a freedom magazines publication · a freedom magazines publication supplement to c l i n ......
TRANSCRIPT

A F R E E D O M M A G A Z I N E S P U B L I C A T I O N
Supplement to
CLIN
ICAL STRATEGIESINLTC
Council for Anemia
An Accredited Program Sponsored by Medical Education Resources Inc., a nonprofit medical education company, through an unrestricted educational grant from Amgen, Inc.

22
Robert P. Geronemus, MDPresidentSouth Florida Nephrology
Associates Private PracticeFt. Lauderdale, Florida
Jeffrey Hoggard, MDMedical DirectorGreenville Dialysis CenterGreenville, North Carolina
Anne M. Murray, MD, MScAssistant Professor of MedicineUniversity of MinnesotaHennepin County Medical Center,
GeriatricsMinneapolis, Minnesota
Armon B. Neel, Jr., PharmD, CGP, FASCP
PresidentMedicationXpert, LLC Griffin, Georgia
Miriam B. Rodin, MD, PhD,CMD
Assistant Professor of ClinicalMedicine
The University of ChicagoChicago, Illinois
Laurence Z. Rubenstein, MD,MPH, FACP
Professor of Geriatric MedicineUCLA School of MedicineDirector, Sepulveda VA GRECCLos Angeles, California
Michael W. Schuster, MDProfessor of Clinical Medicine at
the Weill Medical College ofCornell University
Director of Bone MarrowTransplantationand Clinical ResearchHematology/Oncology Division
New York Presbyterian HospitalNew York, New York
Eric G. Tangalos, MD, CMDChair, Division of Community
Internal MedicineProfessor of MedicineMayo Medical SchoolRochester, Minnesota
Lynn Williams Shipp, RPh,FASCP
President ofSenior Care PharmacyBoulder, Colorado
Shing-shing Yeh, PhD, MDAssociate Professor in MedicineUniversity Hospital SUNY at
Stony BrookGeriatric Division Department
of MedicineVA Medical Center at NorthportNorthport, New York
Council Consensus Committee
Authors
Methods
Council ChairJohn E. Morley, MB, BCh
Dammert Professor of Gerontology Director, Division of Geriatric Medicine
St. Louis University Health Sciences CenterDirector, GRECC, St. Louis Medical Center
St. Louis, Missouri
Consensus CommitteePublication Chair
David R. Thomas, MD, CMD, FACP, AGSFProfessor of Medicine
Division of Geriatric MedicineSt. Louis University Health Sciences Center
St. Louis, Missouri
Diagnosis and Management of Anemia in Long-Term Care
This expert panel of interdisciplinary thought leaders representing academia and the medical community was assembled by Medical Education Resources (MER), a nonprofit medical educationcompany, to review the existing literature and author this publication on thediagnosis and management of anemia in long-term care. Where evidenceexisted, it served as the basis for specific recommendations. In the absenceof evidence, consensus was obtained. Programs in Medicine was selectedto facilitate a summit meeting and a closed Internet discussion forum toobtain consensus agreement by the members of the Council on the information presented within this publication.
August 2003

3
Diagnosis and Management of Anemia in Long-Term Care
SPONSORSHIP AND ACCREDITATION INFORMATION
Target AudienceThis program is intended for long-term care
physicians, pharmacists, and nurses who diag-
nose and treat elderly patients with anemia.
Educational ObjectivesUpon completion of this program, participants
should be able to:
• Describe the epidemiology of anemia in
long-term care.
• Define the differential diagnosis of anemia
in long-term care.
• Discuss the management options for
anemia in long-term care.
Program Completion TimeBased upon trials, the estimated time to
complete this program is 1 hour.
Educational Grant This program is made possible by an unrestricted
educational grant from Amgen, Inc.
SponsorshipThis activity is sponsored by Medical Education
Resources Inc., a nonprofit medical education
company. Programs in Medicine was selected to
manage program logistics.
Physician AccreditationMedical Education Resources is accredited by the
Accreditation Council for Continuing Medical
Education (ACCME) to sponsor continuing med-
ical education for physicians.
Credit DesignationMedical Education Resources designates this
continuing medical education activity for up to
1 credit hour in category 1 of the Physician’s
Recognition Award of the American Medical
Association. Each physician should claim only
those hours of credit that he/she actually spent
in the activity.
This CME activity was planned and produced
in accordance with the ACCME Essentials.
Nursing AccreditationThis program qualifies for 1.25 contact hours.
Medical Education Resources is approved as a
provider of continuing education in nursing
(CNE) by the Colorado Nurses’ Association,
which is accredited as an approver of CNE by
the American Nurses Credentialing Center’s
Commission on Accreditation.
Provider approved by the California Board of
Registered Nursing, Provider CEP # 12299, 1.25
contact hours.
Each participant should claim only those hours of
credit that he/she actually spent in the educational
activity.
Pharmacy AccreditationMedical Education Resources (MER) is approved by
the American Council of
Pharmaceutical Education as a
provider of continuing pharmaceuti-
cal education. MER designates this
continuing education activity for 1.0 contact hour
(0.1 CEUs) in states that recognize ACPE. Universal
Program Number: 816-000-03-043-H04.
DisclaimerThe content and views presented in this educational
program are those of the faculty and do not neces-
sarily reflect those of Medical Education Resources,
Amgen, Inc., or MultiMedia HealthCare/Freedom,
LLC. The authors have disclosed if any unlabeled use
of products is mentioned in the material. Before
prescribing any medicine, primary references and
full prescribing information should be consulted.
August 2003

