a body mind & spirit healing - stvhs.com · a body mind & spirit approach to 2016 annual...
TRANSCRIPT

A Body, Mind & Spirit Approach to
2016 ANNUAL REPORT & 2015 STATISTICAL REVIEW
CANCER PROGRAMHealing

CALL TO ACTIONHealthcare That WorksHealthcare That Is SafeHealthcare That LeavesNo One Behind For Life
CORE VALUESService of the Poor
ReverenceIntegrityWisdom
CreativityDedication
CANCER PROGRAM
ENABLING STRENGTHSInspired People
Trusted PartnershipEmpowering Knowledge
Vital PresenceStewardship
CANCER REPORT | 3
LUNG CANCER is the number one cause of cancer related death in men and women. In our patients this is no different from the rest of the U.S. population. In reviewing our trends in diagnosis of lung cancer over the last 5 years it is apparent that 45% of our patients present with Stage 4 disease which has a higher mortality and worse prognosis. Advanced Stage Lung Cancer has a 5 year survival rate of less than 10%. Our Low Dose Screening CT program should help us find lung cancer in our patients at a much earlier stage.
The National Lung Screening Trial (NSLT) showed a 20% reduction in lung cancer specific mortality and a stage shift towards early diagnosis with 70% of lung cancer being diagnosed at early stages in the study patient population. It has also been shown that earlier diagnosis and treatment of lung cancer is cost effective for our health care system. Various health organizations including the National Comprehensive Cancer Network (NCCN), American Cancer Society, and American Lung Association all have made recommendations to screen the specific high risk patient population with Low Dose Chest CT. In our system we use the
LOW DOSE SCREENING CT FOR LUNG CANCER
Why and How We Are Doing It at St. Vincent’s East Cancer Treatment Center
criteria recommended by the Centers for Medicare and Medicaid Services (CMS) which are generally accepted and similar to recommendations made by various organizations.
In establishing our Low Dose Screening CT program we felt that it was extremely important to make sure our patients receive appropriate follow up and treatment. All patients are scheduled through our cancer center where they can be tracked by our nurse navigator.
Medicare will cover Low Dose Screening CT in patients who meet the following criteria:
• 55 to 77 years of age
• Current smokers or quit smoking in the last 15 years
• Smoking history of at least 30 pack years (smoking one pack /day for 30 years)
• Have a written order from a health care provider and have undergone counseling and shared decision making on risks and benefits of Screening CT for Lung Cancer
Tribute to Dr. MorrosIt is with great sadness that the associates and physicians of the St. Vincent’s East Cancer Treatment Center learned of the passing of Dr. Demetrius “Jimmy” Morros on November 20, 2016. For the past 18 years, Dr. Morros served the patients at St. Vincent’s East with great skill and compassion. He was a dedicated father, husband and physician. He had great enthusiasm for the profession of medicine and devoted much time and energy to continually improving the practice of radiology.
He was a graduate of Birmingham Southern College and the University of Alabama Medical College. He received his four year residency in Radiology at the University of Cincinnati, and completed a year’s Interventional Fellowship in Radiology at the University of Alabama, Birmingham. He was a Fellow of the American College of Radiology, and was actively involved in the Alabama Chapter of the American College of Radiology, serving as President of the chapter for two years.
Demetrius K. Morros, MDRadiology
4 ST. VINCENT’S EAST
Our patient data is reported to the American College of Radiology Lung Cancer Screening Registry, and rescreening and follow up is determined by the American College of Radiology Lung-RADS system which assigns findings on Chest CT into categories by imaging criteria and is a standardized system for follow up and additional testing when necessary. When a nodule is detected on a patient’s CT based on size and other imaging characteristics we know when it is more likely to be cancer and when it is more likely to be benign. This system allows us to follow nodules that are benign when appropriate and refer patients who
have nodules with more worrisome characteristics for earlier biopsy and treatment.
We feel that our Low Dose Screening CT program will help our patients and will find more lung cancers sooner when the prognosis is better and the outcomes for our patients are better. Patients who wish to participate in our program should discuss this with their physician and can be scheduled for the test by contacting the St. Vincent’s East Cancer Treatment Center.
Please contact our Nurse Navigator, Rhonda Reese at 205-838-3657 for more information.
