60:1160-1169,2002 heat generation during implant drilling ... · heat generation during implant...
TRANSCRIPT

J Oral Maxillofac Surg60:1160-1169, 2002
Heat Generation During Implant Drilling:The Significance of Motor Speed
Mohamed Sharawy, BDS, PhD,* Carl E. Misch, DDS, MDS,†
Norman Weller, DMD, MS,‡ and Sherif Tehemar, BDS, PhD§
Purpose: The purpose of this study was to measure the heat generated from 3 drilling speeds (1,225,1,667, and 2,500 rpm) using the armamentarium of 4 implant systems.
Materials and Methods: The mean rise in temperature, the time of drilling, and the time needed forpig jaw bone to return to the baseline temperature were monitored using 4 thermocouple technology.
Results: The mean rise in temperature, the time of drilling, and the time needed for the specimens toreturn to the baseline temperature were lower at 2,500 rpm than at 1,667 or 1,225 rpm (P � .05),regardless of the system used. The rpm also directly correlated to the amount of time the bone remainedat an elevated temperature.
Conclusion: From a heat generation standpoint, we conclude that preparing an implant site at 2500rpm could decrease the risk of osseous damage, which may affect the initial healing of dental implants.This may decrease the devital zone adjacent to an implant after surgery and be most advantageous inimmediate load application to dental implants.© 2002 American Association of Oral and Maxillofacial SurgeonsJ Oral Maxillofac Surg 60:1160-1169, 2002
Dental implants have become an accepted treatmentmodality. According to recent studies, there are morethan 24 implant systems in international dental mar-kets, and more than 400,000 dental implants areplaced annually in the United States.1,2 Previously,healing of the implant was considered “successful”when it became encapsulated with fibrous tissue, ie,fibro-osseous integration.3 However, the presence ofthis pseudoperiodontium was associated with micro-
bial and mechanical problems leading to implant fail-ure.4 The extensive studies conducted in Sweden(University of Goteborg) and Switzerland (Universityof Bern) in the 1970s introduced the concept ofosseointegration, in which bone has a direct contactwith the surface of the implant with no interveningfibrous tissue.5,6 At the present, there is general agree-ment that osseointegration is the more stable situationand results in a high success rate for up to 15 years.7
There are many parameters that must be consid-ered during implant placement for osseous integra-tion to occur. It has been postulated that a cascade ofinteractions follows the manipulation of the osseoustissue during implant bed preparation that determinesthe progress of bone healing. The term “atraumatic”surgical preparation is considered essential, whichincludes several conditions, including avoidance ofexcess heat generation during the preparation of theosteotomy. The amount of bone contact to the implantafter surgical placement and initial healing is variableand dependent on several factors, including the thermalinjury to bone during implant osteotomy.8,9
Heat is always generated during implant drilling.Past implant studies to evaluate this event have beenconducted in vivo and in vitro. The in vivo studieshave shown the harmful role of heat production insubsequent bone healing and identified the criticaltemperature that bone can withstand without necro-sis.8-10 In vitro studies have found that the overallconcept of heat generation is considered multifacto-
*Professor and Director, Oral Biology/Anatomy, and Professor of
Oral and Maxillofacial Surgery, School of Dentistry, Professor of
Anatomy, School of Medicine, Medical College of Georgia, Augusta,
GA.
†Associate Professor, Department of Periodontics, University of
Michigan, School of Dentistry, Ann Arbor, MI
‡Professor and Chairman, Department of Endodontics, Medical
College of Georgia, Augusta, GA.
§Lecturer, Department of Oral and Maxillofacial Surgery, Faculty
of Dental Medicine, Alexandria University, Alexandria, Egypt.
The study was funded in part by the Misch Implant Institute,
Birmingham, MI.
Dr Misch is a consultant for and stockholder of BioHorizons
Implant Company.
Address correspondence and reprint request to Dr Sharawy:
School of Dentistry, Room 1411, Medical College of Georgia, 1120
15th St, Augusta, GA 30912-1122; e-mail: [email protected]
© 2002 American Association of Oral and Maxillofacial Surgeons
0278-2391/02/6010-0011$35.00/0
doi:10.1053/joms.2002.34992
1160

rial in nature,11 and most reports restrict their inves-tigation to 1 or 2 factors.12-16
Previous reports have implied that slow-speed dril-ling during the implant site preparation will reduceheat generation because the frictional heat was as-sumed to be less compared with high-speed motors.For example, the study of Reingewirtz et al17 ob-served that 600 rpm reduced the heat productionduring bone cutting, and the author recommendedreduced drill speeds in dense bone, to reduce heatgeneration. Almost all of the implant systems in theUnited States dental market recommend using a drillspeed between 1,500 and 2,000 rpm, and many com-mercial motors do not rotate more than 1,650 rpm.The purpose of this study was to compare the heatgenerated with different drill speeds during implantsite preparation, using 4 of the most commonly usedimplant systems.
