884354 torahammar inlaga v4 - diva...
TRANSCRIPT

eMedication
– improving medication management using information technology


Linnaeus University Dissertations
No 188/2014
eMEDICATION
– improving medication management using information technology
TORA HAMMAR
LINNAEUS UNIVERSITY PRESS

eMedication – improving medication management using information technology. Doctoral dissertation, Department of Medicine and Optometry, Linnaeus University, Kalmar, Sweden, 2014 ISBN: 978-91-87925-15-3 Published by: Linnaeus University Press, SE-351 95 Växjö, SWEDEN Printed by: Elanders Sverige AB, 2014

Abstract Hammar, Tora (2014). eMedication – improving medication management using information technology. Linnaeus University Dissertations No 188/2014. ISBN: 978-91-87925-15-3. Written in English. Medication is an essential part of health care and enables the prevention and treatment of many conditions. However, medication errors and drug-related problems (DRP) are frequent and cause suffering for patients and substantial costs for society. eMedication, defined as information technology (IT) in the medication management process, has the potential to increase quality, efficiency and safety but can also cause new problems and risks.
In this thesis, we have studied the employment of IT in different steps of the medication management process with a focus on the user's perspective. Sweden is one of the leading countries when it comes to ePrescribing, i.e. prescriptions transferred and stored electronically. We found that ePrescribing is well accepted and appreciated by pharmacists (Study I) and patients (Study II), but that there was a need for improvement in several aspects. When the pharmacy market in Sweden was re-regulated, four new dispensing systems were developed and implemented. Soon after the implementation, we found weaknesses related to reliability, functionality, and usability, which could affect patient safety (Study III). In the last decade, several county councils in Sweden have implemented shared medication lists within the respective region. We found that physicians perceived that a regionally shared medication list generally was more complete but often not accurate (Study IV). Electronic expert support (EES) is a decision support system which analyses patients´ electronically-stored prescriptions in order to detect potential DRP, i.e. drug-drug interactions, therapy duplication, high dose, and inappropriate drugs for geriatric or pediatric patients. We found that EES detected potential DRP in most patients with multi-dose drug dispensing in Sweden (Study V), and that the majority of alerts were regarded as clinically relevant (Study VI).
For an improved eMedication, we need a holistic approach that combines technology, users, and organization in implementation and evaluation. The thesis suggests a need for improved sharing of information and support for decision making, coordination, and education, as well as clarification of responsibilities among involved actors in order to employ appropriate IT. We suggest collaborative strategic work and that the relevant authorities establish guidelines and requirements for IT in the medication management process. Keywords: eMedication, eHealth, medication, ePrescribing, electronic prescribing, information technology, drug-related problems, clinical decision support system, health care, pharmacy, patient


To my family
1

2

LIST OF PAPERS
I. Swedish pharmacists value ePrescribing: a survey of a nationwide
implementation. Hammar T, Nyström S, Petersson G, Rydberg T, Åstrand B.
Journal of Pharmaceutical Health Services Research. 2010; 1(1): 23-32
II. Patients satisfied with e-prescribing in Sweden: a survey of a nationwide implementation. Hammar T, Nyström S, Petersson G, Åstrand B, Rydberg T.
Journal of Pharmaceutical Health Services Research. 2011; 2(2): 97-105
III. Implementation of information systems at pharmacies – a case study from the re-regulated pharmacy market in Sweden. Hammar T, Hanson E, Ohlson M, Petersson G.
Research in Social and Administrative Pharmacy. Published online: 11 August 2014
IV. Implementation of a shared medication list - physicians' views on availability, accuracy and confidentiality. Hammar T, Ekedahl A, Petersson G.
International Journal of Clinical Pharmacy. Published online: 6 September 2014.
V. Potential drug related problems detected by electronic expert support system in patients with multi-dose drug dispensing. Hammar T, Hovstadius B, Lidström B, Petersson G, Eiermann B.
International Journal of Clinical Pharmacy. Published online: 29 June 2014.
VI. Physicians’ views on electronic expert support system: perceived benefits and clinical relevance of the alerts. Hammar T, Lidström B, Petersson G, Gustavsson Y, Eiermann B. Manuscript.
The published papers are reprinted with the permission of the copyright holders.
3

TABLE OF CONTENTS
List of papers ............................................................................................................................. 3 Table of contents ....................................................................................................................... 4 Populärvetenskaplig sammanfattning ........................................................................................ 7 Abbreviations ............................................................................................................................ 9 Introduction ............................................................................................................................ 10
Medication ........................................................................................................................ 10 The medication management process ......................................................................... 11 Drug-related problems and medication errors ............................................................ 11 Medication amongst older people and other frail patient groups ............................... 12 Actors and information in the medication management process ................................ 13 Strategies for improving medication appropriateness ................................................. 14
eMedication - IT in the medication process ..................................................................... 15 ePrescribing ................................................................................................................ 16 Electronic health record (EHR) ................................................................................. 17 Dispensing systems at pharmacies .............................................................................. 19 Clinical decision support systems (CDSS) ................................................................. 19 Other health IT in the medication management process ........................................... 21 Sources of information on medication ........................................................................ 22
Weaknesses and challenges with eMedication .................................................................. 24 Technology aspects, information security and continuity ........................................... 24 Social aspects and usability ......................................................................................... 25 Organizational aspects – and regulation ..................................................................... 25 Evaluation of eMedication .......................................................................................... 26
Aim ......................................................................................................................................... 27 Methods .................................................................................................................................. 28
Setting ............................................................................................................................... 28 Study design and data collection ....................................................................................... 29
Questionnaire ............................................................................................................. 29 Interviews .................................................................................................................... 30 Register study ............................................................................................................. 30
4

Outcome assessment and analysis ..................................................................................... 30 Quantitative analysis .................................................................................................. 30 Qualitative analysis ..................................................................................................... 30
Ethical approval ................................................................................................................ 31 Results .................................................................................................................................... 32
Study I: Pharmacists´ perceptions of ePrescribing ............................................................ 32 Study II: Patients´ perceptions of ePrescribing................................................................. 33 Study III: Implementation of dispensing systems at pharmacies ...................................... 34 Study IV: Physicians' perceptions of a shared medication list .......................................... 35 Study V: Potential DRP detected by EES ....................................................................... 36 Study VI: Physicians’ perceptions of EES alerts ............................................................... 37
Discussion ............................................................................................................................... 38 ePrescribing - pros and cons ............................................................................................ 38 Implementation of new dispensing systems...................................................................... 39 Shared information - and medication list ......................................................................... 40 Decision support systems are important but must mature ................................................ 41 Multi-dose drug dispensing .............................................................................................. 42 Prevention of DRP requires responsibility and collaboration ........................................... 43 Risks with novel technology and poor usability ................................................................ 45 Information security, continuity, and information structure ............................................ 46 Quality assurance of eMedication ..................................................................................... 46 Methodological considerations ......................................................................................... 47
Strengths and weaknesses with study design .............................................................. 47 Limitations ................................................................................................................. 48 General challenges when evaluating eMedication ...................................................... 49
Implications, recommendations, and future research ....................................................... 49 Recommendations for improved eMedication in Sweden .......................................... 50 Future studies ............................................................................................................. 51
Conclusions ............................................................................................................................ 52 Acknowledgements ................................................................................................................. 53 References ............................................................................................................................... 56
5


POPULÄRVETENSKAPLIG SAMMANFATTNING
eMedicinering
– IT-stöd i läkemedelsprocessen
Läkemedel förbättrar och förlänger livet för många och utgör en väsentlig del av dagens hälso- och sjukvård
men om läkemedel tas i fel dos eller kombineras felaktigt med varandra kan behandlingen leda till en försämrad
livskvalitet, sjukhusinläggningar och dödsfall. En del av dessa problem skulle kunna förebyggas med rätt
information till rätt person vid rätt tidpunkt och i rätt form. Informationsteknik i läkemedelsprocessen har
potentialen att öka kvalitet, effektivitet och säkerhet genom att göra information tillgänglig och användbar men
kan också innebära problem och risker. Det är dock en stor utmaning att i läkemedelsprocessen föra in effektiva
och användbara IT-system som stödjer och inte stör personalen inom sjukvård och på apotek, skyddar den
känsliga informationen för obehöriga och dessutom fungerar tillsammans med andra system. Dagens IT-stöd i
läkemedelsprocessen är otillräckliga. Till exempel saknar läkare, farmaceuter och patienter ofta tillgång på
fullständig och korrekt information om en patients aktuella läkemedel; det händer att fel läkemedel blir
utskrivet eller expedierat på apotek; och bristande eller långsamma system skapar frustration hos användarna.
Dessutom är det flera delar av läkemedelsprocessen som fortfarande är pappersbaserade. Därför är det viktigt
att utvärdera IT-system i läkemedelsprocessen.
Vi har studerat IT i olika delar av läkemedelsprocessen, före eller efter införandet, framför allt utifrån
användarnas perspektiv. Sverige har lång erfarenhet och tillhör de ledande länderna i världen när det gäller
eRecept, det vill säga recept som skickas och lagras elektroniskt. I två studier fann vi att eRecept är väl
accepterat och uppskattat av farmaceuter (Studie I) och patienter (Studie II), men att det finns behov av
förbättringar. När apoteksmarknaden omreglerades 2009 infördes fyra nya receptexpeditionssystem på
apoteken. Vi fann att det efter införandet uppstod problem med användbarhet, tillförlitlighet och funktionalitet
som kan ha inneburit en risk för patientsäkerheten (Studie III). I Sverige har man inom flera sjukvårdsregioner
infört gemensamma elektroniska läkemedelslistor. I en av studierna kunde vi visa att detta har inneburit en
ökad tillgänglighet av information, men att en gemensam lista inte alltid blir mer korrekt och kan innebära en
ökad risk att känslig information nås av obehöriga (Studie IV).
7

I två av studierna undersöktes beslutsstödssystemet elektroniskt expertstöd (EES):s potential som stöd för
läkare att upptäcka läkemedelsrelaterade problem till exempel om en patient har två olika läkemedel som inte
passar ihop, eller ett läkemedel som kanske är olämpligt för en äldre person. Studierna visade att EES gav
signaler för potentiella problem hos de flesta patienter med dosdispenserade läkemedel i Sverige (Studie V), och
läkarna ansåg att majoriteten av signalerna är kliniskt relevanta och att några av signalerna kan leda till
förändringar i läkemedelsbehandlingen (Studie VI).
Sammantaget visar avhandlingen att IT-stöd har blivit en naturlig och nödvändig del i läkemedelsprocessen i
Sverige men att flera problem är olösta. Vi fann svagheter med användbarhet, tillförlitlighet och funktionalitet i
de använda IT-systemen. Patienterna är inte tillräckligt informerade och delaktiga i sin läkemedelsbehandling.
Läkare och farmaceuter saknar fullständig och korrekt information om patienters läkemedel, och de har i
dagsläget inte tillräckliga beslutsstöd för att förebygga läkemedelsrelaterade problem. Eftersom
läkemedelsprocessen är komplex med många aspekter som påverkar utfall behöver vi ett helhetstänkande när vi
planerar, utvecklar, implementerar och utvärderar IT-lösningar där vi väger in både tekniska, sociala och
organisatoriska aspekter. Avhandlingens resultat visar på ett behov av ökad koordination och utbildning samt
förtydligande av ansvaret för inblandade aktörer. Vi föreslår gemensamt strategiskt arbete och att inblandade
myndigheter tar fram vägledning och krav för IT i läkemedelsprocessen.
8

ABBREVIATIONS
ADE – adverse drug event
ADR – adverse drug reaction
CDSS – clinical decision support system
CPOE – computerized prescriber order entry
DRP – drug-related problems
EES – electronic expert support
EHR – electronic health record
IT – information technology
MDDD – multi-dose drug dispensing
NEF – national ePrescription format
OTC – over-the-counter
PIP – potentially inappropriate prescription
SIL – Swedish information database for medications
9
INTRODUCTION
Medication is an essential part of health care and the appropriate treatment with drugs enables the cure and
prevention of many conditions [1]. However, drug-related problems (DRP) are frequent and cause suffering for
patients, and substantial costs for society [2-4]. Some of these problems could be prevented with the right
information to the right person at the right time and in the right form [5, 6]. There are many expectations and
hopes that the employment of information technology (IT) and eHealth will solve many health care problems
and improve health [7-9]. The EU has launched a number of calls within Horizon 2020 to promote eHealth
[10]. In Sweden, there is a national strategy for eHealth and medication, respectively [11, 12]. In the different
steps of the medication management process, IT has the potential to increase efficiency and safety by making
information accessible and useful, but IT can also cause new problems and risks [9, 13-16]. It is a major
challenge to implement appropriate IT that supports, not interferes with, professionals in healthcare and
pharmacies, protects sensitive information from unauthorized access, and is interoperable with other existing
systems [7, 17, 18]. Therefore, evaluation of IT in the medication management process is important [14, 19].
Medication The word medication can describe both an act and an item. In this thesis, medication is used to describe the act
of treatment with or utilization of drugs in medicine, while the words medications and drugs are used
interchangeably to describe the substance used in the treatment. Prescribing of drugs is the most frequent and
cost-effective medical intervention performed by physicians and can prevent or cure many diseases, and increase
quality of life [20, 21]. Drugs are used in all age groups but the use is related to morbidity, age, gender, and
socioeconomic factors [22-24]. Prescription drugs represent the vast majority of all drugs being used, but drugs
are also administered in hospitals, and sold as over-the-counter (OTC) drugs, dietary supplements, or
complementary and alternative medicine [25, 26]. Rational use of medications can be described as physicians
prescribing appropriate drugs to the patients according to the patients´ clinical needs, in doses that meet
individual requirements, for an adequate period of time, and at the lowest cost to patients and communities
[27]. The use of drugs and the proportion of people prescribed multiple drugs simultaneously have increased,
increasing the risk of DRP [24, 28-30].
10
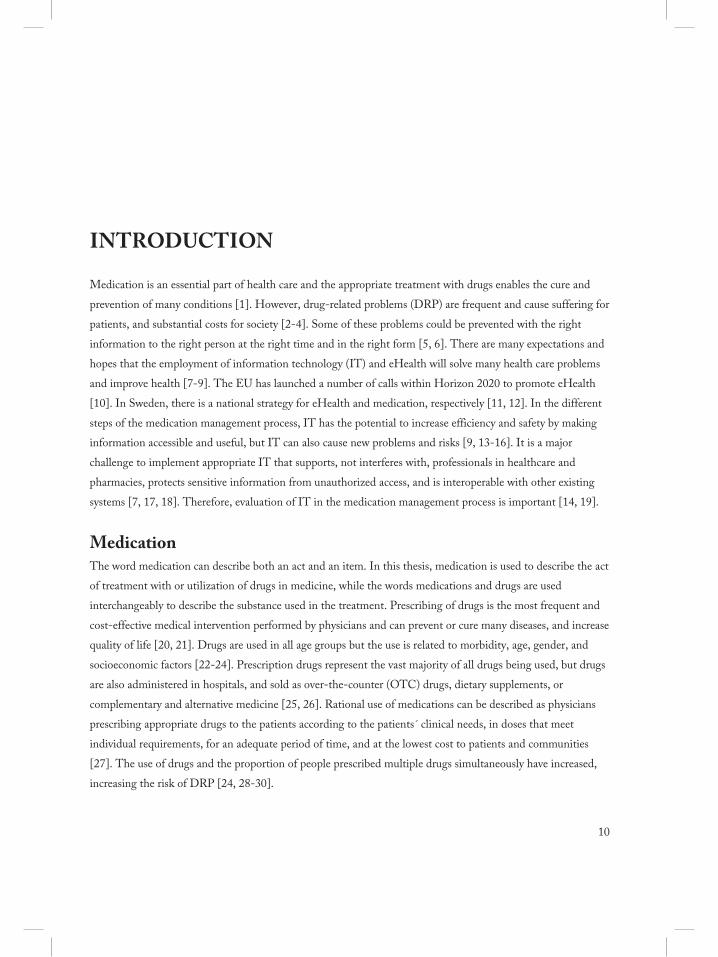
The medication management process Medication management is a complex process requiring communication and information sharing among many
actors, across different settings [1, 3, 21]. This complexity can lead to medication errors that may result in
DRP. The medication management process includes assessing and making decisions on medication,
prescribing, order communication, dispensing, administering and use, monitoring and evaluation of treatment
(Figure 1) [16, 31]. In outpatient health care, the medication management process differs from that within
hospitals since prescribed medications are primarily dispensed at community pharmacies [32]. In hospitals,
medications are often dispensed and administered by nurses from a local medical supply. If living at home, the
patient or a relative is responsible for medications being administered according to the prescription, or if living
in a nursing home, the patient’s medications are being handled by nurses or other health care personnel [33].
Monitoring and follow-up are important parts of medication, but sometimes insufficient [1].
Figure 1. The steps in the medication management process in primary and secondary care. In primary care, prescribed medications are
primarily dispensed at community pharmacies and administered either at home or at a nursing home. In secondary care, medications are
often dispensed and administered by nurses from a local medical supply.
Drug-related problems and medication errors DRP are events or circumstances that involves a patient’s drug treatment that actually, or potentially, interferes
with the achievement of an optimal outcome and may occur in any of the steps in the medication management
process [2, 34]. DRP are frequent and cause suffering for patients and substantial costs for society [35-38].
DRP are a common reason for hospital care and can even be fatal [4, 34, 36, 38-40]. A large portion of DRP
can be prevented [41-43]. There are a number of terms and concepts related to DRP, and partly overlapping, as
well as a variety of definitions for each term (Table 1) [2, 21]. DRP, the term primarily used in this thesis,
include adverse drug reactions (ADR), adverse drug events (ADE), medication errors, and potentially
inappropriate prescriptions (PIP), as well as other circumstances such as therapy failure, underuse of drug,
11

overuse of drug, contraindication, drug-drug- interaction, drug duplication, unmet need for additional
treatment, uncertainty about the aim of the drug, or other practical problems among other things [2, 34].
Medication errors are failures in the medication management process and may cause harm, but far from all
errors lead to patient harm [2, 6, 21]. In contrast, ADE, relate to actual harm and may be caused by errors but
often there is no error involved. Medication errors in health care can be caused by human factors, e.g. memory
lapses, action slips, knowledge and rule based mistakes or violations [44]. These actions can in turn be caused
by social or organizational factors, e.g. insufficient training and experience, poor communication, lack of
information, heavy workload, local working culture, or inadequate procedures.
Table 1. Descriptions of terms related to DRP.
Term Description
Drug-related problem (DRP) A circumstance that involves a patient’s drug treatment that actually, or potentially, interferes
with the achievement of an optimal outcome [2].
Medication error Any error in the process of prescribing, dispensing or administering a drug, whether there are
adverse consequences or not [2].
Adverse drug reaction (ADR) Any response to a drug which is noxious and unintended and which occurs at doses normally
used in humans for prophylaxis, diagnosis or therapy of disease, or for the modification of
physiological function [2, 4].
Adverse drug event (ADE) An injury related to the use of a drug [2, 4].
Potentially inappropriate
prescription (PIP)
Prescriptions in which risks outweigh benefits, especially used when assessing medication for
older people [45].
Medication amongst older people and other frail patient groups Increasing proportion of older people in the population and, in parallel, an increased lack of personnel and
resources are anticipated [1]. Drug treatment in the elderly is especially challenging due to an increased
prevalence of multi-morbidity, and changes in physiology, pharmacokinetics, and pharmacodynamics [1, 46].
In addition, many older people may have difficulties handling their medication due to cognitive impairment.
Medication in children is also challenging due to large variations in weight and metabolism in combination
with lack of knowledge and documentation concerning efficacy and safety of many medications [47].
Multi-dose drug dispensing (MDDD) is a service in which patients receive their medication machine-packed
into unit dose bags for each time of administration [48-51]. Patients with MDDD are often old, have several
diseases and many different medications. MDDD has been suggested to reduce medication errors, increase
drug adherence, and decrease waste of unused drugs [51, 52]. However, a high prevalence of potential DRP, a
lower quality of drug treatment than for other patients, an increased number of drugs after a patient’s transition
to MDDD, and fewer changes in drug treatment have been found among patients with MDDD [29, 48-50,
53].
12

