a clinical study on the utility of nerve biopsy in peripheral...
TRANSCRIPT

i
A CLINICAL STUDY ON THE UTILITY OF NERVE
BIOPSY IN PERIPHERAL NEUROPATHY
Thesis submitted for the partial fulfilment for the requirement of
the degree of DM Neurology
DR. JITESH GOEL
DM NEUROLOGY RESIDENT
2014–2016
DEPARTMENT OF NEUROLOGY
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL
SCIENCES AND TECHNOLOGY, TRIVANDRUM, KERALA 695011

ii
DECLARATION
I, Dr Jitesh hereby declare that the thesis “A CLINICAL STUDY ON THE UTILITY OF
NERVE BIOPSY IN PERIPHERAL NEUROPATHY” was undertaken by me under the
guidance and supervision of Dr MD Nair, Senior Professor and Head of Department,
Department of Neurology at the Sree Chitra Tirunal Institute for Medical Sciences and
Technology, Thiruvananthapuram.
Dr.Jitesh Goel
Thiruvananthapuram Senior Resident
Date: Dept. of Neurology
SCTIMST
Thiruvananthapuram

iii
CERTIFICATE
This is to certify that the thesis titled “A CLINICAL STUDY ON THE UTILITY OF NERVE
BIOPSY IN PERIPHERAL NEUROPATHY”, is the bonafide work of Dr Jitesh Goel, Senior
Resident, DM Neurology and has been done under my direct guidance and supervision
at the Sree Chitra Tirunal Institute for Medical Sciences and Technology,
Thiruvananthapuram. He has shown keen interest in the research project and actively
participated in all its phases.
Thiruvananthapuram Dr MD Nair (Guide)
Date: Senior Professor and Head of Department
Department of Neurology,
SCTIMST. Thiruvananthapuram

iv
CONTENTS
Sl. No. Title Page No.
1 Introduction 1
2 Review of Literature 3
3 Aim of The Study 32
4 Materials And Methods 32
5 Results 34
6 Discussion 62
7 Conclusion 72
8 References 75
9 Annexures 84
IEC Approval
Proforma

1
INTRODUCTION
Peripheral neuropathy is among the common disorders in patients attending
neuromuscular clinic. Systematic approach comprising a comprehensive clinical
history, thorough neurological and systemic examination, nerve conduction studies,
EMG and relevant biochemical tests should be undertaken in all cases.
Nerve biopsy is indicated with a strong suspicion of disorders, like amyloidosis,
vasculitis, leprosy, and tumor infiltration. Nerve biopsy is useful for atypical
presentations of CIDP, and is helpful in exclusion of other etiologies. The yield of nerve
biopsy result is dependent on number of factors, including appropriate selection of
patients for biopsy, expertise of the laboratory, and techniques used in the analysis.
A prospective study by Gabriel etal has shown altered management in nearly 60 % of
cases after nerve biopsy, and nerve biopsy was more diagnostic in severe
demyelinating, distal asymmetric, and multifocal type of neuropathy 1, similar results
have been shown in another retrospective study 2. The yield of nerve biopsy in
vasculitic neuropathy is around 20 %, as observed in some other studies 3,4.
Combined nerve and muscle biopsy has shown improved yield in vasculitic neuropathy,
due to the more frequent involvement of the peroneal nerve and the involvement of
muscular arteries in vasculitis neuropathy. Higher yield in vasculitis neuropathy has
2
been shown to be useful by performing a biopsy of the superficial peroneal nerve
combined with a peroneus brevis muscle biopsy, confirmed in a multicenter
prospective study5. Nerve biopsy is more contributive in the diagnosis in multifocal
neuropathy than in the other patterns of neuropathy.

3
REVIEW OF LITERATURE
In a community-based study conducted in Bangalore, the age adjusted prevalence rate
of neuropathy in population was found to be 0.067 % 6, and in another study
conducted in Parsi community in Bombay, prevalence rate was found to 2.3 % 7.
Prevalence of peripheral neuropathy in Community based surveys in Italy have been
reported between 1-3% 8. In the Italian field screen study for distal symmetrical
polyneuropathy, out of 4191 subjects aged more than 55 years, 888 patients had
peripheral neuropathy and of these nearly 47.3 % of patients had diabetes mellitus.
Detailed analysis revealed a prevalence of distal symmetric polyneuropathy to be 3.3
– 3.6 per 100 population. Most common symptoms reported by these patients were
distal paraesthesias and muscle cramps. Most common signs reported were impaired
reflexes and impaired sensations9.
The approach to patients with suspected polyneuropathy starts with a comprehensive
clinical history and identification of risk factors. Detailed neurologic examination and
electro-diagnostic studies are used to identify the distribution of the neuropathy and
to characterize the process as sensory (large or small fiber types, or mixed), motor,
sensorimotor, or autonomic, and as axonopathic, demyelinating, or combined. The
decision for nerve biopsy is taken on the basis of these results. Nerve biopsy remains
a useful diagnostic tool in cases of multifocal, asymmetrical, painful or autonomic
neuropathies where vasculitis, sarcoidosis and amyloidosis are diagnostic possibilities.

4
Besides, nerve biopsy is also useful to detect or confirm histologically other causes
of peripheral neuropathy such as infections (e.g. leprosy, cytomegalovirus infection),
tumors like lymphoma or neurinoma, and granulomatous diseases.
In a prospective study by C M Gabriel etal, diagnostic utility of sural nerve biopsy in 50
consecutive patients with peripheral neuropathy was studied. Nerve biopsy was
useful in nearly 60 % cases, especially in cases with demyelinating neuropathy and
multiple mononeuropathy, besides helpful in confirmation of clinical diagnosis in
nearly 70 % cases. Nerve biopsy revealed an otherwise unsuspected diagnosis in 14%
of the patients and in 16% the biopsy findings were non - contributory. This study also
showed that the yield of nerve biopsy done after site selection as guided by clinical
and electrodiagnostic findings are higher 1. In another prospective study of 38 patients
who underwent nerve biopsy, nerve biopsy proved to be useful in defining the etiology
in 14 patients (37%). The diagnostic yield of nerve biopsy was highest in acute/ sub
acute symmetric and sub acute asymmetric neuropathies, followed by chronic
symmetric and chronic asymmetric neuropathies. The biopsy was diagnostic in 6
patients (16%), in cases where histopathological features were suggestive of
vasculitis, and was supportive of diagnosis in 8 patients (21%) 10.
In the current scenario, due to availability of newer genetic, and pathological
diagnostic modalities, and recognition of newer diagnostic entities, the percentage of
cases of neuropathy of undetermined etiology has considerably decreased. However,

5
inspite of rapid advances, etiology of neuropathy remains elusive in approximately
20% cases, especially axonal neuropathies.
Indications for nerve biopsy
1. Vasculitic neuropathy: Nerve biopsy is indicated in vasculitic neuropathy, to
establish definitive diagnosis before starting treatment. It has been seen that
in vasculitis, nerves are more commonly involved than other readily biopsied
structures like skin and muscle, and hence a search for vasculitis will have
higher yield with a nerve biopsy. Peripheral neuropathy is reported in nearly
52-60 % cases with vasculitis 11.
2. Diabetic neuropathy, especially in cases where superimposed CIDP or vasculitis
is suspected.
3. Toxic neuropathies (amiodarone)
4. Infections (HIV, Leprosy)
5. CIDP, and paraproteinemic neuropathies (deposits of IgM in the nerve usually
precede IgM gammopathy in serum)
6. Amyloidosis.
7. Hereditary neuropathies with negative appropriate genetic tests. Nerve biopsy
can also be helpful by identification of characteristic features, thereafter
planning appropriate genetic tests, for example MPZ gene mutations with
failure of myelin compaction, MTMR2 gene mutations with numerous myelin

6
outfoldings, or MFN2 mutations with abnormalities of intraaxonal
mitochondria.
8. Diagnostic etiology of neuropathy is not established even after a detailed
investigation. In a study of 365 nerve biopsies studied in patients with
undetermined etiology, Shin J. Oh etal found clinically relevant information or
helpful information in nearly 45 % cases. In the same study, specific diagnosis
was reached in 24 % of cases. A diagnosis of vasculitis was established in 12 %
cases, making it the most common diagnosis among those with specific
diagnosis 12.
Selection of nerve for biopsy
Selection of nerve for biopsy including sural nerve, superficial peroneal nerve,
superficial branch of radial nerve, dorsal cutaneous branch of ulnar nerve is done
depending on the clinical scenario. Biopsy should preferably be obtained from a nerve
indicating clinical and electrophysiological abnormalities. The nerve to be biopsied
may also be indicated by imaging techniques (MRI and ultrasonography)
demonstrating affected nerve segments. Sural nerve is usually preferred for biopsy,
due to long length of the nerve, pure sensory distribution, and protection behind the
lateral malleoli and easily testable electro physiologically. Because of the above
mentioned reasons, the yield of sural nerve biopsy is more with only mild sensory loss
as a sequalae and free from compression artefacts 12. Superficial peroneal nerve

7
biopsy combined with peroneus brevis muscle biopsy is preferred in cases of
vasculitic neuropathy. Studies have demonstrated that such combined muscle and
nerve biopsy has a moderately increased yield in demonstrating vasculitis in
comparison to nerve biopsy alone 13, 14, however, study by Bennette et al showed no
significant increase in yield with combined biopsy compared to nerve biopsy alone 15.
Other sensory nerves such as the superficial femoral, superficial radial and the
antebrachial cutaneous nerves may also be biopsied. The nerve specimen should be
processed in a specialized laboratory that analyzes at least paraffin and embedded
(plastic) semi-thin sections. Ultrastructural studies are sometimes required, and
teased fiber preparation is helpful, especially in assessing demyelination and
remyelination.
Procedure of nerve biopsy
The patient is positioned, nerve if palpable marked, and site is cleaned and prepared.
The skin is infiltrated with Lidocaine and incision made. The nerve is identified by
glistening appearance and differentiated from veins by branching pattern. The nerve is
cut taking care not to produce crush artifacts. Skin is closed with vicryl after securing
hemostasis. A bandage is applied to prevent oozing or edema formation and dressing
is done anti-septic ointments.

8
Parameters affecting the diagnostic yield of nerve biopsy
Various parameters affect the yield of nerve biopsy. In a retrospective
Clinicopathological study done by Deprez et al, in 355 patients to evaluate the clinical
and neuropathological parameters affecting the yield of nerve biopsy, it was seen that
contributive biopsies formed nearly 35.5% of total cases16. Clinical parameters
affecting the yield of nerve biopsy were:
(a) Pre-biopsy diagnosis: Greater yield was associated with clinically suspected
vasculitis, inflammatory demyelinating neuropathy and hereditary
sensorimotor neuropathies.
(b) Distribution of symptoms: Contributive findings were more often reported
with multifocal or asymmetrical presentations.
(c) Interval between disease onset and biopsy: Contributive findings were more
often reported with onset-to-biopsy interval of less than 6 months.
(d) Neuropathological techniques used: Serial sections on frozen, paraffin-
embedded and resin-embedded material improved sensitivity for interstitial
pathology; Combined muscle biopsy increased sensitivity in the detection of
vasculitis; and teasing of nerve fibers added critical information to the
classical techniques in 4% cases.

9
Inflammatory Neuropathies
Clinical, electro diagnostic, and cerebrospinal fluid findings are usually diagnostic in
most cases of acute and chronic inflammatory demyelinating polyneuropathies (CIDP).
The role for nerve biopsies is specially important in patients with neuropathy
detected to have only subtle evidence of a demyelinating component on
electrophysiologic studies but clinical features are strongly suggestive of CIDP. The
diagnostic criteria as proposed by American Academy of Neurology (AAN) research
criteria
(Ad Hoc Subcommittee of the American Academy of Neurology AIDS Task Force, 1991)
are tabulated in Table -1 17 . Subsequently, EFNS/PNS consensus guidelines (Joint Task
Force of the EFNS and the PNS, 2010) 18 were designed which provide more even
specificity and sensitivity to the diagnostic criteria (Table – 2).
According to American Academy of Neurology (AAN) criteria, biopsy evidence of
demyelination in sural nerve is mandatory for diagnosis of CIDP, which requires
teased fiber preparation and electron microscopy. While subperineurial edema,
inflammatory cell infiltration, onion bulb formation, and variation in fascicular
involvement are considered supportive of the diagnosis. Variability in the pathological
findings is determined by duration of disease, response to treatment, and the nerve
chosen for biopsy. Various autopsy studies have demonstrated that inflammation and
demyelination more often involves the spinal radicals in a patchy multifocal manner
and it may be completely lacking in the segment of distal (e.g., sural) nerve sampled.

10
The frequency of detection of various specific pathological features appear to be
highly variable in different studies [Table - 3]
In a study done in NIMHANS, in forty-six patients with idiopathic CIDP satisfying AAN
clinical and electrophysiological criteria for CIDP, 32 patients had a progressive clinical
course and 14 with relapsing-remitting course. The frequency of four supportive
pathological alterations - demyelination, inflammation, onion bulb formation, and
axonal changes in sural nerve biopsies were seen in nearly 100% of cases.
Electrophysiological abnormalities were detected in 90.8%, suggesting that supportive
histologic AAN criteria are helpful in diagnosis of CIDP. Besides, endoneurial
inflammation was frequent in the relapsing-remitting form and epineurial
inflammation and axonal changes in those with progressive course. Greater disability
at presentation, poor response to immunomodulation, and lower CSF protein levels
was seen in those with axonal pathology 19.
Onion bulbs, a characteristic feature in CIDP have been reported in 15%-40% of cases.
Dyck and Engelstad 20 reported a mixed pattern of distribution, with well-developed
large onion bulbs intermixed with smaller evolving forms as a characteristic finding in
CIDP.
In a study done by Molenaar et al to investigate the additional diagnostic value of sural
nerve biopsy in 64 CIDP patients, multivariate logistic regression analysis was used
to study the additional diagnostic value of sural nerve biopsy along with six clinical

11
features (remitting course, symmetric sensorimotor neuropathy in arms and legs,
areflexia, raised CSF protein concentration, nerve conduction studies consistent with
demyelination, and absence of co morbidity or relevant laboratory abnormalities). This
study showed that CSF protein concentration >1 g/l and NCS studies suggestive of
demyelination were strong predictors of CIDP. In this study, an independent predictive
value of sural nerve biopsy could not be confirmed 21. Due to the presence of
significant overlap in histopathological findings between CIDP and chronic idiopathic
axonal neuropathies (CIAP), sural nerve biopsy found found to have limited
diagnostic value in CIDP.
More specific alterations in nerve biopsies to differentiate CIDP from other
inflammatory
neuropathies, particularly vasculitis have been described; which include signs of T
cell activation, detection of matrix metalloproteinases 2 and 9, chemokine receptors
and interferon-γ- inducible protein (IP-10), and up regulation of Th1 cytokine IL-17 and
IFN-γ 22. Study using macrophage differentiation antigens and ‘macrophage clustering’
(defined as presence of three or more macrophages around a blood vessel) around
endoneurial vessels have been used to differentiate between inflammatory and
hereditary neuropathies 23.