Reference:Christiansen, Jared, Laroia, Archana et al. Lung Cancer Screening Education From Science to Practice, 2015, Kanne, Jeffrey, Online Course, American College of Radiology < http://www.acr.org/Education/e-Learning/Lung-Cancer-Screening-Education>
Earlier diagnosis and treatment of lung cancer is cost effective for our
health care system
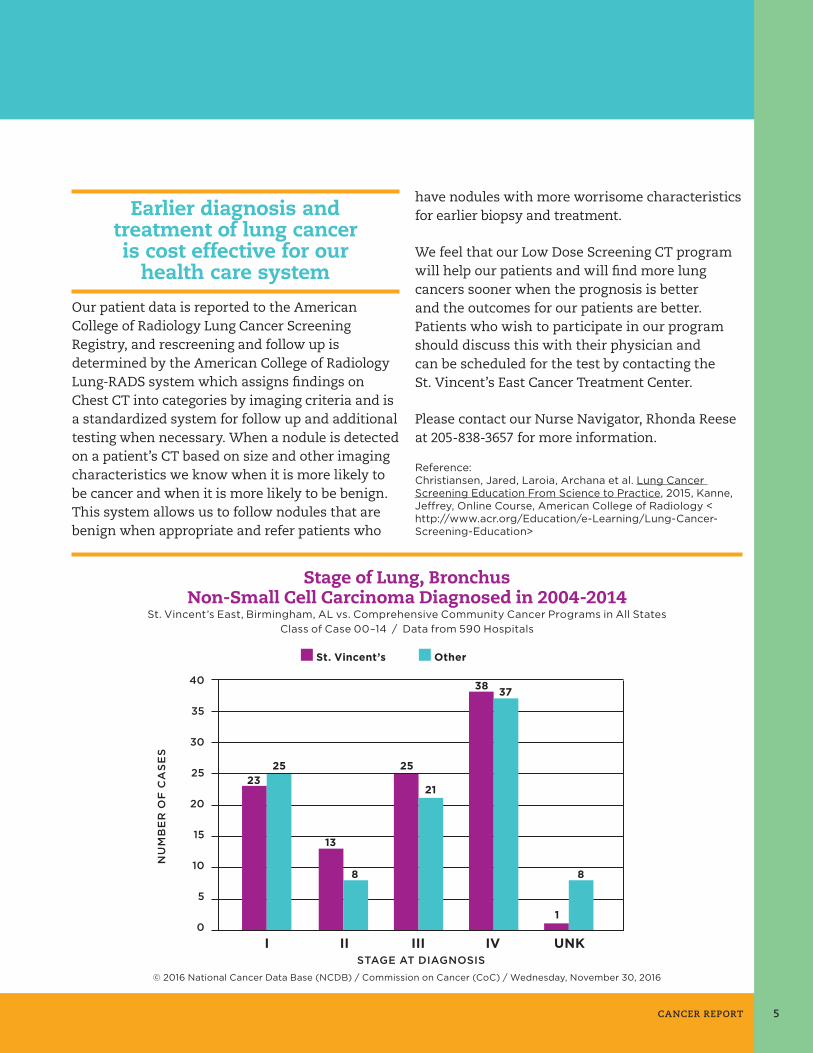
Stage of Lung, BronchusNon-Small Cell Carcinoma Diagnosed in 2004-2014
St. Vincent’s East, Birmingham, AL vs. Comprehensive Community Cancer Programs in All StatesClass of Case 00–14 / Data from 590 Hospitals
St. Vincent’s Other
STAGE AT DIAGNOSIS
40
35
30
25
20
15
10
5
0I II III IV UNK
NU
MB
ER
OF
CA
SE
S
2325 25
21
38 37
13
8 8
1
© 2016 National Cancer Data Base (NCDB) / Commission on Cancer (CoC) / Wednesday, November 30, 2016
CANCER REPORT 5

DIRECTOR’S LETTER
Best regards,
Johnny Karr BS, (R) ARRTAdministrative Director of Clinical Services
THE CANCER PROGRAM at St. Vincent’s East is committed to the delivery of excellent and compassionate care for all our patients. This Fiscal Year we are excited to announce that the Cancer Treatment Center at East has added the latest cancer-fighting technology with the Varian TrueBeam. The TrueBeam is an advanced radiotherapy system from Varian that dynamically synchronizes imaging, patient positioning, motion management and treatment delivery. This new technology will go a long way to consistently improve patient outcomes and increase our patient satisfaction.
Since early detection of cancer saves lives, the Cancer Program continues to focus on community events that promote cancer awareness, screening, early detection and prevention. St. Vincent’s East is also designated by the American College of Radiology as a Lung Cancer Screening Site.
We appreciate the support of the St. Vincent’s Foundation, St. Vincent’s East Auxiliary, physicians, and associates who continue to work together to ensure we are able to meet the needs of our patients and their families during their diagnosis, treatment, and recovery. As always we look forward to a very successful year for our patients and for the Cancer Program at St. Vincent’s East.
