7 day services practical tips for achieving consultant review of patients within 14 hours clinical...
TRANSCRIPT

Seven Day Hospital Services Webinar Connect, Share and Learn Hosted by Sustainable Improvement NHS England South Region
January 2017
Establishing a Virtual Community for All to
Connect, Share and Learn
• Series of National and Local webinars
• Share practical examples – discuss barriers and generate improvement solutions
• NHS E Specialist Support Team - Sustainable Improvement
• Work in collaboration with NHS Improvement and the UEC Programme Board, South Region
Connect Share Learn
7 Day Hospitals – Virtual Learning
Webinar objectives
This webinar aims to provide you with:
• An overview of the updated guidance for the priority clinical standards and timing of the forthcoming self assessment survey
• Practical examples of how commissioners and acute providers are working together to support delivery of timely Consultant assessment (clinical standard 2) – their successes, challenges and opportunities
• An opportunity to ask questions of your colleagues and identify key areas of support required
Connect Share Learn
7 Day Hospitals – session objectives

Our guest speakers today are:
Connect Share Learn
7 Day Hospitals – Guest Speakers
• Sue Cottle, Programme Lead, 7 Day Services, Sustainable Improvement, NHS England South
• Celia Ingham Clark, MBE, Medical Director for Clinical Effectiveness, NHS England
• Claire Gorzanski, Head of Clinical Effectiveness, Salisbury NHS Foundation Trust
• Sam Burrows, Director of Strategy, NHS Wokingham CCG

Seven Day
Hospital
Services Clinical Standard 2 – Time to first
consultant review Celia Ingham Clark, Medical Director for Clinical Effectiveness, NHS England
The four priority clinical standards for 7 day hospital services
ensure that patients receive the same high quality assessment,
diagnosis, treatment and review in hospital on any day of the week
• Standard 2: Time to first consultant review
• Standard 5: Diagnostics
• Standard 6: Consultant directed interventions
• Standard 8: On-going review
Priority clinical
standards
Standard 2: All emergency admissions must be seen and have a thorough clinical
assessment by a suitable consultant as soon as possible but at the latest within 14
hours from the time of admission to hospital.
There is a large body of evidence associating timely consultant input to patient care with
improved outcomes. This meets with patients’ expectations and their care becomes more
effective and efficient. The Royal College of Physicians’ Acute Care Toolkit 4 suggests that
all patients admitted in an emergency should be seen promptly by a suitable consultant and
at the latest within 14 hours of admission.

Following extensive engagement with clinicians, standard 2 has
been clarified to ensure best clinical practice is supported
Time to first consultant
review
• Measured from the time of
admission to hospital rather than
the time of arrival at hospital.
• Reflects the original source
document for this standard (Royal
College of Physicians acute care
toolkit number 4).
• Aligns with pattern of emergency
patient admissions and associated
consultant staffing rosters.
• The definition of consultant remains
a doctor who has completed all of
their specialist training and been
placed on the GMC’s specialist
register
Pathways that are not
consultant-led
Patients with a clear diagnosis on a
well-defined pathway (e.g. midwife-led
maternity, simple superficial abscess
management) may have their clinical
care delegated from a consultant to
another clinician under the following
circumstances:
• A clear written local protocol agreed
within the Trust clinical governance
system and by commissioners.
• Protocol must describe actions to
take in the event of clinical concern
including rapid escalation to a
consultant where appropriate.
• Patient's care is still recorded as
being under a named consultant
(excluding patients specifically on
midwife-led care pathways)

When measured from time of admission, results from the
September 2016 7DS self-assessment survey showed that meeting
standard 2 presented the greatest challenge to trusts
Table 1: Achievement of the four individual clinical standards
Number of
trusts achieving
the standard
% of trusts
achieving the
standard
% of national
population
these trusts
serve
Standard 2: Time to
consultant review
9 6% 6%
Standard 5: Access to
diagnostic tests
8 5% 3%
Standard 6: Access to
consultant directed
interventions
80 54% 63%
Standard 8: Ongoing review 49 33% 31%
Table 2: Achievement of the four standards at different thresholds
Over 90% 70-90% 50-70% Under 50%
Standard 2: Time to
consultant review 6% 30% 53% 11%
Standard 5: Access to
diagnostic tests 3% 71% 26% 0%
Standard 6: Access to
consultant directed
interventions 63% 27% 8% 2%
Standard 8: Ongoing review 31% 45% 21% 2%

Staff rotas and working practices
Ensure acute take consultant presence from 8am to 8pm every day (especially for high volume specialties such as medicine).
On high volume units such as most AMUs use rolling ward rounds through the day to keep up with the new patients arriving.
Best clinical practice
Write into policy the expectation that patients admitted before 8pm will be seen by the evening take consultant before he/she goes home.
Ensure that handover lists used for take ward rounds include time of arrival, admission and ward for all patients to support the on take consultant to prioritise the order in which they see patients on the ward rounds.
Effective recording
Ensure that entry in the medical notes makes clear that consultant is assessing the patient and the time.
Ensure patients assessed by an appropriate consultant in ED or in clinic prior to admission to hospital are recorded as meeting the standard.
Clinical Engagement
Ensure that all team members, particularly junior doctors and senior ward nurses know the importance of a prompt consultant assessment for new and undifferentiated patients
Senior staff demonstrate commitment to the aims of the 7DS programme
Trusts could take the following steps to support delivery of
clinical standard 2, taking into account the recently published
clarifications