12
Table 3: Comparison of pathologic findings in CIDP in published literature
Author, No. of cases
Inflammation Demyelination Onion bulbs
Axonal changes
Mixed Normal
Dyck et al 20
(n=26)
54% NA 15%
More common than demyelination
NA
NA
Prineas and MacLeod
24
(n=23)
No significant inflammation
26% 40% NA NA 24%
Barohn et al
25
(n=60) (56 biopsied)
10% 48% NA 21% 12% 17.9%
Krendel et al
26
(n=14)
29%
50%
36%
NA
NA
NA
Bouchard et al 27 (n=100)
18% 68% NA 5% 20% NA
Haq et al 28
(n=24)
36% 50% (teased fiber) 79% (EM), 93% (semithin)
58% 71% NA Nil
Rizzuto et al
29
(n=105)
25% 100% 48% NA NA NA
Vital et al 30
(n=42)
100% 40.4% NA 9.5% 76.1% NA
Vallat et al 31
(n=44)
75% 100% Variable Variable NA NA
Kulkarni et al
19
(n=46)
58.7% 82.8% 28.3% 8.7% 23.9% Nil
NA – Information not available.

13
Vallat et al. retrospectively studied 44 consecutive patients diagnosed clinically as
CIDP. Sensory findings predominated in all the cases. Eight cases did not have a
clear-cut electrophysiologic diagnosis of CIDP, but they satisfied the pathologic
features suggestive of CIDP. Five of these eight patients responded to
immunosuppressive therapy. Thus, nerve biopsy provided unequivocal evidence of
CIDP with no diagnostic EPS findings 31. However, study by Bosboom et al. reported
limited diagnostic utility of sural nerve biopsy in CIDP. In this study, sural nerve biopsy
specimens were taken from 21 consecutive patients who met established criteria for
diagnosis of CIDP, as well as sural nerves from 13 patients with idiopathic axonal
polyneuropathies and six autopsy nerves were taken as controls. There was no
difference in demyelinating features between patients with CIDP and axonal
neuropathies, besides evidence of axonal degeneration was found in both groups 32.
Role of nerve biopsy in diabetic patients and CIDP : There is also an important role
for nerve biopsy in diabetic patients with demyelinating polyneuropathy. The
importance is underlined by possible benefit of immunomodulatory therapy if there
are histopathological features similar to CIDP. Haq et al.28 retrospectively reviewed 10
patients with CIDP (nine of whom had diabetic polyneuropathy) and at least one of the
proposed electrodiagnostic criteria for demyelination, and 21 diabetic patients with
axonal polyneuropathy who underwent sural nerve biopsy. The diabetic patients with
demyelinating polyneuropathy had similar clinical, electrophysiologic, and histologic

14
features as the patients diagnosed with CIDP alone. The majority of patients in both
groups exhibited subperineurial and endoneurial edema, and only 2% to 20% had
inflammatory cells. Onion bulbs were seen in 88% of patients with diabetes and
demyelinating polyneuropathy; thinly myelinated and “naked” axons were frequently
present, but myelin stripping was very uncommon. Six patients with diabetes and
demyelinating polyneuropathy were treated with immunomodulatory therapy and
showed favorable response.
Use of inflammatory markers in nerve biopsy specimens to differentiate CIDP in
diabetes patients from typical diabetic peripheral neuropathy: Certain inflammatory
markers are useful to differentiate the two conditions. One such marker described is
MMP-9, Jann et al. 33 found increased immunoreactivity for MMP-9 in endoneurial
vessels and in epineurial T cells in diabetic CIDP nerves diabetic peripheral neuropathy
nerves. Patients with MMP-9 reactive nerve responded better to intravenous
immunoglobulin.
Peripheral neuropathy has been described with hepatitis C infection, with or without
cryoglobulinemia. Nemni et al. 34 provided an excellent report of 51 patients with
hepatitis C infection. Forty of 51 had cryoglobulinemia. Significant polyneuropathy was
more prevalent in the cryoglobulinemia patients; however, mononeuropathy or
multiple mononeuropathy were more prevalent in the cryoglobulin-negative patients.
Cranial neuropathies occurred in five of 11 (46%) patients with neuropathy who were
cryoglobulinemia-negative and in three of 40 (7.5%) patients who had

15
cryoglobulinemia. Nerve biopsy evidence of vasculitis was present in one third of
patients with cryoglobulinemia and in two out of three cryoglobulinemia-negative
patients. Differential fascicular axon loss suggestive of ischemia was present in 30% to
40% of all biopsies. Axonopathic changes were seen in majority, and combination of
demyelination and axon loss was present in 28% of the specimens from
cryoglobulinemia patients. Peripheral neuropathy is rare in sarcoidosis. Said et al. 35
studied 11 patients undergoing nerve biopsy that revealed epineurial granulomas
and perineuritis. The neuropathies varied from focal to multifocal and included a
patient with multifocal neuropathy with conduction blocks and one with a Guillain-
Barre-like presentation, and chronic, symmetrical, sensory, and sensorimotor
polyneuropathies, facial neuropathies. Multinucleated giant cells were found in eight
of 11 specimens, and vasculitis was present in seven. Muscle biopsy specimens from
10 patients showed inflammatory infiltrates and granulomas in nine patients and
necrotizing vasculitis in two. This study showed that necrotizing vasculitis with
ischemia may be a major mechanism for nerve injury in sarcoid neuropathies 35.
Pathological criteria for demyelination proposed by Ad hoc committee of AAN AIDS
task force (table – 1):
A. Mandatory : Nerve biopsy specimen showing unequivocal evidence of
demyelination and remyelination : Demyelination by either electron
microscopy(> 5 fibres), or teased fibre study (> 12 % of teased fibres), minimum
of 4 internodes each, demonstrating demyelination and remyelination.

16
B. Supportive criteria :
a. Subperineurial or endoneurial edema.
b. Mononuclear cell infiltration.
c. Onion-bulb formation.
d. Prominent variation in degree of demyelination between the fascicles.
C. Exclusion: vasculitis, neurofilamentous swollen exons, amyloid deposits,
intracytoplasmic inclusions in Schwann cells or macrophages indicating
adrenoleucodystrophy, Metachromatic leucodystrophy, globoid cell
leucodystrophy or other evidence of specific pathologic process.
European Federation of Neurological Societies (EFNS)/Peripheral Nerve Society (PNS)
Guideline Electrodiagnostic Criteria [Joint Task Force of the EFNS and PNS, 2010]
table - 2.
I. Definite: at least one of the following :
A. At least 50% prolongation of motor distal latency above the upper limit of normal
values in two nerves, or
B. At least 30% reduction of motor conduction velocity below the lower limit of
normal values in two nerves, or
C. At least 20% prolongation of F-wave latency above the upper limit of normal values
in two nerves (>50% if amplitude of distal negative peak compound muscle action
potential [CMAP] <80% of lower limit of normal values), or

17
D. Absence of F-waves in two nerves if these nerves have amplitudes of distal negative
peak CMAPs at least 20% of lower limit of normal values + at least one other
demyelinating parameter in at least one other nerve, or
E. Partial motor conduction block: at least 50% amplitude reduction of the proximal
negative peak CMAP relative to distal, if distal negative peak CMAP at least 20% of
lower limit of normal values, in two nerves, or in one nerve + at least one other
demyelinating parameter in at least one other nerve, or
F. Abnormal temporal dispersion (>30% duration increase between the proximal and
distal negative peak CMAP) in at least two nerves, or
G. Distal CMAP duration (interval between onset of the first negative peak and return
to baseline of the last negative peak) of at least 9 ms in at least one nerve + at least
one other demyelinating parameter in at least one other nerve II.
Probable : At least 30% amplitude reduction of the proximal negative peak CMAP
relative to distal, excluding the posterior tibial nerve, if distal negative peak CMAP at
least 20% of lower limit of normal values, in two nerves, or in one nerve + at least one
other demyelinating parameter in at least one other nerve III.
Possible : As in ‘I’ but in only one nerve.
Vasculitic neuropathy
Systemic vasculitis involving small to medium-sized arteries commonly affects
epineurial vessels in vasa nervorum and thereby produce peripheral neuropathies.

18
Peripheral neuropathy can either be the sole manifestation of vasculitis, or it may
represent one of the manifestations of systemic necrotizing vasculitis 36.
Classification system for classifying vasculitides associated with peripheral neuropathy
was proposed by Dyck et al 36, which recognized two broad categories based on
etiopathogenesis.
(a) Vasculitis resulting from direct infection: Microorganisms related vasculitis
related to direct cytopathic effect of peripheral neurons are HSV and CMV.
Viruses associated with persistent replication such as HBV, HCV, HIV and HTLV-
1 have strongest association with vasculitic neuropathy 37.
(b) Vasculitis resulting from immunological mechanism
a. Systemic necrotizing vasculitis
i. Classic PAN: Peripheral neuropathy occurs in 50-75 % of patients
37. Vasculitic neuropathy mostly presents as mononeuritis
multiplex, or rarely as distal polyneuropathy affecting most
frequently the lower extremities. Cranial nerve involvement
occurs in nearly 2 % of patients.
ii. Microscopic polyangitis: Peripheral neuropathy has been
described in 20-60 % of patients 37. Mononeuritis multiplex is
the most common neurological manifestation, caused by
inflammation of epineurial arterioles, leading to ischemia of
both sensory and motor nerves.

19
iii. Churg-Strauss syndrome: Peripheral neuropathy is the second
most common manifestation after pulmonary involvement,
occurring in nearly 70 % of patients 38. The most common
pattern is mononeuritis multiplex which tends to evolve into
polyneuropathy, and symmetrical polyneuropathy is seen in
advanced disease. Necrotizing vasculitis of epineurial arterioles,
eosinophilic infiltration and granuloma formation are the
characteristic features of vasculitic neuropathy associated with
Churg-Strauss syndrome.
iv. Wegener’s granulomatosis: Peripheral neuropathy occurs in 15-
44 % of patients 39. The most common presentation is
Mononeuritis multiplex, the onset of symptoms is usually
sudden with involvement of one or more peripheral nerves,
followed by widespread sensori-motor polyneuropathy. Multiple
cranial neuropathies most commonly involving optic, abducent
and facial nerves occurs in about 10 % of patients 40.
v. Connective tissue disorders
1. Rheumatoid arthritis: Approximately 20 % patients have
vasculitis, and vasculitic neuropathy occurs in nearly 10-
25 % of cases with Rheumatoid arthritis 41. Most patients
have slowly progressive distal symmetrical sensory or

20
sensori-motor polyneuropathy and approximately half
are predominantly sensory neuropathies 42.
2. SLE: Approximately 5-10 % patients develop vasculitic
neuropathy, and most common pattern is multifocal
neuropathy at onset which evolves into symmetrical
polyneuropathy 41.
3. Sjogrens syndrome: Prevalence of peripheral neuropathy
is around 25 % 43. Distal symmetrical sensory
predominant pattern is seen in nearly 75 % of
neuropathies. Sensory neuronopathy caused by dorsal
root ganglionitis is a distinctive feature accounting for
15-20 % of neuropathies.
4. Scleroderma : Peripheral neuropathy is seen in 20-25 %
patients with scleroderma. Motor predominant
neuropathy is common and trigeminal sensory
neuropathy is described in 3 % of scleroderma patients
44. Vasculitic neuropathy is seen in 0.5 % of scleroderma
patients and 1 % of patients with CREST syndrome.
5. Behcet disease: Peripheral neuropathy is seen in 0.5 % of
patients 45.

21
b. Hypersensitivity vasculitis: Essential mixed cryoglobulinemia, serum
sickness with radiculoneuropathy as manifestation of Hypersensitivity
vasculitis has been described 46.
c. Giant cell arteritis: Casseli et al (1988) have described peripheral
neuropathy in nearly 15 % of patients, and there is 15-20 % risk of
permanent vision loss from anterior ischemic optic neuropathy 47.
d. Non Systemic Vasculitic neuropathy (NSVN) : The term NSVN was first
described by Dyck et al 1987, who described 20 such patients. NSVN
refers to localized form of vasculitis, mediated by immune response
against tissue specific antigens (peripheral nervous system), with
different pathogenesis and prognosis compared to systemic
vasculitides. NSVN has overlapping features with systemic vasculitides
including presence of constitutional symptoms, elevated ESR, anemia,
leucocytosis, thrombocytosis, presence of auto antibodies in 20-40 % of
patients, detection of vasculitic changes in skeletal muscles, and better
therapeutic response with combination therapy36.

22
Diagnostic criteria for NSVN:
Inclusion criteria:
1. Clinical evidence of neuropathy by history and examination
2. Electro diagnostic findings consistent with neuropathy
3. Nerve or nerve/muscle biopsy diagnostic of necrotizing
vasculitis.
Exclusion criteria:
1. Clinical, laboratory, radiological or pathological evidence of organ
involvement outside the peripheral nervous system (except muscle)
2. Identified etiological agent(drug exposure, infections especially HIV,
HBV, HCV, CMV or HZV).
3. Underlying systemic conditions predisposing to vasculitis
(connective tissue disease, malignancy, diabetes mellitus, mixed
cryoglobulinemia).