Dr. James M. Kamplain, MDRadiation/Oncology Chairman
Stephen Heinzman, MDGeneral Surgery/Cancer Liaison Physician
Dr. Kent Tucker, MDHematology/OncologyConference Coordinator
Jared Cox, MD Urology
Bryan Pruitt, M.D.Obstetrics and Gynecology
Patrick Druhan, MDRadiology
Maria Johnson, MDInternal/Pulmonary Medicine
Jonathan G. Phillips, MDPathology
Shaily Lakhanpal, MDHematology/Oncology
Emily Hopkins, RHITHealth Information Management
Barry Bruce, M.Div., BCCSpiritual Care
Deidra Bentley, RN, BSNOperating Room Representative
Rose Waddell, RNCase Management
Karen Willette, MS, CCC-SLPPhysician Therapy
Erin Adamson, BS, CRCClinical Research Coordinator
Kimberly Wigley, MSHA, LPC, FACHEPsychosocial Services Coordinator
Anna Lisa WeigelAmerican Cancer SocietyHealth Systems Manager
Marc Bloomston, M.D. V.P. Medical Staff Affairs
Diana Scalici, MSHA, MBAV.P. Operations
Johnny Karr, BS, (R) ARRTCancer Program Director
Rhonda Reese, BSN, RNNavigatorCommunity Outreach Coordinator
Carol Kennemur, RHIT, CTRCancer Registry Coordinator
Sharon Cooper Davison, RN, BSNUnit Manager, 5 East, 5 West
Linda Adams, RPh., MBAPharmacy Director
Donna Odom, RN, MSNQuality Improvement Coordinator
CANCER COMMITTEE 2017
6 ST. VINCENT’S EAST

CHAIRMAN’S LETTER
ON BEHALF OF the multidisciplinary Cancer Committee of St. Vincent East Hospital, I am pleased to present the 2016 Annual Report. This report reflects our goals, studies of quality and quality improvements, screening and prevention activities and incidence data, for the calendar year 2015. Our comprehensive cancer program provides a network of oncology services specializing in the prevention, diagnosis, treatment, and management of patients with cancer. The experienced and caring staff of the Cancer Program offers a multidisciplinary approach to the diagnosis and treatment of each individual cancer patient.
This report reflects this approach to patient care including not only physicians but also chaplains, social workers, nurses and other healthcare workers. The goal of the Cancer Program is to provide the highest quality of patient care, exceeding the expectations of patients and their families throughout the course of a cancer illness. In addition, with the help of our Education Department, the Cancer Committee supports a wide range of preventive and educational programs designed to enhance early detection of cancer when the disease is most curable. The Cancer Committee continues to meet quarterly to supervise the activities of the Cancer Program. The multidisciplinary Cancer Conferences which meet twice a month as well as a Chest Cancer Conference which meets once a month provide an excellent forum for a prospective discussion of cancer cases where current treatments available both here at the hospital but also thru national investigational protocols are discussed.
To members of our community, our Cancer Program offers quality cancer care that is close to home. St. Vincent East now offers cutting edge screening programs with the development of our lung cancer screening program. By offering low dose CT scans of the lungs for particular individuals at significant risk of developing lung cancer this offers the ability to diagnose the cancer at its earliest stage. Lung cancer continues to be a significant cause of cancer deaths but has an 88 percent survival rate when caught in early stages. The program provides prompt detection and timely care for patients whose test results indicate abnormalities. I am happy to report that with the installation of our new linear accelerator we will be able to offer advanced cancer care, including radiosurgery capabilities to our patients in a community hospital setting.
St. Vincent East continues to be involved in its support of community cancer screenings, cancer prevention activities and education. We are truly fortunate to be able to offer such programs as Bosom Buddies, TOUCH, Camp Bluebird, and “Look Good Feel Better” for emotional support of our patients.
The Tumor Registry is involved in collecting data on cancer type, stage of disease, first course of treatments, and offers lifelong patient follow-up. A total of new 606 analytic cancer cases diagnosed in 2015 were added to the Cancer Registry’s database. We are truly fortunate to have the particular specialists here at St. Vincent East to manage these challenging cases.
The Cancer Committee is also involved in studies that measure the quality of care and outcomes for patients with cancer. This year we have reported on lung cancer. There has been significant progress in the screening, and treatment of this disease with the use of low dose CT scans for screening and in the treatment of the disease with the use of stereotactic radiosurgery and targeted molecular therapies. Both of which are now and will soon be available here.
I would also like to congratulate all Cancer Committee members, Cancer Leadership members, medical staff physicians, nurses, ancillary departments and other support personnel for another job well done. It is through these cooperative efforts that make our Cancer Program successful. We will continue to improve and advance the level of care and service we provide to patients and families in our community.
James M. Kamplain, M.D. FACRRadiation Oncologist
CANCER REPORT 7

COMMUNITY OUTREACH ANNUAL REPORT
PREVENTION / AWARENESS PROGRAM
PROGRAM/ COMMUNITY NEED
ADDRESSEDACTIVITIES DATE DISCUSSED
DATE PROGRAM HELD
# OF PARTICIPANTS
GUIDELINE USEDSUMMARY OF
EFFECTIVENESS
SVE hospital auxiliary breast presentation.
CNA – over ¼ all cancers reported were
breast 78% seldom or never perform SBE (avg. age
55-70)
Breast Cancer Awareness. Printed
educational material: How to check your
breast.Breast model to learn how to perform self-breast examinations.
8/9/2016 at Cancer
Committee
9/19/2016 33 American College of Obstetricians
and Gynecologists
American Cancer Society
(recommends)
100% reported presentation informative and learned something
new.
Oktoberfest – Trussville
Educational presentation based on community needs of knowledge related to
cancer
Informational booth for breast cancer
awareness. Printed material available
related to prevention, early detection,
and mammograms. A breast model to
practice self-exams.
8/9/2016 10/8/2016 112 American Cancer Society
59 people took printed material related to breast
cancer/mammograms.
79 people practiced on the breast model.
88% stated they were not aware of the amount of
pressure needed for breast exams
Cross Point – women’s group
PresentationCNA – 78% unaware
of importance of self-exam to be
familiar with their body
Breast Cancer Awareness. Supplied printed material: How to check your breast.
