a brief guide to snake envenomations in malaysia and antivenom therapy (edited)
DESCRIPTION
A Brief Guide to snake ENvenomations in Malaysia and Antivenom TherapyTRANSCRIPT

1
A Brief Guide to Snake Envenomations in Malaysia and Antivenom Therapy
Prof Tan Nget Hong (PhD, University of Chicago)a, Dr Tan Choo Hock (MBBS, University of Malaya) b,
Leong Poh Kuan (BBMedSc, University Malaya)b
Venom and Toxin Research Group aDepartment of Molecular Medicine, Faculty of Medicine, University of Malaya; bDepartment of
Pharmacology, Faculty of Medicine, University of Malaya
1. Introduction
Venomous snakebite leading to envenomation syndrome is a classifiable “disease” indexed by the WHO International Classification of Disease (ICD-10), and appropriately categorized as a Neglected Tropical Disease (WHO, 2009) that constitues a serious public health problem in the tropics (Chippaux, 1998; Kasturiratne et al., 2008). The severity of the issue unfortunately has been neglected systemically (Gutiérrez et al., 2006; Alirol et al., 2010), partly due to under-reporting and inconsistent
epidemiological studies that includes Malaysia. Earlier reports (year 1958 to 1980) estimated as many as 55000 cases of snakebites admitted to the hospitals in Malaysia, with majority of the bite cases came from northern states of Peninsular Malaya where agricultural activities were common. While the mortality rate of snakebite in Malaysia is only 0.3 per 100000 population (this figure appears though to be underestimated), complications like crippling deformity caused by the necrotizing effect of some venoms, and psychological trauma, are among features of prolonged morbidity that add to the human suffering, and significantly jeopardize the victims’ quality of life.
A survey at General Hospital Kuala Lumpur (1999-2003) alone indicated that snakebite affected
not only rural places but also suburban areas neighboring cities like Kuala Lumpur. It reflected
the fact that rapid and intense urbanization increased the chances of snake encounter as more
humans were encroaching into their habitats. In view of the global experience and the
development trend in our country, precautions and clinical guidelines need to be addressed
despite the fact that a more systematic and updated epidemiological study is yet unavailable.
2. Venomous Snakes of Malaysia
In Malaysia and the coastal waters of the region, there are at least 18 different species of
venomous front-fanged land snakes and more than 22 different species of sea snakes. These
venomous snakes belong to the following 2 families (3 subfamilies):

2
Table 1: Medically important venomous snakes in Malaysia
Family Subfamily Genus Common names Main habitat
Viperidae Crotalinae - Calloselasma
- Cryptelytrops
- Tropidolaemus
- Parias
- Malayan pit viper (ular
kapak bodoh)
- Asian lance-headed pit
viper(ular kapak)
- Land
- Tree
Elapidae Elapinae
Hydrophiinae
- Naja
- Bungarus
- Ophiophagus
- Calliophis/
Maticora
- Laticauda
- Enhydrina
- Kerilia
- Hydrophis
- Thalassophis
- Pelamis
- Kolpophis
- Aipysurus
- Cobra (ular senduk)
- Krait (ular katang)
- King cobra (ular tedung selar)
- Coral* snake (ular karang*)
- Sea snake (ular laut)
- Land
*the name
‘coral/karang’
does not indicate
its habitat
- Seas and coastal
region
Only a few of the Malaysian venomous snakes can be regarded as of medical importance.
Epidemiological studies showed that in Malaysia, bites were mainly due to four species of land
snakes: Calloselasma rhodostoma (Malayan pit viper), Naja (Asian common cobra, there are
two species: Naja sumatrana (equatorial spitting cobra) and Naja kaouthia (monocellate cobra),
Cryptelytrops purpureomaculatus (mangrove pit viper) and Tropidolaemus wagleri (Wagler’s pit
viper). Other venomous snakes indigenous to Malaysia that are potentially dangerous to human
include Bungarus candidus (Malayan krait), Bungarus fasciatus (banded krait), Bungarus
flaviceps (red-headed krait), Ophiophagus hannah (king cobra), Parias sumatranus (Sumatran
pit viper) and the sea snakes. The species Cryptelytrops purpureomaculatus, Parais sumatranus
and Tropidolaemus wagleri (Wagler’s pit viper) belong to the Trimeresurus complex (Asian
lance-headed pit vipers). There are more than 7 different species of Asian lance-headed pit
vipers in Malaysia. Refer to Figure 1 (a-f: Elapidae; g-j: Viperidae; typical features for quick