Materials and Methods
The present study was conducted on porcine jawbone following the clinical procedures commonlyused in implant dentistry.7,18 The rationale for choos-ing pig jaws was the histologic and chemical similarityof pig bone with human bones.19
Nine fresh pig heads were obtained and preparedin a manner to separate the maxillae from the mandi-bles. The edentulous region between the canine andthe first premolar was selected for drilling and wasradiographed to observe the limiting structures anddetermine the osteotomy depths in the maxillary(Mx) and mandibular (Md) specimens. Then the spec-imens were kept frozen until used. Two hours beforeeach study, the specimens were thawed in a thermo-stat-controlled bath filled with isotonic saline (0.9% ofNaCl) adjusted at 37°C. Mucoperiosteal flap surgerywas then performed to expose the bone in the regionof interest, in a routine similar to that used for implantsurgery. Temperature measurements were made dur-ing each site preparation with 4 type K Chromel-Alumel thermocouples (Omega Engineering, Stam-ford, CT). Each thermocouple was placed at 1 mmfrom the anticipated periphery of the hole, corre-sponding to each drill, at the buccal, mesial, distal,and lingual sites, respectively. The thermocoupleswere inserted into 0.15-mm-diameter holes preparedby a twist drill and an endodontic file No. 15. Thesethermocouples were inserted 8 mm below the sur-face and parallel to the prepared sites. Once thethermocouples were placed, the specimens were re-immersed in the warm saline bath for 10 minutes tore-establish the baseline temperature. Care was takenduring the study to ensure each of the initial speci-mens was at 37°C before drilling. If the temperature
dropped under 37°C, the specimen was reimmersedin the warm saline bath.
The surgical sites were prepared to a constant8-mm depth to avoid the mandibular canal, maxillarysinus, or opposing cortical plate and to eliminate thevariable of drilling depth. Two contra-angled hand-pieces were used with different gear ratios mountedto a surgical motor (Steri-Oss surgical console; NobelBioCare, Yorba Linda, CA) to control the differentrpm values of the study. The surgical motor providesthe operator with a specific combination of the gearratio and the reduction percentage of the motor toobtain the 3 different speeds (�) that were studied(�1 � 1,225 rpm, �2 � 1,667 rpm, and �3 � 2,500rpm).
The 2 wire leads of each thermocouple were con-nected to the appropriate channel of a thermocoupleinput nodule (Keithley Data Acquisition and DataControl, Cleveland, OH). This model system was in-terfaced to a personal computer (Multitech 900; Mul-titech Industrial Corp, Taiwan, Republic of China)using an Easyest LX data acquisition software program(Keithley Asyst Data Acquisition, Taunton, MA). Theprogram was configured to simultaneously record in-put from all 4 thermocouples. The sampling rate wasset at 1 measurement per second for each thermocou-ple, with a reported accuracy of 0.01°C. The softwareallowed plotting the time and the change in temper-ature (�T) in the x-y axes.
To ensure a constant clinical distance (1 mm) be-tween the edge of the hole and the thermocouple foreach osteotomy, the drill was first placed onto thebone to measure its diameter. Then the 4 holes werecreated 1 mm beyond the edge of the predicted sur-gically produced hole for the thermocouples to adepth of 8 mm. The thermocouples were then in-serted before the drilling. The orifice of each thermo-couple-containing hole was isolated by pink wax toprevent irrigation fluid from entering and reducingthe bone temperature. These preoperative proce-dures were repeated for each consecutive drill evalu-ated, to allow recording of the intrabone temperaturethrough a constant amount of intervening bone (1mm3). That is, using the smallest-diameter drill, tem-perature measurements were made 1 mm from thedrilling site at a depth of 8 mm from the surface (ie, atthe extreme depth of the hole). Then the thermocou-ples were removed, the diameter of the next largerdrill was measured on the bone, and new thermocou-ple channels were drilled 1 mm beyond the boundaryof the new hole. This was repeated until the largest-diameter drill had been used.
Four implant drilling systems were evaluated in thisstudy: Two internally irrigated systems (Steri-Oss [No-bel BioCare] and Paragon [Sulzberg, Germany]) and 2externally irrigated systems (Branemark [Nobel Bio-
SHARAWY ET AL 1161

Care] and the first generation of the Maestro system[BioHorizons, Birmingham, AL]). Between 3 and 6different diameter drills were compared (Table 1).
