58633929
TRANSCRIPT
8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 1/9
SPECIAL FEATURES: METHODS
Predictive Factors of theNursing Diagnosis Sedentary Lifestyle
in People with High Blood Pressure NirlaGomes Guedes, MarcosVen| ¤ cios de Oliveira Lopes,Thelma Leite de Araujo, Rafaella Pessoa Moreira, and Larissa Castelo Guedes Martins
ABSTRACT Objectives: To verify the reproducibility of defining the characteristics and related factorsin order to identify a sedentary lifestyle in patients with high blood pressure. Design and Sample: A cross-sectional study. 310 patients diagnosed with high blood pressure. Measures: Socio-demographics and variables related to defining the characteristics and related factors of a sedentary lifestyle. The coefficient Kappa was utilized to analyze the reproducibility. The sensitivity, specificity, and predictive value of thedefining characteristics were also analyzed. Logistic regression was applied in the analysis of possible
predictors. Results: The defining characteristic with the greatest sensitivity was demonstrates physical deconditioning (98.92%). The characteristics chooses a daily routine lacking physical exercise and verbalizes
preference for activities low in physical activity presented higher values of specificity (99.21% and 95.97%,respectively). Conclusions: The following indicators were identified as powerful predictors (85.2%) for theidentification of a sedentary lifestyle: demonstrates physical deconditioning, verbalizes preference for activitieslow in physical activity, and lack of training for accomplishment of physical exercise.
Key words: blood pressure, cardiovascular diseases, lifestyle, measurement, statistics.
The term ‘‘clinical indicator’’ has been used as a
synonym of defining characteristics, clinical evidence,and signs and symptoms (Chang et al., 1998). Identi-
fying clinical indicators with a good predictive value
for a specific nursing diagnosis can contribute to
increasing diagnostic accuracy and to improving th
reliability of the diagnostic inference process (Parke& Lunney, 1998).
Defining characteristics are understood as a group
of signs and symptoms that indicate the presence of a
particular diagnosis. They constitute clinical evidenc
that needs to be studied with regard to their represen
tation in practice. This also includes related factors tha
can predict a diagnosis, such as etiological agent
(NANDA International [NANDA-I], 2009).
Accurate diagnostic inferences increase the effec
tiveness of care by permitting nurses to choose specifi
actions oriented toward the resolution and control o
identified problems. Conversely, interpretations of low
accuracy can lead to neglect of real or potential prob
lems and cause damage to the patient (Lunney, 2001).
Backgr ound The validation of diagnostic categories in population
and diverse clinical situations is important. Mos
likely, there will be language problems because thes
Nirla Gomes Guedes, R.N., M.S.N., is Doctoral Student, Nursing Professor, Catholic Faculty Rainha do Serta ì o,QuixadaŁ /CearaŁ , Brazil. Marcos Ven| ¤ cios de Oliveira Lopes, Ph.D., is Nursing Professor, Federal University of CearaŁ , Fortaleza/CearaŁ , Brazil. Thelma Leite de Araujo, Ph.D., is Nursing Professor, Federal University of CearaŁ ,
Fortaleza/CearaŁ , Brazil. Rafaella Pessoa Moreira, R.N., M.S.N., is Doctoral Student, Nursing Professor, Catholic Faculty Rainha do Serta ì o, QuixadaŁ /CearaŁ , Brazil. Larissa Castelo Guedes Martins, R.N., is Assistant Nurse, AlbertSabinHospital, Fortaleza/CearaŁ , Brazil.Correspondence to: Marcos Ven| ¤ cios de Oliveira Lopes, 1055, Esperanto St,Vila Unia ì o. Fortaleza -- CE/Brazil 60410-620. E-mail: [email protected]
193
Public Health Nursing Vol. 28 No. 2, pp. 193–200
0737-1209/r 2010 Wiley Periodicals, Inc.doi: 10.1111/j.1525-1446.2010.00902.x

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 2/9
categories have been developed in other cultures;
consequently, there is a need to reconstruct these
categories to include a cross-cultural approach. The
sensitivity, specificity, and predictive value of clinical
indicators are factors that can contribute to the vali-
dation of this process.
Concerned with growing global sedentarism,NANDA-I realized the need for adding a diagnosis
that could better represent insufficient physical activity.
Existing diagnostic categories, such as ‘‘intolerance of
activity,’’ ‘‘fatigue,’’ ‘‘impaired physical mobility,’’
and ‘‘self-care deficit,’’ were all based on individuals
with various levels of physical injury (Damewood
& Carlson-Catalano, 2000). Some researchers have
proposed ‘‘deficit of physical activity’’ as a diagnostic
category related to a sedentary lifestyle, with its own
defining characteristics and related factors.