3
identification were given in parentheses but remember variations do exist) for pictures of some
medically important snakes in Malaysia, or contact the authors.
Figure 1 a: Naja sumatrana (white bands on neck); b: Naja kauthia (oval mark on hood);
Bungarus flaviceps (red-headed, red-tailed, body and belly black); d: Bungarus candidus
(alternate dark bluish and yellowish white bands); e: Bungarus faciatus (alternate black and
yellow bands); f: Enhydrina eschistosa (dark grey back, whitish sides);
a b
c d
e f

4
Figure 1. g: Calloselasma rhodostoma (large scale over the head, stout, light brownish body
with dark brown saddles); h: Cryptelyptrops purpureomaculatus (olive to dark purplish brown;
a white line may present along each side); i: Cryptelyptrops albolabris (green above, pale green
or white below the eyes including lips); j: Tropidolaemus wagleri (green body with dark-
bordered scales; multiple green-yellow crossbars on the back).
Table 2 shows statistics of snakebites in West Malaysia, 1965-1971, based on data from 28
hospitals. Some recent reports, however, suggested that cobra bites are more prevalent that
bites by other snakes (Tan et al., 1990; Jamaiah et al., 2004; 2006).
g h
i j

5
Table 2: Snakebites in West Malaysia
Snake Species Total Cases Fatal Cases
Malayan pit viper (Calloselasma
rhodostoma)
1136 4
Sea snake 158 5
Asian common cobra (Naja) 112 3
Asian lance-headed viper (Trimeresurus) 25 0
King cobra (Ophiophagus hannah) 6 0
Krait (Bungarus) 1 0
Unidentified 3765 6
Non-venomous 184 0
Report from monthly statistics of 28 hospitals throughout Malaysia, 1965-1971.
3. Biochemical composition of Snake Venoms
Snake venom contains mainly proteins (70-90%) and small amounts of metals, amino acids,
peptides, nucleotides, carbohydrates, lipids and biogenic amines. The protein components
include enzymes and non-enzymatic proteins/polypeptides and are usually the main toxic
compounds.
The main toxic principles in the venoms of elapid snakes (cobra, krait and sea snakes) include
polypeptide neurotoxins, polypeptide cardiotoxins and phospholipases A that may exhibit
presynaptic neurotoxicity or myotoxicity.
The main toxic principles of crotalid (pit viper) snake venoms are thrombin-like enzymes,
hemorrhagic proteases and platelet-aggregation inducers.
4. Elapid (cobras, kraits and sea snakes) Envenoming
Elapid venoms generally produce neurotoxicity and cardiotoxicity.
The earliest symptom of systemic elapid envenoming is a feeling of drowsiness or intoxication,
which starts from 15 min to 5 hr after cobra bites. Neurotoxicity manifested as progressive
descending flaccid paralysis often begin with bilateral ptosis (difficulty in opening the eyes:

6
eyelids may remain completely closed though the patient usually remains conscious until
respiratory failure is advanced where hypoxia compromises consciousness), ophthalmoplegia,
facial muscle paralysis (with difficulty in opening the mouth, moving the lips) and bulbar palsy
(with aphonia, dysphagia, difficulty in protruding the tongue beyond incisors) within 1 to 4 hrs.
“Broken-neck sign” is a telltale sign that should be elicited as part of routine clinical
examination, especially in pediatric, delirious or semi-conscious patients. Fixed, dilated pupils,
limb weakness, loss of tone and deep tendon reflexes are other important signs. However, once
the paralysis involves the diaphragm and intercostals muscles, respiratory failure sets in even as
fast as 30 minutes within the bite. Mechanical ventilation hence should be on standby in any
case suspected of venomous snakebite.
Cardiotoxicity is caused by polypeptide cardiotoxin that affects both excitable and nonexcitable
cells, causing irreversible depolarization of the cell membrane and consequently impairing the
structure and function of various cells, thus contributing to muscle paralysis postsynaptically;
and cardiac complications e.g. arrhythmias leading to circulatory failure and systolic arrest.
Electrocardiogram (ECG) monitoring and perhaps cardiac enzymes test are therefore valuable in
monitoring the victims’ clinical progress.
Cobra (Naja sp.) venoms cause extensive local necrosis of the bitten limb, while krait and sea
snake bites do not usually cause local envenoming and can be virtually painless – hence the
possibility of late discovery and delayed treatment. Although it may not be fatal, local tissue
destruction should receive early attention and surgical intervention if indicated, in order to
salvage the limb function as much as possible. In addition, the equatorial spitting cobra is also
potentially responsible for ‘cobra-spit ophthalmia’ (with corneal ulceration and scarring,
secondary endophthalmitis) from its venom spat onto victims’ eyes.
Sea snake venoms contain both polypeptide neurotoxin (homologous to elapid neurotoxin) and
myotoxin, which is usually a basic phospholipase A2. The venoms cause respiratory failure
(neurotoxic effect) and myonecrosis (myotoxic effect), leading to rhabdomyolysis,
myoglobinuria and acute kidney injury. Generalized muscle pain/tenderness and stiffness,
trimus; and dark-brown urine are suggestive clinical features. Urine output and renal function
in these patients deserve close monitoring in anticipation of renal failure.
7
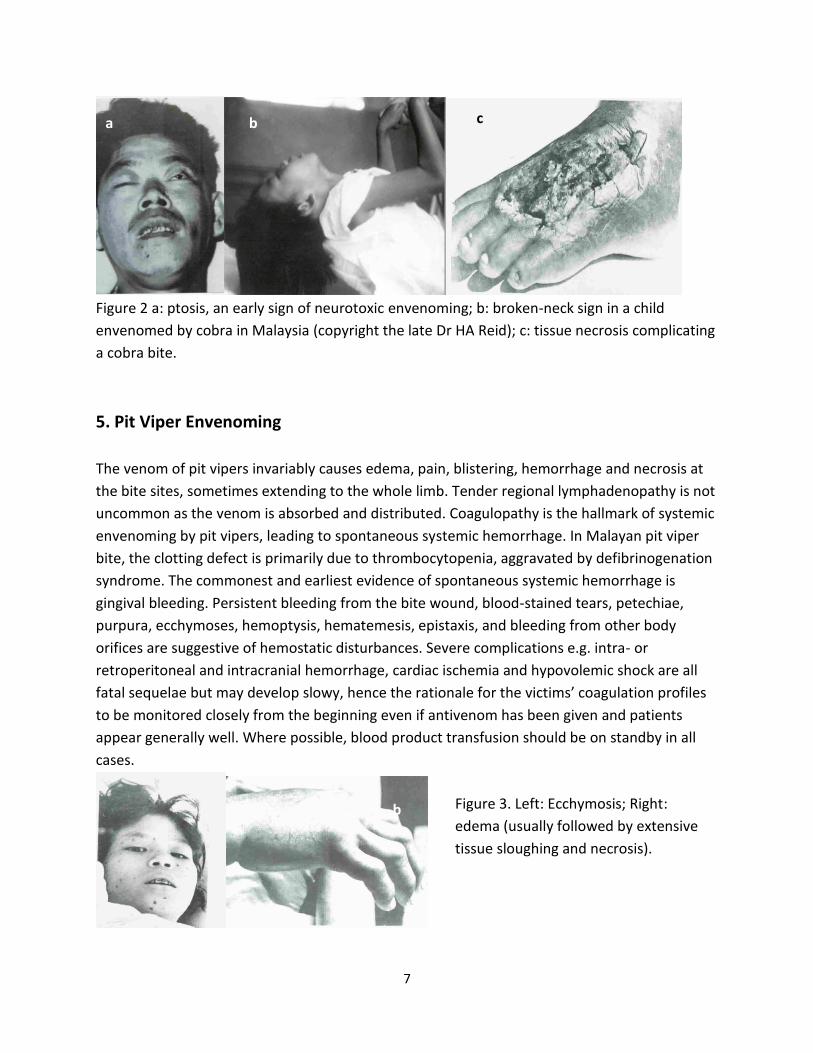
Figure 2 a: ptosis, an early sign of neurotoxic envenoming; b: broken-neck sign in a child
envenomed by cobra in Malaysia (copyright the late Dr HA Reid); c: tissue necrosis complicating
a cobra bite.
5. Pit Viper Envenoming
The venom of pit vipers invariably causes edema, pain, blistering, hemorrhage and necrosis at
the bite sites, sometimes extending to the whole limb. Tender regional lymphadenopathy is not
uncommon as the venom is absorbed and distributed. Coagulopathy is the hallmark of systemic
envenoming by pit vipers, leading to spontaneous systemic hemorrhage. In Malayan pit viper
bite, the clotting defect is primarily due to thrombocytopenia, aggravated by defibrinogenation
syndrome. The commonest and earliest evidence of spontaneous systemic hemorrhage is
gingival bleeding. Persistent bleeding from the bite wound, blood-stained tears, petechiae,
purpura, ecchymoses, hemoptysis, hematemesis, epistaxis, and bleeding from other body
orifices are suggestive of hemostatic disturbances. Severe complications e.g. intra- or
retroperitoneal and intracranial hemorrhage, cardiac ischemia and hypovolemic shock are all
fatal sequelae but may develop slowy, hence the rationale for the victims’ coagulation profiles
to be monitored closely from the beginning even if antivenom has been given and patients
appear generally well. Where possible, blood product transfusion should be on standby in all
cases.
a b c
b Figure 3. Left: Ecchymosis; Right:
edema (usually followed by extensive
tissue sloughing and necrosis).

