a first-in-human study and biomarker ... - cancer discovery · like symptoms (68%), pruritus (64%),...
TRANSCRIPT
JUNE 2019�CANCER DISCOVERY | 711
RESEARCH BRIEF
A First-in-Human Study and Biomarker Analysis of NKTR-214, a Novel IL2Raf-Biased Cytokine, in Patients with Advanced or Metastatic Solid Tumors Salah-Eddine Bentebibel 1 , Michael E. Hurwitz 2 , Chantale Bernatchez 1 , Cara Haymaker 1 , Courtney W. Hudgens 1 , Harriet M. Kluger 2 , Michael T. Tetzlaff 1 , Mary A. Tagliaferri 3 , Jonathan Zalevsky 3 , Ute Hoch 3 , Christie Fanton 3 , Sandra Aung 3 , Patrick Hwu 1 , Brendan D. Curti 4 , Nizar M. Tannir 1 , Mario Sznol 2 , and Adi Diab 1
1 The University of Texas MD Anderson Cancer Center, Houston, Texas. 2 Yale School of Medicine, New Haven, Connecticut. 3 Nektar Therapeutics, San Francisco, California. 4 Providence Cancer Institute and Earle A. Chiles Research Institute, Portland, Oregon. Note: Supplementary data for this article are available at Cancer Discovery Online (http://cancerdiscovery.aacrjournals.org/). S.-E. Bentebibel, M.E. Hurwitz, and C. Bernatchez contributed equally to this article.
ABSTRACT NKTR-214 (bempegaldesleukin) is a novel IL2 pathway agonist, designed to provide sustained signaling through heterodimeric IL2 receptor βγ to drive increased pro-
liferation and activation of CD8 + T and natural killer cells without unwanted expansion of T regulatory cells (Treg) in the tumor microenvironment. In this fi rst-in-human multicenter phase I study, NKTR-214 administered as an outpatient regimen was well tolerated and showed clinical activity including tumor shrinkage and durable disease stabilization in heavily pretreated patients. Immune activation and increased numbers of immune cells were observed in the periphery across all doses and cycles with no loss of NKTR-214 activity with repeated administration. On-treatment tumor biopsies demon-strated that NKTR-214 promoted immune cell increase with limited increase of Tregs. Transcriptional analysis of tumor biopsies showed that NKTR-214 engaged the IL2 receptor pathway and signifi cantly increased genes associated with an effector phenotype. Based on safety and pharmacodynamic mark-ers, the recommended phase II dose was determined to be 0.006 mg/kg every three weeks.
SIGNIFICANCE: We believe that IL2- and IL2 pathway–targeted agents such as NKTR-214 are key com-ponents to an optimal immunotherapy treatment algorithm. Based on its biological activity and tolerabil-ity, NKTR-214 is being studied with approved immuno-oncology agents including checkpoint inhibitors.
See related commentary by Sullivan, p. 694.
Corresponding Author: Adi Diab, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030. Phone: 713-745-7336; Fax: 713-745-1046; E-mail: [email protected] doi: 10.1158/2159-8290.CD-18-1495 Cancer Discov 2019;9:711–21
© 2019 American Association for Cancer Research.
INTRODUCTION
In the treatment of patients with cancer, low levels of tumor-infi ltrating lymphocytes (TIL) prior to the introduc-tion of checkpoint inhibitors is predictive of a poor response ( 1–3 ). Stimulation of the IL2 receptor (IL2R) pathway is a
potent means of expanding and activating immune cells, specifi cally lymphocytes including cytotoxic CD8 + T cells ( 4 ). FDA-approved high-dose (HD) IL2 (aldesleukin) treat-ment mediates durable clinical benefi t in a limited number of patients with melanoma and renal cell carcinoma (RCC), presumably through CD8 + T-cell expansion ( 5 ). However, the
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

Bentebibel et al.RESEARCH BRIEF
712 | CANCER DISCOVERY JUNE 2019 www.aacrjournals.org
frequent and rapid induction of the IL2 cytokine signaling cascade is associated with an increased risk for serious adverse events (SAE; refs. 6–10). The ability of IL2 to broadly expand many lymphocyte cell populations is a critical feature of its mechanism of action as an immunotherapy and a nonredun-dant role of IL2 biology.
NKTR-214 (bempegaldesleukin) is a human recombinant IL2 attached to an average of six releasable polyethylene glycol (PEG) chains (11, 12). In the 1980s, PEG-modified IL2 (PEG-IL2) was developed in an effort to improve the solubility and decrease the plasma clearance of IL2 (13). Results of a phase I study describing the use of PEG-IL2 in combination with HD IL2 to treat patients with metastatic RCC and melanoma were reported in 1995 (14). Results from the phase I study concluded that the toxicities and tumor response rates to combination treatment with HD IL2 followed by administration of PEG-IL2 were similar to those of HD unconjugated IL2 alone. Further development of PEG-IL2 was discontinued. In the case of NKTR-214, attachment of PEG chains can also be creatively utilized to not only alter a molecule’s pharmacokinetics but also alter its receptor binding. NKTR-214 is engineered to bias recep-tor selectivity and alter pharmacokinetics of IL2 (11, 12), while leaving the well-understood amino acid sequence of IL2 (aldesleukin) unaltered. When fully PEGylated, NKTR-214 is a prodrug that has essentially no biological activity. Upon i.v. administration, the PEG chains slowly release to generate active cytokine species with limited binding to the IL2Rα subunit, thereby biasing signaling to favor the dimeric IL2Rβγ (CD122). Consequently, NKTR-214 increases the proliferation, activation, and effector func-tion of CD8+ T cells and natural killer (NK) cells within the tumor microenvironment (TME) without expanding the undesirable intratumoral T regulatory cells (Treg; ref. 11). In murine tumor models, NKTR-214 generated a ratio of CD8+ cytotoxic T cells to Tregs of >400:1 in tumor, and when combined with an anti-CTLA4 checkpoint inhibitor antibody, there was a strong synergistic effect (11). Based on supportive preclinical efficacy, immunobiology data, and pharmacology and toxicology studies performed in rats and monkeys, a first-in-human study was initiated using NKTR-214 in patients with advanced solid tumors. We report here on the safety, pharmacodynamics, and immunologic and antitumor activity of NKTR-214 mono-therapy in patients treated with multiple prior lines of therapy.
RESULTSPatient Characteristics and Disposition
Twenty-eight patients with advanced or locally advanced solid tumor malignancies were enrolled across three cent-ers from December 2015 to April 2017. Demographics and disease characteristics are summarized in Supplementary Table S1. The majority of patients had a diagnosis of meta-static RCC (n = 15; 53.6%) or melanoma (n = 7; 25.0%). All patients had received prior anticancer treatment: 16 (57.1%) had received targeted therapy; 16 (57.1%) had received an immune checkpoint inhibitor; and 6 (21.4%) had received an immune checkpoint inhibitor in addition to other immuno-
therapy. The median number of prior therapies was 2 (range, 1–12; Supplementary Fig. S1A). The most common reason for study drug discontinuation was progressive disease by RECIST (n = 15; 53.6%) or physician decision (n = 6; 21.4%), primarily for patients who did not respond rapidly and had other therapeutic options. One patient discontinued treat-ment due to an infusion-related reaction. Patients received a median of 3 infusions of NKTR-214 (range, 1–25 infusions), with a median duration of exposure of 69.5 days (range, 15–533 days).
Safety and TolerabilityAll 28 patients enrolled in the study had treatment-emergent
adverse events (TEAE), with 26 patients having TEAEs that were considered related to the study drug. TEAEs and treat-ment-related adverse events (TRAE) occurring in ≥3 patients across all doses are listed in Table 1 and in Supplementary Table S2, respectively. Six of 28 (21.4%) patients reported grade 3 TRAEs; there were no grade 4 or 5 TRAEs. At the highest NKTR-214 dose tested (0.012 mg/kg), 1 patient expe-rienced two dose-limiting toxicities (DLT; grade 3 hypoten-sion and grade 3 syncope), which resolved within 24 hours following i.v. fluid treatment and one dose of tocilizumab. This patient was discharged from the hospital 2 days after admission for the events and continued on study, receiving two additional doses of NKTR-214 0.006 mg/kg that were well tolerated. No other patients were dosed at 0.012 mg/kg. At a NKTR-214 dose of 0.009 mg/kg, 1 patient discontinued the study due to an SAE of grade 3 infusion-related reaction. The reaction occurred following the first dose of NKTR-214 and resolved with treatment. This patient had a history of an infusion-related reaction to a previous immuno-oncology agent. There was one reported immune-related adverse event (irAE) of hypothyroidism associated with NKTR-214, which was treated with replacement therapy. The MTD was defined as the highest dose of NKTR-214 that was administered with-out causing any unacceptable side effects or AEs. DLTs and AEs were considered in the determination of the MTD, which was deemed to be 0.009 mg/kg every three weeks (q3w).