All osteotomies were performed by the same oper-ator (S.T.) following the manufacturer’s operatingmanual and using room-temperature normal saline ascoolant. The bone density was D2 in the mandible(Md) and D3 in the maxilla (Mx), using the tactilemethods described by Misch.20 The number of sitesperformed and the groups studied are illustrated inTable 2.
The mean rise in temperature (�T) was recordedfor each drill in each system, at each site (Md or Mx),relative to the baseline temperature and the rotationalspeed used. This was accomplished by recording thebaseline temperature (°C) and the peak temperature(°C) displayed for each of the 4 thermocouples. Themean and the standard deviation of these 4 valueswere calculated for each group. Data were stored in apersonal computer and then statistically analyzed us-ing the statistic software package SAS (SAS Institute,Cary, NC) for personal computers. Data were sub-jected to a 3-way analysis of variance (ANOVA) andthe 2-paired Student Newman-Keuls tests. The � levelwas set a priori at .05.
Results
TEMPERATURE RISE (�T)
Internal Irrigated SystemsIn the Steri-Oss system, the mean rise in tempera-
ture (�T) in Md and Mx specimens with differentspeeds is presented in Figure 1. The mean tempera-ture rise at Md sites (Fig 1A) was significantly lowerfor �3 (2,500 rpm) with drill diameters of 2 and 3.8mm and was similar at all speeds for the 3.25-mm-diameter drill and slightly higher for the 2.7-mm-di-ameter drill at 2,500 rpm versus 1,667 rpm but similarto 1,225 rpm. The slowest rpm (1,225) produced thehighest temperature in the first and last drill in thesequence and similar to the fastest rpm for the inter-mediate drills.
For Mx specimens (Fig 1B), the 2,500 rpm speed(�3) caused slightly less rise in temperature at all drilldiameters, except for the 2.7-mm drill. However, nosignificant statistical difference could be noted amongthe 3 speeds, except for the 3.8-mm drill. The inter-mediate speed (1,667 rpm) produced the highest tem-perature for all diameter drills.
FIGURE 1. Graph representing the mean rise in bone temperature(�T) recorded using the Steri-Oss system in mandibular (A) and maxil-lary (B) specimens with different motor speed. Values are means, andbars represent SD. Values with different symbols (eg, ‡‡ vs †) aresignificantly different (P � .05), and difference applies to only thesame drill diameter. No statistical comparison was performed be-tween mandibular and maxillary.
Table 1. SYSTEM EVALUATED, NUMBERS, ANDDIAMETER OF DRILLS EXAMINED
SystemNo. ofDrills Drill Diameter (mm)
BioHorizons 6 1.5 2 2.5 3 3.4 4Branemark 4 2 3 3.85 4.3 NA NASteri-Oss 4 2 2.7 3.35 3.8 NA NAParagon 3 2.3 3.2 4.2 NA NA NA
NOTE. BioHorizons and Branemark are external irrigated systems;Steri-Oss and Paragon are internal irrigated systems.
Abbreviation: NA, not applicable.
Table 2. EXPERIMENTAL SITES, SPEEDS, ANDSPECIMEN NUMBERS
Steri-Oss(Internal
Irrigation)Branemark
(External Irrigation)
Maxillae1,225 rpm, n � 6 1,225 rpm, n � 61,667 rpm, n � 6 1,667 rpm, n � 62,500 rpm, n � 6 2,500 rpm, n � 6
Mandible1,225 rpm, n � 6 1,225 rpm, n � 61,667 rpm, n � 6 1,667 rpm, n � 62,500 rpm, n � 6 2,500 rpm, n � 6
NOTE. This design was repeated for the Paragon (internal irriga-tion) and BioHorizons (external irrigation). Four implant systemswere evaluated at 6 sites for each of 3 speeds, for a total of 72 sites/mandibles and 72 sites/maxillae (144 drilled sites in 9 heads).