Actors and information in the medication management process There are several actors in the medication management process: patients, physicians, pharmacists, nurses, other
health care professionals, relatives and carers, as well as health care providers, non-governmental organizations,
and authorities (Figure 2) [16, 17]. From a legal point of view, physicians are responsible for the prescribed
medication being appropriate in relation to the patient’s entire medication [54]. However, physicians have
various opinions concerning their responsibility for performing medication reconciliation, providing an accurate
medication list, or reviewing whether the treatment is appropriate [55-58]. Pharmacists are primarily involved
in medication management during the dispensing of medications where they often are the last health care
provider the patient encounters before using (or not using) a medication. At community pharmacies,
pharmacists are responsible for safe dispensing of prescription drugs, and examine prescriptions before
dispensing. Pharmacists’ modification of prescription errors has been shown to be of clinical value [59-63].
Clinical pharmacists are increasingly included in the health care team, and their interventions has been shown
to be of clinical value [64].
Figure 2. Actors’ exchange of information in the medication management process: e.g. patients’ current medication, patient specific
parameters, reimbursement and generic substitution, knowledge and instructions regarding medication, as well as regulation,
guidelines, and recommendations. Information exchange can be oral, paper based, or electronic.
13

One of the key components to achieving appropriate drug treatment is the access to the needed information for
the involved actors [5, 6, 65]. It has been estimated that half of the medication errors are associated with the
insufficient information on the patient and/or drug [5]. Information exchange between different actors can be
oral, paper based, or electronic. Physicians making decisions on treatment need patient specific information,
current medication list, and other patient specific information, e.g. age, weight, allergies, co-morbidities,
medical history, and other factors that may affect the pharmacokinetics of the drug such as renal and hepatic
function [66]. In addition, drug specific information, e.g. dosage information for certain age groups, indications
and contraindications, information about drug-drug interactions, and related guidelines are necessary to provide
optimal care. Pharmacists also need information on reimbursement and generic substitution. Patients, or
relatives/carers, need information on which drugs to use and how to use them. Health care organizations,
authorities, and non-governmental organizations request information for monitoring but also provide
information in form of e.g. regulation, guidelines, and recommendations. Information and knowledge need to
be continuously updated [5, 7-9, 14, 17]. Information overload can result in new knowledge not being adopted
into clinical practice [67]. Thus, information has to be presented and made accessible in a usable form.
Patient adherence to drug treatment is vital to reach the desired outcome. However, non-adherence to
treatment is common for various reasons such as ADR, lack of motivation or knowledge [1, 68]. Patients can
be more or less involved in decisions and handling of their medication, and are at times assisted by relatives
[69]. Patients are generally becoming increasingly engaged in their health care and this development is
supported by the growth of IT in society, e.g. a majority of Internet users search for health information on the
Internet [70-73]. The importance of patient centered care, empowering patients, and involving them in the
medication management process is becoming more and more prioritized. Informed and motivated patients are
more likely to continue using health care services, value and maintain relationships with health care providers,
comply with treatment, and take an active role in their own health care [74, 75].
Strategies for improving medication appropriateness The transition between different health care providers and settings is a known risk for DRP and medication
errors [1, 76]. An increased number of prescribers or dispensing pharmacies can also increase the risk of DRP
[1]. Consequently, medication reconciliation has been endorsed as a method of improving the accuracy of the
medication list. Medication reconciliation is the process of obtaining a complete and accurate list of all the
medications an individual is taking from different sources, and communicating that list to all the patient’s
health care encounters, and is recognized as a method for preventing medication errors [46, 57, 77-79].
However, this process is seldom straightforward and can often be time consuming depending on the accuracy
and availability of information sources.
14

To monitor the quality of prescribing, different measurements and indicators can be used. Since inappropriate
prescribing for older people has become an important public health issue, there are different approaches in
measuring and detecting inappropriate prescribing, and measuring quality of prescribing [46, 80, 81].
Many DRP can be avoided by different strategies such as evaluation of therapy, education of professionals or
patients, medication review, or other actions performed by clinical pharmacists joining the health care team [1,
3, 41, 43, 46, 82]. To increase safety and prevent errors, health care systems and processes should be designed
to make it harder for people to do something wrong and easier for them to do it right [5]. Since the medication
management process is complex and many actors are involved, there is a need for facilitating the information
handling in order to make it simpler and safer, reducing human errors, and if possible automatize some parts.
Here, there are many expectations associated with the opportunities to take advantage of modern IT in the
medication management process.
eMedication - IT in the medication process For an appropriate, safe, and efficient medication, there is a need for tools that can support professionals in
handling the information and making it available to the actors involved. eHealth has received increasing
attention in the past decade defined by the European Commission as:
eHealth is the use of IT in health products, services and processes combined with organizational change in healthcare systems and new
skills, in order to improve health of citizens, efficiency and productivity in healthcare delivery, and the economic and social value of
health. eHealth covers the interaction between patients and health-service providers, institution-to-institution transmission of data, or
peer-to-peer communication between patients and/or health professionals.
eMedication, in this thesis defined as IT in the medication management process, has been suggested to reduce
cost, improve efficiency, medication appropriateness, and safety by for example increasing legibility,
standardization, and availability of information, as well as reducing the need for manual re-entering of
information and providing automated checks for potential DRP [5, 7-9, 14, 16, 17, 83]. However, in contrast
to the large expectations and investments, the effects of IT in health care and the medication management
process are inconsistent, partly unidentified, and not always expected, and IT has even created new problems
[7, 13, 15, 84, 85].
During the last decades, the prescribing of medications and handling of information in the medication
management process have gone through a major transition from paper to electronic based [86, 87]. The
adaptation of the traditional process to the electronic era offers new opportunities as well as challenges for the
involved actors. Worldwide, there is a large variation in the degree to which IT is implemented in the
medication management process, some variation that can be explained in differences in the model of health
care delivery and insurance [88, 89]. Sweden has been one of the leading countries in the implementation of
ePrescribing and electronic documentation in health care, with the world’s first ePrescription being transmitted
15

in Sweden [32, 90]. However, IT has become widely used in health care in many other countries in the past
decade [89, 91-93].
In the eMedication process, IT is used in several steps, e.g. ordering and prescribing in health care, electronic
transfer and storing of prescriptions, processing and dispensing of prescriptions at pharmacies, accessing
information on a patient’s current prescriptions, and support for decision making and detection of potential
DRP. Terminology and description of the main IT involved in the thesis is found in Table 2 below.
Table 2. Involvement of IT in the different steps of the medication management process.
IT system Description
Electronic prescribing
(ePrescribing)
Electronic entering and transmission of prescriptions.
Alternative terminology: electronic prescribing, e-prescribing, eRx. (Note that ePrescribing in the
literature sometimes refers to stand-alone technology for entering and reviewing, but not transmitting
ePrescriptions [32].)
Electronic health record
(EHR)
A record of electronic health information about an individual patient or population.
Alternative terminology: The terms EHR, EPR (electronic patient record) and EMR (electronic
medical record) are often used interchangeably, although differences between them can be defined.
Computerized prescriber
order entry (CPOE)
Information systems that enable providers to prescribe medications.
Alternative terminology: Computerized physician order entry, medical order entry systems.
Dispensing system The information system used at pharmacies for processing and dispensing prescriptions.
Dispensing systems are often studied as a part of ePrescribing.
Alternative terminology: eDispensing, pharmacy computer system, pharmacy information system,
pharmacy computer software.
Clinical decision support
systems (CDSS)
Computer-based information systems used to integrate clinical and patient information and
provide support for decision-making in patient care.
Alternative terminology: Computerized clinical decision support systems, decision support.
ePrescribing ePrescribing is a broad term used to describe a variety of IT systems to support the prescribing process [32, 88].
Some make a distinction between first and second generation of ePrescribing. The first generation of
ePrescribing, implemented for example in the US, was stand-alone technology for electronic entering and
reviewing of prescriptions, but where prescriptions were printed and handed to the patient. The second
generation of ePrescribing includes the electronic transmission of prescriptions from the prescriber to the
pharmacy, either to a specific pharmacy (push model) or to a centralized repository (pull model) [32]. In this
thesis, ePrescribing refers primarily to the Swedish ePrescribing model including electronic entering and
transmission of a prescription from the prescriber to the pharmacy as well as electronic storing and handling of
prescriptions, i.e. second generation of ePrescribing with the pull model for electronic transmission (Figure 3).
16

A prescription, no matter the route of transfer, functions to communicate decisions on drug therapy from the
physician to the pharmacist dispensing the medication and should be unambiguous, correct, and complete [90].
The handwritten prescription has a number of well recognized weaknesses, including risk of misinterpretation
of poorly written prescriptions, unidirectional communication, and risk of falsification or patient losing the
prescription [94, 95]. ePrescribing has been proposed as an important tool to improve quality, safety, efficiency,
and cost-effectiveness in prescribing and dispensing processes [88, 90, 96]. Although some of the proposed
strengths with ePrescribing have been confirmed, weaknesses with paper prescriptions are not necessarily
solved, and ePrescribing may even create new errors [87, 97, 98]. The electronic handling of prescriptions in
health care and at pharmacies enables the use of computerized tools to assist physicians and pharmacists in
decision making and dispensing [6, 31].
In Sweden, ePrescribing has been used for more than three decades and has been the primary way of
prescribing in the last decade with more than 90% of prescriptions being electronic today [90]. In addition,
since 2005, it has been possible for patients to store their valid prescriptions electronically in the national
prescription repository [90, 94]. At the pharmacy, patients can choose to store their prescriptions electronically,
or to have their prescriptions in paper form. Patients can have their medication from electronically stored
prescriptions dispensed at any pharmacy with the presentation of valid identification, and prescriptions can also
be accessed via the Internet, by means of secure digital authentication. To increase the quality of ePrescriptions
and thereby patient safety, as well as facilitate future development of related services, a National ePrescription
Format (NEF) has been implemented. After a nationwide implementation in June 2009, NEF has introduced
more formal requirements with automated quality checks of all ePrescriptions, improving interoperability and
decreasing errors [99].
Electronic health record (EHR) An electronic health record (EHR) is used for documentation and information sharing in health care, often
also for support of clinical care and decision making, as well as patient administration functions. The
information system enabling electronic prescribing and order entry is often referred to as computerized
prescriber order entry (CPOE) system. In this thesis, EHR will be used to describe the information system
used for documentation as well as prescribing because the prescribing module in Sweden is a part of the EHR.
EHRs are almost completely implemented in all Swedish health care units in primary and secondary care [100,
101]. Each county council makes its own procurement of an EHR system. In the last decade, Sweden has
moved towards using region-wide EHR systems, i.e. EHR shared between care providers within the region.
Currently, the six most common EHRs have a market share of 95%. In addition to the EHR, a large number
of other electronic information systems are used to support the needs of health care providers.
17

Figure 3. Electronic handling of prescriptions in primary care in Sweden. Prescribers can prescribe a medication via a prescribing
module in the EHR system. The prescription is transferred to the national prescription repository, where it can be stored for several
iterations through the entire period of its validity. Prescribers can cancel their own prescriptions if their EHR system supports this
function, but they cannot view the patient’s prescriptions stored in the prescription repository. Prescribing for patients with MDDD is
managed in a separate system usually not linked to the EHR. From the prescription repository, the medication can be dispensed at any
Swedish pharmacy. Pharmacists can, upon request, view and dispense patients’ prescriptions via their dispensing system.
(EHR=electronic health record, MDDD=multi-dose drug dispensing)
18

Dispensing systems at pharmacies Pharmacists at community pharmacies play an important role in detecting prescription errors and preventing
DRP [33, 61, 102]. A pharmacy dispensing information system, referred to as a dispensing system in this
thesis, is a system used at pharmacies for processing and dispensing prescriptions. To dispense a prescription,
pharmacies in Sweden are obliged to use a dispensing system in order to handle all relevant information.
Dispensing systems are used as a support for almost all tasks performed to dispense prescriptions in outpatient
healthcare, e.g. accessing the electronic prescriptions in the prescription repository, managing reimbursement
for medications, and printing labels for medications. When the Swedish pharmacy market was re-regulated in
2009, Sweden moved from a one state-owned pharmacy chain to several private pharmacy companies, and four
new dispensing systems emerged to replace the system that had been used at all Swedish pharmacies for more
than 20 years [103].
Effective support from IT in pharmacies has the potential to facilitate safe dispensing and support pharmacists
[61, 62, 104-107]. However, there are few studies that have addressed the IT system supporting pharmacists
when dispensing medications at community pharmacies, most of them related to ePrescribing rather than the
dispensing system [16, 95, 104, 106, 108-110].
Clinical decision support systems (CDSS) Decision making in the medication management process most often refers to physicians making decisions
regarding new or current treatment, but some forms of decisions are made in every step of the process and
require a range of information [14]. Information and knowledge on medications can be made available in
different forms, paper based or electronic, and thus can be analyzed in different ways [111]. Information or
knowledge that is available in a structured electronic machine readable format may be processed and analyzed
automatically by a computer and thus can be utilized in a CDSS. Information and knowledge regarding
medications is continuously increasing and changing as new treatments emerge, or findings in research or
clinical practice change previous recommendations [111]. However, for a clinician making decisions regarding
medications on a daily basis, it is difficult or impossible to keep up with evolving knowledge and at the same
time keep in mind the latest recommendations according to guidelines or health economic estimations.
The rationale for CDSS is that characteristics of individual patients are matched with a computerized
knowledge base, and software algorithms generate patient specific recommendations or alerts [15, 84]. CDSS
in the medication management process are used to support decisions regarding medication, facilitate evidence
based medicine, reduce the incidence of DRP, and improve health care quality and efficiency [85, 112].
Nevertheless, clinicians will make the final decision; the system is merely assisting with a time efficient analysis
of a mass of information. The input of patient data can be automatic via integration of patient information
through e.g. an EHR, or require manual entry [85]. CDSS alerts can be delivered to the decision maker
through e.g. EHR, CPOE, dispensing systems, or a separate solution. There are different types of CDSS in
19

the medication management process; the basic principles are shown in Figure 4 below. A common type is a
system giving alerts if a potential DRP is detected in the current medication. There are also CDSS that can
provide dosing instructions, treatment recommendations, or detect the need for additional treatments
concerning a patient [112]. CDSS can have beneficial effects such as reduction in DRP, but results are varying
[7, 8, 13, 15, 112, 113]. Effects of CDSS can be related to factors such as its implementation, design, timing of
alerts, and clinical relevance of alerts as well as other social factors [114, 115].
Figure 4. Principles of clinical decision support systems (CDSS) in the medication management process. Information on patients’ current
medication can be derived from different sources. Patient specific information can include e.g. age, gender, weight, diagnoses, renal and
hepatic function. Drug information, knowledge and guidelines include for example recommended dosing related to different factors, drug-
drug interactions, contraindications, and inappropriate drugs for older people, children, pregnant or breast feeding women.
Current CDSS have various limitations in the different types of information included as well as how
information is processed and alerts are presented to the user [13, 66, 116]. Many alerts from CDSS are being
ignored; override rates ranging between 29-91%, with variation between different categories of alerts [117-
120]. Designing an appropriate CDSS is a major challenge and an insufficient CDSS can actually do more
harm than good [111, 121]. Weaknesses with current CDSS are that the systems often do not have access to an
accurate and complete list of patients’ medications, that the CDSS lacks important patient specific information
such as renal function or weight or that this information is out of date or has to be entered manually by the
20

physician, or limitations in the knowledge base and algorithms. This can result in both problems that are
missed or that the CDSS gives rise to an excessive amount of alerts, that may disturb the clinician rather than
support him/her. Alert fatigue can be described as an excessive amount of alerts that decreases clinicians’
attention of the alerts and may result in alert override and thus the risk of important alerts being missed among
the clinically less relevant alerts [114]. Other risks with CDSS are that they might diminish medical judgment,
cause disturbances in clinical workflow or introduce new errors [111, 122].
In Sweden, most of the EHR systems have CDSS implemented in various ways. Some of the knowledge bases
within the CDSS are provided through a national database containing medication information, called SIL
(Svensk informationsdatabas för läkemedel) [123]. The knowledge bases included in SIL can also be reached
online or integrated in other systems. The decision support system include recommendations from the regional
drug and therapeutics committee, knowledge bases for drug-drug interactions (SFINX), drugs contraindicated
in elderly, drugs during pregnancy or breast-feeding (alert for female age 13-55 years) [111, 124, 125].
Additionally, some health care providers have implemented a knowledge base providing information on drug
use related to renal function (NjuRen) [126], or a CDSS for pediatric medication (ePed) or other
recommendations regarding drug treatment. There are also other separate systems supporting decision making
in the medication management process, such as miniQ.
The Electronic Expert Support (EES) system is a CDSS developed by Medco Health Solutions, USA, and
adapted to Swedish clinical practice, and managed by the eHealth Agency. EES analyzes patients´
electronically stored prescriptions to detect DRP, including drug-drug interactions, therapy duplication, high
dose, drug-disease contraindication, drug gender warning, and inappropriate drugs for geriatric or pediatric
patients [127, 128]. EES is primarily intended for pharmacies where alerts can be viewed, with patient consent,
by the pharmacists through a function in the information system used for dispensing prescriptions. EES is
available at most Swedish pharmacies (>90%), but is currently used only in a relatively small proportion of
patients. The potential value of EES alerts for physicians in health care is under discussion.
Other health IT in the medication management process In addition to the technologies described above, other forms of IT can support various parts in the medication
management process such as barcode medication administering, and medication cabinets for administration of
medications, at hospitals, nursing homes or at home [6, 129].
As a part of patient centered care and empowerment, there are different forms of support for patients taking an
active part in their medication, e.g. applications for adherence and learning. In addition, patients can access
different types of personal health information, such as their health record (so far to various extents) or
prescription history [130-132]. The Internet has provided new ways of communication between patients and
health care providers [70-72, 133, 134].
21

