a common ground theory of medical decision-making 1: the credo stack john fox department of...
TRANSCRIPT

A common ground theory of medical decision-making
1: The CREDO stack
John Fox Department of Engineering Science
University of Oxford and OpenClinical

Thanks to …
Psychologists, Informatics/CS/AI
• Andrew Coulson• Ioannis Chronakis • Subrata Das• David Glasspool• Omar Khan• Paul Krause• Simon Parsons• Mor Peleg• Ali Rahmanzadeh• Matt South• Rory Steele• Paul Taylor • Richard Thomson
Clinicians
• Alyssa Alabassi• John Bury• Robert Dunlop• John Emery• Marc Gutenstein • Andrzej Glowinski • Mike O’Neil• Vicky Monaghan• Vivek Patkar • Jean-Louis Renaud-Salis• Robert Walton• Matt Williams• Guy Wood-Gush

Summary
• Medicine is a rich and challenging domain for decision science and decision engineering
• It raises major challenges and curiously neglected questions at many levels– theory, technology, applications and more …
• The common ground theory aims to provide a general framework in which to– Promote discussion across disciplines– Clarify research questions and – Develop practical solutions
• The CREDO stack is a particular instance, but there are many others
The borders of the common ground
• “Prescriptive” (axiomatic, rational) theories– Lindley “there is only one correct way to take a decision”– EUT, Multicriteria DT, game theory, … and many ad hoc variants
• “Descriptive” (empirical, explanatory) theories– Cognitive (Nobel Laureates - Herbert Simon, Daniel Kahneman)– Neuroscience (neuroanatomy, neuropsychology, “hot cognition”)– Ecological (e.g. Gary Klein “naturalistic” theories)
• “Practical” (engineering, design) theories– Decisions are often framed and made with respect to standard practice– Decision systems may need to engage with accepted practice

Medical motivation:Quality and safety of patient care
• UK National health service– Vincent data on medical error in Acute Hospitals
• >10% acute hospital admissions in NHS lead to avoidable medical error
• US Institute of Medicine– IOM: “To err is human”; “Crossing the quality chasm”– McGlynn: Quality of Health Care Delivered to Adults in the
USA

Quality of Health in the USAMcGlynn NEJM 2003

The CREDO stack
Diversity of medical decisions
1. Screening for and classification of hazards; 2. Risk stratification and management;3. Selection of tests and investigations; 4. Diagnosing the cause(s) of clinical complaints; 5. Selecting treatments and other interventions; 6. Prescribing drugs (routes, dosages, polypharmacy etc.); 7. Referring patient to a colleague8. Deciding whether a decision is needed;9. Initiating, adjusting and stopping treatments; 10. Deciding whether earlier decisions are correct or not; if not
why not; adjust; reverse, reframe, retake;

Diversity of medical decisions
1. Screening for and classification of hazards; 2. Risk stratification and management;3. Selection of tests and investigations; 4. Diagnosing the cause(s) of clinical complaints; 5. Selecting treatments and other interventions; 6. Prescribing drugs (routes, dosages, polypharmacy etc.); 7. Referring patient to a colleague8. Deciding whether a decision is needed;9. Initiating, adjusting and stopping treatments; 10. Deciding whether earlier decisions are correct or not; if not
why not; adjust; reverse, reframe, retake;

MDM is reason based
Refer to specialist colleague if …
1. There is a possible life threatening condition 2. I don’t know what to do or lack sufficient knowledge3. The NICE clinical guideline says I should4. Patient is eligible for a research trial 5. Difficult patient, and I can’t resolve issue by myself6. Patient has asked to be referred7. Colleague or mentor has suggested I should …

MDM is dynamic
• Decision-makers must deal with changing and often unpredictable circumstances
• Decisions are not just choices, they are points in an evolving narrative (patient and professional)
• Common ground theory should address the whole cycle of decision-making: – When is a decision needed? what is the goal of the decision? – What knowledge and strategies are relevant? – When is it appropriate and safe to commit?– When is it necessary to revisit and revise commitments as the
situation evolves?