1162 HEAT GENERATION DURING IMPLANT DRILLING
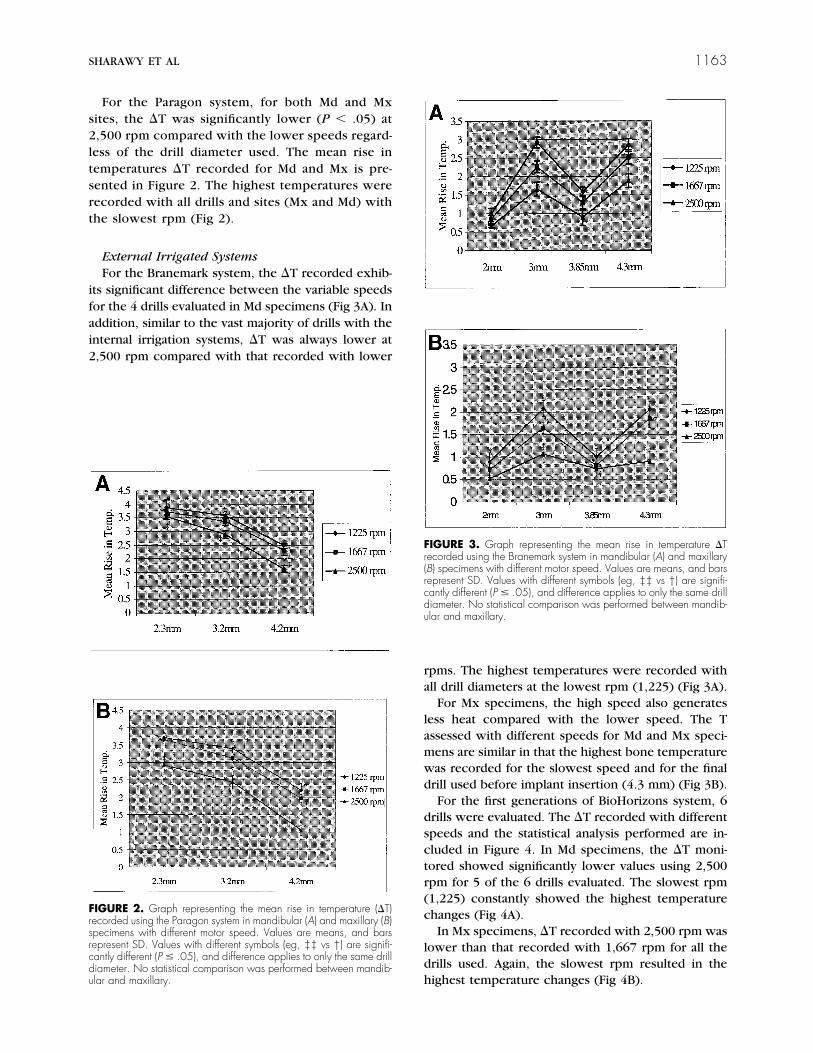
For the Paragon system, for both Md and Mxsites, the �T was significantly lower (P � .05) at2,500 rpm compared with the lower speeds regard-less of the drill diameter used. The mean rise intemperatures �T recorded for Md and Mx is pre-sented in Figure 2. The highest temperatures wererecorded with all drills and sites (Mx and Md) withthe slowest rpm (Fig 2).
External Irrigated SystemsFor the Branemark system, the �T recorded exhib-
its significant difference between the variable speedsfor the 4 drills evaluated in Md specimens (Fig 3A). Inaddition, similar to the vast majority of drills with theinternal irrigation systems, �T was always lower at2,500 rpm compared with that recorded with lower
rpms. The highest temperatures were recorded withall drill diameters at the lowest rpm (1,225) (Fig 3A).
For Mx specimens, the high speed also generatesless heat compared with the lower speed. The Tassessed with different speeds for Md and Mx speci-mens are similar in that the highest bone temperaturewas recorded for the slowest speed and for the finaldrill used before implant insertion (4.3 mm) (Fig 3B).
For the first generations of BioHorizons system, 6drills were evaluated. The �T recorded with differentspeeds and the statistical analysis performed are in-cluded in Figure 4. In Md specimens, the �T moni-tored showed significantly lower values using 2,500rpm for 5 of the 6 drills evaluated. The slowest rpm(1,225) constantly showed the highest temperaturechanges (Fig 4A).
In Mx specimens, �T recorded with 2,500 rpm waslower than that recorded with 1,667 rpm for all thedrills used. Again, the slowest rpm resulted in thehighest temperature changes (Fig 4B).
FIGURE 2. Graph representing the mean rise in temperature (�T)recorded using the Paragon system in mandibular (A) and maxillary (B)specimens with different motor speed. Values are means, and barsrepresent SD. Values with different symbols (eg, ‡‡ vs †) are signifi-cantly different (P � .05), and difference applies to only the same drilldiameter. No statistical comparison was performed between mandib-ular and maxillary.
FIGURE 3. Graph representing the mean rise in temperature �Trecorded using the Branemark system in mandibular (A) and maxillary(B) specimens with different motor speed. Values are means, and barsrepresent SD. Values with different symbols (eg, ‡‡ vs †) are signifi-cantly different (P � .05), and difference applies to only the same drilldiameter. No statistical comparison was performed between mandib-ular and maxillary.
