a better way oregon 2016providers.kaiserpermanente.org › info_assets › cpp_knw › ...product...
TRANSCRIPT

For Oregon groups with 101 or more employeesProduct portfolio
A BETTER WAYto take care of business
50LBG-15/9-15
All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest. 500 NE Multnomah St., Suite 100, Portland, OR 97232.
O R E G O N
2016

2
TRADITIONAL PLANS Our sensible approach to health care has benefited individuals and families in the Northwest for more than 65 years. Employees will pay simple copayments for most services when they come in for care. Most preventive services are provided at no additional charge. There are no claim forms or deductibles to worry about.
DEDUCTIBLE PLANS To help balance the needs of businesses and their employees, we offer multiple plans with various copayments, coinsurance levels, deductibles, and out-of-pocket maximums. Employees will pay simple copayments for most outpatient visits, and preventive services are provided at no additional charge. Employers can choose the plans that best meet their needs, whether the overall goal is to keep employee costs down or reduce premiums. These plans may also be paired with a Kaiser Permanente health reimbursement arrangement (HRA) or flexible spending account (FSA).
ADDED CHOICE® PLANS Would you like to give your employees the opportunity to keep their current doctor or the option of seeing any licensed provider for covered services — at any time? Do you have employees who travel for extended periods and need access to routine care? Only Kaiser Permanente offers the option to see any licensed provider across the nation for covered services — along with exclusive access to our Select Providers and Select Facilities.• Go to a Select Provider or Select Facility and receive
quality integrated care at an affordable price.• Go to a Select Provider or Select Facility and receive
preventive care at no additional charge.*• Go to a PPO provider or facility anywhere in the nation
and receive covered services with higher copayments and coinsurance. Kaiser Permanente has partnered with First Choice Health to provide an extensive PPO network for our members.
• Go to any other non-participating provider or facility nationwide for covered services. Since these providers are not contracted with us, they may require payment in advance of or at the time services are rendered. They may also be unwilling to bill us on the member’s behalf. We’ll reimburse charges for covered services paid by members at the allowed amount† (less applicable coinsurance) once they’ve satisfied their deductible.
Added Choice may also be paired with a Kaiser Permanente HRA or FSA. With Added Choice, employees choose their own best balance among cost, choice, and coverage!
KAISER PERMANENTE'S INTEGRATED CONSUMER-DIRECTED CARE OFFERINGS Consumer engagement meets Kaiser Permanente's high-quality care
HSA-QUALIFIED HIGH DEDUCTIBLE PLANS We combine the cost savings of a high deductible health plan with a collaborative approach to care that helps keep employees healthier and more productive — at work and at home. Helping prevent issues before they start, most preventive services are provided at no additional charge and are not subject to the deductible. HSA-qualified plans may be paired with a Kaiser Permanente HSA, HRA, or FSA.
KAISER PERMANENTE HEALTH PAYMENT SERVICESWith consumer-directed health care — HRAs, HSAs, and FSAs — you can have workers who are more fully engaged in maintaining their health. Our integrated offering blends one of the nation’s most experienced consumer-directed health care administrators with the high-quality integrated care that sets Kaiser Permanente apart.
You pick the plan design from a wide range of deductibles, copays, and coinsurance. Your employees will be encouraged to participate in managing their personal and financial health. With Kaiser Permanente’s integrated solution, your employees can access their plan information — and their health information — right from their desktop or mobile device.
You get:• Comprehensive administrative support.• Multiple account-funding options.• Easy transition to a Kaiser Permanente consumer-
directed plan.• Online enrollment and eligibility management.• A customizable employee portal.• Reports and notifications delivered to you automatically.
Your employees get:• A single Kaiser Permanente health payment card that
works for HRAs, individual HSAs, and FSAs as well as stacked FSA/HRA accounts.
• Ability to access all accounts, manage their personal health information, and file financial account claims just by signing on to kp.org.
• Real-time transaction information.• Live phone support.
PLAN OVERVIEWS
* Members who live and work outside our service area may be eligible to receive preventive care at no additional cost through the PPO network.† Allowed amount: See your Evidence of Coverage (EOC) for complete details.

3
Kaiser Permanente Health Payment Services Financial Account Pairing Options
Take advantage of Kaiser Permanente’s integrated consumer-directed health care offerings by choosing the health plan and financial arrangement that works for you.
All Kaiser Permanente deductible plans may be paired with HRAs, FSAs, and stacked FSA/HRA accounts.
Kaiser Permanente’s HSA-qualified high deductible health plans may be paired with any of the above, in addition to HSAs.
MEDICAL PLANFINANCIAL ACCOUNT1
HRA HSA FSA Stacked FSA/HRA Limited Purpose HRA3
DEDUCTIBLE PLAN NA2
HSA-QUALIFIED HIGH DEDUCTIBLE HEALTH PLAN (HDHP)
ADDED CHOICE PLAN NA2
HSA-QUALIFIED ADDED CHOICE® PLAN
TRADITIONAL PLAN NA NA2 NA NA1All financial account options above are subject to IRS 213d rules for reimbursement and are supported by a Kaiser Permanente Health Payment
Card.2HSA may only be paired with an HSA-qualified plan per U.S. Treasury guidelines. Additional financial accounts may affect HSA tax-exempt status.3Limited purpose HRA is available for dental, vision hardware, or pharmacy services.
Additional financial account options are available. Please contact your broker or sales associate for more information on Kaiser Permanente’s plan designs for groups with 101 or more employees.

4
PLAN OPTIONS Plan B Plan C Plan D Plan E Plan F Plan G Plan H Plan J Plan K
BENEFIT/FEATURE*
Member pays
Member pays
Member pays
Member pays
Member pays
Member pays
Member pays
Member pays
Member pays
DEDUCTIBLE (PER CALENDAR YEAR)
$0 $0 $0 $0 $0 $0 $0 $0 $0
OFFICE VISITS —PRIMARY
$10 copayment
$10 copayment
$15 copayment
$15 copayment
$20 copayment
$20 copayment
$25 copayment
$30 copayment
$35 copayment
SPECIALTY CARE
$20 copayment
$20 copayment
$25 copayment
$25 copayment
$30 copayment
$30 copayment
$35 copayment
$40 copayment
$45 copayment
OFFICE VISITS — URGENT CARE
$30 copayment
$30 copayment
$35 copayment
$35 copayment
$40 copayment
$40 copayment
$45 copayment
$50 copayment
$60 copayment
PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES
$0 $0 $0 $0 $0 $0 $0 $0 $0
INPATIENT HOSPITAL CARE
$50 copayment per day, up to $250 per admission
$100 copayment per day, up to $500 per admission
$50 copayment per day, up to $250 per admission
$200 copayment per day, up to $1,000 per admission
$100 copayment per day, up to $500 per admission
$200 copayment per day, up to $1,000 per admission
$500 per admission
$750 per admission
$800 per admission
EMERGENCY CARE
$200 copayment
$200 copayment
$200 copayment
$200 copayment
$200 copayment
$200 copayment
$200 copayment
$200 copayment
$200 copayment
OUTPATIENT SURGERY
$20 copayment
$50 copayment
$20 copayment
$50 copayment
$50 copayment
$50 copayment
$75 copayment
$100 copayment
$150 copayment
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES
$10 copayment per visit
$10 copayment per visit
$15 copayment per visit
$15 copayment per visit
$20 copayment per visit
$20 copayment per visit
$25 copayment per visit
$30 copayment per visit
$35 copayment per visit
CT, MRI, AND PET SCANS
$50 copayment
$50 copayment
$50 copayment
$50 copayment
$50 copayment
$50 copayment
$50 copayment
$50 copayment
$50 copayment
OUT-OF-POCKET MAXIMUM
$600 individual, $1,200 family
$600 individual, $1,200 family
$600 individual, $1,200 family
$1,500 individual, $3,000 family
$1,000 individual, $2,000 family
$1,500 individual, $3,000 family
$1,500 individual, $3,000 family
$2,000 individual, $4,000 family
$3,000 individual, $6,000 family
These plans are subject to exclusions and limitations. A complete list of the exclusions and limitations is included In the Evidence of Coverage (EOC). To obtain a copy of the EOC, call the Client Services Unit at 1-866-246-3613 (toll free).* These plans include limited coverage for dependent children outside the Kaiser Foundation Health Plan of the Northwest service area. For
covered services, the member pays 20 percent of the actual fee. Services are limited to 10 office visits, 10 diagnostic labs or X-rays, and 10 prescription drug fills.
For specific plan information, see the following form: EOLGTRAD0116
PLAN HIGHLIGHTS FOR TRADITIONAL COPAYMENT PLANS