The most common TRAEs included fatigue (71%), flu-like symptoms (68%), pruritus (64%), hypotension (57%), rash (50%), decreased appetite (46%), and arthralgia and cough (each 32%). Flu-like symptoms were managed with acetaminophen and NSAIDs. The median duration of flu-like symptoms, including fever, was 72 hours and became less pronounced after cycle 2. Rash and pruritus were either self-limited or treated with antihistamines. Hypotension usually occurred around 48 to 72 hours following the first NKTR-214 infusion. Declines in blood pressure follow-ing administration of NKTR-214 were generally clinically asymptomatic.
All grade 3 TEAEs of hypotension [5 of 28 (18%) patients] were rapidly reversed with i.v. fluid administration, and no patients discontinued treatment due to hypotension. Risk minimization guidelines, which included oral and i.v. fluids during the first week of dosing, were implemented and success-fully reduced the incidence of grade 3 hypotension. The fre-quency of drug administration, every two weeks (q2w) or q3w at a NKTR-214 dose of 0.006 mg/kg, did not appear to affect the safety profile. Based on safety and pharmacodynamic
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

NKTR-214 in Patients with Advanced Solid Tumors RESEARCH BRIEF
JUNE 2019 CANCER DISCOVERY | 713
(continued)
Table 1. TEAEs occurring in 3 or more patients across all doses
Preferred term a
Grades 1–2 Grades 3–5
Total (%)
0.003 mg/kg(q3w)( n = 4)
0.006 mg/kg(q3w)
( n = 11)
0.006 mg/kg(q2w)( n = 6)
0.009 mg/kg(q3w)( n = 6)
0.012 mg/kg(q3w)( n = 1)
0.003 mg/kg(q3w)( n = 4)
0.006 mg/kg(q3w)
( n = 11)
0.006 mg/kg(q2w)( n = 6)
0.009 mg/kg(q3w)( n = 6)
0.012 mg/kg(q3w)( n = 1)
15/28 (54%) patients reported grade ≥ 3 TEAE
Hypotension 2 (50) 8 (73) 2 (33) 1 (17) 1 (9) 2 (33) 1 (17) 1 (100) 18 (64)
Syncope 1 (9) 1 (17) 1 (100) 3 (11)
Headache 3 (75) 2 (18) 1 (17) 2 (33) 1 (9) 1 (17) 10 (36)
Anemia 2 (50) 1 (9) 1 (17) 1 (9) 1 (17) 6 (21)
Metastases to central nervous system 2 (18) 1 (17) 3 (11)
Constipation 2 (50) 3 (27) 2 (33) 1 (17) 1 (25) 9 (32)
Edema peripheral 4 (36) 1 (17) 1 (17) 1 (17) 7 (25)
Abdominal pain 1 (25) 1 (9) 1 (17) 2 (33) 5 (18)
Pleural effusion 1 (25) 2 (18) 1 (17) 1 (25) 5 (18)
Confusional state 2 (33) 1 (9) 3 (11)
Infusion related reaction 1 (9) 1 (17) 2 (7)
Presyncope 1 (9) 1 (9) 2 (7)
Brain edema 1 (9) 1 (4)
Disease progression 1 (17) 1 (4)
Gastroduodenal hemorrhage 1 (9) 1 (4)
Hemiparesis 1 (9) 1 (4)
Hypovolemic shock 1 (17) 1 (4)
Lipase increased 1 (25) 1 (4)
Liver function test abnormal 1 (17) 1 (4)
Lower gastrointestinal hemorrhage 1 (17) 1 (4)
Metastases to meninges 1 (9) 1 (4)
Sepsis 1 (17) 1 (4)
Fatigue 3 (75) 9 (82) 5 (83) 5 (83) 1 (100) 23 (82)
Flu-like symptoms b 3 (75) 8 (73) 4 (67) 5 (83) 20 (71)
Pruritus 2 (50) 7 (64) 5 (83) 4 (67) 1 (100) 19 (68)
Decreased appetite 1 (25) 6 (55) 4 (67) 4 (67) 15 (54)
Rash c 3 (75) 6 (55) 4 (67) 2 (33) 15 (54)
Arthralgia 1 (25) 3 (27) 5 (83) 2 (33) 1 (100) 12 (43)
Cough 1 (25) 5 (45) 2 (33) 3 (50) 1 (100) 12 (43)
Nausea 3 (75) 3 (27) 3 (50) 2 (33) 11 (39)
Diarrhea 3 (75) 2 (18) 1 (17) 3 (50) 9 (32)
Dyspnea 3 (75) 4 (36) 1 (17) 8 (29)
Nasal congestion 1 (25) 2 (18) 2 (33) 3 (50) 8 (29)
Dizziness 2 (50) 3 (27) 1 (17) 1 (17) 7 (25)
Myalgia 3 (27) 1 (17) 2 (33) 6 (21)
Vomiting 1 (25) 2 (18) 2 (33) 1 (17) 6 (21)
Weight decreased 2 (50) 1 (9) 2 (33) 5 (18)
Flushing 1 (9) 2 (33) 1 (17) 4 (14)
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

Bentebibel et al.RESEARCH BRIEF
714 | CANCER DISCOVERY JUNE 2019 www.aacrjournals.org
markers, the recommended phase II dose (RP2D) was deter-mined to be 0.006 mg/kg q3w.
Pharmacokinetics and Pharmacodynamics NKTR-214–related cytokine (NKTR-214-RC) represents
a mixture of compounds containing IL2 independent of the PEG-conjugation status, and NKTR-214–active cytokine (NKTR-214-AC) represents a mixture of 2-PEG-IL2 and 1-PEG-IL2, and potentially unconjugated IL2, although this species is often undetectable in patient samples; the mean observed plasma concentration–time profi les are shown in Supplementary Fig. S2A. NKTR-214-RC maximal concentra-tions were achieved shortly after the end of the infusion and declined monoexponentially thereafter. NKTR-214-RC con-centrations remained detectable for 8 to 11 days post-dose. NKTR-214-AC concentrations increased gradually after dos-ing with T max between 24 and 48 hours. NKTR-214-RC and NKTR-214-AC exposures were similar across patients within a dose cohort and cycles, without indication of accumula-tion with either the q3w or q2w administration schedules (data not shown). Unconjugated IL2 levels were detected in 76 of 425 samples with reportable results. Unconjugated IL2 concentrations in samples with detectable levels ranged between 0.509 and 4.44 ng/mL with one concentration at 19.4 ng/mL. Out of 425 samples analyzed, 378 samples (89%) had concentrations of unconjugated IL2 that were below the limit of quantitation or less than 1 ng/mL (the lower limit of quantitation was 0.5 ng/mL; data not shown). Soluble CD25 (sCD25) and lymphocyte levels were measured as pharmacodynamic indicators of immune system activation (Supplementary Fig. S2B and S2C). Changes in absolute lym-phocyte counts were observed with each q3w treatment cycle and included lymphopenia on day 3 followed by lymphocy-
tosis, which peaked between days 8 and 11, and returned to near-baseline levels prior to the next cycle. Similarly, sCD25 levels increased within each treatment cycle, peaked around day 8, and returned to near-baseline levels prior to each q3w cycle. PD kinetics were observed at all dose levels and at the q2w dosing schedule (data not shown). Anti–NKTR-214 or anti-IL2 antidrug antibodies were not present in any samples tested for this study (data not shown).