SHARAWY ET AL 1163

DRILLING TIME VERSUS THE TIME IT TAKES FORBONE TO RETURN TO THE BASELINE TEMPERATURE
Internal Irrigation SystemsThe results of the drilling time (t) and time required
for the specimens to return to baseline temperature(TB) using the Steri-Oss system are presented in Fig-ure 5, for Md and Mx specimens, respectively. Therewas positive correlation between t and TB in all theparameters studied; that is, the longer it takes to drill,the longer it takes for the temperature to return to TB.In addition, the ANOVA showed a significant differ-ence between t with different � values; that is, thehigher speed, the shorter was the drill time. It is ofnote that TB varied with the speed �, and this obser-vation was true for all of the drills used, regardless ofthe drilling site, whether it was Md or Mx, (P� .001).
The graphs illustrating the t and TB for each drillsequence in the system (2, 2.7, 3.25, and 3.8 mm)show negative correlation with the diameter (d) ofthe drill; that is, the largest drill diameter led to thelowest value of t and TB.
The Paragon system behaved similar to the Steri-Oss system (Fig 6A). The statistical analysis showedsignificant difference between t and TB at variablespeed (P � .001). The maxilla had less t and TBcompared with the mandible for each drill in thesequence for both of the internally cooled systemstested.
External Irrigation SystemsFor the Branemark system, positive correlation be-
tween t and TB was also observed (Fig 7). In addition,as in all systems tested, the higher the speed �, theshorter was the t (P � .001).
In contrast to the internal irrigation systems, nocorrelation could be found among the t, TB, and thatof d. The lowest values of t and TB were obtainedwith the first drill (2 mm), whereas the highest valueswere detected with the second drill (3 mm). The third(3.85 mm) and the fourth (4.3 mm) drills exhibitedlesser values than the second, but a higher value thanthe first. All values differ significantly from each other(P � .005).
For the BioHorizons system, the results of t and TBare illustrated in Figure 8. Positive correlation wasfound between t and TB with all of the drills used.Also, comparable results could be noticed between tand TB relative to the speed. The higher the speed,the lower were the t and TB.
Similar to the Branemark system, no correlationexisted among t, TB, and d, albeit a lesser value thanthat of Branemark system was observed. The lowestvalue of t/d and TB/d was assigned to the fifth drill(3.4 mm), while the highest recorded was that for thefirst drill (1.5 mm).
Discussion
Previous studies have shown that osteonecrosis af-ter bone drilling is a function of the rpm (degree andtime).8,9,17 In this study, 3 speeds were evaluated andthe time of drilling (t) or time required for the bone toreturn to baseline temperature (TB) was monitored.Results of this investigation clearly show that thehigher the speed, the less was the heat generated.These findings were true regardless of the site ofdrilling, whether Md or Mx, or the implant systemused. This is not to imply that rpm is the only factor.For example, the higher the rpm, the faster the drillreached the 8-mm depth of cutting. Thus, drillingtime (t) was inversely related to the rotational speedof the drill. Slower rotational speeds required moredrilling time, which produced more frictional heat.
No attempt was made during this study to assessthe pressure (load) applied on the drill. Past studiesindicate that varying amounts of pressure on the drillcan modify the temperatures and the length of time to
FIGURE 4. Graph representing the mean rise in temperature �Trecorded using the BioHorizons system in mandibular (A) and maxillary(B) specimens with different motor speed. Values are means, and barsrepresent SD. Values with different symbols (eg, ‡‡ vs †) are signifi-cantly different (P � .05), and difference applies to only the same drilldiameter. No statistical comparison was performed between mandib-ular and maxillary.
1164 HEAT GENERATION DURING IMPLANT DRILLING

FIGURE 5. Graphic presenta-tion of the data showing the influ-ence of the speed and both dril-ling time (t) and time to return tobaseline (TB) using Steri-Oss sys-tem in mandibular (A and B) andmaxillary (C and D) specimens.Values are means, and bars rep-resent SD.
FIGURE 6. Graphic presenta-tion of the data showing the influ-ence of the speed and both dril-ling time (t) and time to return tobaseline temperature (TB) usingParagon system in mandibular (Aand B) and maxillary (C and D)specimens. Values are means,and bars represent SD.
SHARAWY ET AL 1165

FIGURE 7. Graphic presenta-tion of the data showing the influ-ence of the speed and both dril-ling time (t) and time to return tobaseline temperature (TB) usingBranemark system in mandibular(A and B) and maxillary (C andD) specimens. Values are means,and bars represent SD.
FIGURE 8. Graphic presenta-tion of the data demonstrating theinfluence of the speed and bothdrilling time (t) and time to returnto baseline temperature (TB) us-ing BioHorizons system in man-dibular (A and B) and maxillary(C and D) specimens. Values aremeans, and bars represent SD.