Breast model to learn how to perform
self- breast exams.
8/9/2016 at Cancer
Committee
8/31/2016 23 American College of Obstetricians
and Gynecologists
American Cancer Society
(recommends)
83% stated they learned something
new.
3 women stated they would schedule a
mammogram.
Follow up – all 3 negative.
SCREENING PROGRAM
PROGRAM/ COMMUNITY NEED
ADDRESSEDACTIVITIES DATE DISCUSSED
DATE SCREENING HELD
# OF PARTICIPANTS
GUIDELINE USEDSUMMARY OF
EFFECTIVENESS
LDCT lung screening month Nov. 1-30, 2016
Community Needs Assessment (CNA) – to decrease the # late
stage lung cancers. NCI – lung cancer rate: Al. rate 71.3 / USA rate
62.4
Flyers placed in the community with
criteria for screening. Educational materials
placed throughout hospital and clinics.
8/9/2016 at cancer
committee
Month of November
4 American College of Radiology
American Cancer Society
3 of 4 were negative.
One screen requires a follow up in 3 months.
8 ST. VINCENT’S EAST

2017 SCHEDULE OF EDUCATIONAL AND CANCER SUPPORT PROGRAMS
BOSOM BUDDIESBosom Buddies is a breast cancer support group that meets once per month to give women the opportunity to talk with others who have been through similar experiences. The group is usually comprised of 15–20 women, some recently diagnosed and others who are long-term survivors of breast cancer. Bosom Buddies meets on the third Wednesday of every month from 12–1 p.m. Pre-registration is required.
LOOK GOOD… FEEL BETTERThis program is for any woman undergoing cancer treatment. A certified professional teaches women how to cope with the appearance-related side effects of cancer treatment which may include hair loss and changes in complexion. Free make-up kits valued at $300 are provided. Look Good… Feel Better is scheduled quarterly. Registration is required to ensure availability of make-up kits. For more information call Support Services at 205-838-3519 or the American Cancer Society at 205-930-8876.
All Programs are offered at no cost. Please call 205-838-3519.
REACH TO RECOVERYReach to Recovery is an American Cancer Society volunteer visitation program that helps breast cancer survivors meet the emotional, physical and cosmetic needs related to breast cancer. Call the American Cancer Society at 205-930-8876 for a referral to the Reach to Recovery program.
US TOOUs TOO is a prostate cancer survivors support group that meets once per month to give men the opportunity to discuss symptoms and side effects of their diagnosis. The prostate cancer support group meets the second Wednesday of every month from 12–1 p.m.
TOUCH (TODAY OUR UNDERSTANDING OF CANCER IS HOPE)TOUCH is a general support group that provides information, understanding, caring and hope for cancer survivors and their families. TOUCH meets the first Wednesday of every month from 12–1 p.m.
Cancer screening for 2017, featuring colorectal cancerMarch is Colorectal Cancer Awareness Month, lets support the American Cancer Society by reaching the goal of 80% screened for colorectal cancer by 2018.
According to U.S. Preventive Services Task Force (USPSTF), colorectal cancer is the second leading cause of death from cancer. The key to reducing the mortality rate from colorectal cancer is early detection and prevention. While colonoscopy is considered the first choice for screening, the fecal immunochemical tests (FIT) is an alternative method for detecting colorectal cancer. However, there are some advantages and disadvantages to the FIT.
ADVANTAGES• No cleansing of the colon is necessary
• No dietary restrictions are needed before FIT
• Samples can be collected at home
• Cost is low compared with other screening tests
• No sedation is needed
DISADVANTAGES• The test does not detect some polyps and cancers
• False-positive test results are possible
• Additional procedures, such as colonoscopy, may be needed if the test result shows blood in the stool
CANCER REPORT 9

LUNG CANCER is the second most common malignancy diagnosed in both men and women. In the state of Alabama there are expected to be 27000 new cases of cancer with 4200 new cases being lung cancer. Although the incidence of lung cancer has decreased in men by 3% and 1.9% in women since 2008 the actual numbers of patients is increasing due to the increased numbers of people who are at risk of developing lung cancer due to advancing age. The median age at diagnosis is 70.
Lung cancer accounts for more deaths than any other cancer in men and women accounting for 1 in 4 deaths due to cancer nation-wide. Fortunately the death rates have declined by 38% in men since 1990 and 12% in women due to the drop in smoking prevalence which is the by far the most important risk fact for lung cancer. However, lung cancer is the 4th most prevalent cancer in the world. Of the various types of lung, non-small cell lung cancer is the most prevalent type with adenocarcinoma being the most frequent followed by squamous cell type. These types of lung cancer are felt to be distinct from the small cell or oat cell type of lung cancer which spreads much more rapidly and represent the remaining 15% of lung cancers. Previously there really was no good way to screen for lung cancer. However now with the use of low-dose spiral CT scans lung cancer can be detected at a much earlier stage and has been shown to reduce lung cancer mortality by 20% compared to standard chest x-ray among adults with at least a 30-pack year smoking history. Such a screening program is now available here at St. Vincent East and is actively accepting patients. The fact that untreated early Stage I lung cancer of all non-small cell lung cancer types has an overall mean survival time of only 12 months further confirms the very grim prognosis of having lung cancer.
