a comprehensive and practical approach to the management ...€¦ · a comprehensive and practical...
TRANSCRIPT
Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=ierx20
Expert Review of Respiratory Medicine
ISSN: 1747-6348 (Print) 1747-6356 (Online) Journal homepage: https://www.tandfonline.com/loi/ierx20
A comprehensive and practical approach to themanagement of idiopathic pulmonary fibrosis
Onofre Moran-Mendoza, Rebecca Colman, Meena Kalluri, Czerysh Cabalteja& Ingrid Harle
To cite this article: Onofre Moran-Mendoza, Rebecca Colman, Meena Kalluri, CzeryshCabalteja & Ingrid Harle (2019) A comprehensive and practical approach to the managementof idiopathic pulmonary fibrosis, Expert Review of Respiratory Medicine, 13:7, 601-614, DOI:10.1080/17476348.2019.1627204
To link to this article: https://doi.org/10.1080/17476348.2019.1627204
Published online: 08 Jun 2019.
Submit your article to this journal
Article views: 60
View Crossmark data
REVIEW
A comprehensive and practical approach to the management of idiopathicpulmonary fibrosisOnofre Moran-Mendozaa, Rebecca Colmanb, Meena Kalluric, Czerysh Cabaltejad and Ingrid Harlee
aDivision of Respiratory Medicine, Department of Medicine, Queen’s University, Kingston, ON, Canada; bDivision of Respirology, Department ofMedicine, University Health Network, Toronto, ON, Canada; cDivision of Pulmonary Medicine, Department of Medicine, University of Alberta,Edmonton, AB, Canada; dHoffmann-La Roche Ltd, Mississauga, ON, Canada; eDivision of Palliative Medicine, Department of Medicine andDepartment of Oncology, Queen’s University, Kingston, ON, Canada
ABSTRACTIntroduction: Idiopathic pulmonary fibrosis (IPF) is a debilitating, progressive, and fatal fibrotic pul-monary disease with a prognosis comparable to that of lung cancer. IPF management is a complexprocess that involves pharmacological and nonpharmacological interventions, extensive patient educa-tion, and addressing patient needs that change through the course of the illness.Areas covered: This review summarizes the key aspects of a multifaceted, multidisciplinary, individua-lized approach to IPF care that incorporates available treatment options, strategies to improve com-pliance with antifibrotic therapies, pulmonary rehabilitation, and the integration of palliative care forsymptom management. Aspects of care discussed include the use of antifibrotic therapy and non-pharmacological treatments, targeted education and psychosocial support, evaluation and manage-ment of comorbidities, and early integration of palliative care.Expert opinion: By incorporating this comprehensive approach to disease management, physicians canaddress most aspects of care for a patient with IPF to optimize survival and quality of life.
ARTICLE HISTORYReceived 11 February 2019Accepted 31 May 2019
KEYWORDSIdiopathic pulmonaryfibrosis; interstitial lungdisease; diseasemanagement; diseaseprogression; pirfenidone;nintedanib
1. Introduction
Idiopathic pulmonary fibrosis (IPF) is a progressive, irreversible,and fatal fibrosing lung disease with a median survival of2–5 years from diagnosis [1–3]. The 5-year survival rate of20–40% associated with IPF is worse than that of many can-cers [4]. IPF is the most common idiopathic interstitial lungdisease (ILD), affecting ≈5 million persons worldwide, particu-larly males; the mean age at presentation is 66 years [5,6].Smoking, environmental exposures, gastroesophageal refluxdisease (GERD), infections, and genetic predisposition arepotential risk factors for the development of IPF [1,7].
The clinical course of IPF is progressive, highly variable andunpredictable in individual patients and is frequently asso-ciated with a significant symptom burden [4]. Disease progres-sion can be accelerated by an acute exacerbation, a clinicallysignificant, rapid decline in lung function [8,9]. Risk factors forshort-term mortality include acute exacerbations, absoluteand relative decline of ≥10% in % predicted forced vital capa-city (FVC) over 52 weeks, high supplemental oxygen flow-rates, and respiratory-related hospitalizations [10–14].Whether disease progression is rapid or slow, managementof IPF is challenging because the needs of individual patientsare variable and change throughout the course of the disease.
Current models of IPF care emphasize multidisciplinaryteams, early diagnosis, the use of antifibrotic therapy, andmonitoring of disease progression [15–17]. The 2011American Thoracic Society/European Respiratory Society/
Japanese Respiratory Society/Latin American ThoracicAssociation (ATS/ERS/JRS/ALAT) consensus guidelines recom-mend clinical follow-up every 4–6 months, long-term oxygentherapy if hypoxemia is present, pulmonary rehabilitation (PR),and treatment of comorbidities such as GERD for the majorityof patients with IPF, as well as lung transplant for selectpatients [1]. In 2015, the conditional use of approved antifi-brotic therapies, which slow disease progression, was addedto the ATS/ERS/JRS/ALAT guidelines for IPF treatment [18].
The management of dyspnea, cough, and psychological suf-fering, which nearly all patients with IPF develop as the diseaseprogresses, are important aspects of care [1,4,15,19,20].A comprehensive care approach that includes pharmacologicaland nonpharmacological treatment, palliative care, patient edu-cation, and increased support throughout the course of illness isneeded. Disease-centric caremodels focus on specific treatmentsfor IPF but do not adequately meet all patient and caregiverneeds. In addition to controlling disease, the goals for deliveringcare should include improving quality of life (QoL), decreasingsymptom burden, providing caregiver support, and reducing theeconomic burden of IPF.
A single-center, retrospective cohort study (conducted beforethe approval of antifibrotics) in 284 patients with IPF showed thata bundled care approach for IPF based on the 2011 ATS/ERS/JRS/ALAT guidelines improved transplant-free survival [21]. Thisapproach included semiannual visits to an ILD clinic, PR, anannual 6-minute walk distance (6MWD) test, an annual
CONTACT Onofre Moran-Mendoza [email protected] Interstitial Lung Disease Clinic, Division of Respiratory and Sleep Medicine, Queen’s University,102 Stuart Street, Kingston, Ontario K7L 2V6, Canada
EXPERT REVIEW OF RESPIRATORY MEDICINE2019, VOL. 13, NO. 7, 601–614https://doi.org/10.1080/17476348.2019.1627204
© 2019 Informa UK Limited, trading as Taylor & Francis Group

echocardiogram, and GERD therapy [21]. In a recent exploratoryanalysis of experience at a single center in Canada,a multidisciplinary collaborative care model was associatedwith a reduction in healthcare utilization and more at-homedeaths compared with care received at the same center priorto the implementation of the collaborative care model [22]. Thecollaborative care team included a pulmonologist with expertisein ILD, a pulmonologist with expertise in palliative care, a nurse,a respiratory therapist, a physiotherapist, and a dietitian [22].A single-center survey of bereaved caregivers of patients withIPF indicated that targeted education, advance care planning,and improved communication can positively impact symptomcontrol, QoL, and caregiver burden in IPF [23]. These 3 studieshighlight the benefit of a holistic approach to IPF managementthat encompasses all aspects of care.
In this review, we provide evidence-based recommenda-tions when available and, in cases when no evidence-basedrecommendations are available, the consensus approach usedby experts in the management of patients with IPF from 3 ILDcenters in Canada. These recommendations based on expert
opinion should be applied as appropriate, given availabletreatment options wherever the treating physician practices.The available evidence is derived from randomized controlledtrials (RCTs)and cohort studies or extrapolated from studies ofother chronic pulmonary conditions. Our goal is to providea thorough overview of all care components that we considerimportant and necessary in a comprehensive approach to IPFmanagement (Figure 1). We describe treatment options andstrategies to mitigate antifibrotic-related adverse events (AEs)and explain the benefits of PR and the need for managementplans that are tailored to meet the needs of the specificpatient. We review the value of a multifaceted, multidisciplin-ary, individualized approach to treatment with early integra-tion of palliative care to optimize symptom control, improveQoL, and ease transitions throughout the illness journey.
2. Multifaceted IPF management approach
2.1. Education
Education for patients with IPF needs to be specific to theirdisease and to the treatments the individual patient receives.Disease education should address patient concerns about dis-ease progression and health deterioration and help them toprepare for the future [24]. Important components of educationinclude patient empowerment that prepares patients to copeand to live well with IPF [25,26]. Internet resources alone areinadequate, and clinicians should consider the informationalneeds of both patients and caregivers throughout the course ofthe illness [27–30]. Specialist ILD nurses and nurse practitionersare well positioned to support education, AE management, andadherence [31–33]. Several specific aspects of patient educationare noted in the relevant sections throughout this review.
2.2. Antifibrotic therapy
The two currently available antifibrotic therapies, pirfenidone(ideal dose, 801 mg 3 times daily [TID]) and nintedanib (ideal
Article Highlights
● The management of IPF is complex due to the unpredictable rate ofdisease progression, adverse events associated with antifibrotic thera-pies, the burden of comorbidities, the significant symptom burden,and the changing care and education needs of patients throughoutthe course of the disease
● A multifaceted, multidisciplinary approach to IPF management, tai-lored to each patient’s individual needs is recommended to optimallymanage a patient’s overall health and expectations
● Key aspects of a multifaceted approach to IPF management includeextensive patient education; early initiation of antifibrotic therapy,supplemental oxygen therapy, and pulmonary rehabilitation; moni-toring and management of IPF-associated comorbidities; early inte-gration of palliative care for managing IPF symptoms, especiallycough and dyspnea; psychosocial support and nutritional counseling;and dynamic conversations on advance care planning and to estab-lish goals of care throughout the illness journey
Figure 1. Overview of a multifaceted IPF management approach. COPD, chronic obstructive pulmonary disease; GERD, gastroesophageal reflux disease; IPF,idiopathic pulmonary fibrosis; O2, oxygen; OSA, obstructive sleep apnea.
602 O. MORAN-MENDOZA ET AL.

dose 150 mg twice daily [BID]), were approved for the treat-ment of IPF in Canada in 2012 and 2014, in Europe in 2011and 2015, and in the United States in 2014 and 2014, respec-tively, and received a conditional recommendation in the 2015ATS/ERS/JRS/ALAT treatment guidelines in 2015 [18]. Bothantifibrotics can slow disease progression as measured bythe rate of decline in % predicted FVC [34–37].
A meta-analysis of the phase 3 ASCEND (Study 016,NCT01366209) and CAPACITY (Studies 004 and 006;NCT00287716 and NCT00287729, respectively) trials and 2Japanese trials (Shionogi) of pirfenidone vs. placebo showedthat pirfenidone reduced the risk of all-cause mortality (HR,0.52; P = 0.01) and IPF-related mortality (HR, 0.35; P = 0.003)[38]. Post hoc analyses also found that pirfenidone reduced therisk of respiratory-related hospitalizations (HR, 0.52; P = 0.001)[39]. The INPULSIS-1 and -2 trials (NCT01335464 andNCT01335477) showed that nintedanib had a nonsignificanttrend toward reducing all-cause mortality (HR, 0.70; P = 0.14)[40]. The reasons for differences between nintedanib and pirfe-nidone regarding mortality and acute exacerbations are notwell understood, but the magnitude of the reduction in FVC(mL) decline was very similar in the phase 3 trials [34–37].Open-label long-term extension studies of pirfenidone (RECAP[NCT00662038] and INPULSIS-ON [NCT01619085]) supportedthe safety findings of the phase 3 trials [41,42].