Antitumor Activity Twenty-eight patients were enrolled in the study, and 26
were evaluable for effi cacy. Treatment exposure is shown in Supplementary Fig. S1B. Although no objective responses were observed using RECIST criteria, 9 of 26 patients (35%) experienced maximum tumor reductions ranging from 2% to 30%. One patient with RCC had a 40% reduction on the right adrenal gland at the fi rst on-treatment scan [the overall response was stable disease (SD)] and experienced a 30% reduction of the sum of 2 target lesions at the second post-treatment scan; a CT scan of a lung lesion is shown in Supplementary Fig. S1C. Best overall response included SD in 14 patients (53.8%; Supplementary Table S3). One patient with metastatic melanoma, previously treated with ipilimumab and a BRAF inhibitor, received 25 cycles of NKTR-214 and had durable SD for 15 months. A second patient with metastatic RCC, who had progressed on HD IL2 and was refractory to single-agent anti-OX40 and nivolumab, was treated with 19 cycles of NKTR-214 and had durable SD for 13 months. Of note, there were 3 immunotherapy-naïve patients with RCC that showed immunologic changes in the blood and tumor, who received standard-of-care nivolumab within 1 month immediately following end of treatment with NKTR-214, and all 3 patients experienced a partial response
Preferred term a
Grades 1–2 Grades 3–5
Total (%)
0.003 mg/kg(q3w)( n = 4)
0.006 mg/kg(q3w)
( n = 11)
0.006 mg/kg(q2w)( n = 6)
0.009 mg/kg(q3w)( n = 6)
0.012 mg/kg(q3w)( n = 1)
0.003 mg/kg(q3w)( n = 4)
0.006 mg/kg(q3w)
( n = 11)
0.006 mg/kg(q2w)( n = 6)
0.009 mg/kg(q3w)( n = 6)
0.012 mg/kg(q3w)( n = 1)
Anxiety 1 (25) 1 (9) 1 (17) 3 (11)
Blood creatinine increased 1 (9) 1 (17) 1 (17) 3 (11)
Cytokine release syndrome 2 (33) 1 (100) 3 (11)
Dry skin 1 (25) 2 (18) 3 (11)
Dyspepsia 1 (17) 1 (17) 1 (100) 3 (11)
Generalized edema 1 (9) 1 (17) 1 (100) 3 (11)
Muscular weakness 1 (25) 1 (9) 1 (17) 3 (11)
Oropharyngeal pain 1 (25) 2 (18) 3 (11)
Pain in extremity 1 (9) 1 (17) 1 (17) 3 (11)
NOTE: Patients reporting more than one AE within the same preferred term are counted once at the highest severity reported. a Does not include events that occurred in <3 patients at grade 1 and 2 severity. b Flu-like symptoms include the following preferred terms: “Infl uenza-like illness,” “Infl uenza,” “Pyrexia,” and “Chills.” c Rash includes the following preferred terms: “Erythema,” “Rash,” “Rash erythematous,” “Rash maculo-papular,” “Rash pruritic,” “Rash pustular,” “Rash vesicular,” “Rash generalized,” and “Rash macular.”
Table 1. TEAEs occurring in 3 or more patients across all doses (Continued)
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495
NKTR-214 in Patients with Advanced Solid Tumors RESEARCH BRIEF
JUNE 2019 CANCER DISCOVERY | 715
at their first post-treatment scan after follow-on therapy with nivolumab.
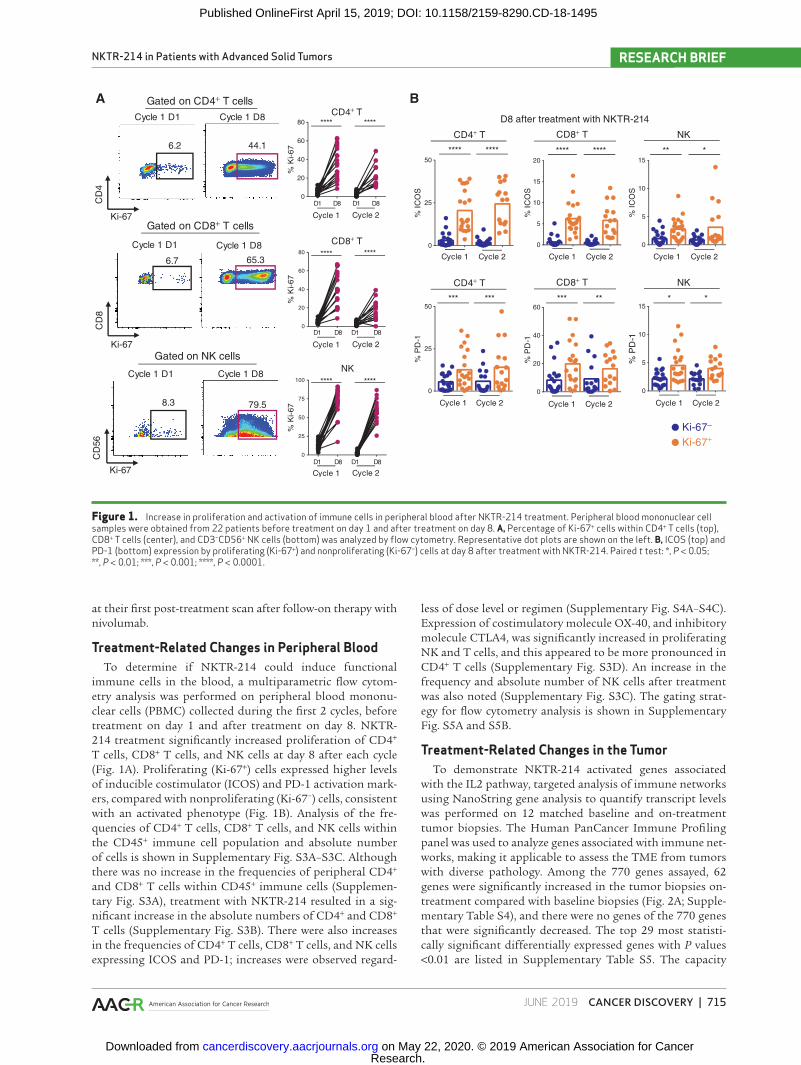
Treatment-Related Changes in Peripheral BloodTo determine if NKTR-214 could induce functional
immune cells in the blood, a multiparametric flow cytom-etry analysis was performed on peripheral blood mononu-clear cells (PBMC) collected during the first 2 cycles, before treatment on day 1 and after treatment on day 8. NKTR-214 treatment significantly increased proliferation of CD4+ T cells, CD8+ T cells, and NK cells at day 8 after each cycle (Fig. 1A). Proliferating (Ki-67+) cells expressed higher levels of inducible costimulator (ICOS) and PD-1 activation mark-ers, compared with nonproliferating (Ki-67−) cells, consistent with an activated phenotype (Fig. 1B). Analysis of the fre-quencies of CD4+ T cells, CD8+ T cells, and NK cells within the CD45+ immune cell population and absolute number of cells is shown in Supplementary Fig. S3A–S3C. Although there was no increase in the frequencies of peripheral CD4+ and CD8+ T cells within CD45+ immune cells (Supplemen-tary Fig. S3A), treatment with NKTR-214 resulted in a sig-nificant increase in the absolute numbers of CD4+ and CD8+ T cells (Supplementary Fig. S3B). There were also increases in the frequencies of CD4+ T cells, CD8+ T cells, and NK cells expressing ICOS and PD-1; increases were observed regard-
less of dose level or regimen (Supplementary Fig. S4A–S4C). Expression of costimulatory molecule OX-40, and inhibitory molecule CTLA4, was significantly increased in proliferating NK and T cells, and this appeared to be more pronounced in CD4+ T cells (Supplementary Fig. S3D). An increase in the frequency and absolute number of NK cells after treatment was also noted (Supplementary Fig. S3C). The gating strat-egy for flow cytometry analysis is shown in Supplementary Fig. S5A and S5B.