23
Clinical profile of Primary vasculitides associated with peripheral neuropathy 48(Schaublin et al 2005)
Peripheral Nerve
Upper Respiratory
Lower Respiratory
Renal GIT Arthralgias Cardiac Skin CNS C-ANCA P-ANCA
Microscopic polyangiitis
60 – 70 % -- 20-80 % 70-90% 30% 50% 10-20% 50-70% 10-20% 10-50% 50-80%
PAN 50-70% -- -- -- 20-60% 50-80% 5-30% 25-50% 5-20% -- --
Churg-strauss syndrome
60-80% 50-60% 40-70% 10-40% 30-60% 50% 10-40% 50-60% 5-30% 3-35% 2-50%
Wegeners Granulomatosis
40-50% 95% 70-85% 70-80% <5% 60-70% 10-25% 40-50% 5-10% 75-90% 5-20%
Profile of Secondary vasculitides associated with peripheral neuropathy48
Neuropathy Clinical pattern Associated features
Laboratory findings Electrophysiology Nerve pathology
Rheumatoid arthritis Uncommon Sensory/sensorimotor Joint-100%, skin 70%
RF 90%, ESR(elevated) 85%
Distal sensori-motor axonal, mononeuritis multiplex
Necrotising arteritis; IgM deposits
SLE Rare Distal sensorimotor; mononeuritis multiplex , cranial
Skin 90%, joint 85 %, renal 50 %
ANA 90-100% DSDNA 60%
Distal sensori-motor axonal Asymmetric
Necrotising arteritis; Complement deposits
Sjogrens syndrome Common Distal sensory cranial; ganglionopathy
Sicca 50-90%, skin 75%
ANA 90%,RA 60%,SSA/SSB 50%
Axonopathy; ganglionopathy
Perivascular Infiltrates, axonal loss
Systemic Sclerosis
Rare Distal symmetrical; cranial; mononeuritis multiplex
Fibrotic skin, Raynauds phenomenon, calcinosis
ANA 100% Anti-centromere antibody 70%
Distal motor predominant neuropathy
Endoneurial vasculopathy; Multifocal axonal loss
Sarcoidosis Uncommon Distal symmetrical; cranial; mononeuritis multiplex; radiculopathy
Pulmonary 90%, skin 25%
ACE 70%,ESR(elevated) 50%
Distal sensori-motor axonal Asymmetric
Noncaseating granuloma
Cryoglobulinemia Common 20-80%
Asymmetrical sensori-motor; mononeuritis multiplex
Purpura 90% Skin ulcers
Cryoglob 100% HCV 50-70%
Asymmetric sensori-motor; symmetric
Necritizing arteritis, immune complex deposits

24
Pathological diagnosis:
Definite diagnosis of vasculitic neuropathy is dependent on histopathology. In
vasculitic neuropathy, the yield of peripheral nerve biopsy is much more than skin
or muscle biopsy 41. The yield of peripheral nerve biopsy is higher than muscle
biopsy in cases of NSVN, whereas both muscle and nerve biopsies have almost
similar yield in systemic vasculitis 20. In a study by Vrancken et al 49, the additional
yield of combined nerve and muscle biopsy compared to nerve biopsy alone is
about 5% in patients with clinically suspected vasculitis, and around 15% in patients
with vasculitic neuropathy.
The comparison of diagnostic sensitivities in vasculitic neuropathy are highlighted
in table –
Comparison of diagnostic sensitivities in vasculitic neuropathy (Collins et al 2005)
Biopsy site Reference Vasculitis sensitivity
Sural nerve Collins et al(2003) NSVN 14/30(47%)
Hattori et al(2002) Microscopic polyangitis
20/26(80%)
Clausen et al (2000)
Systemic & NSVN 27/45(60%)
Dyck et al (1987) Systemic & NSVN 31/65 (48%)
Hattori et al(2002 Churg Strauss Syndrome
16/30 (53%)
Combined total Systemic & NSVN 109/196 (56%)
Peroneus brevis & superficial peroneal nerve
Collins et al (2000) Systemic 15/25 (60%)
Collins et al (2003) NSVN 11/19 (58%)
Chia et al ( 1996) Systemic & NSVN 23/33 (70%)
Combined total Systemic & NSVN 49/77 (64%)

25
Histopathological classification of vasculitic neuropathy
Definite vasculitis 50:
Active lesion: Inflammatory infiltrate within the vessel wall and one or more signs
of vascular destruction such as fibrinoid necrosis, vascular/perivascular
hemorrhage, or endothelial cell disruption.
Chronic lesion with signs of repair or healing: Nerve biopsy showing mononuclear
inflammatory cells in the vessel wall and one or more of the following – intimal
hyperplasia, fibrosis of media, adventitial/periadventitial fibrosis; chronic
thrombosis with recanalisation.
No evidence of another primary disease process that may mimic vasculitis
pathologically such as lymphoma, lymphomatoid granulomatosis or amyloidosis.
Probable / suspicious vasculitis 50:
Predominant axonal changes and perivascular inflammation accompanied by signs
of active or chronic vascular damage or perivascular inflammation plus one or more
of the following: Asymmetrical/multifocal nerve fibre loss, hemosiderin deposits
(Perls stain for iron); Vascular deposition of complement; Ig M or fibrinogen by
direct IF; active axonal degeneration, myofibre necrosis, regeneration, or infarcts in
concomitant peroneus brevis muscle biopsy.
Possible vasculitis 50:
Presence of predominant axonal changes and inflammation in vessel wall without
other signs of definite vasculitic neuropathy, in absence of above criteria for
definite and probable vasculitis OR

26
One or more signs of active/chronic vascular damage or pathological criteria of
definite vasculitic neuropathy without vessel wall or perivascular inflammation.
Diagnostic criteria for clinically probable vasculitic neuropathy in patients lacking
biopsy proven necrotizing vasculitis 51
1. Clinical presentation typical for a vasculitic neuropathy: asymmetrical or
multifocal painful sensorimotor neuropathy; Acute/sub acute relapsing,
progressive or relapsing progressive course.
2. Laboratory evidence of a systemic inflammatory state, for example elevated
ESR.
3. Electro diagnostic evidence of an active asymmetrical axonal sensori-motor
neuropathy.
4. Clinical response to immunosuppressive therapy.
5. Suggestive neuromuscular pathology: vascular thickening narrowing or
obliteration of vascular lumen , thrombosis, periadventitial capillary
proliferation, hemosiderin deposits, asymmetrical nerve fibre loss or
wallerian like degeneration.
6. Clinicopathological evidence of a systemic/ secondary etiology : concurrent
condition known or suspected to predispose to vasculitis ( connective tissue
disease, infections, certain drugs, cryoglobulinemia, malignancy/
paraproteinemias); simultaneous multi-organ non peripheral nerve
involvement; Biopsy proven vasculitis in other tissues.

27
At least 3 of first 5 criteria required for NSVN, criterion 6 is mandatory for systemic
vasculitis.
Neuropathies Associated with Infections
1. HIV infection: Polyneuropathies in HIV infection include sensori - motor
neuropathies affecting large and small myelinated and unmyelinated fibers.
Mechanism of HIV-mediated neuropathy includes inflammatory,
demyelinating, mononeuritis-multiplex, cytomegalovirus-induced
neuropathy, as well as mixed neuropathy as part of the diffuse
inflammatory lymphocytosis syndrome. Macrophage activation in the
presence of pro-inflammatory cytokines mediates axonal injury. Patients
with toxic neuropathies due to antiretroviral therapies have similar
pathologic findings, and mitochondrial disruptions are described. Diffuse
infiltrative lymphocytosis syndrome is painful, usually symmetrical, and
acute or sub acute. There is axon loss and marked CD8 lymphocytic
angiocentric infiltration in nerve biopsy specimens in the epineurium and
endoneurium, along with a massive HIV proviral load. Mononeuritis
multiplex due to vasculitis has also been reported. Other infections in HIV
like CMV, HCV, and Syphilis are also responsible for neuropathy 52.
2. West Nile virus: Usually presents with a new paralytic illness affecting
anterior horn cells and motor roots. Histopathological studies have shown
presence of perivascular chronic inflammation in the spinal cord, along with

28
loss of anterior horn cells, and neuronophagia. There is presence of
inflammation around lumbar spinal cord nerve roots 53.
3. Leprosy :
Paraproteinaemic Neuropathies
Anti–myelin-associated glycoprotein (anti-MAG) IgM monoclonal gammopathies:
Gammopathies are characterized by myelin abnormalities including the presence of
tomacula, increased myelin loops, redundant myelin infolding or outfolding,
enlargement of the adaxonal space, and tomacula in fibers containing paranodal or
internodal demyelination. Eurelings etal. have described the presence of T-cell
inflammation in monoclonal gammopathy, and thus usefulness of nerve biopsy
in identification of these patients with superimposed vasculitis who will respond
favourably to immunotherapy 54.
Amyloidosis
Peripheral neuropathy is the cardinal clinical feature of familial amyloid
polyneuropathies, and occurs in 15% to 35% of patients with acquired amyloidosis.
Peripheral nerve amyloidosis is typically characterized by accumulations of amyloid
in the endoneurium, epineurium, perineurium, and in blood vessel walls. There is
preferential loss of small myelinated and unmyelinated fibers, with characteristic
clinical features of painful neuropathy with autonomic symptoms 55. In a
retrospective study done by Andrews etal to compare the utility of sub-
cutaneous fat aspiration and nerve biopsy in diagnosing amyloidosis in patients

29
with isolated sensorimotor peripheral neuropathy, only 6% of patients had a
positive aspirate for amyloid, and most of these patients had a monoclonal protein
or other clinical findings associated with amyloidosis. Thus concluding that the
yield of subcutaneous fat aspirate in patients with isolated peripheral neuropathy is
low and this biopsy should be reserved for patients with systemic amyloidosis 56.
Hereditary Neuropathies
Nerve biopsies are not indicated if hereditary neuropathy is clinically suspected.
However, nerve pathology is helpful in sporadic cases and it provides relevant
information regarding the genetic study to be performed in selected cases.
Longitudinal study by Gabreëls-Festen 57 in 25 patients with Dejerine-Sottas
syndrome, patients with PMP22 mis-sense mutations had thin myelin sheaths,
suggestive of hypomyelination and patients with PMP22 duplications had increased
myelin thickness, more age-related pathology, with early active demyelination,
followed by onion bulb formation and stabilization, and then late axon loss.
Inflammation plays an important role in neuropathic attacks in hereditary
neuropathies, including hereditary brachial plexus neuropathy. Klein et al. 58
examined upper extremity nerve biopsy specimens from four patients during
exacerbations of hereditary brachial plexus neuropathy. These patients had
evidence of active axonal degeneration and prominent perivascular inflammation
with disruption of vessel walls; however teased fibers showed no evidence of
reduplicated myelin (tomacula). It was concluded that inflammation, probably

30
immune mediated, was the cause of these attacks, and use of immune modulation
was indicated.
Giant axonal neuropathy is a rare autosomal recessive disorder, affecting both the
peripheral and central nervous system. Nerve biopsy shows evidence of axonal
swellings with tightly packed filaments, and uniform onion bulbs. Kuhlenbäumer et
al. 59 investigated two generations of a family with five members affected by giant
axonal neuropathy. The authors identified two novel mutations in the gigaxonin
gene.
Toxic Neuropathies
Several toxic agents and drugs have characteristic histo-pathological changes.
Amiodarone is one such drug that has characteristic histopathology. Pulipaka et al.
60 reported three patients with amiodarone-induced mixed polyneuropathies and
vacuolar myopathy. Pathological changes are characterized by presence of
lysosomal inclusions in the endoneurium, especially in the cytoplasm of Schwann
cells and in endothelial cells and fibroblasts, and presence of osmiophilic inclusions,
best seen on semi-thin plastic sections and on ultrastructural studies. Chloroquine
is also described to be associated with osmiophilic inclusions. Most other toxins,
such as thalidomide and alcohol, cause nonspecific, length-dependent
sensorimotor axonal degeneration. Small axons are primarily affected in alcoholic
neuropathy, which is not associated with thiamine deficiency 61.

31
Acquired Metabolic Neuropathy
Diabetes mellitus remains the most common cause of neuropathy with
multifactorial pathogenesis. Nerve biopsy is usually indicated in diabetic patients
with distal polyneuropathy with consideration of vasculitis and CIDP. In patients
with diabetic radiculoplexus neuropathy, biopsies often reveal perivascular
inflammation or vasculitis and features suggestive of nerve ischemia. The
administration of immunomodulatory therapy in this group of patients is useful.
Peripheral neuropathy, likely due to thiamine deficiency, occurs after gastrectomy
or gastrostomy. Evaluation of 12 patients with post-gastrectomy sensorimotor
polyneuropathy, and 7 of whom had features suggestive of autonomic dysfunction;
there was electrophysiological evidence of an axonal neuropathy with mild
demyelination. Sural nerve biopsy specimens revealed loss of large and small
myelinated and unmyelinated fibers, active axonal degeneration, and rare
segmental demyelination and remyelination, with subperineurial “edema.” These
patients had evidence of thiamine deficiency and they improved with thiamine
administration62.
32
AIMS AND OBJECTIVES
1. To study the utility of nerve biopsy in providing diagnostic, therapeutic or
prognostic information that aid in clinical management of patients with
peripheral neuropathy.
2. To study the clinical and demographic profile of patients undergoing nerve
biopsy.
INCLUSION CRITERIA
Patients with established diagnosis of peripheral neuropathy who
underwent nerve biopsy.
EXCLUSION CRITERIA
Nerve biopsy samples in which the diagnostic labeling was not possible.
METHODS
All patients admitted in Neurology ward – Sree Chitra Tirunal Institute of Medical
Sciences and Technology, Trivandrum between 2010 and 2015, with established
diagnosis of peripheral neuropathy who underwent nerve biopsy were included in
the study.
Retrospective analysis of patients who have undergone nerve biopsy during period
2010 – 2015, was undertaken. A detailed clinical, socio-demographical data for all
patients, essential investigations (routine hematology, blood glucose and other
biochemical parameters, serological tests for HIV and paraproteinemia, and
vasculitis workup), including CSF Study and electrophysiological study was

33
collected. Detailed histopathological studies was done on all the specimens, and
special stains were done in selected cases, if indicated. An attempt was made to
correlate histopathological features of biopsy with electrophysiological study.
Indications for nerve biopsy
Based on clinical evaluation, indications for biopsy were classified into:
1. Suspected vasculitis, CIDP, amyloidosis, HMSN, or other inherited metabolic
diseases;
2. Multiple potential causes of neuropathy, biopsies used to narrow
differential diagnosis;
3. Absence of presumptive etiology (no working diagnosis, NWD);
STATISTICAL ANALYSIS : The demographic details and outcomes of the study
population was entered in Microsoft Excel sheet, and descriptive analysis was done
using SPSS 17.0. Data was presented as numbers and percentages.

34
RESULTS
In this study, nerve biopsies of 84 patients done between the period 2010 -2015
were studied.
Demographic details:
The subjects whose nerve biopsy results were included in the study included 53
males and 31 females (Figure – 1). Mean age of onset of symptoms was 58.6 +/-30.2
years (range 2 - 75 years) and the mean age at the time of nerve biopsy was 59.8 +
/-35.2 years. Mean duration of symptoms was 12.6 months (range 5 days – 240
months).
The age distribution of patients is shown in Figure – 2. Majority of patients (19) were
in between the age group 60-70 years, in addition 11 patients were between age
group 5-60 years and 10 each in between the age group 10-20 years and 30-40
years.