Lung cancer is an extremely heterogeneous family of malignant neoplasms, with well over 50 different histological variants recognized under the 4th revision of the World Health Organization (WHO) typing system with 98% being malignant in nature. The most widely used lung cancer classification scheme separates lung cancer into two basic types, i.e. small cell or oat cell type and non-small cell type.
Because these variants have differing genetic, biological, and clinical properties, including response to treatment, correct classification of lung cancer cases are necessary to assure that lung cancer patients receive optimum management.
Treatment of lung cancer is based on whether the tumor is the small cell or non-small cell type. This is due to
LUNG CANCER FACTS
the small cell type spreading so rapidly chemotherapy is the mainstay of therapy. The treatment of non-small cell type lung cancer is based on the stage of the disease which determines the type of therapy which can include surgery, radiation, and chemotherapy in various combinations. It is now recognized that even in the specific types of non-small cell lung cancer; there exist specific molecular types which can be identified by special molecular testing procedures done on the original tumor tissue. These tests help to differentiate a particular type which would potentially respond to the newest type of systemic therapy with what are referred to as targeted or biological agents. Targeted therapy of lung cancer refers to using agents specifically designed to selectively target molecular pathways responsible for, or that substantially drive, the growth of lung cancer cells, and as a consequence of this (relative) selectivity, cause fewer toxic effects on normal cells.
As noted in our patient population most of the patients who are diagnosed are of advanced age and with advanced Stage III-IV disease. The addition of targeted therapies in these patients with advanced disease has significantly changed the options available to this group of patients.
A more optimistic outlook in patient with lung cancer hopefully will result from the use of screening with low-dose CT scanning. This would hopefully significantly change the distribution to earlier stage disease where the results of treatment are significantly better. Another reason for a more optimistic prognosis
First Course Treatment of Lung, Bronchus
Non-Small Cell Carcinoma Diagnosed in 2004-2014
St. Vincent’s East, Birmingham, AL vs. Comprehensive Community Cancer Programs in All States
Class of Case 00–22 / Data from 590 Hospitals