Treatment-Related Changes in the TumorTo demonstrate NKTR-214 activated genes associated
with the IL2 pathway, targeted analysis of immune networks using NanoString gene analysis to quantify transcript levels was performed on 12 matched baseline and on-treatment tumor biopsies. The Human PanCancer Immune Profiling panel was used to analyze genes associated with immune net-works, making it applicable to assess the TME from tumors with diverse pathology. Among the 770 genes assayed, 62 genes were significantly increased in the tumor biopsies on-treatment compared with baseline biopsies (Fig. 2A; Supple-mentary Table S4), and there were no genes of the 770 genes that were significantly decreased. The top 29 most statisti-cally significant differentially expressed genes with P values <0.01 are listed in Supplementary Table S5. The capacity
Figure 1. Increase in proliferation and activation of immune cells in peripheral blood after NKTR-214 treatment. Peripheral blood mononuclear cell samples were obtained from 22 patients before treatment on day 1 and after treatment on day 8. A, Percentage of Ki-67+ cells within CD4+ T cells (top), CD8+ T cells (center), and CD3−CD56+ NK cells (bottom) was analyzed by flow cytometry. Representative dot plots are shown on the left. B, ICOS (top) and PD-1 (bottom) expression by proliferating (Ki-67+) and nonproliferating (Ki-67−) cells at day 8 after treatment with NKTR-214. Paired t test: *, P < 0.05; **, P < 0.01; ***, P < 0.001; ****, P < 0.0001.
Gated on CD4+ T cells CD4+ T
CD4+ T
AC
D4
Ki-67
Ki-67
Ki-67
Cycle 1 D1 Cycle 1 D8
Gated on CD8+ T cells
Gated on NK cells
Cycle 1 D1 Cycle 1 D8
CD
8
Cycle 1 D1 Cycle 1 D8
CD
56
8.3 79.5
****
% K
i-67
****
Cycle 1 Cycle 2
D1 D8 D1 D8
NK
NK
****
% K
i-67
****
Cycle 1 Cycle 2D1 D8 D1 D8
CD8+ T
CD8+ T
****
% K
i-67
****
Cycle 1 Cycle 2
D1 D8 D1 D8
0
20
40
60
80
0
20
40
60
80
0
25
50
75
100
BD8 after treatment with NKTR-214
% IC
OS
**** ****
Ki-67−
Ki-67+
% P
D-1
*** ***
% IC
OS
**** ****
% P
D-1
*** **
% IC
OS
** *
CD4+ T NKCD8+ T
% P
D-1
* *
Cycle 1 Cycle 2
Cycle 1 Cycle 2
Cycle 1 Cycle 2 Cycle 1 Cycle 2
Cycle 1 Cycle 2 Cycle 1 Cycle 2
6.2 44.1
6.7 65.3
0
5
10
15
20
0
25
50
0
5
10
15
0
25
50
0
20
40
60
0
5
10
15
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

Bentebibel et al.RESEARCH BRIEF
716 | CANCER DISCOVERY JUNE 2019 www.aacrjournals.org
of NKTR-214 to induce immune activation, cytotoxic and effector gene signatures in the tumor was assessed. Our analysis revealed an increased expression of genes associated with T-cell infiltration and signaling (CD3G, CD3D, CD3E, CD247, and ZAP70; P ≤ 0.05), T-cell activation and coinhibi-tory molecules (ICOS, TNFRSF9, PDCD1, CTLA4, TIGIT, and LAG3; P ≤ 0.05), and of cytotoxic effector genes (PRF1, GZMB, GZMA, and GZMK; P ≤ 0.05). Genes encoding for PD-L1 and PD-L2 (CD274, PDCD1LG2; P ≤ 0.05; Fig. 2B–E), SOCS1, and IDO1 were also significantly increased, whereas HAVCR2 (TIM3) and MHC class 1 molecules had no change (Supple-mentary Fig. S6A). Notably, CD8 and CD4+ Th1-associated genes were increased after treatment (CD8A, CD8B, EOMES, TBX21, and IFNG; P ≤ 0.05), with no significant change noted in Th2, Th17, or inhibitory cytokine-associated genes (IL4, GATA3, IL17A, RORC, TGFB1, TGFB2, and IL10; Fig. 2F and G). Several immune NK-cell genes (KLRC2, KLRD1, KLRK1, and KLRC1; P ≤ 0.05) were increased (Fig. 2H). CXCR3, encoding a chemokine receptor expressed by NK cells, CD4+ Th1, and CD8+ cytotoxic T lymphocytes, is essential for their localization to the tumor and was also increased after treat-
ment (Fig. 2F). Consistently, the gene signatures associated with the presence and activity of T cells including CD4+ Th1 cells, CD8+ T cells, NK cells, and cytotoxic cells were all significantly increased (Supplementary Fig. S6B). Taken together, our results show that NKTR-214 induced a cyto-toxic and effector gene signature in the TME consistent with its mechanism of action.
To determine if NKTR-214 promoted an increase in TILs, 14 matched pretreatment and on-treatment tumor biop-sies were analyzed by flow cytometry and showed a marked increase in the frequency of CD45+ live cells in 8 of 14 patients after treatment (Fig. 3A). Similarly, the frequency of NK and CD8+ T cells within live CD45+ immune cells increased after treatment in 11 of 14 and 9 of 14 patients, respectively (Fig. 3B). To further assess the increase in immune cells within the tumor, the density of infiltrating CD8+ T-cell infiltrate was measured by IHC; the majority of patients, 6 of 10, showed an increase in the number of CD8+ staining per area (mm2) after treatment compared with baseline, and data from 1 patient are shown (Fig. 3C). Because tumor tissue was lim-ited in several patients, not all samples could be analyzed
Figure 2. Differential expression of mRNA in the TME after NKTR-214 treatment. NanoString gene analysis using the nCounter PanCancer Immune Profiling Panel to quantify transcript levels of 770 genes was performed on 12 matched baseline and on-treatment tumor biopsies. A, Volcano plot displaying each gene’s −log10 (P value) and log2 fold change with the selected covariate. Highly statistically significant genes fall at the top of the plot, and highly differentially expressed genes fall to either side. Horizontal line indicates thresholds for P = 0.05. P values were corrected using Benjamin–Yekutieli-adjusted FDR. B–H, Transcriptional analysis of 12 matched tumor biopsies at baseline (blue) and after NKTR-214 after treatment (orange). P values were obtained using paired t test, *, P < 0.05; **, P < 0.01. B, Selected genes related to T-cell infiltration and signaling. C, Genes reflecting T-cell activation and coinhibitory receptors. D, Genes associated with cytotoxic effector functions. E, Gene expression for PD-L1 (CD274) and PD-L2 (PDCD1LG2). F, CD8+ T and Th1 associated genes. G, Th2/Th17 cells and inhibitory cytokine associated genes. H, Markers found on infiltrating tumor-associated NK cells.
Pretreatment On-treatmentB
CD3G CD3D CD3E CD247 ZAP70
*
**
* **
**
RN
A c
ount
s (L
og2)
G
RN
A c
ount
s (L
og2)
IL17A RORC IL4 GATA3 TGFB1 TGFB2 IL10
C
ICOS TNFR-SF9
PDCD1 CTLA4 TIGIT LAG3
RN
A c
ount
s (L
og2)
***
**** *
*
D
RN
A c
ount
s (L
og2)
GZMK
* **
* *
E
RN
A c
ount
s (L
og2)
CD274 PDCD-1LG2
**
HF
A
Adjusted P = 0.05
−Lo
g 10
(P v
alue
)
CD247
CD8ATIGIT
KLRD1CD3D
TNFRSF9IL32 GZMA
PSMB9CTLA4
IFNG
GZMBCXCR3CD27
Differential expression On-treatment/pretreatment
−0.5 0.0 0.5 1.0 1.5 2.0
0
1
2
3
4
5
6
7
Significantly highly expressed mRNA
Log2 (fold change in gene expression)
4
8
12
4
8
12
5
10
15
5.0
7.5
10.0
RN
A c
ount
s (L
og2)
KLRC1 KLRC2 KLRD1 KLRK1
** * **
0
4
8
12
RN
A c
ount
s (L
og2)
CXCR3CD8A CD8B EOMESTBX21 IFNG
**
***
* **
3
6
9
12
0
5
10
15
PRF1 GZMB GZMA
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

NKTR-214 in Patients with Advanced Solid Tumors RESEARCH BRIEF
JUNE 2019 CANCER DISCOVERY | 717
for flow cytometry, gene expression, and IHC. For example, some patients had samples available for flow cytometry and NanoString analysis but not IHC. However, there were 6 patients for whom both IHC and NanoString data were available (Supplementary Fig. S7A), and there was a good correlation between CD8+ T-cell changes measured by these two different approaches (Supplementary Fig. S7B). In pre-treatment and on-treatment tumor biopsies, sequencing of the T-cell receptor β (TCRβ) repertoire showed an increase in T-cell infiltrates in 10 of 12 patients and changes in clonal-ity with a trend toward increased frequency of specific clones after treatment in 8 of 12 patients (Fig. 3D). One patient with melanoma who had received 12 prior lines of therapy was analyzed for changes in productive clonality and clonal frequency, and NKTR-214 appeared to induce an increase in both existing and new clones at week 3 (Supplementary Fig. S8A). Furthermore, an increase in clonality was associated with increased T-cell infiltration in 7 of 12 patients, reflect-ing the induction of a more oligoclonal T-cell repertoire (Fig. 3D; Supplementary Fig. S8B).