5
SUPPLEMENTAL BENEFITSBelow are just a few of many options available with a medical plan. Contact your sales executive or account manager for more information.
Outpatient prescription drugsThe Kaiser Permanente formulary applies to all plans. Members get up to a 30-day supply for each copayment (up to a 90-day supply of maintenance drugs for two copayments when our Mail-Delivery Pharmacy is used).1 All of these plans, except the $15/50%, are Medicare Part D creditable. View our formulary at kp.org/formulary.
Options Member pays$10/$20/$40/$150 $10 for generic, $20 for preferred brand-name drug, $40 for non-preferred brand-name drug, $150 for specialty drugs
$10/$20/$40 $10 for generic, $20 for preferred brand-name drug, $40 for non-preferred brand-name drug
$10/$30/50%– $100/50%–$150
$10 for generic, $30 for preferred brand-name drug, 50% up to $100 for non-preferred brand-name drug, 50% up to $150 for specialty drugs
$10/$30/50%–$100 $10 for generic, $30 for preferred brand-name drug, 50% up to $100 for non-preferred brand-name drug
$10/$30/$45 $10 for generic, $30 for preferred brand-name drug, $45 for non-preferred brand-name drug
$15/$30/50%–$200 $15 for generic, $30 for preferred brand-name drug, 50% up to $200 for non-preferred brand-name drug
$15/$30/$50/$150 $15 for generic, $30 for preferred brand-name drug, $50 for non-preferred brand-name drug, $150 for specialty drugs
$15/$30/$50 $15 for generic, $30 for preferred brand-name drug, $50 for non-preferred brand-name drug
$20/$40/$60/$150 $20 for generic, $40 for preferred brand-name drug, $60 for non-preferred brand-name drug, $150 for specialty drugs
$20/$40/$60 $20 for generic, $40 for preferred brand-name drug, $60 for non-preferred brand-name drug
Note: Prescription drug cost shares apply to the medical out-of-pocket maximum.1Specialty drugs are provided at one copay (or one maximum) for a 30-day supply.
Chiropractic care*Self-referred chiropractic care is available through The CHP Group–approved network providers in the Kaiser Foundation Health Plan of the Northwest service area. Visit chpgroup.com for a list of providers.
Alternative care (includes chiropractic care)*Self-referred alternative care without prior authorization is available for chiropractic, naturopathic, acupuncture, and mesage therapy from The CHP Group network providers in our service area. Annual benefit maximums of $500, $1,000, or $1,500. Visit chpgroup.com for a list of providers.
Options Member pays$10 $10 per chiropractic, acupuncture, or naturopathic visit; $25 per massage therapy visit for up to 12 visits per year
$15 $15 per chiropractic, acupuncture, or naturopathic visit; $25 massage therapy visit for up to 12 visits per year.
$20 $20 per chiropractic, acupuncture, or naturopathic visit; $25 per massage therapy visit for up to 12 visits per year
$25 $25 per chiropractic, acupuncture, or naturopathic visit; $25 massage therapy visit for up to 12 visits per year.
Vision hardware*Eye exams are covered as a medical benefit at the applicable office visit charge. Vision hardware must be prescribed and purchased at Vision Essentials by Kaiser Permanente. Visit kp2020.org.
Hardware options Member pays
12-month allowance For members 19 and older:Balance after allowance applied toward the purchase of frames and lenses or contacts every 12 months. Allowance options: $150, $200, $250, $300, $400, or $500 For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months. Eyeglasses or contacts outside of the select list are available for purchase with an allowance toward the purchase price, as a buy-up option. (Members cannot use both the standard/free benefit and the allowance benefit within the same calendar year.)
24-month allowance For members 19 and older:Balance after allowance applied toward the purchase of frames and lenses or contacts every 24 months. Allowance options: $100, $150, $200, $250, $300, $400, or $500For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months
Hearing aids* One hearing aid per ear per 48 months up to: $250, $500, $1,000, $1,500 allowance.
*Member payments for supplemental benefits do not apply to the medical out-of-pocket maximum.Note: These supplemental benefits are not available with Senior Advantage plans.
SUPPLEMENTAL BENEFIT OPTIONS FOR TRADITIONAL AND DEDUCTIBLE PLANS

6
PLAN $150–10% TR
PLAN 150–10%
PLAN 150-20%
PLAN 250–10% TR
PLAN 250–10%
PLAN $250–20% TR
PLAN $250–20%
PLAN $500–10% TR
PLAN 500–10%
PLAN $500–20%
DEDUCTIBLE (PER CALENDAR YEAR)
$150 per member,$450 per family
$150 per member,$450 per family
$150 per member,$450 per family
$250 per member,$750 per family
$250 per member,$750 per family
$250 per member,$750 per family
$250 per member,$750 per family
$500 per member,$1,500 per family
$500 per member,$1,500 per family
$500 per member,$1,500 per family
OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
$1,150 per member,$3,450 per family
$1,650 per member,$4,950 per family
$1,650 per member,$4,950 per family
$1,250 per member,$3,750 per family
$2,250 per member,$6,750 per family
$1,750 per member,$5,250 per family
$2,250 per member,$6,750 per family
$2,000 per member,$6,000 per family
$3,000 per member,$9,000 per family
$3,000 per member,$9,000 per family
BENEFITS* Member pays
OFFICE VISITS — PRIMARY CARE
$10† $10† $15† $15† $15† $15† $15† $20† $20† $20†
OFFICE VISITS — URGENT CARE
$30† $30† $35† $35† $35† $35† $35† $40† $40† $40†
OFFICE VISITS FOR PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES
$0† $0† $0† $0† $0† $0† $0† $0† $0† $0†
OFFICE VISITS — PRENATAL CARE
$0† $0† $0† $0† $0† $0† $0† $0† $0† $0†
OFFICE VISITS — SPECIALTY CARE
$20† $20† $25† $25† $25† $25† $25† $30† $30† $30†
ROUTINE EYE EXAMS
$10† $10† $15† $15† $15† $15† $15† $20† $20† $20†
OUTPATIENT SURGERY
10% of charges
10% of charges
20% of charges
10% of charges
10% of charges
20% of charges
20% of charges
10% of charges
10% of charges
20% of charges
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES
$10 per visit†
$10 per visit†
$15 per visit†
$15 per visit†
$15 per visit†
$15 per visit†
$15 per visit†
$20 per visit†
$20 per visit†
$20 per visit†
CT, MRI, AND PET SCANS
$100† $100† $100† $100† $100† $100† $100† $100† $100† $100†
EMERGENCY CARE 10% of charges
10% of charges
20% of charges
10% of charges
10% of charges
20% of charges
20% of charges
10% of charges
10% of charges
20% of charges
INPATIENT HOSPITAL CARE
10% of charges
10% of charges
20% of charges
10% of charges
10% of charges
20% of charges
20% of charges
10% of charges
10% of charges
20% of charges
*These plans include limited coverage for dependent children outside the Kaiser Foundation Health Plan of the Northwest service area. For covered services, the member pays 20 percent of the actual fee. Services are limited to 10 office visits, 10 diagnostic labs or X-rays, and 10 prescription drug fills.
†Deductible does not apply.
Visit our website — kp.org/deductibleplans — for more information on how our deductible plans work.
PLAN HIGHLIGHTS FOR DEDUCTIBLE PLANS
Most of our deductible plans can be paired with an Added Choice plan, and many are included in our multi-plan bundles on page 8. Deductible plans with "TR" in the name are tailored to provide additional pairing combinations within the product pairing guidelines for Added Choice.