A treatment benefit for either pirfenidone or nintedanibhas been shown in patients with less-advanced vs. more-advanced disease across a range of lung function criteria (%baseline FVC ≤50%–90%) in post hoc analyses of clinical trialdata and in real-world studies [43–48]. A post hoc analysis ofdata from ASCEND and CAPACITY showed that patients whoexperienced ≥10% absolute decline in % predicted FVC duringthe first 6 months of treatment and continued treatment withpirfenidone had lower risk of further decline in % predictedFVC or death during the subsequent 6 months compared withplacebo [49]. In a post hoc analysis of patients with IPF whohad ≥10% absolute decline in FVC in the first 24 weeks oftreatment with nintedanib in the INPULSIS trials, continuedtreatment was not associated with further FVC decline in thefollowing 24 weeks compared with placebo [50].
Important factors to consider when selecting antifibrotictherapy include a patient’s preferences, individual burden ofcomorbidities, and potential risks. The selection between pir-fenidone and nintedanib may be influenced by the patient’slifestyle and clinical conditions. Pirfenidone requires avoidanceof direct sun exposure (due to treatment-associated photo-sensitivity); nintedanib should be used with caution in patientswith a risk of bleeding or gastrointestinal (GI) perforation,including those receiving concomitant anticoagulants, corti-costeroids, or nonsteroidal anti-inflammatory drugs (due totreatment-associated increased bleeding risk) [51–56]. It isimportant to note that patients with recent history of myocar-dial infarction or stroke were excluded from the antifibroticclinical trials; however, an increased risk of these AEs has notbeen observed in post hoc analyses [34–37,57,58]. Pirfenidoneis metabolized by cytochrome P450 1A2 (CYP1A2) and shouldnot be used in combination with CYP1A2 inhibitors (e.g. flu-voxamine [absolute contraindication] and ciprofloxacin [per-mitted at 750 mg BID with a reduced dose of pirfenidone
534 mg TID], amiodarone, omeprazole, esomeprazole) due toincreased exposure and thus increased risk of AEs.Consumption of grapefruit juice is associated with CYP1A2inhibition and should be avoided during pirfenidone treat-ment. Pirfenidone should be avoided in combination withCYP1A2 inducers (e.g. rifampin, phenytoin, carbamazepine)due to reduced exposure [51]. Nintedanib is contraindicatedin patients with peanut or soy allergies and during pregnancy;nintedanib should be used cautiously (possibly at reduceddose) in combination with P-glycoprotein (P-gp) and cyto-chrome P450 3A4 (CYP3A4) inhibitors (e.g. ketoconazole, ery-thromycin) due to increased exposure and should be carefullyconsidered in combination with P-gp and CYP3A4 inducers(e.g. rifampicin, carbamazepine, phenytoin, St. John’s Wort)due to decreased exposure [54–56].
A new formulation of pirfenidone was approved in Canada,the United States, and Europe in 2017: 801-mg tablets TIDwith meals for patients maintaining full dose; this new formu-lation reduces the pill burden associated with the 267-mgcapsules, which are used for initial pirfenidone titration [59].However, the approval of the new 801-mg tablets was basedon a single-dose pharmacokinetics study performed in healthyvolunteers; fewer AEs were reported in patients who receivedpirfenidone after a meal than after an overnight fast [59].Therefore, it is important to monitor patients who switch to801-mg tablets; patients who experience significant AEs maybe switched back to the 267-mg capsules to accommodatedose reductions instead of discontinuing treatment.
2.2.1. Consideration of early initiation of antifibrotictherapyPatients may benefit from early initiation of antifibrotics forseveral reasons. Lung function decline is irreversible; therefore,the goal of antifibrotic treatment is to slow disease progression[15,16,60]. Baseline % predicted FVC itself does not predictdisease progression [43,44]. Patients with less-advanced disease(i.e. baseline % predicted FVC ≥50%) experience benefit fromantifibrotics similar to that in patients with more-advanceddisease [43–48]. Finally, disease progression, as measured byeither absolute or relative decline in % predicted FVC, andlower % predicted FVC are associated with an increased riskof IPF exacerbations and mortality [10–13,61,62]. Despite thesefindings, some countries do not provide reimbursement forpatients with less-advanced disease. Patients in these countriesshould be monitored frequently, so antifibrotics can be initiatedas early as possible in the course of the disease.
2.2.2. Antifibrotic-related adverse eventsIn the clinical trials, the most commonly reported treatment-emergent AEs (TEAEs) associated with antifibrotic therapieswere GI TEAEs (Figure 2) [63–65]. In the pooled phase 3pirfenidone clinical trials, the most common TEAEs were nau-sea (pirfenidone vs. placebo, 35.5% vs. 15.1% of patients),cough (23.1% vs. 24.0%), diarrhea (24.6% vs. 18.8%) upperrespiratory tract infection (22.6% vs. 20.2%), fatigue (23.0%vs. 16.8%), headache (20.5% vs. 18.1%), and rash (29.2% vs.9.0%) [66]. Other GI TEAEs reported in ≥10% of pirfenidone-treated patients were dyspepsia, GERD, and vomiting [66]. GITEAEs were most likely to occur within the first 3–6 months of
EXPERT REVIEW OF RESPIRATORY MEDICINE 603

pirfenidone treatment [67]. In the pooled phase 2 TOMORROW(NCT00514683) and phase 3 INPULSIS-1 and −2 nintedanibclinical trials, the most frequent TEAEs were diarrhea (ninteda-nib vs. placebo, 61.5% vs. 17.9%) and nausea (24.3% vs. 7.1%)[40]. Other GI TEAEs occurring in ≥10% of nintedanib-treatedpatients were vomiting and decreased appetite [40].
In the clinical trials, pirfenidone-specific TEAEs includedskin-related TEAEs, such as photosensitivity (pirfenidone vs.placebo, 9.3% vs. 1.1%) and rash (30.2% vs. 10.3%), whereasnintedanib-specific TEAEs included cardiovascular (nintedanibvs. placebo, 2.5% vs. 0.8%) and bleeding events (10% vs. 7%)[35,36,51,54,63,64,66]. Results from INPULSIS-ON, the open-label extension study of the INPULSIS trials, showed rates ofcardiovascular and bleeding events that were similar to thoseobserved in the placebo groups of INPULSIS and were notsignificantly different between previous nintedanib and pre-vious placebo groups [42].
The safety and tolerability profiles of antifibrotics observedin these large, RCTs have been supported by real-world dataand postmarketing experiences, in which patients typicallyhave more-advanced disease and significantly more comor-bidities than those in the clinical trials. In a single-center retro-spective study of 351 patients who received pirfenidone over4.5 years, TEAEs were mostly GI-related and similar to thoseobserved in the clinical trials; 61% of pirfenidone-treatedpatients experienced >2 AEs [68]. The majority of pirfenidone-associated TEAEs were tolerable or manageable by dosereduction and slower dose titrations, and approximately 1 in5 (20%) TEAEs resulted in treatment discontinuation [68]. Over4.5 years, 29% of patients discontinued pirfenidone comparedwith 12% of patients who discontinued over 1 year in thephase 3 trials [66,68]. The same study also reviewed TEAEs in124 patients receiving nintedanib over 1.5 years [68]. Mostnintedanib-associated TEAEs were GI-related, similar to theclinical trial findings [40,68]. Most patients (82%) experienced≥2 TEAEs, and 26% of patients discontinued nintedanib over1.5 years compared with 20.6% who discontinued over 1 yearin the clinical trials [40,68]. Consistent with these findings,
a separate, single-center, retrospective chart review study of129 pirfenidone-treated patients and 57 nintedanib-treatedpatients with IPF reported discontinuation rates of 21% and26% over a mean observation period of 1 year for pirfenidoneand nintedanib, respectively [69].
2.2.3. Prevention and management of antifibrotic-relatedadverse eventsA stepwise approach can be adopted to help patients preventand manage AEs associated with antifibrotics and continuetreatment (Table 1). Real-world studies indicate that access toan ILD nurse can play a critical role in AE management andadherence to antifibrotics through continued patient educa-tion [32,33]. The goal is to provide patients with informationand resources to help prevent the onset of AEs and, if AEs doarise, to implement effective strategies to mitigate the dura-tion and severity of symptoms. It is important for patients tounderstand the progressive and fatal nature of the disease andthe benefits of current treatment options. Education shouldbegin early, ideally at the time of diagnosis, and continuealong the illness trajectory as each patient’s experience willbe different. Whenever feasible, patients should be enrolled inpatient support groups.
If AE symptoms occur, dose reduction or temporary doseinterruptions should be considered to maintain ongoing treat-ment with either pirfenidone or nintedanib [64,70,71]. InPASSPORT, a safety study of pirfenidone in European patients,dose modifications were frequent (39% of patients who hadan AE associated with treatment), and patients who under-went dose modifications were less likely to discontinue treat-ment due to AEs (20% vs. 31%) [72,73]. Similarly, in anExpanded Access Program with pirfenidone in US patients,almost half of patients who had dose modifications wereable to return to the full dose [74]. Furthermore, analyses ofthe pirfenidone and nintedanib clinical trials indicate thatefficacy is maintained at doses below the full recommendeddose [36,37,42,75,76]. If AE symptoms persist or are severe,temporary treatment interruption can be used as a mitigating
Figure 2. Shared and drug-specific treatment-emergent adverse events with antifibrotic therapies [51,54]. ALT, alanine aminotransferase; AST, aspartate amino-transferase; CV, cardiovascular; GI, gastrointestinal.a Although both pirfenidone and nintedanib are associated with gastrointestinal adverse events, the frequency of individual adverse events is different with each drug.