Despite the robust proliferation and increase in the absolute number of CD4+CD25hiFOXP3+ Tregs in the peripheral blood after treatment (Fig. 3E; Supplementary Fig. S9A and S9B) and upregulation of markers asso-ciated with enhanced suppressive function (ICOS and CTLA4; Supplementary Fig. S9C; refs. 4, 15), NKTR-214 administration did not appear to have the same effect on CD4+CD25hiFOXP3+ Tregs in the TME as in the peripheral blood. Flow cytometry analysis showed that the percent-ages of CD4+CD25hiFOXP3+ Tregs were slightly increased in 4 patients and either reduced or did not change in 10 patients (Fig. 3F). From the same tumor biopsies analyzed, FOXP3 staining by IHC showed little to no increase in FOXP3 expression after NKTR-214 administration com-pared with baseline, and FOXP3+ cells were increased in 2 patients or did not change in 8 patients (Fig. 3G). The ratio of CD8+ T cells over CD4+CD25hiFOXP3+ Tregs, as meas-ured by flow cytometry, is shown in Supplementary Fig. S8C. The gating strategy for TIL flow cytometry analysis is shown in Supplementary Fig. S8D.
Figure 3. Intratumoral changes in critical lymphocyte populations and numbers after NKTR-214 treatment. Tumor biopsies were obtained at baseline (blue) and after NKTR-214 treatment (orange). Immune infiltrates, including CD45+ live cells, NK cells, and CD8+ T cells, were analyzed by flow cytometry on freshly disaggregated tumor tissue. Patients #13 and #14 received a NKTR-214 dose of 0.006 mg/kg q2w. A, Percentage of live CD45+ cells within total cells. B, Percentage of NK cells (top plot) and CD8+ T cells (bottom plot) within CD45+ live cells. C, A portion of the tumor biopsy from the chest wall of a patient with RCC (#13) dosed q2w was further analyzed for CD8 staining by IHC (left), 10 patients had pretreatment and on-treatment IHC data (right), and each circle represents one individual tumor sample with red circles indicating increased and black circles indicating similar or reduced number of CD8+ T cells on-treatment compared with pretreatment. D, TCR sequencing examining the percentage of T-cell infiltration (the fraction productive of cells mass estimate values obtained through the immuSeq Analyzer software; top plot) and clonality (bottom plot) in tumor biopsy samples, n = 12. E, Percentage of CD4+CD25hiFOXP3+ Tregs within total CD4+ T cells in the blood before and 8 days after treatment with NKTR-214. A representative result is shown on the left. Paired t test, **, P < 0.01. F, Percentage of CD4+CD25hiFOXP3+ Tregs within CD3+ T cells in tumor biopsies samples was analyzed by flow cytometry, n = 14. G, Quantification of the number of FOXP3+ cells by IHC, n = 10, and each circle represents one individual tumor sample with red circles indicating increased and black circles indicating unchanged or reduced FOXP3+ cells on-treatment compared with pretreatment. H, PD-1 expres-sion within CD4+ (top plot) and CD8+ T cells (bottom plot) in tumor biopsy samples was analyzed by flow cytometry (n = 14).
A C
E
% N
K in
CD
45
+%
CD
8+
T in
CD
45
+
1 2 3 4 5 6 7 8 9 10 11 121314
1 2 3 4 5 6 7 8 9 10 1112 1314
Pretreatment On-treatmentB
0
10
20
40
60
0
10
40
80
Pretreatment On-treatment
Pretreatment On-treatment
In CD4+ T
Cycle 1 D1 Cycle 1 D80.6 14.0
FOXP3
CD
25
CD4+CD25hiFOXP3+ Tregs
Pretreatment On-treatmentF
0
5
10
15
% T
regs
in C
D3+
T
1 2 3 4 5 6 7 8 9 101112 1314
G
H
% P
D-1
in C
D4+
T%
PD
-1 in
CD
8+ T
1 2 3 4 5 6 7 8 9 10111213 14
1 2 3 4 5 6 7 8 9 10 1112 1314
0
1
2
4
810
20
% L
ive
CD
45
+
1 2 3 4 5 6 7 8 9 10 1112 13 14
Pretreatment On-treatment
0 .0
0 .10 .1
0 .20 .30 .4
D
1 2 3 4 7 8 9 10 12 13 14 15
T-c
ell i
nfilt
ratio
n
1 2 3 4 7 8 9 10 12 13 14 150.0
0.1
0.2
0.3
0.4
Clo
nalit
y
0
20
4040
60
80
0
20
40406080
100
0.003(QW3)
0.006(QW3)
0.009(QW3)
0.006(QW2)
0.003(QW3)
0.006(QW3)
0.009(QW3)
0.006(QW2)
0.009(QW3)
0.006(QW2)
0.003(QW3)
0.006(QW3) 0.009
(QW3)0.006(QW2)
0.003(QW3)
0.006(QW3)
0.009(QW3)
0.006(QW2)
0.003(QW3)
0.006(QW3)
0.006(QW3)
Pretreatment
CD8+
0 3000
150
300
800
1,600
2,400
800 1,600 2,400
12
3
5
612
13
14
1617
CD8+ counts/mm2
pretreatment
CD
8+
cou
nts
/mm
2
on-t
reat
men
t
Cycle 1 Cycle 2
**
% T
regs
in
CD
4+ T
**
D1 D8 D1 D80
10
20
30
FOXP3 counts/mm2
pretreatment
0 30 600
30
60
200
400
600
200 400 600
1235
61213 14
16
17
FO
XP
3+
cou
nts
/mm
2
on-t
reat
men
t
CD8+
On-treatment
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

Bentebibel et al.RESEARCH BRIEF
718 | CANCER DISCOVERY JUNE 2019 www.aacrjournals.org
DISCUSSION
This is a first-in-human report of NKTR-214. Treatment with NKTR-214 was well tolerated and feasible as an out-patient regimen. Grade 3 TRAEs were experienced by 21.4% of patients; there were no grade 4 TRAEs or any treatment-related deaths. The most common TRAEs were of grade 1 and 2 severity and included flu-like symptoms, rash, and pruritus, the majority of which coincided with the peak plasma concentrations of the active cytokine and resolved spontaneously or were mitigated by nonprescription oral or topical treatments. NKTR-214–related hypotension was pre-dictable, manageable, and reversible. The incidence of grade 3 hypotension was reduced once hypotension risk mitigation strategies were implemented. Notably, 3 of the 5 patients who experienced grade 3 hypotension had preexisting adrenal insufficiency, were managed conservatively, and continued to be dosed on the study. The Safety Review Committee (SRC) decided to halt enrollment into the 0.012 mg/kg cohort after dosing 1 patient. This decision was based on the composite of hypotension, syncope, and cytokine release syndrome that necessitated a hospital admission of this patient and the goal to identify a NKTR-214 dose that could be delivered as a safe, outpatient treatment. Based on the tolerability, conveni-ent dosing schedule, and pharmacodynamic changes at all NKTR-214 doses tested, a NKTR-214 dose of 0.006 mg/kg q3w was selected as the RP2D.
