6 multiple sclerosis nero medicine
TRANSCRIPT

MULTIPLE SCLEROSIS
Dr.Raed Ahmed MBChB , FIBMSNeurologist
Lec. 810.00 AMMarch /15 / 2015
1

WHAT IS MULTIPLE SCLEROSIS ?
2

Multiple Sclerosis (MS)
A chronic neurological disorder that affects the central nervous system,
in which myelin is destroyed in the brain and
spinal cord and
causes scarring at multiple sites in the CNS.
3

MULTIPLE SCLEROSIS
Most common disabling condition in young adultsMost common demyelinating disorderProgresses to disability in majority of casesUnpredictable course / variety of signs and symptoms; sometimes mistaken for psych dxCurrent theory favors immunologic pathogenesis
4

J.M CharcotThis Disease (MS) without his name is meaningless!first who described MS in 1868.
Yet, after more than 140 years of research , much remains a mystery.
5

MULTIPLE SCLEROSIS
Leading cause of neurologic disability in young adult.
Over 1 million individual worldwideFocal demylination is patholgic
hallmarkPlaque,discreate area of damage
myelinNo known cause, and as yet,No cure
6

“saltatory conduction”
7

Abnormal Conduction
8

WHO GETS THE DISEASE ?
9

>Predominant age: 20-40
MULTIPLE SCLEROSIS AFFECT:0.1%Worldwide incidence
MS is more common in temperate regions, such as northern Europe and North America, but much rarer in the tropics.
The ratio is increasing
now
people in US have MS
400, 000 onset before puberty or after the age of 60 years is rare.
worse prognosis
Highly variable and unpredictable
10

WHAT CAUSES MULTIPLE SCLEROSIS?
11

Genetic susceptibility
•15% to 20% of patients have history of familial MS.
•Twin studies : monozygotic twins (30%) than dizygotic twins (5%).
•3–5% in first degree relatives
The exact cause remains unknown, but
12

• HLA class II region, particularly (HLADRB1*15 and HLA-DQB1*06 —chromosome 6p21 )associated with 3X to 4x fold increased risk of MS.
Environmental factors• Geographic variation in prevalence• Epstein-Barr virus, insufficient vitamin D
intaked and smoking.
13

WHAT IS PATHOPHYSIOLOGY ?
14

When brain is inflammed –lymphocytes cross BBB
Activated T lymphocytes recognise myelin-derived antigens & secrete cytokines
initiates destruction of the oligo -dendrocyte–myelin unit by macrophages.
15

HOW TO CLASSIFY MS?
16

17

Clinically isolated syndromes(CIS)First acute episode suggestive of CNS demyelination,
and it may be the first presentation of MS.
The average risk of developing MS ( 30%-70%)
unilateral ON have a lower risk of converting to multiple sclerosis.
Abnormal MRI at first presentation shown to confer a higher risk of conversion to MS than if MRI is normal.
18

WHAT ARE THE CLINICAL FEATURES?
19

INITIAL SYMPTOMS
Double vision / blurred visionNumbness/weakness in extremitiesInstability while walkingProblems with bladder controlHeat intoleranceMotor weakness
“All symptoms can be precipitated by heat”
20

SENSORY DISTURBANCES
Ascending numbness starting in feetBilateral hand numbnessHemiparesthesia/dysesthesiaGeneralized heat intoleranceDorsal column signs Loss of vibration/proprioception Lhermitte’s sign
21

VISUAL DISTURBANCES
Unilateral or bilateral partial/complete intranuclear ophthalmoplegiaCN VI paresisOptic neuritis Central scotoma, headache, change
in color perception, retroorbital pain with eye movement)
22

MOTOR DISTURBANCES
Weakness (mono-, para-, hemi- or quadriparesis)Increased spasticityPathologic signs (Babinski, Chaddock, Hoffman)Dysarthria
23

Crebellar signs
NystagmusDysarthriaTremorDysmetriaTitubationStance and gait
24

OTHER CLINICAL SIGNS
Urinary incontinence, incomplete emptying Set up for UTI’s
Cognitive and emotional abnormalities (depression, anxiety, emotional lability)FatigueSexual dysfunction
25

MCDONALD DIAGNOSTIC CRITERIA FOR MS
2 or more relapses, objective clinical evidence of 2 or more lesions.2 or more relapses,objective clinical evidence of 1 lesion (Need dissemination in space)1 relapse,objective clinical evidence of 2 or more lesions (dissemination in time).CIS
26

