a disruptive approach to pph prevention and management
TRANSCRIPT
A disruptive approach to PPH prevention and management
By Dr Kihara Anne Beatrice
PPH Steering Committee
President AFOG
Past president KOGS
Senior lecturer, University of Nairobi department of Obs/ Gyn
Consultant Obs/ Gyn Kenya
15th September 2021

Outline of presentation
• Moving from MDG’s to SDG’s
• Epidemiological trends of maternal mortality and causes of mortality
• Risk factors associated with PPH
• COVID 19 Pandemic impact on SRHR in LMIC
• Why are we not bending the curve with PPH?
• Disruptive discourse to prevention and management of PPH


Disruption attaining Sustainable development Goals through RMNCAH thriving, productivity and development
• Women’s health and well being addresses: Population health
Posterity
Prosperity
Peace and security
Planet
• Addressing PPH prevention and management necessitates a holistic approach to maternal SRHR with broader focus beyond pregnancy and related outcomes

Global Trends in maternal mortality 2000-2017
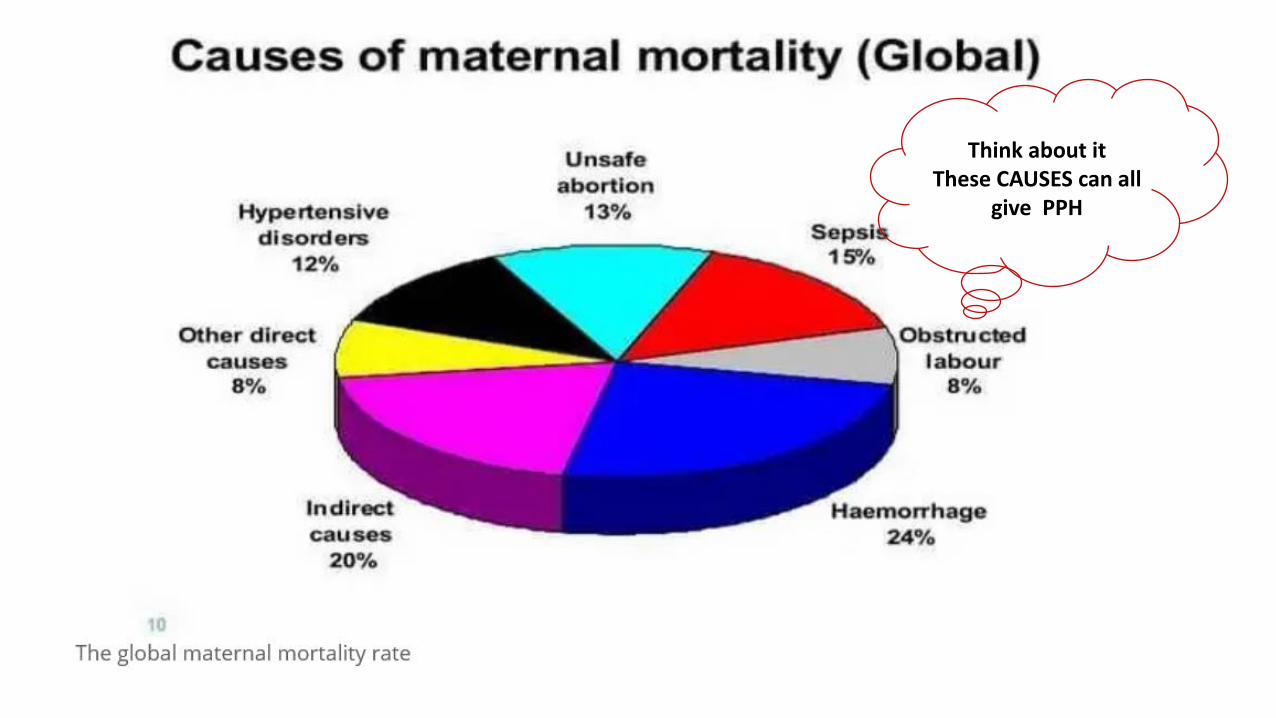
Think about it These CAUSES can all
give PPH

Risk factors for maternal deaths from PPH Obstetric causes • Unsafe Abortion• Severe Antepartum haemorrhage • Chorioamnionitis • Induction of labour • Augmentation of labour • Puerperal Sepsis• Early pregnancy /Ectopic pregnancy, GTD• Pregnancy Induced Hypertension (Eclampsia/ Pre-
eclampsia)• Delayed and Obstructed labour• delayed 2nd stage of labour • Placenta Previa• Adherent placenta • Uterine Rupture• IUFD• Previous PPH
Medical causes
• Anaemia• Thrombosis and Thromboembolism• Jaundice• Non - communicable diseases-
Diabetes, Cardiovascular disease• Hepatic failure• Renal failure• Severe anaesthesia Complications• Communicable diseases: malaria, HIV,
Tuberculosis


Why are we not able to bend the curve with PPH
The context narrative MUST change for PPH • Life course approach and in the continuum of care with inter-generational
outcomes
• Think Nutrition, WASH; environmental degradation and climate change
• Social determinants; self care; Pre-conceptual care with planned pregnancy
• One health and zoonotic diseases
• Robust health system – Life saving commodities; supply chain; intrapartum care( respectful care); immediate postpartum care
• Implementation of policies, guidelines, SOP, protocols
• Need for standardization: Emergency drills; EmONC; care bundles (flight not fright drills!)
• Data; implementation science; big data and machine modelling
• Advocacy

