9 sample lesson (6) =tools
TRANSCRIPT

Lesson (6) =Tools

The Biggest Change

Blame = not
responsible =inaction =
no corrective action










Meeting Burden of Proof Denied
Case Luis Gonzalez (Luis Gonzalez Valladeres), Applicant v. San Cristobal
Distributing, State Compensation Insurance Fund, Defendants No.
ADJ6448504 (Panel Decision)Opinion Filed November 12, 2010 which held:
“When an applicant's case is resolved by a compromise and release with no
admission of liability, a lien claimant has the burden to establish a prima facie
case of industrial injury. After a prima facie case is presented, the burden shifts
to the defendant to rebut the prima facie showing. (Pace Medical Group, inc. v.
Workers' Comp. Appeals Bd. (Valiente) (1994) 59 Cal.Comp.Cases 354, 356
([writ denied].) Contrary to the defendant's argument, it is well established that
a lien claimant can carry its burden by introducing hearsay statements in
medical records, and it is not required to prove its case by presenting an
injured worker's testimony. (Independence Indem. Co. v. IAC (Lohnes) (1935)
2 Cal.2d 397, 410 [20 IAC 311]; Lab. Code, §5708.)
12/11/2016 www.workcompliens.com 14

Defective Notices –Resulting In
Unreasonable Offer of Care
Bruce Knight, United Parcel Service; and Liberty Mutual Insurance Company October 10, 2006 71 Cal. Comp. Cases 1423 “The Board held that an employer or insurer's failure to provide required notice to an employee of rights under the MPN (medical provider network) that results in a neglect or refusal to provide reasonable medical treatment renders the employer or insurer liable for reasonable medical treatment self-procured by the employee.

9767.9. Transfer of Ongoing Care
into the MPN
9767.9 (j) If the treating physician does not agree with the employer's or insurer's determination that the injured covered employee's medical condition does not meet the conditions set forth in subdivisions (e)(1) through (e)(4), the transfer of care shall not go forward until the dispute is resolved.
Big issue for providers, they are ignoring these notice
to transfer into MPN when all they had to do was
object to make it an none issue and continue to treat
until resolved by the WCAB

The King is defined as the burden
of proof.
The King is defined as the burden of proof. The reason is, that if the King is
captured or more correctly checkmated, it ends the game, although not the
most powerful piece as it can only move one space at a time in any direction
(exception, castling ), it is the most important piece, as without it, the game is
over. In workers comp, based on the 2012 en banc "Torres" case, although a
WCAB decision, all stages and or processes involved in a Provides' dispute,
revolves around the burden of proof. From medical reports justify billing
codes, medical facts in medical reports for authorization, overcoming MPNs
and most importantly, issues at the WCAB, all are determined based on
the burden of proof, without it you lose, with it and the game is won. From the
start to the end of the game, one always protects the King, using pawns and or
any other piece to accomplish that. Thus like workers comp, from the start,
you use other processes and evidence to develop your burden of proof

The King is defined as the burden
of proof.
The King is defined as the burden of proof. The reason is, that if the King is
captured or more correctly checkmated, it ends the game, although not the
most powerful piece as it can only move one space at a time in any direction
(exception, castling ), it is the most important piece, as without it, the game is
over. In workers comp, based on the 2012 en banc "Torres" case, although a
WCAB decision, all stages and or processes involved in a Provides' dispute,
revolves around the burden of proof. From medical reports justify billing
codes, medical facts in medical reports for authorization, overcoming MPNs
and most importantly, issues at the WCAB, all are determined based on
the burden of proof, without it you lose, with it and the game is won. From the
start to the end of the game, one always protects the King, using pawns and or
any other piece to accomplish that. Thus like workers comp, from the start,
you use other processes and evidence to develop your burden of proof

The Queen is defined as, Medical-
Legal, WCAB and Petitions. The Queen is defined as, Medical-Legal, WCAB and Petitions. The Queen is the most
powerful piece in the game, although many a games are won without it, one does not let it
go easily, as it can move like any piece on the board, except the knight, that can jump over
pieces. In workers comp, Medical-Legal services / disputes have a carve out, outside the
requirement of normal authorization, not subject to MPN rules and defenses, not subject to
the determination of the case-in-chief, nor subject to lien fees and time limits, making
medical-legal services the most powerful of all services in workers comp. Only a master
chessman or chess-woman, truly knows the importance of the Queen and how to
maximizes its function and power. Because of the many powerful tools in workers comp, I
added to the Queen, the WCAB, Appeals and Petitions, as the additional power tools of the
Queen. Petitions; the Director through the medical unit of the DWC is in control and the
watch dog of the UR, IBR, second review and IMR Process, of which several Petitions and
appeals can be filed, both defined and those yet to be defined. This process is to ensure the
King (burden of proof), is not compromised by fouls in the game. The Queen, also defines
the WCAB, with the massive influx of laws, a tremendous amount of case law should be
being created as to the interpretation and function of the new laws, of which is presently
lacking, thus the lack of the use of the queen.

The Queen is defined as, Medical-
Legal, WCAB and Petitions. The Queen is defined as, Medical-Legal, WCAB and Petitions. The Queen is the most
powerful piece in the game, although many a games are won without it, one does not let it
go easily, as it can move like any piece on the board, except the knight, that can jump over
pieces. In workers comp, Medical-Legal services / disputes have a carve out, outside the
requirement of normal authorization, not subject to MPN rules and defenses, not subject to
the determination of the case-in-chief, nor subject to lien fees and time limits, making
medical-legal services the most powerful of all services in workers comp. Only a master
chessman or chess-woman, truly knows the importance of the Queen and how to
maximizes its function and power. Because of the many powerful tools in workers comp, I
added to the Queen, the WCAB, Appeals and Petitions, as the additional power tools of the
Queen. Petitions; the Director through the medical unit of the DWC is in control and the
watch dog of the UR, IBR, second review and IMR Process, of which several Petitions and
appeals can be filed, both defined and those yet to be defined. This process is to ensure the
King (burden of proof), is not compromised by fouls in the game. The Queen, also defines
the WCAB, with the massive influx of laws, a tremendous amount of case law should be
being created as to the interpretation and function of the new laws, of which is presently
lacking, thus the lack of the use of the queen.

§10451.1. Determination of Medical-
Legal Expense Disputes. PETITIONS
The following procedures shall be utilized for the determination of medical-legal expense disputes.
(b) For purposes of this section:
(1) “medical-legal expense” shall mean any cost or expense incurred by or on behalf of any party for the purpose of proving or disproving a contested claim, including but not limited to:
(A) goods or services expressly specified by Labor Code section 4620(a);
(B) services rendered by a non-medical expert witness;
(C) services rendered by a certified interpreter during a medical-legal examination; and
(D) all costs or expenses for copying and related services.
(2) “medical-legal provider” shall mean any person or entity that seeks payment for or reimbursement of a medical-legal expense, other than an employee, a dependent, or the attorney or non-attorney representative of an employee or dependent who directly paid for medical-legal goods or services.
(c) Medical-Legal Expense Disputes Not Subject to Independent Bill Review

§ 10301. Definitions(dd) “Party”
means § 10301. Definitions(dd) “Party” means: (1) a person claiming to be an
injured employee or the dependent of a deceased employee; (2) a
defendant; (3) an appellant from an independent medical review or
independent bill review decision or an injured employee or
provider seeking to enforce such a decision; (4) a medical-legal
provider involved in a medical-legal dispute not subject to independent
bill review; (5) an interpreter filing a petition for costs in accordance
with section 10451.3; or (6) a lien claimant where either (A) the
underlying case of the injured employee or the dependent(s) of a
deceased employee has been resolved or (B) the injured employee or
the dependent(s) of a deceased employee choose(s) not to proceed with
his, her, or their case.

