a comparative study on the risk factors of musculoskeletal
TRANSCRIPT

89
A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
Golchin Shahijani
Faculty of Nursing and Midwifery
Isfahan University of Medical Sciences Hezar Jerib street, Isfahan, Iran 8174673461
Phone: +98 31 3792 3071
Mahnaz Shakerian
Department of Occupational Health
Shiraz University of Medical Science Central building of Shiraz University of Medical Sciences, Zand St., Shiraz, Iran
PO Box: 71348-14336
Ahmad Ghadami
Nursing and Midwifery Care Research Center, Faculty of Nursing and Midwifery
Isfahan University of Medical Sciences Hezar Jerib street, Isfahan, Iran 8174673461
Phone: +98 31 3792 3071 [email protected]
Abstract
Background: Musculoskeletal disorders are of the most important occupational injuries and
diseases, in which the work environment and individual activities play an essential role in their
prevalence. Since laparoscopy has become a preferred approach to treating many of the actions, the
aim of this study was to determine the risk factors of musculoskeletal disorders among laparoscopic
surgery technologists and comparing them between circulatory and scrubbing roles.
Materials and Methods: In this descriptive-analytical cross-sectional study, 49 participants
were evaluated by REBA method in Al-zahra Hospital, Isfahan, Iran, 2017. Data was collected
through REBA form and analyzed using SPSS software version 20. Results: 94% of our samples
were women mostly married with an age range of 32/17 years. The prevalence of musculoskeletal
disorders was 98.87% with a mean overall risk of 7.2 ± 0.75 in the role of circulatory and 5.31 ±
0.63 in the role of scrub.
Conclusion: Considering the fact that surgical technologists are at risk due to the nature of
their job and to promote their health, ergonomic interventions are critically suggested for
equipment, tools and environments as well as including ergonomics in their educational curriculum
and regular exercise programs.
Keywords: Musculoskeletal Disorders; Risk Factors, Postures; Laparoscopy; Circulatory
and Scrub.
1. Introduction
Laparoscopic techniques for minimally invasive surgery (MIS) are rapidly developing (Janki
et. al., 2017; Bartnicka et. al., 2013) so that it might have been considered as the first choice for
many surgeries such as cholecystectomy And has become a golden standard for removal of the
gallbladder (Janki et. al., 2017; Bartnicka et. al., 2018; Kramp et. al., 2014). Although there are many
advantages in laparoscopic procedures such as less pain after surgery, shorter recovery time and
better results for patients (Janki et. al., 2017; Bartnicka et. al., 2018; Choi et. al., 2018), they require
a fixed port position contributing to different awkward postures (El-Badry et. al., 2018) and certain
technical constraints (Sánchez-Margallo et. al., 2017). There may be ergonomic problems, therefore,

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
90
with techniques or tools (Bartnicka et. al., 2018). Among health workers, especially nurses, Work-
related Musculoskeletal Disorders (WMSDs) are a major global concern (Nur Azma et. al., 2016)
and the number of cases has risen since 1980 (Athena et. al., 2014). For example, the number of
WMSDs complaints in Taiwanese nurses, has gone up from 28.35% in 2006 to 33.65% in 2010
(Chung et. al., 2013). Also, based on the statistics, the reported complains among nurses who
experienced WMSDs symptoms at least in one region of their body were 88% in Malaysia, (Nur
Azma et. al., 2016), 48% in the United States (Zhang et. al., 2018), 85% in Saudi Arabia (Attar.,
2014), 66% in Switzerland (Nützi et. al., 2015), 80.8% in Africa 80.8% (Munabi et. al., 2014), 100%
in Iran (Zamanian et. al., 2017). The cost of these disorders is estimated about 4% of the world's
gross domestic product. For instance, back injuries among the operating room staff have caused
direct costs of $ 37,000 and indirect costs of $ 147,000 (King, 2011). In addition, ignoring the risk
factors and injuries of musculoskeletal disorders over time, it may result in increasing absenteeism,
medical expenses, pre-retirement, and reducing the working quality and productivity, as well as the
lack of workforce, abundant economic effects on individuals, organizations, and societies or even in
more severe cases the death of a person (Ballester Arias & García, 2017; Taghinejad et. al., 2015).
Therefore, by assessing the WMSDs risk factors, high risk tasks can be identified and it may be
possible to eliminate or reduce these risk factors through ergonomically designing the layout
(Choobineh et. al., 2013; Choobineh et. al., 2012), tools and equipment (Choobineh et. al., 2012)
contemporary with an organized educational intervention (Copenhaver et. al., 2017; Epstein et. al.,
2018) with the aim of adopting suitable work postures (El-Badry et. al., 2018; Abdollahzade et. al.,
2016), exercise (Stolt et. al., 2018; Heba et. al., 2018) aerobics and physical strength training (Szeto
et. al., 2013; Wang et. al., 2017) prevented the spread of it (Dana et. al., 2013; Wang et. al., 2017). As
previously mentioned, laparoscopic approach encompasses unique ergonomic challenges compared
to open surgery (Wang et. al., 2017). Although, some studies have shown a relationship between
laparoscopy and more musculoskeletal pain in surgeons (Dalager et. al., 2018; Choi, 2015), some
other studies like Wang Robert et. al. (2017) a reduction of ergonomic stress was observed in some
muscles among surgeons doing laparoscopic practice compared with that of open surgery (Wang et.
