a collaboration led by. interact2: protocol reduced number of in-hospital assessments but includes...
TRANSCRIPT

A collaboration led by

INTERACT2:Protocol

Reduced number of in-hospital assessments but includes and assessment of ICU stay and use of renal dialysis
Repeat 24 hr CT scan to be collected only in 600 patients (300 Chinese and 300 non-Chinese)
Option of telephone-based outcome assessments at 28 and 90 days
Screening logs kept for only 1 month of the year sites to be notified of the randomly selected
month in advance. Use of an Interactive Voice Randomisation System
(IVRS) in China
INTERACT2: New design features

INTERACT2 BP Management
Evaluation of a management policy and NOT of a single agent
Inclusion of BP lowering management protocols for key available agents
Pragmatic approach to treatment Agents readily available in hospitals Agents approved for clinical use Lower study costs

Study Outline
Acute spontaneous ICHonset <6 hours
SBP ≥150 and ≤220 mmHgNo definite indications or contraindications to treatment
Able to be actively managedProvide informed consent
Repeat CT scans 24 hrs in selected patients
Vital signs and BP over 7 days28 day and 3 month follow-up
Intensive BP loweringTarget systolic BP 140 mmHg within 1 hour and for 24+ hrs
Conservative BP managementAHA Guideline-based
(treatment if systolic BP >180 mmHg)
R
Standard best
practice stroke
unit care

Sample Size
2800 patients from 140+ sites 90% power for:
14% RRR in death/dependency in active vs control
20% RRR in (50%) randomised <4 hours

Network
Australia14 centres
China49 centres
India /Pakistan
13 centres
USA (Rochester)
1 centre
Chile6 centres
Argentina6 centres
Brazil9 centres
EuropeAustria, Finland, France,
Germany, Portugal, Spain, Switzerland, The Netherlands,
Italy, Poland
64 centres
UK27
centres

Inclusion Criteria
Age 18 years or above Acute spontaneous ICH (history and CT) At least two systolic BP 150-220 mmHg,
recorded ≥2 min apart Able to be randomly assigned BP lowering
therapy within 6 hours of stroke onset Able to receive active (‘intensive’) care in a
monitored facility

Exclusion Criteria
Known definite contraindication to intensive BP lowering
Known definite indication to intensive BP lowering
ICH secondary to a structural abnormality Ischemic stroke in last 30 days High likelihood of death within 24 hours
(GCS 3-5)

Exclusion Criteria (cont.)
Known advanced dementia or significant pre-stroke disability
Concomitant medical illness
Planned early surgical intervention
Participation in other trial
Unlikely to adhere to treatment or follow-up

Eligibility
To be eligible for INTERACT2:
All inclusion criteria questions must be answered “YES”
All exclusion criteria questions must be answered as “NO”

Randomisation system
Patients are stratified according to: time since stroke onset (0-4 vs. 4-6 hours), site and country of recruitment
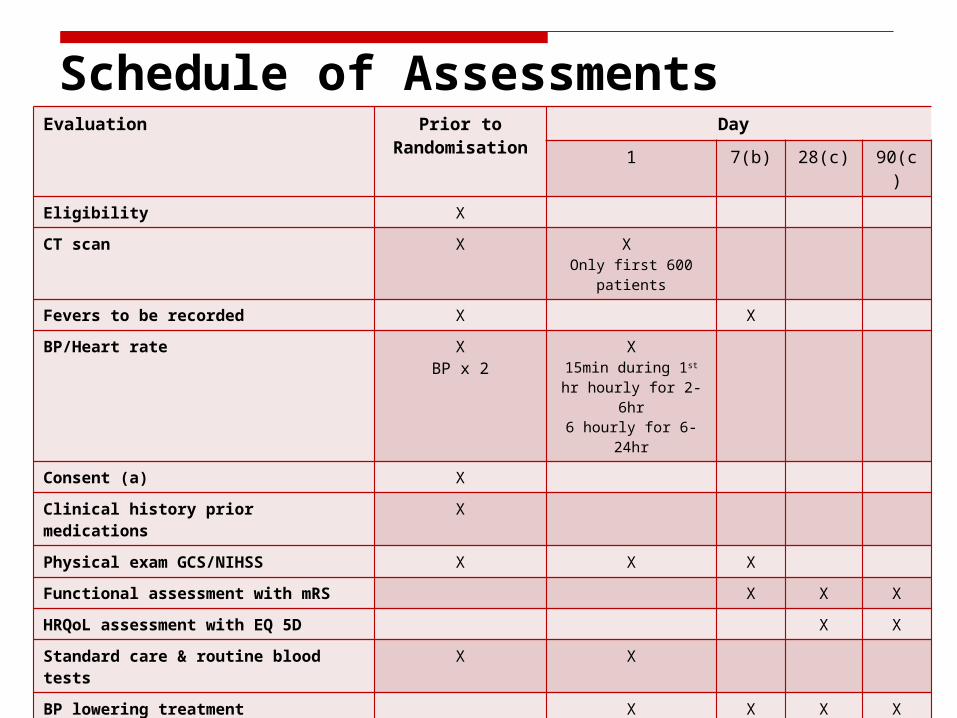
Schedule of AssessmentsEvaluation Prior to
RandomisationDay
1 7(b) 28(c) 90(c)
Eligibility X
CT scan X X Only first 600
patients
Fevers to be recorded X X
BP/Heart rate XBP x 2
X15min during 1st hr
hourly for 2-6hr6 hourly for 6-24hr
Consent (a) X
Clinical history prior medications X
Physical exam GCS/NIHSS X X X
Functional assessment with mRS X X X
HRQoL assessment with EQ 5D X X
Standard care & routine blood tests
X X
BP lowering treatment X X X X
Standard stroke care X X X X
Hospitalised or not X X X X
Contact details for Follow-Up X X