Case Law
The definition of "contested claim" is varied, and can mean any of the
following: a rejected claim; a presumptively compensable claim; a
claim where temporary disability has not timely commenced or has not
issued a timely notice of delay; a claim where liability is accepted but
there are disputed medical facts.
If the PTP is requested by a "party" (applicant, Applicant Attorney,
Insurance), to do a P&S, a consultation , or any other report regarding
a "contested claim" , the PTP can then request (designate) and transfer
that request by a "party", to a another Provider (different specialty say a
psych which would include all necessary testing) to perform a Medical
Legal, and then those services are treated as a Medical- Legal and paid
as the same under the medical-legal fee schedule not the OMFS.


Case Law
En Banc Decisions of Warren Brower v David Jones Construction; State Compensation Insurance Fund May 21, 2014 Case No: ADJ802221 (SJO 0258870) 79 Cal. Comp. Cases 550
In a recent En Banc Decision the Court Held: Moreover, a medical-legal expense is ordinarily allowable if it is capable of proving or disproving a contested claim, if the expense was reasonably necessary at the time incurred, and if the cost incurred was reasonable. (§§ 4620 et seq., 5307.6.) The mere fact that the parties had agreed to an AME in a particular specialty does not mean that a party cannot reasonably obtain a comprehensive medical-legal report from a treating physician in the same or similar specialty

Adjuster States 0 Allowed Claim in
Litigation

Lesson (2) =The Pawn: no
Payments EORs:

Lesson (4) =IBR Process
Showing Prior Decisions

The Rook
The Rook or slang, castle (because it looks like a castle) , is defined as, the
IBR process and fee schedule issues. The castle is a strong and powerful piece
and each player has two. The rook can move forward and backward or from
side to side and covers a wide range of the board. However, because of its
limited function, all players always look to see where the rook is, thus few
surprises, as it is more of a matter of fact piece. The IBR process is a powerful
tool and regardless of the $195.00 fee, it has to be used, because of the several
IBR decisions already posted, going to the IBR and knowing the results before
hand should be no surprise. However, mastering the rook is knowing how the
rook has been played in other games to achieve a wining game, i.e. sometimes
it addresses; authorization issues, PPO issues and usual and customary, making
those who read the IBR decisions a master of playing the rook, for winning
moves

Burden of
Proof the
King
The Rook
IBR
Process
The Queen
ML ,
WCAB,
Petitions
The Queen
ML ,
WCAB,
Petitions

Why One Is Right
"Lien claimant, Passages Malibu, seeks reconsideration and removal
from the Findings and Award, issued July 1, 2015,- in which a workers'
compensation administrative law judge (WCJ) ordered defendant
Liberty Mutual/Wausau, to pay lien claimant the sum of $272,533.26,
as the reasonable value of the services provided to applicant Bruno
Sabato, less credit for sums paid. Lien claimant contends the WCJ's
finding of the reasonable value of lien claimant's services is
not substantiated by the evidence, and requests that the Appeals Board
remove this matter to itself and find that it is entitled to payment of
$1,130,975.60. Lien claimant contends that there is no dispute as to its
entitlement for payment as defendant pre-authorized 300 days of
services at its residential treatment
facility."

ML104-95 Evaluation, 96101 and 96118 Psychological Testing
performed on Injured Worker 10/07/2014
ISSUE IN DISPUTE: Provider seeking remuneration for ML104-95 Evaluation, 96101
and 96118 Psychological Testing performed on Injured Worker 10/07/2014.
Claims Administrator reimbursed $0.00 of $6,331.45 with the following rational:
Claim denied and is currently in litigation.
May 29, 2014 Letter from Claims Admin Legal parties, addressed to the Provider
indicated the following: Defendants do not believe that the applicant is entitled to a
Psychiatric Panel at this time.
August 12, 2014 Letter to Provider from Claimants Attorney requesting PQM
Psychological Evaluation to include Causation and Apportionment.
Court Order, 07/17/2014, signed by Workers Compensation Administrative Law Judge
Granted the following: Applicant to go to PQME Eval w/ (Provider) to resolve psych
issues.
Provider is the PQME evaluator stated in the court order

The New With Billing payments is
The Unusual

96118-59 and 9611-59 Claims Administrator denied codes indicating on the Explanation of Review Payment based on
individual pre-negotiated agreement for this specific service and Service exceeds agreed utilization
Letter dated 02/25/2015 from Utilization Review authorized 6 units Neuropsych Testing by TE for
insomnia nos. Service dates from 02/25/2015 through 03/25/2015
96119 -Neuropsychological testing (eg, Halstead-Reitan Neuropsychological Battery, Wechsler Memory
Scales and Wisconsin Card Sorting Test), with qualified health care professional interpretation and report,
administered by technician, per hour of technician time, face-to-face
Interpretation and report by the technician were not found for this review. Therefore, documentation does
not support billed code 96119 and reimbursementis not warranted.
CPT 96118 -Neuropsychological testing (eg, Halstead-Reitan Neuropsychological Battery, Wechsler
Memory Scales and Wisconsin Card Sorting Test), per hour of the psychologist's or physician's time,
both face-to-face time administering tests to the patient and time interpreting these test results and
preparing the report
Report dated March 25, 2015 titled Neuropsychological Evaluation signed by Provider above, documents
a consultation with the injured worker as 1.5 hours and 7 hours of interpretation & report writing by the
neuropsychologist