4
Diagnosis and Management of Anemia in Long-Term Care
August 2003
4
Faculty Disclosure Policy It is the policy of Medical Education Resources
(MER) to ensure balance, independence, objec-
tivity, and scientific rigor in all its educational
activities. All faculty participating in our pro-
grams are expected to disclose any relationships
they may have with commercial companies
whose products or services may be mentioned
so that participants may evaluate the objectivi-
ty of the presentations.
Dr. Robert P. Geronemus reported that he
serves on the Speakers’ Bureau for Amgen, Inc.,
Ortho Biotech Products, and Watson
Laboratories.
Dr. Jeffrey Hoggard reported that he serves
on the Speakers’ Bureau for Amgen, Inc.
Dr. John Morley reported that he receives
Grant/Research support from Organon Inc.,
Merck & Co. Inc, Nestec Ltd, Bayer Corporation,
and B. Braun McGaw. He serves on the
Speakers’ Bureau for LXN, Organon Inc.,
GeriMed of America, UniMed Pharmaceuticals
Inc., Solvay Pharmaceuticals, Essentia, Alza
Pharmaceuticals, Pharmacia & Upjohn, Glaxo
Wellcome, B. Braun McGaw, Bristol-Myers
Squibb, Novartis, Pfizer Inc/Parke-Davis and
GlaxoSmithKline. He receives grant support
from Solvay Pharmaceuticals to undertake a
study on testosterone and renal failure. He is
also an 8% shareholder of CUM
Pharmaceuticals, which is developing an
inhalation form of testosterone.
Dr. Anne M. Murray reported that she is a
consultant for Amgen, Inc.
Dr. Miriam B. Rodin reported that she is a
consultant for Amgen, Inc.
Dr. Michael W. Schuster reported that he
receives Grant/Research support from Amgen,
Inc. He serves on the Speakers' Bureau for
Amgen, Inc. and Ortho Biotech Products.
Dr. Eric G. Tangalos reported that he is a con-
sultant for Omnicare, Eli Lilly and Company,
Janssen Pharmaceutica, and Abbott Laboratories.
Dr. David Thomas reported that he is a con-
sultant for Amgen, Inc.
Dr. Armon B. Neel, Dr. Lawrence Z.
Rubenstein, Dr. Lynn Williams Shipp, and
Dr. Shing-shing Yeh reported that they do
not have a financial arrangement or affiliation
with commercial companies whose products
may be mentioned in this program.
Obtaining Continuing Education CreditTo receive credit, participants must complete
the CME/CE Test Questionnaire that appears at
the end of this program and fax or mail it to:
Medical Education Resources1500 West Canal Court
Littleton, CO 80120Fax: 303-798-5731
A minimum score of 70% on the Continuing
Pharmaceutical Education Test is required for
credit. A certificate of completion will be
mailed within 4 weeks of receipt of the com-
pleted answer sheet.
Program Release Date: August 2003 Program Expiration Date: August 2005
FACULTY DISCLOSURE POLICY

August 2003
5
AAnemia is very common in nursing home resi-
dents and is associated with increased morbidity
and mortality. While some of this anemia is due
to deficiencies in iron, folate, or vitamin B12, the
most common cause is anemia of chronic dis-
ease. Much of the anemia of chronic disease is
associated with chronic kidney disease. Erythro-
poietin, or epoetin alfa, has been demonstrated
to restore hemoglobin concentrations approach-
ing normal in these persons. Darbepoetin alfa
has a longer half-life than that of epoetin alfa,
and can thus be administered every other week.
Studies are in progress on less frequent dosing.
The Council for Anemia Clinical Strategies in
Long-Term Care recommends that the causes of
anemia should be aggressively sought and that
appropriate treatment should be given to correct
underlying causes and restore hemoglobin con-
centrations to normal.
Anemia is not a normal finding in older per-
sons, and hemoglobin concentration should
not be adjusted downward in older persons.1,2
Hemoglobin and hematocrit values differ little
between the healthy elderly population and the
younger population. A hemoglobin concentra-
tion of less than 13 g/dL in men and less than
12 g/dL in women defines anemia, according
to World Health Organization standards.
While the World Health Organization cutoffs
for anemia may be reasonable, they should not
be considered optimal hemoglobin concentra-
tion. For example, women with a hemoglobin
concentration between 13-14 g/dL have better
mobility and lower mortality compared to
those with a hemoglobin concentration of less
than 12 g/dL.3
We know from the third National Health and
Nutrition Examination Survey (NHANES II)
that there is a significant increase in anemia with
each decade of life over the age of 70. The preva-
lence jumps from 10.6% in males aged 70-79
years to 22% in males aged 80-89 years. For
each decade of life over the age of 70 years, the
percentage of anemic patients is consistently
higher in men than in women, probably in part
due to falling androgen levels. Sex differences in
hemoglobin concentration result chiefly from
differences in testosterone concentration. Hypo-
gonadism in older males (andropause) is com-
monly associated with approximately a 1 g/dL

6
Diagnosis and Management of Anemia in Long-Term Care
fall in hemoglobin concentration.4 Further-
more, men who have functional hypogonadism
from pituitary adenomas are anemic,5 and men
with prostate cancer who are undergoing thera-
py with total androgen blockade are anemic.6
Anemia is as abnormal in the elderly as it is
in the young. It should be investigated and
treated appropriately, irrespective of age.
A Brief History of Blood As long ago as 2500 BCE, Egyptians induced ane-
mia to cure disease by bleeding from the foot and
neck. In 350 BCE, Aristotle considered blood to
be the mirror of the soul. However, it was not
until 1628 that William Harvey demonstrated
that blood circulates throughout the body. Thirty
years later, Jan Swammerdam, a Dutch micro-
scopist, described red blood cell morphology.
The first recorded blood transfusion was car-
ried out in 1665 by Richard Lower, who used a
syringe made from a goose quill and bladder to
connect the jugular vein of one dog to another.
The anemic dog survived. Two years later, Jean-
Baptiste Denis transfused a teenage boy with
camel blood, and the boy lived. In 1795, Philip
Syng Physick performed the first human-to-
human blood transfusion, although it was not
until 1818 that another blood transfusion
between humans was published. In 1907, at
Mount Sinai Hospital in New York, the first
transfusion using crosstyping of blood was per-
formed. In 1917, the United States Army started
to use type O blood preserved with a citrate-glu-
cose solution to store blood for casualties during
August 2003
FIGURE I