604 O. MORAN-MENDOZA ET AL.
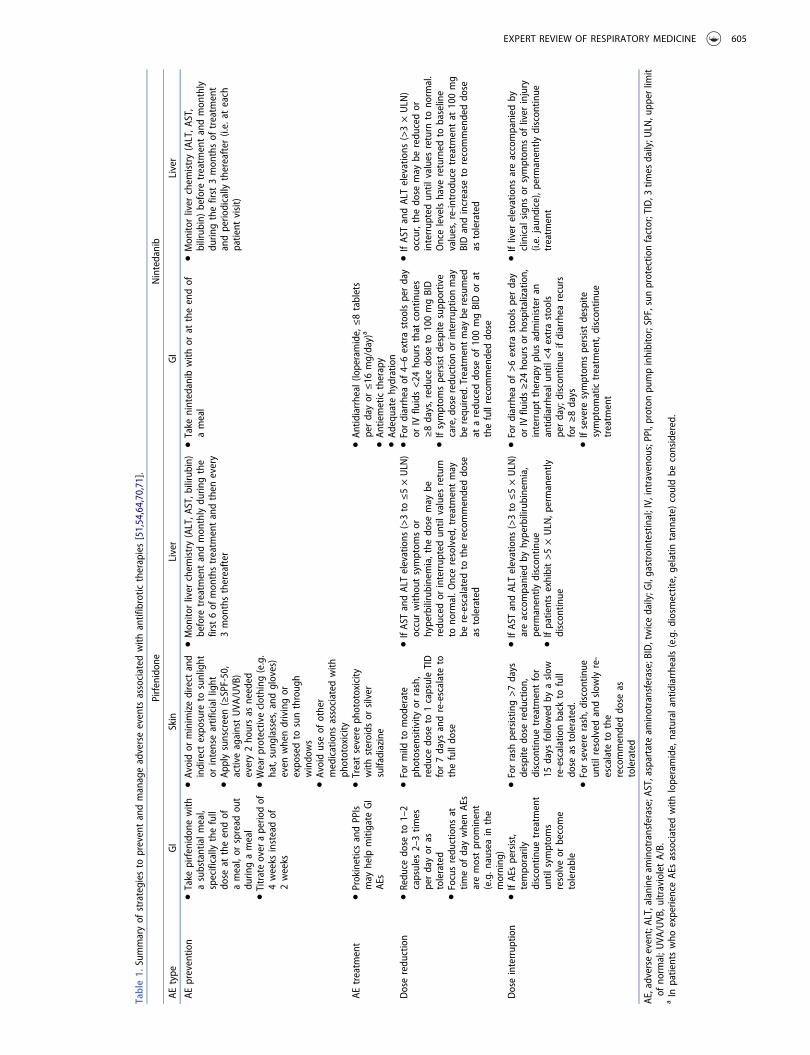
Table1.
Summaryof
strategies
topreventandmanageadverseevents
associated
with
antifibrotic
therapies[51,54,64,70,71].
Pirfenidon
eNintedanib
AEtype
GI
Skin
Liver
GI
Liver
AEpreventio
n●Take
pirfenidon
ewith
asubstantialm
eal,
specifically
thefull
dose
attheendof
ameal,or
spread
out
durin
gameal
●Titrateover
aperio
dof
4weeks
insteadof
2weeks
●Avoidor
minimizedirect
and
indirect
expo
sure
tosunlight
orintenseartificiallight
●Ap
plysunscreen(≥SPF-50,
activeagainstUVA
/UVB
)every2ho
ursas
needed
●Wearprotectiveclothing
(e.g.
hat,sung
lasses,and
gloves)
even
whendrivingor
expo
sedto
sunthroug
hwindo
ws
●Avoiduseof
other
medications
associated
with
phototoxicity
●Mon
itorliver
chem
istry(ALT,A
ST,b
ilirubin)
before
treatm
entandmon
thlydu
ringthe
first6of
mon
thstreatm
entandthen
every
3mon
thsthereafter
●Take
nintedanib
with
orat
theendof
ameal
●Mon
itorliver
chem
istry(ALT,A
ST,
bilirub
in)before
treatm
entandmon
thly
durin
gthefirst
3mon
thsof
treatm
ent
andperio
dically
thereafter
(i.e.at
each
patient
visit)
AEtreatm
ent
●ProkineticsandPPIs
may
help
mitigate
GI
AEs
●Treatsevere
phototoxicity
with
steroids
orsilver
sulfadiazine
●An
tidiarrheal(loperamide,≤8tablets
perdayor
≤16
mg/day)a
●An
tiemetictherapy
●Ad
equate
hydration
Doseredu
ction
●Redu
cedo
seto
1–2
capsules
2–3tim
esperdayor
astolerated
●Focusredu
ctions
attim
eof
daywhenAE
saremostprom
inent
(e.g.n
auseain
the
morning
)
●Formild
tomod
erate
photosensitivity
orrash,
redu
cedo
seto
1capsuleTID
for7days
andre-escalateto
thefulldo
se
●IfAS
TandALTelevations
(>3to
≤5×ULN
)occurwith
outsymptom
sor
hyperbilirubinemia,the
dose
may
beredu
cedor
interrup
tedun
tilvalues
return
tono
rmal.O
nceresolved,treatmentmay
bere-escalated
totherecommendeddo
seas
tolerated
●Fordiarrhea
of4–6extrastoolsperday
orIV
fluids<24
hoursthat
continues
≥8days,reducedo
seto
100mgBID
●Ifsymptom
spersistdespite
supp
ortive
care,doseredu
ctionor
interrup
tionmay
berequ
ired.Treatm
entmay
beresumed
ataredu
ceddo
seof
100mgBIDor
atthefullrecommendeddo
se
●IfAS
TandALTelevations
(>3×ULN
)occur,thedo
semay
beredu
cedor
interrup
tedun
tilvalues
return
tono
rmal.
Oncelevelshave
returned
tobaseline
values,re-introd
ucetreatm
entat
100mg
BIDandincrease
torecommendeddo
seas
tolerated
Doseinterrup
tion
●IfAE
spersist,
tempo
rarily
discon
tinue
treatm
ent
until
symptom
sresolveor
become
tolerable
●Forrash
persistin
g>7days
despite
dose
redu
ction,
discon
tinue
treatm
entfor
15days
followed
byaslow
re-escalationback
tofull
dose
astolerated.
●Forsevere
rash,d
iscontinue
until
resolved
andslow
lyre-
escalate
tothe
recommendeddo
seas
tolerated
●IfAS
TandALTelevations
(>3to
≤5×ULN
)areaccompanied
byhyperbilirubinemia,
perm
anently
discon
tinue
●Ifpatientsexhibit>5×ULN
,permanently
discon
tinue
●Fordiarrhea
of>6extrastoolsperday
orIV
fluids≥24
hoursor
hospitalization,
interrup
ttherapyplus
administeran
antid
iarrhealun
til<4extrastools
perday;discon
tinue
ifdiarrhea
recurs
for≥8days
●Ifsevere
symptom
spersistdespite
symptom
atictreatm
ent,discon
tinue
treatm
ent
●Ifliver
elevations
areaccompanied
byclinicalsign
sor
symptom
sof
liver
injury
(i.e.jaun
dice),perm
anently
discon
tinue
treatm
ent
AE,adverse
event;ALT,alanineam
inotransferase;A
ST,aspartate
aminotransferase;BID,twicedaily;G
I,gastrointestinal;IV,intravenou
s;PPI,proton
pumpinhibitor;SPF,sunprotectio
nfactor;TID,3
times
daily;U
LN,upp
erlim
itof
norm
al;U
VA/UVB
,ultravioletA/B.
aIn
patientswho
experienceAE
sassociated
with
loperamide,naturala
ntidiarrheals(e.g.d
iosm
ectite,gelatin
tann
ate)
couldbe
considered.
EXPERT REVIEW OF RESPIRATORY MEDICINE 605

strategy. Once symptoms have resolved, the patient’s doseshould be slowly titrated back to the full dose or to themaximum tolerated dose. Slow dose titration at treatmentinitiation can be considered with either pirfenidone or ninte-danib, particularly in patients with history of GI conditions.
2.3. Smoking cessation
Resources to assist in the cessation of smoking should beprovided to patients who are smokers. These may includediscussions, websites (American Lung Association [www.lung.org/stop-smoking/] and National Cancer Institute [www.smokefree.gov]), and referral for PR or counseling. At many trans-plant centers, in accordance with the 2014 InternationalSociety for Heart and Lung Transplantation (ISHLT) guidelines,tobacco addiction within the past 6 months is an absolutecontraindication to lung transplant [77]. Finally, pharmacoki-netics studies have revealed that both antifibrotics clear morerapidly in smokers vs. nonsmokers, resulting in lower exposureto the medications [51,54]. Thus, cigarette smoking should beavoided to prevent reduced exposure to antifibrotics.
2.4. Management of gastroesophageal reflux diseaseand other comorbidities
GERD is highly prevalent in patients with IPF, but only 25–50%of patients are symptomatic [78,79]. Chronic microaspirationsecondary to GERD may play a role in IPF pathogenesis andprogression and may trigger acute exacerbations [80–82].Antacid treatment has received a conditional recommendationin the 2015 update to the ATS/ERS/JRS/ALAT treatment guide-lines, but with very low confidence in estimates of effect [18].
A post hoc analysis of data from ASCEND and CAPACITYfound that patients receiving antacid therapy (histamine H2
blockers and/or proton pump inhibitors [PPIs]) and pirfeni-done had similar disease progression (absolute decline in %predicted FVC ≥10%, decline in 6MWD ≥50 m, or death) andall-cause mortality compared with those receiving pirfenidonewithout antacids; a similar analysis of the INPULSIS trials foundno additional benefit of antacids in combination with ninte-danib [83,84]. An analysis of the placebo groups of 3 IPFClinical Research Network clinical trials showed that patientsreceiving antacids had less decline in FVC (mL) and feweracute exacerbations at 30 weeks than those without antacids[85]. A study in patients with IPF from 2 US academic centersfound that antacids (88% of patients received PPIs) wereassociated with longer survival and decreased radiologic pul-monary fibrosis [80].
A recent meta-analysis reported that pharmacologic treat-ment of GERD is associated with a reduction in IPF-relatedmortality but not overall mortality [86]. However, the benefi-cial effects of antacids on mortality observed in patients withIPF in observational studies may be due to immortal time biasbecause in several studies, ≥12 months’ exposure to antacidswas required for inclusion in survival analysis; thus, patientshad a 12-month ‘immortal’ time period [86]. A separate meta-analysis found beneficial effects for antacids in 4 studies thatwere affected by immortal time bias but no beneficial effectsin 5 studies that avoided immortal time bias [87].
In summary, data suggest a beneficial role for antacids, PPIsin particular, in slowing disease progression and reducingmortality in patients with IPF, but the findings are inconsistent,highlighting a need for RCTs to clarify the role of antacids inIPF [85]. A recently published phase 2 trial of omeprazole in 45patients with IPF, which included patients who were receivingstable antifibrotics (≥4 weeks before enrollment), showeda reduction in cough in omeprazole-treated patients com-pared with placebo, but larger studies are needed to deter-mine the role of PPIs in other clinically relevant outcomes [88].The phase 2 WRAP-IPF trial of laparoscopic antireflux surgeryin patients with IPF demonstrated the safety of the procedure,but additional data are needed to determine if a clear benefitexists [89]. In addition to antacids, dietary changes, includingthe avoidance of heavy or fatty foods and the avoidance ofcaffeine and alcohol ≤3 hours before bedtime, and elevatingthe head of the bed 4–6 inches may be useful GERD manage-ment strategies in patients with IPF [85].