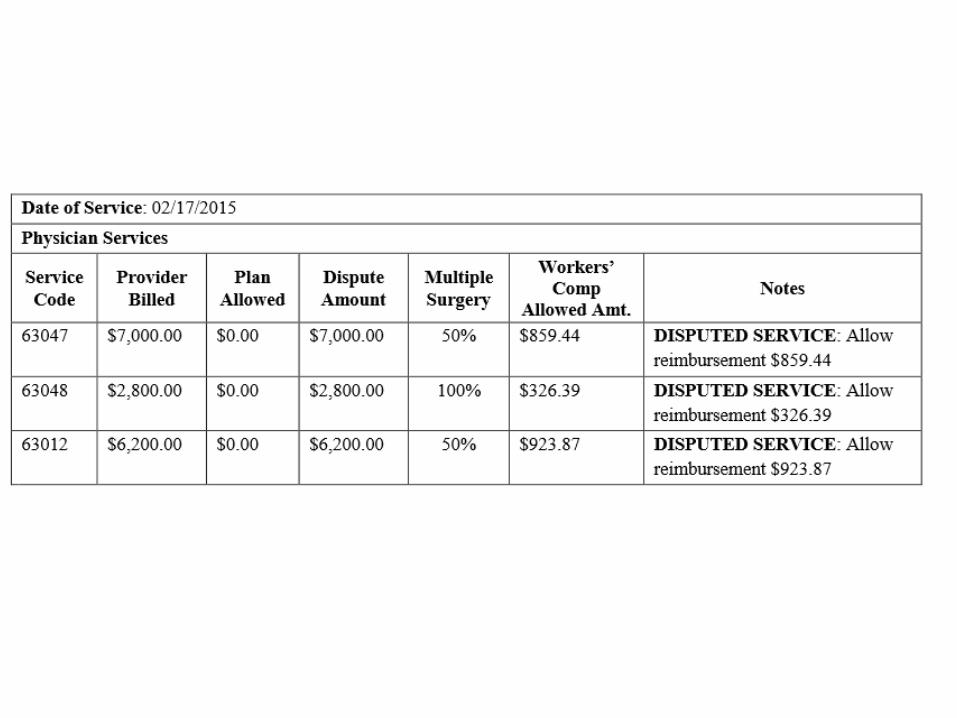
22848, 63012, 63044, 63047, and
63048 ISSUE IN DISPUTE: Provider is dissatisfied with denial of codes 22848, 63012,
63044,
63047, and 63048
Claims Administrator denied code 22848 indicating on the Explanation of Review
Per CCI Edits, the value of this procedure is included in the value of the comprehensive
procedure
If modifier column shows 1 for pair codes, if an approved modifier is appended to the
column 2 code and documentation is submitted to support the billed service, then the
edit may be overridden.
As a pair code exists between billed code 22848 and reimbursed code 27280, provider
did not apply a proper modifier to 22848 on the CMS 1500 form. Therefore,
reimbursement of 22848 is not warranted.

22848, 63012, 63044, 63047, and
63048 CHAP8-CPTcodes60000-69999_final10312013.doc; NATIONAL CORRECT CODING
INITIATIVE POLICY MANUAL FOR MEDICARE SERVICES Revision Date: 1/1/2014C. Nervous System: 18. A laminectomy includes excision of all the posterior
vertebral components, and a laminotomy includes partial excision of posterior vertebral components. Since a laminectomy is a more extensive procedure than a laminotomy, a laminotomy code should not be reported with a laminectomy code for the same vertebra
Provider s report documents Next, decompressive laminectomies/facetectomies were performed from T12-S1. From T12-L3 laminotomies/laminectomies were performed
Reimbursement of codes 63047 and 63048 is warranted.
Reimbursement of 63044 is not warranted.
CPT 63012 was denied by Claims Administrator as �The submitted documentation does not support the service being billed for. We will re-evaluate this upon receipt of clarifying information
63012 - Laminectomy with removal of abnormal facets and/or pars inter-articularis with decompression of cauda equina and nerve roots for spondylolisthesis, lumbar (Gill type procedure)
Provider s documentation describes At L4-5, a Gill-type procedure was performed
Reimbursement of 63012 is warranted.

63081, 63082-59 X 3, 22851-59 X 3, 69990-59,
and 76001-59
SSUE IN DISPUTE: Provider is dissatisfied with reimbursement of codes 63081, 63082 -
59 X 3, 22851-59 X 3, 69990-59, and 76001-59
Provider denied codes indicating on the Explanation of Review The charge for this
procedure was not paid since the value of this procedure is included/bundled within The
value of another procedure performed
Provider billed code 69990-59 along with reimbursed billed code 22554. Per NCCI Edit of
the pair code between these two states they are never to be billed together and a modifier is
not allowed to override the edit. As such, reimbursement of 69990 is not warranted.
Claims Administrator also denied code 76001-59, Fluoroscopy, physician or other
qualified health care professional time more than 1 hour, assisting a nonradiologic
physician or other qualified health care professional (eg, nephrostolithotomy, ERCP,
bronchoscopy, transbronchial biopsy)
Providers report submitted does not document 76001 and therefore, reimbursement is not
warranted for 76001.

63081, 63082-59 X 3, 22851-59 X 3,
69990-59, and 76001-59 Provider also billed 3 units of 22851-59,Application of intervertebral biomechanical device(s) (eg,
synthetic cage(s), methylmethacrylate) to vertebral defect or interspace (List separately in addition to
code for primary procedure)which is documented in the providers report.
Reimbursement of 22851 x 3 is warranted.
Provider also billed 63081, Vertebral corpectomy (vertebral body resection), partial or complete, anterior
approach with decompression of spinal cord and/or nerve root(s); cervical, single segment
Providers report documents A partial corpectomy had to be carried out before we were able to remove the
posterior osteophyte and decompress the spinal cord because of the very narrow disc space
Reimbursement of 63081 is warranted.
Provider documents �The same happened at C4-5 as well where partial corpectomy had to be carried
out as well�which supports billed code 63802, Vertebral corpectomy (vertebral body resection), partial
or complete, anterior approach with decompression of spinal cord and/or nerve root(s); cervical, each
additional segment (List separately in
addition to code for primary procedure) for 1 unit.
•


CPT 97750, ANALYSIS AND FINDING
Based on review of the case file the following is noted: ISSUE IN DISPUTE: Provider is dissatisfied with denial of CPT 97750, Physical
performance test or measurement (eg, musculoskeletal, functional capacity), with written report, each 15 minutes
EOR does not indicate 97750 as unauthorized but does state No separate payment was made because the value of the service is included within the value of another service performed on the same day
EOR s received only show CPT code 97750 billed along with CMS 1500 form billing only 97750.
Provider s report submitted documents 2 hours spent face to face and 60 minutes of report preparation
Opportunity to Dispute sent to Claims Administrator 08/12/2015; response not yet received
Based on the aforementioned documentation and guidelines, additional reimbursement is warranted for 97750 x12
Provider states a 10% PPO discount is to be applied to reimbursement

97670 “Functional Capacity Evaluation ” No Value 99499 at Customary Charges $1,687.50 /2nd
$2,375.00
Claims Administrator denied code indicating on the Explanation of Review “The Official Medical Fee
Schedule does not list this code(97670). No payment is being made at this time. Please resubmit your
claim with the OMFS codes that best describe the service(s) provided and your supporting
documentation”
Report Entitled “Functional Capacity Evaluation” reflects date of service 1/19/2015 OMFS allows for
Unlisted Procedure Codes to be reimbursed by “By Report.”
§9789.12.4 (c) “In determining the value of a By Report procedure, consideration may be given to the
value assigned to a comparable procedure or analogous code. The comparable procedure or analogous
code should reflect similar amount of resources, such as practice expense, time, complexity, expertise,
etc. as required for the procedure performed.”A code used in Functional Capacity Evaluation has been
99499.
There is no allowance or comparable code listed under the OMFS for service billed with procedure code
99499 or, more specifically, a Functional Capacity Evaluation;
Initial payments was zero allowed order for payments of billed charges in the amount of $1,687.50.
The correct billing code for a Functional Capacity Evaluation, 99499