First Course Treatment SVE (N) Oth. (N) SVE (%) Oth. (%) TOTAL 885 499934 100% 100%Radiation & Chemotherapy 172 98434 19.44% 19.69%Surgery Only 168 97009 18.98% 19.40%No 1st Course Rx 165 119483 18.64% 23.90%Chemotherapy Only 131 68288 14.80% 13.66%Radiation Only 130 64723 14.69% 12.95%Surgery & Chemotherapy 72 22754 8.14% 4.55%Surgery, Radiation & Chemotherapy 31 11946 3.50% 2.39%Surgery & Radiation 14 4157 1.58% 0.83%Other Specified Therapy 2 9391 0.23% 1.88% Surgery, Radiation & Hormone Therapy . 13 . 0%
10 ST. VINCENT’S EAST
in early stage lung cancers will be the addition of a new linear accelerator here at St. Vincent East which will make available stereotactic body radiation. This type of therapy also known as stereotactic ablative radiotherapy is a technique of external beam radiation that delivers precisely targeted, ablative doses of radiation. For patients with early stage non-small cell lung cancer, surgical resection is the most established treatment. However, due to many patients having significant lung and heart problems many patients are not felt to be surgical candidates. With the use of stereotactic radiotherapy, this type of therapy has demonstrated that it is just as successful in curing early stage lung cancer as surgery with similar rates of local control and survival, and yet has very low risks
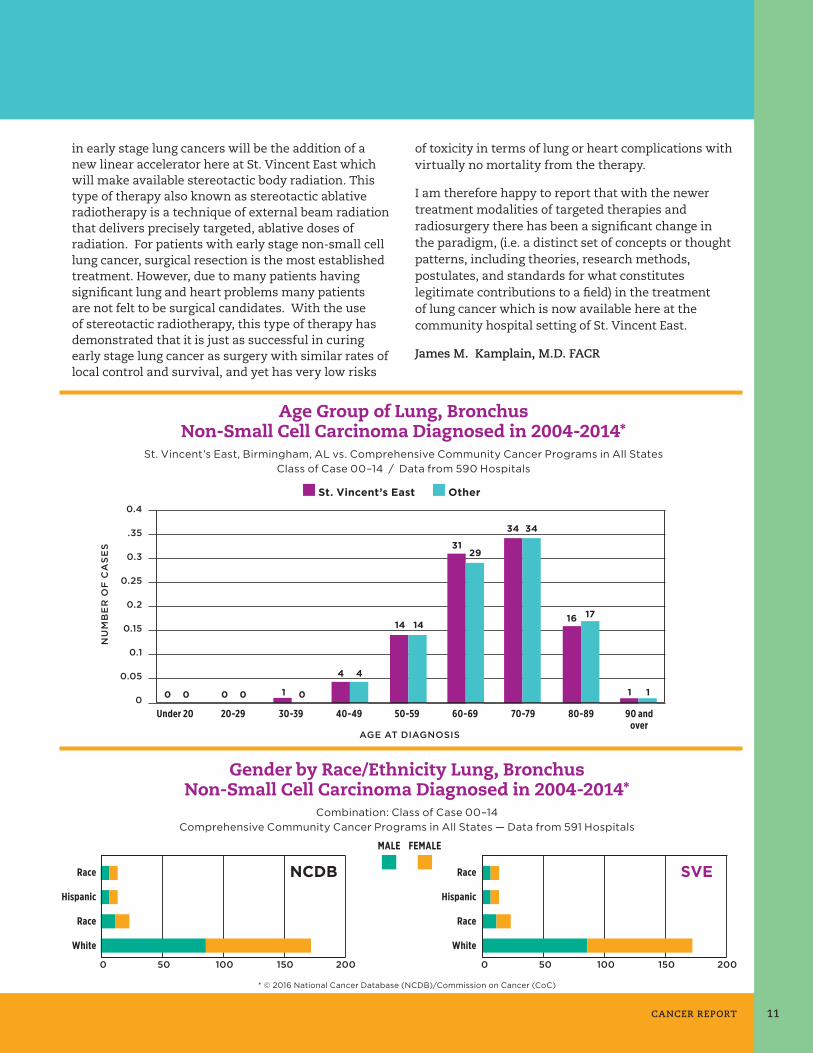
Age Group of Lung, BronchusNon-Small Cell Carcinoma Diagnosed in 2004-2014*
St. Vincent’s East, Birmingham, AL vs. Comprehensive Community Cancer Programs in All StatesClass of Case 00–14 / Data from 590 Hospitals
St. Vincent’s East Other0.4
.35
0.3
0.25
0.2
0.15
0.1
0.05
020-29Under 20 30-39 40-49 50-59 60-69 70-79 80-89 90 and
over
NU
MB
ER
OF
CA
SE
S
AGE AT DIAGNOSIS
0 0 1
4
14
34
16
1
31
0 0 0
4
14
34
17
1
29
of toxicity in terms of lung or heart complications with virtually no mortality from the therapy.
I am therefore happy to report that with the newer treatment modalities of targeted therapies and radiosurgery there has been a significant change in the paradigm, (i.e. a distinct set of concepts or thought patterns, including theories, research methods, postulates, and standards for what constitutes legitimate contributions to a field) in the treatment of lung cancer which is now available here at the community hospital setting of St. Vincent East.
James M. Kamplain, M.D. FACR
Gender by Race/Ethnicity Lung, BronchusNon-Small Cell Carcinoma Diagnosed in 2004-2014*
Combination: Class of Case 00–14Comprehensive Community Cancer Programs in All States — Data from 591 Hospitals
0 50 100 150 200
Race
Hispanic
Race
White
NCDB
0 50 100 150 200
Race
Hispanic
Race
White
SVE
MALE FEMALE
