a cardiovascular and pulmonary pt residency? where do we start? ellen hillegass, pt, ccs, phd...
TRANSCRIPT

A Cardiovascular and Pulmonary PT Residency? Where Do We Start?
Ellen Hillegass, PT, CCS, PhD
Rebecca Crouch, PT, CCS
Alexandra Sciaky, PT, DPT, MS, CCS

Disclosures
• The speakers: Ellen Hillegass, Rebecca Crouch and Alexandra Sciaky are co-founders of PTcardiopulmonaryeducators.com, an independent provider of cardiovascular and pulmonary physical therapy education and consultation services.

Session Learning Objectives
After this session, the learner will be able to:• Discuss different program models for Cardiovascular and
Pulmonary (CV&P) Residency programs. • Compare and contrast clinical competencies for entry level
versus advanced level practice in cardiovascular and pulmonary physical therapy.
• Identify criteria for establishing a residency program as well as resources for a residency program.
• Discuss the pros and cons of a residency program from a resident’s perspective.
Overview of CV&P Entry Level Competencies
• Resources to identify CV & P entry level competencies:– www.cardiopt.org website of the CV & P Section– CAPTE criteria for entry level programs– A Normative Model of Physical Therapist Professional Education– CPI tool
Why do you need to know the entry level criteria?
• Residency is ABOVE entry level.• Advanced Practice is defined by DSP: Description of Specialty
Practice• Before you progress into Advanced Practice : MUST determine
resident meets all entry level criteria.– MAY HAVE HOLES in their entry level education or clinical
practice
Examples of CAPTE criteria for Assessment
Select and competently administer tests and measures appropriate to the patient’s age,
diagnosis and health status including, but not limited to
• a. Aerobic Capacity/Endurance • b. Anthropometric Characteristics • d. Assistive and Adaptive Devices• d. Gait, Locomotion, and Balance• e. Circulation (Arterial, Venous, Lymphatic) • f. Self-Care and Civic, Community, Domestic, Education, Social and Work Life ux. Work (Job/School/Play),
Community, and Leisure Integration or Reintegration• h. Environmental Factors• j. Integumentary Integrity • l. Mental Functions• m. Mobility (including Locomotion• n. Motor Function • o. Muscle Performance (including Strength, Power, Endurance, and Length)• q. Pain • r. Posture • s. Range of Motion • t. Reflex Integrity • u. Sensory Integrity • w. Ventilation and Respiration or Gas Exchange
Examples of CAPTE criteria for Interventions
Competently perform physical therapy interventions to achieve patient/client goals and outcomes. Interventions include:
a. Airway Clearance Techniques
b. Assistive Technology: Prescription, Application, and, as appropriate, Fabrication or Modification
c. Functional Training in Self-Care and Home Management
d. Functional Training in Work (Job/School/Play), Community, and Leisure Integration or Reintegration
e. Integumentary Repair and Protection Techniques
f. Motor Function Training (balance, gait, etc)
g. Patient/client education
h. Therapeutic Exercise
i. Physical Agents and Mechanical Modalities

Resource for Self Assessment for Entry Level
Types of Residency Models

Types of Residency Models
• MODEL must have:– Mentor(s)/faculty, at least one must be a CCS– At least one resident– Residency Director– Curriculum– Clinical Learning Environment to practice & CVP diagnoses
• Must have 100 of 150 mentoring hours as 1 to 1 with mentor• 2000 hours of direct patient care in the specialty area
– Didactic Learning Environment• Must have 75 hours
– With Cardio: must have research project to sit for CCS– Evaluation Methods– Financial resources/budget– Equipment
Types of Residency Models
• MODEL 1/Medical System Based Model– All components within “same” environment
• Example: DUKE MEDICAL CENTER• Residents are hired by Duke University and practice clinically treating
patients on in patient as well as outpatient basis. • Multiple residents can be present as there are multiple mentors available• Residents receive Didactic component at Duke University in a variety of
settings• Multiple Mentors due to the presence of multiple CCS as well as clinical
experts at Duke Medical Center and University• Residency Director over all programs, CCS is co-director over
cardiopulmonary residency

Types of Residency Models
• Model 2/ Facility Based Model– Residency programs reside in multi-facility healthcare system– Residents are hired by member facility as “trainees”– Mentoring primarily provided by CCS and other clinical experts in each
member facility– Didactic portion provided to residents by clinical faculty and affiliated
academic programs– An overall residency director is at each site– Residents and mentors rotate to provide optimal
learning experiences– Collaboration with affiliated clinical sites under
one umbrella• Example VA Medical Center

Types of Residency Models
• Model 3/Academic Based Model in Conjunction with a Clinical Facility– Residency Director over entire residency program– Mentor hired by facility to perform mentoring activities with resident– Resident is hired by facility and has release time or fewer hours to
have time to perform residency mentoring hours with mentor– Didactic Education can be provided by Webinars as well as other
educational opportunities– Curriculum prepared by Residency Director and agreed upon with
Mentor…can be provided by webinars and other opportunities• Ptcardiopulmonaryeducators.com
Why aren’t there MORE Residency Programs????