Sources of information on medication Different sources of information of patients’ medications are available in different settings. There may be
information in health records or registers of prescribed or dispensed medications locally, regionally, or
nationally. It is vital that information on the patient’s current ongoing medication is available and accurate for
the patients as well as all health care professionals [8, 55, 79, 83, 135, 136]. However, health care professionals
often lack accurate information, and discrepancies occur frequently and can be particularly problematic with
patients with multiple medications, older patients, and the transfer of patients between different health care
settings [33, 77, 78, 137, 138]. Inaccurate or unavailable medication lists/records may result in medication
errors such as inappropriate prescribing (e.g. drug-drug interactions or duplicate therapy), or wrong
medications being administered at hospitals, nursing homes, or taken at home [44, 139]. Physicians’
unawareness of patients’ co-medication has been described as an important cause of medication errors [33].
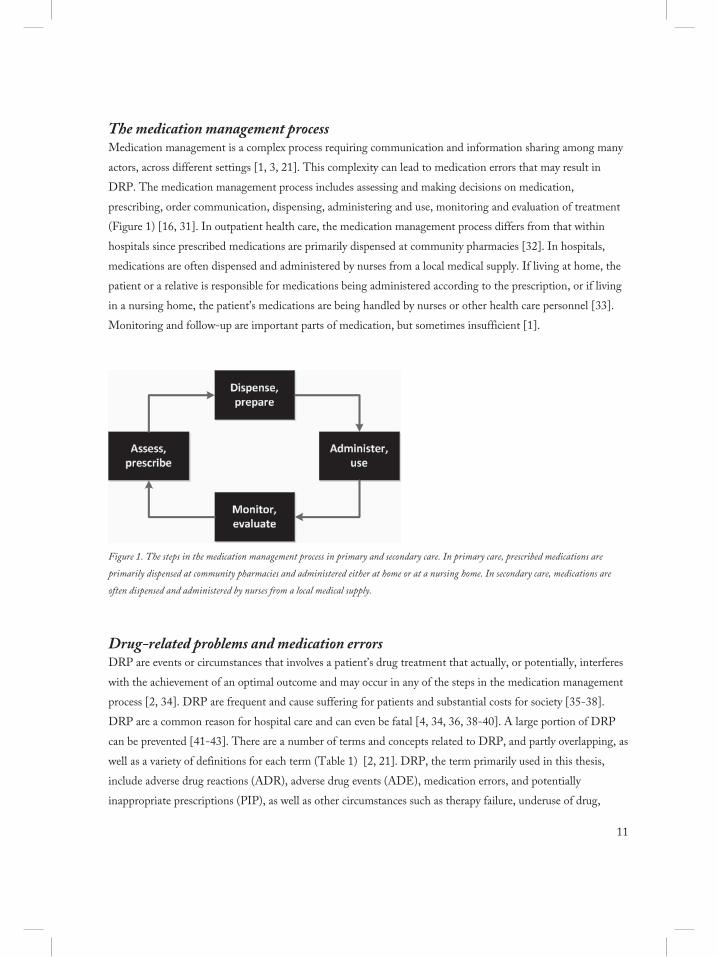
In Sweden, there are several different sources of information on a patient’s medication (Table 3). The different
sources on patients’ medications are often incorrect and rarely correspond to each other or with the patient’s
current ongoing medication [140, 141]. In the EHR, a specific prescribing module includes a medication list as
well as an inpatient drug list [100]. During the past decade, by sharing an EHR system, three quarters of all
counties in Sweden have implemented shared medication lists for their county council managed health care
(hospital, psychiatry, primary care), sometimes including private health care providers as well [76]. There is no
automatic transfer of information on patients’ medications between EHRs in different counties. Dispensing
pharmacists and patients have access to the national prescription repository, including all electronically stored
prescriptions in Sweden, which covers approximately 90% of all prescriptions (the remaining 10% being paper
prescriptions). At pharmacies, prescriptions are dispensed from this prescription repository. Due to legal
reasons for the protection of patient privacy, physicians are not allowed access to the prescription repository.
Prescriptions for patients with MDDD [49, 51] are separated from ordinary prescriptions (although stored in the
national prescription repository) and primarily handled using a different tool in a separate system and
information is usually not automatically transferred to the medication list in the EHR. In addition, the national
pharmacy register is a historic register for patients’ dispensed prescriptions during the past 15 months available
for patients or health care professionals with patient consent [73]. There are registers for research and statistics;
the national prescribed drug register automatically includes data at an individual level for all prescription
medications dispensed [142]. There is ongoing work to plan and prepare the implementation of a nationally
shared medication list in Sweden (NOD, Nationell Ordinationsdatabas) [143].
Different solutions for sharing or reconciling medication information electronically between providers have
been implemented or piloted or are planned worldwide [65, 79, 89, 92, 135, 136, 144-146]. Although a shared
medication list is often referred to as a path to provide safer medication by providing an accurate and complete
list of patients’ medications, the consequences of a transition from a local to a shared medication list are unclear
and depending on several aspects.
22
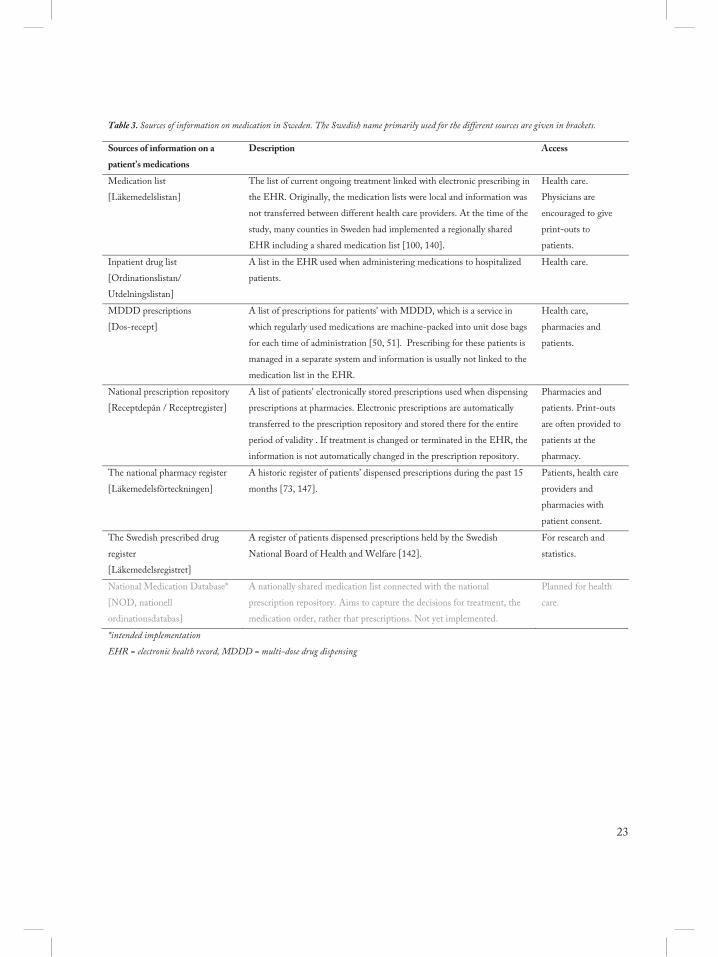
Table 3. Sources of information on medication in Sweden. The Swedish name primarily used for the different sources are given in brackets.
Sources of information on a
patient’s medications
Description Access
Medication list
[Läkemedelslistan]
The list of current ongoing treatment linked with electronic prescribing in
the EHR. Originally, the medication lists were local and information was
not transferred between different health care providers. At the time of the
study, many counties in Sweden had implemented a regionally shared
EHR including a shared medication list [100, 140].
Health care.
Physicians are
encouraged to give
print-outs to
patients.
Inpatient drug list
[Ordinationslistan/
Utdelningslistan]
A list in the EHR used when administering medications to hospitalized
patients.
Health care.
MDDD prescriptions
[Dos-recept]
A list of prescriptions for patients' with MDDD, which is a service in
which regularly used medications are machine-packed into unit dose bags
for each time of administration [50, 51]. Prescribing for these patients is
managed in a separate system and information is usually not linked to the
medication list in the EHR.
Health care,
pharmacies and
patients.
National prescription repository
[Receptdepån / Receptregister]
A list of patients' electronically stored prescriptions used when dispensing
prescriptions at pharmacies. Electronic prescriptions are automatically
transferred to the prescription repository and stored there for the entire
period of validity . If treatment is changed or terminated in the EHR, the
information is not automatically changed in the prescription repository.
Pharmacies and
patients. Print-outs
are often provided to
patients at the
pharmacy.
The national pharmacy register
[Läkemedelsförteckningen]
A historic register of patients’ dispensed prescriptions during the past 15
months [73, 147].
Patients, health care
providers and
pharmacies with
patient consent.
The Swedish prescribed drug
register
[Läkemedelsregistret]
A register of patients dispensed prescriptions held by the Swedish
National Board of Health and Welfare [142].
For research and
statistics.
National Medication Database*
[NOD, nationell
ordinationsdatabas]
A nationally shared medication list connected with the national
prescription repository. Aims to capture the decisions for treatment, the
medication order, rather that prescriptions. Not yet implemented.
Planned for health
care.
*intended implementation
EHR = electronic health record, MDDD = multi-dose drug dispensing
23

Weaknesses and challenges with eMedication Despite decades of experience and world-wide recognition of the potential benefits of IT in the medication
management process, we are still struggling with major problems in the medication management process, and
IT systems does not meet the expectations of efficiency and safety [14, 101]. Medication errors remain and new
types of errors are revealed [5, 83, 148]. There are issues with information security [149]. IT-related incidents
are reported in health care [150]. The actors in the medication management process still lack vital information
or describe an information overload [67]. Knowledge and evidence is disseminated into clinical practice in an
incomplete manner [1, 84]. There are frequent reports of health care professionals being unsatisfied and
frustrated with the system they are using [17, 151]. There are recurrent reports of IT systems in health care not
being successfully implemented, failing to meet expectations, or even being cancelled during implementation
[14, 17]. The weaknesses and challenges with eMedication involve technology, social, organizational or wider
political aspects, respectively.
Technology aspects, information security and continuity Robust technology is a necessity and an enabler of a safe and efficient handling of information in the
medication management process but reliability and stability of a system are affected by limitations in technical
infrastructure [17, 152]. Communication and linkage between different systems are limited by the lack of
technical interoperability as well as a common information structure [152]. The need for a common, structured
documentation as well as requirements for basic interoperability have been mentioned in several national
strategies and government documents [11, 152].
To ensure sufficient patient safety in today’s health care, it is necessary that information follows the patient
across providers, settings, and regional borders. A major challenge is the balancing of increased information
sharing and availability on the one hand and the protection of patient integrity on the other hand. In Sweden,
information exchange in health care is restricted in several ways due to legal reasons in order to protect patient
privacy. The appropriateness of the legislation regarding handling of information in health care and data
protection is under review by the Swedish government in order to identify any need for changes [153]. Mutual
trust between the staff and patient is crucial to achieve patient safety and assumes proper protection of patient
integrity; thus, management of information security in health care is essential [149, 154]. Patient safety is
maintained by information availability and accuracy, whereas patient integrity is maintained by confidentiality
of information [155].
There are risks for disturbances in each of the steps from manufacturing, delivery, prescribing, dispensing, and
use of medications [156]. Occasionally, there are reports of system breakdowns in health care resulting in
information being unavailable, health care providers not being able to document appropriately, or risk of
patient harm. However, strategies for continuity during disturbances are insufficient both nationally and in
24

many organizations which limit our ability to provide safe medication independent of interruptions of normal
procedures or system breakdowns [156].
Social aspects and usability The implementation of IT is affected by social aspects such as attitudes and concerns, resistance and
workarounds, expectations, benefits, involvement and user input in design, training and support, and
integration with existing work practices [17, 101]. In order to achieve maximum benefit in the medication
management process, it is necessary that IT is supporting health care professionals rather than being perceived
as an obstacle to providing good care in an efficient manner. An important part of developing and
implementing technology in health care is usability. Usability has been defined as: "The extent to which a product
can be used by specified users to achieve specified goals with effectiveness, efficiency, and satisfaction in a specified context
of use" (ISO 9241-11). Despite the recognized importance, usability aspects are not always incorporated
sufficiently in the design and testing of information systems in health care [151, 157-159]. If changes in work
process are not considered during development and implementation, the potential benefits of IT may not be
achieved [17, 18, 160]. When implementing IT in health care, there might be social challenges such as
attitudes, preconceived notions, changed routines or roles for health care professionals or changes in the
existing hierarchy or power structure, affecting the outcome [161].
Organizational aspects – and regulation Challenges related to organizational issues when implementing IT in the medication management process
include preparing the organization for change, planning, leadership and management, realistic expectations and
financing, teamwork and communication, learning and evaluation [17, 19]. Although most actors in health care
regard eHealth as an organizational development, the procurement of IT systems in health care is still often
handled as a technical matter [152]. Benefits and cost-savings from new technology will be evident at later
stages. Initially, costs and time consumed might increase but must be regarded as an investment.
The importance of eHealth, including eMedication, is increasingly recognized. In Sweden, a number of
authorities are involved in regulation, supervision, and strategic activities related to the medication management
process, as well as managing some of the related information sources or services. The area of responsibilities of
different authorities regarding medication management, including the use of IT in the medication management
process, is somewhat unclear [152, 162].
Many information systems have been implemented without sufficient quality assurance due to a sometimes
immature regulatory situation, and lack of clear requirements or guidelines for evaluation of IT systems in
health care [14, 18]. Drugs and medical devices (such as infusion pumps or respirators) are approved by
authorities, e.g. Food and Drug Administration in the US and Medical Products Agency in Sweden, and have
clearly regulated methods for quality assurance. In contrast, IT implemented in health care, although involved
in many critical steps of medication management and known to directly affect patient care, are often not subject
25

of any independent assessment of safety and fitness for purpose [18]. Medical information systems, such as
EHR, have been classified as medical devices in Sweden since 2009 [163]. As a consequence, there are
demands for quality assurance, including a clinical evaluation of the intended purpose. However, it is unclear
among most involved actors, including system vendors and health care organizations, as well as authorities, how
this should be performed and controlled in practice [164]. On the other hand, dispensing systems at
pharmacies have not qualified as medical devices in the EU [163]. The eHealth Agency (a new Swedish
authority) has performed evaluations to ensure that the dispensing systems’ interface and format work correctly
with the agency’s managed services and databases [165]. However, the agency’s evaluation is not an overall
quality control of the dispensing system and is not a certification similar to the EC certificate used for medical
devices.
Evaluation of eMedication The introduction of IT in health care affects the users, working procedures, organization and outcome, and
does not only have the potential to solve problems, but may also create new ones [166]. Therefore, we must
evaluate the implementation of IT in the medication management process in order to ensure that it meets our
expectations, delivering the desired outcome and does not create new problems [167]. Evaluation of IT in
health care is in itself not a goal, instead it should be used to improve existing technology or procedures, and
provide knowledge for future development, implementation, or wider strategic work. Ammenwerth et al.[166]
describes evaluation in the following way:
Evaluation is the act of measuring or exploring properties of a health information system (in planning, development, implementation,
or operation), the result of which informs a decision to be made concerning that system in a specific context.
eMedication can be studied and evaluated in different settings, using different perspectives, and methods.
When evaluating IT in health care, we have to consider the environment in which IT is used and the human-
computer interaction [19]. Since medication management process is complex, a holistic view with a
sociotechnical perspective is often required when evaluating [14, 87, 149]. A sociotechnical approach means
that the implementation outcome has organizational, technological, and behavioral explanations. There is a
large gap between postulated and empirically demonstrated effects of eHealth technologies. Thus, IT is not
sufficiently evaluated, and when evaluated, the results are often not disseminated [7, 15, 17, 166].
26

AIM
The overall aim of this thesis was to study eMedication in different parts of the medication management
process.
Specific aims in the six papers were:
I. To evaluate Swedish pharmacists’ attitudes towards ePrescribing, including the transfer of
ePrescriptions, electronic storing of prescriptions and mail-order prescriptions.
II. To evaluate Swedish patients’ attitudes towards ePrescribing, including the transfer of ePrescriptions,
electronic storing of prescriptions and mail-order prescriptions.
III. To explore the implementation of four new information systems for dispensing at pharmacies.
IV. To describe physicians’ views on changes in accuracy, availability and confidentiality of information in
the transition from local medication lists to a regionally shared medication list.
V. To analyze potential DRP detected by means of EES in patients with MDDD.
VI. To explore physicians´ perceptions on and clinical relevance of alerts generated by EES for patients
with MDDD, performed actions and changes due to the alerts, and perceived benefits and needs for a
CDSS providing alerts for potential DRP.
27

METHODS
Setting In this thesis, four main aspects of the eMedication process are covered: electronic transfer and storing of
prescriptions (Study I and II), electronic processing and dispensing of prescriptions at pharmacies (Study III),
obtaining accurate information on a patient’s current prescriptions (Study IV), and decision support systems for
detecting potential DRP (Study V and VI). Figure 5 shows where in the medication management each of the
studies can be situated, and Table 4 provides an overview methodology for each study.
Figure 5. Overview of the thesis’ studies of the medication management process.
28

Table 4. Overview of the six studies in the thesis.
Study Research question Study period Data sources Study population
I Pharmacists’ attitudes
towards ePrescribing
April 6 – May 4,
2009
Web-based questionnaire 500 community
pharmacists
II Patients’ attitudes towards
ePrescribing
September 14 –
October 19, 2009
Postal questionnaire 1500 patients
III Describing the
implementation of
dispensing systems at
pharmacies
February – June,
2012
Interviews and questionnaire 4 system vendors of
dispensing system, 13
pharmacy companies’
management and 350
pharmacists
IV Physicians’ perceived
consequences of shared
medication list
in EHR
September –
November 2013
Interviews 7 physicians
V Potential DRP detected by
EES in patients with
MDDD
March 5 – June 5,
2013
Register study. Prescription
repository and alerts generated
by EES for these prescriptions
180 059 patients with
MDDD
VI Physicians’ perception of
EES alerts for patients with
MDDD
March – November
2013
Interviews and physicians
assessment of EES alerts
254 patients with MDDD
and 10 physicians
Study design and data collection Studies I-IV were performed after large scale implementation while an intervention was performed in Study
VI. All studies except one involved the exploration of attitudes, perceptions, needs, satisfaction or experiences
among different users of the implemented health IT, pharmacists (I, III), patients (II), and physicians (IV, VI).
Study III was designed as a case study and included representatives from system vendors and pharmacy
company management as well, using mixed methods to combine data from different perspectives to give insight
on a unique case. Below, the methods for data collection are described.
Questionnaire Questionnaires specifically developed for the study aim were used in Study I, II, and III. Two of them were
electronic and sent to the respondents via their email (I, III), and one was a postal questionnaire (II). The
questionnaires included statements to which respondents gave their degree of agreement on a six-point (I, II)
or five-point (III) Likert-type rating scale, multiple choice questions, and open-ended questions. All
questionnaires were tested among a small number of subjects representing the study population, and adjusted
prior to the large-scale survey.
29