8
6. Death Times
Generally speaking, deaths are most rapid following elapid bites and most protracted following
pit viper bites:
Snake species Average Death
time (hr)
Death time (hr)
– Range
King cobra (Ophiophagus hannah) -- ‘few min’- 6
Cobra (Naja) 8.4 ¼- 60
Malayan pit viper (Calloselasma
rhodostoma)
64.6 5-240
Mangrove pit viper (Cryptelytrops
purpureomaculatus
-- 12
The estimation of death times does not imply the allowance for delaying medical treatment,
but rather highlight the urgency to initiate indicated treatment as soon as possible, and to
thoroughly monitor the clinical progress of the patients.
7. First-Aid Measure in Snake Envenoming
1. Do not panic! Keep calm, reassure the individual as complete recovery is the rule.
2. Lie the patient down to ensure minimum activity. Keep the bitten part at rest, immobilize
the bitten limb with a splint or a sling – musculature contraction may increase the
absorption and dissemination of venom through bloodstream and lymphatics.
3. Consider pressure immobilization with compression bandage (using a broad, elastic,
stretchable crepe bandage) bound as tightly as for a sprained ankle, without
compromising the distal pulses. Only recommended for non-locally necrotizing
neurotoxic snakebite (king cobra, kraits, coral snakes and maybe sea snakes), otherwise
might cause more severe local tissue destruction and increased intracompartmental
pressure.
4. Avoid any interference with the bite wound to prevent hastening venom absorption,
worsening local bleeding or introducing infection. Washing or wiping the wound is
controversial (in addition, traces of snake oral secretion on the wound may be of value
for diagnostics in future). Do not attempt to cut the wound and suck out the venom.
5. Arterial tourniquets (and any tight ligature applied around the bitten limb) are not
recommended as this can lead to limb ischemia and gangrene; and worse still, when

9
released there may be a dramatic increase of the venom dissemination systemically via
hyperemic response.
6. All patients with snake bites must be as soon as possible brought to the hospital for
treatment with absolute minimum movement of the body especially the bitten limb.
Where vehicles are not available, the victim should be carried using a stretcher.
7. Do not attempt to catch or kill the biting snake. However, if the snake has been killed,
bring it to the hospital for identification – but never allow handling of the snake bare-
handed as even a severed head can bite with reflex!
8. Diagnosis and Early Assessment of Snakebite Envenomation:
Two major questions when a snakebite victim presents at a healthcare centre are: the identity
of the snake inflicting the bite (diagnosis), and the severity of envenoming (early assessment):
a. Diagnosis of the biting species:
This can be ascertained by
i) Identification of the snake if the patient brings the snake to the hospital.
ii) Immunodiagnosis: this is costly and can be performed only in a well-equipped
laboratory. Presently not available in Malaysian hospitals. The facilities are
available at the Venom and Toxin Research Group at Faculty of Medicine,
University of Malaya.
iii) Clinical observation and inquiring circumstances of bite:
Systemic pit viper envenoming (bites by Malayan pit viper (Calloselasma
rhodostoma) and the Asian lance-headed pit vipers (Trimeresurus complex) is
characterized by non-clotting blood and other hemorrhagic syndrome
accompanied by rapid local swelling after the bite.
Systemic elapid envenoming (due to cobras and kraits) is characterized by
neurotoxic effects including ptosis, bulbar palsy, respiratory paresis and
sometime cardiac effects.
Systemic sea snake envenoming is characterized by myotoxic effects such as
myalgia, paresis, myoglobinuria, hyperkalaemia.
Note: NOT all snakes are venomous – for confirmed non-venomous bite, manage as
puncture wound.
b. Early assessment of the severity of snakebite envenoming can generally be made by
observing the extent of local envenoming effects and initial laboratory investigations.