Neuro Consortium
Neurologic Physical Therapy Professional Education Consortium was developed in 2010 initially to support local neurologic residency programs in Southern California. The curriculum is now offered annually to support neurologic residency education and individuals interested in a comprehensive neurologic continuing education curriculum.
www.ptneuroconsortium.org
Data from Neuro Consortium since 2010:
Pre consortium: 5 neuro residency programs
Since consortium: 25 neuro residency programs
Consortium started with 2 residency programs
2015: consortium now has 20 residency programs

Residency Program Specifics

Is Resident at Entry-Level to Begin CVP Residency?
• Patient Practical
– Reviews medical history– Performs an interview that is patient centered– Integrates knowledge of diseases with medical history– Adjusts communication to best match the patient's cognitive level
and learning style– Performs physical evaluation– Performs appropriate outcome measures– Administers treatment

Resource for Self Assessment

Is Resident at Entry-Level to Begin CVP Residency?
• Competencies for example……..
– 6 Minute Walk Test
– Vital Signs Measurement
– Lung/Heart Sounds
– ECG (single lead)

Is Resident at Entry-Level to Begin CVP Residency?
• Pre-Test
– Pen/Paper knowledge test
– Various types of question formats: multiple choice, T/F, discussion, case study, short answer
– Determine “score”
– Identify strengths and weaknesses
** Review with Resident! Design a Learning Plan

Is Resident at Entry-Level to Begin CVP Residency?
Other options to assess ability…….
• Various patients with various diagnoses– Observe verbal and practical skill of Resident with the patient– Knowledge integration– Ability to alter evaluation and treatment specific to patient and/or
diagnosis
• Case Study Discussion
**Review and develop learning plan
Feedback
• Set expectations and “scoring” beforehand
• Immediately discuss with Resident
• Assess different abilities: verbal, manual, educational, interpretation and understanding of written material contained in case study or patient records
• **Develop Learning Plan Together
Ideas for Bringing Resident up to Acceptable Level
Duke Model:• Through Blackboard, Sakai, You Tube,Websites, or written material,
design or include self-instruction packages with self-testing at the end of each module
• Examples: Arterial Blood Gases, Pulmonary Function Testing, 6 Minute Walk Test, Lab Panels, Cardiac and Pulmonary diagnostic testing, X-ray interpretation, EKG, etc.
• Series of meetings with Faculty to address key topics• Journal clubs with CVP staff • Narrative reasoning meeting with other Residents where a case,
diagnosis, or treatment regime is discussed• Attending other discipline meetings or “Rounds” to expand
knowledge base and broaden perspective

Ideas for Bringing Resident up to Acceptable Level
• VA Ann Arbor offers:– Didactic classes with faculty for the first 6 months of Residency
covering intermediate CVP topics (those beyond entry-level)– Second half of Residency is focused on case studies for advanced
CVP topics
• Duke offers:– Observation of faculty with patient– Selected articles and self-instructional packets– Attending Medical-center standardized classes – Chart reviews

Description of Specialty Practice
Advanced CVP Topics
• In January 2005, the Cardiovascular and Pulmonary Specialty Council began the process of specialty practice revalidation for the second time. A project team was created to represent Cardiovascular and Pulmonary specialty practice across diverse ages, practice settings, geographic regions, and lengths of time as a specialist. This project team met to create a survey to validate the state of specialty practice in cardiovascular and Pulmonary physical therapy. Both specialist and non specialist Section members were surveyed and the results were analyzed to create the Description of Specialty Practice: Cardiovascular and Pulmonary Physical Therapy.4 This document was approved by ABPTS in 2007.