al., 2017). However, there is no detailed ergonomic information on the impact of this new
technology on the activities of surgical technologists during laparoscopic surgery since so far few
studies have been conducted specifically on these people, especially in the role of Circular. In the
surgical team, surgical technologists are only part of the team with two different roles of circulatory
and scrub among surgical operations. They in surgical procedures of most medical centers, the
surgical technologists would act as a circulatory, the interface between the surgical sterilization
team and the non-sterile environment (Choobineh et. al., 2010) and in the role of scrub, they act
simultaneously as scrubs and as the first assistant throughout the entire course of surgery which
means, ergonomically working in worse situation than even nursing.
So, Although new technology may yield credible advantages for surgical team like
improving patient surgery outcomes (Dalager et. al., 2017) or even reducing the risk of transmitting
biological agents; it is unclear in terms of ergonomics what impacts would have on the person with
the role(s) of the circulatory and/or scrub. Based on the mentioned points, the need for a study with
regard to the risk factors leading to WMSDs is felt among these people. Therefore, this study aimed
at comparing the WMSDs risk factors among laparoscopic surgery technologists with the two roles
of circular and scrubbing.
Laparoscopic History
Laparoscopy goes back to 1901 (Supe et. al., 2010), the first laparoscopy in Alzahra hospital,
however, dates back to 1995, firstly done by attend Thorax on laparoscopic cholecystectomy.
Today's other operations such as herniorrhaphy, bariatric, diagnostic laparoscopy,
hysterectomy, cystectomy, thymectomy, pulmonary, nephrectomy, and diagnostic Infertility have
also been developed. Cholecystectomy in the studied hospital is performed based on the American
method, i.e. the surgeon standing on the left side of the patient (Kramp et. al., 2014), through 4

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
91
separate ports with Trendelenburg reversal of the patient after pneumoperitoneum with an average
time of 103 minutes (from patient arrival to departure).
Ergonomic Problems
The advent of Minimal Invasive Surgery (MIS) has changed the environment of today's
operating rooms (Wasielewski et. al., 2017). These operating rooms, which are originally designed
for open surgical operations, are not responsive to large equipment used in laparoscopic devices.
Although the laparoscopic method has currently become a preferred approach to many practices, the
shortage of laparoscopic equipment is critically felt as in the 11 rooms where laparoscopic surgery
takes place; only 7 tray Carts exist containing laparoscopic equipment (monitor, insufflator, cold
light source, DVD and CCD drawer). These carts are, inevitably, kept outdoors and away from the
operating room contributing to personnel’s obligation to relocate, reconnect, and reassemble these
equipment for each operation. The 6 monitors available include one very low qualified 14 inch, two
ordinary 20 inch and four fairly good qualified flat monitors permanently located on the highest
floor of each card. The heights of the monitor center to the ground are 1640, 1665, 1680, 1750 mm
in the ordinary and flat ones, respectively. The CCD drawer is also placed on the lowest floorboard
with a height of 280 and 230, 470, 490 mm from the floor. despite open operations through which
only a pack and a set are required, laparoscopic cholecystectomy needs more widespread sets and
dishes Including at least one pack cloth (6900 kg) or disposable (approx. 200 g), a small set (2700
g) or a large general (3900 g) dish of homolog handhold (6200 g) laparoscopic dish (6200 g) dish
hook and lens (3900 g) and sometimes also dishes of advance (6900 g), the trocar dish (3600 g) and
the additional instrument dishes (6100 g). These dishes are also kept in the workroom at a height of
1880 mm from the ground floor and at 5 floors away from the main operating room.
Sets (small and general) and packs (fabric and disposable) are also located in the hall away
from the rooms and have the heights of 1040, 830 and 1150,230 mm from the floor, respectively,
(Figure 1).
Figure 1. Sets and packs are located in the hall away
The hospital surgical beds are of the two types of manual and automatic with the minimum
and maximum adjustable heights of 750- 970mm and 700-1000 mm, respectively, adjusted to the
surgeon.
The laparoscopic instrument used in cholecystectomy, including Scissor (length 470 and
455 mm), Clip applier (455, 460 and 470 mm), Grasper 470 mm, hook 355 mm, lens and CCD
altogether were (395+1353 = 530 mm) (Figure 2).

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
92
Figure 2. The laparoscopic instrument used in cholecystectomy
To use electro cautery and Ligasure for a dissection, cut and coagulate tissues, a foot pedal
should be placed on the floor where the surgeon is standing.