10
In ‘dry bite’ cases, venom was not injected although bite was inflicted by a venomous
species. Local signs and laboratory investigations usually are unremarkable. As with a
puncture wound, inflammation and potential infection should be managed accordingly.
In mildly envenomed cases, there are minimal local signs, with swelling in the
immediate vicinity of the wound, no oozing blood from bite site, and no significant
systemic manifestations. Laboratory investigations reveal no abnormalities.
In severe cases, there is swelling, usually massive and rapidly extending, accompanied
by greater pain. Early tender lymphadenopathy indicates fast venom systemic spread.
Early systemic features include nausea, vomiting, diarrhea, drowsiness, ‘heavy’ eyelids,
bleeding from gum or venepuncture and bite site, myalgia, passing brown urine, oliguria
and abnormal laboratory results (e.g. prolonged clotting time, or 20 min whole blood
clotting). In these patients, close monitoring is warranted and antivenom is usually
indicated.
9. Management Principles in Snake Envenomation
9.1 General management of snakebite:
General management of snakebite envenoming includes first-aid and the following
measures:
Adequate reassurance;
Immobilization particularly the bitten limb.
Venous access – precaution needs to be exercised in patients with coagulopathy.
All bitten patients, even without local or systemic features, should be admitted to
hospital for observation of at least 24 hours.
9.2 Antivenom Therapy
Antivenom is the only specific treatment for snake envenomation that is of proven value.
Early (anaphylactic), pyrogenic and late (serum sickness) reactions can occur following
antivenom treatment. Incidence of early reactions following antivenom administration
ranges from 3 to 5%. About 40% of these reactions involve severe systemic anaphylaxis
(bronchospasm, hypotension or angioneurotic edema), though few fatal cases have been
reported. Most authorities have recommended that antivenom should be diluted in
isotonic fluid and given by slow intravenous infusion. Prophylactic regimen e.g. adrenaline,
antihistamines and corticosteroids has been practiced in many places empirically especially

11
for high risk patients. In asthmatic patients, prophylactic use of an inhalational adrenergic β2
agonist e.g. salbutamol has the rationale to prevent bronchospasm. Certainly, resuscitation
facility should be made available prior to the use of antivenom.
Antivenoms Suppliers
9.2.1. Thailand antivenoms
The main antivenoms producer in Thailand is Queen Saovabha Memorial Institute (QSMI),
Bangkok, Thailand. (Tel: 02-2520162, email [email protected], 1871, Rama IV Road,
Bangkok 10330).
Due to the geographical proximity of Thailand and Malaysia, many venomous snakes in
Thailand are similar or closely related to the venomous snakes in Malaysia, and hence
antivenoms produced by QSMI could effectively neutralize venoms from many species of
Malaysia venomous snakes. By adopting an evidence-based approach, the efficacy of Thai
antivenoms in neutralizing local (Malaysian) snake venoms has been researched in the
laboratory (of University of Malaya) for their potential therapeutic use in Malaysia (see
below and Table 3 for types of antivenoms and their efficacies).
QSMI Monovalent antivenoms:
Monovalent Thai cobra antivenom: effective against the two species of cobra in
Malaysia (Naja sumatrana and Naja kaouthia), as well as king cobra (Ophiophagus
hannah);
Monovalent king cobra antivenom: effective against king cobra (Ophiophagus hannah),
efficacy against Malaysian cobra venoms has not been examined;
Monovalent banded krait antivenom: effective against Malaysian banded krait
(Bungarus fasciatus) but not other kraits;
Monovalent Malayan pit viper antivenom: effective against Malayan pit viper
(Calloselasma rhodostoma) but not against Asian lance-headed viper (Trimeresurus
complex)
Monovalent green pit viper antivenom: effective against Asian lance-headed viper
(Trimeresurus complex) in general but not against Malayan pit viper
Monovalent Russell’s viper antivenom: there is no Russell’s viper (Daboia russelli) in
Malaysia

12
QSMI polyvalent antivenoms
Recently, QSMI produced two new polyvalent antivenoms: Neuro polyvalent antivenom for
treatment of elapid (cobra/krait) bites, and Hemato polyvalent antivenom for treatment of
viper/pit viper bites
Neuro Polyvalent Snake Antivenom
This polyvalent antivenom is raised against venoms of Thai cobra (Naja kaouthia) king
cobra (Ophiophagus hannah), banded krait (Bungarus fasciatus) and Malayan krait
(Bungarus candidus). Preclinical tests in our laboratory indicated that the polyvalent
antivenom could effectively neutralize all cobras and kraits of Malaysia origin, and is
more effective against cobra venoms compare to the monovalent Thai cobra antivenom
produced by the same institute. (see Table 3 below)
Table 3: Neutralizaiton capactigy of venoms from Malaysia venomous snakes by the
Neuro polyvalent snake antivenom
Venomous snake Neutralization capacity of Neuro polyvalent antivenom
Neutralization capacity of Monovalent Thai cobra antivenom
Equatorial spitting cobra (Naja sumatrana)
1.84 mg/mL 0.92 mg/mL
Monocellate cobra (Naja kaouthia)
0.55 mg/mL 0.55 mg/mL
King cobra (Ophiophagus hannah)
8.19 mg/mL 2.46 mg/mL
Banded krait (Bungarus fasciatus)
1.38 mg/mL Not effective
Malayan krait (Bungarus candidus)
0.73 mg/mL Not effective
Red headed krait (Bungarus flaviceps)
1.47 mg/mL Not effective
All the venoms tested are from snakes captured in Malaysia. Neutralization capacity
is defined as the amount of venom neutralized by 1 mL of reconstituted antivenom.
The antivenom was reconstituted according to manufacturer’s recommendation: 10
mL of sterile water was added to each vial of antivenom.