Outcomes
Primary – composite of death or dependency (ie score 3–5 on the modified Rankin Scale [mRS]) at 90 days
Secondary: Key – primary endpoint in patients <4 hrs of ICH onset Others
Death Dependency; Disability on the mRS HRQoL (using the EuroQoL and health utility score EQ5D) Recurrent stroke after 24 hrs of initial ICH Other major CV events (myocardial infarction or sudden death) Need for permanent residential care Duration of initial hospitalisation.

Summary
INTERACT2 has been designed to provide a definitive answer to the management of elevated BP in patients with acute ICH
If successful, thousands of patients could benefit, with associated major health gains

Acknowledgements
Patients and families Participating hospitals and staff Many project staff in multiple countries Funding:
National Health and Medical Research Council of Australia
The George Institute for Global Health
Acknowledgements
Executive committee: Craig Anderson (Principal Investigator), John Chalmers (Chair), Hisatomi Arima, Stephen Davis, Emma Heeley, Yining Huang, Richard Lindley, Bruce Neal, Mark Parsons, Christian Stapf, Christophe Tzourio and Jiguang Wang.China steering committee: Yining Huang, Jiguang Wang, Liying Cui, Shengdi Chen, Zhenguo Liu, Chuanzhen Lu, Qidong Yang, En Xu, Jingfen Zhang, Chaodong Zhang, Shizheng Wu and Xining Yan ChenEuropean advisory board: Austria – Ronny Beer, Erich Schmutzhard; Belgium – Patricia Redondo; Finland – Markku Kaste, Lauri Soinne, Turgut Tatlisumak; France – Christian Stapf, Christophe Tzourio, Eric Vicaut; Germany – Katja Wartenberg; Italy – Stefano Ricci; Netherlands – Karin Klijn; Portugal – Jose´ Ferro; Spain – Angel Chamorro; Switzerland – Marcel Arnold, Urs Fischer; UK – Tom Robinson.Operations committee: Emma Heeley, Candice Delcourt.International coordinators: Michelle Leroux, Tara Sasse, Jun Hata, Gouyjen, Tina Cheung, Cathy Boreham, Sarah Leighton. Regional coordinators: Americas – Alejandro Rabinstein; Argentina – Conrado J. Estol, Mariana Zimmermann; Brazil – Gisele Silva, Joyce Marinho; Chile – Pablo Lavados; China – Jian Sun, Nan Li, Zhao Yan, Chen Xiaoying; France – Sofiane Kabla, Cecile Dert; India –K Mallickarjuna, Najam Hassan, Jeyaraj Pandian.DSMB members: John Simes (Chair), Marie-Germaine Bousser, Graeme Hankey, Konrad Jamrozik (deceased in 2010), Claiborne Johnston and Li Shunwei.Statisticians: Laurent Billot, Stephane Heritier and Qiang Li.