Curriculum Development
• The overall curriculum must cover all areas in the Description of Specialty Practice (DSP).
• Some areas will be covered in the clinical learning experiences and some will be covered by didactic coursework. ABPTRFE determines the minimum required hours for each.
• The residency director can develop the curriculum with a team and should design the it based on available mentors/instructors.
• For a sample CV&P residency curriculum, go to
www.ptcardiopulmonaryeducators.com/ResidencyDevelopmentResources

Mentoring: A Key Component of Residency

Faculty/Mentor Development
• Mentors must be physical therapists with CV&P experience but don’t have to be a CCS.
• The residency director can support mentor development by doing the following:– Assessing the mentors strengths and challenges and planning resident
assignments accordingly– Providing advanced learning opportunities to allow mentors to lead
with their expertise– Providing individualized training in the act of mentoring (see
ABPTRFE Mentoring Handbook)
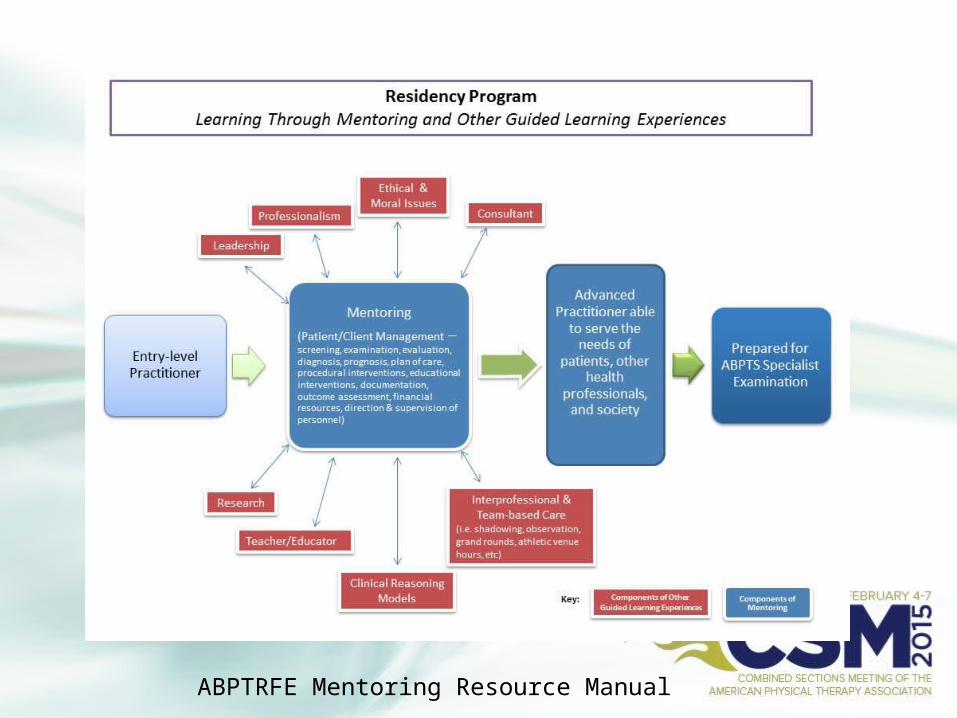
ABPTRFE Mentoring Resource Manual

Mentor’s Ability to Manage Multiple Sources of Information
Characteristics of a Good Mentor
• Skilled in the CV&P PT specialty, CCS optional• Excellent communication skills, written and verbal• Able to use questioning as a teaching tool• Able to utilize the CV&P DSP as a reference for desired
performance outcomes for each resident• Able to collaborate with other faculty and residents to provide
the optimal learning environment and experiences• Able to navigate and utilize CV&P evidence that supports
clinical decisions• Demonstrates leadership in the clinic and in the profession

Measurement of Resident Performance
• You can create your own resident performance tools or modify an existing ones.
• Tools include written exams, clinical performance tools, live practical exam tools, self-evaluation tools, project assignments/papers (ie. Research) and teaching/speaking assignments.
• For examples go to www.ptcardiopulmonaryeducators.com
And http://www.abptrfe.org/ForPrograms/ApplicationManual/
Performance Evaluation Process
• Establish learning objectives based on the DSP• Set timetable for each type of evaluation/tool to be used• Include a self-evaluation by the resident when possible• Provide time for reflection and note changes in performance
with feedback from mentor(s) between formal evaluations• Provide learning experiences designed to address individual
resident’s needs• Keep performance information confidential (Buckley Act)

REMEMBER!!
• Remember the residency is designed to prepare residents to sit for the ABPTS Cardiovascular and Pulmonary Specialty examination.
• The resident’s clinical practice must be at the specialty level by the end of the residency and all other requirements must be successfully completed by the end of the residency (12 months at VA Ann Arbor) in order to successfully complete the residency.
• Other requirements include teaching, consultation, program administration and research.