35
Figure – 1
Figure – 2
Males : 53(63.8%)
Females : 31 (36.2%)
Gender distribution
0
2
4
6
8
10
12
14
16
18
20
< 10 y 10-20 y 20-30 y 30-40 y 40-50 y 50-60 y 60-70 y > 70 y
Age distribution

36
Clinical profile of patients:
The course of symptom progression was acute in 7 (7.6 %), sub acute in 11(12.7 %),
and chronic in 66 (79.7 %) patients. The onset involving lower limbs in 64, upper
limbs in 11, and simultaneous upper and lower limbs in 9. The presenting symptoms
are summarized in Table – 1. Majority of patients presented with positive sensory
symptoms in form of paraesthesias
(n – 34, 43 %). Negative sensory symptoms were present in 18 patients (22.8 %).
Motor complaints in lower limbs and upper limbs as presenting symptoms were
seen in 26(23.4%) and 10(12.5 %) patients respectively (Table – 1).
The clinical features of these patients are summarized in Table 2.
Motor system abnormalities included weakness in 67 (84.8 %) and muscle wasting in
15(19 %) patients. Cranial neuropathy was seen in 5 patients, in the form of facial
nerve weakness in 5 patients, trigeminal nerve involvement in 4 patients, bulbar
palsy in 2 and external ophthalmoplegia in 2 patients. In addition, 2 patients had
evidence of SNHL. Features of autonomic dysfunction in form of orthostatic
hypotension, sweating abnormalities and gastrointestinal abnormalities were noted
in 11 patients. Asymmetric onset of symptoms was seen in 19 patients and
asymmetric clinical profile was seen was noted in 58 patients. Thickened nerves
were noted in 8 patients. Most common sites of nerve thickening was ulnar nerve,
in addition, dorsal cutaneous branch of ulnar nerve, superficial branch of radial
nerve and superficial peroneal nerve were thickened in 2 patients each.

37
Presenting symptoms(Table-1)
1. Positive sensory symptoms in lower limbs 26 (32.9 %)
2. Negative sensory symptoms in lower limbs 14 (17.7 %)
3. Motor weakness in lower limbs – proximally 19 (14.5 %)
Motor weakness in lower limbs – distally 7 (8.9 %)
4. Motor weakness in upper limbs – proximally 2 (2.5 %)
Motor weakness in upper limbs – distally 8 (10 %)
5. Positive sensory symptoms in upper limbs 8 (10.1 %)
6. Negative sensory symptoms in upper limbs 3 (2.6 %)
7. Cranial neuropathy 1 (1.3 %)
Clinical features (Table-2)
1. Motor weakness in lower limbs Proximal : 21 (30 %)
Distal : 48 (64.8 %)
Proximal and distal : 67 (84.8 %)
2. Motor weakness in upper limbs Proximal : 12 ( 14.5 %)
Distal : 58 ( 68.6 %)
Proximal and distal : 65 (82.3 %)
3. Negative sensory symptoms 58 (73.4 %)
4. Positive sensory symptoms 41 (51.9 %)
5. Skin and hair changes 50 (63.3 %)
7. Wasting Upper limbs :11 (13.9 %)
Lower limbs :4 (5.1 %)
Both upper and lower limbs : 13 (16.5 %)
8. Cranial neuropathy 10 ( 12.7 %)

38
Examination (Table – 3)
1. Motor weakness in lower limbs Proximal: 18 (23.4 %)
Distal: 54 (71.3 %)
Proximal and distal: 61 (77.2 %)
2. Motor weakness in upper limbs Proximal: 14 (17.2 %)
Distal: 56 (68.6 %)
Proximal and distal: 60 (75.9 %)
3. Loss of pinprick sensations 48 (60.8 %)
4. Loss of temperature sensations 40 (45.6 %)
5. Loss of touch sensation 32 (40.4 %)
6. Loss of JPS, vibration sensations 36 (45.6 %)
7. Orthostatic hypotension 13 (16.5 %)
8. Peripheral nerve thickening 8 (10.2 %)
9. Deformities Kyphoscoliosis: 2 (2.6 %)
Pes cavus : 11 (13.9 %)
Hammer toes : 1(1.3 %)
Clawing : 8 (10.1 %)
10. Positive Rhombergs sign 33 (41.8 %)
11. Deep tendon jerks 38 (48.1 %)
12. Wasting Lower limbs distally : 8.9 %
Upper limbs distally : 12.7 %
Both upper and lower limbs : 17.7 %
13. mRS at presentation 0 : 1 (1.3 %)
1 : 1 (1.3 %)
2 : 10 (12.7 %)
3 : 26 (32.9 %)
4 : 37(46.8 %)
5 : 3(3.8 %)
Examination finding are summarized in Table-3. Most common findings were motor
weakness in lower limbs (77.2 % patients), followed by motor weakness in upper
limbs (75.9% cases). Evidence of peripheral nerve thickening was present in 8 cases
(10.2 %), in 3 cases of CIDP, and 5 cases with Hansens disease. Most common nerves
thickened were bilateral ulnar nerves (5 cases), 3 cases showing involvement of
peroneal nerves, and one case each with involvement of great auricular nerve and
superficial radial nerve. The clinical features of patients with a diagnosis of CIDP and
Vasculitis are summarized in Table – 4 and 5 respectively.

39
Clinical features of patients with diagnosis of CIDP on nerve biopsy(Table – 4)
Feature Observation ( n- 23)
Duration of symptoms(months) 9.25 +/-13.6
Nerve biopsy delay duration(days) 36 +/-12
Initial / onset neuropathic symptom Sensory Sensori-motor Motor
19 (82.6 %) 2 (8.5 %) 3 (13 %)
Onset of neuropathic symptoms Upper limbs Lower limbs
2 (8.8 %) 21 (91.2 %)
Clinical pattern of neuropathy Symmetric sensori-motor neuropathy Asymmetric sensori-motor neuropathy Symmteric sensory neuropathy
11 ( 30.4 %) 25 (69.6 %) 1(4 %)
Clinical features Positive sensory symptoms Negative sensory symptoms Weakness in BLL Weakness in BUL, BLL Areflexia Loss of pain, temperature sensations Loss of JPS, Vibration sensations History of falls Rhombergs sign Cranial nerve involvement
20 (87 %) 18 (78.3 %) 23 (100 %) 21 (91.3 %) 18(78.3 %) 12 (52.2 %) 20 (87 %) 12(52.2 %) 18 (78.3 %) 1 (4.3 %)
Clinical features of patients with diagnosis of vasculitic neuropathy on nerve
biopsy(Table – 5)
Feature Observation (n – 18)
Presence of systemic symptoms 8 (44.4 %)
Duration of systemic symptoms (months) 16.87 +-13.66
Duration of neuropathic symptoms(months) 9.25 +-13.6
Initial neuropathic symptom Positive sensory symptoms in LL Positive sensory symptoms in UL Motor weakness in UL Motor weakness in LL
7 (38.9 %) 3 (16.73 %) 1 (5.6 %) 7 (38.9 %)
Onset of neuropathic symptoms Upper limbs Lower limbs
5 ( 13.6 %) 31 ( 86.4 %)
Clinical pattern of neuropathy Mononeuritis multiplex Diffuse polyneuropathy
11(61.1 %) 7 (38.9 %)
Sensori-motor and sensory neuropathy(clinical) Sensori-motor Pure sensory
28 ( 77.8 %) 8 ( 22.2 %)
Cranial nerve involvement 4 (22.3 %)

40
Co-morbidities(Table – 6)
S. No Co-morbidities N ( percentage)
1. Diabetes mellitus 21 ( 25.5 %)
2. Systemic Hypertension 8 (7.5 %)
3. Lymphoma 1(1.3% )
4. Malignancy 1 (1.3%)
5. Connective Tissue disorder 1 (1.3%)
6. Hypothyroidism 4 (5.1 %)
7. Tuberculosis 3 (3.9 %)
8. Coronary Artery disease 5 (6.5 %)
9. No co-morbidities 43 ( 54.4 %)
Common co-existing systemic illnesses are summarized in Table – 6. The most
common co - existing illnesses were Diabetes mellitus and Systemic hypertension in
21(25.5 %) and 8(7.5 %) patients respectively. History of malignancy was obtained in
2 patients. These included Non-Hodgkin’s lymphoma and carcinoma tonsil
(operated-hemimandibulectomy done 2 years back) – one case each detected 3
years and 2 years prior to the onset of neuropathic symptoms and hence considered
unrelated to neuropathy. Other co-existing medical illnesses included Tuberculosis
in 3 patients (3.9 %), Hypothyroidism in 4 patients (5.1 %). Past history of Hansen’s
disease was present in 2 patients, who had presented with neuropathic symptoms.
History of Undifferentiated polyarthritis was present in 4 patients, and Rheumatoid
arthritis was present in 2 patients.
EPS
Most common electrophysiological pattern was axonopathic neuropathy(n-62, 73.8
%), followed by mixed demyelinating and axonopathic neuropathy(n-16, 19 %) and
pure demyelinating neuropathy(n-6, 7.1 %).

41
Laboratory investigations:
The results are summarized in table 8. CSF study was done in 55 patients, and 42
cases had evidence of elevated CSF protein, with mean value of 91.4 mg/dl (range:
24 - 492 mg/dl). CSF albumin-cytological dissociation was present in 19 cases, out of
total of 24 cases (79.2 %) diagnosed as CIDP.
Positive ANA profile was present in 5 patients, in 3 cases positivity was seen for Anti-
Ro antibodies, and one case each showing positivity for Anti-Smith, and Anti-
PM/SCL. Serum protein electrophoresis was performed in 42 patients and none
revealed an M spike. Non-specific abnormalities in form of polyclonal gamma-
globulinemia and hypo-albuminemia were noted in 7 and 8 patients respectively.
None of patients showed the presence of BJP in urine.
Summary of investigations (Table 7)
ESR (a) 10 – 20 mm fall Ist hr (b) 20 – 30 mm fall Ist hr (c) > 30 mm fall Ist hr
27 (34.2 %) 13 (16.5 %) 37 (46.8 %)
CSF Albumino-cytological dissociation( CIDP) 19/24
CSF protein (N-55) Mean : 91.40 mg/dl (range : 24-492 mg/dl)
Positive ANA Profile (N-6) Anti-Ro – 3
Anti-Smith, Jo-1 – 1
Anti-PM/Scl – 1
HBAIC > 6.5 % 10

42
HISTOPATHOLOGY STUDIES
Most common biopsied nerve was the sural nerve in 75 patients. 3 patients
underwent biopsy of dorsal cutaneous ulnar nerve (sural nerve study normal
electrophysiological), and one patient biopsy of radial cutaneous nerve. Sites of
biopsies are summarized in Table – 8.
Table - 8
Biopsy – site N
Sural nerve 75
Dorsal cutaneous ulnar nerve 3
Radial cutaneous nerve 1
Combined nerve and muscle biopsy 10
Skin biopsy 12
Lip biopsy 6
CIDP
The diagnosis of CIDP was established in 24 cases on the basis of available clinical,
electrophysiological results (as per EFNS 2010 guidelines). Evidence of CSF albumin-
cytological dissociation was present in 19 cases (79.2 %). Sural nerve biopsy findings
were consistent with diagnosis of CIDP in 16 cases, 3 cases showed features
suggestive of vasculitis. 2 cases showed non-specific chronic axonopathic changes,
with no evidence of inflammatory cell infiltration or vasculitis, and 2 cases showed
evidence of diabetic neuropathy with no inflammatory cell infiltration. In addition, 3
cases which had shown evidence of acquired demyelination in form of multiple
conduction block and temporal dispersion, and CSF study showing albumino-
cytological dissociation, there was no evidence of inflammation on sural nerve
biopsy and there was uniform distribution of onion bulbs ( suggestive of CMT). The

43
findings are summaried in Table – 9. Myelin alteration was demonstrated in all
patients, with most common histopathological finding being non-uniform loss of
myelinated fibres in 78.3 % cases and evidence of demyelination/remyelination,
followed by sub-endoneurial edema, in 71.3 % cases, endoneurial inflammation in
43.5 % cases and non-uniform distribution of onion bulbs in 28 % cases. Features
suggestive of diabetic microangiopathy, co-existent with inflammation were seen in
6 cases. Epineurial inflammation and axonopathic changes co-related with
progressive and severe course of CIDP, seen in 4 cases.
Figure 1 shows HPE features seen in a case of CIDP, characterized by nonuniform
loss of myelinated fibers and several fibers show thinned out myelin rings,
perivascular inflammation and endoneurial edema within the fascicle, chronic de-
and re-myelination leads to concentric ‘onion bulb’ Schwann cell hyperplasia.
Figure 4 showing nerve biopsy changes in a case of Diabetic neuropathy, showing
thickened perineurial sheath, and endoneurial hyaline arteriosclerosis, a feature of
diabetic microangiopathy. 4E shows a case Diabetic neuropathy with CIDP,
showing endoneurial lymphocytic inflammation, and nerve fibre loss, involving
small more than large myelinated fibers.
9 cases showed evidence of symmetric predominantly demyelination sensori-motor
neuropathy, the mean CSF protein in these cases was 93.9 mg/dl(range 28 – 273
mg/dl) compared to 11 cases showing demyelination and axonopathic changes
(mean CSF protein 80.8 mg/dl, range 24 – 158 mg/dl). 3 cases showing evidence of
acquired demyelination in form of multiple conduction blocks and temporal

44
dispersion, and CSF study showing albumin-cytological dissociation, there was no
evidence of inflammation on sural nerve biopsy and there was uniform distribution
of onion bulbs ( suggestive of CMT).
HPE findings in CIDP (Table – 9)
Nerve biopsy findings Observation (n-24)
Sub-endoneurial edema 17 (71.3%
Myelinated fibre loss ( non-uniform) 18 (78.3 %)
Acute axonal breakdown 30.4 %
De / remyelination Uniform: 10 (43.5 %)
Non-uniform: 12 (52.2 %)
Onion bulb formation 10 (43.5 %)
Bands of Bungner 4 (18.5 %)
Fibrosis Epineurial Endoneurial Perineurial
6 (26.1 %) 10 (43.5 %) 5 (21.4 %)
Epineurial inflammation Endoneurial inflammation Perineurial inflammation
4 (16.7 %) 10 (43.5 %) 6 (26.1 %)
Diabetic micro-angiopathy 6
Endoneurial vascular thickening 39.1 %
Vasculitic neuropathy
Histopathological evidence of vasculitic neuropathy was present in 26 nerve
biopsies. This included 16 patients with definite vasculitis, and 10 patients with
probable vasculitis (as per Collins criteria). The findings are summarized in Table –
10.
Definite vasculitis was demonstrated in 10 patients, with evidence of fibrinoid
necrosis in medial coat seen in 10(55.6 %) cases, best demonstrable in Massons
trichrome stains. There was predominant involvement of nutrient vessels in
45
epineurium, showing segmental infiltration of vascular walls with irregular dilatation
and narrowing, peri-vascular cuffing by lymphocytes, macrophages and plasma cells
in surrounding epineurial small arterioles and venules. 10 cases with probable
vasculitis showed presence of chronic vascular changes and ischemia with medial
hypertrophy and fibrosis narrowing the lumen. 6 cases had mild endoneurial or
epineurial inflammation, along with vascular changes and sectoral loss. Within the
endoneurium, axonal changes were prominent with acute axonal degeneration
being seen in 13(58.8 %) cases, reflecting acute changes, while axonal regeneration
accompanying chronicity was evident in 10(43.5 %) cases. Myelinated fibre
depletion was seen in 12(66.7 %) cases, non-uniform involvement with fascicle to
fascicle variation was common reflecting ischemia, with some cases demonstrating
sectoral loss in central/perifascicular distribution. Presence of sectoral loss of
myelinated fibres and hemosiderin deposits reflected ongoing vascular injury.
The pre-biopsy diagnosis in these cases was mononeuritis multiplex (n–13), CIDP (n-
3), and neuropathy with undetermined etiology (n-10).
Figure 1 shows nerve biopsy in a case of vasculitic neuropathy, showing inflamed
nutrient blood vessel (large arteriole) in the epineurium exhibiting marked vascular
wall thickening, striking luminal narrowing, and dense perivascular and transmural
inflammation (inflammation extending through the vessel wall). Acute axonal
breakdown (Wallerian degeneration) is evident as clear spaces caused by acute
axonal swelling and granular breakdown of the axoplasm, and the fibre loss is
sectorial and non uniform.