Example: cancer care

Example: cancer care


The CREDO stack

A common ground theory
From decision science to decision engineering: the CREDO stackResearchGate 2014
Beliefs
Commitments Plans
Goals
Options
Actions
Options Commitments
Beliefs
Plans
Goals Actions
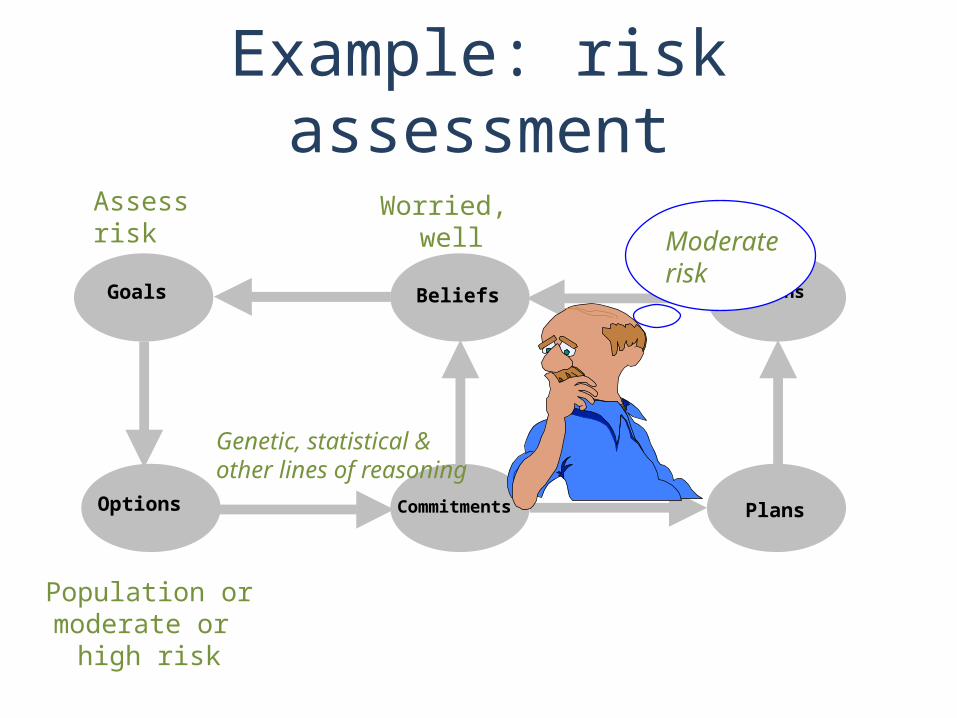
Example: risk assessment
Moderaterisk
Worried, well
Population ormoderate or
high risk
Genetic, statistical &other lines of reasoning
Assess risk

Example: test selection
tr
Options Commitments
Beliefs
Plans
Goals Actions
Pain, nodule
UltrasoundMammogram
CT etc.
Age, symptoms, …Family history
Mammogram, ultrasound
Investigate for possible
cancer Order Mammogram &ultrasound

Reasons and decisions
Argument construction
Knowledge U Data LA (Claim, Reason, Qualifier)
Argument aggregation
{(Claim, Reason, Qualifier)} Agg (Claim, Modality)
Fox et al ECAI, 1992; UAI 1994; Fox and Das, 2000Krause et al Computational Intelligence 1995

Uncertainty and arguments
• Quantitative [0,1] degree of belief (e.g. probability, possibility)[-1,+1] bipolar measures (e.g. belief functions){1,2,3,…n} ad hoc weighting of arguments
• Qualitative + “supporting” arguments{+,-} “supporting” and “opposing”
arguments{++,--, +, -} … plus “confirming” and “excluding”
• ModalLinguistic (perhaps, possible, probable, plausible …)