Several other key comorbidities require monitoring andmanagement in patients with IPF. Patients with IPF shouldbe evaluated for obstructive sleep apnea (OSA) because OSAis highly prevalent in the IPF population [90]. If OSA is present,continuous positive airway pressure therapy may improvenight-time oxygenation [91]. Coexisting chronic obstructivepulmonary disease (COPD) and emphysema in patients withIPF should be evaluated with pulmonary function tests andhigh-resolution computed tomography (HRCT), respectively;;although evidence for treatments is lacking, inhaled broncho-dilators could be considered if any of these conditions ispresent [92]. Pulmonary hypertension (PH) is common inpatients with more-advanced IPF and increases mortality risk;however, to date no therapies have been approved to treat PHin the IPF population [1,18,93,94]. A recent trial of nintedanibwith concomitant sildenafil in patients with advanced IPF(diffusing capacity for carbon monoxide [DLCO] ≤35%) didnot meet the primary endpoint of change in St. George’sRespiratory Questionnaire over 12 weeks, and a trial isongoing to evaluate pirfenidone with concomitant sildenafilin patients with advanced IPF (DLCO ≤40%) and risk of PH[95,96]. Lung cancer is more prevalent in patients with IPFthan in the general population, but treatment options arelacking [97,98]. Whether antifibrotics can be combined withchemotherapy or radiation therapy remains an open question,and patients with more-advanced IPF may not be eligible forsurgical resection, radiation therapy, or other treatments thatcan impair lung function [99,100].
2.5. Transplant referral
The 2011 ATS/ERS/JRS/ALAT and 2014 ISHLT treatment guidelinesstrongly recommend early lung transplant referral for patientswith IPF, so modifiable contraindications (e.g. obesity and decon-ditioning) can bemanaged accordingly despite the unpredictabil-ity of disease progression [1,77]. Patients must be appropriatelyeducated, with discussions starting at the time of diagnosis, aboutappropriate expectations, the realities of life posttransplant, andmanaging contraindications. Palliative care and opioids are nota barrier for transplant in most centers and should not be delayedif needed [101]. Similarly, prior use of antifibrotics has not been
606 O. MORAN-MENDOZA ET AL.

observed to compromise wound healing in patients undergoinglung transplant; therefore, patients who are listed for transplantcan receive antifibrotics [102]. Finally, when referred for transplant,patients should also be referred for PR and encouraged to exerciseregularly while awaiting a transplant evaluation to maintain asmuch physical function as possible.
The estimated 5-year survival rates after lung transplant forIPF are 50–56% [103]. One single-center study identified a 75%reduced risk of death at 5 years in 46 patients with IPF whohad lung transplants [104]. Many patients with IPF (14–67%)die after listing and before receiving a lung transplant due toshortage of donor organs [103].
2.6. Psychosocial support
Patients with IPF should be assessed for the presence ofanxiety and depression, as these conditions frequently occurduring IPF progression [19,20]. Offering counseling for bothpatients and caregivers, providing connections to individual orgroup support networks, and promoting overall well-being areall important when addressing a patient’s psychological dis-tress throughout their illness. These means of support areoptimally addressed by a multidisciplinary team. Medicationscan be prescribed as necessary, although RCTs in this patientpopulation are lacking: such as methylphenidate (to improveenergy and reduce fatigue); serotonin and norepinephrinereuptake inhibitors (for anxiety and depression); serotoninselective reuptake inhibitors (for depression); less commonlyused tricyclic antidepressants (for depression and sleep dis-turbances); bupropion (for depression); mirtazapine (fordepression, to improve appetite, sleep, and potentiallycough), which should be avoided in combination withCYP1A2 inhibitors and pirfenidone; benzodiazepines (use cau-tiously for anxiety or sleep); and buspirone (for sleep) [51,105].In addition to reducing the psychological burden of IPF, parti-cipation in patient support groups may improve adherence toantifibrotic therapy and other treatments [32]. Online supportgroups, such as the Pulmonary Fibrosis Foundation website(www.pulmonaryfibrosis.org), may benefit patients who havelimited mobility or live in rural areas. Patients and caregivershave also expressed the need for more community-basedmedical support, including at-home disease monitoring withmechanisms to identify decline and to respond appropriatelybefore the next clinic visit [28]. This can be facilitated throughcommunity support systems and working collaboratively tomonitor and support patients at home [106,107].
2.7. Updated vaccinations
Respiratory infections may trigger acute exacerbations of IPF[108]. Therefore, the vaccination status of patients should beassessed. No specific studies regarding vaccinations in patientswith IPF have been performed. The specific vaccination poli-cies and recommendations vary from country to countryregarding schedules for the annual influenza vaccination, 23-valent pneumococcal polysaccharide vaccine, and 13-valentpneumococcal vaccine based on a patient’s age and medicalhistory [109,110]. Clinicians should consult local guidelines.
2.8. Regular exercise/pulmonary rehabilitation
Per the 2011 ATS/ERS/JRS/ALAT treatment guidelines, PR shouldbe used in the majority of patients with IPF and encouragedimmediately after diagnosis before disease progression reducestheir functional status [1]. The goals of PR are to reduce dyspnea,depression, anxiety, and fatigue, leading to the benefits ofincreased exercise capacity, QoL, and cognitive function [111].
Several RCTs in patients with IPF or ILD have assessed thebenefits of PR. One study showed that 6MWD was significantlyimproved immediately following PR (+36 m, P = 0.0004) [112].Increased endurance and improved dyspnea during exertionwere reported when supplementary oxygen was provided topatients with IPF without resting hypoxemia [113]. A meta-analysis in patients with IPF found that PR had short-termbenefits in exercise capacity and health-related QoL but nodetectable effects at long-term follow-up (6–12 months) [114].In contrast, a recent RCT in 60 patients with ILD showedexercise and health benefits of a 6-month PR program per-sisted for an additional 6 months after completion [115].Continued PR is important for improving exercise capacity,particularly in patients waiting to receive a lung transplant.
Prior to initiating PR, the patient’s safety should be ensured[116]. An evaluation of baseline lung function and comorbiditiesshould be conducted, and before exercise initiation, a patient’ssupplemental oxygen supply should be assessed to confirm thatit is adequate. No specific guidelines for PR exist for IPF. Existingeducation and exercise programs for patients with COPD maynot be optimal for those with IPF [24]. Patients must be wellrested prior to exercise. Desaturation should be expected, soa supply of supplemental oxygen sufficient to maintain periph-eral capillary oxygen saturation (SaO2) ≥88% should be ensured.Before and after enrollment of patients in a PR program, encoura-ging patients to remain active by performing an aerobic exercisematching their interest and capability (e.g. walking, swimming,and cycling) is advised; however, it is important to assess theneed for supplemental oxygen during exertion.
2.9. Supplemental oxygen therapy
The 2011 ATS/ERS/JRS/ALAT treatment guidelines stronglyrecommend that patients with IPF with clinically significantresting hypoxemia should be treated with long-term oxygentherapy [1]. However, no data on long-term oxygen therapyare available in IPF; indirect evidence from COPD has demon-strated a survival benefit, and limited evidence has shown thatoxygen therapy improves exercise capacity in patients withresting hypoxemia and walk distance in patients with exer-tional hypoxemia [1]. Recently, the prospective, open-label,crossover-controlled AmbOx trial showed a benefit with sup-plemental oxygen in health-related QoL measures in patientswith ILD [117]. Therefore, prescribing supplemental oxygenand titrating to maintain SaO2 at ≥92–95% at rest and ≥88%during exertion is recommended. This value should berechecked every 60–90 days (or more frequently via self-monitoring), adjusting the supplemental oxygen as required.
Patients prescribed supplemental oxygen frequently lackadequate education about the effective use and availabilityof appropriate, ambulatory equipment [118]. The involvement
EXPERT REVIEW OF RESPIRATORY MEDICINE 607

of multiple stakeholders, including patient organizations, pro-fessional organizations, and industry partners, is needed toimprove oxygen access and use in the IPF population.Heterogeneity exists in supplemental oxygen use in clinicalpractice due to differences in policies around the world.Clinicians and ILD nurses should engage in patient educationto ensure both frequent monitoring of SaO2 and the availabil-ity of sufficient supply to meet the oxygen needs of eachindividual patient.
Patient-reported experiences of air travel with supplementaloxygen indicate that the experience can be challenging butmanageable with preparation [119]. In preparation for travel,a high-altitude simulation test should be performed to assessthe need for in-flight oxygen in patients who may not be fit tofly and in those with severe restrictive disease (vital capacity<1 L), advanced COPD (forced expiratory volume in 1 second<30%) especially with resting hypoxemia or hypercapnia, orpulmonary hypertension (New York Heart Association func-tional class III or IV) [120]. Patients deemed to require oxygenshould be instructed how to monitor and adjust the oxygenflow-rate to ensure that SaO2 is ≥90%% while in-flight [120,121].The patient should be advised to arrange oxygen supply logis-tics well in advance of the specific flight, inquiring about spe-cific supplemental oxygen policies with the airline andarranging for local oxygen supply at their destinations [120].
2.10. Symptom management and palliative care
An important component of symptom management is educat-ing patients about common symptoms that arise if diseaseprogression occurs and how they can best monitor theirsymptoms. Patients are more likely to engage in self-monitoring if they understand both why symptoms occurand what their role is managing them. Key symptoms todiscuss include breathlessness, fatigue, cough, anxiety, anddepression, plus it is important to ensure that patients under-stand their oxygen needs.
The goals of early integration of palliative care for patientswith IPF are to (1) establish regular monitoring and optimizesymptom management; (2) introduce appropriate medica-tions, such as opioids, with close monitoring and titration ofdose; (3) assist patients in understanding the trajectory of theillness; (4) engage in discussions about goals of care, includinglong-term goals and advance care planning; (5) facilitate tran-sitions from ambulatory and/or hospital-based care to home-based or hospice care as appropriate; (6) discuss end-of-lifecare expectations with the patient and family members and tomobilize resources close to home to support end-of-life care;(7) arrange transfer to alternate locations if optimal care provi-sion is not possible in the patient’s home; and (8) ultimatelyoptimize QoL as much as possible [22].
Physicians should consider implementing a palliative careapproach at the onset of symptoms of progressive respiratorydisease, concurrentl with curative or restorative care in anindividualized manner [105–107]. Preliminary evidence sug-gests a benefit of initiating palliative care early after an IPFdiagnosis because the disease is a progressive, life-limitingillness. Suggested criteria for referral to palliative care includea score of 4 or 5 on the Medical Research Council dyspnea
scale, the need for supplemental oxygen at rest or with exer-tion, increasing supportive care needs, and/or declining func-tional status (Palliative Performance Scale ≤50%) [105,122].
To provide effective palliative care, symptom managementneeds to be patient-centered and individualized [123].A systematic assessment of symptoms and patient needsmust lead to the prioritization of integrated symptom manage-ment and an understanding of the pathophysiology causingthe symptoms. Specific instructions for each medication pre-scription – dosing, timing, and route of administration, as wellas education about monitoring and managing medication AEs –should be provided to the patient according to the patient’sage and other comorbidities. Drugs that are ineffective orunnecessary for an individual patient should be discontinuedto limit polypharmacy. Changes in medications or doses shouldbe implemented one at a time, with frequent reassessments tomonitor the effect. Encouraging patients to keep a diary ofsymptoms, medication effectiveness, and AEs is also important.