46
Muscle biopsy showed evidence of vasculitis in 3 cases, involving most frequently
small vessels in perimysium or epimysium. Lip biopsy revealed evidence of
sialadenitis in 2 cases, with a clinical diagnosis of Sjogrens syndrome.
HPE results in vasculitis (Table – 10)
Nerve biopsy findings Observation (n-23)
Sub-endoneurial edema 2 (2.7%)
Myelinated fibre loss ( non-uniform) 12 (66.7 %)
Acute axonal breakdown 58.8 %
De / remyelination Uniform : 1 (5.6 %)
Non-uniform : 16 (88.9 %)
Fibrosis Epineurial Endoneurial Perineurial
4 (22.2 %) 6 (33.3 %) 4 (22.2 %)
Epineurial inflammation Endoneurial inflammation Perineurial inflammation
16 (88.8 %) 13 (72.3 %) 15 (83.4 %)
Fibrinoid necrosis of epineurial vessels 10 (55.6 %)
Epineurial vascular changes Vascular thickening Neovascularisation
6 (33.3 %) 2(11.8 %)
Endoneurial vascular thickening Neovascularisation
5.9 % 41.2 %
Hansen’s disease
Nerve biopsy was helpful in 6 cases, to confirm the diagnosis of Hansens disease.
Out of these 6 cases, 4 cases were clinically diagnosed as Hansens disease –
presentation with mononeuritis multiplex, and evidence of hypopigmented skin
patches. One case was a known case of Hansens disease, who had completed course
of MDT nearly one year back, who now presented with ulnar mononeuropathy.
47
Nerve biopsy was helpful to confirm diagnosis of chronic leprous neuritis, in a case
presenting with proximal weakness and areflexia, with evidence of hyper pigmented
skin patches and NCS showing demyelinating neuropathy.
Figure 2 shows features of nerve biopsy in Hansen’s disease, showing expanded
nerve fascicles infiltrated by dense inflammation, forming prominent perineurial
cuffs. 2B shows Hansen’s Neuritis, borderline tuberculoid showing the presence of
a large epithelioid granuloma rimmed by lymphocytes, within a nerve fascicle. 2C
shows case of Hansen’s Neuritis with variable fascicular involvement. 2D shows a
case of borderline lepromatous neuropathy, Fite Faraco stain showing numerous
acid fast Lepra bacilli. 2E is a case of Chronic Hansens disease showing extensive
nerve fibre loss in the myelin stain.
CMT
Three patients who were clinically suspected to have CMT – 1, on the basis of
deformities (champagne-leg deformity, pes cavus, hammer-toes) and there was
evidence of uniform slowing, uniform demyelination had evidence of CMT – 1 on
sural nerve biopsy (uniformly distributed onion bulbs, uniform demyelination).
Three patients, who showed step-wise deterioration with a long history of sensor-
motor complaints, and there was evidence of acquired demyelination (multiple
conduction blocks), inflammatory neuropathy (CSF showing albumin-cytological
dissociation), showed biopsy features suggestive of HMSN-1(lack of inflammation,
and uniformly distributed onion bulbs). CMT – 2 was confirmed in 4 cases

48
presenting clinically as hereditary neuropathy, showing axonopathic changes in
NCS.
Figure 2(F-H) shows histopathological features in a case of HMSN 1, showing
expanded fascicle filled with uniformly distributed concentric Schwann cell hyper
plastic units (‘onion bulbs’), Masson’s trichrome stain for collagen highlighting the
layered pattern of the ‘onion bulbs’ due to alternating layers of collagen and
Schwann cell membrane and uniform reduction in myelinated fibers. Figure 2(I-J)
showing histopathological features in a case of HMSN 2, showing atrophic nerve
fascicle with no ‘onion bulbs’, uniform fiber loss with a striking involvement of large
diameter fibers, and presence of axonal sprouting indicating few regenerating
clusters (three or more myelinated fibers close together).
Figure 4 showing 3 cases : First cases (4G – H), a clinically compatible case of CIDP
showing features of hypertrophic demyelinating neuropathy mimicking a
hereditary etiology, with relatively uniformly distributed ‘onion bulb’, Schwann cell
units, absence of inflammation and mildly thickened epineurial vessels with no
inflammation or vasculitis. Second case (4 I-J). showing a clinically suspected case
of CIDP with histology mimicking HMSN (axonal). Third case (4 K-L), showing a
nerve fascicle with no onion bulbs or inflammation, and a moderate degree of
relatively uniform fiber loss, large fiber loss is somewhat more prominent than
small.
49
Undiagnosed/Idiopathic neuropathies :
Thirty-one patients, with peripheral neuropathy in whom the etiological diagnosis
could not be ascertained, based on the available clinical and laboratory
investigations, underwent nerve biopsy. In these patients, vasculitis was diagnosed
in 7, demyelination in 3 and diabetic neuropathy in 3 cases, and two cases with
Hansens disease. Hence, the nerve biopsy was helpful to yield information which
enabled initiation of definite treatment in 15 out of 31 patients (48.4 %).
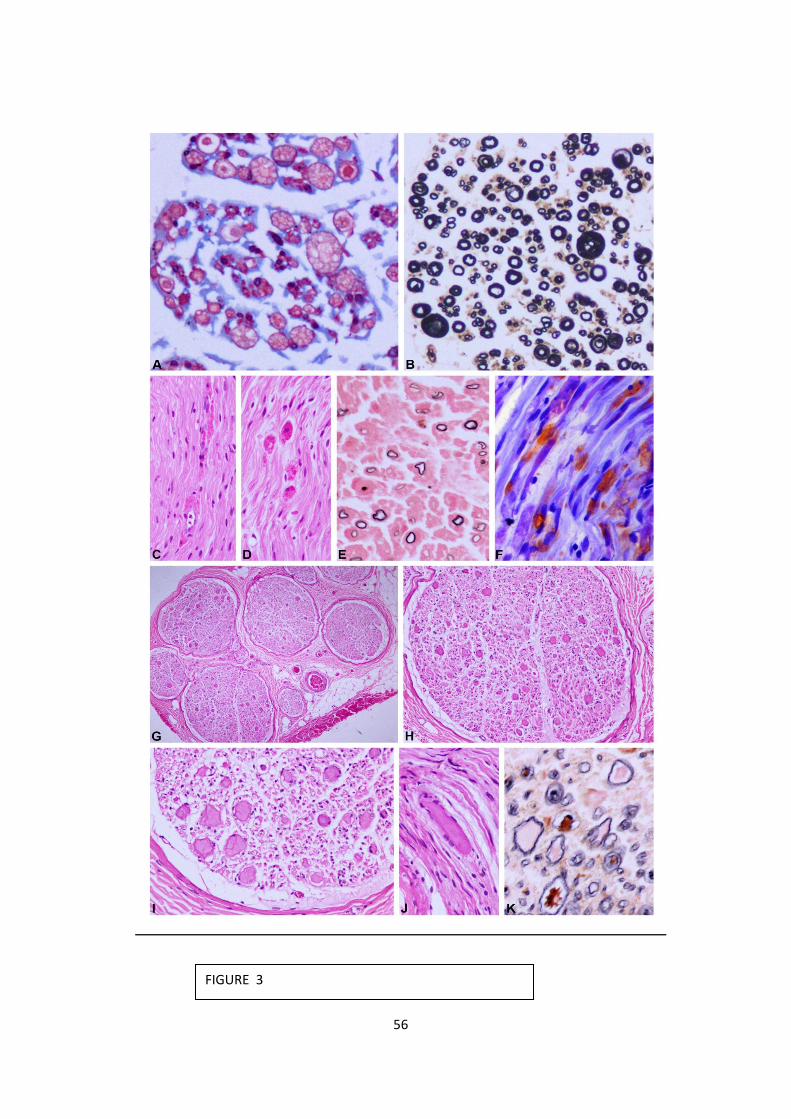
Figure 3(C-F) shows nerve biopsy in Metachromatic Leucodystrophy, displaying
several macrophages with red granular material, demyelination evident on myelin
stain, and metachromatic storage material (sulfatide) showing golden brown color
on staining with cresyl violet (metachromasia). Figure 3(G-K) showing nerve biopsy
in a case of Giant axonal neuropathy (GAN) which displays several enlarged,
markedly distended axons, and thinned out myelin sheaths surround the swollen
axons (secondary demyelination).

50
Co-relation of pre- and post-biopsy diagnosis(Table-11)
Clinically suspected diagnosis
N Biopsy diagnosis N
CIDP 24 CIDP 15
Vasculitis 2
Diabetic polyneuropathy
2
CMT 3
Chronic neuropathy 1
Hansens disease 1
Mononeuritis multiplex
23 Definite vasculitis 9
Probable vasculitis 12
Hansens disease 2
Hansens disease 5 Chronic leprous neuritis
1
BT 2
BL 2
Metachromatic leucodystrophy
1 MLD 1
Undetermined etiology
31 Vasculitis 7
Diabetic neuropathy 3
Hansens disease 2
Chronic axonopathy 15
Demyelination 3
Giant axonal neuropathy
1
CLINICO-PATHOLOGICAL CORELATION
The best possible pre-biopsy diagnosis was arrived at based on the available clinical,
laboratory and electrophysiological data. Clinico-pathological co-relation and
treatment initiated subsequently is summarized in Table – 11. Mononeuritis
multiplex was the most common indication for biopsy in 30 patients. Nerve biopsy
was helpful to confirm the clinical diagnosis of vasculitis in 16 cases, Hansen’s
disease in 2 patients, and establish histopathological diagnosis of vasculitis in 7
patients with undifferentiated neuropathy. These included 3 patients, positive for

51
Anti-Ro, Anti-Jo and Anti-SSA antibodies. 24 patients with clinical diagnosis of CIDP,
nerve biopsy was helpful to confirm the diagnosis in 16 cases, 2 cases had features
suggestive of vasculitis, and 2 cases showed histopathological features of diabetic
neuropathy. Nerve biopsy was thus helpful to delineate the treatment plan in these
groups of patients. 3 cases presenting with long standing neuropathy and
deformities, NCS showing multiple conduction blocks and presence of CSF albumino-
cytological dissociation, Nerve biopsy showed no evidence of inflammation and
uniformly distributed onion bulbs. These patients showed improvement following
immunomodulatory treatment with IVMP, oral steroids.
Utility of nerve biopsy:
In peripheral neuropathy with undetermined etiology, nerve biopsy revealed
diagnostic features in 15 patients, and proved essential for management. This
included cases with vasculitis (n-7), Hansen’s disease (n-2), diabetic neuropathy (n-
3), demyelinating neuropathy with no inflammation(n-3). Nerve biopsy was helpful,
to confirm the clinical / pre-biopsy diagnosis, in 44 cases, these cases included CIDP
(n-16), and mononeuritis multiplex (n-16), Hansens disease (n-5), CMT (n-5),
Metachromatic leucodystrophy and Giant axonal neuropathy one case each. In 3
cases with a pre-biopsy diagnosis of CIDP, 2 turned out to be Diabetic neuropathy,
and one was a non-specific chronic axonopathy. In 16 patients, nerve biopsy was
suggestive of chronic axonopathy, with undetermined etiology. Thus, nerve biopsy
provided some form of information that was helpful in initiating therapy or guided
focused investigation in 63 out of 84 patients(79.7 %).

52
Treatment details following biopsy (Table – 12)
Clinically suspected diagnosis
Biopsy diagnosis Treatment
CIDP(N-24) CIDP(N-16) PLEX (6)
IVIG(5)
IVMP(10)
Oral steroids(6)
Azathiopurine(6)
Cyclophosphamide(1)
MMF(1)
Vasculitis(N-2) IVMP, Oral steroids
Diabetic polyneuropathy(N-2)
Supportive treatment
CMT(N-3) IVMP, oral steroids
Chronic neuropathy(N-1) --
Hansens disease(N-1) MDT
Mononeuritis multiplex (N-23)
Definite vasculitis(N-9) IVMP(16)
Oral steroids(10)
Probable vasculitis(N-11) IVMP(16)
Oral steroids(10
Hansens disease(N-2) MDT
Hansens disease(N-5) Chronic leprous neuritis(N-1)
MDT
BT(N-2) MDT
BL(N-2) MDT
Metachromatic leucodystrophy(N-1)
MLD(N-1) --
Undetermined etiology (N-31)
Vasculitis(N-7) Oral steroids
Diabetic neuropathy (N-3) --
Hansens disease(N-2) MDT
Chronic axonopathy(N-15) --
Demyelination(N-3) --
Giant axonal neuropathy(N-1)
--
Outcomes on follow-up of patients (following initiation of definite treatment)
Response to treatment was decided on the basis of data available in MRD. The
follow-up was available in 62 patients. Among 16 patients diagnosed with CIDP, 4
patients have a gradually progressive course with frequent relapses, on plasma
exchanges. These patients are on regular follow-up, while being on immune-

53
modulation (steroids and azathiopurine). Biopsy was helpful to delineate the
diagnosis of vasculitis in 7 cases with undetermined etiology, thereby initiation of
definite treatment in these cases. However, in 19 cases no definite diagnosis could
be established after biopsy, 12 of these cases are on regular follow-up (10 have
remained status quo, while 2 have shown improvement gradual improvement).