NKTR-214 engaged the IL2R pathway and provided robust systemic immune activation with repeated admin-istration, as demonstrated by dynamic changes in absolute lymphocyte counts and sCD25. Most importantly, these pharmacodynamic changes did not wane after repeated cycles. NKTR-214 induced robust proliferation of CD4+ T cells, CD8+ T cells, and NK cells in the blood, and the cells were activated as indicated by high levels of ICOS, PD-1, CTLA4, and OX40 expression. Importantly, treatment with NKTR-214 resulted in a significant increase in the absolute numbers of CD4+ T cells, CD8+ T cells, and NK cells. The induction of CD4+ T-cell, CD8+ T-cell, and NK-cell prolif-eration in the peripheral blood was also observed in patients treated with human recombinant IL15 (rhIL15), and these changes were most evident in NK and CD8+ T cells and to a lesser degree in CD4+ T cells (16). IL15 shares the IL2/IL15Rβ (CD122) chain with IL2 and is known to stimulate prolifera-tion of T cells, induce generation of cytotoxic lymphocytes, and stimulate prolonged expansion of NK cells. In contrast to IL2, IL15 has no marked effects on the stimulation of Tregs and does not cause substantial toxicity necessitating intense supportive care. However, the use of rhIL15 as a therapeu-tic agent may not be optimal due to the low expression of IL15Rα and the need for high doses to achieve biological responses in vivo (17). The administration of rhIL15 as a daily i.v. bolus infusion for 12 consecutive days to 5 patients with metastatic malignant melanoma or metastatic RCC proved to be difficult due to clinical toxicities produced by intense cytokine secretion that occurred in the first 2 hours after treatment (16).
Importantly, treatment with NKTR-214 induced mean-ingful immunologic changes within the TME. At the RP2D, freshly isolated TILs showed that there was a 15.1-, 3.5-,
and 0.7-fold increase in CD8+ T cells, NK cells, and Treg cells, respectively (Supplementary Fig. S10). Transcriptional analysis of the on-treatment tumor biopsies highlighted dif-ferentially expressed genes that were significantly increased on-treatment, which support a fundamental reshaping of the TME toward immune cell activation and effector functions. NKTR-214 also triggered immune regulatory pathways as seen in the increased gene expression of PD-L1/PD-L2, TIGIT, LAG3, SOC1, and IDO1. Interestingly, NKTR-214 induced a gene signature associated with the presence and activity of T cells including Th1 cells and CD8+ T cells. The increase of this Th1/CD8 gene signature was not associated with an increase in the gene signature representing Th2 or Th17 cells that are known to be mediators of inflammation associated with anti–PD-1 and anti-CTLA4 therapy–induced irAEs (18, 19). A study of patients with melanoma treated with anti-CTLA4 combined with HD IL2 demonstrated a trend toward a decreased incidence of grade 3/4 irAEs compared with patients receiving anti-CTLA4 without IL2 (17% vs. 29% and 32%; refs. 20, 21). Prieto and colleagues proposed an elegant theory that the Tregs induced by HD IL2 may decrease the activity of autoreactive T cells to reduce the incidence of irAEs (21). It is well established that IL2 signals control the polarization of CD4+ T-cell subsets leading to enhancement of Th1 and Tregs while limiting the differentiation into Th17 (22, 23). Several mechanisms have been proposed to explain the negative effect of IL2 on Th17, including lowering the expression of the IL6Rβ on CD4+ T cells, thereby reducing the IL6-mediated STAT3 phosphorylation that is essential for the induction of Th17 (24). Other studies showed that the IL2 signaling through STAT5, which competes with STAT3 for binding the IL17 gene locus, constrains the generation of Th17 (25, 26). Hence, the immune effect of NKTR-214 on the tumor appeared to be Th1-dominant with no induction of Th2 or Th17 gene signatures. Despite the increases in Tregs in the periphery with NKTR-214 administration, expansion of these cells was limited in the tumor. Preclinical evidence from mouse tumor models indicates that NKTR-214 limits intratumoral Treg proliferation and survival by way of pro-moting apoptosis, thereby polarizing the TME toward CD8+ T cells and consequently driving a very high CD8+/Treg ratio (12, 27). Exploratory studies are in progress to further probe the mechanisms by which peripheral Tregs are preserved while intratumoral Tregs are not.
A key immunologic observation was the increase in the percentage of proliferating CD8+ T cells also expressing increased levels of PD-1 in the TME (Fig. 3H). Studies have demonstrated that PD-1 identifies CD8+ tumor-reactive T cells in infiltrating tumors (2, 28–31). The increase in the percentage of CD8+PD-1+ T cells in patients’ tumors and the tumor shrinkage observed in 35% of patients, includ-ing one unconfirmed partial response, is promising. Durable SD greater than 1 year was seen in 2 patients, with 1 patient having failed 3 prior immunotherapies. It is possible that compensatory mechanisms, namely PD-L1/PD-L2 (Fig. 2E), may have dampened the potential of these CD8+PD-1+ T cells to convert patients into responders (31–33). Intriguingly, 3 patients with RCC who were anti–PD-1 treatment-naïve experienced TIL elevation with tumor reductions of 1%, 10%, and 20%; all 3 patients ended NKTR-214 with SD and within
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

NKTR-214 in Patients with Advanced Solid Tumors RESEARCH BRIEF
JUNE 2019 CANCER DISCOVERY | 719
1 month started anti–PD-1 treatment and experienced rapid tumor reductions at first scan on-treatment, resulting in partial responses (34). These anecdotal observations sup-ported the hypothesis that NKTR-214 treatment may have conditioned the TME by expanding activated TILs, thereby potentially providing synergy with therapies that block inhibi-tory signals, such as those of the PD-1/PD-L1 axis.
In summary, every patient evaluated showed evidence for activation of the immune response, at all four doses tested, and these effects were reproduced with repeated administration. Given the small number of patients evaluable at q2w (n = 4), no conclusions can be made on the impact of immune activa-tion with a shorter frequency of dosing. Based on the biological activity and tolerability of NKTR-214 as well as the nonoverlap-ping toxicities with approved checkpoint inhibitors, NKTR-214 is being combined with approved anti–PD-1/PD-L1/CTLA4 agents in ongoing clinical trials. NKTR-214, as a T-cell and NK-cell growth factor, may serve as a central mechanism for boosting tumor-specific T-cell proliferation and activation in the TME and has the potential to serve as a backbone therapy for combination therapy with a variety of agents.
METHODSPatients and Study Design
This was a multicenter, open-label dose-escalation study using a 3+3 design. Eligible patients were treatment-refractory to ≥1 prior therapy for advanced or locally advanced disease. Twenty-eight patients with a histologically confirmed diagnosis of RCC, melanoma, urothelial carcinoma, breast cancer, leiomyosarcoma, chondrosarcoma, or colorectal carcinoma not amenable to curative therapy were enrolled. All patients provided written informed con-sent before any protocol-specified procedures. The primary objec-tives were to assess the safety, MTD, RP2D, and antitumor clinical activity. Secondary objectives were to characterize pharmacokinetics, pharmacodynamics, and immunologic changes in blood and tumor. NKTR-214 was administered at 0.003, 0.006, 0.009, and 0.012 mg/kg as a 15-minute i.v. infusion q3w or 0.006 mg/kg q2w until disease progression or unacceptable toxicities occurred. Patients were held for 24 hours in an infusion center after the first dose of NKTR-214; however, subsequent cycles were administered on an outpatient basis. If no DLTs were observed in a cohort after 21 days, the dose was escalated for the following cohort after review by the SRC, which consisted of the sponsor and at least one site investigator. Additional patients were added to a lower-dose cohort to further assess the safety and tolerability. All patients who received study treatment and one post-treatment scan were evaluable for antitumor activity. Investigator-assessed antitumor activity was evaluated using RECIST 1.1. Baseline tumor imaging was completed within 4 weeks before starting therapy and every 8 weeks thereafter. Tumor responses were confirmed with a repeat scan at least 4 weeks later.