Interviews Interviews (III, IV, VI) followed a semi-structured protocol with questions developed by the researchers for the
specific study, with one researcher (TH) performing all interviews.
Register study All prescribed drugs dispensed for patients with MDDD (n=180 059) during three months (March 5 – June 5,
2013) as well as alerts generated for these drugs were included in the analysis (V). Prescription data were
collected from the national prescription repository.
Outcome assessment and analysis Quantitative as well as qualitative methods were used, and combined in four of the studies (I, II, III, VI).
Quantitative analysis Answers to the questions on Likert scales were regarded as nominal or ordinal data and analyzed accordingly (I,
II, III) [168]. To study any statistical relationship between variables, two different methods were used. In
Studies I, II and VI, the chi-square test was used and statistical significance set at p<0.05 (I, VI) or p<0.01 (II).
In Study V, the relationship between the number of alerts and age, gender, and the number of drugs was
modelled using Poisson regression, a Generalized Linear Model with the logarithmic link function. Poisson
regression is suitable for modelling count data which typically have low mean values and variances, with both
the mean and variance varying with the levels of the independent variables [169]. Analysis was performed using
SPSS (IBM SPSS statistics 20).
Qualitative analysis The responses to the questionnaire in free text were analyzed and categorized using manifest content analysis
methods (I, II, III) [170, 171]. Meaning units, i.e. a section of the free text answer that described one aspect
related to the question, were identified for each free-text answer after reading the answers several times and
subsequently grouped into categories. The categories were not predefined but emerged and changed during the
analysis to best capture the meaning units identified. An individual´s answer could include several different
meaning units that could be grouped into different categories. Representative quotes were chosen for each
category and translated from Swedish to English. One of the researchers (TH) performed the analysis.
With the respondents’ permissions, all the interviews were recorded and transcribed (IV, VI). After completing
all interviews, a qualitative analysis of manifest content was performed in order to identify physicians’ views in
relation to the study questions [170, 171]. The information was sorted into the main aspects and categories.
The categories were not predefined but emerged and changed during the analysis. However, the main
categories identified were mostly in line with the interview questions (for example physicians’ views on how the
accuracy of information had changed with a shared list in Study IV), but some categories not covered in the
30

questions emerged (such as perceived risks and problems with patients with MDDD in Study IV).
Respondents’ answers within each main category were then further analyzed and could be divided into
subcategories to capture the different views on each aspect. Representative quotes were selected and translated
from Swedish to English.
The analysis and categorization of data were performed using Microsoft Office Excel (I, II) and the software
QSR NVivo 10 (III, IV, VI).
Ethical approval Ethical approval was granted for patient involvement and handling of sensitive data for Study II by the
Regional Ethical Review Board in Linköping, Sweden (Dnr 2009-M153-09) and for Study V and VI by the
Regional Ethical Review Board in Umeå (Dnr 2012-359-31M).
The ethical implications of remaining studies were considered based on the guidelines from the Ethical
Advisory Board in South-East Sweden. Following advice from the committee, no formal application for ethical
approval was recommended due to the nature of the information handled and the respondents included.
However, we followed the guidelines from the committee regarding the information to potential participants as
well as handling and presentation of data so that privacy was protected and identity would not be revealed. No
incentives have been offered to the respondents.
31

RESULTS
Study I: Pharmacists´ perceptions of ePrescribing Swedish community pharmacists were generally satisfied with ePrescribing (98%, 253/259). Differences in the
general satisfaction could not be explained by the respondents’ age, gender, or years in practice (p>0.05). A
majority of the respondents regarded ePrescriptions and electronic storing of prescriptions as being safe for
patients (95% for ePrescriptions and 93% for electronic storing of prescriptions respectively), providing patient
benefits (96% and 95%, respectively), and being cost-effective for the pharmacy (92% and 91%, respectively)
(Figure 6). The positive aspects of ePrescribing most frequently mentioned in free text answers were being safe
(72%, 187/259) and saving time (55%, 143/259). Described weaknesses were related to the dispensing system
or related services being used (e.g. inconvenient to make changes or corrections, unreliable technique), a
perceived gap between health care and pharmacies (e.g. different supply registers used by prescriber and
pharmacy, prescriber using abbreviations different than the pharmacy), and legal limitations (e.g. prescriber
cannot view, cancel or change prescriptions in the prescription repository). Pharmacists also described problems
related to patients with MDDD.
Figure 6. Pharmacists’ attitudes towards ePrescriptions and electronic storing of prescriptions. Respondents (n = 259) gave their degree
of agreement with statements on a six-point Likert-type rating scale where 1 represented “do not agree at all” and 6 “completely agree”.
32

Study II: Patients´ perceptions of ePrescribing The vast majority of patients in the study had a positive attitude towards ePrescriptions (85%, 628/739) and
electronic storing of prescriptions (86%, 633/739), and regarded ePrescriptions to be safe (79%, 584/739),
creating benefits for them (78%, 576/739) and promoting faster dispensing (69%, 512/739) (Figure 7).
Attitudes towards ePrescriptions and electronic storing of prescriptions differed with age (p<0.01). The 25–39
years age group had the largest proportion of respondents who had a positive attitude (94%, 95/101), and the
75 years and older age group had the smallest proportion of respondents with a positive attitude (70%, 87/123).
Patients storing all their prescriptions electronically were more positive towards both ePrescriptions and
electronic storing of prescriptions than patients who stated they had paper prescriptions: of the respondents
storing all their prescriptions electronically 92% (413/450) were positive towards ePrescriptions, compared to
59% (27/46) of the respondents who only had paper prescriptions.
The most common suggestion (n=27) for improvement was to extend the information given about the services:
e.g. information about how to use the services, and the safety aspects of using them. Two of the most common
comments were that the respondents had limited experience with the services (n=26) and that they did not have
a computer (n=10). The study population had limited experience with mail-order prescriptions and the vast
majority of the study population (79%–86%) answered with ‘do not know’, or did not answer at all the
questions regarding mail-order prescriptions.
Figure 7. Patients’ attitudes towards ePrescriptions and electronic storing of prescriptions. Respondents (n = 739) gave their degree of
agreement with statements on a six-point Likert-type rating scale where 1 represented “do not agree at all” and 6 “completely agree”.
33

Study III: Implementation of dispensing systems at pharmacies The implementation of four new dispensing systems followed a strict timeframe set by political decisions,
involved actors completely new to the market, lacked clear regulation and standards for functionality and
quality assurance, was complex, and resulted in variations in quality. With pharmacies legally responsible for
the quality of dispensing systems, there were variations in quality assurance: one system was an in house
developed product, the larger pharmacy companies had a significant involvement in the system development
and testing, and the smaller pharmacy companies had to rely on the vendors’ quality management systems. It
was unclear how quality assurance was shared among actors in practice, i.e. who validated what, when, and
how. System vendors and pharmacy companies´ management described several different problems during the
development, implementation and use of the dispensing systems including among other things: short time
frame resulting in incomplete systems in use; lack of a common interpretation of applicable laws that were
regarded as rather non-specific; unclear roles of different authorities, and the fact that those authorities had not
always been in alignment; new dispensing system changing the workflow and requiring major adaptation and
training of the staff. More than half of the pharmacists (58%, 66/115) perceived their current dispensing system
as supporting safe dispensing of medications, 26% (30/115) were neutral and 15% (17/115) did not perceive it
to support a safe dispensing (Figure 8). Most pharmacists (80%, 95/115) had experienced problems with their
dispensing system during the previous month. The pharmacists experienced problems including reliability
issues (e.g. slowness, bugs, or system crashes), usability issues (e.g. not showing information at the right time,
complicated methods to undo actions or change products, and redundant steps and excessive requests to login)
and missing functionality (e.g. support for advice or detecting drug-drug interactions). The EES decision
support system was only available in some pharmacies and was only used infrequently at the time of the study;
an active choice and consent from the patients was required to view the alerts for potential DRP. Pharmacists
also described problems related to patients with MDDD.
Figure 8. Pharmacists’ (n=115) degree of agreement (%) on a 5-point Likert scale with three statements regarding their dispensing
system where 1 represented “do not agree at all” and 5 “completely agree”.
34

Study IV: Physicians' perceptions of a shared medication list Interviews with physicians’ (n=7) showed that the transition from local medication lists to a shared medication
list was perceived to increase the availability of information: from being time consuming or not possible to
obtain information from other caregivers to most information being available in one place. However, there was
still a risk for events limiting the availability of information, such as system breakdowns. A regionally shared
medication list was perceived as having the potential to provide a greater accuracy of information but not
always; the shared medication list was perceived as more complete but with an increased number of non-current
drugs. Most physicians considered that the non-current prescriptions in the medication lists were primarily due
to incorrect working routines. On the other hand, a shared medication list implied an increased risk of violating
patient privacy, placing greater demands on IT security in order to protect the confidentiality of information.
The majority of physicians had experienced few or no patients who had ever had concerns with a physician
being able to access their medication information; quite the opposite, patients were usually surprised to hear
that the physician had not always had access to the information. Physicians described other aspects of
information risks related to information regarding patients’ medications, such as the physicians’ unclear
responsibility for medication lists, the need for information other than the medication list to provide a context
or a better overview, patients still often lacking information on current medications, and specific issues related
to patients with MDDD (Figure 9).
Figure 9. Summary of the main findings on physicians views on changes in availability, accuracy and confidentiality in the transition
to a shared medication list.
35

Study V: Potential DRP detected by EES The study population (n=180 059) had 10.0 different medications (SD ±4.7, range 1-53). EES alerted for
potential drug related problems in 76% of the population with a mean of 2.2 alerts per patient (SD±2.4, range
0-27). The older patients received a lower number of alerts compared to younger patients despite having a
higher number of drugs (Figure 10). The most frequent alert categories were drug-drug interactions (37% of all
alerts), duplicate therapy (30%), and geriatric warnings for high dose or inappropriate drugs (23%).
Psycholeptics, psychoanaleptics, antithrombotic agents, anti-epileptics, renin-angiotensin system agents, and
analgesics represented 71% of all drugs involved in alerts (Table 5).
Figure 10. Mean number of drugs and alerts in different age groups of patients with multi-dose drug dispensing (n=180 059).
Table 5. Proportion (%) of each alert type represented by the six most common therapeutic groups of drugs in patients with multi-dose
drug dispensing (n=180 059). B01=Anti-thrombotic agents, C09=Renin-angiotensin system agents, N02=Analgesics, N03=Anti-
epileptics, N05=Psycholeptics, N06=Psychoanaleptics
Alert type B01 (%) C09 (%) N02 (%) N03 (%) N05 (%) N06 (%) Other (%)
Drug-drug interaction (n=301 018) 24.1 10.9 6.6 4.4 9.0 16.6 28.5
Therapy duplication (n=245 280) 0.4 1.5 9.7 10.7 19.5 17.7 40.5
Geriatric warning (n=128 275) 0.1 9.9 2.5 0.6 58.7 15.2 13.1
Drug disease inferred (n=43 319) 1.6 0.6 5.5 24.1 34.8 19.8 13.7
High dose (n=15 848) 0.8 0.2 1.7 1.3 39.1 14.0 42.8
Drug gender warning (n=668) 0.0 0.0 0.0 0.0 0.0 0.0 100.0
Pediatric warning (n=209) 0.0 0.5 19.6 18.7 34.9 12.4 13.9
All drugs involved in alerts (n=734 617) 10.1 6.7 6.7 6.9 23.3 16.8 29.3
36
Study VI: Physicians’ perceptions of EES alerts Patients with MDDD included in the study (n=254) received on average 11.4 different drugs (SD±3.9, range
5-23). They had a total of 740 alerts, 89% of all patients had at least one alert from the EES and the mean
number of alerts was 2.9 (SD±2.3, range 0-14). Physicians perceived 68% (502/740) of EES alerts as clinically
relevant, indicated an intended action for 37%, and made changes in the treatment in accordance with
indicated action for 11% of all alerts. Alerts generated were therapy duplication (37.4% of all alerts, n=277),
drug-drug interactions (34.7%, n=257), geriatric warnings (22.6%, n=167), drug-disease inferred (3.8%, n=28),
and high dosage (1.5%, n=11) (Figure 11). Clinical relevance and likelihood to make changes in drug treatment
were related to alert category and substances involved in the alert. For example more than 80% of the geriatric
warnings were regarded as clinically relevant and 19% were followed by a change in drug treatment, compared
with alerts for therapy duplication where only 50% were regarded as relevant and 9% were followed by changes.
Physician interviews revealed that most perceived a need for a CDSS regarding medications, that the alerts
from EES could be useful in clinical practice, and that most alerts were regarded as relevant although they did
not necessarily lead to a change in drug treatment. If alerts from EES should be made available for physicians
they considered that it had to be in an integrated form in their EHR and some aspects should be improved.
Figure 11. Physicians’ assessment of clinical relevance (black), any intended action stated for alert (grey) and alerts for which the stated
change was actually made (striped). Given as a proportion of all alerts within each alert type (%).
37

DISCUSSION
During the past decades, IT has been increasingly used to support the medication management process, and is
necessary due to the demands of an efficient, safe, and patient centered medication, requiring certain
information to be available to involved actors. However, the implementation of IT in the medication
management process has proven to be a challenging task due to unfulfilled expectations [14, 17, 18].
In this thesis, we have studied the employment of IT in different steps of the medication management process
during different stages of implementation with focus on the users' perspectives. In summary, we found that IT
has become a natural and necessary part of medication in Sweden but several problems remain to be solved:
weaknesses with usability, functionality, and reliability of the IT systems used; insufficient patient involvement;
involved actors still lack accurate and complete information as well as appropriate knowledge-based support for
decision making.
ePrescribing - pros and cons ePrescribing, including electronic storing of prescriptions, was accepted and appreciated by pharmacists and
patients (I, II). Similar attitudes among physicians have been demonstrated previously in Sweden [86, 172].
Even if the vast majority of pharmacists in our study were satisfied, several weaknesses were revealed in the
survey. Described weaknesses were related to the dispensing system used, lack of coordination between
pharmacies, legal restriction of information access and health care and reliability; several of these are in line
with those reported previously by physicians [86]. Studies from other countries support prescribers’ and
pharmacists’ positive attitudes towards ePrescribing [32, 91, 173, 174]. Fewer studies have been directed
towards patient attitudes [31].
The finding that ePrescribing in itself is accepted and appreciated indicates a successful implementation. Early
implementation of ePrescribing paved the way with integration of the infrastructure and acted as a driving force
for eMedication in a wider perspective. Electronic handling of prescriptions enables new services both for
patients and health care professionals. The rather successful implementation of ePrescribing in Sweden may be
due to several factors including the implementation of ePrescribing at a time when there was only one state-
owned pharmacy company being a strong actor in the medication management in Sweden. Introduction of the
38

NEF resulted in a significant reduction of errors among electronic prescriptions [99]. Described weaknesses
indicate a need for improvement of usability and reliability in the information systems used for handling
prescriptions, as well as the information accessible and coordination of systems. There have been some work to
identify factors with ePrescribing related to success or errors, respectively [32, 106, 167, 175-177]. The use of
evidence based strategies might improve ePrescribing.
Implementation of new dispensing systems The implementation of new information systems for dispensing prescriptions at pharmacies in Sweden was
related to weaknesses of reliability, functionality, and usability that could affect patient safety (III). Some of the
weaknesses with ePrescribing described by pharmacists before the re-regulation were related to the dispensing
system they used (I). Similar weaknesses described with both old and new dispensing systems indicate that not
all issues arose with the new dispensing systems. In addition, some of the problems identified were not directly
part of the dispensing systems themselves, but rather other parts of the technical infrastructure involved in the
process of dispensing prescriptions (III). This reflects the importance of ensuring the quality of each
component involved in a process, as well as the interoperability between components [99].
A limited amount of research has been reported regarding information systems for dispensing prescriptions at
pharmacies, and the terminology used in those studies varies [16, 95, 106, 108]. As with other health IT,
dispensing systems have the potential to increase patient safety, for example by decreasing manual entry of
information, increasing the availability of information, and supporting an appropriate workflow, but they can
also cause problems. Technology is reported to be one of the factors that may contribute to variations in
pharmacists’ prescription intervention practices, such as intervening in the event of prescribing errors and DRP,
and providing counselling to patients [61]. Although these tasks are important for pharmacists’ work, the actual
procedures are insufficiently regulated or defined in guidelines, and are insufficiently considered when
designing a dispensing system.
The weaknesses of the dispensing systems implemented in Sweden after the re-regulation seem to result from
the limited time for the development and implementation, the lack of comprehensive and evidence-based
requirements for dispensing systems, and the unclear distribution of quality assurance responsibilities among
involved stakeholders. Thus, there seems to be a need for information and commitment from responsible
authorities.
39

