Adler whose publications inspired our efforts and who provided invaluable assistancein helping us to locate the patient.
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from
VISUAL AGNOSIA REVISITED 799
REFERENCES
ABADI RV, KUUKOWSKI JJ, MENDELL P (1981) Visual performance in a case of visual agnosia. In:Functional Recovery from Brain Damage. Edited by M. W. van Hof and G. Mohn. Amsterdam andOxford: Elsevier, pp. 275-286.
ADLER A (1944) Disintegration and restoration of optic recognition in visual agnosia: analysis of a case.Archives of Neurology and Psychiatry, Chicago, 51, 243—259.
ADLER A (1950) Course and outcome of visual agnosia. Journal of Nervous and Mental Disease, 111,41—51.AJAX ET (1967) Dyslexia without agraphia: prognostic considerations. Archives of Neurology, Chicago,
17, 645-652.ALEXANDER MP, ALBERT ML (1983) The anatomical basis of visual agnosia. In: Localization in
Neuropsychology. Edited by A. Kertesz. New York and London: Academic Press, pp. 393-415.BAUER RM, RUBENS AB (1985) Agnosia. In: Clinical Neuropsychology. Second edition. Edited by
K. M. Heilman and E. Valenstein. New York and Oxford: Oxford University Press, pp. 187-241.BENSON DF, GESCHWIND N (1969) The alexias. In: Handbook of Neurology, Volume 4. Edited by
P. J. Vinken and G. W. Bruyn. Amsterdam: North-Holland, pp. 112-140.BENSON DF, GREENBERG JP (1969) Visual form agnosia: a specific defect in visual discrimination. Archives
of Neurology, Chicago, 20, 82-89.BRIERLEY JB, GRAHAM DI (1984) Hypoxia and vascular disorders of the central nervous system. In:
Greenfield's Neuropathology. Fourth edition. Edited by J. H. Adams, J. A. N. Corsellis andL. W. Duchen. London: Edward Arnold, pp. 145-148.
CAMPION J (1984) Evoked potentials and discriminative capacities in a case of visual agnosia. In: EvokedPotentials II: The Second International Evoked Potentials Symposium. Edited by R. H. Nodar andC. Barber. Boston and London: Butterworth, pp. 485-472.
COBB S, LINDEMANN E (1943) Symposium on management of Cocoanut Grove burns at MassachusettsGeneral Hospital; neuropsychiatric observations. Annals of Surgery, 117, 814—824.
DEJERINE J (1892) Contribution a l'&ude anatamopathologique et clinique des differents variet£s de cecit6verbal. Mimoires de la Sociiti Biologique, 4, 61 —90.
DE RENZI E, VIGNOLO LA (1962) The Token Test: a sensitive test to detect receptive disturbances inaphasics. Brain, 85, 665-678.
DURRELL DD (1955) Durrell Analysis of Reading Difficulty. New York: Harcourt Brace Javonovich.FARAH MJ (1984) The neurological basis of mental imagery: a componential analysis. Cognition, 18,
245-272.GARLAND H, PEARCE J (1967) Neurological complications of carbon monoxide poisoning. Quarterly Journal
of Medicine, 36, 445-455.GESCHWIND N (1965) Disconnexion syndromes in animals and man. Parts I and n. Brain, 88, 237-294,
585-644.GiLMORE JV, GILMORE EC (1968) Gilmore Oral Reading Test. San Antonio, TX: Psychological Corporation.GINSBERG MD (1980) Carbon monoxide. In: Experimental and Clinical Neurotoxicology. Edited by
P. S. Spencer and H. H. Schaumburg. Baltimore and London: Williams and Wilkins, pp. 374-394.GOLDSTEIN K (1948) Language and Language Disturbances: Aphasic Symptom Complexes and their
Significance for Medicine and Theory of Language. New York: Grune and Stratton, pp. 119-125.GOLDSTEIN K, GELB A (1918) Psychologische Analysen hirnpathologischer Falle auf Grand von
Untersuchungen Hirnverletzter. Zeitschrifi fUr die Gesamte Neurologie und Psychiatrie, 41, 1 —142.GOODGLASS H, KAPLAN E (1972) The Assessment of Aphasia and Related Disorders. Philadelphia: Lea
and Febiger.GREENBLATT SH (1973) Alexia without agraphia or hemianopsia: anatomical analysis of an autopsied case.