7
Diagnosis and Management of Anemia in Long-Term Care
the Battle of Cambrai. This led to the establish-
ment of blood banks in hospitals in the 1920s.
During World War II, the Red Cross widely
advertised for blood donations using a series of
posters to encourage Americans to give blood for
the soldiers (Figure 1). In 1963, Paul Beeson
reported jaundice in persons who had received a
blood transfusion. Thus, the understanding of
the nonbenign nature of transfusions was
enhanced with the first report of transfusion-
transmitted hepatitis.
Erythropoietin is a 30,400 dalton glycopro-
tein that is produced by the kidney and stimu-
lates erythropoiesis. Its existence was first hinted
at by Camot and Deflande in 1906, when they
demonstrated that serum from anemic rabbits
increased red cell mass in nonanemic rabbits.
They named this substance “hematopoietine,”
and it was renamed erythropoietin in 1948 by
Bonddorf and Jelaviste after it was shown to
have a specific effect on red blood cells. In 1957,
Jacobson and colleagues identified the kidney as
the source of erythropoietin. Erythropoietin was
purified in 1957, and the gene was cloned in
1985. One year later, it was clearly established to
reverse the anemia of chronic renal disease.
Prevalence of Anemia inOlder PersonsThere is a marked increase in the prevalence of
anemia with aging. In a population-based
study in Olmsted County, Minnesota, among
618 persons older than 65 years, the corrected
annual incidence of anemia was higher in men
(90.3 per 1000; 95% CI, 79.2-101.4) than
women (69.1 per 1000; 95% CI, 62.3-75.8),
and rose with age.7 Using the Established
Population data for 3946 adults aged 71 years
or older in three communities, hemoglobin
concentration level was inversely associated
with age. In men and women aged 71-74 years,
9% were anemic. The proportion of anemic
persons increased differentially with age, reach-
ing 41% for men and 21% for women, aged
90 years or older, respectively.8
In a study of 732 consecutively admitted
hospital patients to an acute geriatric ward,
26% had a hemoglobin concentration below
11.5%.9 Recent studies in long-term care insti-
tutions in Israel and Spain have shown a very
high prevalence of anemia in these settings. In
481 long-term care patients with an average
age of 81.4 years, the prevalence of anemia was
31.4%.10 In the Spanish study, the prevalence
of anemia was 40%.11
Anemia associated with chronic renal insuf-
ficiency is common. Approximately 13.5 mil-
lion adults have a creatinine clearance of 50
mL/min or less, and about 800,000 adults have
chronic renal insufficiency–associated anemia,
defined as a hemoglobin concentration of
<11 g/dL, according to a study of NHANES III
data. In that study, it was found that a statisti-
cally significant decrease in hemoglobin con-
centration was seen among men starting at a
creatinine clearance of 70 mL/min or less and
among women starting at 50 mL/min or less.
At any given level of creatinine clearance, men
had a larger decrease in hemoglobin concentra-
tion than women. For example, compared to
subjects with a creatinine clearance of greater
than 80 mL/min, the decrease in hemoglobin
concentration for subjects with a creatinine
clearance of 20-30 mL/min was 1.0 g/dL in
August 2003
8
Diagnosis and Management of Anemia in Long-Term Care
women and 1.4 g/dL in men.7
A substantial number of subjects with
chronic renal insufficiency may not have suffi-
cient iron stores to support erythropoiesis, as
judged by the National Kidney Foundation
targets for transferrin saturation or serum fer-
ritin. In NHANES III, among those persons
with a creatinine clearance of 20-30 mL/min,
46% of women and 19% of men had a trans-
ferrin saturation of less than 20%, and 47% of
women and 44% of men had a serum ferritin
of less than 100 ng/mL.12
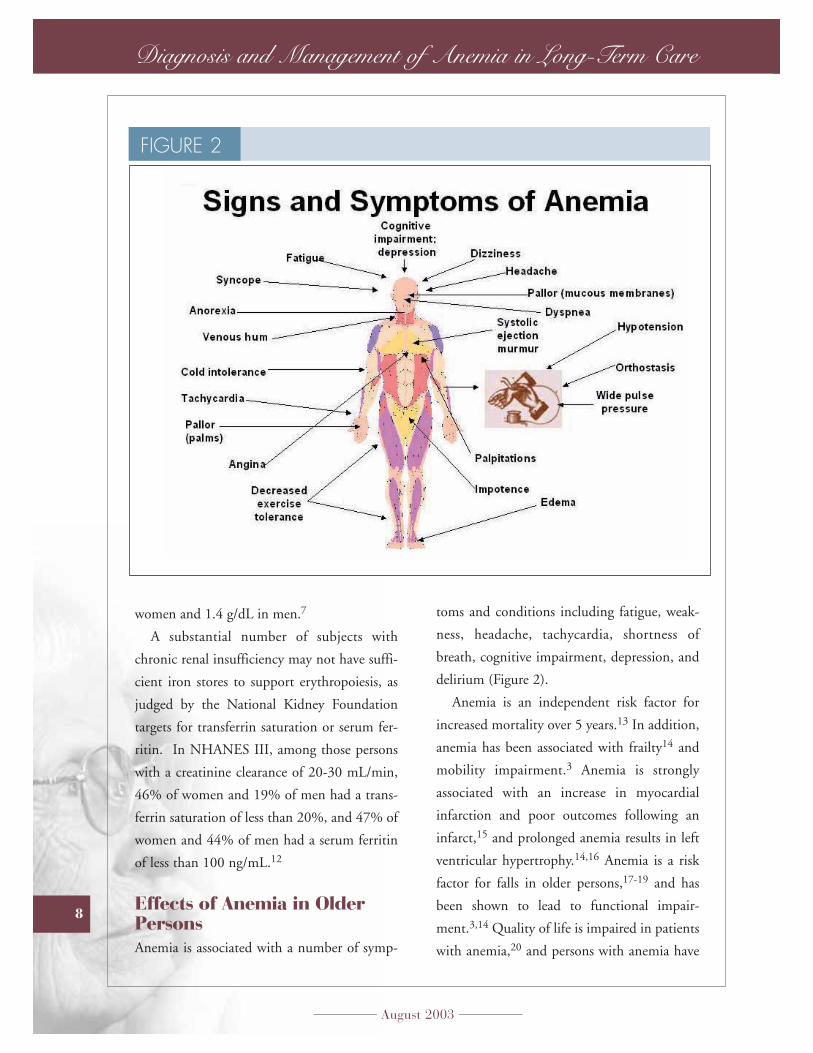
Effects of Anemia in OlderPersonsAnemia is associated with a number of symp-
toms and conditions including fatigue, weak-
ness, headache, tachycardia, shortness of
breath, cognitive impairment, depression, and
delirium (Figure 2).
Anemia is an independent risk factor for
increased mortality over 5 years.13 In addition,
anemia has been associated with frailty14 and
mobility impairment.3 Anemia is strongly
associated with an increase in myocardial
infarction and poor outcomes following an
infarct,15 and prolonged anemia results in left
ventricular hypertrophy.14,16 Anemia is a risk
factor for falls in older persons,17-19 and has
been shown to lead to functional impair-
ment.3,14 Quality of life is impaired in patients
with anemia,20 and persons with anemia have
August 2003
FIGURE 2

9
Diagnosis and Management of Anemia in Long-Term Care
a high level of fatigue.21 Figure 3 summarizes
the major adverse effects of anemia on older
persons.
Causes of AnemiaIn one study of the prevalence of anemia in
hospitalized older persons, the most common
cause of anemia was anemia of chronic disease,
accounting for 35-40%. Iron deficiency ane-
mia accounted for between 8% and 15%,
blood loss accounted for 7%, myelodysplasia
for about 5%, Vitamin B12 deficiency for
another 5%, and chronic kidney disease was
responsible for 6-8%. As in most studies of
older persons, a large number of anemias had
no diagnosis.9 The causes and prevalence of
anemia vary between patient care settings,
depending on the population studied and the
author’s classification system.
Renal insufficiency accounts for the greatest
percentage of anemic individuals with the
diagnosis of anemia of chronic disease (27%).
Most of these patients have an erythropoietin
deficiency. However, other causes of anemia of
chronic disease account for 73% of cases.
These conditions include cancer (non-
chemotherapy patients), congestive heart fail-
ure, hepatitis C, inflammation, diabetes, and
rheumatoid arthritis. Of course, patients can
have more than one cause of anemia of chron-
ic disease (eg, iron deficiency, chronic kidney
disease, and rheumatoid arthritis).
August 2003
FIGURE 3