Shared information - and medication list A regionally shared medication list was perceived by physicians to increase the availability of the information
about current prescriptions but may decrease the confidentiality of information (IV). A regionally shared list
was considered as having the potential to increase accuracy, yet in reality, many lists were still inaccurate.
Although the medication list was more complete, many physicians experienced an increased amount of non-
current prescriptions. This view is in line with previous findings that regionally shared lists reduce the number
of missing medications, but non-current medications remain a significant problem [141]. In addition, some
issues remained unsolved with the regionally shared medication lists: the medication list still not being linked
to the prescription repository, not including information on dispensing, most often not being the information
source used by patients, not being shared across county borders or with municipalities, and not automatically
including prescriptions for patients with MDDD. Furthermore, the issue of OTC and other non-prescription
medications remains.
Several studies indicated issues related to the national prescriptions repository, such as non-current or duplicate
prescriptions, and physicians being unable to access or change prescriptions (I, II, III). Since Sweden has more
than 90% electronically stored prescriptions, an almost complete access to information on current prescriptions
would be expected, but due to legal reasons, prescribers are not allowed to access the prescription repository in
its present form. As a result, prescribers are still bound to use local or regional medication lists in their EHR.
This is an example of when current regulation for protection of patient integrity is perceived to be in conflict
with patient safety.
Although a shared medication list is often referred to as a path to provide safer medication by providing an
accurate and complete list of patients’ medications, the consequences of a transition from a local to a shared
medication list are related to several aspects. A Swedish study found that the implementation of a region-wide
EHR increased accessibility and readability of information but that the EHR did not provide sufficient
support, had low usability, and was time-consuming to use [101]. In the US, a shared medication list improved
accuracy [136], and a similar implementation in Austria was perceived as having the potential to improve
patient safety, but both studies described difficulties [135]. Internationally, there are different approaches for
sharing medication information and health records, both regionally, nationally and internationally [65, 79, 89,
92, 135, 136, 144-146]. Implementing shared systems for health information has turned out to be more
challenging, complex, and expensive than expected [178]. The major issues are usually not related to
technology, but rather strategies, and management [145].
Accurate and available information on patients’ current medications is vital for safe medication. Thus, the
implementation of a nationally shared medication list is at the core of improving eMedication. Physicians
believed a nationally shared medication list would be useful, but only if the technical solution was sufficient, fit
40

their process, was implemented properly, and responsibilities clarified (IV). Thus, the success of a nationally
shared medication list is related to several factors. Ideally, a nationally shared medication list should include all
prescriptions, and the same information source should be available and used by pharmacies, patients, and
municipalities. With the nationally shared medication list (NOD) being planned in Sweden, different counties
would still have separate EHR systems, and information on medications would be shared through a common
database that would also be linked to the prescription repository used at pharmacies. To implement a shared
medication list, we recommend providing a clear description of responsibilities and routines for normal
activities as well as back-up routines, considering IT security and data protection early in the development, and
involving patients to improve the accuracy of the list, as well as to monitor and evaluate the implementation.
Decision support systems are important but must mature It is recognized that a CDSS can be a valuable tool for physicians and pharmacists to improve safety and
efficiency [6, 15, 112, 113, 179, 180]. EES is initially intended for use in pharmacies but has been proposed as
a potential support in health care as well. Potential DRP were detected in the majority of patients with
MDDD, on average two alerts per patient (V). In addition, we found that physicians regarded the majority of
alerts (68%) as clinically relevant and several alerts (11%) were followed by changes in drug treatment (VI). The
clinical relevance and likelihood to make changes in drug treatment were related to alert category and
substances involved in the alerts. Most physicians perceived a need for a CDSS regarding medications, and
deemed the alerts from EES as useful in clinical practice, if integrated into their EHR with some aspects
improved. Physicians’ description (VI) of their need for a CDSS regarding medications is in line with the
findings in another study, i.e. automatically generated alerts for severe drug-drug interactions and functions for
calculating glomerular filtration rate to enable appropriate dose adjustments [66].
Appropriate decision support is important in pharmacies as well to support pharmacists in detecting potentially
inappropriate prescriptions [113, 181]. At the time of the study, two of the dispensing systems had integrated
EES as a support for pharmacists and many pharmacists wanted a CDSS or some support system to aid in
counselling patients about their medications (III). Even among pharmacists with access to EES, the use was
limited due to several factors: the decision support was regarded as complicated and time consuming, there was
limited awareness of the system and had not been enough education, and viewing the alerts of the EES
required an active choice as well as patient consent. However, even if pharmacists have access to an integrated
CDSS, the awareness of CDSS functionalities is often limited, emphasizing the need for user training [109].
Although our studies showed that EES alerts could detect potential DRP, we cannot conclude any actual
patient benefits due to the study design (V, VI). From our studies, we cannot know how well suited EES is for
integration and use in health care. EES in its current form does not meet all of the current and future needs of
decision support in medication management in health care [66]. A report by the Medical Products Agency
41

conclude that the drug-drug interaction support SFINX, currently used in health care, has several advantages
compared with the corresponding knowledge base in EES [182]. Nevertheless, EES includes other knowledge
bases, for example the maximum daily dose where alerts based on the dose calculated from a prescription
generate an alert when the maximum daily dose is exceeded , that may be useful in health care (as well as
pharmacies) and should therefore not be neglected. For the current situation in Sweden, we suggest to combine
the best of available knowledge bases after thorough investigation, provided through an optimal graphical user
interface and available infrastructure and solutions. CDSS for medication holds great promise but for progress
we need substantial research and development. A flexible system that can continuously be developed is
necessary to follow changes and progress and allowing maturation.
Ideally, a CDSS for detecting potential DRP should have a high selectivity and specificity, i.e. only give alerts
that are clinically relevant and useful [114]. There are different strategies for increasing the specificity of alerts
[183-185]. Patient specific information, such as renal function or other lab-values or diagnoses, should be
included in algorithms [66]. The ideal CDSS should be flexible and easily adopted and further developed to
allow for integration of new functions, e.g. the inclusion of genetic profiles as support for decisions on
treatment and dose. In addition, alerts should be provided at the right time when the decision is being made,
and in the right form [114, 122, 186]. Some users want a system that can be adjusted for different situations
and different professionals according to their preferences and needs (VI). Open data in a structured machine
readable format allows for utilization of knowledge bases in other settings, solutions or applications. Knowledge
bases should be quality assured, continuously updated by experts according to evidence, new findings, and
clinical praxis, and a plan for maintenance and responsibility for the content is also important during its entire
life cycle [111].
Multi-dose drug dispensing Patients with MDDD were included in the studies on EES primarily due to legal reasons only allowing
physicians to view the complete drug list from the national prescription repository for this specific group of
patients (V, VI). Although not a part of the study aim, issues with MDDD emerged in the other studies as
well. Pharmacists described problems of dispensing and handling prescriptions for patients with MDDD in the
dispensing systems (I, III). Physicians raised issues specifically regarding patients with MDDD (IV); in
primary care, medications for patients with MDDD were prescribed in a separate prescribing tool with
information usually not connected to the EHR, which was not always recognized at hospitals, sometimes
resulting in medications from an outdated and inaccurate medication list being administered among other
things.
The service of MDDD aims at improving medication safety, adherence and reduce workload in health care
[187, 188]. Several Swedish studies have indicated that patients with MDDD have a lower quality of drug
42

treatment than other patients, an increased number of drugs after a patient’s transition to MDDD, and fewer
changes in drug treatment [29, 48-50, 53]. However, problems with patients with MDDD do not seem to be
the result of the dose-dispensing itself, but rather the tools and procedures for handling prescriptions being
different than those used for ordinary patients and they are not integrated with each other. Some of the
problems may be due to weaknesses with the systems or tools used; many problems were described after the
introduction of Pascal, which is an online tool for order entry used for patients with MDDD [189]. However,
some problems might simply be due to the fact that patients with MDDD often are being handled in a separate
system using different procedures than for other patients. Thus, there seems to be a need for exploration of how
medication quality and safety can be improved for patients with MDDD.
Prevention of DRP requires responsibility and collaboration To prevent DRP it is important to have accurate information, knowledge, and cooperation, as well as
clarification of responsibility among involved actors. One part in the prevention of DRP is the prevention of
medication errors. Medication management and health care is not unique. There are general concepts for
reducing human error and increasing safety drawn from numerous disciplines described in the report “To err is
human: Building a safer health system” [190]. Several of these apply to the use of IT in the medication
management process: e.g. user-centered design (building on human strengths and avoiding human weaknesses
in processes and technologies), avoid reliance on memory (standardize and simplify), involving patients in their
care, anticipating the unexpected (be cautious and expect errors with new technology), and improving access to
accurate and timely information (information coordinated over time and across settings).
To improve patient safety, the involvement of patients in the medication process is regarded as a key strategy
[77, 130]. We found that patients wanted more information about ePrescribing and safety aspects of using the
services, highlighting the need for more detailed information delivered in different ways and disseminated in
different settings and formats (II). In addition, we found issues related to some older people having a less
positive attitude towards ePrescribing that might be related to a general resistance towards, or exclusion from,
the digital society (II). Information and education to patients is important, as satisfied patients are more likely
to adhere with treatment and take an active role in their own health care [74]. To achieve a collaborative
relationship between patient and provider concerning medication treatment, it seems necessary to share
information regarding current medication via a common medication list. Many patients are currently using the
list from the prescription repositories which often does not correspond to the medication list physicians are
using [191]. Patients should provide information regarding use of OTC drugs and other non-prescription
drugs since these could be involved in drug-drug interactions and other DRP as well [192]. For a safe
medication, the patient should be properly informed and have control of her/his drugs, and decision making
should be shared. Initially, it might take more time with extended consultation and education, but patient
43

involvement often has positive effects in the long run [3]. Many patients want access to their health records or
medication information and want to take part in treatment and providing information [73, 130, 193].
Physicians are responsible for medication, but we found variations in perceived responsibility for medication
(IV, VI). Physicians’ responsibility for the accuracy and completeness of the medication list and the
appropriateness of medication treatment were perceived in different ways and were unclear, in line with
previous findings [55, 56] and similarly to findings with regards to medication reconciliation [57]. The
responsibility of the medication list might be affected by the system for reimbursement [58]. The shared
medication list does not in itself result in any formal changes in the responsibility for medications, but the
shared list is a tool that enables increased opportunity for prescribers to take a greater responsibility. That
physicians are not regarding alerts involving medications outside their specific competence and expertise as
relevant is worrisome but also in line with other studies regarding physicians’ perceived responsibility for
patients’ medications [55]. There seems to be a need for clarification regarding physicians’ responsibility for the
accuracy and appropriateness of the medication list. The network for the Swedish regional drug and
therapeutics committees (LOK) has recently presented their recommendations for guidelines regarding
responsibility for a patient’s medication list, based on current regulation and the thesis by Pia Bastholm
Rahmner [54, 194]. The recommended guidelines are specifically considering the implementation of a
nationally shared medication list (NOD) and suggest that the shared medication list should be the main source
of information regarding patients’ current drugs in health care, but also for pharmacies and patients themselves.
The recommendations also include specific procedures for starting, changing or ending a treatment, to increase
the accuracy of medication lists.
Pharmacists, nurses, and other health care professionals are also important in the prevention of DRP [33].
Pharmacists have pharmaceutical expertise with potential of improving outcome and patient quality of life by
identifying, resolving, and preventing many DRP. However, presently the pharmacists seem to be an underused
resource of pharmaceutical expertise, with too little focus on improving drug treatment or providing
pharmaceutical care during patient encounters in community pharmacies [102, 195]. Increased recognition of
the pharmacist’s role, improving the possibility for pharmaceutical counseling, and increased understanding of
pharmacists work and interventions could be one part in improving medication management [61].
For an efficient collaboration and information exchange, the possibility for increased two-way communication
in the medication management process should be explored [32, 94, 133]: e.g. pharmacists send a question to
the prescriber regarding an ePrescription, or patients using the shared medication list to communicate which
medications they are taking. Some of the weaknesses perceived in the medication management process were
that there was a lack of coordination between pharmacies and physicians, in line with other studies [33, 94].
44

Risks with novel technology and poor usability Although aiming at improving patient safety and efficiency, novel technology can have negative consequences
for various reasons [97]. New errors or problems related to the implementation of IT in the medication
management process include e.g. errors in data entry, missing or unavailable prescriptions, work-arounds,
double documentation, more time-consuming work, mix-up of patients, selection of wrong medication due to
how it is presented on the computer screen, frustration among users, and confidentiality breaches [5, 17, 94, 97,
101, 196]. Over-dependence on technology can be a risk in itself, e.g. if inappropriate prescribing is missed
because the CDSS does not give an alert, or if a medication list is perceived as more complete than it actually is
[87]. New technology can also result in changed communication and working procedures [87, 106]. Designing
IT to support, and not interfere with, clinical work is a major challenge. Many systems are perceived as having
low usability [101, 151, 157, 159]. A poor fit between technology and clinical workflow might cause errors, and
unintended changes in the actual workflow might have unanticipated consequences [17, 87]. The pharmacist’s
workflow was often perceived as having been changed by the new dispensing systems (III). Medication lists
being inaccurate seemed to partly result from physicians working in different ways when using the same shared
list (IV). Some issues may be related to users being unaccustomed with a particular EHR system, rather than
the fact that it is a shared list. The specific technical solutions, usability of systems, implementation strategy,
and routines were perceived as affecting the accuracy of information in the medication lists (IV).
Physicians and pharmacists who had experienced a large scale implementation of new IT systems described
major initial problems (III, IV). End-user involvement and the possibility of changing and improving the IT
system after implementation have been described as important for successful implementation and as a strategy
of improving usability. The Swedish dispensing systems were developed in an iterative process and further
developed substantially in the years after their introduction. The dispensing systems were described as
unfinished when they were initially used which might have jeopardized patient safety (III). This study was
performed early after implementation, capturing many of the early errors, corrected later on. Nevertheless,
these findings suggest flaws in systems that had passed the regulatory bar at the time of the study and were used
in real patient situations. The pros and cons of the iterative process, involving user feedback as part of the
development, compared with standard solutions is under debate [164].
Identifying the needs that an information system should fulfill is not a trivial task. Simply asking end-users
what they want and providing it to them does not necessarily result in an optimal system [18]. A major obstacle
is the communication between developers and clinicians where differences in understanding and terminology
may lead to systems failing to meet users’ needs [164, 197]. Observation or meeting in the clinical setting where
the system is used might be a way to reach better understanding of the actual work the technology should
support, including interaction between people, technology, and environment, as well as potential problems and
solutions.
45

Information security, continuity, and information structure In the endeavor to implement IT in order to increase the effectiveness and availability of information in the
medication management process, patient safety and integrity have to be protected. Some of the problems in
several steps of medication management seem to be related to the current regulation for information sharing in
health care (I, III, IV, VI). It is important that the legislation protecting patient safety is reasonable and clear,
and is adjusted to modern health care and IT systems. Physicians experienced that most patients primarily
perceived the benefits of medical information to be shared between care providers (IV). However, it is
important to study patients perspective on sharing information [198]. Risks of unauthorized access of
information increase with the number of users and the larger amount of information stored in one place [89].
Pharmacists and physicians described disturbances where information was temporarily unavailable (I, III, IV).
We should be able to provide a safe medication regardless of situation, place or time, even in a time of crisis,
deviation from normal procedures or system breakdowns. Thus, there is a need for strategies for handling
disturbances in the medication management process on different levels [156]. Back-up routines for system
breakdowns should be provided and these should be known and practiced.
Large variation and lack of standards regarding information in health care limits the ability to share, exchange
and re-use information for different purposes [14]. A large amount of the information documented in the
EHR is in an unstructured free text format and there are large variations in the terms and vocabularies used. As
a consequence, information is rarely re-used, although it could be valuable for clinicians as well as research
[199]. The need for a common, appropriate and structured documentation has been mentioned in several
national strategies and government documents [11, 152].
To continuously improve medication, it is vital that we learn from our mistakes. Therefore, reporting,
collecting and analyzing data on ADRs, DRP and errors in the medication management process is important as
feedback to health care professionals as well as organizations, decision makers and vendors [14, 21, 34, 200-
202].
Quality assurance of eMedication Sometimes IT in the medication management process is introduced without being properly tested among users
[5, 14, 17, 19]. Users must be able to trust the quality of the system delivered by the vendors. Thus, when
implemented in health care, IT must be combined with mechanisms counteracting errors with fatal or severe
consequences.
Dispensing systems are not regulated under a specific product safety regulation as are medical devices [163].
Although pharmacy companies are legally responsible for the quality of dispensing systems, it does not seem
realistic for them to conduct the quality assurance themselves, as at least some of them lack the required
46

knowledge, capacity, and resources [197]. Quality assurance by several stakeholders with insufficiently defined
responsibilities may result in duplicated work, or worse, failure of any party to test some aspects of the system.
The findings revealed some confusion regarding the evaluation of all dispensing systems by the eHealth agency.
Some vendors and pharmacy companies perceived the eHealth agency to perform a broader quality assurance,
when the agency in reality is responsible only for securing the connection with their own systems (III).
Following the study regarding dispensing systems in Sweden, the Medical Products agency introduced a new
regulation for national medical information systems, including dispensing systems, with increased requirements
for quality assurance [203].
Even with systems classified as medical devices, it is unclear among most involved actors, including system
vendors, health care organizations as well as authorities, how quality assurance and clinical evaluation in
practice should be performed and controlled [164]. The need for increased evaluation and quality assurance of
IT in health care is increasingly recognized. However, what it means, how it should be done and by whom, as
well as how it should be regulated, is under discussion in different settings worldwide with many different
opinions. Many argue that IT in health care should be assessed and approved in a similar process as drugs and
other medical devices, while others believe in different approaches [14, 18, 163, 167, 204]. Factors
complicating evaluation or certification of IT in health care includes: e.g. the complexity of many systems,
difficulties in describing the indented purpose, many systems consisting of several software components from
different vendors, and the heterogeneity of health care settings and users, as well as an ever changing
environment they are used in. There is also a fear of strict regulation reducing innovation and limiting the
flexibility and adaptability of IT systems [18, 19, 204]. Nevertheless, quality assurance of IT in each part of the
medication management process, as well as clarification of responsibility among involved actors, is of vital
importance.
Methodological considerations When studying the implementation of IT in the medication management process there is a need to use several
methods in order to cover different perspectives since the implementation concerns not only the technology
itself but also social and organizational aspects, i.e. a sociotechnical perspective [19, 97, 166]. Although,
important to study each component per se when studying implementation of IT, it is important to be aware of
a holistic perspective, how things might affect one another and the outcome [14]. In this thesis, a variety of
methods have been employed, mainly questionnaires and interviews, but also register analysis. The analyses
have focused mainly on the user perspective.
Strengths and weaknesses with study design Most studies were based on the subjective views of different informants, and do not represent an objective
evaluation. Subjective views do not always reflect the reality; e.g. a perceived increase in safety or efficiency does
47

not necessarily mean that the same could be measured with an objective method, on the other hand an IT
system might be perceived as lacking functionality or having low usability when the user is unaccustomed to the
system or has received insufficient training. Nevertheless, subjective views are real to the user and thus may
affect the outcome. Ideally, methods should be combined to include both subjective and objective
measurements in an evaluation. Qualitative studies are vital to understand the complex nature of how systems
are used and valued [205]. Subjective views of (actual or potential) changes and effects of IT in the medication
management are widely used and can give insight of benefits, experienced problems, and need for
improvements [206]. An important part in the outcome of the implementation of eMedication is the attitudes
of the involved actors towards the new technology, including the perceived advantages the technology offers
compared to the traditional method. Different groups of health professionals or other actors often have
different needs and expectations [133, 193, 206].
Only potential DRP were detected in the studies with EES, and we cannot conclude how many of them would
have cause a manifest DRP. Also, there are potential DRP that we could not detect with our method.
Additionally, from our studies, we cannot draw any conclusions whether patients with MDDD are more prone
to DRP compared to patients with ordinary prescriptions. Since the study had no control group, we cannot
state if changes in drug treatment were due to the alerts or would have been accomplished anyhow.
Nevertheless, it demonstrates a relationship between the potential DRP and changes made, i.e. it strengthens
the clinical relevance of alerts, but does not show any causal relationship. To study the effects of IT such as
clinical outcomes, and to know that the changes are related to the technology, randomized controlled trials are
needed [8]. There was no analysis of patient outcomes and no cost-benefit analysis in this thesis.
Limitations The relatively low response rate for the questionnaires might have biased the results of the study if the non-
responses were not random. Pharmacists choosing to answer a web survey may perhaps have a more positive
attitude towards using technology in general, compared with the total study population. In the study involving
patients, we tried to minimize the risk of our results being biased towards more computer-friendly respondents
by using a postal questionnaire instead of a web-based questionnaire.
In the studies with interviews, the low number of respondents is a limitation. We cannot rule out that with a
larger number of respondents other aspects or perspectives could have emerged. However, we believe that the
main aspects captured would not have changed substantially with more interviews.
The selection of respondents for questionnaires and interviews may also bias the results. We had problems
involving pharmacists in Study III, with the number of pharmacists from different companies and different
dispensing systems being unevenly distributed, making the results less representative for all pharmacists in
Sweden. The selection of physicians in Study IV might also have biased the results to represent physicians more
48