13
Hemato Polyvalent Snake Antivenom:
This polyvalent antivenom is raised against venoms of Malayan pit viper (Calloselasma
rhodostoma), White-lipped pit viper (Cryptelytrops albolabris) and Russell’s viper
(Daboia russelli). Preclinical tests in our laboratory showed that the Hemato polyvalent
snake antivenom could effectively neutralize venoms of:
(a) Malayan pit viper (Calloselasma rhodostoma), neutralization capacity of 7.2 mg/mL.
This is more potent that the monovalent Malayan pit viper antivenom produced by
the same institute (neutralization capacity 3.2 mg/mL)
(b) Mangrove pit viper (Cryptelytrops purpureomaculatus), neutralization capacity of
4.2 mg/mL;
(c) White-lipped pit viper (Cryptelytrops albolabris), neutralization capacity of 3.64
mg/mL.
It is likely that the Hemato polyvalent antivenom can neutralize venoms of other species
of pit vipers belonging to the Trimeresurus complex (Asian lance-headed vipers), as our
early work demonstrated extensive cross-neutralization of antivenom against species of
Trimeresurus complex (Tan et al 1994).
9.2.2 Australian CSL antivenom against sea snake
The Commonwealth Serum Laboratories from Parkville, Victoria, Australia produced
antivenom against sea snake. The sea snake antivenom is effective against sea snake
envenomation in Malaysia.
Antivenoms raised against cobra or krait venoms may be able to neutralize sea snake
venom, as they possess common (similar) venom toxins. The efficacy of cobra or krait
antivenoms against sea snake envenomation, however, has not been investigated.
9.2.3 Indonesia polyvalent antivenom serum
The Perum Bio Farma (Pasteur Institute) of Indonesia produced a polyvalent antivenom
serum. The antivenom (in liquid form) was raised against venoms from three venomous
snakes: Malayan pit viper (Calloselasma rhodostoma), Banded krait (Bungarus fasciatus)
and Javan spitting cobra (Naja sputatrix). The efficacy of this polyvalent antivenom against
envenomations by Malaysian venomous has not been investigated. However, it is possible
that this antivenom could neutralize venoms of Malayan pit viper, cobra and Banded krait
from Malaysia. However, the antivenom is likely to be ineffective against venom of Malayan
krait (Bungarus candidus) and Asian lance-headed viper (Trimeresurus complex). The

14
contact address of Perum Bio Farma is Jl Pasteur 28, PO Box 1136, Bandung 40161. (Tel
+6222-83755).
9.2.4 India Polyvalent Antivenoms
There are several antivenoms manufactuers in India, most of them produced polyvalent
antivenom raised agains the ‘Big Four’ of India venomous snakes: Indian cobra (Naja naja),
Indian krait (Bungarus caeruleus), Russell’s viper (Daboia russelli) and saw-scaled viper
(Echis carinatus). Followings are results of the preclinical assessment of the efficacy of
Indian polyvalent antivenom (against Malaysian snake venoms) produced by two different
manufacturers: Vins Bioproducts Ltd (Hyderabad, India) and Bharat Serums and Vaccines
Limited (Mumbai, India). The polyvalent antivenom produced by Vins is termed ‘Snake
Venom Antiserum I.P.’ whereas the antivenom produced by Bharat is termed Anti Snake
Venom Serum, or ASVS.
Vins Snake Venom Antiserum I.P.
Vins’ polyvalent antivenom is weakly to moderately effective against venoms of Malaysia
cobras (neutralization capacity 0.22 mg/mL and 1.18 mg/mL, respectively, against Naja
kaouthia and Naja sumatrana venom), weakly effective against king cobra (O. hannah, 0.22
mg/mL) and Malayan krait (B. candidus 0.22 mg/mL). It is not effective against another
common krait in Malaysia: Banded krait (B. fasciatus). It is not effective against Malayan pit
viper (Calloselasma rhodostoma) and Asian lance-headed viper (Trimeresurus complex)
Bharat ASVS
The Bharat’s ASVS is only weakly effective against venom of the Equatorial spitting cobra (N.
sumatrana, neutralization potency 0.31 mg/mL) and Malayan krait (B. candidus,
neutralization potency 0.14 mg/mL). It is not effective against other Malaysian elapid
venoms or pit viper venoms.
Note: the fact that both Vins and Bharat polyvalent antivenoms were not effective against
Malaysian pit viper venoms is not surprising as the Indian polyvalent antivenoms were
raised against venoms from Russell’s viper and saw-scaled viper, both from the subfamily
Viperidae (true viper or Old World viper), whereas the Malaysian pit vipers (Malayan pit
viper and Asia lance-headed vipers) belong to a different (evolutionary distant) subfamily,
Crotalinae (pit viper). The toxinology of venoms from Viperidae snakes is significantly
different from that of venoms from Crotalinae snakes.