10
Diagnosis and Management of Anemia in Long-Term Care
Similar findings on the etiology of anemia
in long-term care have been reported. In the
previously cited study in Israel, it was found
that 65.6% of nursing home residents who
were anemic had anemia of chronic disease,
13.2% had anemia attributed to chronic kid-
ney disease, and 4% had nutritional causes for
their anemia.
In summary, in the older population, ane-
mia of chronic disease and anemia associated
with chronic renal disease are the most com-
mon causes of anemia. However, nutritional
anemias including deficiency in iron, vitamin
B12, or folate, and anemia due to blood loss
and drug side effects should be excluded.
ErythropoiesisNormal hematopoiesis consists of the transfor-
mation of multipotential stem cells to commit-
ted progenitors and then into erythrocytes
(Figure 4). Once a progenitor is committed to
forming erythrocytes, it is stimulated by ery-
thropoietin and testosterone, and inhibited by
a variety of cytokines (eg, tumor necrosis factor
alpha, interferon gamma, and interleukin-6).
Dependent on the balance of the stimulus, the
cells either become mature erythrocytes or
undergo an apoptotic death.
Differential Diagnosis ofAnemiaAnemia can be due to failure of the bone mar-
row to manufacture adequate blood compo-
nents, gradual or rapid blood loss from hemor-
rhage, or rapid breakdown of blood compo-
nents from hemolysis. Causes of failure of the
August 2003
FIGURE 4

11
Diagnosis and Management of Anemia in Long-Term Care
bone marrow to produce adequate blood com-
ponents include inadequate nutrients (vitamin
B12, folate, pyridoxine, or iron) necessary for
blood production, primary impairment of
hemoglobin synthesis (hemoglobinopathy), or
altered maturation of blood cells (myelodys-
plastic syndromes). This complex progression
of erythrocyte maturation lends itself to sever-
al strategies for the differential diagnosis of
anemia.
A corrected reticulocyte count is useful to
determine bone marrow function. Anemia
associated with an increased reticulocyte count
occurs when the bone marrow responds to red
cell destruction (hemolysis) or hemorrhage.
The presence of elevated concentrations of
unconjugated bilirubin and lactic dehydroge-
nase usually accompany hemolysis. If these
concentrations are normal, a source of blood
loss should be sought, including gastrointesti-
nal bleeding, intracranial bleeds, epistasis,
hemoptysis, trauma (consider liver, spleen, or
hip), vaginal bleeding, and severe ecchymoses.
Since gastrointestinal bleeding is the most
common cause of occult blood loss, a stool
occult blood test should be obtained.
Absence of elevated lactate dehydrogenase
(LDH) and indirect bilirubin only tell us that
there is no hemolysis. Many conditions—not
just blood loss—may be present. For example,
myelodysplastic syndrome, which is on the rise
in the elderly in the U.S., is associated with a
August 2003
FIGURE 5

12
Diagnosis and Management of Anemia in Long-Term Care
normal LDH, normal bilirubin, and low retic-
ulocyte count. A low or normal corrected retic-
ulocyte count in the presence of anemia indi-
cates an inadequate bone marrow response
(Figure 5). In the presence of a low corrected
reticulocyte count, determination of red cell
morphology indices is useful. An elevated
mean corpuscular volume (macrocytosis) sug-
gests vitamin B12 or folate deficiency, hepatic
disease, myelodysplasia, hypothyroidism, and
alcoholism. Drugs may cause either hemolysis
or macrocytosis—notably, phenytoin, metho-
trexate, and azathioprine.
Measurement of vitamin B12 and folate
concentrations will determine anemia due to
these causes in the majority of cases.
Confirmation of nutritional deficiency in
those patients who have values in the lower
normal range should be obtained. Diagnosis
of vitamin B12 deficiency is typically based on
measurement of serum vitamin B12 levels;
however, about 50% of patients with subclin-
ical disease have normal B12 levels. A more
sensitive method of screening for vitamin B12
deficiency is measurement of serum methyl-
malonic acid and homocysteine levels, which
August 2003
Diagnosis and Management of Myelodysplasia
DIAGNOSIS TEST FINDINGHemoglobin Decreased (100%)Neutrophils Decreased (50%)Thrombocytes Decreased (25%)Peripheral smear Hyposegmented white cell nuclei
Unusual white cell granular content
Megakaryocytes Erythropoietin May be very highBone marrow Hypercellularity
Ringed sideroblasts Increased blasts
Karyotype analysis Deletion chromosome 5qMonosomy chromosome 5 or 7
Vitamin B12 NormalFolate Normal
MANAGEMENTErythropoietinGranulocyte-colony stimulating factorTransfusion when symptomatic
TABLE I

13
Diagnosis and Management of Anemia in Long-Term Care
are increased early in vitamin B12 deficiency. A
homocysteine level will be elevated in both
vitamin B12 and folate deficiencies, but a
methylmalonic acid level will be elevated only
in vitamin B12 deficiency. Renal failure is the
only other confounding cause of an elevated
methylmalonic acid concentration. Use of the
Schilling test for detection of pernicious ane-
mia has been supplanted for the most part by
serologic testing for parietal cell and intrinsic
factor antibodies.
Myelodysplastic syndrome is a bone marrow
failure state associated with varying degrees of
pancytopenia. About half of these patients will
also have neutropenia. An elevated mean cor-
puscular volume with abnormalities in red cell
corpuscular shape suggests myelodysplastic
(MDS) anemia when nutritional deficiency,
drugs, and chemotherapy have been excluded.
A peripheral blood smear in patients with
MDS may show hyposegmented nuclei in the
neutrophils (pseudo Pelger-Huët phenome-
non) or abnormal granular content in the
white cells. Approximately one-quarter of the
patients have thrombocytopenia with
megakaryocytes in the peripheral smear. Bone
marrow examination confirms the diagnosis
with increased cellularity, maturational abnor-
malities, ringed sideroblasts, and an increase in
blasts as well as karyotype abnormalities (eg,
loss of the long arm of chromosome S). The
bone marrow examination may reveal different
abnormalities that are useful in classifying the
subtype of MDS. Measurements of erythropoi-
etin should be undertaken because those with
concentration below 200 μm/mL often have
an excellent response to treatment with ery-
thropoietin and granulocyte-colony stimulat-
ing factor. The diagnosis and treatment of
myelodysplasia are summarized in Table I.
In persons with a low or normal mean cor-
puscular volume, the likely diagnoses include
anemia of chronic disease, anemia of renal dis-
ease, iron deficiency anemia, or thalassemia
minor. The differential diagnosis of iron defi-
ciency anemia from anemia of chronic disease
is given in Table II. Persons with microcytosis,
a low serum iron, and low ferritin concentra-
August 2003
Comparison of Iron Deficiency Anemia and Anemia of Chronic Disease
IRON DEFICIENCY ANEMIA OF ANEMIA CHRONIC DISEASE
Mean corpuscular volume Normal or Decreased Decreased or Normal Serum iron Decreased DecreasedTotal iron-binding capacity Increased Normal to DecreasedSerum ferritin Decreased IncreasedSoluble transferrin receptor Increased Normal to Decreased
TABLE II