interested in questions related to medication and IT in health care. Thus, the findings do not represent the
view of physicians in general.
The register study (V) had a large population size, including all patients in the study population. The data from
the prescription repository used in the study has high coverage (more than 90%) of prescription medications in
the Swedish population. However, it does not cover OTC medications. The reason for using the prescription
repository instead of the national prescribed drug register intended for and extensively used for research was
because the algorithms in EES are implemented for analysis of prescriptions in the prescription repository.
There are some important differences between the registers. However, the researchers regarded that, for
patients with MDDD, the prescription repository could be used to capture current prescriptions. Findings from
the studies with patients with MDDD, cannot be generalized to all geriatric or other patients as patients with
MDDD differ from patients in general with ordinary prescriptions.
General challenges when evaluating eMedication There is a large diversity in the methodology employed in research and evaluation of IT in health care, which is
a challenge in itself. A major challenge in the evaluation of eMedication, and IT in health care in general, is the
lack of common terminology which makes it difficult to find similar research and compare results. There are
also vast differences between the systems, organizations, settings, regulation, and procedures between different
countries limiting the generalizability of findings. Thus, a positive outcome of an IT system being implemented
in one setting may not have the same effect in another setting, no matter the strength of the methodology.
Continuously changing and developing IT systems, as well as related aspects, are another challenge in
evaluation. Some models and unified terminology have been proposed to facilitate analysis and comparison of
eMedication systems [88, 207]. To improve future research, there is a need for further validations of the
instruments or models used.
Implications, recommendations, and future research Appropriate IT with sufficient quality is necessary to meet the challenges of future health care, including the
medication management process. When implementing IT in the medication management process, we need to
identify the advantages as well as the potential problems that may emerge in order to prevent them.
For appropriate, safe, and rational medication, we need increased availability of information in a usable form,
more involved patients, and support by information systems that are usable and reliable. For this, we should
make use of our experiences, learn from mistakes and successes, recognize the obstacles but also the final goal,
plan the road ahead, encourage innovation but also work strategically at national level.
Below, we provide recommendations for improved eMedication in Sweden as well as suggestions for future
studies.
49

Recommendations for improved eMedication in Sweden Based on the research in this thesis, other publications and experiences, the following is recommended for
improved eMedication in Sweden:
1. Improve usability of the IT systems in the medication management process. Determine the needs of
users and let the desired working process direct technical solutions, and not vice versa.
2. Provide high quality decision support systems for physicians and pharmacists. Recognize the potential
benefits but also the complexity in providing/implementing a good decision support.
3. Implement a nationally shared medication list. Provide a clear description of responsibility for the
appropriateness of medication and accuracy of information, as well as actual procedures for keeping the
information accurate. Medication for patients with MDDD should be managed in the same systems as
other patients.
4. Increase patient involvement and education. Give patients access to the same medication list as being
used in health care, and involve patients to improve the accuracy of the information.
5. Improve continuity planning. Provide back-up routines for system breakdowns and make sure they are
known and practiced. Consider IT security and data protection early in order to protect confidentiality
of information without jeopardizing patient safety.
6. Cooperate strategically. Joint efforts by authorities, vendors, pharmacy companies, end users and
researchers are needed to avoid a gap between standardized regulatory requirements and user needs
when developing health systems.
7. Facilitate improved communication and integration of systems, organizations and actors, by increased
standardization regarding interoperability and information structure. Consider increased implementation
of electronic two-way communication among actors in the medication management process and
include assessment of potential benefits as well as risks.
8. Clarify responsibilities for quality assurance among involved authorities and organizations regarding the
entire process of eMedication. Clarify who is functionally and legally responsible for which parts and
how it is controlled. Improved regulation, transparent and standardized requirements are needed as
well as guidelines, with the support of regulatory surveillance.
9. Monitor and evaluate the implementation of technology. Test the technology on a small scale before
implementing it on a full scale.
10. When planning, implementing and evaluating IT in health care, it is important to consider a holistic
view with the different aspects affecting the outcome: i.e. technology, users, and organization.
50

Future studies Since health care is increasingly team based, the role of all professionals involved in the medication process has
to be studied. So far, the prescribers, i.e. mainly the physicians, are well studied. There is a need for more
studies on nurses, pharmacists, and other health care providers, their needs and practice patterns as they are also
the frontline practitioners who are directly interacting and dealing with patients who are taking medications on
a regular basis. In addition, there is a need for studies on how all health care professionals interact and how IT
could support and facilitate these processes. Clearly, patients and relatives are of central importance to keep
informed in order to help ensure their optimal involvement in the management of their own/patient’s
medication and to maintain adherence. Here, more studies are suggested to identify success factors of how IT
can improve adherence.
There is a need for studies on how IT in the medication management process affects patient outcomes as well
as cost-benefit studies of IT in the medication management process. There is a need for more research on how
the design and features of IT systems in the medication management process affect usability and patient safety,
as well as how IT systems can support optimal working procedures in health care and pharmacies.
Future studies should compare different solutions for sharing medication information. There is a need for
studies related to the implementation of a nationally shared list: how it should be integrated and implemented
to best achieve the goal of complete and shared medication information, what the consequences are for
information security and patient safety, and what the patients’ views are on shared information on medications.
Further studies are needed to understand the need for decision support in health care and how they should be
designed as well as when and how alerts should be integrated. Clinical effects and outcomes of CDSS in
clinical practice should be studied. Overrides and reasons for them should be monitored to improve systems in
use.
Potential DRP should be further studied in the population including e.g. in the pediatric population. Different
methods for measuring DRP should be compared and assessed.
We should also monitor effects of any regulatory actions or changes in requirements regarding the medication
management process.
Researchers need to describe context and technology better to facilitate comparison [32]. Evaluation earlier in
the life cycle of technology, i.e. during planning, development or implementation instead of after large scale
implementation, would be valuable.
51

CONCLUSIONS
The conclusions from each of the six studies in the thesis:
I. Swedish community pharmacists are generally satisfied with ePrescribing, including the transfer of
ePrescriptions, electronic storing of prescriptions and to a lower degree mail order prescriptions.
II. A vast majority of Swedish patients had positive attitudes towards ePrescriptions and electronic storing
of prescriptions. However, a need for extended information regarding ePrescribing was identified.
III. After the implementation of new information systems for dispensing prescriptions at pharmacies in
Sweden, weaknesses related to reliability, functionality and usability were identified and could affect
patient safety. The weaknesses of the systems seem to result from the limited time for the development
and implementation, the lack of comprehensive and evidence-based requirements for dispensing
systems, and the unclear distribution of quality assurance responsibilities among involved stakeholders.
IV. Physicians perceived a regionally shared medication list as increasing the availability of the information
about current prescriptions and potentially the accuracy but may decrease the confidentiality of
information.
V. EES detected potential DRP in the majority of patients with MDDD. The number of potential DRP
was associated with the number of drugs, age, gender, and type of medication.
VI. In most patients with MDDD, EES detected potential DRP with many of the alerts regarded as
clinically relevant and some followed by measurable changes in drug treatment. The alerts from EES
might be useful for physicians by providing alerts for different kinds of DRP.
In summary, we found that IT has become a natural and necessary part of medication in Sweden but several
problems remain to be solved. For an improved eMedication, we need a holistic approach that combines
aspects of technology, users, and organizations in development and implementation of IT as well as evaluation.
The thesis suggests a need for improved sharing of information and support for decision making, coordination,
and education, as well as clarification of responsibilities among involved actors in order to employ appropriate
IT in the medication management process. We suggest collaborative strategic work and that the relevant
authorities set up guidelines and requirements for IT in the medication management process.
52

ACKNOWLEDGEMENTS
I'm deeply grateful for this journey as a PhD student, for the possibility to learn about medication, eHealth,
research, and even about myself, but primarily for all the people I've had the privilege to meet and work with in
different ways. This thesis was carried out at the eHealth Institute, Linnaeus University. During my time as a
PhD student I've worked with many people outside the University from different settings: before the re-
regulation Apoteket AB initiated and financed the first two studies, Medical Products Agency
(Läkemedelsverket) initiated and financed the third study but have also been the main financer for my entire
time as a PhD student, The Civil Contingencies Agency (Myndigheten för samhällsskydd och beredskap)
initiated and partly financed the fourth study, and the eHealth Agency (eHälsomyndigheten) initiated and
partly financed the fifth and sixth study. It has been really valuable for me to work with people from all of these
settings to get their quite different perspectives on this field. I believe it has made view medication
management and eHealth in a wider perspective.
Many people have played a significant part in getting me where I am today. There are more to thank than I
have room for here, but especially I want to thank:
Göran Petersson, my main supervisor, for making the eHealth institute what it is today, for believing in me and
giving me this fantastic opportunity, for your excellent support and guidance every step of the way, and for
making me feel like I could always get your full attention when needed even though I know you had hundreds
of other things on your plate.
Lina Hellström, my co-supervisor and friend, for your encouragement and help from the start, for being the one
who could always give me a good answer to all of my stupid questions especially in the beginning, and for being
a role model to me.
Bo Hovstadius, my co-supervisor, for your support and truly excellent feedback on manuscripts and my thesis,
and for reminding me (at least trying) to take a step back when work has become a bit too stressful.
Sven Tågerud, my co-supervisor, for sharing your wisdom, helping and guiding me through my time as a PhD
student but also for being one of my favorite teachers during my five years of education in pharmacy and
biomedical science before this.
53

Birgit Eiermann, my co-author, who I worked very closely with during the past two years and has become like
my fifth supervisor and even a valued friend, for sharing your knowledge and experiences, and for great
collaboration as well as company during the conference in Dublin (even though it didn't go as planned…).
Bengt Åstrand, Tony Rydberg, and Sofie Nyström, my co-authors, for letting me be a part of your team during the
first two studies, sharing your knowledge on ePrescribing, pharmacy and research.
Anders Ekedahl, my co-author, for valuable advice and support during several of my studies, and for sharing
your knowledge.
Mats Ohlson, my co-author, for support during the third study, for sharing your knowledge on safety, quality
assurance and medical devices and giving me a new perspective on this field.
Bodil Lidström, my co-author, for letting me in on the EES studies, for your valuable advice and warming
encouragement.
Yngve Gustavsson, my co-author, for sharing your expertise in geriatric medicine and valuable feedback on the
manuscript.
Tom Andersson, for opening my eyes to information security through practical and down-to-earth discussions,
and for your inspiration and contagious enthusiasm.
Elizabeth Hanson, my co-author, for your advice regarding qualitative research as well as excellent language
editing, and for fantastic help and encouragement these last weeks of thesis writing.
I would also like to thank all of my co-workers and friends at the eHealth institute (old and new), for
interesting and fun discussions during seminars lunch or “fika”, for all the laughs, for giving me feedback and
advice during my work, for sharing your knowledge with me, for supporting me, and for making it such a nice
and warm (despite the occasional need for mittens) environment to work in. Anna-Lena, Clara, Lisa, Malin,
Hanna, Diana, Nils, Victoria, Jean, Birgitta, Sten-Erik, Pauline, Gunnel, My, Alexandra, Alastair, Nadja, Lena,
Annika, Thomas, Benny, Pia, Tove and many others. You have made it a true pleasure to come to work!
Abdul Aziz Ali, for helping me with statistical advice during several of the studies.
Henry Potts, for language editing one of my manuscripts as well as the thesis.
Nisse Nilsson, for helping me capture eMedication in pictures, including the picture for the thesis cover.
SINGS (Swedish Interdisciplinary Graduate School in Register-Based Research) and SFMI (Svensk Förening
för Medicinsk Informatik) for financial support during courses and conferences.
All the respondents or others involved in the studies, for contributing with their valuable time.
54
I would also like to thank all of the people I’ve been privileged to meet, and even call my friends, during my five
years of education here at Linnaeus University: Elina, Lasse, Anna E, Per, Stina, Anna P, Sofie, Madeleine, Erika
and many others. Norrgård will always have a special place in my heart! I’ve meet many fantastic people during
conferences or during PhD-courses at other Universities as well. One of them I would like to thank especially:
Anton Pottegård, for being a true inspiration with your extreme productivity yet friendly and helpful way. I hope
we do get time for that pharmaepi collaboration we’ve been talking about for years now that we both get our
PhD.
I also want to express my gratitude to my friends outside of work and education, Fanny, Afsaneh, Jonas, Jerry,
Sofia, Lisa, Linnea, and many others, for sticking with me despite my lack of time. I hope you all know how
much you mean to me. I enjoy every minute of it when we do get to meet, and even when we are not together I
feel warm and happy just by knowing that you are there for me.
To my amazing beloved big family! Thank you for being who you are, making me who I am, and sharing your
creative energy, enthusiasm and love. We may have different family names but to me all of you are family:
Hammar, Lövström, Nordin, Jönsson, Svahnberg, Cronström, Barimani, Ekberg, Ottosson, and Nilsson as well as
bonus members with other names. You are too many to mention each one. However, there are four names I
have to mention:
My deepest gratitude goes out to my parents, my mother Ina and father Benny, for encouraging and helping me
ever since I came into this world, for always being there for me when I really need you, and for actually being
two of my closest friends that I love spending time with.
My son, Milo, who came into this world in the middle of my time as a PhD student, for keeping me down-to-
earth and reminding me of what really matters in life. You are the best thing that ever happened to me and I
love you more than I can ever explain!
Last but certainly not least, my beloved husband Mats, my closest friend and the love of my life, who has
encouraged me and held my hand every step of the way for the past 14 years. Thank you for your endless love
and support! I love you and look forward to spending more time together now that I finally finish my thesis.
From the bottom of my heart I thank you all!
55

REFERENCES
1. Topinkova E, Baeyens JP, Michel JP, Lang PO. Evidence-based strategies for the optimization of
pharmacotherapy in older people. Drugs Aging. 2012;29(6):477-494.
2. van den Bemt PM, Egberts TC, de Jong-van den Berg LT, Brouwers JR. Drug-related problems in
hospitalised patients. Drug Saf. 2000;22(4):321-333.
3. Avery AJ, Sheikh A, Hurwitz B, Smeaton L, Chen YF, Howard R, et al. Safer medicines
management in primary care. Br J Gen Pract. 2002;52 Suppl:S17-22.
4. Salvi F, Marchetti A, D'Angelo F, Boemi M, Lattanzio F, Cherubini A. Adverse drug events as a
cause of hospitalization in older adults. Drug Saf. 2012;35 Suppl 1:29-45.
5. Bates DW, Cohen M, Leape LL, Overhage JM, Shabot MM, Sheridan T. White paper - Reducing
the frequency of errors in medicine using information technology. J Am Med Inform Assoc. 2001;8(4):299-308.
6. Forni A, Chu HT, Fanikos J. Technology utilization to prevent medication errors. Curr Drug Saf.
2010;5(1):13-18.
7. Black AD, Car J, Pagliari C, Anandan C, Cresswell K, Bokun T, et al. The impact of eHealth on
the quality and safety of health care: a systematic overview. PLoS Med. 2011;8(1):e1000387.
8. McKibbon KA, Lokker C, Handler SM, Dolovich LR, Holbrook AM, O'Reilly D, et al. The
effectiveness of integrated health information technologies across the phases of medication management: a
systematic review of randomized controlled trials. J Am Med Inform Assoc. 2012;19(1):22-30.
9. Appari A, Carian EK, Johnson ME, Anthony DL. Medication administration quality and health
information technology: a national study of US hospitals. J Am Med Inform Assoc. 2012;19(3):360-367.
10. European Commission. HORIZON 2020 - The EU Framework Programme for Research and
Innovation [cited 2014 2014-09-01]. Available from: http://ec.europa.eu/programmes/horizon2020/en/h2020-
section/health-demographic-change-and-wellbeing.
11. Socialdepartementet. Nationell eHälsa - strategin för tillgänglig och säker information inom vård
och omsorg. 2010.
12. Regeringskansliet. Nationella Läkemedelsstrategin. 2011.
13. Coiera E, Westbrook J, Wyatt J. The safety and quality of decision support systems. Yearb Med
Inform. 2006:20-25.
14. Huckvale C, Car J, Akiyama M, Jaafar S, Khoja T, Bin Khalid A, et al. Information technology for
patient safety. Qual Saf Health Care. 2010;19 Suppl 2:i25-33.
56

15. Garg AX, Adhikari NK, McDonald H, Rosas-Arellano MP, Devereaux PJ, Beyene J, et al. Effects
of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic
review. JAMA. 2005;293(10):1223-1238.
16. McKibbon KA, Lokker C, Handler SM, Dolovich LR, Holbrook AM, O'Reilly D, et al. Enabling
medication management through health information technology (Health IT). Evid Rep Technol Assess (Full Rep).
2011(201):1-951.
17. Cresswell KM, Bates DW, Sheikh A. Ten key considerations for the successful implementation and
adoption of large-scale health information technology. J Am Med Inform Assoc. 2013;20(e1):e9-e13.
18. Karsh BT, Weinger MB, Abbott PA, Wears RL. Health information technology: fallacies and sober
realities. J Am Med Inform Assoc. 2010;17(6):617-623.
19. Ammenwerth E, Graber S, Herrmann G, Burkle T, Konig J. Evaluation of health information
systems-problems and challenges. Int J Med Inform. 2003;71(2-3):125-135.
20. Rochon PA, Gurwitz JH. Optimising drug treatment for elderly people: the prescribing cascade.
BMJ. 1997;315(7115):1096-1099.
21. Classen DC, Metzger J. Improving medication safety: the measurement conundrum and where to
start. Int J Qual Health Care. 2003;15 Suppl 1:i41-47.
22. Haider SI, Johnell K, Weitoft GR, Thorslund M, Fastbom J. The influence of educational level on
polypharmacy and inappropriate drug use: a register-based study of more than 600,000 older people. J Am Geriatr
Soc. 2009;57(1):62-69.
23. Johnell K, Weitoft GR, Fastbom J. Sex differences in inappropriate drug use: a register-based study
of over 600,000 older people. Ann Pharmacother. 2009;43(7):1233-1238.
24. Hovstadius B, Hovstadius K, Astrand B, Petersson G. Increasing polypharmacy - an individual-
based study of the Swedish population 2005-2008. BMC Clin Pharmacol. 2010;10:16.
25. Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA. Recent patterns of medication
use in the ambulatory adult population of the United States: the Slone survey. JAMA. 2002;287(3):337-344.
26. Qato DM, Alexander GC, Conti RM, Johnson M, Schumm P, Lindau ST. Use of prescription and
over-the-counter medications and dietary supplements among older adults in the United States. JAMA.
2008;300(24):2867-2878.
27. Holloway K, Dijk Lv. The world medicines situation 2011 - Rational use of medicines. Geneva:
2011.
28. Astrand E, Astrand B, Antonov K, Petersson G. Potential drug interactions during a three-decade
study period: a cross-sectional study of a prescription register. Eur J Clin Pharmacol. 2007;63(9):851-859.
29. Johnell, Klarin. The relationship between number of drugs and potential drug-drug interactions in
the elderly: a study of over 600 000 elderly patients from the swedish prescribed drug register. Drug Safety.
2007;30(10):911-918.
30. Espinosa-Bosch M, Santos-Ramos B, Gil-Navarro MV, Santos-Rubio MD, Marin-Gil R,
Villacorta-Linaza P. Prevalence of drug interactions in hospital healthcare. Int J Clin Pharm. 2012;34(6):807-817.
57