DIAGNOSTIC TESTS DIAGNOSTIC TESTS
MRI Evoked potentials CSF
Blood and urine
27

28
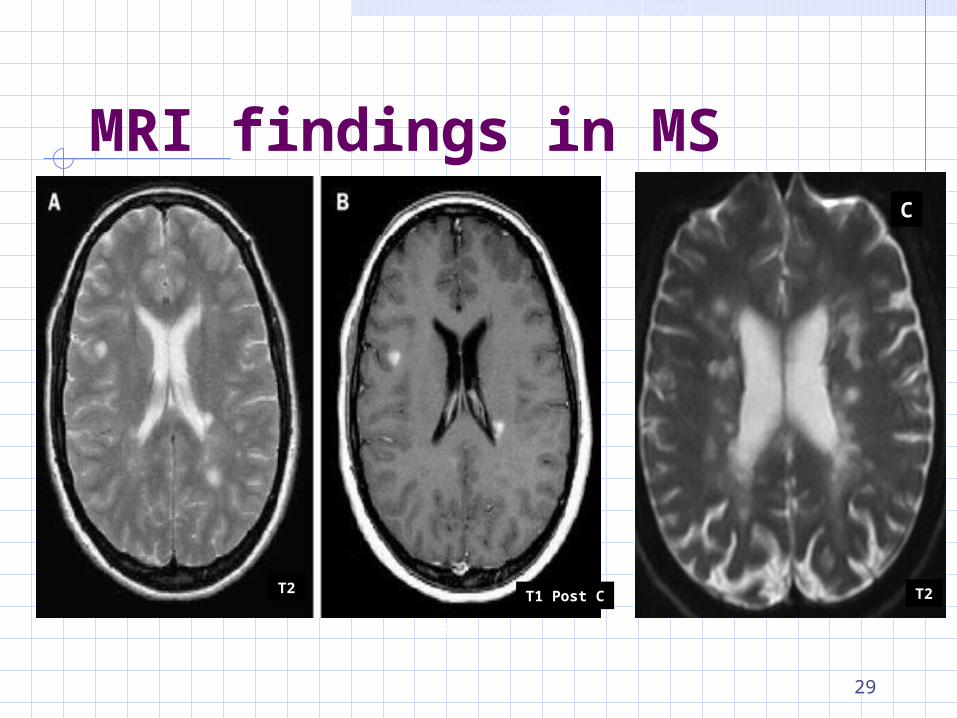
MRI findings in MS
T2
T2 T2T1 Post CT2 T2
C
29

T1 Post C
30

EVIDENCE FOR DIS1 or more T2 lesion in at least 2 out of 4
areas of CNS : periventricular, juxtacortical , infratentorial, or spinal cord
EVIDENCE FOR DITSimultaneous presence of asymptomatic Gd-enhancing and non enhancing lesion at any time ORA new T2 and/or Gd-enhancing lesion(s) on follow-up MRI irrespective of the timing of baseline MRI scan
31

RED FLAGS FOR OTHER DIAGNOSES
Onset before age 10 or after age 50Absence of sensory or genitourinary symptomsDeficit developing within minutesSeizuresRigidity Cortical deficits
(aphasia, apraxia, alexia, neglect)
32

DISORDERS THAT CAN MIMIC MS (DDx) =
VITAMINS
Auto-immune
Traumati
c
Psychiatri
c
Neoplastic
Idiopathi
c Metaboli
c
Vascular
Infectious
33

Natural History Of MS
34

Management A.Treatment of acute attacks
Relapse should be differentiated from a pseudoexacerbation
Glucocorticoid treatment is usually administered as i.v. methylprednisolone
Monitering side effects ST need Plasma exchange
TREATMENTACUT ATTACK
TREATMENTACUT ATTACK
35

B.Treatment with disease-modifying agents
For relapsing form of MS (RRMS, SPMS with exacerbations.
Seven such agents are approved by the U.S. FDA:
(1) IFN-β-1a (Avonex ), (2) IFN-β-1a (Rebif ), (3) IFN-β-1b (Betaseron), (4) Glatiramer acetate (Copaxone), (5) Natalizumab (Tysabri), (6) Fingolimod (Gilenya), and (7) Mitoxantrone - (cytotoxic) (Novantrone).
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
36