15
RECOMMENDATIONS RE USAGE OF ANTIVENOMS IN TREATMENT OF SNAKE BITES IN
MALAYSIA
In Malaysia, particularly in the rural areas, species diagnosis is usually not possible. Hence
there is a need to have a polyvalent antivenom that can be used to for treatment of all
snake bites with systemic envenoming. Unfortunately, to date there is no such ‘cure all’
antivenom available.
The Indian polyvalent antivenom will not be effective against Malaysian pit viper bites. It
may be moderately effective in neutralization of cobra venom but unlikely to be of use in
krait bites.
The efficacy of Indonesia polyvalent antivenom against Malaysian snake venoms has not
been investigated, however, it is highly unlikely to be effective against venoms of the
Malayan krait, red-headed krait and pit viper of the Trimeresurus complex (eg, the
Cryptelytrops).
At the moment, the two Thai QSMI polyvalent antivenoms appear to be the most suitable
for treatment of systemic envenomations in Malaysia. It is easy to distinguish between
elapid (krait and cobra) bites and pit viper bites clinically—the former is mainly neurotoxic,
whereas the latter hemorrhagic. Neuro polyvalent antivenom can neutralize venoms from
all Malaysian cobras and kraits, whereas Hemato polyvalent antivenom can neutralize
venoms from all Malaysian pit vipers; except the Wagler’s pit viper, Tropidolaemus wagleri .
At the moment, there is no antivenom available to neutralize the venom of Wagler’s pit
viper.
9.3 Supportive/ Ancillary Treatment
a. If there is danger of respiratory paralysis, intubate or ventilate via tracheostomy.
Mechanical ventilation is recommended for patients with respiratory paralysis.
b. Treatment of local lesion: Massive tissue sloughing and necrosis, intracompartmental
syndrome, suppurative complications etc may need surgical intervention, however the
risks of surgery in a patient with hemostatic disturbances must be balanced against the
life-threatening complications of local envenoming.
c. Treatment of shock; correction of fluid imbalance (venous access is vital but topmost
care is needed for patients with hemostatic disturbances).
d. Renal replacement therapy (peritoneal dialysis in acute setting) if indicated.

16
e. Anticholinesterases e.g. edrophonium can partly overcome blockade by postsynaptic
neurotoxins.
f. Tetanus prophylaxis: A booster of tetanus toxoid is recommended for all snakebite
patients in the absence of coagulopathy.
g. Antibiotic use if indicated for infected wound.