* © 2016 National Cancer Database (NCDB)/Commission on Cancer (CoC)
CANCER REPORT 11
CANCER REGISTRY REPORT
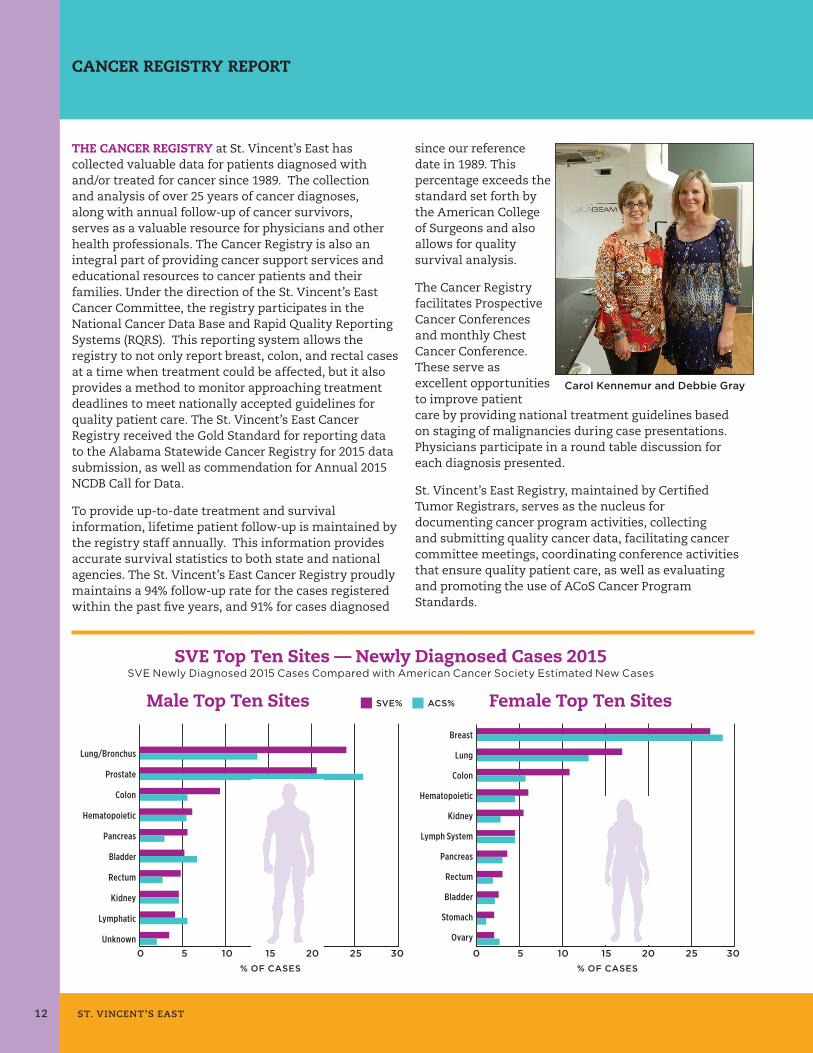
THE CANCER REGISTRY at St. Vincent’s East has collected valuable data for patients diagnosed with and/or treated for cancer since 1989. The collection and analysis of over 25 years of cancer diagnoses, along with annual follow-up of cancer survivors, serves as a valuable resource for physicians and other health professionals. The Cancer Registry is also an integral part of providing cancer support services and educational resources to cancer patients and their families. Under the direction of the St. Vincent’s East Cancer Committee, the registry participates in the National Cancer Data Base and Rapid Quality Reporting Systems (RQRS). This reporting system allows the registry to not only report breast, colon, and rectal cases at a time when treatment could be affected, but it also provides a method to monitor approaching treatment deadlines to meet nationally accepted guidelines for quality patient care. The St. Vincent’s East Cancer Registry received the Gold Standard for reporting data to the Alabama Statewide Cancer Registry for 2015 data submission, as well as commendation for Annual 2015 NCDB Call for Data.
To provide up-to-date treatment and survival information, lifetime patient follow-up is maintained by the registry staff annually. This information provides accurate survival statistics to both state and national agencies. The St. Vincent’s East Cancer Registry proudly maintains a 94% follow-up rate for the cases registered within the past five years, and 91% for cases diagnosed
since our reference date in 1989. This percentage exceeds the standard set forth by the American College of Surgeons and also allows for quality survival analysis.
The Cancer Registry facilitates Prospective Cancer Conferences and monthly Chest Cancer Conference. These serve as excellent opportunities to improve patient care by providing national treatment guidelines based on staging of malignancies during case presentations. Physicians participate in a round table discussion for each diagnosis presented.
St. Vincent’s East Registry, maintained by Certified Tumor Registrars, serves as the nucleus for documenting cancer program activities, collecting and submitting quality cancer data, facilitating cancer committee meetings, coordinating conference activities that ensure quality patient care, as well as evaluating and promoting the use of ACoS Cancer Program Standards.
SVE Top Ten Sites — Newly Diagnosed Cases 2015SVE Newly Diagnosed 2015 Cases Compared with American Cancer Society Estimated New Cases