The first six agents were approved for RRMS, and mitoxantrone is indicated for worsening forms of MS and for SPMS.
For PPMS : No therapies but symptomatic measures.
The three IFN-β drugs and Glatiramer reduce the relapse rate by approximately one third.
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
37

Interferon- β
(1) Downregulating expression of MHC molecules on antigen-presenting cells, (2) Inhibiting proinflammatory and increasing regulatory cytokine levels, (3) Inhibition of T cell proliferation, and (4) limiting the trafficking of inflammatory cells in the CNS.
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
38

Interferon- β : SE sInflammation at site of injection.Flu-like symptoms(myalgia,fever, rigor, rhinitis and fatigue).Rare side effects
Depression, suicide, epileptic events Thyroid abnormalities , lymphopenia,
thrombocytopenia, asymptomatic elevated liver transaminase levels and rarely symptomatic hepatitis
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
39
Glatiramer acetate A synthetic, random polypeptide designed to mimic myelin basic proteinReduces the attack rate in RRMS. (Similar efficacy to interferon-beta)Erythema, pain, mild swelling.Chest tightness, dyspnea, tachycardia, palpitation occur seconds to minutes of injection
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
40

Fingolimod A sphingosine-1-phosphate (S1P) inhibitor.Trapping of lymphocytes in the periphery, preventing them reaching the brain. Reduces the attack rate (superior efficacy to interferon-beta)Administered orally each daySE : Mildly elevated liver function tests or lymphopenia , first-dose bradycardia, macular edema, and respiratory infections.
DISEASE MODIFYING TREATMENT
DISEASE MODIFYING TREATMENT
41

C.Treatment of Specific Symptoms
healthy lifestyleSpasticity :physical therapy, baclofen, Local (IM) injection of botulinum toxin
For severe spasticity, a baclofen pumpAtaxia often intractable. Clonazepam,ST IsoniazidWeakness potassium channel blockers such as dalfampridine
MANAGE MS SYMPTOMS
MANAGE MS SYMPTOMS
42

Bladder dysfunction Urodynamic testings oxybutynin, tamsulosin, Bethanechol for an atonic bladder, but intermittent catheterization is often required.
UTIs should be treated promptlyPsychosocial
prompt Dx and Rx of Depression, Fatique Sexual Dysfunction
MANAGE MS SYMPTOMS
MANAGE MS SYMPTOMS
43

FAVORABLE PROGNOSTIC FACTORS
Female gender Onset before age 40Visual or somatosensory, rather than pyramidal or cerebellar dysfunction.Low rate of relapses per yearComplete recovery from early attacksLong interval between 1st and 2nd attackMinimal impairment after 5 years of disease onset
44

Acute Disseminated EncephaloMyelitis (ADEM): An acute monophasic demyelinating condition
Widely disseminated throughout the brain and spinal cord.
Spontaneously but often occurs a week or so after a viral infection,or following vaccination,
Immunologically mediated response to MBP (Molecular mimicry)
45
Clinical features ADEM is more common in children
Mean age of onset 5–8 years. it is more common in males
History of recent vaccination or viral illness.
Headache, vomiting, pyrexia, confusion and meningism may be presenting features . Seizures or coma may occur.
ADEM evolves rapidly over hours to days.
ADEMADEM
46

InvestigationsMRI shows multiple high-signal areas in a
pattern similar to that of MSCSF may be normal or show an increase in
protein and lymphocytes
ManagementICU, with adequate hydration ,pyrexia,
seizures High-dose i.v methylprednisolone, If unresponsive to steroids, plasmapheresis
or IVIG may be considered.
ADEMADEM
47

Neuromyelitis optica (also known as Devic’s disease)
an inflammatory demyelinating disease of the CNS distinct from multiple sclerosisyoung adults (mean age 40), Predominantly female (4 : 1). Commonly in Asian and African.Antibody to a neuronal membrane channel, aquaporin 4. (autoantibody, NMO-IgG)
48

Clinical features
Severe episodes of transverse myelitis and optic neuritis without clinical involvement of other parts of the CNS. Contiguous spinal cord MRI lesion extending over ≥3 vertebral segments. Brain MRI not meeting diagnostic criteria for multiple sclerosis. NMO-IgG seropositive status.
NMONMO
49

Management
Acute attacks of high dose i.v gluco- corticoids for 5–10 days followed by a prednisone taper.Unresponsive to high-dose steroids, the next line is plasma exchange.In relapsing NMO long-term immunosuppression is indicated.
NMONMO
50

THANK YOU
51