1166 HEAT GENERATION DURING IMPLANT DRILLING

prepare the bone site. Brisman21 compared the dril-ling at 1,200 rpm and 2,400 rpm under loads of 1.2 kgand 2.4 kg in dry bovine femoral bone. Less heat wasgenerated with 2,400 rpm under 2.4 kg of force.Cordioli and Majzoub16 found that a drilling force of 2kg falls in the range of values used under clinicalcondition.
The first drill of the Branemark externally cooledsystem tested in our study generated less heat thanthe final drill, while the first drill of externally cooledBioHorizons drill generated more heat than the finaldrill. On the contrary, the internal cooled systems hadthe most heat generated from the first drill. However,the differences are less than 1.4°C elevation above thebody temperature. This report differs from that of,Lavelle and Wedgewood,12 which reported that inter-nal cooling prepares bone at a lower temperature. Itshould be emphasized that this report was not de-signed to evaluate internal versus external cooling. Toaccomplish this, the same design drill should be used.This study used differently designed drills manufac-tured by different companies. Hence, the lower tem-peratures for the 2 external cooled systems is inter-esting but, because the drill designs were all different,no comparison may be made between the generalconcepts of external versus internal cooling for a drillpreparation.
Earlier studies8-12 delineated the critical bone tem-perature beyond which bone necrosis may occur.However, the range of the safe drill speeds that aclinician could use was not clearly identified. All ofthe implant systems evaluated in this study providedan implant site, without exceeding the critical 4°Crise in bone temperature, and are acceptable forproper healing processes to proceed and create adirect bone-to-implant contact. However, there is ahigher implant failure rate in the most dense bonetypes.22 Therefore, in some clinical situations, subtledifferences in procedures such as the speed of drillingmay alter the expected outcome. In all of these sys-tems, the higher the rpm, the lower was the temper-ature rise. Thus, it is suggested that higher drill speedsbe considered in clinical use, especially in more densebone types.
Contrary to this report, Reingewirtz et al17 ob-served a positive correlation between the tempera-ture rise and the rotation speed in an internal cooledsystem with rotations ranging from 0 to 10,000 rpm.However, their findings were based on 1 thermocou-ple inserted in dry ox femoral bone, 0.8 mm from thedrilling site. The drilling was performed using a2.3-mm round steel bur. The studies of Eriksson etal23,24 were designed to monitor the effect of heat onbone, which was assessed histologically, microradio-graphically, and through vital observation, withoutregard to the drilling sequences. Their observations
were also based on 1 thermocouple, which may beinsufficient in monitoring the overall temperature riseof bone surrounding the implant site. In the presentinvestigation, 4 thermocouples were inserted 1 mmfrom the drilling site, and the mean of the 4 readingswas calculated for each drill. Thus, the overall thermalprofile could be detected from different regions sur-rounding the site of drilling.
A positive correlation could be found between dril-ling time (t) and the time required to return to the TB,regardless of the drilling site or the implant systemused. Thus, the more drilling time, the higher was thebone temperature and the more time was needed forthe specimens to return to TB. More time was alwaysneeded to prepare the bone site at a drilling speed of1,225 rpm than with either 1,667 or 2,500 rpm. TheANOVA always detected significant difference be-tween drilling time and speed of rotation. This obser-vation is in accordance with earlier reports. Reingewirtzet al17 also found that the temperature change was afunction of the time of drilling and the motor speedrather than the drilling time alone. In addition, theyobserved that with greater rpm, less time was re-quired to complete the drilling. For example, thedrilling time recorded at 1,600 rpm was 6.24 seconds,while it was 3.69 seconds at 3,200 rpm.17 In anotherexperiment, Brisman21 observed a reduction rangingfrom 30% to 40% in drilling time when drilling speedincreases from 1,800 rpm to 2,400 rpm at 2,400 g offorce. He also noticed that the drill geometry couldsignificantly influence the results. Those observationswere comparable to our results. For the Steri-Osssystem, doubling the rpm results in 30% reduction indrilling time t and a 25% reduction in the TB in Mdspecimens, while in Mx specimens, the same drilldiameter produced a 45% reduction in drilling timeand a 19% reduction in TB. Similar findings could beseen in all of the other systems.
Interesting, although a similar relationship existsbetween change in bone temperature (�T) and bothdrilling time (t) and TB, this was true only within eachsystem, rather than as an overall observation that canbe applied to all implant systems (Table 3).