Brain, 96, 307-316.HOOPER H (1981) Hooper Visual Organization Test. Los Angeles: Western Psychological Services.Hsu YK, CH'ENG YL (1938) Cerebral subcortical myelinopathy in carbon monoxide poisoning. Brain,
61, 384-392.KAPLAN E, GOODGLASS H, WEINTRAUB S (1978) The Boston Naming Test. Philadelphia: Lea and Febiger.KERTESZ A (1979) Visual agnosia: the dual deficit of perception and recognition. Cortex, 15, 403-419.KRAUT MA, AREZZO JC, VAUGHAN HG (1985) Intracortical generators of the flash VEP in monkeys.
Electroencephalography and Clinical Neurophysiology, 62, 300—312.
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from

800 S. A. SPARR AND OTHERS
LACEY DJ (1981) Neurologic sequelae of acute carbon monoxide intoxication. American Journal of Diseasesof Children, 135, 145-147.
LANDIS T, GRAVES R, BENSON DF, HEBBEN N (1982) Visual recognition through kinaesthetic mediation.Psychological Medicine, 12, 515-531.
LAPRESLE J, FARDEAU M (1967) The central nervous system and carbon monoxide poisoning. II. Anatomicalstudy of brain lesions following intoxication with carbon monoxide (22 cases). Progress in BrainResearch, 24, 31-74 .
LEVINE DN, WARACH J, FARAH M (1985) Two visual systems in mental imagery: dissociation of 'what'and 'where' in imagery disorders due to bilateral posterior cerebral lesions. Neurology, Cleveland,35, 1010-1018.
LISSAUER H (1890) Ein Fall von Seelenblindheit nebsteinem Beitrage zur Theorie derselben. Archiv fUrPsychiatrie und Nervenkrankheiten, 21, 222-270.
NIELSEN JM (1946) Agnosia, Apraxia, Aphasia, Their Relative Value in Cerebral Localization. New Yorkand London: Paul Hoeber, pp. 74—75.
RAVEN JC (1960) Guide to the Standard Progressive Matrices. London: H. K. Lewis.RIDDOCH MJ, HUMPHREYS GW (1987) A case of integrative visual agnosia. Brain, 110, 1431-1462.SCHILDER P, ISAKOWER O (1928) Optisch-raumliche Agnosie und Agraphie. Zeitschrift far die Gesamte
Neurologie und Psychiatrie, 113, 102-142.SCHWEDENBERG TH (1959) Leukoencephalopathy following carbon monoxide asphyxia. Journal of
Neuropathology and Experimental Neurology, 18, 597—608.SOLOMON AP (1932) Acalculia, other agnosias and multiple neuritis following carbon monoxide poisoning.
Medical Clinics of North America, 16, 531-538.VINCENT FM, SADOWSKY CH, SAUNDERS RL, REEVES AG (1977) Alexia without agraphia, hemianopia,
or color-naming defect: a disconnection syndrome. Neurology, Minneapolis, 27, 689—691.VON HAGEN KO (1941) Two clinical cases of mind blindness (visual agnosia) one due to carbon monoxide
intoxication, one due to diffuse degenerative process. Bulletin of the Los Angeles Neurological Society,6, 191-194.
WECHSLER D (1945) Standardized memory scale for clinical use. Journal of Psychology, 19, 87-95.WECHSLER D (1981) Wechsler Adult Intelligence Scale—Revised. San Antonio, TX: Psychological
Corporation.WOODCOCK RW (1973) Woodcock Reading Mastery Tests. Circle Pines, MI: American Guidance Service.
{Received March 7, 1989. Revised April 27, 1990. Accepted May 15, 1990)
at National Sun Y
at-sen University on A
ugust 22, 2014http://brain.oxfordjournals.org/
Dow
nloaded from