Moving maternal mortality from PPH towards SDG and ICPD +25

Life course approach in the continuum of care optimizing maternal health and pregnancy outcomes
INTERGENERATIONAL CONTINUUM

Life course approach in the continuum of care with intergenerational outcomes
Childhood Adolescence Preconceptual care
First 1000 days critical period Biomedicalbehavioural social health environmental influences
Optimizing health in preparation for planned pregnancy reduces maternal and child morbidity and mortality Inter-pregnancy interval: FP and contraception Risk assessment : Prevents complications in pregnancy and childbirth
Prevents birth defectd;prevents malnutrition/ prevents STI/HIV propagationTtreatment and control of non communicable diseases 1 in 3 women of reproductive age is anaemicWASH ,deworming , communicable and non communicable diseases micronutrients +macronutrients - Think nutrition and healthy plate
prophylaxis, supplements , fortification of foods , treatment address BMI
Malnutrition with risk for NCD Stunting wasting obesity
Health promotion and preventive strategies Attention to IKS:Menstrual health management rites of passage: early marriages , sexual debut; FGM; GBV( IPV)
Physical activity eliminate substance abuse
Wellness: self carehealthy recreation social livelihoods and demographic dividends
Development milestones Breast feeding practices
Endogenous oxytocin with early rooming in prevention of PPH
contraception Nourishment Immunogenic role maternal – neonatal bonding
Poverty reduction with address to multidimensional poverty index In SSA women and girls spend 40 Bilion hours each year collecting water
Education and early stimulation Parent indirect learning system ( (e.g. Kitchen garden ,
healthy foods)
Parent and role models . Mentorship/ apprenticeship
Environment and climate change Address the vulnerable and marginalized population
Political , Legislature and policy environment Investment and value proposition

Prenatal care Intrapartum care Postpartum care Inter-pregnancy
Interval
Risk assessmentPrenatal screening Diagnosis
Treatment
Risk assessment at triage Assess factors that predispose to PPH
Facility of home based birthTBA, Doula or skilled birth attendance
Monitoring of maternal and foetal surveillance Labour care guide Doppler / CTG
Companionship
Triage Immediate post partum care and warning signs 24-48 HoursImmediate postpartum contraception
immediate rooming in of the neonate treatment for puerperal sepsis
Interval of t least 24 months FP and contraception
Nutrition to avert maternal depletion syndrome Resumption of social livelihoods Resumption of sexual relationship
Macronutrients + micronutrients Hb11 gm % ( WHO)
Implementation of Standardized guidelines and protocols ; EmONCPrevention of PPH Uterotonics : AMTSL: OxytocinImmediate rooming in of the new-born Misoprostol Heat stable Carbetocin
Psychosocial support Puerperal blues to puerperal psychosis
Management of morbidities or disability from pregnancy and childbirth
Lifestyle: BMI, substance abuse
Medical co- morbidity Previous Obstetric performance
Challenge with PPH Estimation of blood loss Treatment of PPH NASGUBTAortal compression
Tranexamic acid Oxytocin MisoprostolCarboprost ProstaglandinsBlood and blood products Surgical approaches: B Lynch; Ligation of pelvic vasculature ; Hysterectomy
Partner and extended family engagement Reintegration into the community Provision of basic needs dn social livelihoods
3 delays needs a Supportive health system and robust referral mechanism Quality of care ; Clinical audit and MPDSR
Communications strategy; community engagement, mobilization and social accountability Rights based approach
Multisector intersectionality Social determinants , environmental and climate change
CARE
BUNDLES

Unplanned /mistimed / unwanted pregnancy Abortion services
• Access and coverage • Legislature • GAG Rule • VCAT • CAC/safe abortion • unsafe abortion / PAC• Telemedicine • Self care • timing of abortion , safety and follow up
outcomes Immediate post abortion FP
Family planning and contraception• Primary and secondary prevention strategy for
PPH • Access and coverage • Unmet need especially for primary actors • Immediate postpartum FP
Environment and climate change • population health • natural resources depletion • One health – zoonotic diseases • Reduction of environmental degradation :
overgrazing, energy source , lack of plant diversity • IEC in LMIC especially with primary actors and
women
Geo-political – socio- economic analysisLegislative and policy environment Leadership and governance Why investment in SRHR- SAFE MOTHERHOOD gives value proposition for developmentpopulation demographics and Demographic dividendsEnvironment preservation and climate change Universal health coverage – essential health benefit package Primary Health Care: level and competencies of service delivery Social accountability
Gender mainstreaming and integration • Gender equality and equity is
associated with better health outcomes
• A fundamental Human right
• Challenges gender norms and values, power relationships and decision making
• Health for all – Universality of health

Gender equality continuum tools

Social accountability
• ‘Social accountability’ has been highlighted as a potential mechanism to improve the performance of the health system in contributing to better maternal health outcomes.
• Social accountability refers to the mechanisms that citizens can use to hold the state and service providers to account for their actions.
Evidence based practices( dissemination and implementation continuum)
Policies and their analytics (living documents)
Budgetary allocations and expenditure tracking
Drives patients demand and utilization of quality services
Impact evaluations in PPH programs cannot be underscored

Research, innovations, creativity and development • Workforce competencies • Multidisciplinary and multisector strategies • Standardized tools and reporting (?ICD 11) • Data has the power for transformation• Collation and analytics • Benchmarking –clinical audits; scorecards, near
misses, MPDSR• Forecasting• Systems thinking • Informs – practice , policy , advocacy • Dissemination and the need for access to resources
for knowledge translation • Home grown solutions, innovations and creativity • MUST embrace big data , AI, machine learning in this
new frontier
Thank you