To make an appropriate lighting of the operation field, before and after using the camera,
the ceiling-connected siliatic lights are applied. Depending on the presence of one or two residents,
the scrub can be placed either on the left or right side of the patient. Since the monitor is adjusted to
be placed on the right side of the patient depending on the surgeon location, the distances between
the surgical technologist's eye to the center of the image on the right or left are 774 and 1372 mm,
respectively, and the average distance between the elbow of the scrub to the ground floor is 1005
mm. The minimum distance traveled by a surgical technologist in each operation include: 18
surgical room to a stoke Set and Pack 42 steps, patient admission 172steps, the pharmacy 118 steps,
workshop 148 steps, Recovery for sample delivery 282 steps, record patient profile in the book 20
steps and computer out of the room 32 steps, scrub sink 116 steps, computer in the room 10 steps,
set Sialtic light 12 steps, the cautery and the suction device 20 steps, Connect the serum 12 steps,
pouring formalin solution 22 steps and unpacking the inside of the commode each is 18 steps
2. Methods
2.1. Participants and Procedures
This study is descriptive analytical and cross-sectional performed after obtaining the code of
ethics from Isfahan University of Medical Sciences from March2017 to July 2018, at al-Zahra
Hospital ,Isfahan, Iran. A written consent was given to the participants to partook in the study for 5
months.
The study population included 57 (50 females and 7 males) of laparoscopic technologists in
the hospital voluntarily enrolled in the study. After considering inclusion criteria (participation in
laparoscopic cholecystectomy in scrub and circulatory roles, voluntary and satisfactory partaking in
the research, not having any musculoskeletal disorder and history of bone or joint surgery and no
pregnancy) and exclusion criteria(The participants dissatisfaction with continuing cooperation,
inactivity in the laparoscopic field, reluctance to take photos, leaving and death), 8 people were
excluded from the study and 49 people partook in this study to be evaluated at least 2 times and up
to 4 times(139 scrub role and 149 circular role).
2.2. Data Collection and Procedure
Initially, the researcher made a list of the most important tasks performed by the circular
[bringing pack and surgical sets, opening sterile instruments on the surgical table, pushing or
pulling equipment, attaching the delivery of scrub connectors to the corresponding devices(cautery
pen, cord, serum set , etc.), Delivery of instrumentation and materials to the surgical team (Cautery
Pedal and CCD), patient relocation] and scrub [delivering sterile instruments from the circulatory,

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
93
surgical table setup, pulling up the surgical table, helping the surgeon in the field of operation and
delivery of dirty tools used to operate the workroom] pre prepared.
In the following days, a two-part general Nordic questionnaire was used containing
demographic information (age, gender, weight, height, dominant hand, regular exercise, level of
education, work experience, marital status, ergonomic awareness, job satisfaction, visual
requirement, satisfaction from the monthly program and the operating room's agent).
The following tool were used to evaluate the persons:
REBA: An observational method validated and verifiable used to assess the health jobs
work statuses.
To evaluate the circulatory (by the researcher) and the scrub (by the occupational health
professional) in the tasks determined by rapid entire body assessment, with a digital camera Sony
HX1, One or more photos of each task are provided. Then the REBA checklist was scored; also,
force exertion rating score (less than 5 kg = 0, 10 kg = 1 and more than 10 kg = 2), hand pairing
with load score (load with proper handle = 0, acceptable with hand = 1, unacceptable with hand = 2
and load without handle with inappropriate postures = 3) and activity type (static or dynamic = 1)
were involved. Finally, the other person who did not know the details of the checklist for
interpretation in the course of the work and the research objectives entered the REBA software.
Score 1: negative level of risk that no corrective action is required. 2 to 3: low risk level, further
studies are required. 4 to 7: moderate level of risk and corrective action is required.
There are 8 to 10 levels of risk that corrective actions should be implemented in the near future. 11
to 15 levels are very high and immediate ergonomic action is required (Pazouki et. al., 2017).
2.3. Data Analysis
The research data were both quantitative (continuous and consecutive) and qualitative
(nominal) and were analyzed using SPSS 20 software. In order to determine the overall risk score of
musculoskeletal disorders in the role of scrub and circulatory, descriptive statistics (Mean, standard
deviation, percentage and frequency) was applied. For comparing the scores of the two tasks, paired
t-test was used. A repeated measure of variance analysis was applied to determine the average risk
score in each of the tasks by separating the circular and scrub roles (after assuring that the
assumption of sphere was determined by the Makhli test). Then, using the LFB test, two tasks were
compared. Finally, we used independent T-test to determine the distribution of musculoskeletal
disorders and the comparison of the mean overall risk score of circulatory and scrub.
3. Results
3.1. Sample Characteristics
Approximately 94% of the research population was women (46 women, 3 men). The
participants aged 23 to 48 years (mean 32.17±64.6) with mean height and weight was 163.8 and
61.8, respectively. Most of the participants were right-handed (83.7%) and job tenure ranged from
1 to 25 years (9.26± 6.2). 68.8 % of them were married and 79.6% had no regular exercise.