97670 “Functional Capacity Evaluation ” No Value 99499 at Customary Charges $1,687.50 /2nd $2,375.00
ANALYSIS AND FINDING
Based on review of the case file the following is noted:
ISSUE IN DISPUTE: Provider dissatisfied with reimbursement of code 97799-86
Based on review of the Physician’s Initial Evaluation, procedure code 97799-86 is substantiated as the Provider
documented services performed and Provider’s Usual and Customary charge.
The Physician Evaluation details the injured worker’s medical history, current medications, physical examination
including functional strength, range of motion, function movement and lifting, dynamic posture and stabilization,
psychological evaluation, treatment plan and a formal request for authorization, a thorough evaluation was performed on
this injured worker
Claims Administrator based its reimbursement of 97799 86 on97670. The OMFS does not list an allowance for 97799 or
97670; these are described as “By Report” codes.
Documents reviewed included the Request for Authorization of Medical Treatment for an Initial Interdisciplinary
Evaluation documenting Provider’s cost at $2500.00.
Utilization Review Decision letter documented: Approved Initial Evaluation from 10/30/2013 –11/30/2013 Per the
supplied PPO contract, covered services billed with a procedure code for which there is no assigned value, Provider shall
be reimbursed at 95% of Eligible billed charge $ 2375.00

ANALYSIS AND FINDING
Based on review of the case file the following is noted: ·
ISSUE IN DISPUTE: Provider dissatisfied with reimbursement of code 97799-30·
Provider was reimbursed $471.81and is seeking additional reimbursement of $923.13.·
Claims Administrator sent a partial payment in the amount of $471.81 indicating on the Explanation of Review:
“The charge exceeds the official medical Fee Schedule allowance. The charge has been adjusted to the
scheduled allowance.” and “The Fee Schedule does not include a value for the procedure code billed. An
allowance has been made which is based on charges for similar/comparable services. Reimbursement is based
on the applicable reimbursement fee schedule.”
Claims Administrator does not state which code the 97799-30 is based on. ·
Included in this review is the Authorization Request –F.C.E. as a Panel QME, dated 4/8/2014 from the Provider.
The Request shows the CPT Request with Fee’s as 97799-30, Functional Capacity Evaluation/Unlisted Code, in
the amount $1395.00.
·
Claims Administrator sent Approved notification for Functional Capacity Evaluation dated April 17, 2014.
Instructions included “Services will be paid pursuant to the Official Medical Fee Schedule or an appropriate
PPO Contract” and the Authorization will expire in 60 Days
.
97799-30

97799-30
Physician’s Functional Capacity Evaluation report documents “Approximately 5 hours and 40 minutes of physical
testing, report preparation, research, calculations and editing were performed in the completion of this Functional
Capacity Evaluation.” Provider also states: “Completion of the intake forms, health-screening questionnaire, job demand
questionnaire, the history, interview and eMTAP required reading and writing, while sitting and took approximately 50
minutes to complete” as well as “The patient is slightly restricted upon standing for 90 minutes during the functional
capacity evaluation.”
·
The Provider documents the numerous tests performed on this patient including strength test, sitting and standing
tolerance, aerobic step test, hand functional tests, manual muscle testing of the upper and lower extremity, tendon
reflexes, abnormal sensation, lifting capacity and carrying test, pushing and pulling, activities of daily living, fine motor
dexterity, cool down and activity log, functional capacity assessment and the Physician’s Permanent and
Stationary Report.
·
CPT code 97799 is an unlisted code the Provider billed at $1395.00. Claims Administrator reimbursed a partial payment
of $ 471.81 but failed to report what this figure was based on. Therefore, CPT code 97750, Physical Performance Test or
Measurement (egMusculoskeletal, Functional Capacity) with written report, each 15 minutes best describes the procedure
demonstrated and will replace the 97799-30 billed by the Provider.
·
CPT 97750 is listed on the Official Medical Fee Schedule at $38.34/unit and the provider spent a total of 340 minutes or
23 units. 38.34 x 23 = 881.82, this will be the appropriate Official Medical Fee to use on this review


OUTPATIENT FUNCTIONAL CAPACITY
EVALUATION (FCE):Overturned
Claims Administrator guideline: Decision based on MTUS Chronic Pain Treatment Guidelines.
MAXIMUS guideline: Decision based on MTUS ACOEM Chapter 5 Cornerstones of Disability Prevention and Management Page(s): 89-92. Decision based on Non-MTUS Citation Official
Disability Guidelines (ODG) Chapter Fitness for Duty Chapter, FCE.

ACOEM guidelines
Decision rationale: ACOEM guidelines indicate there is a functional assessment tool available
and that is a Functional Capacity Evaluation, however, it does not address the criteria. As such,
secondary guidelines were sought. Official Disability Guidelines indicates that a Functional
Capacity Evaluation is appropriate when a worker has had prior unsuccessful attempts to return
to work, has conflicting medical reports, the patient had an injury that required a detailed
exploration of a workers abilities, a worker is close to maximum medical improvement and/or
additional or secondary conditions have been clarified. However, the evaluation should not be
performed if the main purpose is to determine a worker's effort or compliance or the worker has
returned to work and an ergonomic assessment has not been arranged. The clinical
documentation submitted for review indicated the patient had prior unsuccessful attempts to
Return to work and was close to maximum medical improvement. Given the above, the request
for a Functional Capacity Evaluation is medically necessary

EPIDURAL INJECTION
The criteria for the use of epidural steroid injections are as follows:
1) Radiculopathy must be documented by physical examination and corroborated by imaging studies
and/orelectrodiagnostic testing.
2) Initially unresponsive to conservative treatment (exercises, physical methods, NSAIDs and muscle
relaxants).3) Injections should be performed using fluoroscopy (live x-ray) for guidance.
4) If used for diagnostic purposes, a maximum of two injections should be performed. A second block is
notrecommended if there is inadequate response to the first block. Diagnostic blocks should be at an
interval of at least one to two weeks between injections.
5) No more than two nerve root levels should be injected using transforaminal blocks.
6) No more than one interlaminar level should be injected at one session.
7) In the therapeutic phase, repeat blocks should be based on continued objective documented pain and
functional improvement, including at least 50% pain relief with associated reduction of medication use
for six to eight weeks, with a general recommendation of no more than 4 blocks per region per year.
(Manchikanti,2003) (CMS, 2004) (Boswell, 2007) 8) Current research does not support a "series-of-
three" injections in either the diagnostic or therapeutic phase.