For worsening dyspnea, there is no satisfactory treatment,but several options can be explored [105]. PR can instructpatients in techniques that may help manage dyspnea, andsupplemental oxygen use should be evaluated. Medicationssuch as low-dose opioids, methotrimeprazine, anxiolytics,mucolytics, and occasionally antibiotics can help somepatients, but direct evidence of efficacy in patients with IPFis lacking. For initial dyspnea management, we suggestimmediate-release morphine 2.5 mg (or 5 mg in patientswith high body mass index [BMI]) orally (PO) every 4 hours(q4h) while awake. Hydromorphone 0.5 mg (or 1 mg inpatients with high BMI) q4h while awake may be consideredif morphine should be avoided [106,107]. The opioid doseshould be titrated to the lowest effective dose that decreasesthe sensation of dyspnea and minimizes AEs. After the appro-priate dose has been determined, initiation of a controlled-released opioid could be considered for ease of administra-tion. If a patient is nearing the end of life, then immediate-release formulations are recommended to allow more rapiddose titration depending on the patient’s needs (titration after≥24 hours at a specific dose). In addition, it may becomenecessary to replace orally administered opioids with equipo-tent parenteral opioids (subcutaneous/intravenous) whenrapid symptom relief is needed or if patients can no longertake medications orally. Alternative therapies (e.g. relaxationtherapy, acupuncture, imagery) and a fan blowing cool airacross the face may help some patients control dyspnea [124].
For worsening cough, opioids are commonly prescribed[125]. Hydrocodone cough syrup is not more effective thanother opioids, so it should not be added to other opioid pre-scriptions. Systematic assessments should be performed toidentify and treat other etiologies of cough, such as sinusitis,GERD, and respiratory infections. Treatment could be initiatedwith a low dose of opioid with regular reassessment and titra-tion as needed. Inhaled corticosteroids or long-acting beta-agonists can be tried if concomitant asthma or COPD is present.
Common side effects from opioids include drowsiness andnausea, both of which are transient, typically resolving in4–6 days; constipation, which typically worsens with doseescalation; confusion and urinary retention, which are morefrequent in the elderly with comorbidities and polypharmacy.
608 O. MORAN-MENDOZA ET AL.

For opioid-induced nausea, metoclopramide 5 or 10 mg PO orhaloperidol 0.5 or 1 mg PO q4h as needed can be considered.Patients should be monitored for the development of opioid-induced constipation. A bowel routine should be initiatedconcurrently with the initiation and titration of opioids. Thefollowing regimens are suggested: senna glycoside 8.6 mg (2tablets) PO at bedtime, increased as needed (maximum 8tablets/day), or the total dose may be divided into BID dosing.Alternatively, polyethylene glycol 3350 at 8.5 g/day (one-halfcapful or one-half packet) or 17 g/day (1 capful, 1 packet, or≈1 heaping tablespoon) dissolved in 250 mL of liquid may beused and increased to BID if needed to ensure soft, easy-to-pass stool every 1–2 days.
2.11. IPF exacerbations
Acute worsening or the development of dyspnea, typicallyoccurring over the course of <30 days, may be an acuteexacerbation. IPF exacerbations are also characterized bynew bilateral ground glass opacities on HRCT, not fullyexplained by hydrostatic pulmonary edema (heart failure andfluid overload) [9]. Alternative diagnoses should be consideredin a patient with acute worsening dyspnea. In a patient witha history of smoking, emphysema, or chronic bronchitis,a COPD exacerbation should be considered if imaging studiesdo not show evidence of IPF exacerbation, because IPF canmask COPD in pulmonary function tests, due to the increasedelastic recoil of the lungs secondary to fibrosis, resulting inincreased airflows [9,126].
A chest x-ray can be used as an initial diagnostic test toeliminate differential diagnoses, such as atelectasis, pneumonia,pneumothorax, or congestive heart failure. If a patient’s chestx-ray is unchanged, a computed tomography pulmonary angio-gram (CTPA) should be considered to determine whether pul-monary embolism is present, provided renal function allowsadministration of the intravenous contrast required for CTPA[9]. The presence of ground glass opacities on CTPA or on chestHRCT would support the diagnosis of an IPF exacerbation.
IPF exacerbations are relatively uncommon (annual risk of5–15%), but have a very high short-term mortality (≈50%);therefore, the prevention, prompt diagnosis, and managementof IPF exacerbations are all very important [127]. Commonlyreported risk factors or triggers of IPF exacerbations includemore-advanced disease (low FVC or low DLCO), infections,GERD with microaspiration, air pollution, bronchoscopy, andsurgical procedures [9,108,128]. High pressures duringmechanical ventilation and high oxygen use during anesthesiahave been proposed as possible causes of alveolar injuryleading to an IPF exacerbation [9]. Therefore, if mechanicalventilation or anesthesia is required, judicious use of oxygenand low pressures is recommended. Other proposed preven-tive measures for IPF exacerbations are antacids, antifibrotics(to slow the IPF progression to advanced stages), and vaccina-tions against influenza and pneumococcus [127].
The management of IPF exacerbations typically includessupportive treatment, supplemental oxygen, and, despitevery limited evidence, systemic corticosteroids [1,94]. ThePANTHER-IPF trial found increased risk of mortality in patientsreceiving prednisone, azathioprine, and N-acetylcysteine, and
a single-center nonrandomized study of 24 patients with IPFwho experienced acute exacerbations found lower survival inthose who had previously received immunosuppressive ther-apy compared with those who had not [129,130]. Additionaldata are needed to evaluate the safety and efficacy of corti-costeroids and immunosuppressive therapy in patients whoexperience an IPF exacerbation [131].
We cautiously suggest initiating intravenous high-dose corti-costeroids (intravenous methylprednisolone 125–500 mg every12 hours) for 3 days followed by oral prednisone (50–100 mg/day) with a plan of tapering to discontinuation over 2–4 weeks.Oral methylprednisolone or dexamethasone might be consid-ered instead of prednisone, due to their lack of mineralocorti-coid effect, in patients with congestive heart failure, systemichypertension, or fluid retention (e.g. leg edema).
Small nonrandomized studies have reported associationsbetween other treatments and improved survival in patientswith IPF exacerbations; these treatments include preventiveantacids, cyclophosphamide, cyclosporine, tacrolimus, andcombined rituximab with plasma exchange and intravenousimmunoglobulin [9]. Initiation of empiric broad spectrum anti-biotics during IPF exacerbations is also routinely recom-mended by experts because bacterial infections are frequenttriggers of exacerbations and they are difficult to exclude incritically ill patients [132]. Whenever possible, sputum cultureand sensitivity should be ordered to guide antimicrobial ther-apy, especially in patients with suspected bacterial lowerrespiratory tract infection. Routine bronchoscopy in the clinicalassessment of acute respiratory failure in patients with ILD isnot indicated because diagnostic yield is low (13%), the pro-cedure is high risk in these patients, and it does not changemanagement approaches or in-hospital mortality [133].Supplemental oxygen, especially high-flow oxygen by nasalcannula or noninvasive ventilation, are recommended inpatients with IPF exacerbations to manage their dyspnea andhypoxemia [134]. Intubation and mechanical ventilation arenot recommended by the 2011 ATS/ERS/JRS/ALAT treatmentguidelines, based on the high rates of in-hospital mortality(90%) in these patients [1].
Patients with IPF should self-monitor for increased breath-lessness or fatigue, new or worsening cough, anxiety ordepression, and SaO2. A home pulse oximeter is an objectivemethod that patients can use to assess whether their worsen-ing dyspnea is due to hypoxemia, to determine the properflow-rate of oxygen at rest and during exertion, and to detectany increase in oxygen requirements. If a patient notices anychanges in symptoms, they should inform their physician orhome care nurse (if applicable) because the change couldindicate an acute exacerbation of IPF. Patients should seekimmediate medical attention for any sudden worsening ofdyspnea or increase in oxygen needs.
2.12. Nutrition
Both IPF itself and GI-related AEs associated with antifibrotictherapy can affect patients’ nutritional status, and their BMIshould be considered in many management decisions [63–65,135,136]. The needs for nutritional support to optimizecalories with protein and fat content varies in individual
EXPERT REVIEW OF RESPIRATORY MEDICINE 609

patients; both patients and their caregivers should be includedin discussions related to appropriate nutrition [136]. Dietarychanges may be needed to address obesity, which isa contraindication for lung transplant, or to control GERDsymptoms. Eating full meals can also help in the managementof gastrointestinal AEs associated with antifibrotic therapy,and dose reductions or interruptions should be consideredin patients with nausea or reduced appetite, with the knowl-edge that pirfenidone and nintedanib can maintain their effi-cacy at doses less than recommended [51,54,64,71]. In patientswith progressive weight loss due to nausea and reducedappetite despite antifibrotic dose reductions and the use ofPPIs and prokinetics (e.g. domperidone or metoclopramide),consider nutritional supplements (e.g. Ensure, Boost),a possible trial of oral cannabis where medical cannabis ispermitted, and referral to a dietician.
2.13. End-of-life preparations
End-of-life care should be discussed as early as possible toensure that patients and their families have the support theyneed to help the patient live as fully and comfortably as possi-ble [23,105]. This care can be provided in multiple settings,including a hospital, hospice facility, or the patient’s home.Documentation of a patient’s goals of care should includespecific information on their values, wishes, and beliefs; theirdesired level of medical interventions; the preferred site of caredelivery; and their life-support preferences. Documentationshould provide a clear understanding of a patient’s goals ofcare and should be communicated to the patient’s family, lovedones, and physicians. These are dynamic discussions thatshould begin early in the illness and continue throughout thecourse of the disease, especially at transition points, such assignificant worsening of pulmonary status or a decline in thepatient’s functional abilities. An interdisciplinary approach topalliative and end-of-life care is paramount and should includethe physicians, nurses, and social worker and could also includea spiritual health practitioner, volunteers, and counselors.
3. Conclusion
In summary, managing the care of a patient with IPF requiresa multifaceted approach that combines disease-specific stra-tegies for slowing disease progression and extending patientsurvival, simultaneously with palliative care to improve symp-tom management and QoL. This approach includes the follow-ing components: early initiation of antifibrotic therapy,assessment of physical and psychological needs, early inte-grated symptom management as part of a palliative careapproach, patient and caregiver education and support,open and often difficult communications, shared decision-making to facilitate time-sensitive decisions and advancecare planning, and ongoing reassessment of the patient’sgoals of care as the disease progresses. A patient’s preferencesand comorbidities should be considered prior to choosingantifibrotics, and TEAEs can be mitigated through educationand dose modifications. In addition to antifibrotics and inte-grated palliative care, PR, supplemental oxygen therapy, lungtransplant evaluation and referral, and advance care planning
should be established early in the disease course. ThroughoutIPF progression, oxygen requirements and the management ofdyspnea and cough need to be continually monitored. Theuse of opioids, antifibrotics, and a palliative care approach arenot barriers for lung transplant. Frequent communicationsshould occur with the patient and family to ensure theirunderstanding of the disease, treatment goals, and specificpatient goals and plans, particularly around end-of-life care.Finally, the importance of promoting collaborative practicebetween interdisciplinary team members needs to be high-lighted. Use of a multifaceted approach that targets all aspectsof IPF management throughout the course of the illness willensure that patients receive the most appropriate, compre-hensive, and patient-centered care possible.