3.2. Working Postures
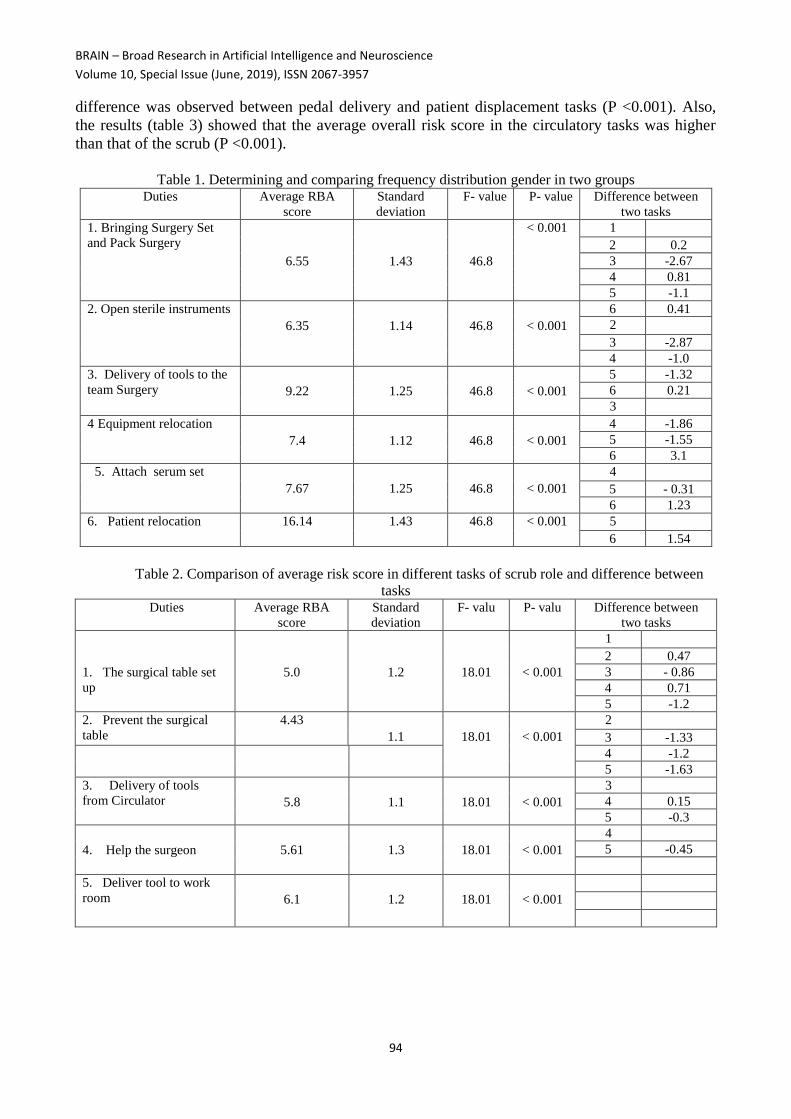
The average RBA score for all of the evaluated activities was obtained higher than 6 (Table 1).
Also, the task of the instrument delivery to the surgical team (foot pedal) had the highest
score of 9.29± 1.25 (P <0.001) and the task of patients transfer had the lowest score of 6.4± 1.43 (P
<0.001). Based on the score obtained from the scrub tasks shown in Table (2); It was found that the
RBA score was between 4 and 6. The lowest score for surgical operation was 4.3± 1.11 (P <0.001),
and the highest score for delivery of the surgical instrument used in the work room was 6.1 ± 1.2 (P
<0.001). Based on the results, (Tables 1 and 2), it was found that the average risk score was
significantly different between some tasks of circular and (P <0.001) in a way that the greatest
BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
94
difference was observed between pedal delivery and patient displacement tasks (P <0.001). Also,
the results (table 3) showed that the average overall risk score in the circulatory tasks was higher
than that of the scrub (P <0.001).
Table 1. Determining and comparing frequency distribution gender in two groups
Duties Average RBA
score Standard
deviation F- value P- value Difference between
two tasks 1. Bringing Surgery Set
and Pack Surgery
6.55
1.43
46.8
< 0.001 1 2 0.2 3 -2.67 4 0.81
5 -1.1 2. Open sterile instruments
6.35
1.14
46.8
< 0.001
6 0.41
2 3 -2.87 4 -1.0
3. Delivery of tools to the
team Surgery
9.22
1.25
46.8
< 0.001
5 -1.32 6 0.21
3 4 Equipment relocation
7.4
1.12
46.8
< 0.001
4 -1.86 5 -1.55 6 3.1
5. Attach serum set 7.67
1.25
46.8
< 0.001
4 5 - 0.31 6 1.23
6. Patient relocation 16.14 1.43 46.8 < 0.001 5 6 1.54
Table 2. Comparison of average risk score in different tasks of scrub role and difference between
tasks Duties Average RBA
score Standard
deviation F- valu P- valu Difference between
two tasks
1. The surgical table set
up
5.0
1.2
18.01
< 0.001
1 2 0.47 3 - 0.86 4 0.71
5 -1.2 2. Prevent the surgical
table 4.43
1.1
18.01
< 0.001
2 3 -1.33
4 -1.2
5 -1.63 3. Delivery of tools
from Circulator
5.8 1.1
18.01
< 0.001
3
4 0.15
5 -0.3
4. Help the surgeon
5.61
1.3
18.01
< 0.001
4
5 -0.45
5. Deliver tool to work
room
6.1
1.2
18.01
< 0.001
G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
95
Table 3. Level of risk and priority level of corrective actions based on REBA score in different tasks
4. Discussion The new method of laparoscopy threatens the ergonomic conditions of surgical technologists
working as circulator and scrub. Based on the results, the level of risk for Circulator role was
obtained medium and high in each of its tasks. Therefore, implementing ergonomic interventions as
well as corrective actions should be taken into account. In a study carried out by Murty et. al.