7
For standard plans, the following services are not subject to deductible: most outpatient office visits; labs, X-rays, and special diagnostic procedures; urgent care; and supplemental options such as alternative care, adult hearing aids, prescription drugs, physical, speech, and occupational therapies and vision hardware (if purchased).The deductible and most copayments and coinsurance apply to the medical out-of-pocket maximum.
For specific plan information, see the following form: EOLGDED0116
PLAN 750–20% TR
PLAN 750–20%
PLAN 1000–20%
PLAN 1500–20%
PLAN 2000–20% TR
PLAN 2000–30%
PLAN 2500–20%
PLAN 3000–20% TR
PLAN 3000–20%
PLAN 3500–20%
PLAN 4000–20% TR
PLAN 5000–20%
$750 per member,$2,250 per family
$750 per member,$2,250 per family
$1,000 per member,$3,000 per family
$1,500 per member,$4,500 per family
$2,000 per member,$6,000 per family
$2,000 per member,$6,000 per family
$2,500 per member,$7,500 per family
$3,000 per member,$9,000 per family
$3,000 per member,$9,000 per family
$3,500 per member,$10,500 per family
$4,000 per member,$12,000 per family
$5,000 per member,$12,700 per family
$2,250 per member,$6,750 per family
$3,250 per member,$9,750 per family
$4,000 per member,$12,000 per family
$5,000 per member,$10,000 per family
$5,000 per member,$10,000 per family
$6,850 per member,$13,700 per family
$5,000 per member,$10,000 per family
$5,000 per member,$10,000 per family
$6,850 per member,$13,700 per family
$6,850 per member,$13,700 per family
$5,000 per member,$10,000 per family
$6,850 per member,$13,700 per family
Member pays
$20† $20† $25† $25† $25† $30† $25† $30† $30† $30† $30† $30†
$40† $40† $45† $45† $45† $50† $45† $50† $50† $50† $50† $50†
$0† $0† $0† $0† $0† $0† $0† $0† $0† $0† $0† $0†
$0† $0† $0† $0† $0† $0† $0† $0† $0† $0† $0† $0†
$30† $30† $35† $35† $35† $40† $35† $40† $40† $40† $40† $40†
$20† $20† $25† $25† $25† $30† $25† $30† $30† $30† $30† $30†
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
30% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
$20 per visit†
$20 per visit†
$25 per visit†
$25 per visit†
$25 per visit†
$30 per visit†
$25 per visit†
$30 per visit†
$30 per visit†
$30 per visit†
$30 per visit†
$30 per visit†
$100† $100† $100† $100† $100† $100† $100† $100† $100† $100† $100† $100†
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
30% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
30% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
20% of charges
*These plans include limited coverage for dependent children outside the Kaiser Foundation Health Plan of the Northwest service area For covered services, the member pays 20 percent of the actual fee. Services are limited to 10 office visits, 10 diagnostic labs or x-rays, and 10 prescription drug fills.
†Deductible does not apply.

8
PLAN 250 DD
DEDUCTIBLE PLAN 250 - 20% TR ADDED CHOICE DD
DEDUCTIBLE (PER CALENDAR YEAR)
$250 per member,$750 per family
INDIVIDUAL/FAMILY
Tier 11 $250 / $750
Tier 22 $500 / $1,500
Tier 33 $750 / $2,250
OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
$1,750 per member,$5,250 per family
Tier 11 $1,750 / $5,250
Tier 22 $3,000 / $9,000
Tier 33 $4,000 / $12,000
LIFETIME BENEFIT MAXIMUM Unlimited NA
OFFICE VISITS — PRIMARY CARE $15*
Tier 11 $20
Tier 22 $30
Tier 33 45%†
OFFICE VISITS — URGENT CARE $35*
Tier 11 $40
Tier 22 $50
Tier 33 45%†
OFFICE VISITS FOR PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES
$0* NA
OFFICE VISITS — PRENATAL CARE $0* NA
OFFICE VISITS — SPECIALTY CARE $25*
Tier 11 $30
Tier 22 $40
Tier 33 45%†
ROUTINE EYE EXAMS $15* NA
OUTPATIENT SURGERY 20% of charges NA
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES $15 per visit*
Tier 11 $20 / $100
Tier 22 $30 / 30%†
Tier 33 45%†
CT, MRI, AND PET SCANS $100* NA
EMERGENCY CARE 20% of charges All $200
INPATIENT HOSPITAL CARE 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 45%†
PLAN 500 DE
DEDUCTIBLE PLAN 500 - 20% ADDED CHOICE DE
$500 per member,$1,500 per family
INDIVIDUAL/FAMILY
Tier 11 $500 / $1,500
Tier 22 $1,000 / $3,000
Tier 33 $1,500 / $4,500
$3,000 per member,$9,000 per family
Tier 11 $3,000 / $6,000
Tier 22 $4,750 / $9,500
Tier 33 $6,000 / $12,000
Unlimited NA
$20*
Tier 11 $20
Tier 22 $30
Tier 33 45%†
$40*
Tier 11 $40
Tier 22 $50
Tier 33 45%†
$0* NA
$0* NA
$30*
Tier 11 $30
Tier 22 $40
Tier 33 45%†
$20* NA
20% of charges NA
$20 per visit*
Tier 11 $20 / $100
Tier 22 $30 / 30%†
Tier 33 45%†
$100* NA
20% of charges All $200
20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 45%†
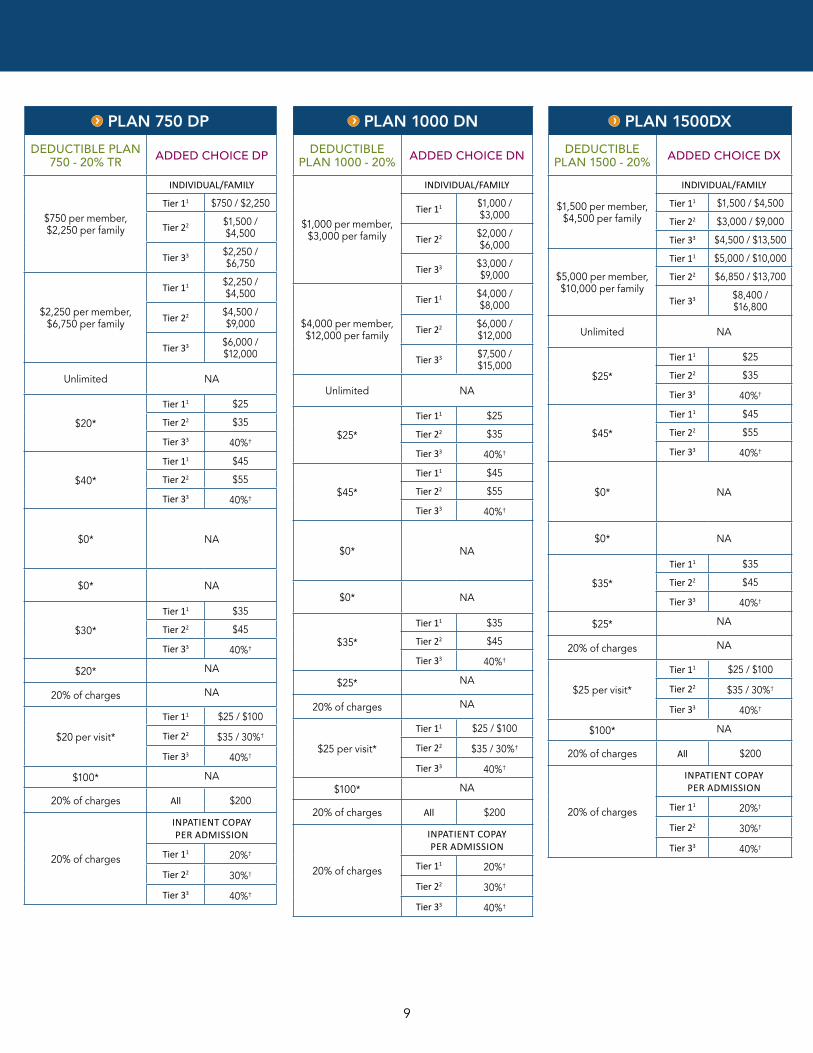
BUNDLED DEDUCTIBLE AND ADDED CHOICE PLANS
*Deductible does not apply. †Deductible applies. See footnotes in the deductible plans and Added Choice plans sections of this booklet for restrictions and more information.
9
PLAN 750 DP
DEDUCTIBLE PLAN 750 - 20% TR ADDED CHOICE DP
$750 per member,$2,250 per family
INDIVIDUAL/FAMILY
Tier 11 $750 / $2,250
Tier 22 $1,500 / $4,500
Tier 33 $2,250 / $6,750
$2,250 per member,$6,750 per family
Tier 11 $2,250 / $4,500
Tier 22 $4,500 / $9,000
Tier 33 $6,000 / $12,000
Unlimited NA
$20*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
$40*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
$0* NA
$0* NA
$30*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
$20* NA
20% of charges NA
$20 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
$100* NA
20% of charges All $200
20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†
PLAN 1000 DN
DEDUCTIBLE PLAN 1000 - 20% ADDED CHOICE DN
$1,000 per member,$3,000 per family
INDIVIDUAL/FAMILY
Tier 11 $1,000 / $3,000
Tier 22 $2,000 / $6,000
Tier 33 $3,000 / $9,000
$4,000 per member,$12,000 per family
Tier 11 $4,000 / $8,000
Tier 22 $6,000 / $12,000
Tier 33 $7,500 / $15,000
Unlimited NA
$25*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
$45*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
$0* NA
$0* NA
$35*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
$25* NA
20% of charges NA
$25 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
$100* NA
20% of charges All $200
20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†
PLAN 1500DX
DEDUCTIBLE PLAN 1500 - 20% ADDED CHOICE DX
$1,500 per member,$4,500 per family
INDIVIDUAL/FAMILY
Tier 11 $1,500 / $4,500
Tier 22 $3,000 / $9,000
Tier 33 $4,500 / $13,500
$5,000 per member,$10,000 per family
Tier 11 $5,000 / $10,000
Tier 22 $6,850 / $13,700
Tier 33 $8,400 / $16,800
Unlimited NA
$25*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
$45*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
$0* NA
$0* NA
$35*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
$25* NA
20% of charges NA
$25 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
$100* NA
20% of charges All $200
20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†