31. Clyne B, Bradley MC, Hughes C, Fahey T, Lapane KL. Electronic prescribing and other forms of
technology to reduce inappropriate medication use and polypharmacy in older people: a review of current evidence.
Clin Geriatr Med. 2012;28(2):301-322.
32. Motulsky A, Lamothe L, Sicotte C. Impacts of second-generation electronic prescriptions on the
medication management process in primary care: a systematic review. Int J Med Inform. 2013;82(6):473-491.
33. Teinila T, Kaunisvesi K, Airaksinen M. Primary care physicians' perceptions of medication errors
and error prevention in cooperation with community pharmacists. Res Social Adm Pharm. 2011;7(2):162-179.
34. Westerlund T, Gelin U, Pettersson E, Skarlund F, Wagstrom K, Ringbom C. A retrospective
analysis of drug-related problems documented in a national database. Int J Clin Pharm. 2013;35(2):202-209.
35. Juurlink DN, Mamdani M, Kopp A, Laupacis A, Redelmeier DA. Drug-drug interactions among
elderly patients hospitalized for drug toxicity. JAMA. 2003;289(13):1652-1658.
36. Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a
meta-analysis of prospective studies. JAMA. 1998;279(15):1200-1205.
37. Strandell J, Wahlin S. Pharmacodynamic and pharmacokinetic drug interactions reported to
VigiBase, the WHO global individual case safety report database. Eur J Clin Pharmacol. 2011;67(6):633-641.
38. Jonsson AK, Spigset O, Tjaderborn M, Druid H, Hagg S. Fatal drug poisonings in a Swedish
general population. BMC Clin Pharmacol. 2009;9:7.
39. Tache SV, Sonnichsen A, Ashcroft DM. Prevalence of adverse drug events in ambulatory care: a
systematic review. Ann Pharmacother. 2011;45(7-8):977-989.
40. Wester K, Jonsson AK, Spigset O, Druid H, Hagg S. Incidence of fatal adverse drug reactions: a
population based study. Br J Clin Pharmacol. 2008;65(4):573-579.
41. Jonsson AK, Hakkarainen KM, Spigset O, Druid H, Hiselius A, Hagg S. Preventable drug related
mortality in a Swedish population. Pharmacoepidemiol Drug Saf. 2010;19(2):211-215.
42. Howard RL, Avery AJ, Howard PD, Partridge M. Investigation into the reasons for preventable
drug related admissions to a medical admissions unit: observational study. Qual Saf Health Care. 2003;12(4):280-
285.
43. Strandell J, Bate A, Lindquist M, Edwards IR. Drug-drug interactions - a preventable patient safety
issue? Br J Clin Pharmacol. 2008;65(1):144-146.
44. Keers RN, Williams SD, Cooke J, Ashcroft DM. Causes of medication administration errors in
hospitals: a systematic review of quantitative and qualitative evidence. Drug Saf. 2013;36(11):1045-1067.
45. Rancourt C, Moisan J, Baillargeon L, Verreault R, Laurin D, Gregoire JP. Potentially inappropriate
prescriptions for older patients in long-term care. BMC Geriatr. 2004;4:9.
46. Spinewine A, Schmader KE, Barber N, Hughes C, Lapane KL, Swine C, et al. Appropriate
prescribing in elderly people: how well can it be measured and optimised? Lancet. 2007;370(9582):173-184.
47. Kimland EE. Drug treatment in children with focus on off-label drug use (Dissertation): Karolinska
Institutet, Stockholm, Sweden; 2010.
58

48. Johnell K, Fastbom J. Multi-dose drug dispensing and inappropriate drug use: A nationwide
register-based study of over 700000 elderly. Scand J Prim Health Care. 2008;26(2):86-91.
49. Sjoberg C, Edward C, Fastbom J, Johnell K, Landahl S, Narbro K, et al. Association between multi-
dose drug dispensing and quality of drug treatment--a register-based study. PLoS One. 2011;6(10):e26574.
50. Wallerstedt SM, Fastbom J, Johnell K, Sjoberg C, Landahl S, Sundstrom A. Drug treatment in
older people before and after the transition to a multi-dose drug dispensing system--a longitudinal analysis. PLoS
One. 2013;8(6):e67088.
51. Sinnemaki J, Sihvo S, Isojarvi J, Blom M, Airaksinen M, Mantyla A. Automated dose dispensing
service for primary healthcare patients: a systematic review. Syst Rev. 2013;2:1.
52. Gerber Andreas SB, Lauterbach Karl W, Stock Stephanie,, Buscher Guido RT, Lungen Markus
Evaluation of multi-dose repackaging for individual patients in long-term care institutions: savings from the
perspective of statutory health insurance in Germany. Int J Pharm Pract. 2008;16:387–394.
53. Sjoberg C, Ohlsson H, Wallerstedt SM. Association between multi-dose drug dispensing and drug
treatment changes. Eur J Clin Pharmacol. 2012;68(7):1095-1101.
54. Bastholm Rahmner P. Doctors and Drugs - How Swedish Emergency and Family Physicians
Understand Drug Prescribing (dissertation). Stockholm: Karolinska Institutet; 2009.
55. Rahmner PB, Gustafsson LL, Holmstrom I, Rosenqvist U, Tomson G. Whose job is it anyway?
Swedish general practitioners' perception of their responsibility for the patient's drug list. Ann Fam Med.
2010;8(1):40-46.
56. Ljungberg C. Prerequisites and responsibility for appropriate prescribing - the prescribers view
(Dissertation). Uppsala: Uppsala Universitet; 2010.
57. Vogelsmeier A, Pepper GA, Oderda L, Weir C. Medication reconciliation: A qualitative analysis of
clinicians' perceptions. Res Social Adm Pharm. 2013;9(4):419-430.
58. Rosenthal TC. The medical home: growing evidence to support a new approach to primary care. J
Am Board Fam Med. 2008;21(5):427-440.
59. Buurma H, De Smet P, Leufkens H, Egberts A. Evaluation of the clinical value of pharmacists'
modification of prescription errors. British Journal of Clinical Pharmacology. 2004;58(5):503-511.
60. Ekedahl A. Problem prescriptions in Sweden necessitating contact with the prescriber before
dispensing. Res Social Adm Pharm. 2010;6(3):174-184.
61. Mandt I, Horn AM, Ekedahl A, Granas AG. Community pharmacists' prescription intervention
practices--exploring variations in practice in Norwegian pharmacies. Res Social Adm Pharm. 2010;6(1):6-17.
62. Peterson GM, Wu MSH, Bergin JK. Pharmacists' attitudes towards dispensing errors: their causes
and prevention. J Clin Pharm Ther. 1999;24(1):57-71.
63. Norden-Hägg A. Failure-Free pharmacies? An exploration of dispensing errors and safety culture in
swedish community pharmacies (Dissertation). Uppsala: Uppsala Universitet; 2010.
59

64. Hellstrom LM, Bondesson A, Hoglund P, Midlov P, Holmdahl L, Rickhag E, et al. Impact of the
Lund Integrated Medicines Management (LIMM) model on medication appropriateness and drug-related hospital
revisits. Eur J Clin Pharmacol. 2011;67(7):741-752.
65. Remen VM, Grimsmo A. Closing information gaps with shared electronic patient summaries: how
much will it matter? Int J Med Inform. 2011;80(11):775-781.
66. Rahmner PB, Eiermann B, Korkmaz S, Gustafsson LL, Gruven M, Maxwell S, et al. Physicians'
reported needs of drug information at point of care in Sweden. Br J Clin Pharmacol. 2012;73(1):115-125.
67. Clarke MA, Belden JL, Koopman RJ, Steege LM, Moore JL, Canfield SM, et al. Information needs
and information-seeking behaviour analysis of primary care physicians and nurses: a literature review. Health Info
Libr J. 2013;30(3):178-190.
68. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient adherence to treatment: three
decades of research. A comprehensive review. Journal of Clinical Pharmacy and Therapeutics. 2001;26(5):331-342.
69. Hassol A, Walker J, Kidder D, Rokita K. Patient experiences and attitudes about access to a patient
electronic health care record and linked web messaging. J Am Med Inform Assoc. 2004;11(6):505-513.
70. Powell JA, Darvell M, Gray JA. The doctor, the patient and the world-wide web: how the internet
is changing healthcare. J R Soc Med. 2003;96(2):74-76.
71. Umefjord G, et al. Medical text-based consultations on the Internet: A 4-year study. International
journal of medical informatics. 2008;77:114-121.
72. Umefjord G, et al. The use of an Internet-based Ask the Doctor service involving family physicians:
evaluation by a web survey. Family Practice Advance Access. 2006.
73. Montelius E, Astrand B, Hovstadius B, Petersson G. Individuals appreciate having their medication
record on the web: a survey of attitudes to a national pharmacy register. J Med Internet Res. 2008;10(4):e35.
74. Naik Panvelkar P, Saini B. Measurements of patient satisfaction with community pharmacy services:
A review. Pharmacy world and science. 2009;31:525-537.
75. Asadi-Lari M, Tamburini M, Gray D. Patients' needs, satisfaction, and health related quality of life:
towards a comprehensive model. Health Qual Life Outcomes. 2004;2:32.
76. Tully MP, Kettis A, Hoglund AT, Morlin C, Schwan A, Ljungberg C. Transfer of data or re-
creation of knowledge - experiences of a shared electronic patient medical records system. Res Social Adm Pharm.
2013;9(6):965-974.
77. Leonhardt KK, Pagel P, Bonin D, Moberg DP, Dvorak ML, Hatlie MJ. Creating an Accurate
Medication List in the Outpatient Setting Through a Patient-Centered Approach. In: Henriksen K, Battles JB,
Keyes MA, Grady ML, editors. Advances in Patient Safety: New Directions and Alternative Approaches (Vol 3:
Performance and Tools). Advances in Patient Safety. Rockville (MD)2008.
78. Fitzsimons M, Grimes T, Galvin M. Sources of pre-admission medication information:
observational study of accuracy and availability. Int J Pharm Pract. 2011;19(6):408-416.
60

79. Tamblyn R, Poissant L, Huang A, Winslade N, Rochefort CM, Moraga T, et al. Estimating the
information gap between emergency department records of community medication compared to on-line access to the
community-based pharmacy records. J Am Med Inform Assoc. 2014;21(3):391-398.
80. Manias E. Detection of medication-related problems in hospital practice: a review. Br J Clin
Pharmacol. 2013;76(1):7-20.
81. Hamilton H, Gallagher P, Ryan C, Byrne S, O'Mahony D. Potentially inappropriate medications
defined by STOPP criteria and the risk of adverse drug events in older hospitalized patients. Arch Intern Med.
2011;171(11):1013-1019.
82. Marcum ZA, Handler SM, Wright R, Hanlon JT. Interventions to improve suboptimal prescribing
in nursing homes: A narrative review. Am J Geriatr Pharmacother. 2010;8(3):183-200.
83. Ammenwerth E, Schnell-Inderst P, Machan C, Siebert U. The effect of electronic prescribing on
medication errors and adverse drug events: a systematic review. J Am Med Inform Assoc. 2008;15(5):585-600.
84. Jaspers MW, Smeulers M, Vermeulen H, Peute LW. Effects of clinical decision-support systems on
practitioner performance and patient outcomes: a synthesis of high-quality systematic review findings. J Am Med
Inform Assoc. 2011;18(3):327-334.
85. Hemens BJ, Holbrook A, Tonkin M, Mackay JA, Weise-Kelly L, Navarro T, et al. Computerized
clinical decision support systems for drug prescribing and management: a decision-maker-researcher partnership
systematic review. Implement Sci. 2011;6:89.
86. Hellstrom L, Waern K, Montelius E, Astrand B, Rydberg T, Petersson G. Physicians' attitudes
towards ePrescribing--evaluation of a Swedish full-scale implementation. BMC Med Inform Decis Mak. 2009;9(37
%U http://www.biomedcentral.com/1472-6947/9/37):37.
87. Odukoya OK, Chui MA. e-Prescribing: characterisation of patient safety hazards in community
pharmacies using a sociotechnical systems approach. BMJ Qual Saf. 2013;22(10):816-825.
88. Marceglia S, Mazzola L, Bonacina S, Tarquini P, Donzelli P, Pinciroli F. A comprehensive e-
prescribing model to allow representing, comparing, and analyzing available systems. Methods Inf Med.
2013;52(3):199-219.
89. Kierkegaard P. Electronic health record: Wiring Europe’s healthcare. Computer Law & Security
Review. 2011;27(5):503-515.
90. Åstrand B. ePrescribing - Studies in pharmacoinformatics (Dissertation). Kalmar: University of
Kalmar; 2007.
91. Parv L, Kruus P, Motte K, Ross P. An evaluation of e-prescribing at a national level. Inform Health
Soc Care. 2014:1-18.
92. Kierkegaard P. E-Prescription across Europe. Health and Technology. 2012;3(3):205-219.
93. Hypponen H, Reponen J, Laaveri T, Kaipio J. User experiences with different regional health
information exchange systems in Finland. Int J Med Inform. 2013.
94. Åstrand B, Montelius E, Petersson G, Ekedahl A. Assessment of ePrescription quality: an
observational study at three mail-order pharmacies. BMC Medical Informatics and Decision Making. 2009;9.
61

95. Murray MD, Loos B, Tu W, Eckert GJ, Zhou XH, Tierney WM. Effects of computer-based
prescribing on pharmacist work patterns. J Am Med Inform Assoc. 1998;5(6):546-553.
96. Papshev D, Peterson AM. Electronic prescribing in ambulatory practice: promises, pitfalls, and
potential solutions. The American Journal of Managed Care. 2001;7(7):725-736.
97. Redwood S, Rajakumar A, Hodson J, Coleman JJ. Does the implementation of an electronic
prescribing system create unintended medication errors? A study of the sociotechnical context through the analysis of
reported medication incidents. BMC Med Inform Decis Mak. 2011;11:29.
98. Carling CL, Kirkehei I, Dalsbo TK, Paulsen E. Risks to patient safety associated with
implementation of electronic applications for medication management in ambulatory care--a systematic review.
BMC Med Inform Decis Mak. 2013;13:133.
99. Ohlund SE, Astrand B, Petersson G. Improving Interoperability in ePrescribing. Interact J Med
Res. 2012;1(2):e17.
100. Jerlvall L, Pehrsson T. eHälsa i landstingen. SLIT 2013.
101. Janols R, Lind T, Goransson B, Sandblad B. Evaluation of user adoption during three module
deployments of region-wide electronic patient record systems. Int J Med Inform. 2014;83(6):438-449.
102. Olsson E, Ingman P, Ahmed B, Kalvemark Sporrong S. Pharmacist-patient communication in
Swedish community pharmacies. Res Social Adm Pharm. 2014;10(1):149-155.
103. Hammar T, Peterson G. Receptexpeditionssystem i Sverige. eHälsoinstitutet, Linnéuniversitetet,
Kalmar: 2012.
104. Cohen MR, Smetzer JL, Westphal JE, Comden SC, Horn DM. Risk models to improve safety of
dispensing high-alert medications in community pharmacies. J Am Pharm Assoc (2003). 2012;52(5):584-602.
105. James KL, Barlow D, McArtney R, Hiom S, Roberts D, Whittlesea C. Incidence, type and causes
of dispensing errors: a review of the literature. Int J Pharm Pract. 2009;17(1):9-30.
106. Odukoya O, Chui MA. Retail pharmacy staff perceptions of design strengths and weaknesses of
electronic prescribing. J Am Med Inform Assoc. 2012;19(6):1059-1065.
107. Volmer D, Haavik S, Ekedahl A. Use of a generic protocol in documentation of prescription errors
in Estonia, Norway and Sweden. Pharm Pract (Granada). 2012;10(2):72-77.
108. Grossman JM, Cross DA, Boukus ER, Cohen GR. Transmitting and processing electronic
prescriptions: experiences of physician practices and pharmacies. J Am Med Inform Assoc. 2012;19(3):353-359.
109. Hines LE, Saverno KR, Warholak TL, Taylor A, Grizzle AJ, Murphy JE, et al. Pharmacists'
awareness of clinical decision support in pharmacy information systems: an exploratory evaluation. Res Social Adm
Pharm. 2011;7(4):359-368.
110. Norden-Hagg A, Andersson K, Kalvemark-Sporrong S, Ring L, Kettis-Lindblad A. Reducing
dispensing errors in Swedish pharmacies: the impact of a barrier in the computer system. Qual Saf Health Care.
2010;19(6):e22.
62