(2010) on 12 endoscopic nurses working in five different tasks, using method, and after 26
observations it was found that the scores related to the back and neck regions in each task were high
or very high among the participants (Murty et. al., 2010). In another study in 2017, 62 surgeons, first
assistant and scrubs were evaluated by the RUlA method, and it was found that during the surgery
almost 95% of people had ergonomic problems among which 37.1% were at high risk (Pazouki et.
al., 2017). In our study, the highest risk score of 9.22 was for those participants working with foot
pedal. The reason is that foot pedal is located on the floor requiring the person bending trunk and
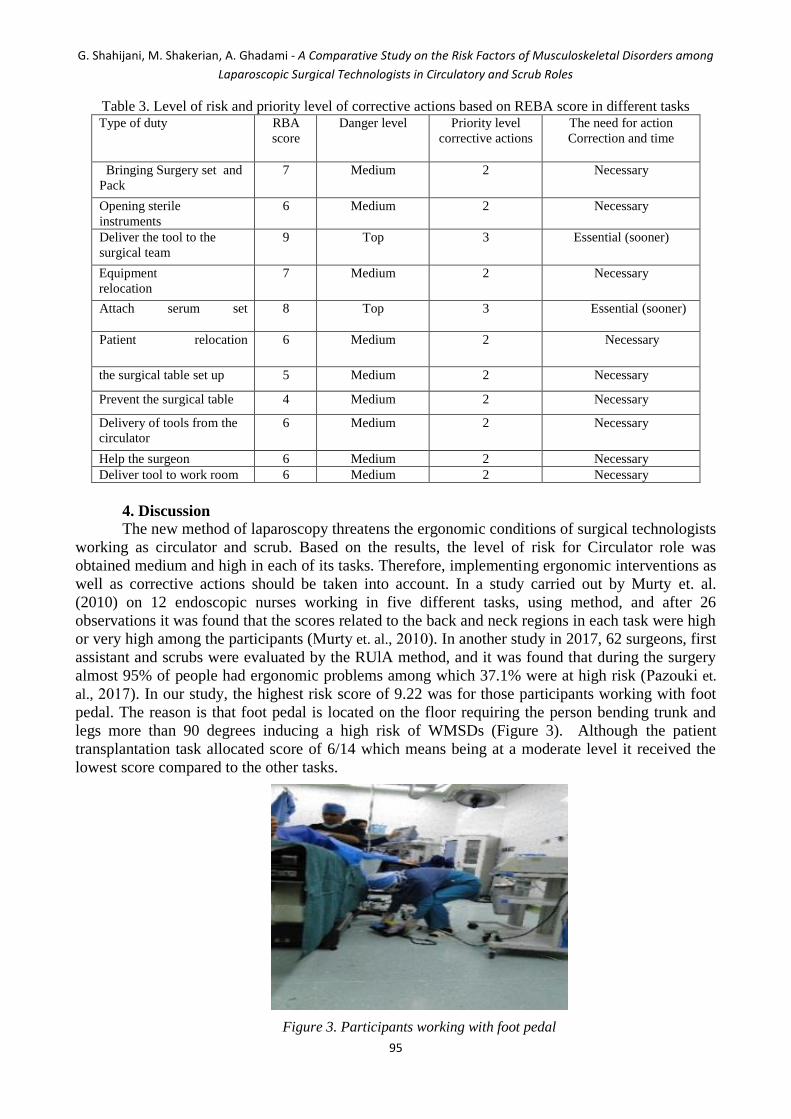
legs more than 90 degrees inducing a high risk of WMSDs (Figure 3). Although the patient
transplantation task allocated score of 6/14 which means being at a moderate level it received the
lowest score compared to the other tasks.
Figure 3. Participants working with foot pedal
Type of duty RBA
score
Danger level Priority level
corrective actions
The need for action
Correction and time
Bringing Surgery set and
Pack
7 Medium 2 Necessary
Opening sterile
instruments
6 Medium 2 Necessary
Deliver the tool to the
surgical team
9 Top 3 Essential (sooner)
Equipment
relocation
7 Medium 2 Necessary
Attach serum set
8 Top 3 Essential (sooner)
Patient relocation
6 Medium 2 Necessary
the surgical table set up 5 Medium 2 Necessary
Prevent the surgical table 4 Medium 2 Necessary
Delivery of tools from the
circulator
6 Medium 2 Necessary
Help the surgeon 6 Medium 2 Necessary
Deliver tool to work room 6 Medium 2 Necessary

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
96
When transferring, the greatest amount of force exertion is concentrated on patient
Transferor. Most of the time, circulator holds only the patient's legs with a relatively acceptable
posture. However, if the Circulator is positioned on the patient's side, the arms are bent up to 45 to
90 degrees forward and the trunk is also bent more than 60 degrees which impose a high level of
risk to the person (Figure 4).