From Table 3, we can conclude that to drill 8 mmin depth using the 2-mm-diameter drill of the Bio-
Table 3. EXAMPLES OF CORRELATION OF DRILLINGTIME (t) AND BASELINE TEMPERATURE (TB) RELATIVETO �T WITHIN THE SYSTEM AT 2 DRILL DIAMETERS
SystemDiameter
(mm) �T t TB
Biohorizons 2 0.9 (0.1) 6.98 (0.08) 34.4 (2.3)Branemark 2 0.97 (0.18) 5.6 (0.27) 45.8 (1.92)Biohorizons 3 1.11 (0.13) 6.46 (0.27) 47.2 (1.48)Branemark 3 2.92 (0.18) 7.44 (0.37) 50.2 (3.89)
SHARAWY ET AL 1167

Horizons system, the time required for drilling will be6.98 � 0.08 second and the rise in temperature was0.9 � 0.1°C, which needed 34.4 � 2.3 seconds toreturn back to the TB of 37°C. The 2-mm drill of theBranemark system, using the same motor speed, dis-played different values (both t and TB were statisti-cally significantly different, P � .05). Thus, it seemsthat the drill design is also an important factor thatinfluences both t and TB. As a result of these studies,the BioHorizons system has modified its drill designsto make them more efficient and able to prepare bonein less time. Further studies are in progress to reeval-uate these modified conditions. Both systems used thesame flow rate of external irrigation solution.
It is also significant to mention that, within the limitof this study, our results indicate that whether theirrigating saline was delivered internally or externally,the rise in temperature at any of the motor speedsused would not cause necrosis to the bone. Thegreatest temperature recorded was 41.5°C for lessthat 20 seconds in the D2 bone of the mandible. Inthe Eriksson and Adell24 study on rabbit bone, a tem-perature of 40°C held for 7 minutes or 47°C for 1minute was found to cause bone necrosis. However,in theory, if the clinician changes the drills and beginsdrilling in the osteotomy before allowing the temper-ature returning to baseline, the 40°C increases foreach drill may indeed gradually rise to a clinical con-cern. If approximately 30 to 60 seconds is required toreturn to the TB, beginning the next size drill in theosteotomy before allowing the bone to return to base-line return may eventually heat the bone more than10°C (47°C when baseline is body temperature).Hence, although independent drill performance mayonly increase bone temperatures 0.5° to 4°C, the useof 2 to 5 additional reentries into the osteotomy bythe sequential drilling may further elevate bone tem-peratures. In addition, it is suggested the cliniciansinterrupt the drilling procedure at least every 5 sec-onds for at least 10 seconds, while saline is applied tothe bone. The interruption will dramatically decreasethe time the bone temperature is elevated. This ismost important in the most dense bone types.
Clinically, a higher failure rate of dental implant inD1 bone has been reported and attributed to (amongother things) the heat generation resulting from thefriction of the drill with the dense cortical bone.21
However, in almost all of the long-term follow-upstudies, the rotation speed used falls within the rangeof 1,500 to 2,000 rpm. The results of the presentstudy using wet pig jaws suggest that it may be ad-vantageous to use higher speed (2,500 rpm) in densebone, because it will reduce the time of drilling and itwill generate less heat that will return back to normaltemperature in a shorter time. Further in vivo studiesare needed to support this conclusion.
Immediate loading of dental implants has been in-creasingly performed during the past 10 years. Intheory, a smaller devitalized zone next to an immedi-ate loaded implant would be beneficial. Because ele-vations in bone temperature above 41°C are able toincrease the devitalized zone after initial surgery, theconcepts presented here may have most benefit inimplants that are loaded before bone remodeling iscompleted. The amount of time to return to a TBsuggests a waiting period should exist between eachdrill sequence in an osteotomy.
Within the limits of the present study, we canconclude that the bone drilling at 2,500 rpm gener-ates less heat than at slower speeds. Published clinicaltrails by BioHorizons Dental Implants have used a drillspeed of 2,500 rpm during a 3-year period and havereported survival above 99% implant integration in allbone densities.25 Further investigation is needed toevaluate the performance of other dental implants inhumans using this drill speed.
The purpose of this in vitro study was to evaluatethe effect of drill speed on the temperature of adja-cent bone using 4 commercial implant drilling sys-tems. Two of these systems were externally irrigated,whereas the other 2 were internally irrigated duringthe drilling procedure. The increase in bone temper-ature, the time required to prepare an 8-mm osteot-omy, and the time required for the bone to return toa TB were measured. In all systems, a drill speed of2,500 rpm resulted in less heat, less time to preparethe osteotomy, and less time for the bone to return tothe original TB. The manufacturers of the systemsevaluated suggest drilling speeds between 1,650(Steri-Oss, Paragon) and 2000 (Branemark) rpm.These speeds have led to very high success rates ofosteointegration. However, in the most dense bonetypes, higher drill speeds may prove to be beneficialbecause of the reduced heat generation. Reducing theheat generated during implant insertion may indeeddecrease the devitalized zone next to an implant aftersurgical placement.