1
0
Northumbria NHS Trust organise their own transport for patients admitted from
home after the afternoon GP home visit so that the patient has more opportunity
to arrive at hospital before the specialty consultants leave for the day at 8pm.
When issues with flow occur the Trust adopts the following strategies: calling
specialty consultants into ED to support early assessment with a view to
reducing conversion rates and proactively sending patients from ED to specialty
wards at 11 am and 4pm to reduce congestion in A&E. This means at the
busiest times patients are still reviewed by the appropriate specialist.
Buckinghamshire Healthcare NHS Trust are making ongoing significant
efforts to improve flow, admission avoidance and rapid front door management
at Stoke Mandeville Hospital, meaning a high proportion of their patients were
admitted and reviewed within 4 hours of attendance. They also use a tracking
system and real time dashboard to ensure patients who have not been seen are
flagged.
There are examples of trusts that have implemented new ways of
working which have led to improved performance and more
patients being seen by a consultant in a timely fashion

Discussion
Please raise your hand if you have a question or comment- or write it in the chat box to ‘all participants’. When speaking please let everyone know your name, and your organisation
7 Day Hospitals – Discussion
Patient-Centred & Safe Friendly Professional Responsive
NHS 7 Day Services
Standard 2 – Time to Consultant review
Claire Gorzanski, Head of Clinical Effectiveness
27 January 2017
An outstanding experience
for every patient

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – Time to consultant review
• All emergency admissions must be seen and have a thorough clinical assessment by a suitable consultant as soon as possible but at the latest within 14 hours of arrival at hospital
• Next survey – within 14 hours of admission

Patient-Centred & Safe Friendly Professional Responsive
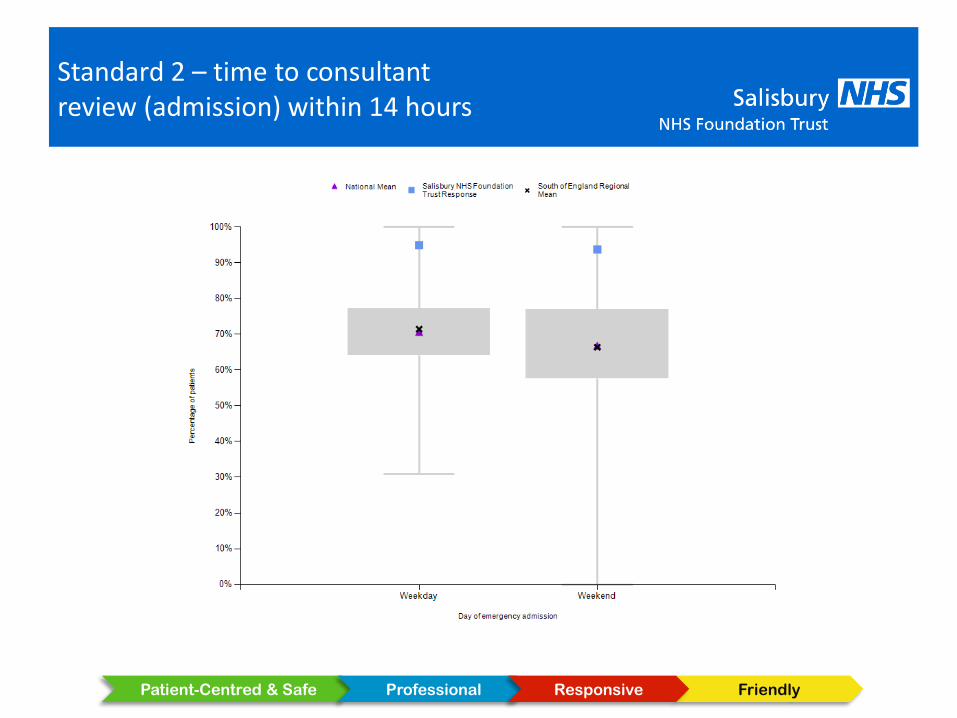
Standard 2 – Suitable consultant
A suitable consultant is one who is trained and competent in dealing with emergency and acute presentations in the speciality concerned and is able to initiate a diagnostic and treatment plan
• 89% within 14 hours of arrival
• 95% within 14 hours of admission

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – time to consultant review (arrival) within 14 hours
Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – time to consultant review (admission) within 14 hours

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – Results – are they credible?
• Clinical engagement – 2 workshops
• Culture of 7 day working accepted & good leadership
• Consultant delivered models in ED, AMU and SAU & resident paediatric consultant led model 24/7.
• Separate consultants for acute take & acute wards at weekends
• Ambulatory care pathways – VTE, TWOCs, gynaecology emergencies, plastics trauma