Elements:
• unresponsiveness to conservative treatment.
• imaging studies
• clear clinical signs of radiculopathy and non-corroborative findings on imaging,
Additional Injections:
• Objective Functional Improvement from prior injections The ODG identifies documentation of at least 50-70% pain relief for six to eight weeks, with a general recommendation of no more than four blocks per region per year, as well as decreased need for pain medications, and functional response as criteria necessary to support the medical necessity of additional epidural steroid injections.
Common Mistakes
• lack of documentation indicating the injured worker had radiating pain with the straight leg raise.•
• lack of documentation of failure of conservative care.
• failed to indicate the laterality, as well as the level for the injection
• no indication for failed conservative trial for diagnoses of cervicalgia and cervical
• no imaging studies provided for review.
• no documentation of unresponsiveness to conservative treatment.
• no more than 2 joint levels are injected in one session is recommended
• no documentation of at least 50-70% pain relief for six to eight weeks following previous injection
Overturned Requests:
• Decision rationale: According to the medical records provided for review, the patient has radicular symptomatology and findings on examination and documented by previous electrodiagnostic studies as well as MRI. Her therapeutic options appear to be limited by external issues restricting the use of analgesics and she has been described as reaching maximal medical improvement. Her clinical picture qualifies her for the lumbar epidural procedure. Therefore the request for the Right Lumbar ransforaminal Epidural Steroid Injection at L5-S1 under fluoroscopy is deemed to be medically necessary and appropriate


Functional Restoration Programs
Functional Restoration Programs be based on comprehensive evaluation of the patient's functional capabilities and psychological overlay.
Functional Restoration Program. The MTUS guidelines page 49 recommends functional restoration programs and indicate it may be considered medically
necessary when all criteria are met including (1) adequate and thorough evaluation has been made (2) Previous methods of treating chronic pain have been unsuccessful (3) significant loss of ability to function independently resulting from
the chronic pain; (4) not a candidate for surgery or other treatments would clearly be (5) The patient exhibits motivation to change (6) Negative predictors of success above have been addressed.
Also, California Medical Treatment Utilization Schedule recommends that a Functional Restoration Program is appropriate for patients who have not
responded to previous chronic pain treatments and are unlikely to show any significant clinical improvement from further treatment.
California Medical Treatment Utilization Schedule recommends a functional restoration program for patients that have had an adequate and thorough baseline evaluation to support functional improvement throughout the program and documentation of willingness and a motivation to change

Common Errors
• Fails to provide any evidence that the patient has undergone a comprehensive psychological or physical evaluation to determine the patient's appropriateness for a Functional Restoration Program.
• Documentation submitted for review does not provide evidence that the patient has exhausted all lesser forms of conservative treatment and will not significantly improve as a result of further conservative treatments.
• Does not clearly identify a duration of treatment.
• The appropriateness of that treatment cannot be established
• The clinical documentation as it is submitted does not contain any evidence of the patient's motivation to change or a functional baseline assessment to assist in determining functional improvements related to the program.
• The clinical documentation submitted for review does not provide evidence that treatment beyond the recommended 20 sessions is necessary
• It is not clear whether the patient is a candidate for surgery or other treatment, whether he had exhibited motivation to change, and whether negative predictors of success have been addressed.
• Request for six weeks of treatment in a functional restoration program is not supported as the patient does not meet all of the criteria and the request for treatment for 6 weeks exceeds the guideline recommendations
• Negative predictors of success have not been addressed
• There are no exceptional factors noted within the documentation to support extending treatment beyond guideline recommendations.

96101 and 99354
ANALYSIS AND FINDING
Based on review of the case file the following is noted:
·
ISSUE IN DISPUTE:
Provider seeking full remuneration 96101, Psychological Testing Per Hour, 99354 Prolonged service in the office or
other outpatient setting requiring direct patient contact beyond the usual service; first hour performed on 05/09/2014.
Claims Administrator $0.00 Reimbursement Rational based on “NCCI Edits.”
·
Pursuant Title 8 CCR Physician Fee Schedule 1/1/2014, § 9789.12.13 Correct Coding Initiative: (a) The National Correct
Coding Initiative Edits (“NCCI”) adopted by the CMS shall apply to payments for medical services under the Physician
Fee Schedule. Except where payment ground rules differ from the Medicare ground rules, claims administrators shall
apply the NCCI physician coding edits and medically unlikely edits to bills to determine appropriate payment. Claims
Administrators shall utilize the National Correct Coding Initiative Coding Policy Manual for Medicare Services. If a
billing is reduced or denied reimbursement because of application of the NCCI, the claims administrator must notify the
physician or qualified non-physician practitioner of the basis for the denial, including the fact that the determination was
made in accordance with the NCCI.

96101 x 7 units, 99354 X 1 UNIT.
CMS 1500 form reflects 96101 x 7 units, 99354 X 1 UNIT.
CMS 1500 reflects multiple services, including 99205.
EOR reflects Provider reimbursed for 99204.
Based on the NCCI edits code pair exist between CPT 99205/99204 and 96101.
Modifier Indicator column shows ‘1’ which states if a proper modifier is appended to the correct code and documentation supports the use of the procedure code then the edit may be overridden.
Article 5.5.0. Rules For Medical Treatment Billing and Payment §9792.5.7. Requesting Independent Bill Review (b)(2) The proper selection of an analogous code or formula based on a fee schedule adopted by the Administrative Director, or, if applicable, a contract for reimbursement rates under Labor Code section 5307.11, unless the fee schedule or contract allows for such analogous coding.
The correct modifier (-59) was not appended to the column 2 codes: 96118. As such, reimbursement is not indicated.
Page 59 of the Phsychological report indicates “15” minutes reviewing medical file.” Breakdown of total visit time –vs-psychological testing, could not be abstracted from report. CPT 99204, reimbursed by the Claims Administrator, has a time factor or 45 min.
Billed Prolonged Services Code, 99354 is a “per hour code” and is not factored into the visit time until, at the very least, an additional 45 minutes have surpassed the time involved with the Evaluation and Management service.
·
Based on the aforementioned documentation and guidelines, additional reimbursement is not indicated for 96101 and 99354


Lesson (4) =IBR Process
Showing Prior Decisions

The Rook
The Rook or slang, castle (because it looks like a castle) , is defined as, the
IBR process and fee schedule issues. The castle is a strong and powerful piece
and each player has two. The rook can move forward and backward or from
side to side and covers a wide range of the board. However, because of its
limited function, all players always look to see where the rook is, thus few
surprises, as it is more of a matter of fact piece. The IBR process is a powerful
tool and regardless of the $195.00 fee, it has to be used, because of the several
IBR decisions already posted, going to the IBR and knowing the results before
hand should be no surprise. However, mastering the rook is knowing how the
rook has been played in other games to achieve a wining game, i.e. sometimes
it addresses; authorization issues, PPO issues and usual and customary, making
those who read the IBR decisions a master of playing the rook, for winning
moves

Burden of
Proof the
King
The Rook
IBR
Process
The Queen
ML ,
WCAB,
Petitions
The Queen
ML ,
WCAB,
Petitions

Why One Is Right
"Lien claimant, Passages Malibu, seeks reconsideration and removal
from the Findings and Award, issued July 1, 2015,- in which a workers'
compensation administrative law judge (WCJ) ordered defendant
Liberty Mutual/Wausau, to pay lien claimant the sum of $272,533.26,
as the reasonable value of the services provided to applicant Bruno
Sabato, less credit for sums paid. Lien claimant contends the WCJ's
finding of the reasonable value of lien claimant's services is
not substantiated by the evidence, and requests that the Appeals Board
remove this matter to itself and find that it is entitled to payment of
$1,130,975.60. Lien claimant contends that there is no dispute as to its
entitlement for payment as defendant pre-authorized 300 days of
services at its residential treatment
facility."