10
PLAN 250/500 DD
DEDUCTIBLE PLAN 250 - 20% TR
DEDUCTIBLE PLAN 500 - 20% ADDED CHOICE DD
DEDUCTIBLE (PER CALENDAR YEAR)
$250 per member,$750 per family
$500 per member,$1,500 per family
INDIVIDUAL/FAMILY
Tier 11 $250 / $750
Tier 22 $500 / $1,500
Tier 33 $750 / $2,250
OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
$1,750 per member,$5,250 per family
$3,000 per member,$9,000 per family
Tier 11 $1,750 / $5,250
Tier 22 $3,000 / $9,000
Tier 33 $4,000 / $12,000
LIFETIME BENEFIT MAXIMUM Unlimited Unlimited NA
OFFICE VISITS — PRIMARY CARE $15* $20*
Tier 11 $20
Tier 22 $30
Tier 33 45%†
OFFICE VISITS — URGENT CARE $35* $40*
Tier 11 $40
Tier 22 $50
Tier 33 45%†
OFFICE VISITS FOR PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES $0* $0* NA
OFFICE VISITS — PRENATAL CARE $0* $0* NA
OFFICE VISITS — SPECIALTY CARE $25* $30*
Tier 11 $30
Tier 22 $40
Tier 33 45%†
ROUTINE EYE EXAMS $15* $20* NA
OUTPATIENT SURGERY 20% of charges 20% of charges NA
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES $15 per visit* $20 per visit*
Tier 11 $20 / $100
Tier 22 $30 / 30%†
Tier 33 45%†
CT, MRI, AND PET SCANS $100* $100* NA
EMERGENCY CARE 20% of charges 20% of charges All $200
INPATIENT HOSPITAL CARE 20% of charges 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 45%†
BUNDLED DEDUCTIBLE AND ADDED CHOICE PLANS
*Deductible does not apply. †Deductible applies. See footnotes in the deductible plans and Added Choice plans sections of this booklet for restrictions and more information.

11
PLAN 500/1000 DE
DEDUCTIBLE PLAN 500 - 20%
DEDUCTIBLE PLAN 1000 - 20% ADDED CHOICE DE
$500 per member,$1,500 per family
$1,000 per member,$3,000 per family
INDIVIDUAL/FAMILY
Tier 11 $500 / $1,500
Tier 22 $1,000 / $3,000
Tier 33 $1,500 / $4,500
$3,000 per member,$9,000 per family
$4,000 per member,$12,000 per family
Tier 11 $3,000 / $6,000
Tier 22 $4,750 / $9,500
Tier 33 $6,000 / $12,000
Unlimited Unlimited NA
$20* $25*
Tier 11 $20
Tier 22 $30
Tier 33 45%†
$40* $45*
Tier 11 $40
Tier 22 $50
Tier 33 45%†
$0* $0* NA
$0* $0* NA
$30* $35*
Tier 11 $30
Tier 22 $40
Tier 33 45%†
$20* $25* NA
20% of charges 20% of charges NA
$20 per visit* $25 per visit*
Tier 11 $20 / $100
Tier 22 $30 / 30%†
Tier 33 45%†
$100* $100* NA
20% of charges 20% of charges All $200
20% of charges 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 45%†
PLAN 750/1500 DP
DEDUCTIBLE PLAN 750 - 20% TR
DEDUCTIBLE PLAN 1500 - 20% ADDED CHOICE DP
$750 per member,$2,250 per family
$1,500 per member,$4,500 per family
INDIVIDUAL/FAMILY
Tier 11 $750 / $2,250
Tier 22 $1,500 / $4,500
Tier 33 $2,250 / $6,750
$2,250 per member,$6,750 per family
$5,000 per member,$10,000 per family
Tier 11 $2,250 / $4,500
Tier 22 $4,500 / $9,000
Tier 33 $6,000 / $12,000
Unlimited Unlimited NA
$20* $25*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
$40* $45*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
$0* $0* NA
$0* $0* NA
$30* $35*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
$20* $25* NA
20% of charges 20% of charges NA
$20 per visit* $25 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
$100* $100* NA
20% of charges 20% of charges All $200
20% of charges 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†