SafetyAll patients who received any study drug were included in the
safety analyses. AEs, SAEs, and laboratory abnormalities were graded per the National Cancer Institute Common Terminology Criteria for Adverse Events, Version 4.03, and monitored throughout the study until 30 days after the last dose of study drug. TRAEs and TEAEs were reported throughout the observation period and recorded once per patient at the highest grade. DLT was defined as any nontransient grade 3, 4, or 5 hematologic or nonhematologic toxicity that occurred within the first 21 days after dosing and was deemed related or possi-bly related to the administration of NKTR-214. The MTD was defined
as the highest dose of NKTR-214 that was administered without caus-ing any unacceptable side effects or AEs. irAEs were considered AEs of special interest due to their potential clinical significance.
Biomarker AnalysisSerial blood and tumor tissue samples were collected to perform
in-depth analysis of immune cells using flow cytometry, nCounter gene expression assay (NanoString), IHC, and TCR sequencing; details are provided in the Supplementary Information.
Statistical MethodsSummary statistics were used for any continuous variables; num-
bers and percentage were used for categorical variables. For all analyses, baseline values were defined as the last value before the first dose of NKTR-214. All statistical calculations were performed using Statistical Analysis System (SAS) version 9.4 (SAS Institute). Statisti-cal analyses for immune profiling by flow cytometry were performed with GraphPad Prism 7.0 (GraphPad Software). The significance of the difference between groups in the experiments was evaluated by a two-tailed paired t test. A value of P <0.05 was considered statistically significant.
Disclosure of Potential Conflicts of InterestM.E. Hurwitz reports receiving commercial research grants from
Apexigen, Astellas, Innocrin, Iovance, Merck, Nektar Therapeutics, Novartis, Pfizer, Progenics, Sanofi Aventis, Seattle Genetics, Astra-Zeneca, Bayer, Bristol-Myers Squibb, Corvus, Eli Lilly, Endocyte, Genentech, and Genmab; is a consultant/advisory board mem-ber for Nektar Therapeutics, Janssen, and CRISPR Therapeutics; and reports the receipt of remuneration from Gamida Cell. H.M. Kluger reports receiving commercial research grants from Bris-tol-Myers Squibb, Merck, and Apexigen; is a consultant/advisory board member for Nektar, Iovance, Merck, Genentech, Corvus, Immunocore, Biodesix, Apexigen, and Alexion; and reports receiv-ing other remuneration from Pfizer and Nektar. M.T. Tetzlaff is a consultant/advisory board member for Novartis LLC, Myriad Genetics, and Seattle Genetics. M.A. Tagliaferri is CMO at Nektar and has ownership interest (including stock, patents, etc.) in the same. J. Zalevsky is Chief Scientific Officer at Nektar Therapeutics and has ownership interest (including stock, patents, etc.) in the same. U. Hoch has ownership interest (including stock, patents, etc.) in Nektar. C. Fanton has ownership interest (including stock, patents, etc.) in Nektar Therapeutics. S. Aung has ownership inter-est (including stock, patents, etc.) in Nektar Therapeutics. P. Hwu is a consultant/advisory board member for Dragonfly, Glaxo-SmithKline, Immatics, and Sanofi. N.M. Tannir reports receiving a commercial research grant from Nektar Therapeutics and is a consultant/advisory board member for the same. M. Sznol is a consultant/advisory board member for Genentech-Roche, Bristol-Myers, Merck US, Theravance, Biodesix, Vaccinex, Janssen/Johnson & Johnson, Modulate Therapeutics, Baxalta-Shire, Incyte, Newlink Genetics, Lion Biotechnologies, AstraZeneca/Medimmune, Ago-nox, Arbutus, Celldex, Inovio, Gritstone, Molecular Partners, Innate Pharma, AbbVie, Immunocore, Genmab, Pfizer, Almac, Hinge, Alla-kos, Anaeropharma, Array, Symphogen-Scientific (advisory board), Adaptimmune-Scientific (advisory board), Omniox-Scientific (advi-sory board), Lycera (formerly on scientific advisory board), Pieris (scientific advisory board), Novartis, Amphivena (stock options only), Adaptive Biotechnologies (stock options only), Intensity (stock options only), Axtym (stock options only), Torque, Torque (stock options), Kyowa-Kirin, Seattle Genetics, Nektar, Pierre-Fabre, and Lilly. A. Diab reports receiving a commercial research grant from Nektar Therapeutics and is a consultant/advisory board member for the same. No potential conflicts of interest of were disclosed by the other authors.
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

Bentebibel et al.RESEARCH BRIEF
720 | CANCER DISCOVERY JUNE 2019 www.aacrjournals.org
Authors’ ContributionsConception and design: M.E. Hurwitz, C. Haymaker, H.M. Kluger, M.A. Tagliaferri, J. Zalevsky, U. Hoch, S. Aung, P. Hwu, B.D. Curti, N.M. Tannir, A. DiabDevelopment of methodology: S.-E. Bentebibel, M.E. Hurwitz, M.T. Tetzlaff, M.A. Tagliaferri, U. Hoch, C. Fanton, S. Aung, A. DiabAcquisition of data (provided animals, acquired and managed patients, provided facilities, etc.): S.-E. Bentebibel, M.E. Hurwitz, H.M. Kluger, M.T. Tetzlaff, S. Aung, B.D. Curti, N.M. Tannir, M. Sznol, A. DiabAnalysis and interpretation of data (e.g., statistical analysis, bio-statistics, computational analysis): S.-E. Bentebibel, M.E. Hurwitz, C. Bernatchez, C. Haymaker, C.W. Hudgens, M.T. Tetzlaff, M.A. Tagliaferri, J. Zalevsky, U. Hoch, C. Fanton, S. Aung, P. Hwu, N.M. Tannir, M. Sznol, A. DiabWriting, review, and/or revision of the manuscript: S.-E. Bentebibel, M.E. Hurwitz, C. Bernatchez, C. Haymaker, H.M. Kluger, M.T. Tetzlaff, M.A. Tagliaferri, J. Zalevsky, U. Hoch, C. Fanton, S. Aung, P. Hwu, B.D. Curti, N.M. Tannir, M. Sznol, A. DiabAdministrative, technical, or material support (i.e., reporting or organizing data, constructing databases): S.-E. Bentebibel, C. Fanton, S. AungStudy supervision: C. Bernatchez, M.A. Tagliaferri, S. Aung, A. Diab
AcknowledgmentsThis project was supported in part by the Translational Molecular
Pathology-Immunoprofiling lab (TMP-IL) at the Department Trans-lational Molecular Pathology, The University of Texas MD Anderson Cancer Center. Funding for this study was provided by Nektar Thera-peutics. We thank the patients, their caregivers and families, and the investigators who participated in this study. We also thank Phillips Gilmore Oncology Communications for providing editorial support, funded by Nektar Therapeutics.
Received December 22, 2018; revised March 25, 2019; accepted April 9, 2019; published first April 15, 2019.
REFERENCES 1. Daud AI, Wolchok JD, Robert C, Hwu WJ, Weber JS, Ribas A, et al.
Programmed death-ligand 1 expression and response to the anti-programmed death 1 antibody pembrolizumab in melanoma. J Clin Oncol 2016;34:4102–9.
2. Daud AI, Loo K, Pauli ML, Sanchez-Rodriguez R, Sandoval PM, Tara-vati K, et al. Tumor immune profiling predicts response to anti-PD-1 therapy in human melanoma. J Clin Invest 2016;126:3447–52.
3. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014;515:568–71.
4. Sim GC, Martin-Orozco N, Jin L, Yang Y, Wu S, Washington E, et al. IL-2 therapy promotes suppressive ICOS+ Treg expansion in mela-noma patients. J Clin Invest 2014;124:99–110.
5. Rosenberg SA. IL-2: the first effective immunotherapy for human cancer. J Immunol 2014;192:5451–8.
6. Dutcher JP, Gaynor ER, Boldt DH, Doroshow JH, Bar MH, Sznol M, et al. A phase II study of high-dose continuous infusion interleukin-2 with lymphokine-activated killer cells in patients with metastatic melanoma. J Clin Oncol 1991;9:641–8.
7. Chang AE, Hyatt CL, Rosenberg SA. Systemic administration of recombinant human interleukin-2 in mice. J Biol Response Mod 1984;3:561–72.