ML104-95 Evaluation, 96101 and 96118 Psychological Testing
performed on Injured Worker 10/07/2014
ISSUE IN DISPUTE: Provider seeking remuneration for ML104-95 Evaluation, 96101
and 96118 Psychological Testing performed on Injured Worker 10/07/2014.
Claims Administrator reimbursed $0.00 of $6,331.45 with the following rational:
Claim denied and is currently in litigation.
May 29, 2014 Letter from Claims Admin Legal parties, addressed to the Provider
indicated the following: Defendants do not believe that the applicant is entitled to a
Psychiatric Panel at this time.
August 12, 2014 Letter to Provider from Claimants Attorney requesting PQM
Psychological Evaluation to include Causation and Apportionment.
Court Order, 07/17/2014, signed by Workers Compensation Administrative Law Judge
Granted the following: Applicant to go to PQME Eval w/ (Provider) to resolve psych
issues.
Provider is the PQME evaluator stated in the court order

The New With Billing payments is
The Unusual

96118-59 and 9611-59 Claims Administrator denied codes indicating on the Explanation of Review Payment based on
individual pre-negotiated agreement for this specific service and Service exceeds agreed utilization
Letter dated 02/25/2015 from Utilization Review authorized 6 units Neuropsych Testing by TE for
insomnia nos. Service dates from 02/25/2015 through 03/25/2015
96119 -Neuropsychological testing (eg, Halstead-Reitan Neuropsychological Battery, Wechsler Memory
Scales and Wisconsin Card Sorting Test), with qualified health care professional interpretation and report,
administered by technician, per hour of technician time, face-to-face
Interpretation and report by the technician were not found for this review. Therefore, documentation does
not support billed code 96119 and reimbursementis not warranted.
CPT 96118 -Neuropsychological testing (eg, Halstead-Reitan Neuropsychological Battery, Wechsler
Memory Scales and Wisconsin Card Sorting Test), per hour of the psychologist's or physician's time,
both face-to-face time administering tests to the patient and time interpreting these test results and
preparing the report
Report dated March 25, 2015 titled Neuropsychological Evaluation signed by Provider above, documents
a consultation with the injured worker as 1.5 hours and 7 hours of interpretation & report writing by the
neuropsychologist


22848, 63012, 63044, 63047, and
63048 ISSUE IN DISPUTE: Provider is dissatisfied with denial of codes 22848, 63012,
63044,
63047, and 63048
Claims Administrator denied code 22848 indicating on the Explanation of Review
Per CCI Edits, the value of this procedure is included in the value of the comprehensive
procedure
If modifier column shows 1 for pair codes, if an approved modifier is appended to the
column 2 code and documentation is submitted to support the billed service, then the
edit may be overridden.
As a pair code exists between billed code 22848 and reimbursed code 27280, provider
did not apply a proper modifier to 22848 on the CMS 1500 form. Therefore,
reimbursement of 22848 is not warranted.
22848, 63012, 63044, 63047, and
63048 CHAP8-CPTcodes60000-69999_final10312013.doc; NATIONAL CORRECT CODING
INITIATIVE POLICY MANUAL FOR MEDICARE SERVICES Revision Date: 1/1/2014C. Nervous System: 18. A laminectomy includes excision of all the posterior
vertebral components, and a laminotomy includes partial excision of posterior vertebral components. Since a laminectomy is a more extensive procedure than a laminotomy, a laminotomy code should not be reported with a laminectomy code for the same vertebra
Provider s report documents Next, decompressive laminectomies/facetectomies were performed from T12-S1. From T12-L3 laminotomies/laminectomies were performed
Reimbursement of codes 63047 and 63048 is warranted.
Reimbursement of 63044 is not warranted.
CPT 63012 was denied by Claims Administrator as �The submitted documentation does not support the service being billed for. We will re-evaluate this upon receipt of clarifying information
63012 - Laminectomy with removal of abnormal facets and/or pars inter-articularis with decompression of cauda equina and nerve roots for spondylolisthesis, lumbar (Gill type procedure)
Provider s documentation describes At L4-5, a Gill-type procedure was performed
Reimbursement of 63012 is warranted.


63081, 63082-59 X 3, 22851-59 X 3, 69990-59,
and 76001-59
SSUE IN DISPUTE: Provider is dissatisfied with reimbursement of codes 63081, 63082 -
59 X 3, 22851-59 X 3, 69990-59, and 76001-59
Provider denied codes indicating on the Explanation of Review The charge for this
procedure was not paid since the value of this procedure is included/bundled within The
value of another procedure performed
Provider billed code 69990-59 along with reimbursed billed code 22554. Per NCCI Edit of
the pair code between these two states they are never to be billed together and a modifier is
not allowed to override the edit. As such, reimbursement of 69990 is not warranted.
Claims Administrator also denied code 76001-59, Fluoroscopy, physician or other
qualified health care professional time more than 1 hour, assisting a nonradiologic
physician or other qualified health care professional (eg, nephrostolithotomy, ERCP,
bronchoscopy, transbronchial biopsy)
Providers report submitted does not document 76001 and therefore, reimbursement is not
warranted for 76001.

63081, 63082-59 X 3, 22851-59 X 3,
69990-59, and 76001-59 Provider also billed 3 units of 22851-59,Application of intervertebral biomechanical device(s) (eg,
synthetic cage(s), methylmethacrylate) to vertebral defect or interspace (List separately in addition to
code for primary procedure)which is documented in the providers report.
Reimbursement of 22851 x 3 is warranted.
Provider also billed 63081, Vertebral corpectomy (vertebral body resection), partial or complete, anterior
approach with decompression of spinal cord and/or nerve root(s); cervical, single segment
Providers report documents A partial corpectomy had to be carried out before we were able to remove the
posterior osteophyte and decompress the spinal cord because of the very narrow disc space
Reimbursement of 63081 is warranted.
Provider documents �The same happened at C4-5 as well where partial corpectomy had to be carried
out as well�which supports billed code 63802, Vertebral corpectomy (vertebral body resection), partial
or complete, anterior approach with decompression of spinal cord and/or nerve root(s); cervical, each
additional segment (List separately in
addition to code for primary procedure) for 1 unit.
•


CPT 97750, ANALYSIS AND FINDING
Based on review of the case file the following is noted: ISSUE IN DISPUTE: Provider is dissatisfied with denial of CPT 97750, Physical
performance test or measurement (eg, musculoskeletal, functional capacity), with written report, each 15 minutes
EOR does not indicate 97750 as unauthorized but does state No separate payment was made because the value of the service is included within the value of another service performed on the same day
EOR s received only show CPT code 97750 billed along with CMS 1500 form billing only 97750.
Provider s report submitted documents 2 hours spent face to face and 60 minutes of report preparation
Opportunity to Dispute sent to Claims Administrator 08/12/2015; response not yet received
Based on the aforementioned documentation and guidelines, additional reimbursement is warranted for 97750 x12
Provider states a 10% PPO discount is to be applied to reimbursement