54
FIGURE 1

55
FIGURE 2
56
FIGURE 3

57
FIGURE 4

58
FIGURE 1:
A- E: Chronic inflammatory demyelinating polyneuropathy (CIDP). A: An expanded
nerve fascicle is surrounded by thickened perineurium. B: Perivascular
inflammation and endoneurial edema within the fascicle. C: The myelin special
stain reveals a nonuniform loss of myelinated fibers and several fibers show
thinned out myelin rings indicating demyelination. D-E: Chronic de- and re-
myelination leads to concentric ‘onion bulb’ Schwann cell hyperplasia which in this
figure is prominent throughout the fascicle mimicking a hereditary etiology,
however the myelin stain reveals the strikingly nonuniform affection of the fascicle
indicating the acquired nature of the underlying pathology (E).
F-M: Vasculitic neuropathy. F-G: The inflamed nutrient blood vessel (large arteriole)
in the epineurium exhibits marked vascular wall thickening, striking luminal
narrowing, and dense perivascular and transmural inflammation (inflammation
extending through the vessel wall) (G). H: Vasculitis involving the smaller calibre
vessels. The adjacent nutrient vessel is not involved. I-J: Acute axonal breakdown
(Wallerian degeneration) is evident as clear spaces caused by acute axonal swelling
and granular breakdown of the axoplasm. This is seen in the longitudinal section (J)
as myelin ovoids formed by secondary collapse and breakdown of the myelin
consequent to acute axonal loss of integrity. K: Chronic vasculitis with past micro
bleeds may lead to hemosiderin pigment formation (K) whose detection is made
easier by the Perl’s Prussian blue stain (inset). L: Shows a previously thrombosed

59
vessel with reparative recanalisation of the lumen. M: The fibre loss is sectorial and
non uniform (M).
FIGURE 2:
A-E: Hansen’s Neuritis. A: Expanded nerve fascicles are infiltrated by dense
inflammation, forming prominent perineurial cuffs. B: Hansen’s Neuritis,
borderline tuberculoid. A large epithelioid granuloma rimmed by lymphocytes, is
seen within a nerve fascicle. C: Hansen’s Neuritis. Variable fascicular involvement is
evident. D: Fite Faraco stain shows numerous acid fast Lepra bacilli in a case of
borderline lepromatous neuropathy. E: Extensive nerve fibre loss in Hansen’s
neuritis in the myelin stain.
F-H: Hereditary demyelinating neuropathy - HMSN 1. F: The fascicle is expanded
and filled with uniformly distributed concentric schwann cell hyperplastic units
(‘onion bulbs’).
G: Masson’s trichrome stain for collagen highlights the layered pattern of the
‘onion bulbs’ due to alternating layers of collagen and Schwann cell membrane. H:
Uniform reduction in myelinated fibers- a feature characteristic of hereditary
neuropathy.
I-J: Hereditary axonal neuropathy - HMSN 2. I: The nerve fascicle is mildly atrophic
with no ‘onion bulbs’. J: Uniform fiber loss with a striking involvement of large
diameter fibers. Few regenerating clusters (three or more myelinated fibers close

60
together) are present indicating axonal sprouting as a reparative reaction of
chronic axonopathy.
(Stains- A,B,C,F,I : H&E. G: Masson’s trichrome. D: Fite Faraco for lepra bacilli. E,H:
Kpal for myelin.
Original magnification: D: x400; F,G, E,H,J: x200; B,C,I: x100; A x40).
FIGURE 3:
A-B: Hereditary neuropathy with liability to pressure palsies (HNPP). A: A fiber with
very thick myelin sheath stands out amidst fibers with myelin sheaths of normal
thickness. B: The myelin stain highlights two such hypermyelinated fibers
(‘tomaculi’).
C-F: Metachromatic Leukodystrophy. C-D: Longitudinal sections display several
macrophages with red granular material. E: The myelin stain reveals thin myelin
sheaths indicating demyelination. F: Metachromatic storage material (sulfatide)
shows golden brown colour on staining with cresyl violet (metachromasia).
G-K: Giant axonal neuropathy (GAN) G-I: Transverse sections display several
enlarged, markedly distended axons. J: Longitudinal section of the segmentally
bloated axon.
K: Thinned out myelin sheaths surround the swollen axons (secondary
demyelination).

61
(Stains- C,D,G,H,I,J: H&E. A: Masson’s trichrome. E&K: Kpal for myelin. F: Cresyl
violet.
Original magnification: A,K,F: x400; B,C,D,E,J,K: x200; H x100; G x40).
FIGURE 4:
A-F: Diabetic neuropathy. A: Low power view of a nerve fascicle bordered by
thickened perineurial sheath. B-C: Endoneurial hyaline arteriosclerosis, a feature of
diabetic microangiopathy. D: Chronic axonopathy. The endoneurium contains
numerous ‘Bands of Bungner’ - empty Schwann cell units. E: Diabetic neuropathy
with CIDP. Endoneurial lymphocytic inflammation. F: Diabetic neuropathy. Fiber
loss, involving small more than large myelinated fibers.
G-J: A clinically compatible case of CIDP showing features of hypertrophic
demyelinating neuropathy mimicking a hereditary etiology. G: Moderately
expanded nerve fascicles. H: Relatively uniformly distributed ‘onion bulb’, Schwann
cell units. Note the absence of inflammation. I: Thinly myelinated fibers. J: Mildly
thickened epineurial vessels with no inflammation or vasculitis.
K-L: A clinically suspected case of CIDP with histology mimicking HMSN (axonal)
K: Nerve fascicle with no onion bulbs or inflammation. L: A moderate degree of
relatively uniform fiber loss, large fiber loss is somewhat more prominent than
small.
(Stains- A,B,D,E,G-K: H&E. C: Masson’s trichrome. F&L: Kpal for myelin.
Original magnification: I: x400; B,C,D,E,H, K: x200; A, F, L: x100; G x40).

62
DISCUSSION
The diagnostic work-up in patients with peripheral neuropathy is tailored to each
individual based on the presenting history and examination, topographic pattern
and evolution of clinical signs. Even after detailed evaluation, in 20 % of axonal
neuropathies, the etiology remains elusive. 63 In this study, we studied the clinical-
pathological data of 84 subjects with established diagnosis of peripheral
neuropathy who underwent nerve biopsy.
Clinical features
A male pre-ponderance of patients was noted in our study, with Male: Female ratio
being 53 : 31. Study by Chia etal, also reports majority of subjects being males 64.
Majority of cases (88 %) presented with a chronic progressive clinical course,
similar to study by Chia et al, who also reported a chronic course in 68 % of the
patients at the time of biopsy 64. Majority of patients (19) were in between the age
group 60-70 years, in addition 11 patients were between age group 50-60 years
and 10 each in between the age group 10-20 years and 30-40 years. In nearly 54
cases (77 %), the symptom onset was in lower limbs (77 %, n – 54), with sensory
disturbances in form of paraesthesias in 32.9 %, and sensory loss in 17.7 % of
patients. Proprioceptive loss was documented in 36 (45.6 %) patients, impaired
pain and temperature in 38 (47.5 %) patients. Pan-sensory loss involving all
modalities was present in 57.6 % patients. Motor system involvement in form of
wasting was noticed in 21.6 % of patients and weakness was noticed in 77.4 %

63
patients. Study by Chia et al, reported motor deficits in 71 %, paraesthesias of
varying severity in 76 %, and sensory loss in 83 % of patients, and most patients
had distal predominant type of neuropathy, documented in nearly 40.2 %64.
The most common pattern was symmetrical sensori-motor axonopathic
neuropathy (29.1 %), followed by asymmetric sensori-motor axonopathic
neuropathy(20.3 %) and mononeuropathy multiplex (17.7 %). Sensori-motor
demyelinating neuropathy with superimposed axonopathic changes were present
in 27.8 % cases. Six patients had evidence of conduction blocks and temporal
dispersion. Chia et al reported distal and symmetrical pattern in 56 % of patients,
distal asymmetrical in 15 % of the patients, and focal/multifocal in 29 % of the
patients 64.
Co-morbidities
The co-morbidities of these patients were noted to assess the role of these factors
in the causation or contribution in each case. Diabetes mellitus was present in 25.5
% of total number of cases in this study. Chia et al reported 6 patients with
diabetes mellitus out of 100 patients who underwent nerve biopsy for disabling
neuropathy 64. Other co-morbidies included Systemic hypertension (7.5 %),
Coronary artery disease (6.5 %), and hypothyroidism (5.1 %). A history of
malignancy was present in 2 cases, in whom a paraneoplastic etiology was
suspected, and 4 cases had history suggestive of undifferentiated polyarthritis in
past.

64
Vasculitic neuropathy
Nerve biopsy was indicated in 23 cases presenting with clinical profile suggestive of
mononeuritis multiplex. Among these patients clinically suspected to have
vasculitis (n- 23), nerve biopsy confirmed the presence of vasculitis in 20 patients
including 9 patients with definite vasculitis and 11 patients with probable vasculitis.
Thus 86.9 % of patients in whom vasculitis was clinically suspected had biopsy
confirmation. Hansen’s disease was diagnosed in one patient from the group with
clinically suspected vasculitis.
Overall, 30 patients had a biopsy diagnosis of vasculitis, including 10 patients with
definite vasculitis and 20 patients with probable vascultis. This is lower when
compared to the study by Chia et al where 35 patients had evidence of vasculitis in
nerve biopsy 64. In a retrospective review of 355 patients, Deprez etal found that
vasculitis was suspected in 10 % of patients, and nerve biopsy provided helpful and
essential information in 50-60 % of patients, this study showed that findings
specific or highly suggestive of necrotizing vasculitis were found in 18 patients with
a mean age of 58 years16. Prayson reported that a significant proportion of
vasculitic neuropathies occurs in the setting of systemic vasculitis, most commonly
polyarteritis nodosa, or may be confined to peripheral nervous system 65. In
patients with systemic vasculitis, a polyneuropathy picture is the most common, in
contrast to isolated peripheral nervous system vasculitis, where a mononeuropathy
multiplex pattern is seen 65. Rheumatoid arthritis is one of the common causes of
systemic vasculitis. The histological findings overlap with those of polyarteritis
65
nodosa, and include necrotizing vasculitis of epineurial vessels42. Peripheral
neuropathy complicates SLE in nearly 5 – 22 % cases, and Sjogrens syndrome in 5 –
40 % of cases. Neuropathy in SLE is usually a distal symmetrical polyneuropathy.
Sjogrens syndrome commonly manifests as sensory ganglionitis, autonomic
neuropathy, or polyneuropathy 43. Peroneal nerve is the most frequently affected
peripheral nerve in vasculitic neuropathy. Sural nerve is invariably affected in
length dependant neuropathies like diabetic or alcoholic neuropathy; it is not the
most common site of affection by vasculitic neuropathy 66. In fact, sural nerve
yields unequivocal evidence of vasculitis in only 20 % of cases compared to
peroneal nerve biopsy that has a sensitivity of 60 %32, 49. Sural nerve biopsy was
done in 24 cases. In 4 patients with predominant upper limb involvement, biopsy of
dorsal cutaneous branch of ulnar nerve was done in 3 patients, and superficial
branch of radial nerve biopsy in one patient. In ten patients, a combined nerve –
muscle biopsy was done, out of a pre-biopsy diagnosis of vasculitis was offered in
23 patients. Combined nerve-muscle biopsy was additionally useful to diagnose
vasculitis in 3 cases. Previous studies have shown that combined superficial
peroneal nerve and peroneus tertius muscle biopsy increases the diagnostic yield
for vasculitis by 15 – 40 % 16, 32, 49. Patients with isolated vasculitis of the peripheral
nervous system have a better prognosis and response to immunomodulatory
therapy compared to those with systemic vasculitis. Some patients with vasculitis
restricted to peripheral nervous system may eventually develop evidence of
systemic disease 65. Of the 30 patients, in the present cohort who was proven to
have vasculitis by biopsy, 4 had a systemic vasculitic disorder characterized by

66
positive auto antibodies. In the remaining 26 patients, non-systemic vasculitis or
isolated vasculitis of peripheral nervous system was considered. The nerve biopsy
has an unchallenged role in the diagnosis of these patients for whom a diagnosis of
vasculitis in the nerve cannot be obtained by any other means. This large
proportion of patients (32 %), who are potentially treatable with immune-
modulators, justifies the role of nerve biopsy in the management.
Hansen’s disease was seen in 6 patients in our study. This is higher than that
reported in other studies of neuropathy. This is probably a reflection of the endemic
nature of the disease. Out of these 6 cases, 4 cases were clinically diagnosed as
Hansen’s disease – presentation with mononeuritis multiplex, and evidence of
hypopigmented skin patches. Nerve biopsy was helpful to confirm leprous neuritis in
2 cases, with neuropathy and undetermined etiology.
Diabetic neuropathy
Two cases had superimposed changes suggestive of diabetic neuropathy and CIDP,
characterized by endoneurial lymphocytic inflammation, and fiber loss, involving
small more and large myelinated fibers. Three cases showed features of diabetic
neuropathy, with thickened perineurial sheath, and endoneurial hyaline
arteriosclerosis, a feature of diabetic microangiopathy. Diabetes mellitus was
present in 21(25.5 %) cases in our study. In the largest clinical studies of
neuropathy in the elderly, diabetes was found to be the commonest cause of

67
neuropathy accounting for 41 % of all cases. This declined with age, commensurate
with an increased proportion of idiopathic neuropathies 67.
CIDP
The diagnosis of CIDP was established in 24 cases on the basis of clinical,
electrophysiological results (as per EFNS 2010 guidelines). Sural nerve biopsy
findings were consistent with diagnosis of CIDP in 16 cases. The most common
histopathological findings were non-uniform loss of myelinated fibres in 78.3 %
cases and evidence of demyelination/remyelination, followed by sub-endoneurial
edema, in 71.3 % cases, endoneurial inflammation in 43.5 % cases and non-
uniform distribution of onion bulbs in 28 % cases. Epineurial inflammation and
axonopathic changes co-related with progressive and severe course of CIDP, seen
in 4 cases. In a study done by Vallat et al, out of 44 suspected cases of CIDP, nerve
biopsy examination was helpful for diagnosis of CIDP in 8 patients (demyelination,
loss of myelinated fibers, cellular infiltrates, and onion bulb proliferation). who
These eight patients had normal results on nerve conduction studies, and based on
histopathology results they were started on immunomodulation, and showed a
significant positive response. 35 In a study done by Kulkarni et al , in forty-six
patients with idiopathic CIDP at NIMHANS, (32 with progressive course and 14 with
relapsing-remitting course) satisfying AAN clinical and electrophysiological criteria
for CIDP, frequency of four supportive pathological alterations - demyelination,
inflammation, onion bulb formation, and axonal changes in sural nerve biopsies
were seen in nearly 100% of cases. Electrophysiological abnormalities were