Formalising the common ground theory
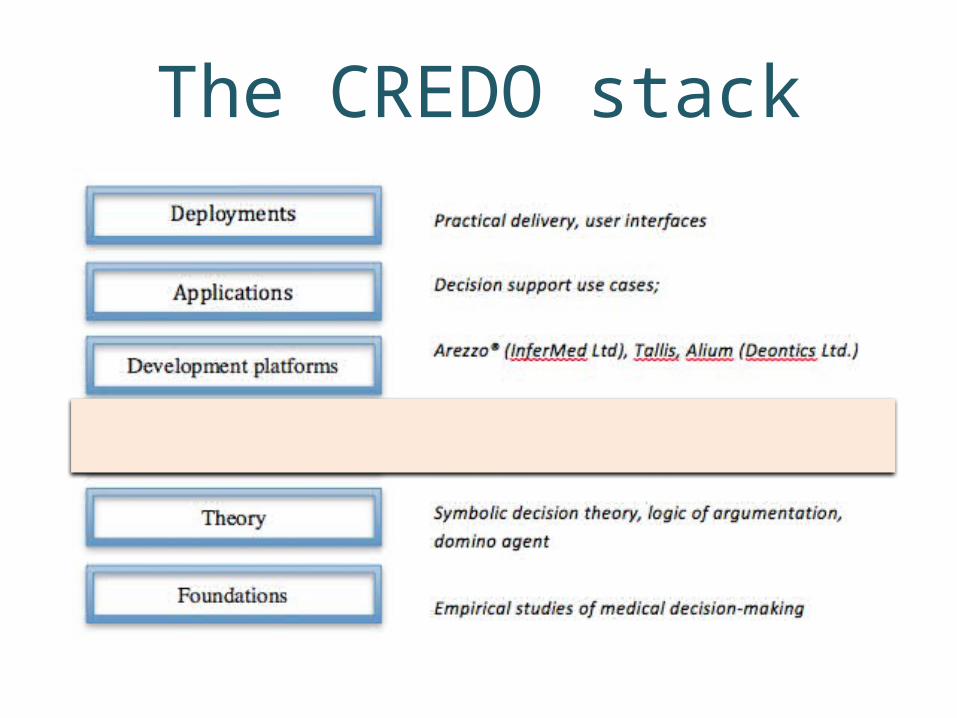
The CREDO stack

Concepts
Symbols
Descriptions
Rules
Decisions
Plans
Class hierarchies, semantic networksDiseases, Symptoms, Findings, Drugs
Medical facts, Clinical notes
Alerts, reminders, interpretations
Reasons (arguments, evidence, preferences)
Care pathways, workflows
Terminologies, coding systems
The knowledge ladderAgents Expert systems, Personal care agents

The CREDO stack

PROforma: Reification into “tasks”
Fox et al, MIE 1996; Fox and Das, AI in hazardous applications, MIT Press, 2000
PlanDecision
Enquiries Actions
Candidates Commitments
Beliefs
Plans
Goals Actions

Decision engineering

The CREDO stack

ApplicationsCare pathways in cardiology UPMC (USA), NHS (NZ) ,
NHS UK
Diagnosis and treatment in endocrine conditions (thyroid, diabetes)
AACE (USA)
Decision support for general practitioners BPAC (NZ)
Triage for common conditions NHS Choices (UK)
Supporting the breast MDT- Royal Free Hospital BASO 2008, ASCO 2009, BMJ Open, 2012
Triple assessment of suspected breast cancer Brit J Cancer 2006
Chemotherapy for children with acute lymphoblastic leukaemia
Brit J Haematology 2005
Planning care for women at risk of breast/ovarian cancer Methods of Information in Medicine 2004
GP referrals for common cancers MEDINFO 2003
Genotype of HIV+ patients interpretation and selection of anti-retrovirals (InferMed, Hoffman la Roche)
AIDS 2002
Genetic risk assessment BMJ 1999, 2000
Support for mammographic screening Medical Imaging 1999
Prescribing in general practice BMJ 1997

The CREDO stack

Decision support: human interaction
Summary
• Medicine is a challenging domain for– Understanding human error and expertise– Developing decision theory, empirical science and
engineering methods• It raises many important questions and some
strangely neglected ones– This will require contributions from many disciplines but
there is a high level of fragmentation in decision science• The “domino” is a first draft of a common ground
theory, to promote interdisciplinary discussion• The CREDO stack validates the theory to a first
approximation demonstrates its practical value