97670 “Functional Capacity Evaluation ” No Value 99499 at Customary Charges $1,687.50 /2nd
$2,375.00
Claims Administrator denied code indicating on the Explanation of Review “The Official Medical Fee
Schedule does not list this code(97670). No payment is being made at this time. Please resubmit your
claim with the OMFS codes that best describe the service(s) provided and your supporting
documentation”
Report Entitled “Functional Capacity Evaluation” reflects date of service 1/19/2015 OMFS allows for
Unlisted Procedure Codes to be reimbursed by “By Report.”
§9789.12.4 (c) “In determining the value of a By Report procedure, consideration may be given to the
value assigned to a comparable procedure or analogous code. The comparable procedure or analogous
code should reflect similar amount of resources, such as practice expense, time, complexity, expertise,
etc. as required for the procedure performed.”A code used in Functional Capacity Evaluation has been
99499.
There is no allowance or comparable code listed under the OMFS for service billed with procedure code
99499 or, more specifically, a Functional Capacity Evaluation;
Initial payments was zero allowed order for payments of billed charges in the amount of $1,687.50.
The correct billing code for a Functional Capacity Evaluation, 99499

97670 “Functional Capacity Evaluation ” No Value 99499 at Customary Charges $1,687.50 /2nd $2,375.00
ANALYSIS AND FINDING
Based on review of the case file the following is noted:
ISSUE IN DISPUTE: Provider dissatisfied with reimbursement of code 97799-86
Based on review of the Physician’s Initial Evaluation, procedure code 97799-86 is substantiated as the Provider
documented services performed and Provider’s Usual and Customary charge.
The Physician Evaluation details the injured worker’s medical history, current medications, physical examination
including functional strength, range of motion, function movement and lifting, dynamic posture and stabilization,
psychological evaluation, treatment plan and a formal request for authorization, a thorough evaluation was performed on
this injured worker
Claims Administrator based its reimbursement of 97799 86 on97670. The OMFS does not list an allowance for 97799 or
97670; these are described as “By Report” codes.
Documents reviewed included the Request for Authorization of Medical Treatment for an Initial Interdisciplinary
Evaluation documenting Provider’s cost at $2500.00.
Utilization Review Decision letter documented: Approved Initial Evaluation from 10/30/2013 –11/30/2013 Per the
supplied PPO contract, covered services billed with a procedure code for which there is no assigned value, Provider shall
be reimbursed at 95% of Eligible billed charge $ 2375.00

ANALYSIS AND FINDING
Based on review of the case file the following is noted: ·
ISSUE IN DISPUTE: Provider dissatisfied with reimbursement of code 97799-30·
Provider was reimbursed $471.81and is seeking additional reimbursement of $923.13.·
Claims Administrator sent a partial payment in the amount of $471.81 indicating on the Explanation of Review:
“The charge exceeds the official medical Fee Schedule allowance. The charge has been adjusted to the
scheduled allowance.” and “The Fee Schedule does not include a value for the procedure code billed. An
allowance has been made which is based on charges for similar/comparable services. Reimbursement is based
on the applicable reimbursement fee schedule.”
Claims Administrator does not state which code the 97799-30 is based on. ·
Included in this review is the Authorization Request –F.C.E. as a Panel QME, dated 4/8/2014 from the Provider.
The Request shows the CPT Request with Fee’s as 97799-30, Functional Capacity Evaluation/Unlisted Code, in
the amount $1395.00.
·
Claims Administrator sent Approved notification for Functional Capacity Evaluation dated April 17, 2014.
Instructions included “Services will be paid pursuant to the Official Medical Fee Schedule or an appropriate
PPO Contract” and the Authorization will expire in 60 Days
.
97799-30

97799-30
Physician’s Functional Capacity Evaluation report documents “Approximately 5 hours and 40 minutes of physical
testing, report preparation, research, calculations and editing were performed in the completion of this Functional
Capacity Evaluation.” Provider also states: “Completion of the intake forms, health-screening questionnaire, job demand
questionnaire, the history, interview and eMTAP required reading and writing, while sitting and took approximately 50
minutes to complete” as well as “The patient is slightly restricted upon standing for 90 minutes during the functional
capacity evaluation.”
·
The Provider documents the numerous tests performed on this patient including strength test, sitting and standing
tolerance, aerobic step test, hand functional tests, manual muscle testing of the upper and lower extremity, tendon
reflexes, abnormal sensation, lifting capacity and carrying test, pushing and pulling, activities of daily living, fine motor
dexterity, cool down and activity log, functional capacity assessment and the Physician’s Permanent and
Stationary Report.
·
CPT code 97799 is an unlisted code the Provider billed at $1395.00. Claims Administrator reimbursed a partial payment
of $ 471.81 but failed to report what this figure was based on. Therefore, CPT code 97750, Physical Performance Test or
Measurement (egMusculoskeletal, Functional Capacity) with written report, each 15 minutes best describes the procedure
demonstrated and will replace the 97799-30 billed by the Provider.
·
CPT 97750 is listed on the Official Medical Fee Schedule at $38.34/unit and the provider spent a total of 340 minutes or
23 units. 38.34 x 23 = 881.82, this will be the appropriate Official Medical Fee to use on this review


OUTPATIENT FUNCTIONAL CAPACITY
EVALUATION (FCE):Overturned
Claims Administrator guideline: Decision based on MTUS Chronic Pain Treatment Guidelines.
MAXIMUS guideline: Decision based on MTUS ACOEM Chapter 5 Cornerstones of Disability Prevention and Management Page(s): 89-92. Decision based on Non-MTUS Citation Official
Disability Guidelines (ODG) Chapter Fitness for Duty Chapter, FCE.

ACOEM guidelines
Decision rationale: ACOEM guidelines indicate there is a functional assessment tool available
and that is a Functional Capacity Evaluation, however, it does not address the criteria. As such,
secondary guidelines were sought. Official Disability Guidelines indicates that a Functional
Capacity Evaluation is appropriate when a worker has had prior unsuccessful attempts to return
to work, has conflicting medical reports, the patient had an injury that required a detailed
exploration of a workers abilities, a worker is close to maximum medical improvement and/or
additional or secondary conditions have been clarified. However, the evaluation should not be
performed if the main purpose is to determine a worker's effort or compliance or the worker has
returned to work and an ergonomic assessment has not been arranged. The clinical
documentation submitted for review indicated the patient had prior unsuccessful attempts to
Return to work and was close to maximum medical improvement. Given the above, the request
for a Functional Capacity Evaluation is medically necessary

EPIDURAL INJECTION
The criteria for the use of epidural steroid injections are as follows:
1) Radiculopathy must be documented by physical examination and corroborated by imaging studies
and/orelectrodiagnostic testing.
2) Initially unresponsive to conservative treatment (exercises, physical methods, NSAIDs and muscle
relaxants).3) Injections should be performed using fluoroscopy (live x-ray) for guidance.
4) If used for diagnostic purposes, a maximum of two injections should be performed. A second block is
notrecommended if there is inadequate response to the first block. Diagnostic blocks should be at an
interval of at least one to two weeks between injections.
5) No more than two nerve root levels should be injected using transforaminal blocks.
6) No more than one interlaminar level should be injected at one session.
7) In the therapeutic phase, repeat blocks should be based on continued objective documented pain and
functional improvement, including at least 50% pain relief with associated reduction of medication use
for six to eight weeks, with a general recommendation of no more than 4 blocks per region per year.
(Manchikanti,2003) (CMS, 2004) (Boswell, 2007) 8) Current research does not support a "series-of-
three" injections in either the diagnostic or therapeutic phase.