8. Kruit WH, Punt CJ, Goey SH, de Mulder PH, Gratama JW, Eggermont AM, et al. Dose efficacy study of two schedules of high-dose bolus administration of interleukin 2 and interferon in metastatic mela-noma. Br J Cancer 1996;74:951–5.
9. Kruit WH, Punt KJ, Goey SH, de Mulder PH, van Hoogenhuyze DC, Henzen-Logmans SC, et al. Cardiotoxicity as a dose-limiting factor in a schedule of high dose bolus therapy with interleukin-2 and -interferon. An unexpectedly frequent complication. Cancer 1994;74:2850–6.
10. Lotze MT, Matory YL, Ettinghausen SE, Rayner AA, Sharrow SO, Seipp CA, et al. In vivo administration of purified human interleukin 2. II. Half-life, immunologic effects, and expansion of peripheral lymphoid cells in vivo with recombinant IL 2. J Immunol 1985;135: 2865–75.
11. Charych DH, Hoch U, Langowski JL, Lee SR, Addepalli MK, Kirk PB, et al. NKTR-214, an engineered cytokine with biased IL2 receptor binding, increased tumor exposure, and marked efficacy in mouse tumor models. Clin Cancer Res 2016;22:680–90.
12. Charych D, Khalili S, Dixit V, Kirk P, Chang T, Langowski J, et al. Modeling the receptor pharmacology, pharmacokinetics, and phar-macodynamics of NKTR-214, a kinetically-controlled interleu-kin-2 (IL2) receptor agonist for cancer immunotherapy. PLoS One 2017;12:e0179431.
13. Katre N, Knauf MJ, Laird WJ. Chemical modification of recombi-nant interleukin 2 by polyethylene glycol increases its potency in the murine Meth A sarcoma model. Proc Natl Acad Sci U S A 1987; 1487–91.
14. Yang JC, Topalian SL, Schwartzentruber DJ, Parkinson DR, Marincola FM, Weber JS, et al. The use of polyethylene glycol-modified interleu-kin-2 (PEG-IL-2) in the treatment of patients with metastatic renal cell carcinoma and melanoma. A phase I study and a randomized prospective study comparing IL-2 alone versus IL-2 combined with PEG-IL-2. Cancer 1995;76:687–94.
15. Martin-Orozco M, Li Y, Wang Y, Liu S, Hwu P, Liu YJ, et al. Melanoma cells express ICOS ligand to promote the activation and expansion of T-regulatory cells. Cancer Res 2010;70:9581–90.
16. Conlon KC, Lugli E, Welles HC, Rosenberg SA, Fojo AT, Morris JC, et al. Redistribution, hyperproliferation, activation of natural killer cells and CD8 T cells, and cytokine production during first-in-human clinical trial of recombinant human interleukin-15 in patients with cancer. J Clin Oncol 2015;33:74–82.
17. Zamai L, Ponti C, Mirandola P, Gobbi G, Papa S, Galeotti L, et al. NK cells and cancer. J Immunol 2007;178:4011–6.
18. von Euw E, Chodon T, Attar N, Jalil J, Koya RC, Comin-Anduix B, et al. CTLA4 blockade increases Th17 cells in patients with metastatic melanoma. Journal Transl Med 2009;7:35.
19. Dulos J, Carven GJ, van Boxtel SJ, Evers S, Driessen-Engels LJ, Hobo W, et al. PD-1 blockade augments Th1 and Th17 and suppresses Th2 responses in peripheral blood from patients with prostate and advanced melanoma cancer. J Immunother 2012;35:169–78.
20. Maker AV, Phan GQ, Attia P, Yang JC, Sherry RM, Topalian SL, et al. Tumor regression and autoimmunity in patients treated with cyto-toxic T lymphocyte-associated antigen 4 blockade and interleukin 2: a phase I/II study. Ann Surg Oncol 2005;12:1005–16.
21. Prieto PA, Yang JC, Sherry RM, Hughes MS, Kammula US, White DE, et al. CTLA-4 blockade with ipilimumab: long-term follow-up of 177 patients with metastatic melanoma. Clin Cancer Res 2012; 18:2039–47.
22. Boyman O, Sprent J. The role of interleukin-2 during homeostasis and activation of the immune system. Nat Rev Immunol 2012;12:180–90.
23. Klatzmann D, Abbas AK. The promise of low-dose interleukin-2 ther-apy for autoimmune and inflammatory diseases. Nat Rev Immunol 2015;15:283–94.
24. Liao W, Lin JX, Wang L, Li P, Leonard WJ. Modulation of cytokine receptors by IL-2 broadly regulates differentiation into helper T cell lineages. Nat Immunol 2011;12:551–9.
25. Laurence A, Tato CM, Davidson TS, Kanno Y, Chen Z, Yao Z, et al. Interleukin-2 signaling via STAT5 constrains T helper 17 cell genera-tion. Immunity 2007;26:371–81.
26. Hodi FS, Chesney J, Pavlick AC, Robert C, Grossman KF, McDermott DF, et al. Combined nivolumab and ipilimumab versus ipilimumab alone in patients with advanced melanoma: 2-year overall survival outcomes in a multicentre, randomised, controlled, phase 2 trial. Lancet Oncol 2016;17:1558–68.
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495

NKTR-214 in Patients with Advanced Solid Tumors RESEARCH BRIEF
JUNE 2019 CANCER DISCOVERY | 721
27. Sharma M, Fa’ak F, Janssen L, Khong H, Xiao Z, Hailemichael Y, et al. NKTR-214 enhances anti-tumor T cell immune responses induced by checkpoint blockade or vaccination. J Immunother Cancer 2017;5:86(Suppl 2; abstr P140).
28. Gros A, Robbins PF, Yao X, Li YF, Turcotte S, Tran E, et al. PD-1 identifies the patient specific CD8(+) tumor-reactive repertoire infil-trating human tumors. J Clin Invest 2014;124:2246–59.
29. Gros A, Parkhurst MR, Tran E, Pasetto A, Robbins PF, Ilyas S, et al. Prospective identification of neoantigen-specific lymphocytes in the peripheral blood of melanoma patients. Nat Med 2016;22: 433–8.
30. Badoual C, Hans S, Merillon N, Van Ryswick C, Ravel P, Benhamouda N, et al. PD-1-expressing tumor-infiltrating T cells are a favora-
ble prognostic biomarker in HPV-associated head and neck cancer. Cancer Res 2013;73:128–38.
31. Simon S, Labarriere N. PD-1 expression on tumor-specific T cells: Friend or foe for immunotherapy? Oncoimmunology 2017;7:e1364828.
32. Gajewski TF, Meng Y, Harlin H. Immune suppression in the tumor microenvironment. J Immunother 2006;29:233–40.
33. Spranger S, Gajewski TF. Impact of oncogenic pathways on evasion of antitumour immune responses. Nat Rev Cancer 2018;18:139–47.
34. Bernatchez C, Haymaker CL, Hurwitz ME, Kluger HM, Tetzlaff MT, Jackson N, et al. Effect of a novel IL-2 cytokine immune agonist (NKTR-214) on proliferating CD8+ T cells and PD-1 expression on immune cells in the tumor microenvironment in patients with prior checkpoint therapy. J Clin Oncol 2017;35(suppl; abstr 2545).
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495
2019;9:711-721. Published OnlineFirst April 15, 2019.Cancer Discov Salah-Eddine Bentebibel, Michael E. Hurwitz, Chantale Bernatchez, et al. Metastatic Solid Tumors
-Biased Cytokine, in Patients with Advanced orγβa Novel IL2RA First-in-Human Study and Biomarker Analysis of NKTR-214,
Updated version
10.1158/2159-8290.CD-18-1495doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerdiscovery.aacrjournals.org/content/suppl/2019/04/13/2159-8290.CD-18-1495.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerdiscovery.aacrjournals.org/content/9/6/711.full#ref-list-1
This article cites 32 articles, 9 of which you can access for free at:
Citing articles
http://cancerdiscovery.aacrjournals.org/content/9/6/711.full#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerdiscovery.aacrjournals.org/content/9/6/711To request permission to re-use all or part of this article, use this link
Research. on May 22, 2020. © 2019 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst April 15, 2019; DOI: 10.1158/2159-8290.CD-18-1495