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – Results – are they credible?
• Understand & streamline clinical processes on admission
• Chairs & trollies in AMU/SAU
• Train nurses to take bloods & ECGs
• Laboratory turnaround for AMU/SAU 1 hour
• Consultant presence AMU 12 hrs weekday, 6 hours weekends. SAU – surgeon of the day
• AMU/SAU dashboard

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – AMU dashboard

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – SAU dashboard

Patient-Centred & Safe Friendly Professional Responsive
Standard 2 – Survey top tips
• Plan the audit
• Same auditors (all clinical) for each survey & time set aside to complete it
• Shared interpretation of a suitable consultant
• Logical paper data collection form – later validation/further analysis
• Pre-populated with date & time of arrival & admission – check against notes
• 4 week interval between sample & audit to allow for coding & reduced notes chasing (80% available)

Patient-Centred & Safe Friendly Professional Responsive
Summary
• Clinical engagement & leadership
• Culture of improvement
• Plan the audit/keep it simple
• Share the results & learning

Discussion
Please raise your hand if you have a question or comment- or write it in the chat box to ‘all participants’. When speaking please let everyone know your name, and your organisation
7 Day Hospitals – Discussion

7 Day Services in
Berkshire West –
Benefits to Collaborative
Approaches
24

Berkshire West – Background & Context
• Self contained health economy covering the area between the Berkshire /
Wiltshire border (West of Newbury) and the East of Wokingham
• Population of approx. 500,000 people
• One major acute provider – Royal Berkshire Hospital Foundation Trust
and one major Community / Mental Health provider – Berkshire
Healthcare Foundation Trust
• Four CCGs work in a very tight Federation covering this whole area
• Strong benchmark data – three of the four CCGs are in the top 5
nationally for NEL admission rate
• Receive one of the lowest funding allocations in the country – South
Reading CCG is the only CCG in England which receives less than
£1,000 per head of population
Really positive conditions for the delivery of change programmes –
including 7 Day Services
25

7 Day Services – Current Performance
Royal Berkshire Hospital – Self-certification
• Priority 1 (Std 2 – Time to First Consultant Review): Above national & regional mean
• Priority 2 (Std 5 – Access to Diagnostics): Partial Compliance
• Priority 3 (Std 6 – Access to Consultant Interventions): Fully Compliant
• Priority 4 (Std 8 – Ongoing Review): Partial Compliance
With clear trajectory agreed to full compliance by end of the current year.
26

Our overall approach to working together
• Significant cultural change underway within our local health economy
• History of joint working – Berkshire West Integration Programme
established three years ago and continues to deliver benefit
• April 2016: Established the Berkshire West Accountable Care System
• Not an ACO / vertical integration of functions
• Greater collaboration, planning over contracting, joint governance
• Deriving the maximum value from the ‘Berkshire West £’
• System wide recognition that we cannot afford constant and continued
improvement but need to delivery 5YFV priorities
• Cultural change is already delivering benefit and 7DS programme fits
within this overall framework
• Regard 7DS as a collaborative programme between the CCGs and the
Provider – not one party having primacy over the other and not the
commissioner ‘assuring’ the provider
27

Joint approach to delivery of 7 Day Services
• Recognise that our simple structure helps drive delivery of these sorts of
programmes
• Meet regularly – dependent on current challenges either monthly or
quarterly
• Defined a contractual mechanism early on but now ‘left in the drawer’ with
focus on collaboration yielding far more positive engagement and
outcomes
• Open and honest collaboration – recognise challenges and priorities
within the context of overall health economy / financial performance
• Use NHS England team wherever we can – supportive and informative
discussion – particularly where there is lack of clarity (i.e. threshold for
compliance
28

Challenges
• Lack of clarity around data, benchmarking, compliance thresholds
• Finance becoming even more scarce – investments being reserved for
maintaining the system rather than improving it
• No clear Return on Investment – appetite for incurring ‘cost’ is severely
limited
• Competing priorities for CCGs and Trust – 7DS has to fight for airtime at
an executive level
• Whole system problem – currently not coming at this with a whole system
solution (but have the structures in place should we need to)
29

Questions?
30

Discussion
Please raise your hand if you have a question or comment- or write it in the chat box to ‘all participants’. When speaking please let everyone know your name, and your organisation
7 Day Hospitals – Discussion

Thank you for joining the South Region Webinar the links to the recording will be sent out shortly For more information: [email protected] Programme Lead [email protected] Senior Improvement Manager (South Central & Wessex) [email protected] Improvement Manager (South East) [email protected] Improvement Manager (South West)
Connect Share Learn
7 Day Hospitals – Information

Future NHS England Sustainable Improvement Team webinars: • 7th February 2017 (National) 13:00 – 14:00: The importance of clinical
leadership in establishing seven day services
• 27th February 2017 (South Region) 12:30 – 13:30: 7DS Practical examples of ensuring access to diagnostics and interventions Clinical Standards 5 & 6
• 7th March 2017 (National) 13:00 – 14:00: 7 Day Services: Top tips to engage your stakeholders
• 29th March 2017 (South Region) 12:30 – 13:30: 7DS Practical examples and models for achieving ongoing review-planning and processes to meet Clinical Standard 8
Connect Share Learn
7 Day Hospitals – Future webinars