12
PLAN 1000/2000 DN
DEDUCTIBLE PLAN 1000 - 20%
DEDUCTIBLE PLAN 2000 - 20% TR ADDED CHOICE DN
DEDUCTIBLE (PER CALENDAR YEAR)
$1,000 per member,$3,000 per family
$2,000 per member,$6,000 per family
INDIVIDUAL/FAMILY
Tier 11 $1,000 / $3,000
Tier 22 $2,000 / $6,000
Tier 33 $3,000 / $9,000
OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE)
$4,000 per member,$12,000 per family
$5,000 per member,$10,000 per family
Tier 11 $4,000 / $8,000
Tier 22 $6,000 / $12,000
Tier 33 $7,500 / $15,000
LIFETIME BENEFIT MAXIMUM Unlimited Unlimited NA
OFFICE VISITS — PRIMARY CARE $25* $25*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
OFFICE VISITS — URGENT CARE $45* $45*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
OFFICE VISITS FOR PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES $0* $0* NA
OFFICE VISITS — PRENATAL CARE $0* $0* NA
OFFICE VISITS — SPECIALTY CARE $35* $35*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
ROUTINE EYE EXAMS $25* $25* NA
OUTPATIENT SURGERY 20% of charges 20% of charges NA
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES $25 per visit* $25 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
CT, MRI, AND PET SCANS $100* $100* NA
EMERGENCY CARE 20% of charges 20% of charges All $200
INPATIENT HOSPITAL CARE 20% of charges 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†
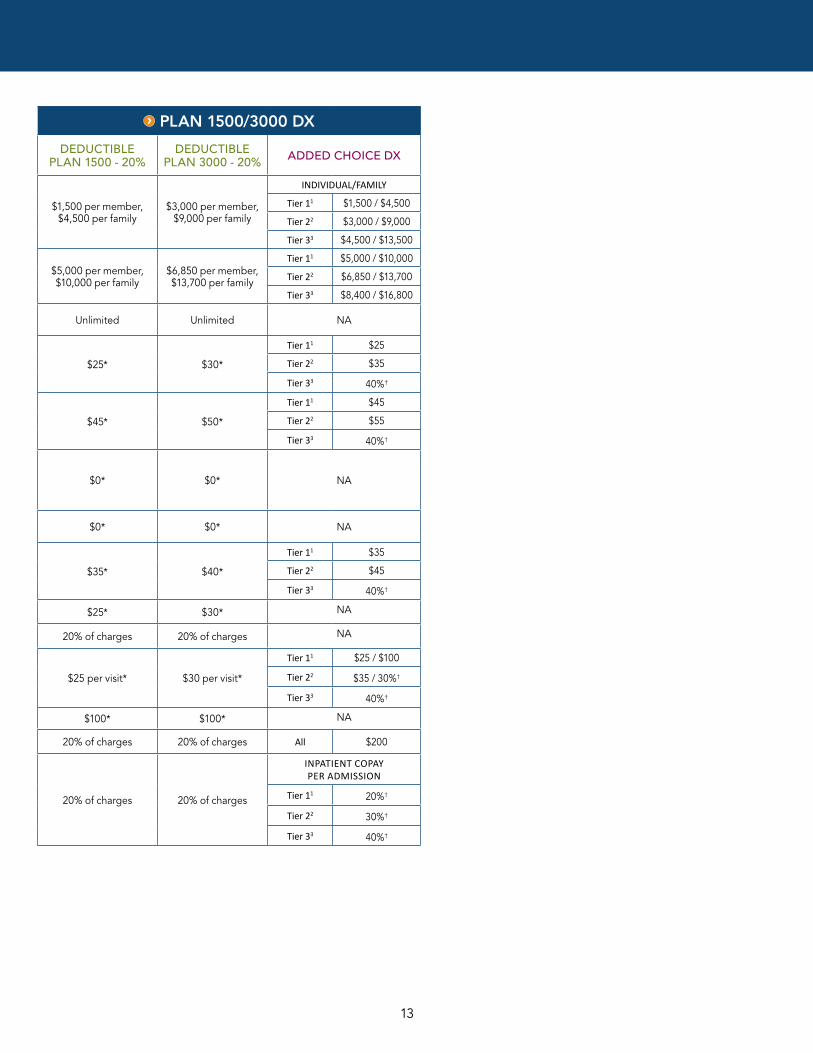
BUNDLED DEDUCTIBLE AND ADDED CHOICE PLANS
*Deductible does not apply. †Deductible applies. See footnotes in the deductible plans and Added Choice plans sections of this booklet for restrictions and more information.
13
PLAN 1500/3000 DX
DEDUCTIBLE PLAN 1500 - 20%
DEDUCTIBLE PLAN 3000 - 20% ADDED CHOICE DX
$1,500 per member,$4,500 per family
$3,000 per member,$9,000 per family
INDIVIDUAL/FAMILY
Tier 11 $1,500 / $4,500
Tier 22 $3,000 / $9,000
Tier 33 $4,500 / $13,500
$5,000 per member,$10,000 per family
$6,850 per member,$13,700 per family
Tier 11 $5,000 / $10,000
Tier 22 $6,850 / $13,700
Tier 33 $8,400 / $16,800
Unlimited Unlimited NA
$25* $30*
Tier 11 $25
Tier 22 $35
Tier 33 40%†
$45* $50*
Tier 11 $45
Tier 22 $55
Tier 33 40%†
$0* $0* NA
$0* $0* NA
$35* $40*
Tier 11 $35
Tier 22 $45
Tier 33 40%†
$25* $30* NA
20% of charges 20% of charges NA
$25 per visit* $30 per visit*
Tier 11 $25 / $100
Tier 22 $35 / 30%†
Tier 33 40%†
$100* $100* NA
20% of charges 20% of charges All $200
20% of charges 20% of charges
INPATIENT COPAY PER ADMISSION
Tier 11 20%†
Tier 22 30%†
Tier 33 40%†

14
PLAN COMPARISON
We recognize that each client has specific needs with regard to their product pairings. Please contact your account manager or sales executive for guidance on which of our traditional and deductible plans best suit your needs when offered alongside an Added Choice plan.1 In most cases, Tier 1 services are provided by Select Providers and Select Facilities. The Evidence of Coverage (EOC) provides a complete definition of Select Provider, Select Facility, and Select Pharmacy. The EOC also explains when Tier 1 services are provided by other providers and facilities.2 Tier 2 services are provided by PPO Providers and PPO Facilities. Refer to the Evidence of Coverage (EOC) for a complete definition of PPO Provider and PPO Facilities. We provide coverage for certain Tier 2 preventive services with no cost share for out-of-area subscribers and their dependents. See the Preventive Care Services section of your 2016 Evidence of Coverage (EOC) for details.3 Tier 3 services are provided by Non-Participating Providers and Non-Participating Facilities. Refer to the Evidence of Coverage (EOC) for a complete definition of Non-Participating Provider and Non-Participating Facility.*Deductible applies.
PLAN HIGHLIGHTS FOR ADDED CHOICE® POINT-OF-SERVICE PLANS
PLAN OPTIONS 83 86 70 71 72 74 75 89E 91 DA DB
DEDUCTIBLE: INDIVIDUAL/FAMILY
Tier 11 N/A N/A N/A N/A N/A N/A N/A N/A N/A $150 / $450
$250 / $750
Tier 22 $200 / $600
$250 / $750
$250 / $750
$300 / $900
$300 / $900
$500 / $1,500
$500 / $1,500
$1,000 / $3,000
$1,500 / $4,500
$300 / $900
$500 / $1,500
Tier 33 $400 / $1,200
$500 / $1,500
$500 / $1,500
$600 / $1,800
$600 / $1,800
$1,000 / $3,000
$1,000 / $3,000
$2,000 / $6,000
$3,000 / $9,000
$450 / $1,350
$750 / $2,250
OUT-OF-POCKET MAXIMUM: INDIVIDUAL/FAMILY (INCLUDES DEDUCTIBLE)
Tier 11 $600 / $1,200
$750 / $1,500
$750 / $1,500
$1,000 / $2,000
$1,000 / $2,000
$1,500 / $3,000
$2,000 / $4,000
$1,000 / $2,000
$3,000 / $6,000
$1,150 / $3,450
$1,250 / $3,750
Tier 22 $1,200 / $3,600
$1,750 / $5,250
$1,750 / $5,250
$1,800 / $5,400
$3,300 / $9,900
$2,500 / $7,500
$3,500 / $10,500
$5,000 / $10,000
$5,500 / $11,000
$2,300 / $6,900
$2,500 / $7,500
Tier 33 $2,150 / $6,450
$3,125 / $9,375
$3,500 / $10,500
$5,100 / $15,300
$6,600 / $19,800
$4,000 / $12,000
$6,500 / $19,500
$8,000 / $16,000
$9,000 / $18,000
$3,450 / $9,900
$3,500 / $10,500
PRIMARY CARE VISIT
Tier 11 $10 $10 $15 $10 $15 $15 $20 $20 $35 $10 $20
Tier 22 $20 $20 $25 $20 $25 $25 $30 $30 $50 $20 $30
Tier 33 35%* 35%* 40%* 30%* 40%* 30%* 40%* 40%* 50%* 35%* 35%*
SPECIALTY CARE VISIT
Tier 11 $20 $20 $25 $20 $25 $25 $30 $30 $45 $20 $30
Tier 22 $30 $30 $35 $30 $35 $35 $40 $40 $60 $30 $40
Tier 33 35%* 35%* 40%* 30%* 40%* 30%* 40%* 40%* 50%* 35%* 35%*
LAB/X-RAY/SPECIAL DIAGNOSTIC PROCEDURES
Tier 11 $10 / $50 $10 / $50 $15 / $50 $10 / $50 $15 / $50 $15 / $50 $20 / $50
$20 / $50
$35 / $50
$10 / $100
$20 / $100
Tier 22 $20 / 20%*
$25 / 20%*
$25 / 20%*
$10 / 10%*
$20 / 20%*
$25 / 10%*
$25 / 20%*
$30 / 20%*
$50 / 30%*
$20 / 20%*
$30 / 20%*
Tier 33 35%* 35%* 40%* 30%* 40%* 30%* 40%* 40%* 50%* 35%* 35%*
URGENT CARE VISIT
Tier 11 $30 $30 $35 $30 $35 $35 $40 $40 $60 $30 $40
Tier 22 $40 $40 $45 $40 $45 $45 $50 $50 $75 $40 $50
Tier 33 35%* 35%* 40%* 30%* 40%* 30%* 40%* 40%* 50%* 35%* 35%*
EMERGENCY CARE All $200 $200 $200 $200 $200 $200 $200 $200 $200 $200 $200
INPATIENT COPAY PER ADMISSION
Tier 11
$50/day max
$250/admit
$100/day max
$500/admit
$200/admit
$200/admit
$100/day max
$500/admit
$200/day max
$1000/max
$200/day max
$1,000/admit
$200/day max
$1,000/admit
$800/admit 10%* 10%*
Tier 22 20%* 20%* 20%* 10%* 20%* 10%* 20%* 20%* 30%* 20%* 20%*
Tier 33 35%* 35%* 40%* 30%* 40%* 30%* 40%* 40%* 50%* 35%* 35%*