Acknowledgments
The authors would like to thank Dr Carl Russell, Medical Collegeof Georgia, for analyzing the data of this study.
References1. Watson MT: Implant dentistry: A 10 year retrospective report.
Dent Prod Rep December:26, 19962. Watson MT: Specialists’ role in implant dentistry rooted in
history: A survey of periodontist and maxillofacial surgeons.Dent Prod Rep January:14, 1997
3. Weiss CM: Tissue integration of dental endosseous implants:Description and comparative analysis of the fibro-osseous inte-gration and osseous integration systems. J Oral Implantol 12:169, 1986
1168 HEAT GENERATION DURING IMPLANT DRILLING

4. Alberktsson T, Sennerby L: Direct bone anchorage of oralimplants: Clinical and experimental considerations of the con-cept of osseointegration. Int J Prosthet 3:30, 1990
5. Branemark P-I: Osseointegration and its experimental back-ground. J Prosthet Dent 50:399, 1983
6. Schroeder A, Van Der Zypen E, Stich H, et al: The reaction ofbone, connective tissue and epithelium to endosteal im-plants with sprayed titanium surfaces. J Maxillofac Surg 9:15,1981
7. Adell R, Lekholm U, Rockler R, et al: A 15 year old study ofosseointegrated implant in the treatment of the edentulousjaw. Int J Oral Surg 10:387, 1981
8. Eriksson A, Alberktsson T, Grane B, et al: Thermal injury tobone: A vital microscopic description of heat effects. Int J OralSurg 1:115, 1982
9. Eriksson RA, Alberktsson T: Temperature threshold levels forheat-induced bone tissue injury: A vital microscopic study inrabbit. J Prosthet Dent 50:101, 1983
10. Eriksson RA, Alberktsson T: The effect of heat on bone regen-eration: An experimental study in rabbit using the bone growthchamber. J Oral Maxillofac Surg 42:705, 1984
11. Tehemar SH: Factors affecting heat generation during implantdrilling: A review of biological observations and future consid-erations. Int J Oral Maxillofac Implantol (in press)
12. Lavelle C, Wedgewood D: Effect of internal irrigation on fric-tional heat generated from bone drilling. J Oral Surg 38:499,1980
13. Matthews LS, Hirsch C: Temperatures measured in humancortical bone when drilling. J Bone Joint Surg Am 54:297, 1972
14. Rafel SS: Temperature changes during high-speed drilling onbone. J Oral Surg Anesth Hosp Dent Serv 20:475, 1962
15. Yacker M, Klein M: The effect of irrigation on osteotomy:depth and bur diameter. Int J Oral Maxillofac Implantol 11:634,1996
16. Cordioli G, Majzoub Z: Heat generation during implant sitepreparation: An in vitro study. Int J Oral Maxillofac Implantol12:186, 1997
17. Reingewirtz Y, Szmukler-Moncler S, Senger B: Influence ofdifferent parameters on bone heating and drilling in implantol-ogy. Clin Oral Implant Res 8:189, 1997
18. Misch CE: Root form surgery in edentulous mandible: Stage Iimplant insertion, in Misch CE (ed): Contemporary ImplantDentistry. St Louis, MO, Mosby, 1999, pp 347-371
19. Buser D, Nydegger T, Hirt HP, et al: Removal torque values oftitanium implants in the maxilla of miniature pigs. Int J OralMaxillofac Implant 13:611, 1998
20. Misch CE: Density of bone: Effect on treatment plans, surgicalapproach, healing and progressive bone loading. Int J OralImplant 6:23, 1990
21. Brisman DL: The effect of speed, pressure and time on bonetemperature during drilling of implant sites. Int J Oral Maxillo-fac Implantol 11:35, 1996
22. Truhlar RS, Morris HF, Ochi S, et al: Second stage failuresrelated to bone quality inpatients receiving endosseous den-tal implants: DICRG Interim report #7. Implant Dent 3:252,1994
23. Eriksson RA, Alberktsson T, Magnusson B: Assessment of boneviability after heat trauma: A histological, histochemical andvital microscopic study in the rabbit. Scand J Plast ReconstrSurg 18:261, 1984
24. Eriksson RA, Adell R: Temperatures during drilling for theplacement of implants using the osseointegration technique.J Oral Maxillofac Surg 44:4, 1986
25. Misch CE, Hoar J, Hazen R, et al: Bone quality based implantsystem (BioHorizons® Maestro™ Dental Implants): A prospec-tive study of the first two years of prosthetic loading. OralImplantd 1999
SHARAWY ET AL 1169