Elements:
• unresponsiveness to conservative treatment.
• imaging studies
• clear clinical signs of radiculopathy and non-corroborative findings on imaging,
Additional Injections:
• Objective Functional Improvement from prior injections The ODG identifies documentation of at least 50-70% pain relief for six to eight weeks, with a general recommendation of no more than four blocks per region per year, as well as decreased need for pain medications, and functional response as criteria necessary to support the medical necessity of additional epidural steroid injections.
Common Mistakes
• lack of documentation indicating the injured worker had radiating pain with the straight leg raise.•
• lack of documentation of failure of conservative care.
• failed to indicate the laterality, as well as the level for the injection
• no indication for failed conservative trial for diagnoses of cervicalgia and cervical
• no imaging studies provided for review.
• no documentation of unresponsiveness to conservative treatment.
• no more than 2 joint levels are injected in one session is recommended
• no documentation of at least 50-70% pain relief for six to eight weeks following previous injection
Overturned Requests:
• Decision rationale: According to the medical records provided for review, the patient has radicular symptomatology and findings on examination and documented by previous electrodiagnostic studies as well as MRI. Her therapeutic options appear to be limited by external issues restricting the use of analgesics and she has been described as reaching maximal medical improvement. Her clinical picture qualifies her for the lumbar epidural procedure. Therefore the request for the Right Lumbar ransforaminal Epidural Steroid Injection at L5-S1 under fluoroscopy is deemed to be medically necessary and appropriate

Functional Restoration Programs
Functional Restoration Programs be based on comprehensive evaluation of the patient's functional capabilities and psychological overlay.
Functional Restoration Program. The MTUS guidelines page 49 recommends functional restoration programs and indicate it may be considered medically
necessary when all criteria are met including (1) adequate and thorough evaluation has been made (2) Previous methods of treating chronic pain have been unsuccessful (3) significant loss of ability to function independently resulting from
the chronic pain; (4) not a candidate for surgery or other treatments would clearly be (5) The patient exhibits motivation to change (6) Negative predictors of success above have been addressed.
Also, California Medical Treatment Utilization Schedule recommends that a Functional Restoration Program is appropriate for patients who have not
responded to previous chronic pain treatments and are unlikely to show any significant clinical improvement from further treatment.
California Medical Treatment Utilization Schedule recommends a functional restoration program for patients that have had an adequate and thorough baseline evaluation to support functional improvement throughout the program and documentation of willingness and a motivation to change

Common Errors
• Fails to provide any evidence that the patient has undergone a comprehensive psychological or physical evaluation to determine the patient's appropriateness for a Functional Restoration Program.
• Documentation submitted for review does not provide evidence that the patient has exhausted all lesser forms of conservative treatment and will not significantly improve as a result of further conservative treatments.
• Does not clearly identify a duration of treatment.
• The appropriateness of that treatment cannot be established
• The clinical documentation as it is submitted does not contain any evidence of the patient's motivation to change or a functional baseline assessment to assist in determining functional improvements related to the program.
• The clinical documentation submitted for review does not provide evidence that treatment beyond the recommended 20 sessions is necessary
• It is not clear whether the patient is a candidate for surgery or other treatment, whether he had exhibited motivation to change, and whether negative predictors of success have been addressed.
• Request for six weeks of treatment in a functional restoration program is not supported as the patient does not meet all of the criteria and the request for treatment for 6 weeks exceeds the guideline recommendations
• Negative predictors of success have not been addressed
• There are no exceptional factors noted within the documentation to support extending treatment beyond guideline recommendations.


96101 and 99354
ANALYSIS AND FINDING
Based on review of the case file the following is noted:
·
ISSUE IN DISPUTE:
Provider seeking full remuneration 96101, Psychological Testing Per Hour, 99354 Prolonged service in the office or
other outpatient setting requiring direct patient contact beyond the usual service; first hour performed on 05/09/2014.
Claims Administrator $0.00 Reimbursement Rational based on “NCCI Edits.”
·
Pursuant Title 8 CCR Physician Fee Schedule 1/1/2014, § 9789.12.13 Correct Coding Initiative: (a) The National Correct
Coding Initiative Edits (“NCCI”) adopted by the CMS shall apply to payments for medical services under the Physician
Fee Schedule. Except where payment ground rules differ from the Medicare ground rules, claims administrators shall
apply the NCCI physician coding edits and medically unlikely edits to bills to determine appropriate payment. Claims
Administrators shall utilize the National Correct Coding Initiative Coding Policy Manual for Medicare Services. If a
billing is reduced or denied reimbursement because of application of the NCCI, the claims administrator must notify the
physician or qualified non-physician practitioner of the basis for the denial, including the fact that the determination was
made in accordance with the NCCI.

96101 x 7 units, 99354 X 1 UNIT.
CMS 1500 form reflects 96101 x 7 units, 99354 X 1 UNIT.
CMS 1500 reflects multiple services, including 99205.
EOR reflects Provider reimbursed for 99204.
Based on the NCCI edits code pair exist between CPT 99205/99204 and 96101.
Modifier Indicator column shows ‘1’ which states if a proper modifier is appended to the correct code and documentation supports the use of the procedure code then the edit may be overridden.
Article 5.5.0. Rules For Medical Treatment Billing and Payment §9792.5.7. Requesting Independent Bill Review (b)(2) The proper selection of an analogous code or formula based on a fee schedule adopted by the Administrative Director, or, if applicable, a contract for reimbursement rates under Labor Code section 5307.11, unless the fee schedule or contract allows for such analogous coding.
The correct modifier (-59) was not appended to the column 2 codes: 96118. As such, reimbursement is not indicated.
Page 59 of the Phsychological report indicates “15” minutes reviewing medical file.” Breakdown of total visit time –vs-psychological testing, could not be abstracted from report. CPT 99204, reimbursed by the Claims Administrator, has a time factor or 45 min.
Billed Prolonged Services Code, 99354 is a “per hour code” and is not factored into the visit time until, at the very least, an additional 45 minutes have surpassed the time involved with the Evaluation and Management service.
·
Based on the aforementioned documentation and guidelines, additional reimbursement is not indicated for 96101 and 99354