15
1 In most cases, Tier 1 services are provided by Select Providers and Select Facilities. The Evidence of Coverage (EOC) provides a complete definition of Select Provider, Select Facility, and Select Pharmacy. The EOC also explains when Tier 1 services are provided by other providers and facilities.2 Tier 2 services are provided by PPO Providers and PPO Facilities. Refer to the Evidence of Coverage (EOC) for a complete definition of PPO Provider and PPO Facilities. We provide coverage for certain Tier 2 preventive services with no cost share for out-of-area subscribers and their dependents. See the Preventive Care Services section of your 2016 Evidence of Coverage (EOC) for details.3 Tier 3 services are provided by Non-Participating Providers and Non-Participating Facilities. Refer to the Evidence of Coverage (EOC) for a complete definition of Non-Participating Provider and Non-Participating Facility.*Deductible applies.
This brochure provides summaries of various plans and is not a contract. These plans are subject to exclusions and limitations. Plan details, including all benefits, exclusions, and limitations, are provided in the Evidence of Coverage (EOC).
PLAN OPTIONS DD DC DE DF DP DN DX DR DS DK
DEDUCTIBLE: INDIVIDUAL/FAMILY
Tier 11 $250 / $750
$500 / $1,500
$500 / $1,500
$500 / $1,500
$750 / $2,250
$1,000 / $3,000
$1,500 / $4,500
$2,000 / $6,000
$3,000 / $9,000
$4,000 / $10,000
Tier 22 $500 / $1,500
$1,000 / $3,000
$1,000 / $3,000
$1,000 / $3,000
$1,500 / $4,500
$2,000 / $6,000
$3,000 / $9,000
$4,000 / $12,000
$6,000 / $12,700
$6,350 / $12,700
Tier 33 $750 / $2,250
$1,500 / $4,500
$1,500 / $4,500
$1,500 / $4,500
$2,250 / $6,750
$3,000 / $9,000
$4,500 / $13,500
$6,000 / $16,800
$8,400 / $16,800
$8,400 / $16,800
OUT-OF-POCKET MAXIMUM: INDIVIDUAL/FAMILY (INCLUDES DEDUCTIBLE)
Tier 11 $1,750 / $5,250
$2,000 / $6,000
$3,000 / $6,000
$3,000 / $6,000
$2,250 / $4,500
$4,000 / $8,000
$5,000 / $10,000
$5,000 / $10,000
$5,000 / $10,000
$5,000 / $10,000
Tier 22 $3,000 / $9,000
$4,000 / $12,000
$4,750 / $9,500
$5,500 / $11,000
$4,500 / $9,000
$6,000 / $12,000
$6,850 / $13,700
$6,850 / $13,700
$6,850 / $13,700
$6,850 / $13,700
Tier 33 $4,000 / $12,000
$5,500 / $16,500
$6,000 / $12,000
$7,500 / $15,000
$6,000 / $12,000
$7,500 / $15,000
$8,400 / $16,800
$8,400 / $16,800
$8,400 / $16,800
$8,400 / $16,800
PRIMARY CARE VISIT
Tier 11 $20 $20 $20 $30 $25 $25 $25 $25 $30 $30
Tier 22 $30 $30 $30 $40 $35 $35 $35 $35 $40 $40
Tier 33 45%* 35%* 45%* 50%* 40%* 40%* 40%* 40%* 40%* 45%*
SPECIALTY CARE VISIT
Tier 11 $30 $30 $30 $40 $35 $35 $35 $35 $40 $40
Tier 22 $40 $40 $40 $50 $45 $45 $45 $45 $50 $50
Tier 33 45%* 35%* 45%* 50%* 40%* 40%* 40%* 40%* 40%* 45%*
LAB/X-RAY/SPECIAL DIAGNOSTIC PROCEDURES
Tier 11 $20 / $100
$20 / $100
$20 / $100
$25 / $100
$25 / $100
$25 / $100
$25 / $100
$25 / $100
$30 / $100
$30 / $100
Tier 22 $30 / 30%*
$30 / 20%*
$30 / 30%*
$35 / 35%*
$35 / 30%*
$35 / 30%*
$35 / 30%*
$35 / 30%*
$40 / 30%*
$40 / 35%*
Tier 33 45%* 35%* 45%* 50%* 40%* 40%* 40%* 40%* 40%* 45%*
URGENT CARE VISIT
Tier 11 $40 $40 $40 $50 $45 $45 $45 $45 $50 $50
Tier 22 $50 $50 $50 $60 $55 $55 $55 $55 $60 $60
Tier 33 45%* 35%* 45%* 50%* 40%* 40%* 40%* 40%* 40%* 45%*
EMERGENCY CARE All $200 $200 $200 $200 $200 $200 $200 20% 20% 20%*
INPATIENT COPAY PER ADMISSION Tier 11 20%* 10%* 20%* 25%* 20%* 20%* 20%* 20%* 20%* 20%*
Tier 22 30%* 20%* 30%* 35%* 30%* 30%* 30%* 30%* 30%* 35%*
Tier 33 45%* 35%* 45%* 50%* 40%* 40%* 40%* 40%* 40%* 45%*
For specific plan information about the plans referred to in this brochure, see the following forms:
EOLGPOSDED3T0116 EOLGPOSDED2T0116
All of the following are non-grandfathered plans:
EOLGPOSDED3T0116 EOLGPOSDED2T0116

16
OUTPATIENT PRESCRIPTION DRUGS
Select Pharmacies MedImpact pharmacies
GENERIC COPAYMENT BRAND COPAYMENT GENERIC COPAYMENTPREFERRED BRAND
COPAYMENT*NON-PREFERRED
BRAND COPAYMENT*
$10 $20 $15 $30 $50
$15 $30 $20 $40 $60
$20 $40 $25 $50 $70
SUPPLEMENTAL BENEFIT OPTIONS FOR ADDED CHOICE PLANS
Select Pharmacies MedImpact Pharmacies
GENERIC COPAYMENT
PREFERRED BRAND-
NAME DRUG COPAYMENT
NON-PREFERRED
BRAND-NAME DRUG
GENERIC COPAYMENT
PREFERRED BRAND
COPAYMENT*
NON-PREFERRED
BRAND COPAYMENT*
SPECIALTY COPAYMENT
$10 $20 $40 $15 $30 $50
$10 $20 $40 $20 $30 $50
$10 $20 $40 $20 $40 $60 $300
$15 $30 $50 $20 $40 $60
$15 $30 $50 $25 $50 $70 $300
$20 $40 $60 $30 $60 $80
$20 $40 $60 $20 $50 or 50%, whichever is greater $300
* If a brand drug with an equivalent generic is prescribed and the member or the prescriber requests the brand drug, the charges will be the copayment plus the difference in retail price between generic and brand drug.
ALTERNATIVE CARE†
Self-referred chiropractic care Self-referred chiropractic, massage,‡ acupuncture, and naturopathic care
OFFICE VISIT COPAYMENT
NUMBER OF VISITS PER CALENDAR YEAR UP TO OFFICE VISIT COPAYMENT
CALENDAR YEAR BENEFIT MAXIMUM UP TO
$10 15, 20, 30 $10 $500, $1,000, $1,500
$15 $15
$20 $20
$25 $25
$30 ‡Massage office copayment is always $25 with a 12-visit limit per calendar year.
†To be covered by your benefit, you must receive care from a provider in our service area who is part of The CHP Group network. If you are on an Added Choice® plan with an alternative care benefit, you may use your benefits at The CHP Group (located in our service area), First Choice, or any licensed non-participating providers and facilities. The amount an Added Choice member pays is based on the provider. For a list of participating providers, visit chpgroup.com.
VISION HARDWARE COVERAGE MEMBER PAYS
12-month allowance For members 19 and older:Balance after allowance applied toward the purchase of frames and lenses or contacts every 12 months. $100, 150, $200, $250, $300, $400, or $500 For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months. Eyeglasses or contacts outside of the select list are available for purchase with an allowance toward the purchase price, as a buy-up option. (Members cannot use both the standard/free benefit and the allowance benefit within the same calendar year.)
24-month allowance For members 19 and older:Balance after allowance applied toward the purchase of frames and lenses or contacts every 24 months. $100, $150, $200, $250, $300, $400, or $500For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months.
HEARING AIDS
One hearing aid per ear per 48 months up to: $250, $500, $1,000, $1,500 allowance
SUPPLEMENTAL BENEFIT OPTIONS FOR ADDED CHOICE® PLANS