14
Diagnosis and Management of Anemia in Long-Term Care
tions have iron deficiency anemia. If the iron is
low and the ferritin is high, this is suggestive of
anemia of chronic disease. Unfortunately, these
and other causes of anemia commonly coexist
in older persons. In these cases, soluble trans-
ferrin receptor may be useful in determining
the diagnosis.
Circulating soluble transferrin receptors are
a relatively new tool in the diagnosis of anemia.
They are elevated in iron deficiency anemia
even in the presence of chronic disease, but
normal or only slightly raised in anemia of
chronic disease. Since ferritin concentrations
are elevated in inflammation, liver disease,
renal disease, cancer, and in some elderly
women, soluble transferrin receptors, can be of
use in making the diagnosis of iron deficiency.
Soluble transferrin receptors divided by the log
of ferritin (< 2.55) is the best method of differ-
entiating anemia of chronic disease from ane-
mia of chronic disease associated with iron
deficiency anemia.22 However, there does not
appear to be much advantage of these newer,
more expensive methods over measuring total
iron-binding capacity.23
Anemia of chronic kidney disease is diag-
August 2003
FIGURE 6

15
Diagnosis and Management of Anemia in Long-Term Care
nosed by recognizing renal disease in associa-
tion with a low erythropoietin level. If the
serum creatinine is greater than 2 mg/dL, it is
unnecessary to measure erythropoietin.
However, older persons can have a declining
glomerular filtration rate in face of a relatively
normal serum creatinine. This is because of the
loss of lean mass (sarcopenia) associated with
aging. This can be even more marked in the
nursing home resident with cachexia. For
example, an 85-year-old female nursing home
resident with a hemoglobin concentration of
10 g/dL who weighs 55 kg and has a serum
creatinine of 1.3 mg/dL (normal range) will
have a creatinine clearance calculated by the
Cockcroft-Gault equation (Figure 6) of 27.5
mL/min.24 For this reason creatinine clearance
should be calculated in all nursing home resi-
dents with anemia to determine their renal sta-
tus. The Cockcroft-Gault equation will
demonstrate that the majority of older female
nursing home residents with a creatinine of 1.2
mg/dL or greater have severe renal impair-
ment.
The Cockcroft-Gault equation is not perfect
but has been shown to be strongly correlated
with more accurate measures of GFR measured
creatinine clearance.25,26 A schematic diagram
for evaluation of anemia in long-term care is
given in Figure 7.
August 2003
FIGURE 7

16
Diagnosis and Management of Anemia in Long-Term Care
Management of Anemia in Long-Term Care
Nutritional Anemia
Anemia due to folate or vitamin B12 defi-
ciency is treated by replacement of the vitamin.
Vitamin B12 can be replaced either by injec-
tions (1000 μg weekly for 1 month, then
monthly thereafter), orally (1000 μg daily,
which should not be given with food), or
intranasally. Folate 1 mg should be used to
treat folate deficiency and should be used dur-
ing the first few weeks of vitamin B12 defi-
ciency.
In persons with iron deficiency, the recom-
mended treatment is iron sulfate 325 mg three
times a day, providing 195 mg of elemental
iron per day.27-29 The sulfate moiety can cause
gastrointestinal distress, and if this occurs, iron
in the form of gluconate or fumerate may be
helpful. Some experts suggest that iron sulfate
once a day may have a similar effect to three-
times-a-day dosing if absorption is normal.
The duration of iron therapy may be longer
when once-a-day dosing is used. Whatever the
chosen dose, a reticulocyte count should be
obtained one week after starting iron. If there
is not a robust reticulocyte response, intra-
venous iron should be considered. An
approach to the management of anemia in
long-term care residents is given in Table III.
Transfusions are regularly given to older
persons who become symptomatic, have their
hemoglobin concentration drop below 8 g/dL,
or who have an acute bleed. However, it is
important to realize that despite adequate care-
ful cross-matching of blood, complications are
all too common. Transfusion reactions can lead
to hemolysis and fever. Transfusions are often
associated with circulatory overload. Since the
original description of blood-born hepatitis A,
numerous infections including AIDS have
been transmitted to patients during blood
transfusions. For these reasons, attempting to
August 2003
Approach to the Management of Anemia in Long-Term Care Residents
DIAGNOSIS TREATMENTIron deficiency Ferrous sulfate 325 mg 1-3 times dailyVitamin B12 deficiency Vitamin B12 1000 μg orally or
intramuscularlyAnemia of chronic kidney disease Epoetin alfa 10,000 U weekly or
darbepoetin alfa 60 mcg every two weeksAnemia of chronic disease Treat underlying condition; consider epoetin
alfa weekly or darbepoetin alfa every two weeks
TABLE III

17
Diagnosis and Management of Anemia in Long-Term Care
maintain hemoglobin concentration by other
approaches is very important in the long-term
care resident. Human recombinant erythropoi-
etin administration can reduce blood transfu-
sion requirements.30
ErythropoietinSince the introduction of human recombinant
erythropoietin (epoetin alfa) in 1989 to treat
anemia in chronic kidney disease patients
(patients on dialysis and patients not yet on
dialysis), the treatment of anemia has been rev-
olutionized. In patients with chronic kidney
disease, the workup for anemia should begin in
an adult female with a hemoglobin concentra-
tion of 11 g/dL or less, and in an adult male
with a hemoglobin concentration of 12 g/dL
or less. Anemia can develop relatively early in
the course of chronic renal failure, and has
been associated with a serum creatinine as low
as 2.0 mg/dL.31 A linear relationship between
glomerular filtration rate and anemia has been
demonstrated. Significant anemia was noted
when the calculated glomerular filtration rate
was less than 20-35 mL/min.32,33 In patients
with impaired renal function and a nor-
mochromic, normocytic anemia, it is rare for
the serum erythropoietin level to be elevated.
Therefore, measurement of erythropoietin lev-
els in such patients is not likely to guide clini-
cal decision-making or therapy.
While the majority of persons on dialysis
receive erythropoietin, there are many persons
who have chronic kidney disease who do not
receive erythropoietin. This is particularly true
in the long-term care setting.
Erythropoietin has been shown to increase
hemoglobin concentration in patients with
anemia associated with surgical blood loss, can-
cer chemotherapy, anemia associated with drug
therapy for AIDS or hepatitis C virus,
myelodysplastic disease, and the anemia of
chronic disease, especially when associated
with rheumatoid arthritis (See Table IV for
Food & Drug Administration-approved indi-
cations for use of erythropoietin). Many condi-
tions involve additional causes for an inade-
quate response to erythropoietin therapy and
should be corrected when possible in order to
reverse the anemia (Table V34).
August 2003
Food & Drug Administration-Approved Indications for Use of Erythropoietin
• Anemia of chronic renal disease (chronic renal insufficiency and end-stage renal disease)
• Chemotherapy-induced anemia in patients with non-myeloid malignancies• Zidovudine-related anemia in HIV-infected patients• Reduction of allogeneic blood transfusion in surgery patients
TABLE IV