Figure 4. Transferring, the greatest amount of force exertion is concentrated on patient Transferor
The average risk score difference between the two tasks of pedal delivery and patient’s
transferring was the highest (P <0.001).After pedal delivery, CCD used by surgery team had the
highest risk score as the CCD was placed at the bottom of the laparoscopic cart slot at less than 500
mm from the floor that required the participants awkward postures to do the task (Figure 5).
Figure 5. CCD used by surgery team
Serum attachment is also associated with a high level of high serum holder (7.67 grade) and
an unpleasant postures of extension and neck rotation, deviation to the front of the arm exceeds 90
degrees, shoulder height, rotation, and extension of 0 to 20 degrees of trunk (Figure 6).

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
97
Figure 6. Serum attachment is also associated with a high level of high serum holder
In front of the device, such as the setting of sialtic light (7/4 grade) Surgical technologist has
to raise more than 90 degrees of arm, Shoulder up, neck extension and the trunk and the unbalanced
position of the legs. This posture can be justified by the attachment of the light to the ceiling and its
height from the ground floor (Figure 7).
Figure 7. The setting of sialtic light
Figure 8. To remove cloth pack from the lower floor of the hallway

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
98
If using cloth pack (6900 g) the surgical technologist will have to remove it from the lower
floor of the hallway at an altitude of 230 mm from the floor which in this case faces a significant
change in posture (Figure 8).
The displacement of heavy dishes (6200 g) stored at high altitudes of the work room
encasement (1880 mm) is considered as one of the other ergonomic issues that the circulators were
encountered with (Figure 9).
Figure 9. The displacement of heavy dishes
Scrub was another role that the surgical technologist was responsible for. According to our
findings, the technologists in this role face a medium-risk (4-6) level. Abdullah Zadeh et. al. (2016) also
found similar results in his study so that the average score of RBA was 7.7 in three scrub activities
(Abdollahzade et. al., 2016). The greatest difference here was between the average risk scores obtained
for pulling the table and delivering the tool to the work room as the lowest score was related to the task
of pulling the surgery table. This finding can be due to the participants’ relatively better postures. In a
way that most participants try to approach tothe surgical bed (arm deviation forward up to 20 degrees)
with holding up trunk in a right posture (straight or bending 0 to 20 degrees) and sometimes slightly
bent (0 to 20 degrees) holding the hand in the middle of the table (no abduction of the arms before
surgery beginning. In this situation, the worst posture was observed in the wrist (abduction and
extensions up to 15 degrees). Noteworthy, sometimes the participants would approach to the table from
the side of the surgical bed requiring trunk to be twisted and bent 20 to 60 degrees, following by an
unbalanced position of the legs, abduction of the arms, an angle of less than 60 degrees for forearms and
the awkward posture of the wrists (Figure 10).
Figure 10. The displacement of heavy dishes

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
99
In the delivery of tools to the work room although the level of risk is moderate but the
highest score is (6/1). At the end of surgery the scrub should put the tool in the sink of the work
room. Since the height of these sinks is low individual puts inside the sink one single instrument on
the surgical table with a rotating posture and bending 20 to 60 degrees trunk, unbalanced position of
the legs, deviation 45 to 90 degrees of arm (Figure 11).
Figure 11. At the end of surgery the scrub should put the tool in the sink of the work room
In the help to the surgeon as well although the trunk is almost in perpendicular position but
with an average risk level (5.61), it encounters ergonomic problems. Janki also believes in
Laparoscopy the neck and back are in the vertical position and static state (Janki et. al., 2017). In the
process of tools delivery to the work room, although the level of risk was moderate, the highest
score was obtained (6/1). At the end of surgery, the scrub was responsible for putting the tool in the
sink of the work room. Since the height of these sinks is low for most of the individuals, they put
the devices one by one inside the sink with a rotating posture with a 20 to 60 degree trunk bending,
unbalanced position of the legs, and an arm deviation of 45 to 90 degree (Figure. 11). Also, when
helping to the surgeon although the trunk was almost in perpendicular position, the average risk
level was obtained relatively high (5.61) Janki also believed that in Laparoscopy process the neck
and back may be in the vertical position and static state (Janki et. al., 2017). This can be explained
by the fact that surgical technologists simultaneously play the both roles of scrub and first assistant.
Pazuki also pointed out this issue in his study (Pazouki et. al., 2017). In case of presence only one
resident or surgeon, the technologist had to use simultaneously both the right and left hands,
respectively, to keep and adjust the camera to accurately transfer the field of surgery image to the
monitor with an average time of 4380 seconds and maintaining and tension tightening the grasper
for a good exposure for bile bladder with an average time of 2640 seconds. This condition caused
the technologist to get an unpleasant static posture due to ports limit which would increase the range
of motion to degree 4 (Bartnicka et. al., 2013). The grasper held the right or left hand with tensing it
on the right side of the patient where the monitor was located. In this case, two inappropriate
ergonomic conditions occur including to reduce the distance to the monitor (mm770) and neck
rotation and extension (Figure 12).