4. Expert opinion
IPF management is complex: a multifaceted approach to man-agement that includes antifibrotic therapy, consideration ofreferral for lung transplant, treatment of comorbidities, pallia-tive care for symptom management, nutritional assessment,psychosocial support for patients, and caregiver support mayimprove QoL in patients with IPF. As new clinical trials areconducted to improve therapeutic options for patients withIPF and IPF-associated comorbidities, there is need forresearch to identify opportunities for improving and standar-dizing comprehensive care delivery in this patient population.A key challenge to achieving the goal of improved compre-hensive care is limited resources – both time and allied health-care providers – available to physicians who manage patientswith IPF within and outside of specialized centers. Here, wehighlight the need for multidisciplinary care to effectivelymanage this complex illness and to optimize patient survivaland QoL life. We hypothesize that the emergence of newpharmacological treatments and active research across thefields of pulmonology, nursing, palliative care, and lung trans-plantation will continue to lead to robust improvements insurvival and QoL in patients with IPF over the next decade.
Acknowledgments
The authors acknowledge Benjamin L. Ricca, PhD, of Health Interactions,Inc – third-party writing assistance funded by Hoffmann-La Roche Ltd.
Funding
This paper was sponsored by Hoffmann-La Roche Ltd.
Declaration of interest
Dr. Moran-Mendoza reports research funding, honoraria, clinical trial par-ticipation fees, and funding of editorial support from Hoffmann-La RocheLtd. and consultancy fees from Boehringer Ingelheim and Hoffmann-LaRoche Ltd. Dr. Colman reports honoraria from Boehringer Ingelheim andHoffmann-La Roche Ltd. and funding of editorial support from Hoffmann-La Roche Ltd. Meena Kalluri declares research funding, honoraria, clinicaltrial participation fees, and funding of editorial support from Hoffmann-LaRoche Ltd. and consultancy fees from Boehringer Ingelheim andHoffmann-La Roche Ltd. Dr Cabalteja is an employee of Hoffmann-LaRoche Ltd. Dr Harle reports funding of editorial support from Hoffmann-La Roche Ltd. The authors have no other relevant affiliations or financial
610 O. MORAN-MENDOZA ET AL.

involvement with any organization or entity with a financial interest in orfinancial conflict with the subject matter or materials discussed in themanuscript apart from those disclosed.
Reviewers Disclosure
Peer reviewers on this manuscript have no relevant financial relationshipsor otherwise to disclose.
References
Papers of special note have been highlighted as either of interest (•) or ofconsiderable interest (••) to readers.
1. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALATstatement: idiopathic pulmonary fibrosis: evidence-based guide-lines for diagnosis and management. Am J Respir Crit Care Med.2011;183(6):788–824.
2. Nicholson AG, Colby TV, Du Bois RM, et al. The prognostic signifi-cance of the histologic pattern of interstitial pneumonia in patientspresenting with the clinical entity of cryptogenic fibrosingalveolitis. Am J Respir Crit Care Med. 2000;162(6):2213–2217.
3. Flaherty KR, Toews GB, Travis WD, et al. Clinical significance ofhistological classification of idiopathic interstitial pneumonia. EurRespir J. 2002;19(2):275–283.
4. Ley B, Collard HR, King TE Jr. Clinical course and prediction ofsurvival in idiopathic pulmonary fibrosis. Am J Respir Crit CareMed. 2011;183(4):431–440.
5. Meltzer EB, Noble PW. Idiopathic pulmonary fibrosis. OrphanetJ Rare Dis. 2008;3:8.
6. Raghu G, Weycker D, Edelsberg J, et al. Incidence and prevalence ofidiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2006;174(7):810–816.
7. Daccord C, Maher TM. Recent advances in understanding idio-pathic pulmonary fibrosis. F1000Res. 2016;5:1046. eCollection 2016.
8. Collard HR, Moore BB, Flaherty KR, et al. Acute exacerbations ofidiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2007;176(7):636–643.
9. Collard HR, Ryerson CJ, Corte TJ, et al. Acute exacerbation ofidiopathic pulmonary fibrosis. an international working groupreport. Am J Respir Crit Care Med. 2016;194(3):265–275.
10. Collard HR, King TE Jr, Bartelson BB, et al. Changes in clinical andphysiologic variables predict survival in idiopathic pulmonaryfibrosis. Am J Respir Crit Care Med. 2003;168(5):538–542.
11. Flaherty KR, Mumford JA, Murray S, et al. Prognostic implications ofphysiologic and radiographic changes in idiopathic interstitialpneumonia. Am J Respir Crit Care Med. 2003;168(5):543–548.
12. Durheim MT, Collard HR, Roberts RS, et al. Association of hospitaladmission and forced vital capacity endpoints with survival in patientswith idiopathic pulmonary fibrosis: analysis of a pooled cohort fromthree clinical trials. Lancet Respir Med. 2015;3(5):388–396.
13. Paterniti MO, Bi Y, Rekic D, et al. Acute exacerbation and decline inforced vital capacity are associated with increased mortality inidiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2017;14(9):1395–1402.
14. Hook JL, Arcasoy SM, Zemmel D, et al. Titrated oxygen requirementand prognostication in idiopathic pulmonary fibrosis. Eur Respir J.2012;39(2):359–365.
15. Raghu G, Richeldi L. Current approaches to the management ofidiopathic pulmonary fibrosis. Respir Med. 2017;129:24–30.
16. Lederer DJ, Martinez FJ. Idiopathic pulmonary fibrosis. N EnglJ Med. 2018;378(19):1811–1823.
17. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathicpulmonary fibrosis. an official ATS/ERS/JRS/ALAT clinical practiceguideline. Am J Respir Crit Care Med. 2018;198(5):e44–e68.
• The new international guidelines on the diagnosis of IPFupdated the 2011 diagnostic guidelines
18. Raghu G, Rochwerg B, Zhang Y, et al. An official ATS/ERS/JRS/ALATclinical practice guideline: treatment of idiopathic pulmonary fibro-sis. an update of the 2011 clinical practice guideline. Am J RespirCrit Care Med. 2015;192(2):e3–e19.
• The 2011 international guidelines on the treatment of IPF wereupdated in 2015 after the approval of antifibrotic therapies
19. Akhtar AA, Ali MA, Smith RP. Depression in patients with idiopathicpulmonary fibrosis. Chron Respir Dis. 2013;10(3):127–133.
20. Ryerson CJ, Arean PA, Berkeley J, et al. Depression is a commonand chronic comorbidity in patients with interstitial lung disease.Respirology. 2012;17(3):525–532.
21. Kulkarni T, Willoughby J, Acosta Lara M, et al. A bundled careapproach to patients with idiopathic pulmonary fibrosis improvestransplant-free survival. Respir Med. 2016;115:33–38.
22. Kalluri M, Claveria F, Ainsley E, et al. Beyond idiopathic pulmonaryfibrosis diagnosis: multidisciplinary care with an early integratedpalliative approach is associated with a decrease in acute careutilization and hospital deaths. J Pain Symptom Manage. 2018;55(2):420–426.
•• This retrospective study found improved outcomes in patientswith IPF who received multidisciplinary care from a team includ-ing an ILD expert pulmonologist, a palliative care pulmonolo-gists, a nurse, a respiratory therapist, a physiotherapist, anda dietitian.
23. Pooler C, Richman-Eisenstat J, Kalluri M. Early integrated palliativeapproach for idiopathic pulmonary fibrosis: a narrative study ofbereaved caregivers’ experiences. Palliat Med. 2018;32(9):1455–1464.
24. Holland AE, Fiore JF Jr, Goh N, et al. Be honest and help me preparefor the future: what people with interstitial lung disease want fromeducation in pulmonary rehabilitation. Chron Respir Dis. 2015;12(2):93–101.
25. van Manen MJG, van ‘t Spijker A, Tak NC, et al. Patient and partnerempowerment programme for idiopathic pulmonary fibrosis. EurRespir J. 2017;49(4):1601596.
26. Senanayake S, Harrison K, Lewis M, et al. Patients’ experiences ofcoping with idiopathic pulmonary fibrosis and their recommenda-tions for its clinical management. PLoS One. 2018;13(5):e0197660.
• This patient survey highlighted the needs of patients and theirfamilies for additional education about IPF and how to makelifestyle changes that improve quality of life.
27. Fisher JH, O’Connor D, Flexman AM, et al. Accuracy and reliabilityof internet resources for information on idiopathic pulmonaryfibrosis. Am J Respir Crit Care Med. 2016;194(2):218–225.
28. Sampson C, Gill BH, Harrison NK, et al. The care needs of patients withidiopathic pulmonary fibrosis and their carers (CaNoPy): results ofa qualitative study. BMC Pulm Med. 2015;15:155.
29. Overgaard D, Kaldan G, Marsaa K, et al. The lived experience withidiopathic pulmonary fibrosis: a qualitative study. Eur Respir J.2016;47(5):1472–1480.
30. Bajwah S, Higginson IJ, Ross JR, et al. The palliative care needs forfibrotic interstitial lung disease: a qualitative study of patients,informal caregivers and health professionals. Palliat Med. 2013;27(9):869–876.
31. National Institute for Health and Care Excellence (NICE 2018).Idiopathic pulmonary fibrosis in adults: diagnosis and management(clinical guideline). London, UK: NICE; 2018.
32. Duck A, Pigram L, Errhalt P, et al. IPF care: a support program forpatients with idiopathic pulmonary fibrosis treated with pirfeni-done in europe. Adv Ther. 2015;32(2):87–107.
33. Chaudhuri N, Duck A, Frank R, et al. Real world experiences: pirfe-nidone is well tolerated in patients with idiopathic pulmonaryfibrosis. Respir Med. 2014;108(1):224–226.
34. King TE Jr, Bradford WZ, Castro-Bernardini S, et al. A phase 3 trial ofpirfenidone in patients with idiopathic pulmonary fibrosis. N EnglJ Med. 2014;370(22):2083–2092.
35. Richeldi L, Du Bois RM, Raghu G, et al. Efficacy and safety ofnintedanib in idiopathic pulmonary fibrosis. N Engl J Med.2014;370(22):2071–2082.
EXPERT REVIEW OF RESPIRATORY MEDICINE 611
36. Richeldi L, Costabel U, Selman M, et al. Efficacy of a tyrosine kinaseinhibitor in idiopathic pulmonary fibrosis. N Engl J Med. 2011;365(12):1079–1087.
37. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone in patients withidiopathic pulmonary fibrosis (CAPACITY): two randomised trials.Lancet. 2011;377(9779):1760–1769.
38. Nathan SD, Albera C, Bradford WZ, et al. Effect of pirfenidone onmortality: pooled analyses and meta-analyses of clinical trials inidiopathic pulmonary fibrosis. Lancet Respir Med. 2017;5(1):33–41.