Patient Populations/Diagnoses
• Residents must see the full spectrum of CV&P diagnoses or have a plan to address any deficits
• Records of numbers of patients seen in each diagnostic category must be kept for accreditation purposes
• Residents must also have didactic learning experiences that cover the full spectrum of CV&P diagnoses.
• Special learning experiences can be added such as wound care, diabetic foot care at the VA Ann Arbor Program

Residency Program Evaluation
• ABPTRFE requires that regular program evaluations are done by residents, faculty, program director and any other pertinent stakeholders.
• Faculty evaluations also need to be done by the residents and the program director
• Documentation of the results of the evaluations are needed for annual reports to ABPTRFE as well as what was done to address the program’s deficits
• Regular faculty meetings are also needed to monitor progress of the residents and the program and to make changes as needed

The Resident’s Perspective
• Meghan Lahart, PT, DPT, CCS Graduate of VA Ann Arbor Healthcare System CVP PT Residency Program (Michigan), on staff at University of Chicago Hospital, Chicago, IL
• Danielle Fiorello, PT, DPT, CCS, Graduate of Duke Residency Program, currently on staff at Beth Israel Hospital, New York
CVP Residency Resources
• Link to ABPTRFE Application Resource Manual is
http://www.abptrfe.org/ForPrograms/ApplicationManual/• American Physical Therapy Association, Cardiopulmonary Section
www.cardiopt.org• http://www.abptrfe.org/ForPrograms/ApplicationManual/• www.Ptcardiopulmonaryeducators.com (Webinar-based didactic series)• http://ptot.duhs.duke.edu/modules/ptot_residencies/index.php?id=7
(Duke Medical Center CVP Residency Program)• http://
www.annarbor.va.gov/careers/Cardiovascular_and_Pulmonary_Physical_Therapy_Residency_Program.asp (Ann Arbor VA CVP Residency Program)
• http://www.abptrfe.org/apta/abptrfe/Directory.aspx?navID=10737432672 (APTA Credentialed CVP Residency Programs)

CVP Residency Resources
• COPD Foundation www.copdfoundation.org• Pulmonary Fibrosis Foundation www.pulmonaryfibrosis.org• Cystic Fibrosis Foundation www.cff.org• www.journalofphysiotherapy.com/article/S0004-9514(07)700
54-5/pdf (Pulmonary Rehabilitation)
• Pulmonary Rehabilitation Tool Kit– https://www.aacvpr.org/.../PulmonaryRehabilitationToolkit/.../
Default.asp– www.pulmonaryrehab.com.au/– www.aarc.org – Lungfoundation.com.au/health “The COPD-X Plan”
CVP Residency Resources
• Canadian PT Society http://www.physiotherapy.ca/Cardioresp• American Thoracic Society (ATS) www.thoracic.org (patient education
materials and Pulmonary Rehabilitation Assembly)• American College of Chest Physicians (ACCP) www.chestnet.org
(Pulmonary Rehabilitation)• American Association of Cardiovascular and Pulmonary Rehabilitation
(AACVPR) www.aacvpr.org (Cardiovascular and Pulmonary Rehabilitation resources)
• American Lung Association (ALA) www.lung.org (Lung diseases and patient education material)
• American Heart Association (AHA) www.heart.org (Conditions and Educator sections)
• European Respiratory Society (ERS) www.ersnet.org (“Assemblies”)• International Society of Heart and Lung Transplantation (ISHLT)
www.ishlt.org• United Network for Organ Sharing (UNOS) www.unos.org

References
• Swisher A, Sciaky A, Campbell A, Lowman J: Cardiovascular and pulmonary specialty practice: determining the current status. Cardiopulmonary Physical Therapy Journal, March 2008, Vol.19, No. 1, pp. 11-15. American Physical Therapy Association.
• Description of Specialty Practice: Cardiopulmonary Physical Therapy. American Physical Therapy Association, Alexandria, VA: Cardiovascular and Pulmonary Specialty Council; 2007.
• American Physical Therapy Association. Evaluative Criteria for Accrediting Residency and Fellowship Programs for Physical Therapists. Alexandria, VA (Adopted and effective 10/26/2010; revised 07/12; revised 5/13) http://www.abptrfe.org/uploadedFiles/ABPTRFEorg/For_Programs/Apply/ABPTRFE_EvaluativeCriteria2014.pdf
References-cont’d
• Self Assessment Tools for Physical Therapists, Cardiovascular and Pulmonary, American Physical Therapy Association, 2008.
• Residency & Fellowship Application Resource Manual. American Board of Physical Therapy Residency and Fellowship Education, 2013. http://www.abptrfe.org/ForPrograms/ApplicationManual/

THANK YOU!
• Sponsored by Cardiovascular and Pulmonary Section
AND• www.Ptcardiopulmonaryeducators.com