17
PLAN HIGHLIGHTS FOR HSA-QUALIFIED HIGH DEDUCTIBLE HEALTH PLANS
CHOOSE FROM THE FOLLOWING DEDUCTIBLE AND OUT-OF-POCKET MAXIMUM COMBINATIONS
THEN CHOOSE A COINSURANCE
Deductible (Individual/Family)
Out-of-Pocket Maximum (Individual/Family)
Accumulation Type* Available Coinsurance per combination
$1,300/$2,600 $2,600/$5,200 Aggregate 10%, 20%
$1,500/$3,000 $2,500/$5,000 Aggregate 10%, 20%, 30%
$2,000/$4,000 $4,000/$6,550 Aggregate 10%, 20%, 30%, 50%
$2,500/$5,000 $5,000/$6,550 Aggregate 10%, 20%, 30%, 50%
$2,600/$5,200 $5,200/$10,400 Embedded 20%, 30%, 40%, 50%
$3,000/$6,000 $6,000/$12,000 Embedded 20%, 30%, 40%, 50%
$3,500/$7,000 $6,550/$13,100 Embedded 20%, 30%, 40%, 50%
$4,000/$8,000 $6,550/$13,100 Embedded 20%, 30%, 40%, 50%
$5,000/$10,000 $6,550/$13,100 Embedded 20%, 30%, 40%, 50%
$6,550/$13,100 $6,550/$13,100 Embedded 0%
Kaiser Permanente combines the cost savings of a high deductible health plan with a collaborative approach to care that helps keep employees healthier and more productive — at work and at home. Our primary care providers, specialists, pharmacists, and other caregivers all work together with one mission: keeping employees healthy.
Choose from plans with a variety of deductible, coinsurance, and out-of-pocket maximum options.
*Aggregate Accumulation: For Services that are subject to the Deductible and Out-of-Pocket Maximum, you must pay Charges for the Services when you receive them, until you meet your Deductible or Out-of-Pocket Maximum. If you are the only Member in your Family, then you must meet the Member Deductible/Out-of-Pocket Maximum. If you are a Member in a Family of two or more Members, you meet the Deductible/Out-of-Pocket Maximum when your entire Family meets the Family Deductible amount. Every Member in your Family must pay charges during the Year until the entire Family meets the Family Deductible or Out-of-Pocket Maximum.
Embedded Accumulation: For Services that are subject to the Deductible and Out-of-Pocket Maximum, you must pay Charges for the Services when you receive them, until you meet your Deductible or Out-of-Pocket Maximum. If you are the only Member in your Family, then you must meet the Member Deductible/Out-of-Pocket Maximum. If there is at least one other Member in your Family, then you must each meet the Member Deductible/Out-of-Pocket Maximum, or your Family must meet the Family Deductible/Out-of-Pocket Maximum, whichever is less. Each Member Deductible amount counts toward the Family Deductible amount. Once the Family Deductible is satisfied, no further Member Deductible will be due for the remainder of the Year.
10% PLAN 20% PLAN 30% PLAN 40% PLAN 50% PLAN 0% PLAN
BENEFIT/FEATURE Member pays
OFFICE VISITS — PREVENTIVE AND WELL- CHILD CARE AND PREVENTIVE SERVICES*
$0 $0 $0 $0 $0 $0
OFFICE VISITS — PRENATAL CARE* $0 $0 $0 $0 $0 $0
OFFICE VISITS — PRIMARY AND URGENT CARE
10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
OFFICE VISITS — SPECIALTY CARE 10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
ROUTINE EYE EXAMS 10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
OUTPATIENT SURGERY 10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES
10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
EMERGENCY CARE 10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible
HOSPITAL INPATIENT CARE 10% after deductible
20% after deductible
30% after deductible
40% after deductible
50% after deductible
0% after deductible

18
PLAN HIGHLIGHTS FOR HSA-QUALIFIED HIGH DEDUCTIBLE HEALTH PLANS
50% VALUE PLAN 40% VALUE PLAN 30% VALUE PLAN
BENEFIT/FEATURE Member pays Member pays Member pays
DEDUCTIBLE (PER CALENDAR YEAR, EMBEDDED ACCUMULATION)
$3,500 per member / $7,000 per family
$4,500 per member / $9,000 per family
$5,500 per member / $11,000 per family
OUT-OF-POCKET MAXIMUM (INCLUDES DEDUCTIBLE, EMBEDDED ACCUMULATION)
$6,550 per member / $13,100 per family
$6,550 per member / $13,100 per family
$6,550 per member / $13,100 per family
OFFICE VISITS — PREVENTIVE AND WELL-CHILD CARE AND PREVENTIVE SERVICES*
$0 $0 $0
OFFICE VISITS — PRENATAL CARE* $0 $0 $0
OFFICE VISITS — PRIMARY AND URGENT CARE 50% after deductible 40% after deductible 30% after deductible
OFFICE VISITS — SPECIALTY CARE 50% after deductible 40% after deductible 30% after deductible
ROUTINE EYE EXAMS 50% after deductible 40% after deductible 30% after deductible
OUTPATIENT SURGERY 50% after deductible 40% after deductible 30% after deductible
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES 50% after deductible 40% after deductible 30% after deductible
EMERGENCY CARE 50% after deductible 40% after deductible 30% after deductible
HOSPITAL INPATIENT CARE 50% after deductible 40% after deductible 30% after deductible
In order to meet minimum value requirements, prescription drug coverage must match plan coinsurance and be subject to the deductible.
KAISER PERMANENTE VALUE PLANS
We have developed a new portfolio of plans designed to meet the needs of employers interested in offering coverage that falls within the requirements of a Minimum Value plan under the Affordable Care Act.
These plans cover medical essential health benefits and exclude those services above and beyond essential health benefits that are typically covered under Kaiser Permanente's standard large group plans.
Excluded non-essential health benefits: routine vision exams for adults (medically necessary eye care is still covered), infertility diagnosis, physician referred alternative care, and dependent child out of area coverage. (See EOC for complete list of exclusions and limitations.)

19

20
Below are the options available with our high deductible health plans. Contact your sales executive or account manager for more information.
Outpatient prescription drugsThe Kaiser Permanente formulary applies to all plans. Members get up to a 30-day supply for each copayment (up to a 90-day supply of maintenance drugs for two copayments when our Mail-Delivery Pharmacy is used).1 View our formulary at kp.org/formulary.
Options Member pays (after deductible is met)*
10% 10% coinsurance (after deductible)
20% 20% coinsurance (after deductible)
30% 30% coinsurance (after deductible)
40% 40% coinsurance (after deductible)
50% 50% coinsurance (after deductible)
$10/$20 $10 generic/$20 brand (after deductible)
$10/$20/$40/$150 $10 generic/$20 brand/$40 non-formulary brand /$150 specialty (after deductible)
$10/$20/$40 $10 generic/$20 brand/$40 non-formulary brand (after deductible)
$10/$30/50%/50% $10 generic/$30 brand/50% non-formulary brand/50% specialty (after deductible)
$10/$30/25%/25% $10 generic/$30 brand/25% non-formulary brand/25% specialty (after deductible)
$10/$30/$45 $10 generic/$30 brand/$45 non-formulary brand (after deductible)
$15/$30 $15 generic/$30 brand (after deductible)
$15/$30/50%/50% $15 generic/$30 brand/50% non-formulary brand/50% specialty (after deductible)
$15/$30/$50 $15 generic/$30 brand/$50 non-formulary brand (after deductible)
$15/$30/$50/$150 $15 generic/$30 brand/$50 non-formulary brand/$150 specialty (after deductible)
$20/$40 $20 generic/$40 brand (after deductible)
$20/$40/$60 $20 generic/$40 brand/$60 non-formulary brand (after deductible)
$20/$40/$60/$150 $20 generic/$40 brand/$60 non-formulary brand/$150 specialty (after deductible)
*The prescription drug rider may also be purchased with preventive drugs not subject to the deductible. Contact your account manager for details.
SUPPLEMENTAL BENEFIT OPTIONS FOR HSA-QUALIFIED HIGH DEDUCTIBLE HEALTH PLANS SUPPLEMENTAL BENEFITS