Lung/Bronchus
Prostate
Colon
Hematopoietic
Pancreas
Bladder
Rectum
Kidney
Lymphatic
Unknown0 5 10 15 20 25 30
% OF CASES
Male Top Ten Sites ACS%SVE% Female Top Ten Sites
0 5 10 15 20 25 30
Breast
Lung
Colon
Hematopoietic
Kidney
Lymph System
Pancreas
Rectum
Bladder
Stomach
Ovary
% OF CASES
Carol Kennemur and Debbie Gray
12 ST. VINCENT’S EAST
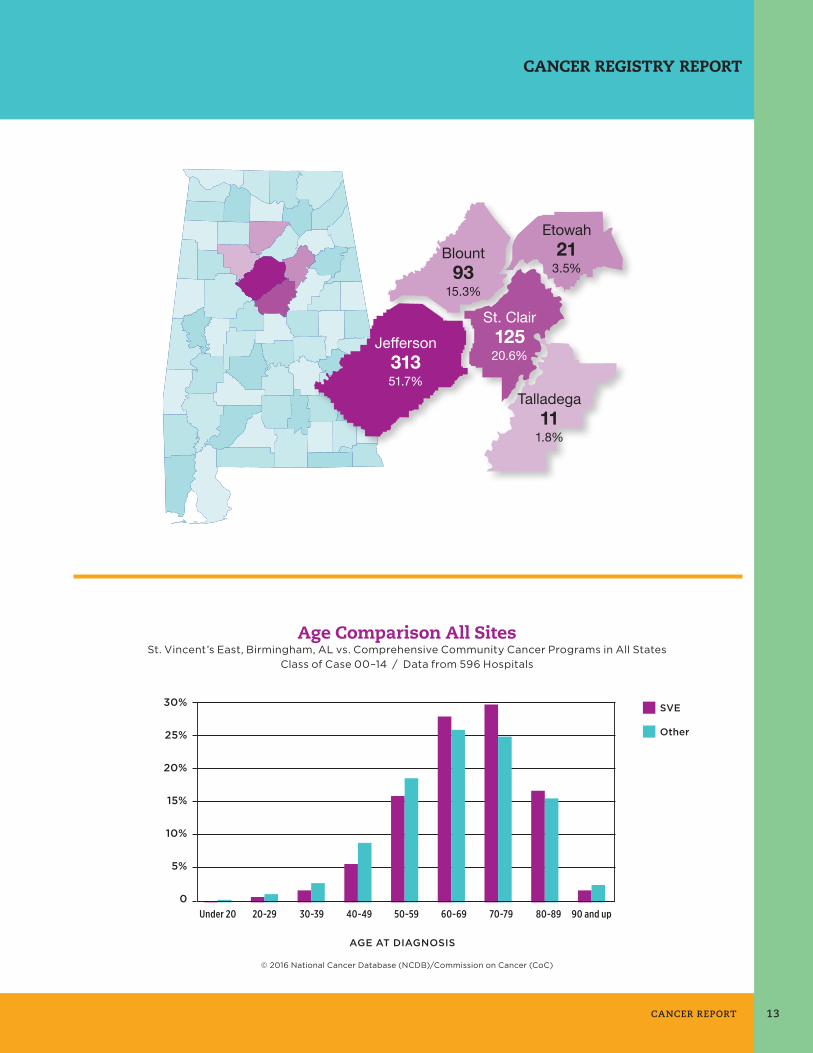
CANCER REGISTRY REPORT
Blount93
15.3%
Etowah21
3.5%
Talladega11
1.8%
Jefferson31351.7%
St. Clair12520.6%
SVE
Other
30%
25%
20%
15%
10%
5%
090 and up20-29Under 20 30-39 40-49 50-59 60-69 70-79 80-89
Age Comparison All SitesSt. Vincent’s East, Birmingham, AL vs. Comprehensive Community Cancer Programs in All States
Class of Case 00–14 / Data from 596 Hospitals
AGE AT DIAGNOSIS
© 2016 National Cancer Database (NCDB)/Commission on Cancer (CoC)
CANCER REPORT 13

PRIMARY SITE TABULATION FOR 2015 ANALYTIC CASES
*Green indicates top ten analytic cases treated at St. Vincent’s East in 2014.
ALL SITES 606 311 295 43 131 144 90 118 11
ORAL CAVITY 6 4 2 0 0 0 2 4 0
Tongue 3 2 1 0 0 0 1 2 0
Oropharynx 0 0 0 0 0 0 0 0 0
Hypopharynx 0 0 0 0 0 0 0 0 0
Other 3 2 1 0 0 0 1 2 0
DIGESTIVE SYSTEM 148 78 70 12 35 42 20 30 8
Esophagus 4 3 1 0 0 2 1 1 0
Stomach 9 3 6 1 2 2 1 2 1
Colon 61 29 32 8 13 21 10 8 1
Rectum 24 15 9 2 9 6 5 2 0
Anus/Anal Canal 5 1 4 1 2 2 0 0 0
Liver 10 7 3 0 1 0 0 6 2
Pancreas 27 17 10 0 7 5 1 11 3
Other 8 3 5 0 1 4 2 0 1
RESPIRATORY SYSTEM 130 77 53 0 21 14 35 60 0
Larynx 3 1 2 0 1 0 1 1 0
Lung/Bronchus 125 75 50 0 20 13 34 58 0
Other 1 1 0 0 0 0 0 1 0
BLOOD & BONE MARROW 37 19 18 0 0 2 0 0 0
Leukemia 18 11 7 0 0 2 0 0 0
Multiple Myeloma 11 5 6 0 0 0 0 0 0
Other 8 3 5 0 0 0 0 0 0
CONNECT/SOFT TISSUE 4 3 1 0 2 0 1 1 0
MELANOMA 4 1 3 0 2 0 2 0 0
BREAST 81 1 80 18 28 21 12 2 0
FEMALE GENITAL 12 0 12 0 3 1 4 4 0
Cervix Uteri 1 0 1 0 0 0 0 1 0
Corpus Uteri 4 0 4 0 2 0 0 2 0
Ovary 6 0 6 0 1 0 4 1 0
Other 1 0 1 0 0 1 0 0 0
PROSTATE 63 63 0 0 4 45 7 7 0
URINARY SYSTEM 57 31 26 13 25 11 3 4 1
Bladder 23 16 7 10 5 6 1 1 0
Kidney/Renal 30 14 16 2 18 5 1 3 1
Other 4 1 3 1 2 0 1 0 0
BRAIN & CNS 15 8 7 0 0 0 0 0 0
Brain (Malignant) 4 3 1 0 0 0 0 0 0
Other 11 5 6 0 0 0 0 0 0
ENDOCRINE 5 1 4 0 4 0 0 0 0
Thyroid 4 1 3 0 4 0 0 0 0
Other 1 0 1 0 0 0 0 0 0
LYMPHATIC SYSTEM 26 13 13 0 7 8 3 5 2
Hodgkin’s Disease 1 1 0 0 0 1 0 0 0
Non-Hodgkin’s 25 12 13 0 7 7 3 5 2
UNKNOWN PRIMARY 16 11 5 0 0 0 0 0 0
OTHER/ILL-DEFINED 2 1 1 0 0 0 1 1 0
PRIMARY SITE TOTAL SEX STAGE GROUP
M F 0 I II III IV UNK
14 ST. VINCENT’S EAST


50 Medical Park East DriveBirmingham, Alabama 35235
205.838.3660stvhs.com
CANCER PROGRAM