39. Ley B, Swigris J, Day BM, et al. Pirfenidone reduces respiratory-relatedhospitalizations in idiopathic pulmonary fibrosis. Am J Respir Crit CareMed. 2017;196(6):756–761.
40. Richeldi L, Cottin V, Du Bois RM, et al. Nintedanib in patients withidiopathic pulmonary fibrosis: combined evidence from theTOMORROW and INPULSIS® trials. Respir Med. 2016;113:74–79.
41. Costabel U, Albera C, Lancaster LH, et al. An open-label study of thelong-term safety of pirfenidone in patients with idiopathic pulmon-ary fibrosis (RECAP). Respiration. 2017;94(5):408–415.
• This open-label extension study of 1058 patients with IPF whocompleted the phase 3 ASCEND or CAPACITY trials supportedthe long-term safety of pirfenidone
42. Crestani B, Huggins JT, Kaye M, et al. Long-term safety and toler-ability of nintedanib in patients with idiopathic pulmonary fibrosis:results from the open-label extension study, INPULSIS-ON. LancetRespir Med. 2019;7(1):60-68.
•• This open-label extension study of 734 patients with IPF whocompleted the phase 3 INPULSIS trials supported the long-term safety and efficacy of nintedanib
43. Albera C, Costabel U, Fagan EA, et al. Efficacy of pirfenidone inpatients with idiopathic pulmonary fibrosis with more preservedlung function. Eur Respir J. 2016;48(3):843–851.
44. Kolb M, Richeldi L, Behr J, et al. Nintedanib in patients with idio-pathic pulmonary fibrosis and preserved lung volume. Thorax.2017;72(4):340–346.
45. Wuyts WA, Kolb M, Stowasser S, et al. First data on efficacy andsafety of nintedanib in patients with idiopathic pulmonary fibrosisand forced vital capacity of ≤50% of predicted value. Lung.2016;194(5):739–743.
46. Costabel U, Albera C, Glassberg MK, et al. Effect of pirfenidone inpatients with more advanced idiopathic pulmonary fibrosis. RespirRes. 2019;20(1):55.
•• These post hoc analyses of data from an open-label long-termextension study found that pirfenidone’s efficacy with regardto slowing lung function decline was maintained over long-term treatment
47. Tzouvelekis A, Ntolios P, Karampitsakos T, et al. Safety and efficacyof pirfenidone in severe idiopathic pulmonary fibrosis: a real-worldobservational study. Pulm Pharmacol Ther. 2017;46:48–53.
48. Harari S, Caminati A, Poletti V, et al. A real-life multicenter nationalstudy on nintedanib in severe idiopathic pulmonary fibrosis.Respiration. 2018;95(6):433–440.
49. Nathan SD, Albera C, Bradford WZ, et al. Effect of continued treat-ment with pirfenidone following clinically meaningful declines inforced vital capacity: analysis of data from three phase 3 trials inpatients with idiopathic pulmonary fibrosis. Thorax. 2016;71(5):429–435.
50. Richeldi L, Kolb M, Azuma A, et al. FVC decline over 1 year predictsmortality but not subsequent FVC decline in patients with IPF. EurRespir J. 2017;50(suppl 61):PA4892.
51. Esbriet (pirfenidone) [monograph]. Mississauga, ON, Canada:F. Hoffmann-La Roche Ltd.; 2018.
52. Esbriet (pirfenidone) capsules and film-coated tablets, for oral use[package insert]. South San Francisco, CA: Genentech, Inc.; 2017.
53. Esbriet (pirfenidone) capsules and film-coated tablets, for oral use[summary of product characteristics]. Grenzach-Wyhlen, Germany:Roche Registration GmbH; 2017.
54. Ofev (nintedanib) [monograph]. Burlington, ON, Canada:Boehringer Ingelheim (Canada) Ltd..
55. Boehringer Ingelheim. Ofev (nintedanib) capsules, for oral use[package insert]. Ridgefield, CT; 2018.
56. Ofev (nintedanib) capsules, for oral use [summary of productcharacteristics] Ingelheim am Rhein, Germany: BoehringerIngelheim International GmbH; 2018.
57. Glassberg MK, Nathan SD, Lin CY, et al. Cardiovascular events inphase 3 trials of pirfenidone in idiopathic pulmonary fibrosis (IPF).Am J Respir Crit Care Med. 2016;193:A4980.
58. Noth I, Wijsenbeek M, Kolb M, et al. Cardiovascular safety of ninteda-nib in subgroups by cardiovascular risk at baseline in the TOMORROWand INPULSIS trials. Am J Respir Crit Care Med. 2017;195:A5383.
59. Pan L, Belloni P, Ding HT, et al. A pharmacokinetic bioequivalencestudy comparing pirfenidone tablet and capsule dosage forms inhealthy adult volunteers. Adv Ther. 2017;34(9):2071–2082.
60. King TE Jr, Pardo A, Selman M. Idiopathic pulmonary fibrosis.Lancet. 2011;378(9807):1949–1961.
61. Kondoh Y, Taniguchi H, Katsuta T, et al. Risk factors of acuteexacerbation of idiopathic pulmonary fibrosis. Sarcoidosis VascDiffuse Lung Dis. 2010;27(2):103–110.
62. Song JW, Hong SB, Lim CM, et al. Acute exacerbation of idiopathicpulmonary fibrosis: incidence, risk factors and outcome. Eur RespirJ. 2011;37(2):356–363.
63. Lancaster L, Morrison L, Auais A, et al. Safety of pirfenidone inpatients with idiopathic pulmonary fibrosis in a US expandedaccess program. Am J Respir Crit Care Med. 2016;193:A2695.
64. Lancaster LH, de Andrade JA, Zibrak JD, et al. Pirfenidone safetyand adverse event management in idiopathic pulmonary fibrosis.Eur Respir Rev. 2017;26(146):170057.
65. Cottin V. The safety and tolerability of nintedanib in the treatmentof idiopathic pulmonary fibrosis. Expert Opin Drug Saf. 2017;16(7):857–865.
66. Noble PW, Albera C, Bradford WZ, et al. Pirfenidone for idiopathicpulmonary fibrosis: analysis of pooled data from three multina-tional phase 3 trials. Eur Respir J. 2016;47(1):243–253.
67. Mason WR, Nathan SD, Zibrak JD, et al. Time-to-event analysis ofcommon adverse events with pirfenidone in patients with IPF—apooled analysis of three phase III clinical trials. Am J Respir Crit CareMed. 2017;195:A6798.
68. Hughes G, Toellner H, Morris H, et al. Real world experiences:pirfenidone and nintedanib are effective and well tolerated treat-ments for idiopathic pulmonary fibrosis. J Clin Med. 2016;5(9):78.
69. Galli JA, Pandya A, Vega-Olivo M, et al. Pirfenidone and nintedanibfor pulmonary fibrosis in clinical practice: tolerability and adversedrug reactions. Respirology. 2017;22(6):1171–1178.
70. Costabel U, Bendstrup E, Cottin V, et al. Pirfenidone in idiopathicpulmonary fibrosis: expert panel discussion on the management ofdrug-related adverse events. Adv Ther. 2014;31(4):375–391.
71. Corte T, Bonella F, Crestani B, et al. Safety, tolerability and appro-priate use of nintedanib in idiopathic pulmonary fibrosis. RespirRes. 2015;16:116-015-0276-5.
72. Cottin V, Maher T. Long-term clinical and real-world experiencewith pirfenidone in the treatment of idiopathic pulmonaryfibrosis. Eur Respir Rev. 2015;24(135):58–64.
73. Cottin V, Koschel D, Günther A, et al. Long-term safety of pirfeni-done: results of the prospective, observational PASSPORT study.ERJ Open Res. 2018;4(4):00084–2018.
74. Lancaster LH, Morrison L, Auais A, et al. Safety of pirfenidone inpatients with idiopathic pulmonary fibrosis: experience from 92sites in an open-label US expanded access program. Pulm Ther.2017;3:317.
75. Nathan SD, Lancaster LH, Albera C, et al. Dose modification anddose intensity during treatment with pirfenidone: analysis ofpooled data from three multinational phase III trials. BMJ OpenRespir Res. 2018;5(1):e000323.
• This post hoc analysis of phase 3 trial data found that patientsreceiving pirfenidone who underwent dose reductions andinterruptions maintained a relatively high dose of treatment,without compromising the treatment effect
76. Maher TM, Inoue Y, Case AH, et al. Effect of dose reductions and/orinterruptions on the efficacy of nintedanib in patients with idio-pathic pulmonary fibrosis (IPF): subgroup analysis of the INPULSIStrials. Am J Respir Crit Care Med. 2017;195:A5381.
612 O. MORAN-MENDOZA ET AL.

77. Weill D, Benden C, Corris PA, et al. A consensus document for theselection of lung transplant candidates: 2014—an update from thepulmonary transplantation council of the international society forheart and lung transplantation. J Heart Lung Transplant. 2015;34(1):1–15.
78. Raghu G, Freudenberger TD, Yang S, et al. High prevalence ofabnormal acid gastro-oesophageal reflux in idiopathic pulmonaryfibrosis. Eur Respir J. 2006;27(1):136–142.
79. Tobin RW, Pope CE 2nd, Pellegrini CA, et al. Increased prevalence ofgastroesophageal reflux in patients with idiopathic pulmonaryfibrosis. Am J Respir Crit Care Med. 1998;158(6):1804–1808.
80. Lee JS, Ryu JH, Elicker BM, et al. Gastroesophageal reflux therapy isassociated with longer survival in patients with idiopathic pulmon-ary fibrosis. Am J Respir Crit Care Med. 2011;184(12):1390–1394.
81. Ghebre YT, Raghu G. Idiopathic pulmonary fibrosis: novel conceptsof proton pump inhibitors as antifibrotic drugs. Am J Respir CritCare Med. 2016;193(12):1345–1352.
82. Johannson KA, Strambu I, Ravaglia C, et al. Antacid therapy inidiopathic pulmonary fibrosis: more questions than answers?Lancet Respir Med. 2017;5(7):591–598.
83. Kreuter M, Spagnolo P, Wuyts W, et al. Antacid therapy and diseaseprogression in patients with idiopathic pulmonary fibrosis whoreceived pirfenidone. Respiration. 2017;93(6):415–423.
84. Costabel U, Behr J, Crestani B, et al. Anti-acid therapy in idiopathicpulmonary fibrosis: insights from the INPULSIS trials. Respir Res.2018;19(1):167.
85. Lee JS, Collard HR, Anstrom KJ, et al. Anti-acid treatment anddisease progression in idiopathic pulmonary fibrosis: an analysisof data from three randomised controlled trials. Lancet Respir Med.2013;1(5):369–376.
86. Fidler L, Sitzer N, Shapera S, et al. Treatment of gastroesophagealreflux in patients with idiopathic pulmonary fibrosis: a systematicreview and meta-analysis. Chest. 2018;153(6):1405–1415.