21
SUPPLEMENTAL BENEFIT OPTIONS FOR HSA-QUALIFIED HIGH DEDUCTIBLE HEALTH PLANS SUPPLEMENTAL BENEFITS
Chiropractic careSelf-referred chiropractic care is available through The CHP Group–approved network providers in the Kaiser Permanante service area. Visit chpgroup.com for a list of providers.
Alternative care (includes chiropractic care)Self-referred alternative care is available from The CHP Group network providers in our service area. Annual benefit maximums of $1,000, or $1,500. Visit chpgroup.com for a list of providers.
Options Member pays$10 $10 per chiropractic, acupuncture, or naturopathic visit; $25 per massage therapy visit for up to 12 visits per year all
after deductible.
$15 $15 per chiropractic, acupuncture, or naturopathic visit; $25 per massage therapy visit for up to 12 visits per year all after deductible.
$20 $20 per chiropractic, acupuncture, or naturopathic visit; $25 per massage therapy visit for up to 12 visits per year all after deductible.
20% coinsurance 20% coinsurance after deductible per chiropractic, acupuncture, naturopathic or massage therapy visit for up to 12 visits per year.
Vision hardware2
Eye exams are covered as a medical benefit at the applicable office visit charge. Vision hardware must be prescribed and purchased at Vision Essentials by Kaiser Permanente. Visit kp2020.org.
Options Member pays12-month allowance For members 19 and older:
Balance after allowance applied toward the purchase of frames and lenses or contacts every 12 months. Allowance options: $150, $200, $250, $300, $400, or $500 For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months. Eyeglasses or contacts outside of the select list are available for purchase with an allowance toward the purchase price, as a buy-up option. (Members cannot use both the standard/free benefit and the allowance benefit within the same calendar year.)
24-month allowance For members 19 and older:Balance after allowance applied toward the purchase of frames and lenses or contacts every 24 months. Allowance options: $100, $150, $200, $250, $300, $400, or $500For members 18 and younger:No charge for one pair of frames from a select list and lenses or contacts every 12 months.
Hearing aids One hearing aid per ear per 48 months up to: $250, $500, $1,000, $1,500 allowance
2Member payments for this benefit do not apply to the medical out-of-pocket maximum or deductible.

22
HSA-Qualified Added Choice® Plans give your employees the opportunity to combine the cost savings of a high deductible health plan with their desire to keep their current doctor or the option to see any licensed provider for covered services. Only Kaiser Permanente offers the option to see any licensed provider across the nation along with exclusive access to Select Providers and Select Facilities.
PLAN HIGHLIGHTS FOR HSA-QUALIFIED ADDED CHOICE® PLANS
AA 1 EE 1 EE 3 EE 4
ACCUMULATION TYPE AGGREGATE EMBEDDED EMBEDDED EMBEDDED
TIER 1 TIER 2 TIER 3 TIER 1 TIER 2 TIER 3 TIER 1 TIER 2 TIER 3 TIER 1 TIER 2 TIER 3
DEDUCTIBLE $1,500 / $3,000
$2,500 / $5,000
$3,500 / $7,000
$2,600 / $5,200
$3,600 / $7,200
$4,600 / $9,200
$2,600 / $5,200
$3,600 / $7,200
$4,600 / $9,200
$2,600 / $5,200
$3,600 / $7,200
$4,600 / $9,200
OUT-OF-POCKET MAXIMUM
$2,500 / $5,000
$4,000 / $6,550
$5,000 / $10,000
$4,000 / $8,000
$5,000 / $10,000
$6,000 / $12,000
$5,200 / $10,400
$6,200 / $12,400
$9,200 / $18,400
$5,200 / $10,400
$6,200 / $12,400
$9,200 / $18,400
OFFICE VISITS — PREVENTIVE
$0 20% 30% $0 20% 30% $0 20% 30% $0 30% 40%
OFFICE VISITS — PRENATAL CARE
$0 20% 30% $0 20% 30% $0 20% 30% $0 30% 40%
OFFICE VISITS —PRIMARY CARE & URGENT CARE
10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%
OFFICE VISITS — SPECIALTY CARE
10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%
ROUTINE EYE EXAMS 10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%
OUTPATIENT SURGERY
10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%
LABS, X-RAYS, AND SPECIAL DIAGNOSTIC PROCEDURES
10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%
EMERGENCY CARE 10% 10% 10% 20%
HOSPITAL INPATIENT CARE
10% 20% 30% 10% 20% 30% 10% 20% 30% 20% 30% 40%

23
SUPPLEMENTAL BENEFIT OPTIONS FOR HSA-QUALIFIED ADDED CHOICE® PLANS
SUPPLEMENTAL BENEFITSBelow are the options available with our HSA-Qualified Added Choice® Plans Contact your sales executive or account manager for more information.
Outpatient prescription drugsThe Kaiser Permanente formulary applies to all plans. Members get up to a 30-day supply for each copayment (up to a 90-day supply of maintenance drugs for two copayments when our Mail-Delivery Pharmacy is used).1 View our formulary at kp.org/formulary. Note: Prescription drug cost shares apply to the medical out-of-pocket maximum.1Specialty drugs are provided at one copay (or one maximum) for a 30-day supply.
Select Pharmacies MedImpact pharmacies
GENERIC COPAYMENT
FORMULARY BRAND COPAYMENT
GENERIC COPAYMENT
FORMULARY BRAND COPAYMENT2
NON-FORMULARY BRAND COPAYMENT2
$10 $20 $15 $30 $50
$15 $30 $20 $40 $60
20% coinsurance 30% coinsurance
Select Pharmacies MedImpact pharmacies
GENERIC COPAYMENT
FORMULARY BRAND COPAYMENT
NON-FORMULARY BRAND COPAYMENT
GENERIC COPAYMENT
FORMULARY BRAND COPAYMENT2
NON-FORMULARY BRAND COPAYMENT2
$10 $20 $40 $15 $30 $50
$15 $30 $50 $20 $40 $60
$20 $40 $60 $30 $60 $80
2 If a brand drug with an equivalent generic is prescribed and the member requests the brand drug, the charges will be the copayment plus the difference in retail price between the generic and the brand drug. If the prescriber indicates brand is medically necessary, the member will pay the applicable copayment.
Alternative care Self-referred alternative care, without prior authorization, is available through The CHP Group–approved network providers. If you are on an Added Choice® plan with an alternative care benefit, you may use your benefits at The CHP Group (located in our service area), First Choice, or any licensed nonparticipating providers and facilities. The amount an Added Choice member pays is based on the provider. For a list of participating providers, visit www.chpgroup.com.
ALTERNATIVE CARE†
Self-referred chiropractic care Self-referred chiropractic, massage,3 acupuncture, and naturopathic care
OFFICE VISIT COPAYMENT
NUMBER OF VISITS PER CALENDAR YEAR UP TO
OFFICE VISIT COPAYMENT
CALENDAR YEAR BENEFIT MAXIMUM UP TO
$10 15, 20, 30 $10 $500, $1,000, $1,500
$15 $15
$20 $20
$25 $25
$30 3Massage office copayment is always $25 with a 12-visit limit per calendar year.
VISION HARDWARE COVERAGE Member pays
12-month allowance For members 19 and above: Balance after allowance applied toward the purchase of frames and lenses or contacts every 12 months. Allowance options: $150, $200, $250, $300, $400, or $500 For members 18 and under: No charge for one pair of frames and lenses or contacts every 12 months. Eyeglasses or contacts outside of the select list are available for purchase with an allowance toward the purchase price, as a buy-up option. (Members cannot use both the standard/free benefit and the allowance benefit within the same calendar year.)
24-month allowance For members 19 and above: Balance after allowance applied toward the purchase of frames and lenses or contacts every 24 months. Allowance options: $100, $150, $200, $250, $300, $400, or $500 For members 18 and under: No charge for one pair of frames and lenses or contacts every 24 months
Hearing aids One hearing aid per ear per 48 months up to: $250, $500, $1,000, $1,500 allowance.

©2015 Kaiser Foundation Health Plan of the Northwest50LBG-15/9-15
kp.org