111. Eiermann Birgit, Rahmner Pia Bastholm, Korkmaz Seher, al. E. Knowledge Bases for Clinical
Decision Support in Drug Prescribing – Development, Quality Assurance, Management, Integration,
Implementation and Evaluation of Clinical Value, . In: Jao CS, editor. Decision Support Systems: InTech.
112. Kuperman GJ, Bobb A, Payne TH, Avery AJ, Gandhi TK, Burns G, et al. Medication-related
clinical decision support in computerized provider order entry systems: a review. J Am Med Inform Assoc.
2007;14(1):29-40.
113. Robertson J, Walkom E, Pearson SA, Hains I, Williamsone M, Newby D. The impact of pharmacy
computerised clinical decision support on prescribing, clinical and patient outcomes: a systematic review of the
literature. Int J Pharm Pract. 2010;18(2):69-87.
114. Coleman JJ, van der Sijs H, Haefeli WE, Slight SP, McDowell SE, Seidling HM, et al. On the
alert: future priorities for alerts in clinical decision support for computerized physician order entry identified from a
European workshop. BMC Med Inform Decis Mak. 2013;13:111.
115. Ranji SR, Rennke S, Wachter RM. Computerised provider order entry combined with clinical
decision support systems to improve medication safety: a narrative review. BMJ Qual Saf. 2014.
116. Teich JM, Osheroff JA, Pifer EA, Sittig DF, Jenders RA. Clinical decision support in electronic
prescribing: recommendations and an action plan: report of the joint clinical decision support workgroup. J Am Med
Inform Assoc. 2005;12(4):365-376.
117. Jani YH, Barber N, Wong IC. Characteristics of clinical decision support alert overrides in an
electronic prescribing system at a tertiary care paediatric hospital. Int J Pharm Pract. 2011;19(5):363-366.
118. Nanji KC, Slight SP, Seger DL, Cho I, Fiskio JM, Redden LM, et al. Overrides of medication-
related clinical decision support alerts in outpatients. J Am Med Inform Assoc. 2014;21(3):487-491.
119. van der Sijs H, Aarts J, Vulto A, Berg M. Overriding of drug safety alerts in computerized physician
order entry. J Am Med Inform Assoc. 2006;13(2):138-147.
120. van der Sijs H, Mulder A, van Gelder T, Aarts J, Berg M, Vulto A. Drug safety alert generation and
overriding in a large Dutch university medical centre. Pharmacoepidemiol Drug Saf. 2009;18(10):941-947.
121. Ojeleye O, Avery A, Gupta V, Boyd M. The evidence for the effectiveness of safety alerts in
electronic patient medication record systems at the point of pharmacy order entry: a systematic review. BMC Med
Inform Decis Mak. 2013;13:69.
122. Horsky J, Phansalkar S, Desai A, Bell D, Middleton B. Design of decision support interventions for
medication prescribing. Int J Med Inform. 2013;82(6):492-503.
123. Sjoborg B, Backstrom T, Arvidsson LB, Andersen-Karlsson E, Blomberg LB, Eiermann B, et al.
Design and implementation of a point-of-care computerized system for drug therapy in Stockholm metropolitan
health region--Bridging the gap between knowledge and practice. Int J Med Inform. 2007;76(7):497-506.
124. Eliasson M, Bastholm P, Forsberg P, Henriksson K, Jacobson L, Nilsson A, et al. Janus
computerised prescribing system provides pharmacological knowledge at point of care - design, development and
proof of concept. Eur J Clin Pharmacol. 2006;62(4):251-258.
63

125. Bottiger Y, Laine K, Andersson ML, Korhonen T, Molin B, Ovesjo ML, et al. SFINX-a drug-drug
interaction database designed for clinical decision support systems. Eur J Clin Pharmacol. 2009;65(6):627-633.
126. Wass S, Carlsson B, Vimarlund V, Korkmaz S, Shemeikka T, Veg A. Towards capturing innovation
effects of a CDSS (NjuRen). Stud Health Technol Inform. 2013;192:1049.
127. Hammar T, Hovstadius B, Lidström B, Petersson G, Eiermann B. Potential drug related problems
detected by electronic expert support system in patients with multi-dose drug dispensing. Int J Clin Pharm. 2014.
128. Läkemedelsverket. Utvärdering av funktioner i EES. Uppsala: 2012 20120330. Report No.
129. Keers RN, Williams SD, Cooke J, Walsh T, Ashcroft DM. Impact of Interventions Designed to
Reduce Medication Administration Errors in Hospitals: A Systematic Review. Drug Saf. 2014.
130. Pyper C, Amery J, Watson M, Crook C. Patients' experiences when accessing their on-line
electronic patient records in primary care. British Journal of General Practice. 2004;54:38-43.
131. Montelius E, Åstrand B, Hovstadius B, Petersson G. Individuals appreciate having their medication
record on the Web: A survey of attitudes to a national pharmacy register. Journal of Medical Internet Research.
2008;10(4 %U http://www.jmir.org/2008/4/e35/).
132. Scandurra I, Holgersson J, Lind T, Myreteg G. Development of Patient Access to Electronic Health
Records as a Step towards Ubiquitous Public eHealth. European Journal of ePractice. 2013(20).
133. Porteous T, Bond C, Robertson R. Electronic transfer of prescription-related information:
comparing views of patients, general practitioners, and pharmacists. British Journal of General Practice.
2003;53:204-209.
134. Umefjord G, et al. Reasons for consulting a doctor on the Internet: Web survey of users of an ask
the doctor service. Journal of Medical Internet Research. 2003;5(4):e26.
135. Janzek-Hawlat S, Ammenwerth E, Dorda W, Duftschmid G, Hackl W, Horbst A, et al. The
Austrian e-Medikation pilot evaluation: lessons learned from a national medication list. Stud Health Technol
Inform. 2013;192:347-351.
136. Stock R, Mahoney ER, Gauthier D, Center L, Minniti M, Scott J, et al. Developing a Community-
Wide Electronic Shared Medication List. In: Henriksen K, Battles JB, Keyes MA, Grady ML, editors. Advances in
Patient Safety: New Directions and Alternative Approaches (Vol 4: Technology and Medication Safety). Advances
in Patient Safety. Rockville (MD)2008.
137. Tamblyn R, Huang AR, Meguerditchian AN, Winslade NE, Rochefort C, Forster A, et al. Using
novel Canadian resources to improve medication reconciliation at discharge: study protocol for a randomized
controlled trial. Trials. 2012;13:150.
138. Weeks DL, Corbett CF, Stream G. Beliefs of ambulatory care physicians about accuracy of patient
medication records and technology-enhanced solutions to improve accuracy. J Healthc Qual. 2010;32(5):12-21.
139. Keers RN, Williams SD, Cooke J, Ashcroft DM. Prevalence and nature of medication
administration errors in health care settings: a systematic review of direct observational evidence. Ann Pharmacother.
2013;47(2):237-256.
64

140. Ekedahl A, Brosius H, Jonsson J, Karlsson H, Yngvesson M. Discrepancies between the electronic
medical record, the prescriptions in the Swedish national prescription repository and the current medication reported
by patients. Pharmacoepidemiol Drug Saf. 2011;20(11):1177-1183.
141. Ekedahl A, Tärning E, Rutberg H, Yngevesson M, Hoffman M. [In Swedish] [Errors in the
pharmaceutical and prescription lists are very common. Patient data on prescriptions compared with medical records
and prescription database] Mycket vanligt med fel i läkemedels- och receptlistorna. Läkartidningen. 2012;109(20-
21).
142. Wettermark B, Hammar N, Fored CM, Leimanis A, Otterblad Olausson P, Bergman U, et al. The
new Swedish Prescribed Drug Register--opportunities for pharmacoepidemiological research and experience from
the first six months. Pharmacoepidemiol Drug Saf. 2007;16(7):726-735.
143. CeHis. En samlad läkemedelslista: Beskrivning av Nationell ordinationsdatabas, NOD.
Stockholm2013.
144. Kierkegaard P. eHealth in Denmark: A Case Study. J Med Syst. 2013;37(6):9991.
145. Deutsch E, Duftschmid G, Dorda W. Critical areas of national electronic health record programs-is
our focus correct? Int J Med Inform. 2010;79(3):211-222.
146. Suna T. Finnish National Archive of Health Information (KanTa). Fujitsu Sci Tech. 2011;47(No.
1):49-57.
147. Westerlund T, Björk T. Pharmaceutical care in community pharmacies: practice and research in
Sweden. The Annals of Pharmacotherapy. 2006;40:1162-1168.
148. Koppel R, Metlay JP, Cohen A, Abaluck B, Localio AR, Kimmel SE, et al. Role of computerized
physician order entry systems in facilitating medication errors. JAMA. 2005;293(10):1197-1203.
149. van Deursen N, Buchanan WJ, Duff A. Monitoring information security risks within health care.
Computers & Security. 2013;37:31-45.
150. Örn P. IT-relaterade problem bakom ett 100-tal lex Maria-fall varje år. Läkartidningen. 2012(17).
151. Scandurra I. Störande eller stödjande? Om eHälsosystemens användbarhet 2013. 2013.
152. e-hälsokommittén. Nästa fas i e-hälsoarbetet: en diskussionspromemoria från e-hälsokommittén.
2014.
153. Statens offentliga utredningar (SOU). Rätt information på rätt plats i rätt tid - Slutbetänkande av
Utredningen om rätt information i vård och omsorg. Stockholm: 2014.
154. Neame R. Effective sharing of health records, maintaining privacy: a practical schema. Online J
Public Health Inform. 2013;5(2):217.
155. Socialstyrelsen. Informationssäkerhet - Vägledning för hantering av information inom vård och
omsorg. 2010.
156. Andersson T. Kontinuitetshantering i praktiken - Fallstudier av läkemedelshantering och
informationshantering i händelse av verksamhetsstörningar. Myndigheten för samhällsskydd och beredskap i
samverkan med Västra Götalandsregionen: 2014 2014. Report No.
65

157. Khajouei R, de Jongh D, Jaspers MW. Usability evaluation of a computerized physician order entry
for medication ordering. Stud Health Technol Inform. 2009;150:532-536.
158. Jaderlund Hagstedt L, Rudebeck CE, Petersson G. Usability of computerised physician order entry
in primary care: assessing ePrescribing with a new evaluation model. Inform Prim Care. 2011;19(3):161-168.
159. Yen PY, Bakken S. Review of health information technology usability study methodologies. J Am
Med Inform Assoc. 2012;19(3):413-422.
160. Koppel R, Wetterneck T, Telles JL, Karsh BT. Workarounds to barcode medication administration
systems: their occurrences, causes, and threats to patient safety. J Am Med Inform Assoc. 2008;15(4):408-423.
161. Nilsson L, Eriksén S, Borg C. Social Challenges When Implementing Information Systems in
Everyday Work in a Nursing Context. CIN: Computers, Informatics, Nursing. 2014.
162. Statens offentliga utredningar (SOU). Gör det enklare! - Slutbetänkande av Statens vård- och
omsorgsutredning. Stockholm: 2012.
163. Medical_Products_Agency. Medical Information Systems – guidance for qualification and
classification of standalone software with a medical purpose. Uppsala, Sweden: 2012.
164. Ericson L, Schönström N, Petersson G. Klinisk utvärdering av medicinska informationssystem-
Fokus på elektroniska patientjournalsystem. eHälsoinstitutet, Linnéuniversitetet, Kalmar: 2014.
165. eHealth Agency. Approval of interface and format [In Swedish] 2014 [2014-05-22]. Available from:
http://www.ehalsomyndigheten.se/ehalsotjanster/Teknisk-infrastruktur/godkannande/.
166. Ammenwerth E, Brender J, Nykanen P, Prokosch HU, Rigby M, Talmon J, et al. Visions and
strategies to improve evaluation of health information systems. Reflections and lessons based on the HIS-EVAL
workshop in Innsbruck. Int J Med Inform. 2004;73(6):479-491.
167. Bonnabry P, Despont-Gros C, Grauser D, Casez P, Despond M, Pugin D, et al. A risk analysis
method to evaluate the impact of a computerized provider order entry system on patient safety. J Am Med Inform
Assoc. 2008;15(4):453-460.
168. Jamieson S. Likert scales: how to (ab)use them. Med Educ. 2004;38(12):1217-1218.
169. Coxe S, West SG, Aiken LS. The analysis of count data: a gentle introduction to poisson regression
and its alternatives. J Pers Assess. 2009;91(2):121-136.
170. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures
and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105-112.
171. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-
340.
172. Steinschaden T, Petersson G, Åstrand B. Physicians' attitudes towards ePrescribing: A comparative
web survey in Austria and Sweden. Informatics in Primary Care. 2010;17(4):241-248.
173. Motulsky A, Winslade N, Tamblyn R, Sicotte C. The impact of electronic prescribing on the
professionalization of community pharmacists: a qualitative study of pharmacists' perception. J Pharm Pharm Sci.
2008;11(1):131-146.
66

174. Abdel-Qader DH, Cantrill JA, Tully MP. Satisfaction predictors and attitudes towards electronic
prescribing systems in three UK hospitals. Pharm World Sci. 2010.
175. Allen AS, Sequist TD. Pharmacy dispensing of electronically discontinued medications. Ann Intern
Med. 2012;157(10):700-705.
176. Bell DS, Marken RS, Meili RC, Wang CJ, Rosen M, Brook RH, et al. Recommendations for
comparing electronic prescribing systems: results of an expert consensus process. Health Aff (Millwood). 2004;Suppl
Web Exclusives:W4-305-317.
177. Devine EB, Hollingworth W, Hansen RN, Lawless NM, Wilson-Norton JL, Martin DP, et al.
Electronic Prescribing at the Point of Care: A Time-Motion Study in the Primary Care Setting. Health Serv Res.
2009;45(1).
178. Greenhalgh T, Potts HW, Wong G, Bark P, Swinglehurst D. Tensions and paradoxes in electronic
patient record research: a systematic literature review using the meta-narrative method. Milbank Q. 2009;87(4):729-
788.
179. van Doormaal JE, van den Bemt PM, Zaal RJ, Egberts AC, Lenderink BW, Kosterink JG, et al.
The influence that electronic prescribing has on medication errors and preventable adverse drug events: an
interrupted time-series study. J Am Med Inform Assoc. 2009;16(6):816-825.
180. Westbrook JI, Reckmann M, Li L, Runciman WB, Burke R, Lo C, et al. Effects of two commercial
electronic prescribing systems on prescribing error rates in hospital in-patients: a before and after study. PLoS Med.
2012;9(1):e1001164.
181. Saverno KR, Hines LE, Warholak TL, Grizzle AJ, Babits L, Clark C, et al. Ability of pharmacy
clinical decision-support software to alert users about clinically important drug-drug interactions. J Am Med Inform
Assoc. 2011;18(1):32-37.
182. Läkemedelsverket. Jämförelse av interaktionsmodulerna i EES och SFINX. Rapport från
Läkemedelsverket 2011.
183. Seidling HM, Klein U, Schaier M, Czock D, Theile D, Pruszydlo MG, et al. What, if all alerts were
specific - estimating the potential impact on drug interaction alert burden. Int J Med Inform. 2014;83(4):285-291.
184. Riedmann D, Jung M, Hackl WO, Ammenwerth E. How to improve the delivery of medication
alerts within computerized physician order entry systems: an international Delphi study. J Am Med Inform Assoc.
2011;18(6):760-766.
185. Lindblad CI, Hanlon JT, Gross CR, Sloane RJ, Pieper CF, Hajjar ER, et al. Clinically important
drug-disease interactions and their prevalence in older adults. Clin Ther. 2006;28(8):1133-1143.
186. Horsky J, Schiff GD, Johnston D, Mercincavage L, Bell D, Middleton B. Interface design principles
for usable decision support: a targeted review of best practices for clinical prescribing interventions. J Biomed Inform.
2012;45(6):1202-1216.
187. Cheung KC, van den Bemt PM, Bouvy ML, Wensing M, De Smet PA. Medication incidents
related to automated dose dispensing in community pharmacies and hospitals - a reporting system study. PLoS One.
2014;9(7):e101686.
67
188. Wekre LJ, Melby L, Grimsmo A. Early experiences with the multidose drug dispensing system--a
matter of trust? Scand J Prim Health Care. 2011;29(1):45-50.
189. Gunnarsdotter S. Pascal stjälper mer än hjälper. Läkartidningen. 2013(5).
190. Institute of Medicine (IOM). To Err is Human: Building A Safer Health System. Washington:
National academy press; 1999.
191. Ekedahl A. Patients' information on their prescribed current treatment. Journal of pharmaceutical
health services research. 2012;3(2):79-84.
192. Indermitte J. Prevalence and patient awareness of selected potential drug interactions with self-
medication. Journal of Clinical Pharmacy and Therapeutics. 2007;32(2):149.
193. Ross SE, Todd J, Moore LA, Beaty BL. Expectations of patients and physicians regarding patient-
accessible medical records. Journal of Medical Internet Research. 2005;7(2):e13.
194. Nätverk för Sveriges läkemedelskommitteer (LOK). Patientens samlade läkemedelslista - ansvar och
riktlinjer för hantering i öppen vård. LOK:s rekommendationer om hur en samlad läkemedelslista bör hanteras 2014.
195. Planas LG, Kimberlin CL, Segal R, Brushwood DB. A pharmacist model of perceived responsibility
for drug therapy outcomes. Social Science & Medicine. 2005;60:2393-2403.
196. Harvey J, Avery AJ, Hibberd R, Barber N. Meeting user needs in national healthcare systems:
lessons from early adopter community pharmacists using the electronic prescriptions service. BMC Med Inform
Decis Mak. 2014;14:16.
197. Vincent C, Blandford A. Designing for Safety and Usability: User-Centered Techniques in Medical
Device Design Practice. Proceedings of the Human Factors and Ergonomics Society Annual Meeting September.
2011;55(1):793-797.
198. Powell J, Fitton R, Fitton C. Sharing electronic health records: the patient view. Inform Prim Care.
2006;14(1):55-57.
199. Velupillai S, Dalianis H, Hassel M, Nilsson GH. Developing a standard for de-identifying
electronic patient records written in Swedish: precision, recall and F-measure in a manual and computerized
annotation trial. Int J Med Inform. 2009;78(12):e19-26.
200. Cheung KC, van den Bemt PM, Bouvy ML, Wensing M, De Smet PA. A nationwide medication
incidents reporting system in The Netherlands. J Am Med Inform Assoc. 2011;18(6):799-804.
201. Norden-Hagg A, Kettis-Lindblad A, Ring L, Kalvemark-Sporrong S. Experiences of a nationwide
web-based system: reporting dispensing errors in Swedish pharmacies. Int J Pharm Pract. 2012;20(1):25-32.
202. Ekman E. Pharmacovigilance - spontaneous reporting in healthcare (Dissertation). Linnaeus
University Press: Linnaeus University, Kalmar; 2013.
203. Läkemedelsverkets föreskrifter om tillämpning av lagen om medicintekniska produkter på nationella
medicinska informationssystem (LVFS 2014:7), (2014).
204. Niinimaki J, Forsstrom J. Approaches for certification of electronic prescription software. Int J Med
Inform. 1997;47(3):175-182.
68

205. Savage I, Cornford T, Klecun E, Barber N, Clifford S, Franklin BD. Medication errors with
electronic prescribing (eP): Two views of the same picture. BMC Health Serv Res. 2010;10:135.
206. Ammenwerth E, Kaiser F, Wilhelmy I, Hofer S. Evaluation of user acceptance of information
systems in health care--the value of questionnaires. Stud Health Technol Inform. 2003;95:643-648.
207. Bell DS, Cretin S, Marken RS, Landman AB. A conceptual framework for evaluating outpatient
electronic prescribing systems based on their functional capabilities. J Am Med Inform Assoc. 2004;11(1):60-70.
69