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
100
Figure 12. Surgical technologists simultaneously play the both roles of scrub and first assistant
Previous studies also showed that if the monitor was not in the proper position, extension,
bending and static neck rotation may occur. To deliver the tool to the surgeon may mostly require a
worse posture. Holding the camera with a hand or grasper and availability of the device on the
Mayo table forced the participants to rotate, bend trunk up to 20 to 60, stretching and abduction of
the arms, unbalanced position of the legs and the neck rotation and extension (Figure 13).
Figure 13. To deliver the tool to the surgeon may mostly require a worse posture
Research Constraints
In this study, the participation of male surgical technologists was very small as a result, the
results cannot be safely attributed to the male society. One of the advantages of this research is the
evaluation of individuals in a completely real and alive surgical condition and the imaging of a
point that is visible to all the angles.
5. Conclusion
The study was conducted for concern about the rapid growth of laparoscopy and the lack of
knowledge of ergonomic conditions in surgical technologists. Polling data and observations indicate
that there is a real problem in this population with a high level of prevalence of disorders. The roles
of both roles raise people with a moderate level of risk. Perhaps this risk is more in the role of a
circulatory. As a result, some challenges require new engineering solutions in equipment, Tools and
environment, and integration of ergonomics in educational curriculum to adapt the working

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
101
conditions to the individual's abilities and characteristics with the aim of increasing the safety,
productivity and job satisfaction of the employees.
Acknowledgement
The present paper is drawn from one of the parts of the master's thesis of the operating room
approved by the code 396858 at Isfahan University of Medical Sciences. Hereby, I express my
gratitude the Nursing and Midwifery Faculty for its collaboration in the research. Also, I thank the
Isfahan University of Medical Sciences and the research office for cooperating and funding.
References
Abdollahzade F, Mohammadi F, Dianat I, Asghari E, Asghari-Jafarabadi M, Sokhanvar Z. (2016).
Working posture and its predictors in hospital operating room nurses. Health promotion
perspectives. 6(1):17.
Athena RP, Elnaz RP, Marzieh P. .(2014).the effect of ergonomic principles on reducing the risk of
musculoskeletal disorders RULA in computer users. Quarterly journal of Iranian ergonomics
and human factors engineering. 3(1):25-30. ] Persian [
Attar SM. .(2014). Frequency and risk factors of musculoskeletal pain in nurses at a tertiary centre
in Jeddah, Saudi Arabia: a cross sectional study. BMC research notes. 7(1):61.
Ballester Arias A, García A. .(2017). Asociación entre la exposición laboral a factores psicosociales
y la existencia de trastornos musculoesqueléticos en personal de enfermería: Revisión
sistemática y meta-análisis. Revista Española de Salud Pública. 91(1):e1-e27.
Bartnicka J, Ziętkiewicz A, Kowalski G. .(2013).Analysis of selected ergonomic problems in the
use of surgical laparoscopic tools. Zeszyty Naukowe/Akademia Morska w Szczecinie.34
(106):19--26.
Bartnicka J, Zietkiewicz AA, Kowalski GJ. .(2018). Ergonomic study on wrist posture when using
laparoscopic tools in four different techniques regarding minimally invasive surgery.
International Journal of Occupational Safety and Ergonomics. 24(3):438-449.
Choi SD. (2018). A review of the ergonomic issues in the laparoscopic operating room. Journal of
Healthcare Engineering. 3(4):587-6.
Choi, S.H. (2015). Re-examining the Dimensionality of Leisure Motivation and Leisure Satisfaction
in a Multicultural Context: Evidence from Macau. Humanities & Social Sciences Reviews,
3(1), 06-10.
Choobineh A, Daneshmandi H, Fallahpour A, Rahimi Fard H. .(2012). ergonomic evaluation of the
risk of musculoskeletal disorders in employees of a petrochemical company. Health of Iran,.
10(3):80-90] .persian [
Choobineh A, Movahed M, Tabatabaie SH, Kumashiro M. .(2010). Perceived demands and
musculoskeletal disorders in operating room nurses of Shiraz city hospitals. Industrial
health. 48(1):74-84.
Choobineh AR, Daneshmandi, HadiPourf, Fard R, Hoda. .(2013).Ergonomic Evaluation of the Risk
of Musculoskeletal Disorders in Employees of a Petrochemical Company. Iranian
Occupational Health Journal. 10 (3): 78-88.
Chung Y-C, Hung C-T, Li S-F, Lee H-M, Wang S-G, Chang S-C, et. al.(2013).Risk of
musculoskeletal disorder among Taiwanese nurses cohort: a nationwide population-based
study. BMC musculoskeletal disorders.14(1):144.
Copenhaver MS, Friend TH, Fitzgerald-Brown C, Fernandez M, Addesa M, Cassidy J.
(2017).Improving operating room and surgical instrumentation efficiency, safety, and
communication via the implementation of emergency laparoscopic cholecystectomy and
appendectomy conversion case carts. Perioperative Care and Operating Room Management.
8:33-7.

BRAIN – Broad Research in Artificial Intelligence and Neuroscience
Volume 10, Special Issue (June, 2019), ISSN 2067-3957
102
Dalager T, Jensen P, Winther T, Savarimuthu T, Markauskas A, Mogensen O, et. al. .(2018).
Surgeons’ muscle load during robotic-assisted laparoscopy performed with a regular office
chair and the preferred of two ergonomic chairs: A pilot study. Applied ergonomics.