87. Tran T, Suissa S. The effect of anti-acid therapy on survival inidiopathic pulmonary fibrosis: a methodological review of observa-tional studies. Eur Respir J. 2018;51(6):1800376.
• This review of observational studies of antacid therapy inpatients with IPF found that several studies indicatinga treatment benefit were affected by immortal time bias,strongly supporting a need for a randomized trial
88. Dutta P, Funston W, Mossop H, et al. Randomised, double-blind,placebo-controlled pilot trial of omeprazole in idiopathic pulmon-ary fibrosis. Thorax. 2019;74(4):346–353.
89. Raghu G, Pellegrini C, Yow ES, et al. A phase 2 randomized, con-trolled trial of laparoscopic anti-reflux surgery for the treatment ofidiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2018;197:A7698.
90. Lancaster LH, Mason WR, Parnell JA, et al. Obstructive sleep apneais common in idiopathic pulmonary fibrosis. Chest. 2009;136(3):772–778.
91. Mermigkis C, Bouloukaki I, Antoniou K, et al. Obstructive sleepapnea should be treated in patients with idiopathic pulmonaryfibrosis. Sleep Breath. 2015;19(1):385–391.
92. Cottin V. The impact of emphysema in pulmonary fibrosis. EurRespir Rev. 2013;22(128):153–157.
93. Lettieri CJ, Nathan SD, Barnett SD, et al. Prevalence and outcomesof pulmonary arterial hypertension in advanced idiopathic pulmon-ary fibrosis. Chest. 2006;129(3):746–752.
94. Alyami S, Yang R, Moran-Mendoza O. Idiopathic pulmonary fibrosismanagement review. SM J Biomed Eng. 2017;3(1):1018.
95. Kolb M, Raghu G, Wells AU, et al. Nintedanib plus sildenafil inpatients with idiopathic pulmonary fibrosis. N Engl J Med.2018;379(18):1722–1731.
• In this randomized controlled trial, a benefit in patient-reported overall health was not observed in patients with IPFwith more-advanced lung function decline treated with ninte-danib plus sildenafil vs. nintedanib plus placebo
96. Behr J, Nathan SD, Harari S, et al. Sildenafil added to pirfenidone inpatients with advanced idiopathic pulmonary fibrosis and risk ofpulmonary hypertension: a phase IIb, randomised, double-blind,
placebo-controlled study - rationale and study design. RespirMed. 2018;138:13–20.
• This ongoing phase 2b trial is investigating the efficacy ofpirfenidone plus sildenafil vs. pirfenidone plus placebo inpatients with IPF and risk of PH
97. Hubbard R, Venn A, Lewis S, et al. Lung cancer and cryptogenicfibrosing alveolitis. A population-based cohort study. Am J RespirCrit Care Med. 2000;161(1):5–8.
98. Le Jeune I, Gribbin J, West J, et al. The incidence of cancer inpatients with idiopathic pulmonary fibrosis and sarcoidosis in theUK. Respir Med. 2007;101(12):2534–2540.
99. Bargagli E, Bonti V, Ferrari K, et al. Lung cancer in patients withsevere idiopathic pulmonary fibrosis: critical aspects. In Vivo.2017;31(4):773–777.
100. Tzouvelekis A, Spagnolo P, Bonella F, et al. Patients with IPF andlung cancer: diagnosis and management. Lancet Respir Med.2018;6(2):86–88.
101. Colman R, Singer LG, Barua R, et al. Outcomes of lung transplantcandidates referred for co-management by palliative care:a retrospective case series. Palliat Med. 2015;29(5):429–435.
102. Leuschner G, Stocker F, Veit T, et al. Outcome of lung transplanta-tion in idiopathic pulmonary fibrosis with previous anti-fibrotictherapy. J Heart Lung Transplant. 2018;37(2):268–274.
103. Kistler KD, Nalysnyk L, Rotella P, et al. Lung transplantation inidiopathic pulmonary fibrosis: a systematic review of theliterature. BMC Pulm Med. 2014;14:139.
104. Thabut G, Mal H, Castier Y, et al. Survival benefit of lung transplan-tation for patients with idiopathic pulmonary fibrosis. J ThoracCardiovasc Surg. 2003;126(2):469–475.
105. Lanken PN, Terry PB, Delisser HM, et al. An official AmericanThoracic Society clinical policy statement: palliative care forpatients with respiratory diseases and critical illnesses. AmJ Respir Crit Care Med. 2008;177(8):912–927.
106. Kalluri M, Richman-Eisenstat J. Breathing is not an option; dyspneais. J Palliat Care. 2014;30(3):188.
107. Kalluri M, Richman-Eisenstat J. Early and integrated palliative careto achieve a home death in idiopathic pulmonary fibrosis. J PainSymptom Manage. 2017;53(6):1111–1115.
108. Moore BB, Moore TA. Viruses in idiopathic pulmonary fibrosis.Etiology and exacerbation. Ann Am Thorac Soc. 2015;12(Suppl 2):S186–92.
109. Public Health Agency of Canada. Canadian immunization guide.Ottawa, Canada: 2018. (update): https://www.canada.ca/en/public-health/services/canadian-immunization-guide.html. AccessedFebruary 11, 2019.
110. Tomczyk S, Bennett NM, Stoecker C, et al. Use of 13-valent pneu-mococcal conjugate vaccine and 23-valent pneumococcal polysac-charide vaccine among adults aged ≥65 years: recommendationsof the advisory committee on immunization practices (ACIP).MMWR Morb Mortal Wkly Rep. 2014;63(37):822–825.
111. Swigris JJ, Brown KK, Make BJ, et al. Pulmonary rehabilitation inidiopathic pulmonary fibrosis: a call for continued investigation.Respir Med. 2008;102(12):1675–1680.
112. Dowman L, Hill CJ, Holland AE. Pulmonary rehabilitation for inter-stitial lung disease. Cochrane Database Syst Rev. 2014;10:CD006322.
113. Dowman LM, McDonald CF, Bozinovski S, et al. Greater endurancecapacity and improved dyspnoea with acute oxygen supplementa-tion in idiopathic pulmonary fibrosis patients without restinghypoxaemia. Respirology. 2017;22(5):957–964.
114. Cheng L, Tan B, Yin Y, et al. Short- and long-term effects of pulmon-ary rehabilitation for idiopathic pulmonary fibrosis: a systematicreview and meta-analysis. Clin Rehabil. 2018;32(10):1299–1307.
115. Perez-Bogerd S, Wuyts W, Barbier V, et al. Short and long-termeffects of pulmonary rehabilitation in interstitial lung diseases:a randomised controlled trial. Respir Res. 2018;19(1):182.
• In this randomized controlled trial of 60 patients with ILD,a 6-month pulmonary rehabilitation program was associatedwith benefits in exercise capacity and health status 6 monthsafter the program ended
EXPERT REVIEW OF RESPIRATORY MEDICINE 613

116. Vainshelboim B, Fox BD, Oliveira J, et al. Exercise training inidiopathic pulmonary fibrosis. Expert Rev Respir Med. 2016;10(1):69–77.
117. Visca D, Mori L, Tsipouri V, et al. Effect of ambulatory oxygen onquality of life for patients with fibrotic lung disease (AmbOx):a prospective, open-label, mixed-method, crossover randomisedcontrolled trial. Lancet Respir Med. 2018;6(10):759–770.
• This open-label, mixed-method, crossover trial found that ambu-latory oxygen improved quality of life in patients with ILD
118. Jacobs SS, Lindell KO, Collins EG, et al. Patient perceptions of theadequacy of supplemental oxygen therapy. results of the AmericanThoracic Society nursing assembly oxygen working group survey.Ann Am Thorac Soc. 2018;15(1):24–32.
119. Campbell CD, Smyth MW, Brown L, et al. Air travel for subjectsreceiving long-term oxygen therapy. Respir Care. 2018;63(3):326–331.
120. Ahmedzai S, Balfour-Lynn IM, Bewick T, et al. Managing pas-sengers with stable respiratory disease planning air travel:British Thoracic Society recommendations. Thorax. 2011;66(Suppl 1):i1–i30.
121. Cramer D, Ward S, Geddes D. Assessment of oxygen supplementa-tion during air travel. Thorax. 1996;51(2):202–203.
122. Anderson F, Downing GM, Hill J, et al. Palliative performance scale(PPS): a new tool. J Palliat Care. 1996;12(1):5–11.
123. Lee JS, McLaughlin S, Collard HR. Comprehensive care of thepatient with idiopathic pulmonary fibrosis. Curr Opin Pulm Med.2011;17(5):348–354.
124. Kreuter M, Bendstrup E, Russell AM, et al. Palliative care in interstitiallung disease: living well. Lancet Respir Med. 2017;5(12):968–980.
125. Birring SS, Kavanagh JE, Irwin RS, et al. Treatment of interstitial lungdisease associated cough: CHEST guideline and expert panelreport. Chest. 2018;154(4):904–917.
126. Nava S, Rubini F. Lung and chest wall mechanics in ventilatedpatients with end stage idiopathic pulmonary fibrosis. Thorax.1999;54(5):390–395.
127. Richeldi L. Time for prevention of idiopathic pulmonary fibrosisexacerbation. Ann Am Thorac Soc. 2015;12(Suppl 2):S181–S185.
128. Winterbottom CJ, Shah RJ, Patterson KC, et al. Exposure to ambientparticulate matter is associated with accelerated functional declinein idiopathic pulmonary fibrosis. Chest. 2018;153(5):1221–1228.
129. Idiopathic Pulmonary Fibrosis Clinical Research Network, Raghu G,Anstrom KJ, King TE Jr, et al. Prednisone, azathioprine, andN-acetylcysteine for pulmonary fibrosis. N Engl J Med. 2012;366(21):1968–1977.
130. Papiris SA, Kagouridis K, Kolilekas L, et al. Survival in idiopathicpulmonary fibrosis acute exacerbations: the non-steroid approach.BMC Pulm Med. 2015;15:162.
131. Papiris SA, Kagouridis K, Kolilekas L, et al. Idiopathic pulmonaryfibrosis acute exacerbations: where are we now? Expert Rev RespirMed. 2014;8(3):271–273.
132. Ryerson CJ, Cottin V, Brown KK, et al. Acute exacerbation of idio-pathic pulmonary fibrosis: shifting the paradigm. Eur Respir J.2015;46(2):512–520.
133. Arcadu A, Moua T. Bronchoscopy assessment of acute respiratoryfailure in interstitial lung disease. Respirology. 2017;22(2):352–359.
134. Frat JP, Thille AW, Mercat A, et al. High-flow oxygen through nasalcannula in acute hypoxemic respiratory failure. N Engl J Med.2015;372(23):2185–2196.
135. Nouha A, Walid F, Rim M, et al. Assessment of nutritional status inpatients with idiopathic pulmonary fibrosis. Eur Respir J. 2016;48:PA3703.
136. Nguyen L, Morello Gearhart A, Cavallazzi R, et al. Nutrition therapyin end-stage lung disease. Curr Nutr Rep. 2017;6(3):291–298.
614 O. MORAN-MENDOZA ET AL.