18
Diagnosis and Management of Anemia in Long-Term Care
Erythropoietin therapy increases hemoglo-
bin concentration, improves quality of life, and
may improve long-term health outcome and
even survival.20,21 Erythropoietin causes a
decrease in the left ventricular hypertrophy
associated with anemia.16 As may be expected
with increased blood volume, erythropoietin
therapy increases blood pressure, necessitating
close monitoring in patients with known car-
diovascular disease.
Recently, a novel erythropoietin, or erythro-
poiesis-stimulating protein, darbepoetin alfa,
has become available. Darbepoetin alfa is indi-
cated for the treatment of anemia associated
with chronic renal failure, including patients
on dialysis and those not yet on dialysis, and
for chemotherapy-induced anemia in patients
with non-myeloid malignancies. Darbepoetin
alfa is compared to epoetin alfa in Table
VI.35,36 Because of its longer half-life, darbe-
poetin alfa appears to
have great potential in the
long-term care setting.
The approximate
threefold longer half-life
with darbepoetin alfa
compared to epoetin alfa
has allowed for less fre-
quent administration.
Epoetin alfa is given 1-3
times a week or once
weekly. A study has evalu-
ated the efficacy of darbe-
poetin alfa dosed every 2
weeks in anemic patients
with chronic renal insuffi-
ciency. Darbepoetin alfa
has been demonstrated to
maintain hemoglobin
concentrations between
the study target hemoglo-
bin of 11-13 g/dL while
being administered every 2 weeks. When
administered every 2 weeks, darbepoetin alfa
produces a hemoglobin response at a median
time of 5-6 weeks with a range of 1-25 weeks.
The median darbepoetin alfa dose at the time
of hemoglobin response was 60 mcg every 2
weeks. Ninety-five percent of those completing
the study reached the target hemoglobin con-
centration. Side effects seen with darbepoetin
alfa were similar to those seen with epoetin
August 2003
Potential Causes for Inadequate Response to Erythropoietin Therapy
• Iron/B12/folate deficiency• Infection/inflammation (eg, access infections,
surgical inflammation, AIDS, systemic lupus erythematosus)
• Chronic blood loss• Osteitis fibrosa• Hemoglobinopathies (eg, alpha and beta
thalassemias, sickle cell anemia)• Multiple myeloma• Malnutrition• Hemolysis• Aluminum toxicity• Malignancy• Hyperparathyroidism• Hypogonadism• Other: angiotensin-converting enzyme inhibitors
(reported, but not verified)
TABLE V34

19
Diagnosis and Management of Anemia in Long-Term Care
alfa.37 Further studies are evaluating extending
the dosing interval to once a month. Initial
dosing of epoetin alfa and darbepoetin alfa
should follow package insert guidelines.
Thereafter, dose adjustments should be made
as needed based on an individual’s hemoglobin
response.
Recommendations of theCouncil for Anemia ClinicalStrategies in Long-TermCareThe Council for Anemia Clinical Strategies in
Long-Term Care developed recommendations
for the treatment of anemia in long-term care.
The Council recommends that a hemoglobin
concentration of less than 12 g/dL should be
evaluated and treated when appropriate.
The Council recognized that there were lim-
ited data on erythropoietin use in long-term
care. Nevertheless, there are positive clinical
outcomes for treating anemia of chronic kid-
ney disease such as improved quality of life and
decreased hospitalization and mortality.
Chronic kidney disease and its associated ane-
mia are often underdiagnosed in the elderly.
The Council recommends increasing aware-
ness of chronic kidney disease in the elderly by
using conventional formulas to calculate the
creatinine clearance. Furthermore, the Council
recommends consideration of treating the ane-
mia of chronic kidney disease in the long-term
care setting. Pending future clinical studies of
treating other types of anemia of chronic dis-
ease in the elderly, current clinical research on
treating anemia of chronic kidney disease
should focus on measuring important out-
comes in the long-term care patient, such as
improved quality of life (physical and mental)
and decreased hospitalization (secondary to
decreased falls and fractures), and cardiovascu-
lar morbidity.
Erythropoietin should clearly be considered
in all anemic residents with chronic kidney dis-
ease whose serum creatinine is greater than 2
mg/dL. A calculated creatinine clearance
should be done to identify residents with
chronic renal failure whose creatinine is less
than 2 mg/dL. In patients with impaired renal
function and a normochromic, normocytic
August 2003
Comparison of Epoetin Alfa and Darbepoetin Alfa
EPOETIN ALFA DARBEPOETIN ALFA
Sialic acid35 ~14 ~22Half-life (hours), intravenously35 ~8.5 ~26.3Biological activity36 Less GreaterDosing36 Frequent Less often
TABLE VI