68
detected in 90.8%, suggesting that supportive histologic AAN criteria are helpful in
diagnosis of CIDP 37.
Endoneurial inflammation was frequent in the relapsing-remitting form and
epineurial inflammation and axonal changes in those with progressive course.
Greater disability at presentation, poor response to immunomodulation, and lower
CSF protein levels was seen in those with axonal pathology. In addition, 3 cases
which had shown evidence of acquired demyelination in form of multiple
conduction block and temporal dispersion, and CSF study showing albumin-
cytological dissociation, there was no evidence of inflammation on sural nerve
biopsy and there was uniform distribution of onion bulbs ( suggestive of CMT).
Patients with no pre-biopsy diagnosis
31 patients had no pre-biopsy diagnosis. Nerve biopsy revealed vasculitis in 7
patients, with 1 case showing definite vasculitis, and 6 cases showing features of
probable vasculitis. A diagnosis of Hansen’s disease was made in 2 cases and
features suggestive of diabetic neuropathy were present in 3 cases. One case
showed features suggestive of Giant axonal neuropathy on nerve biopsy. In 15
cases, chronic axonopathy was found without further clues from the nerve biopsy.
Thus nerve biopsy proved to be essential in 3 cases, and helpful in 12 cases out of
31 cases with un-determined etiology. In 15 cases (52 %), the biopsy was either
essential (n-3) or helpful (n-12). Hence, nerve biopsy findings were useful in this
group with no definite pre-biopsy diagnosis despite investigations and had been

69
useful for guiding treatment and prognosis in 15 out of 31 cases. This would be
helpful in resource limited settings, wherein financial and human resources are
limiting factors.
Nerve biopsy: utility and side effects
The indication for performing nerve biopsy should be balanced against the
expected diagnostic yields and post-surgical complications after biopsy. The
diagnostic yield of nerve biopsy ranges from 24 – 94 % 1, 12, 16, 68. Nerve biopsy is
associated with residual complications and morbidity in 33 % of patients 1.
20 patients who underwent nerve biopsy were diagnostic in our study including 9
patients with definite vasculitis, 5 patients with Hansens disease and 6 patients
with features of inflammatory demyelinating neuropathy. These biopsies confirmed
the diagnosis in each case. Another 40 patients with nerve biopsies, biopsy was
helpful, since the findings helped to confirm, or exclude the clinical diagnosis.
These included 18 cases with probable and possible vasculitis, 13 cases with
inflammatory demyelinating neuropathy, 5 cases with Hansens disease, 2 cases
with diabetic neuropathy and chronic axonopathy(with past history of nutritional
neuropathy). Nerve biopsy was not helpful in 16 patients.
The current study shows that nerve biopsy proved to be essential and helpful in 20
patients and 40 patients respectively. Several studies have shown varying results
of yield of nerve biopsy in peripheral neuropathies. Study on 44 cases of peripheral
neuropathy undergoing nerve biopsy, Gabriel et al concluded that nerve biopsy
70
contributed in the therapeutic management in nearly 60 % of patients and
confirmed the suspected diagnosis in 70 %. The biopsy altered the diagnosis in 14
%, and was non-contributory in 16 % 1. Another study by Neundorfer et al showed
that 27 % of nerve biopsies were essential, by establishing definite diagnosis, and
37 % of biopsies were helpful, by providing valuable diagnostic information
confirming the clinical diagnosis68. Similarly, study by Oh et al reported that 24 %
of biopsies established specific diagnosis and provided helpful or diagnostic
information in 45 % 12. Chia et al showed a much higher yield of nerve biopsy, being
diagnostic in 94 % of patients, by making use of combination of histological and
clinical data64 .
Several clinical and histo-pathological factors affect the diagnostic yield of nerve
biopsy16. The pre-biopsy diagnosis of vasculitis, inflammatory demyelinating
disease, HMSN, distribution of symptoms in a multifocal and asymmetrical fashion
and symptom onset to biopsy interval of less than 6 months are associated with a
better yield. The higher yield in multifocal and asymmetric neuropathies is related
to a high proportion of vasculitis in these patients 16. Combined muscle nerve
biopsy increased the diagnostic yield for vasculitis, and serial sections on frozen
paraffin embedded and resin embedded material improves the sensitivity for
diagnosis of interstitial pathology.
In our study, 14 patients had axonal neuropathy of unknown etiology. Previous
studies have shown that despite extensive evaluation, the etiology of neuropathy
remains undiagnosed in 10 to 20 % of patients. These patients most commonly

71
have axonal polyneuropathy, this entity is called Chronic Idiopathic Axonal
Polyneuropathy (CIAP)69. This disorder presents with an insidious onset, slowly
progressive distal symmetrical sensory or sensori-motor symptoms in the 6th
decade, and is not associated with severe disability even after 5-10 years into the
disease process69.

72
SUMMARY AND CONCLUSION
This retrospective study analyzed 84 patients with established diagnosis of
peripheral neuropathy who had undergone nerve biopsy at SCTIMST during the
period 2010-2015, to determine the clinical, electrophysiological and pathological
profile of peripheral neuropathy and further examine the utility of nerve biopsy in
providing diagnostic, therapeutic or prognostic information in the clinical
management of patients with peripheral neuropathy.
Majority were males (M: F= 53:31), with a mean age at nerve biopsy of 59.8
years. The mean duration of symptoms(prior to nerve biopsy) was 12.6
months.
Majority of patients (n-19) were in the age group 60-70 years, 11 patients
were in the age group 50-60 years and 10 each in the age group 10-20 years
and 30-40 years, respectively.
The majority of patients had chronic progressive clinical course, seen in 79.7
% patients. Motor involvement (weakness in 84.8 % and wasting in 19 %)
was more common than sensory symptoms in the form of paraesthesias (43
%), impaired sensations (22.8 %).
Most common co-morbidities seen in this group of patients were Diabetes
mellitus(25.5 %), and Hypertension(7.5 %) cases.
Most common clinical and electrophysiological pattern of neuropathy
observed was Symmetric sensori-motor axonopathic neuropathy (29.1 %),

73
sensori-motor predominantly demyelinating neuropathy (27.8 %), followed
by mononeuritis multiplex (17.7 %) cases.
53 (63 %) patients had a pre-biopsy etiological diagnosis on the basis of
available data. The pre-biopsy diagnosis was CIDP (n-21), vasculitis(n-20),
Hansens disease(n-5), Metachromatic leucodystrophy(n-1). In the rest (n-
31), no definite etiological cause for neuropathy could be established
before biopsy.
Most common histopathological features seen in patients with CIDP were
non-uniform loss of myelinated fibres (78.3 %), followed by sub-endoneurial
edema (71.3 %), endoneurial inflammation (43.5 %) and non-uniform
distribution of onion bulbs (28 %) cases. Epineurial inflammation and
axonopathic changes co-related with progressive and severe course of CIDP,
seen in 4 cases.
Most common histopathological features in patients with definite vasculitis
were fibrinoid necrosis in medial coat (55.6 %), peri-vascular cuffing by
lymphocytes, macrophages and plasma cells in surrounding epineurial small
arterioles and venules (51.6 %), medial hypertrophy and fibrosis narrowing
the lumen(30.6 %) and evidence of acute axonal degeneration (28.8 %)
cases.
Among 24 cases with pre-biopsy diagnosis of CIDP, nerve biopsy
histopathology confirmed the clinical diagnosis in 15 cases,
histopathological diagnosis in the remaining 9 cases was: vasculitis (n-2),
diabetic polyneuropathy(n-2), CMT(n-3), Hansens disease(n-1) and chronic

74
neuropathy(n-1). Histopathological diagnosis in 23 cases with prebiopsy
diagnosis of mononeuritis multiplex was definite vasculitis(n-9), probable
vasculitis(n-12), and Hansens disease(n-2). Nerve biopsy confirmed the
clinical diagnosis of Hansens disease(n-5), and Metachromatic
leucodystrophy(n-1).
In 31 cases(37 %) without definite diagnosis, despite extensive work-up,
nerve biopsy proved to be essential in 3 cases (definite vasculitis-1,
Hansen’s disease-2). Besides, nerve biopsy was helpful in 12 cases (probable
vasculitis-6, diabetic neuropathy-3, Giant axonal neuropathy-1,
demyelinating neuropathy without inflammation-2). Thus, nerve biopsy
proved to be essential and helpful in 16 out of 31 cases with no pre-biopsy
diagnosis (51.6 %).
Our study suggests that nerve biopsy becomes useful in potentially
treatable peripheral neuropathies, particularly in patients with
Mononeuritis multiplex, or in patients with undetermined etiology. Also it
clarified the etiology in patients presenting with demyelinating CIDP.

75
REFERENCES
1. Gabriel CM, Howard R, Kinsella N, Lucas S, McColl I, et al. (2000) Prospective
study of the usefulness of sural nerve biopsy. J Neurol Neurosurg Psychiatry
69: 442-446.
2. Argov Z, Steiner I, Soffer D (1989) The yield of sural nerve biopsy in the
evaluation of peripheral neuropathies. Acta Neurol Scand 79: 243-245.
3. Rappaport WD, Valente J, Hunter GC, Rance NE, Lick S, et al. (1993) Clinical
utilization and complications of sural nerve biopsy. Am J Surg 166: 252-256.
4. Hellmann DB, Laing TJ, Petri M, Whiting-O'Keefe Q, Parry GJ (1988).
Mononeuritis multiplex: the yield of evaluations for occult rheumatic
diseases. Medicine (Baltimore) 67: 145-153.
5. Said G, Lacroix-Ciaudo C, Fujimura H, Blas C, Faux N (1988) The peripheral
neuropathy of necrotizing arteritis: a clinicopathological study. Ann Neurol
23: 461-465.
6. Gaurie Devi M, Gururaj G, Satishchandra P, Subbakrishna DK. Prevalence of
neurological disorders in Bangalore, India : a community-based study with a
comparison between urban and rural areas. Neuroepidemiology. 2004;
23(6) : 261-8.
7. Bharucha NE, Bharucha AE, Bharucha EP. Prevalence of peripheral
neuropathy in the Parsi community of Bombay. Neurology. 1991; 41(8):
1315 – 7.

76
8. Beghi E, Monticelli ML. Chronic symmetric symptomatic polyneuropathy in
the elderly : a field screening investigation of risk factors for polyneuropathy
in two Italian communities. Italian General Practitioner Study
Group(IGPST). J Clin Epidemiolo. 1998;51(8) : 697 – 702.
9. Beghi E, Monticelli ML. Chronic symmetric symptomatic polyneuropathy in
the elderly : a field screening investigation in two Italian regions. Italian
General Practitioner Study Group(IGPST). Neurology. 1995; 45(10) : 1832 –
6.
10. Kathi Schweikerta Peter Fuhra Alphonse Probstb Marcus Tolnayb Susanne
Renauda Andreas J. Steck ; Contribution of Nerve Biopsy to Unclassified
Neuropathy. Eur Neurol 2007;57:86–90.
11. Wees SJ, Sunwoo IN, Oh SJ. Sural nerve biopsy in systemic necrotizing
vasculitis. Am J Med 1981 ; 71 (4) : 525 – 32.
12. Oh SJ. Diagnostic usefulness and limitations of the sural nerve biopsy.
Yonsei Med J. 1990;31 (1) : 1 – 26.
13. Collins MP, Mendell JR, Periquet MI, et al. Superficial peroneal
nerve/peroneus brevis muscle biopsy in vasculitic neuropathy. Neurology
2000;55:636–43.
14. Vital C, Vital A, Canron MH, et al. Combined nerve and muscle biopsy in the
diagnosis of vasculitic neuropathy. A 16-year retrospective study of 202
cases. J Peripher Nerv Syst 2006;11:20–9. .

77
15. D L H Bennett, M Groves, J Blake, J L Holton. The use of nerve and muscle
biopsy in the diagnosis of vasculitis: a 5 year retrospective study. J Neurol
Neurosurg Psychiatry 2008;79:1376–1381
16. M. Deprez, C. Ceuterick-de Grooteb, L. Gollogly, M. Reznik, J.J. Martin.
Clinical and neuropathological parameters affecting the diagnostic yield of
nerve biopsy; Neuromuscular Disorders 10 (2000) 92 - 98.
17. Research criteria for diagnosis of chronic inflammatory demyelinating
polyneuropathy (CIDP). Report from an Ad Hoc Subcommittee of the
American Academy of Neurology AIDS Task Force. Neurology 1991;41:617–
8.
18. Van den Bergh PY, Hadden RD, Bouche P, et al. European Federation of
Neurological Societies/Peripheral Nerve Society guideline on management
of chronic inflammatory demyelinating polyradiculoneuropathy: report of a
joint task force of the European Federation of Neurological Societies and
the Peripheral Nerve Society: first revision. Eur J Neurol 2010;17:356–363..
19. Girish B. Kulkarni, Anita Mahadevan, Arun B. Taly, A. Nalini, S.K. Shankar.
Sural nerve biopsy in chronic inflammatory demyelinating polyneuropathy:
Are supportive pathologic criteria useful in diagnosis? Neurology India 2010
20. Dyck PJ, Lais AC, Ohta M, Bastron JA, Okazaki H, Groover RV. Chronic
inflammatory polyradiculoneuropathy. Mayo Clin Proc. 1975;50:621-37.
21. D S M Molenaar, M Vermeulen, R de Haan Diagnostic value of sural nerve
biopsy in chronic inflammatory demyelinating polyneuropathy. J Neurol
Neurosurg Psychiatry 1998;64:84-89

78
22. Kieseier BC, Tani M, Mahad D, Oka N, Ho T, Woodroofe N, et al. Chemokines
and chemokine receptors in inflammatory demyelinating neuropathies: a
central role for IP-10. Brain 2002;125:823-34.
23. Sommer C, Koch S, Lammens M, Gabreels-Festen A, Stoll G, Toyka KV.
Macrophage clustering as a diagnostic marker in sural nerve biopsies of
patients with CIDP. Neurology 2005;65:1924-9.
24. Prineas JW, McLeod JG. Chronic relapsing polyneuritis. J Neurol Sci
1976;27:427-58.
25. Barohn RJ, Kissel JT, Warmolts JR, Mendell JR. Chronic inflammatory
demyelinating polyradiculoneuropathy. Clinical characteristics, course, and
recommendations for diagnostic criteria. Arch Neurol 1989;46:878-84.
26. Krendel DA, Parks HP, Anthony DC, St Clair MB, Graham DG. Sural nerve
biopsy in chronic inflammatory demyelinating polyradiculoneuropathy.
Muscle Nerve 1989;12:257-64.
27. Bouchard C, Lacroix C, Planté V, Adams D, Chedru F, Guglielmi JM, et al.
Clinicopathologic findings and prognosis of chronic inflammatory
demyelinating polyneuropathy. Neurology 1999;52:498-503.
28. Haq RU, Fries TJ, Pendlebury WW, Kenny MJ, Badger GJ, Tandan R. Chronic
inflammatory demyelinating polyradiculoneuropathy: a study of proposed
electrodiagnostic and histologic criteria. Arch Neurol 2000;57:1745-50.
29. Rizzuto N, Morbin M, Cavallaro T, Ferrari S, Fallahi M, Galiazzo Rizzuto S.
Focal lesions area feature of chronic inflammatory demyelinating
polyneuropathy (CIDP). Acta Neuropathol 1998;96:603-9.