Dalager T, Søgaard K, Bech KT, Mogensen O, Jensen PT. .(2017).Musculoskeletal pain among
surgeons performing minimally invasive surgery: a systematic review. Surgical endoscopy.
31(2):516-26.
Dana, A., Hamzeh A. (2013). The Relationship between Religiosity and Athletic Aggression in
Professional Athletes, UCT Journal of Social Sciences and Humanities Research, 4, 01-05.
El-Badry A, Allam H, Marawan H. .(2018). Neck and upper limb pain among gynecologists
working at menoufia governorate in egypt. Egyptian Journal of Occupational Medicine.
42(1):123-32.
Epstein S, Sparer EH, Tran BN, Ruan QZ, Dennerlein JT, Singhal D, et. al. .(2018).Prevalence of
Work-Related Musculoskeletal Disorders Among Surgeons and Interventionalists: A
Systematic Review and Meta-analysis. JAMA surgery. 153(2):e174947-e.
Heba Ali Hassan A, Eglal Hassanein A-H. .(2018).The Effect of Ergonomics Program on Nurses'
Knowledge and Practice in Operating Room. Journal of Nursing and Health Science ( IOSR-
JNHS). 7(1):6-15.
Janki S, Mulder EE, IJzermans JN, Tran TK. (2017).Ergonomics in the operating room. Surgical
endoscopy. (2017). 31(6):2457-66.
King CA. .(2011).Health care worker safety in surgery. AORN journal. 94(5):457-68.
Kramp KH, van Det MJ, Totte ER, Hoff C, Pierie J-PE.(2014). Ergonomic assessment of the French
and American position for laparoscopic cholecystectomy in the MIS Suite. Surgical
endoscopy.28 (5): 1571-8.
Munabi IG, Buwembo W, Kitara DL, Ochieng J, Mwaka ES. (2014). Musculoskeletal disorder risk
factors among nursing professionals in low resource settings: a cross-sectional study in
Uganda. BMC nursing. 13(1):7.
Murty M. (2010). Musculoskeletal disorders in endoscopy nursing. Gastroenterology
Nursing.;33(5):354-61.
Nur Azma B, Rusli B, Oxley J, Quek K.(2016).Work related musculoskeletal disorders in female
nursing personnel: prevalence and impact. International Journal of Collaborative Research
on Internal Medicine and Public Health. 8(3):294-98.
Nützi M, Koch P, Baur H, Elfering A. .(2015).Work–Family conflict, task interruptions, and
influence at work predict musculoskeletal pain in operating room nurses. Safety and health
at work. 6(4):329-37.
Pazouki A, Sadati L, Zarei F, Golchini E, Fruzesh R, Bakhtiary J.(2017).Ergonomic Challenges
Encountered by Laparoscopic Surgeons, Surgical First Assistants, and Operating Room
Nurses Involved in Minimally Invasive Surgeries by Using RULA Method. Journal of
Minimally Invasive Surgical Sciences. 6 (4).p:344-6
Sánchez-Margallo JA, Sánchez-Margallo FM.(2017).Initial experience using a robotic-driven
laparoscopic needle holder with ergonomic handle: assessment of surgeons’ task
performance and ergonomics. International journal of computer assisted radiology and
surgery. 12(12):2069-77.
Stolt M, Miikkola M, Suhonen R ,Leino-Kilpi H. .(2018).Nurses’ Perceptions of Their Foot Health:
Implications for Occupational Health Care. Workplace health & safety. 2018;66(3):136-43.
Supe AN, Kulkarni GV, Supe PA. .(2010).Ergonomics in laparoscopic surgery. Journal of minimal
access surgery. 6(2):31.
Szeto G, Wong T, Law R, Lee E, Lau T, So B,.(2013). The impact of a multifaceted ergonomic
intervention program on promoting occupational health in community nurses. Applied
ergonomics. 44(3):414-22.
Taghinejad H, Azadi A, Suhrabi Z, Sayedinia M. .(2015).Musculoskeletal disorders and their related
risk factors among iranian nurses. Biotechnology and Health Sciences. 3(1).

G. Shahijani, M. Shakerian, A. Ghadami - A Comparative Study on the Risk Factors of Musculoskeletal Disorders among
Laparoscopic Surgical Technologists in Circulatory and Scrub Roles
103
Wang R, Liang Z, Zihni AM, Ray S, Awad MM. .(2017).Which causes more ergonomic stress:
Laparoscopic or open surgery? Surgical endoscopy. 31(8):3286-90.
Wasielewski A.(2017). Guideline implementation: minimally invasive surgery, part 1 .AORN
journal.106(1):50-9.
Zamanian Z, Norouzi F, Esfandiari Z, Rahgosai M, Hasan F, Kohnavard B. .(2017). Assessment of
the prevalence of musculoskeletal disorders in nurses. Armaghane danesh. (10):976-86.
Zhang Y, Duffy JF, de Castillero ER, Wang K. .(2018). Chronotype, Sleep Characteristics, and
Musculoskeletal Disorders Among Hospital Nurses. Workplace health & safety;66(1):8-15.