17
Literatures on Malaysian venomous snakes and clinical observations and treatment of
snakebites in Malaysia:
Alirol, E., Sharma, S.K., Bawaskar, H.S., Kuch, U., Chappuis, F., 2010. Snake bite in South Asia: a
review. PLoS Negl Trop Dis. 4, e603.
Chippaux, JP and Goyffon, M., 1998. Venoms, antivenoms and immunotherapy.
Toxicon. 36, 823-846.
Gutiérrez, J.M., Theakston, R.D.G., Warrell, D.A., 2006. Confronting the Neglected Problem of
Snake Bite Envenoming: The Need for a Global Partnership. PLoS Med. 3, e150.
Harrison, R.A., Hargraves, A., Wagstaff, S.C., Faragher, B., Lalloo, D.G. 2009., Snake envenoming:
a disease of poverty. PLoS Negl Trop Dis. 3, e569.
Jamaiah, I., Rohela, M., Roshalina, R. and Undan, R.C. (2004) Prevalence of snake bites in Kangar
District Hospital, Perlis, West Malaysia: A retrospective study (Jan 1999-Dec 2000).
Southeast Asian J Trop Med Public Health, 35: 962-965.
Jamaiah, I., Rohela, M., Ng, T.K., Ch’ng, K.B.H., Teh, Y.S., Nurulhuda, A.L. and Suhaili, N. (2006)
Retrospective prevalence of snaket bites from hospital Kuala Lumpur (HKL), Southeast
Asian J. Trop. Med. Public Health, 37:200-206.
Kasturiratne, A., Wickremasinghe, A.R., de Silva, N., Gunawardena, N.K., Pathmeswaran, A.,
Premaratna R., Savioli, L., Lalloo, D.G., de Silva, H.J. (2008) Estimation of the global
burden of snakebite. PLoS Med 5(11): e218. doi:10.1371/journal.pmed.0050218
Lim, B.L. (1982) Poisonous Snakes of Peninsular Malaysia. 2nd Ed. Malayan Nature Society,
Kuala Lumpur, 72pp.
Mitrakul, C. (1973). Effects of green pit viper venoms on blood coagulation, platelets and the
fibrinolytic enzyme systems: studies in vivo and in vitro. Am. J. clin. Pathol. 60, 654-662.
Reid, H.A., Lim, K.J. (1957). Sea-snake bite. Br. Med. J. 2, 1266-1272.
Reid, H.A., Chan, K.E. and Thean, P.C. (1963). Prolonged coagulation defect (defibrination
syndrome) in Malayan viper bite. Lancet, i, 621-626.
Reid, H.A., Thean, P.C., Chan, K.E. and Baharom, A.R. (1963). Clinical effects of bites by Malayan
viper. Lancet i, 617-621.
Reid, H.A. (1964). Cobra bites. Br. Med. J. 2, 540-545.
Reid, H.A. (1968) Symptomatology, pathology and treatment of land snake bites in India and
Southeast Asia. In: Venomous Animals and Their Venoms. Vol.1. (Buckely, E.D., Bucheri,
W., and Deulofeu, V. Eds.), Academic Press, New York. Pp. 611-642.
Reid, H.A., Theakston, R.D.S. (1983). The management of snake bite. Bull. W.H.O., 61, 885-895.
Tan, K.K., Choo, K.E., Ariffin, W.A. (1990) Snake bite in Kelantanese children: A five year
experience. Toxicon, 28:225-230.
Tan, N.H. (1991) The biochemistry of venoms of some venomous snakes of Malaysia. – A
Review. Tropical Biomedicine 8, 91-103.

18
Tan, N.H., Choy, S.K., Chin, K.M. and Gnanajothy, P. (1994): Cross-reactivity of monovalent and
polyvalent Trimeresurus antivenoms with venoms from various species of Trimeresurus
(lance-headed pit viper) snake. Toxicon, 32, 849-853.
Tweedie, M.W.F. (1983). The snakes of Malaya. (3rd Ed.) Singapore National Printers, Singapore.
Warrell, D.A. (1999). WHO/SEARO guidelines for the clinical management of snake bites in the
South East Asian Region. Southeast Asian J. Trop. Med. Pub. Health, 30, Supplement 1.
(available on-line: http://www.tm.mahidol.ac.th/seameo/1999-30-spp-1/Clinical-
Manage-Snake-Bites-Southeast-1999-30-Suppl-1-Cover.pdf)
Warrell, D.A., Looareesuwan, S., White, N.J., Theakston, R.D.G., Warrell, M.J., Kosakarn, W.,
Reid, H.A. (1983). Severe neurotoxic envenoming by the Malayan krait, Bungarus
candidus: response to antivenom and anti-cholinesterase. Br. Med. J. 286, 678-689.
Warrell, D.A., Theakston, R.D.G., Phillips, R.E., Chanthavanich, P., Viravan, C., Supanaranond, W.,
Karbwang, J., Ho, M., Hutton, R.A., Vejcho, S. (1986). Randomized comparative trial of
three monospecific antivenoms for bites by the Malayan pit viper (Calloselasma
rhodostoma) in southern Thailand: clinical and laboratory correlations. Am. J. Trop. Med.
Hyg. 35, 1235-1247.
World Health Organization (2009. Neglected tropical disease: snakebite. WHO: Geneva.
Websitee:
http://www.who.int/neglected_diseases/diseases/snakebites/en/index.htmlhttp://jpet.asp
etjournals.org/cgi/ijlink?linkType=ABST&journalCode=jpet&resid=269/3/1079
World Health Organization (2011). The clinical management of snake bites in the South East
Asian Region. WHO Regional Office of South East Asia. Website:
http://www.searo.who.int/en/Section10/Section17/Section53/Section1024_3899.htm