79
30. Vital C, Vital A, Lagueny A, Ferrer X, Fontan D, Barat M, et al. Chronic
inflammatory demyelinating polyneuropathy: immunopathological and
ultrastructural study of peripheral nerve biopsy in 42 cases. Ultrastruct
Pathol 2000;24:363-9.
31. Vallat JM, Tabaraud F, Magy L, Torny F, Bernet-Bernady P, Macian F, et al.
Diagnostic value of nerve biopsy for atypical chronic inflammatory
demyelinating polyneuropathy: evaluation of eight cases. Muscle Nerve
2003;27:478-85.
32. W. M. J. Bosboom, L. H. van den Berg, H. Franssen, Diagnostic value of
sural nerve demyelination in chronic inflammatory demyelinating
polyneuropathy. Brain 2001(124) 2427-38.
33. Jann S, Bramerio MA, Beretta S, et al.: Diagnostic value of sural nerve matrix
metalloproteinase-9 in diabetic patients with CIDP. Neurology 2003,
61:1607–1610.
34. Nemni R, Sanvito L, Quattrini A, et al.: Peripheral neuropathy in hepatitis C
virus infection with and without cryoglobulinaemia. J Neurol Neurosurg
Psychiatry 2003, 74:1267–1271.
35. Said G, Lacroix C, Planté-Bordeneuve V, et al.: Nerve granulomas and
vasculitis in sarcoid peripheral neuropathy. Brain 2002, 125:264–275
36. Dyck PJ, Benstead TJ, Conn DL, Stevens JC(1987). Nonsystemic vasculitic
neuropathy. Brain ; 110:843-53.
37. Guillevin et al (2001); HBV related PAN . Arthritis Rheumat; 43 (suppl) s 271

80
38. Hattori N, Ichimura M, Nagamatsu M et al. Clinicopathological features of
Churg Strauss syndrome – associated neuropathy. Brain 1999; 122 : 427-39.
39. deGroot K, Arlt AC; standardized neurological evaluation of 128 patients
with Wegeners granulomatosis; Arch Neurol 58 : 1215;2001
40. Nishino H, Rubino FA, DeRemee RA (1993) . Neurological involvement in
Wegeners granulomatosis : analysis of 324 consecutive patients at Mayo
clinic. Ann Neurology : 33-4.
41. Kissel JT, Slivika AP, Warmolts JR, Mendell JR (1992) ; Vasculitic neuropathy.
Neurol clinics 1992; 10: 761-81.
42. Puechal X, Said G, Hilliquin P et al (1995) ; Peripheral neuropathy with
necrotizing vasculitis in Rheumatoid arthritis : a clinicopathologic and
prognostic study of 32 patients. Arthritis Rheumat; 38 : 1618.
43. Gemignani F, Pavesi G (1994) ; Peripheral neuropathy associated with
Sjogrens syndrome. J. Neurology Neurosurg Psychiatry 57 : 983-986.
44. Hietaharju A, Kalimo H (1993) ; Peripheral neuromuscular manifestations of
systemic sclerosis. Muscle nerve ; 16 : 1204-12.
45. Sbai A, Duhatt DL (2002); Neurological complications in Behcets disease –
evaluation of 109 patients. Arthritis Rheumat; 46 : s 180.
46. Belman AL, Leicher CR, Moshe SL (1985). Neurological manifestations of
Henoch Schonlein purpura : report of 3 cases and review of literature.
Pediatrics ; 75 : 687.
47. Caselli R, Hunder GG (1988) ; Peripheral neuropathic syndromes in giant cell
arteritis. Neurology 38: 685-689.

81
48. Schaublin GA, Clement J, Burns TM (2005) ; An update on classification and
treatment of vasculitic neuropathy. Lancet Neurol ; 4 : 853-65.
49. Vrancken AF, Notermans NC, Said G (2011); The additional yield of
combined muscle/nerve biopsy in vasculitic neuropathy, European Journal
of neurology : 18; 49-58.
50. Collins MP, Dyck PJ, Hadden RD (2010) : Peripheral nerve society guideline
on the classification, diagnosis, investigation and immunosuppressive
therapy of non-systemic vasculitic neuropathy : executive summary. Journal
of the peripheral nervous system;
15 : 176-184.
51. Collins MP, Mendell JR, Kissel JT (2000); Superficial peroneal
nerve/peroneus brevis muscle biopsy in vasculitic neuropathy. Neurology
55(5) : 636-643
52. Brew BJ: The peripheral nerve complications of human immunodeficiency
virus (HIV) infection. Muscle Nerve 2003, 28:542–552
53. Jeha LE, Sila CA, Lederman RJ, et al.: West Nile virus infection: a new acute
paralytic illness. Neurology 2003, 61:55–59.
54. Eurelings M, van den Berg LH, Wokke JH, et al.: Increase of sural nerve T
cells in progressive axonal polyneuropathy and monoclonal gammopathy.
Neurology 2003, 61:707–709.
55. Reilly MM, Staunton H: Peripheral nerve amyloidosis. Brain Pathol 1996,
6:163–177.

82
56. Andrews TR, Colon-Otero G, Calamia KT, et al.: Utility of subcutaneous fat
aspiration for diagnosing amyloidosis in patients with isolated peripheral
neuropathy. Mayo Clin Proc 2002, 77:1287–1290.
57. Gabreëls-Festen A: Dejerine-Sottas syndrome grown to maturity: overview
of genetic and morphological heterogeneity and follow-up of 25 patients. J
Anat 2002, 200:341–356.
58. Klein CJ, Dyck PJ, Friedenberg SM, et al.: Inflammation and neuropathic
attacks in hereditary brachial plexus neuropathy. J Neurol Neurosurg
Psychiatry 2002, 73:45–50.
59. Kuhlenbäumer G, Young P, Oberwittler C, et al.: Giant axonal neuropathy
(GAN): case report and two novel mutations in the gigaxonin gene.
Neurology 2002, 58:1273–1276.
60. Pulipaka U, Lacomis D, Omalu B: Amiodarone-induced neuromyopathy:
three cases and a review of the literature. J Clin Neuromusc Dis 2002, 3:97–
105.
61. Koike H, Iijima M, Sugiura M, et al.: Alcoholic neuropathy is
clinicopathologically distinct from thiamine-deficiency neuropathy. Ann
Neurol 2003, 54:19–29.
62. Koike H, Misu K, Huttori N, et al.: Postgastrectomy polyneuropathy with
thiamine deficiency. J Neurol Neurosurg Psychiatry 2001, 71:357–362.
63. Doris Lubec, Wolf Müllbacher, Josef Finsterer , Diagnostic work-up in
peripheral neuropathy: an analysis of 171 cases ; Postgrad Med J
1999;75:723-726

83
64. L. Chia, A. Fernandez, C. Lacroix, D. Adams, V. Plante and G. Said.
Contribution of nerve biopsy findings to the diagnosis of disabling
neuropathy in the elderly A retrospective review of 100 consecutive
patients; Brain (1996), 119, 1091-1098.
65. Prayson RA, Sedlock DJ.Clinicopathologic study of 43 patients with sural
nerve vasculitis. Hum Pathol. 2003 May;34(5):484-90
66. Said G. Value of nerve biopsy ? Lancet 2001; 357(9264) : 1220-21.
67. J. Verghese, P.L. Bieri, C. Gellido , H.H. Schaumburg MD, Peripheral
neuropathy in young-old and old-old patients. Muscle Nerve 2001;24 (11) :
1476-81.
68. Neundörfer B, Grahmann F, Engelhardt A, Harte U. Postoperative effects
and value of sural nerve biopsies: a retrospective study. Eur Neurol.
1990;30(6):350-2.
69. Vrancken AF, Franssen H, Wokke JH, Teunissen LL, Notermans NC , Chronic
idiopathic axonal polyneuropathy and successful aging of the peripheral
nervous system in elderly people. Arch Neurol. 2002 Apr;59(4):533-40.

84
PROFORMA
1.Identification information
1.1 Serial number ---------------------------
1.2 Unique identification number ---------------------------
2. Demographic data
2.1 Age --------------------------- years
2.2 Sex --------------------------- 1. Male 2. Female
2.3 Occupation ------------------------
2.4 Year of registration ------------------
3. History(1 = Yes, 0 = No)
3.1 Age of onset -----------------------
3.2 Duration of illness ------------------------
3.3 Developmental delay -------------------------
3.3.1 If yes, specify------------------------
3.4 Poor athletic performance -------------------------
3.5 Distal lower limb weakness ------------ Duration ----------------
3.6 Proximal lower limb weakness --------- Duration ----------------
3.7 Distal upper limb weakness ------------ Duration ----------------
3.8 Proximal lower limb weakness --------- Duration ----------------
3.9 Gait difficulty --------- Duration ------------------

85
3.10 Falls--------------- Duration --------------------
3.11 Neck weakness ---------------
3.12 Trunk weakness ---------------
3.13 Respiratory difficulty --------------
3.14 Cranial nerve involvement -----------
3.14.1 I yes, specify -------------------
3.15 Sensory symptoms --------------- Duration ----------------
3.15.1 If yes, specify ---------------
3.16 Pain ----------------
3.17 Cramps-----------------
3.18 Deformities----------------
3.19 Functional status -----------------
(0 = normal, 1 = mild difficulty, independent, 2= moderate difficulty, independent,
3 = partly dependent, 4 = bed/ wheel chair bound)
4.Other history ( 1= Yes, 0 = No)
4.1 Other illnesses ---------------------------------
4.1.1 If yes, details ---------------------------------
4.2 Family history ---------------------------------
4.2.1 If yes, details ---------------------------------
4.3 Consanguinity ----------------------------------

86
4.9.1 If yes, details -----------------------------------
5.Physical signs (1 = Yes, 0 = No)
5.1 Systemic signs ---------------- Specify ---------------
5.2 Cranial neuropathy --------------- Specify -----------------
5.3 Deformities ---------------
5.3.1 Pes cavus ----------------
5.3.2 Hammer toes ------------------
5.3.3 Equinovarus ------------------
5.3.4 Claw hands ------------------
5.3.5 Kyphoscoliosis ------------------
5.3.6 Others ------------------
5.4 Contractures ------------------ Specify --------------
5.5 Wasting ------------------ Specify --------------
5.6 Power of lower limbs (Right/ Left)
5.6.1 Toe flexors ------------------
5.6.2 Toe extensors ------------------
5.6.3 Ankle dorsiflexion ------------------
5.6.4 Ankle plantar flexion ------------------
5.6.5 Knee flexion ------------------
5.6.6 Knee extension ------------------
87
5.6.7 Hip abduction ------------------
5.6.8 Hip adduction ------------------
5.6.9 Hip flexion ------------------
5.6.10 Hip extension ------------------
5.7 Power of upper limbs (Right/ Left)
5.7.1 Intrinsic muscles ------------------
5.7.2 Hand grip ------------------
5.7.3 Wrist flexion ------------------
5.7.4Wrist extension ------------------
5.7.5 Elbow flexion ------------------
5.7.6 Elbow extension ------------------
5.7.7 Shoulder abduction ------------------
5.7.8 Shoulder adduction ------------------
5.7.9 Shoulder flexion ------------------
5.7.10 Shoulder extension ------------------
5.8 Axial muscles
5.8.1 Neck flexion ------------------
5.8.2 Neck extension ------------------
5.8.3 Trunk ------------------
5.9 Reflexes

88
5.9.1 Biceps jerk ------------------
5.9.2 Supinator jerk ------------------
5.9.3 Triceps jerk ------------------
5.9.4 Knee jerk ------------------
5.9.5 Ankle jerk ------------------
5.9.6 Abdominal reflex ------------------
5.9.7 Plantar response ------------------
5.10 Sensory involvement ------------------
5.10.1 Pain impairment ------------------
5.10.2 Touch impairment ------------------
5.10.3 Vibration impairment ------------------
5.10.4 Joint position sense impairment ------------------
5.10.5 Pattern ------------------
(1= stocking-glove, 2=stocking, 3= glove, 4=asymmetric)
5.11 Gait (describe) ------------------
5.12 Tremors of upper limbs ------------------
5.13 Other signs (specify) ------------------
6. Electrophysiology and nerve biopsy
6.1 Conduction velocity (right/ left)
6.1.1 Median ------------------
6.1.2 Ulnar ------------------

89
6.1.3 Peroneal ------------------
6.1.4 Tibial ------------------
6.2 CMAP amplitude
6.2.1 Median ------------------
6.2.2 Ulnar ------------------
6.2.3 Peroneal ------------------
6.2.4 Tibial ------------------
6.3 Sensory peak latency
6.3.1 Median ------------------
6.3.2 Ulnar ------------------
6.3.3 Sural ------------------
6.4 Sensory amplitudes
6.4.1 Median ------------------
6.4.2 Ulnar ------------------
6.4.3 Sural ------------------
6.5 EMG ------------------
(0=normal, 1= denervation, 2= reinnervation only, 3= not done)
6.6 Final impression ------------------
(1 = Axonal, 2 = demyelinating, 3= intermediate, 4 = indeterminate)
6.7 Final clinical diagnosis --------------------------------

90
7. Laboratory parameters
7.1 Hemoglobin
7.2 ESR
7.3 Total leucocyte count, Differential leucocyte count
7.4 CSF Study
7.5 ANA Profile
8. Nerve biopsy histopathology
8.1 Endothelial edema
8.2 Endothelial fibrosis
8.3 Sub-epithelial edema
8.4 Sub-epithelial fibrosis
8.5 Transmural necrosis
9. Post-biopsy diagnosis
10. Treatment initiated
11. Follow up
11.1 Date of last follow up ------------------
11.2 Total follow up duration ------------------
11.3 Status at last follow up ---



4%SIMILARITY INDEX
1
2
3
4
5
6
7
Jitesh Goel_Thesis.docxORIGINALITY REPORT
PRIMARY SOURCES
www.bioline.org.brInternet
Anish, L., M. Nagappa, A. Mahadevan, and A. B. Taly."Neuropathy in elderly: lessons learnt from nervebiopsy", Age and Ageing, 2014.Crossref
Said, Gérard. "Indications and Usefulness of NerveBiopsy", Archives of Neurology, 2002.Crossref
G. said. "Contribution of never biopsy f indings tothe diagnosis of disabling neuropathy in theelderly", Brain, 1996Crossref
ael.physic.ut.eeInternet
Prayson, R.A.. "Clinicopathologic study of 43patients with sural nerve vasculitis", HumanPathology, 200305Crossref
A. Gordon Smith. "A Rational Diagnostic Approachto Peripheral Neuropathy", Journal of ClinicalNeuromuscular Disease, 06/2003Crossref
74 words — 1%
74 words — 1%
35 words — < 1%
21 words — < 1%
21 words — < 1%
18 words — < 1%
15 words — < 1%