20
Diagnosis and Management of Anemia in Long-Term Care
anemia, measurement of erythropoietin levels
is not likely to guide clinical decision-making
or therapy.
The Council suggests that the long half-life
of darbepoetin alfa may make it very useful in
long-term care where a once- or twice-a-month
dosing regimen could be utilized. When used,
the dosing regimen of erythropoietin should
lead to an increase of hemoglobin concentra-
tion by no more than 1 g/dL in a 2-week peri-
od, and target hemoglobin concentration
should not exceed 12 g/dL. Transferrin satura-
tion and ferritin concentration should be mon-
itored and iron replaced, either orally or intra-
venously, if iron deficiency develops. In addi-
tion, the Council strongly supports the devel-
opment of increased research in this area.
References1. Tran KH, Udden MM, Taffer GE, et al.
Erythropoietin regulation of hematopoiesis is preserved in healthy elderly people. Clin Res1993;41:116A.
2. Zauber NP, Zauber AG. Hematologic data ofhealthy very old people. JAMA 1987;257:2181-2184.
3. Chaves PH, Ashar B, Guralnik JM, Fried LP. Lookingat the relationship between hemoglobin concentra-tion and prevalent mobility difficulty in olderwomen. Should the criteria used to define anemiain older people be reevaluated? J Am Geriatr Soc2002;50:1257-1264.
4. Weber JP, Walsh PC, Peters CA, Spivak JL. Effect ofreversible androgen deprivation on hemogblobinand serum immunoreactive erythropoietin in men.Am J Hematol 1991;36:190-194.
5. Ellegala DB, Alden TD, Couture DE, et al. Anemia,testosterone, and pituitary adenoma in men. JNeurosurg 2003;98:974-977.
6. Bogdanos J, Karamanolakis D, Milathianakis C, etal. Combined androgen blockade-induced anemiain prostate cancer patients without bone involve-ment. Anticancer Res 2003;23:1757-1762.
7. Ania BJ, Suman VJ, Fairbanks VF, et al. Incidenceof anemia in older people: An epidemiologic studyin a well defined population. J Am Geriatr Soc1997;45:825-831.
8. Salive ME, Cornoni-Huntley J, Guralnik JM, et al.Anemia and hemoglobin levels in older persons:Relationship with age, gender, and health status. JAm Geriatr Soc 1992;40:489-496.
9. Joosten E, Pelemans W, Hiele M, et al. Prevalenceand causes of anaemia in a geriatric hospitalizedpopulation. Gerontology 1992;38:111-117.
10. Chernetsky A, Sofer O, Rafael C, Ben-Israel J.Prevalence and etiology of anemia in an institution-alized geriatric population [Hebrew]. Harefuah2002;1412:591-594.
11. Ania Lafuente BJ, Fernandez-Burriel Tercero M,Suarez Almenara JL, et al. Anemia and functionalincapacity at admission to a geriatric home[Spanish]. An Med Interna 2001;18:9-12.
12. Hsu CY, McCulloch CE, Curhan GC. Epidemiologyof anemia associated with chronic renal insufficien-cy among adults in the United States: Results fromthe Third National Health and NutritionExamination Survey. J Am Soc Nephrol2002;13:504-510.
13. Izaks GJ, Westendorp RGJ, Knook DL. The defini-tion of anemia in older persons. JAMA1999;281:1714-1717.
14. Kamenetz Y, Beloosesky Y, Zelter C, et al.Relationship between routine hematological para-meters, serum IL-3, IL-6 and erythropoietin and mildanemia and degree of function in the elderly. AgingClin Exp Res 1998;10:32-38.
15. Wu WC, Rathore SS, Wang Y, et al. Blood transfu-sion in elderly patients with acute myocardialinfarction. N Engl J Med 2001;345:1230-1236.
16. Levin A, Singer J, Thompson CR, et al. Prevalent leftventricular hypertrophy in the predialysis popula-tion: Identifying opportunities for intervention. Am JKidney Dis 1996;27:347-354.
17. The prevention of falls in later life: A report of theKellogg International Work Group on the Preventionof Falls by the Elderly. Dan Med Bull1987;34(suppl 4):1-24.
18. Baker SP, Harvey AH. Fall injuries in the elderly.Clin Geriatr Med 1985;1:501-512.
19. Herndon JG, Helmick CG, Sattin RW, et al. Chronicmedical conditions and risk of fall injury events athome in older adults. J Am Geriatr Soc1997;45(6):739-743.
20. Valderrabano F. Quality of life benefits of early ane-mia treatment. Nephrology Dialysis Transplantation2000:15(suppl):23-28.
21. Cella D. Factors influencing quality of life in cancerpatients: Anemia and fatigue. Semin Oncol1998;25(3 suppl 7):43-46.
22. Malope BI, MacPhail AP, Alberts M, Hiss DC. Theratio of serum transferrin receptor and serum ferritinin the diagnosis of iron status. Br J Haematol2001;115(1):84-89.
August 2003

21
Diagnosis and Management of Anemia in Long-Term Care
23. Wians FH Jr, Urban JE, Keffer JH, Kroft SH.Discriminating between iron deficiency anemia andanemia of chronic disease using traditional indices ofiron status vs transferrin receptor concentration. Am JClin Pathol 2001;115(1):112-118.
24. Cockcroft DW, Gault MN. Prediction of creatinineclearance from serum creatinine. Nephroj1976;349:163:31-41.
25. Robertshaw M, Lai KN, Swaminathan R. Prediction ofcreatinine clearance from plasma creatinine:Comparison of five formulae. Br J Clin Pharmacol1989;28:275-80.
26. Waller DG, Fleming JS, Ramsey B, Gray J. The accu-racy of creatinine clearance with and without urinecollection as a measure of glomerular filtration rate.Postgrad Med J 1991;67:42-46.
27. Provan D. Mechanisms and management of iron defi-ciency anaemia. Br J Haematol 1999;105(suppl1):19-26.
28. Goddard AF, McIntyre AS, Scott BB. Guidelines forthe management of iron deficiency anaemia. BritishSociety of Gastroenterology. Gut 2000;46(suppl 3-4):IV1-IV5.
29. Frewin R, Henson A, Provan D. ABC of clinicalhaematology. Iron deficiency anaemia. BMJ1997;314(7077):360-363.
30. Corwin HL, Gettinger A, Pearl RG, et al. Efficacy ofrecombinant human erythropoietin in critically illpatients: A randomized controlled trial. JAMA2002;288(22);2827-2835.
31. Hakim RM, Lazarus JM. Biochemical parameters inchronic renal failure. Am J Kidney Dis 1988;11:238-247.
32. Jacobs A, Worwood M. Ferritin in serum. Clinicaland biochemical implications. N Engl J Med1975;292:951-956.
33. McGonigle RJS, Boineau FG, Beckman B, et al.Erythropoietin and inhibitors of in vitro erythropoiesisin the development of anemia in children with renaldisease. J Lab Clin Med 1985;105:449-458.
34. Steinberg EP, Eknoyan G, Levin NW, et al. Methodsused to evaluate the quality of evidence underlyingthe National Kidney Foundation-Dialysis OutcomesQuality Initiative Clinical Practice Guidelines:Description, findings, and implications. Am J KidneyDis 2000;36:1-11.
35. Egrie JC, Browne JK. Development and characteriza-tion of novel erythropoiesis stimulating protein(NESP). Br J Cancer 2001;84(suppl 1):3-10.
36. Macdougall IC, Gray SJ, Elston O, et al.Pharmacokinetics of novel erythropoiesis stimulatingprotein compared with epoetin alfa in dialysispatients. J Am Soc Nephrol 1999;10(11):2392-2395.
37. Suranyi MG, Lindberg JS, Navarro J, et al. Treatmentof anemia with darbepoetin alfa administered denovo once every other week in chronic kidney dis-ease. Am J Nephrol 2003;23:106-111.
August 2003

August 2003
22
Diagnosis and Management of Anemia in Long-Term Care
CME/CE TEST QUESTIONNAIRE
Please provide the following information (please print) in order toreceive your CME/CE certificate:Name ______________________________________________________Degree __________________________
Institution or Affiliation __________________________________________________________________________
Address ______________________________________________________________________________________
City, State, Zip ________________________________________________________________________________
Telephone __________________________________________Fax ____________________________________
To receive credit, participants must complete the form above and fax or mail it to: Medical Education Resources
1500 West Canal CourtLittleton, CO 80120Fax: 303-798-5731
1. A hemoglobin concentration of less than13 g/dL in men and less than 12 g/dL inwomen defines anemia, according toWorld Health Organization standards.
❏ True
❏ False
2. Anemia of chronic disease is the most com-mon cause of anemia in older persons.
❏ True
❏ False
3. Chronic kidney disease accounts for the great-est percentage of anemic individuals with thediagnosis of anemia of chronic disease.
❏ True
❏ False
4. Anemia can be due to a) failure of the bone marrow to manu-
facture adequate blood components b) rapid loss of formed blood from
hemorrhagec) rapid breakdown of blood components
from hemolysis d) all of the above.
5. Amemia in the elderly is not associatedwith increased mortality or quality of life.
❏ True
❏ False
Using a scale from 1 to 5, with 5=excellent, 4=very good, 3=adequate, 2=fair, 1=poor,please circle the number corresponding to your rating of the following:
Excellent Poor
1. Overall quality of the material 5 4 3 2 1
2. Clinical applicability or relevance of thematerial to participant’s practice 5 4 3 2 1
3. Extent to which the material met stated objectives 5 4 3 2 1
4. Extent to which participant will modify his/her practice as a result of participation in the program 5 4 3 2 1
5. Fair balance and objectivity of the material 5 4 3 2 1
6. Completion time 5 4 3 2 1
Please answer the following questions:

23
Diagnosis and Management of Anemia in Long-Term Care
August 2003
This special report was sponsored by Medical Education Resources, Inc,
and produced by MultiMedia HealthCare/Freedom, LLC, under an
unrestricted educational grant from Amgen, Inc.
The views expressed in this publication are not necessarily
those of Amgen, Inc. or the publishers.
This publication may not be reproduced in whole or in part
without the express written permission of
MultiMedia HealthCare/Freedom, LLC.
Copyright © 2003 MultiMedia HealthCare/Freedom, LLC.
All rights reserved. Office Center at Princeton Meadows, Building 400,
Plainsboro, NJ 08536. Telephone: (609) 275-3800.
Printed in USA.
AMG-03543

If you would like to be added to the mail list to receive future Council publications and materials, please complete the following information:
Full Name Degree(s)Title/PositionPractice Name Full AddressCity State ZipPhone Fax E-mail
Thank you for your responses. They are very important to us.
1. Please indicate your area of specialty:❏ Medical Director❏ Attending Physician❏ Consultant Pharmacist❏ Director of Nursing❏ Other; please specify___________________
2. Overall, how many patients are youresponsible for in each of the followingsettings? If none, please put “0.”Skilled nursing facility Assisted living Home health care Private practice
We’d now like to focus on your skilled nursing patients only.3. How many skilled nursing facilities do
you serve?❏ 1-2 ❏ 3-5 ❏ > 5
4. Is your facility(ies) a member of a chain?❏ Yes ❏ NoIf yes, please specify name of chain:____________________________________
5. What is the average number of skilledcare beds in your facilities?❏ < 100 ❏ 100 – 150 ❏ 151 – 200 ❏ > 200
6. On average, how frequently do you seeeach of your skilled care patients?❏ Daily❏ Once a week❏ At least once a month❏ Once every 2-3 months
7. On average, what percentage of yourskilled care patients are anemic (Hgb <12 g/dL)? __________%
8. What are the top three diseases or con-ditions associated with anemia in yourskilled care patients? Please rank inorder 1 to 3, with 1 being the mostcommon of the 3.____ End-Stage Renal Disease (ESRD)____ Repeated Blood Draws____ Chronic Kidney Disease (CKD)____ Poor Diet/Nutrition____ Cancer (CIA/AOC)____ Iron Deficiency____ Acute Illness____ Myelodysplasia____ GI Bleeding____ Vitamin B12 Deficiency____ Surgery____ Blood Loss (from dialysis procedure
and/or vascular access site)____ Other; please specify:_____________________________________
9. Which of the following assessments doyou use to detect anemia in your skilledcare patients?❏ Circulating Soluble Transferrin
Receptor❏ Creatinine Clearance❏ Erythropoietin Level❏ Folate
❏ Hematocrit❏ Hemoglobin Concentration❏ Serum Methylmalonic Acid Level❏ Serum Vitamin B12 Level❏ Iron (T-Sat Ferritin Level)❏ Other; please specify_______________
10. How frequently is an anemia assessmenttypically performed on your skilled carepatients?❏ Once every 2 weeks❏ Once a month❏ Once every 3 to 6 months❏ If less frequent, please specify_____________________________________
11. Who typically first becomes aware thatyour skilled care patients have anemia?❏ Attending Physician❏ Consultant Pharmacist❏ Director of Nursing❏ Consultant Dietitian❏ Other; please specify_______________
12. At what point are your skilled carepatients first treated for anemia? ❏ At a hemoglobin concentration
of <12 g/dL❏ At a hemoglobin concentration
of <10 g/dL ❏ Only when the patient is
symptomatic❏ Other; please specify________________
13. In your anemic skilled care patients witha hemoglobin of less than 12 g/dL butgreater than 10 g/dL, what is your first-line treatment?❏ Drug Therapy❏ Ferrous Sulfate❏ Vitamin B12❏ Other; please specify__________________
14. In your anemic skilled care patients witha hemoglobin of less than 10 g/dL, whatis your first-line treatment?❏ Drug Therapy❏ Ferrous Sulfate❏ Vitamin B12❏ Other; please specify__________________
15. In your anemic patients with a hemoglo-bin of less than 12 g/dL, what percent-age is treated at any point with drug therapy? __________%
16. Of the following drugs, please checkthose with which you are familiar:❏ darbepoetin alfa (Aranesp)❏ erythropoietin alfa (Epogen, Procrit)❏ Other; please specify_________________
17. In your skilled care anemic patients thatare currently being treated with drugtherapy, please indicate the percentagethat are being treated with the follow-ing therapies. Total must equal 100%.❏ darbepoetin alfa (Aranesp)______%
❏ erythropoietin alfa
(Epogen, Procrit) _______%
❏ Other, please specify _______%
18. Considering the most common diseaseor condition associated with anemiathat you ranked as #1 in Question 8,please indicate your most frequent dosing regimen for each of the following therapies:
❏ darbepoetin alfa (Aranesp)______ mcg ______ interval ❏ N/A; don’t prescribe
erythropoietin alfa (Epogen,Procrit)______ units ______ interval ❏ N/A; don’t prescribe
❏ Other, please specify________ interval_________________________
19. Please rank in order of importance theimpact of the following factors in yourdrug selection using a scale of 1 to 7,where “1” means most important and“7” means least important:____ Product efficacy____ Product cost____ Ease of use and patient compliance____ Dosing frequency____ Prior experience with product____ Patient/family request____ Product is on formulary or part of
formal protocol____ Other; please specify_____________
20. Please rate the degree of influence thateach of the following parties has on yoursupportive care prescribing decisionsusing a scale of 1 to 5, where “1” meansnot at all influential and “5” meansextremely influential (circle rating).
Not at all ExtremelyInfluential Influential
Skilled nursing home formulary1 2 3 4 5
Skilled care director of nursing1 2 3 4 5
Consultant pharmacist1 2 3 4 5
Consultant dietitian 1 2 3 4 5
Patient/family1 2 3 4 5
Other; please specify _________________1 2 3 4 5
21. What type of educational programsfocusing on anemia would you like tosee?____________________________________________________________________
FAX-BACK SURVEYPlease Fax to 1-888-427-4997 (toll free)
The Council for Anemia is working to sponsor educational programming that meets the unique needs of elder care clinicians.In order to provide you with the most valuable and relevant educational programming, we would like to learn more about
your elderly patient population and your practice. Please take a few minutes to answer the following questions:
August 2003