Sedentarism has also been suggested as a diagnostic
label and a content validation by Fehring’s method
showed a global content validation index of .84 for the
same (Guirao-Goris, Pina, & Campo, 2000). A comple-
mentary study identified two different related factors,
‘‘expression of laziness’’ and ‘‘low performance of activ-
ities of daily living,’’ that are similar to two defining
characteristics proposed by the NANDA-I taxonomy.
The high index of the ‘‘diagnostic content validation’’
among specialized nurses has also been highlighted
(Guirao-Goris & Duarte-Climents, 2007).
Interest in validating the nursing diagnosis
sedentary lifestyle in the NANDA-I arose due to a lack of diagnostic labels and prior taxonomies dealing with
human behavioral responses related to insufficient
physical activity. The diagnosis was recognized by
the NANDA-I in 2004; it was defined as, ‘‘reports
a habit of life that is characterized by a low physical
activity level.’’ The defining characteristics include the
following: chooses a daily routine lacking physical
exercise, demonstrates physical deconditioning, and
verbalizes preference for activities low in physical
activity. The related factors are deficient knowledge
of health benefits of physical exercise, lack of
training for accomplishment of physical exercise,
lack of resources (time, money, companionship,
facilities), lack of motivation, and lack of interest
(NANDA-I, 2009).
Because of the recent inclusion of these elements
in the NANDA-I taxonomy, the number of studies
dealing with sedentary lifestyle as a nursing diagnosis
is low. However, there are global concerns about
this lifestyle because it constitutes a health risk
capable of having severe consequences for the lives of
individuals, families, and communities. Therefore,
the defining characteristics and related factors of
sedentary lifestyle need analysis with regard to their
representation in clinical practice. Patients with high
blood pressure can serve as an example population
here. Adequate assessment of individuals with high blood pressure and sedentary lifestyles is essential for
improved quality of care because it directs assistance
toward the specific needs of these individuals.
Rese arch ques tion sThis is a study to evaluate the predictors of sedentary
lifestyle in people with high blood pressure. The
research questions for this study were as follows:
(1) what is the reproducibility of the defining char-
acteristics and related factors of the sedentary lifestyle
diagnosis in patients with high blood pressure; (2)
what are the sensitivity, specificity, and predictive
value of the defining characteristics; and (3) what
are the possible predictors of the nursing diagnosis
sedentary lifestyle in patients with high blood pressure?
Methods
Desi gn and sa mple A cross-sectional study was conducted among 310 indi-
viduals (ranging in age from 18 to 69 years) with
confirmed high blood pressure and who were followed
up in the hypertension program. Any medical contrain-dications for physical activity mentioned by individuals
were criteria for exclusion, as were cognitive problems
that rendered data collection of pertinent information
impossible. Ethical approval was obtained from the
internal committee of the institute.
Patients were consecutively selected and the sample
size was defined based on the indicated formula for
cross-sectional studies with finite populations using the
following parameters: confidence coefficient of 95% and
sample error of 5%; population size of 6,042 patients
with high blood pressure registered in the program;
and sedentarism prevalence of 70% (Murphy et al.,
2005). It was not possible to use prevalence of the
diagnosis as a reference in the study because this value
was not found in the literature related to patients with
high blood pressure.
Measur esPrimary data were collected on a questionnaire admin-
istered to individuals on entry into the study during
194 Public Health Nursing Volume 28 Number 2 March/April 2011

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 3/9
a clinical consultation for follow-up of hypertension.
The questionnaire included variables related to the
assessment of defining characteristics and related
factors of the sedentary lifestyle diagnosis. The study
considered either the presence or the absence of the
diagnosis ‘‘sedentary lifestyle’’ as an outcome variable.
The long form of the International Physical Activity Questionnaire (IPAQ) was used in this study
(IPAQ, 2005; Benedetti et al., 2007). The question-
naire was divided into four parts. The first part was
designed to obtain personal and socio-demographic
data. The second part recorded behavior that related
to the habitual practice of physical activity, which
enabled the collection of data related to the defining
characteristics chooses a daily routine lacking physical
exercise and verbalizes preference for activities low in
physical activity.
The third part of the questionnaire assessed physical
conditioning by means of an instrument proposed
by the Cooperative Project-World Organization of
National Colleges and Academies (COOP/WONCA).
This instrument was validated for use in assessing
short-term physical conditioning processes and had
a Spearman correlation coefficient ranging from .66
to .81 (Tudela & Ferrer, 2002).
The fourth part of the questionnaire permitted
the collection of information concerning related factors
of the nursing diagnosis sedentary lifestyle. The instru-
ment facilitated gathering data related to possible
obstacles to practicing and understanding the relevanceof physical activities. In order to identify these barriers,
we used an instrument measuring the perception of the
difficulty of practicing physical activity. Testing showed
that the proposed questionnaire was satisfactory in its
applicability and clarity. It also permitted an acceptable
index of response reproducibility, with Pearson corre-
lation values ranging between .67 and .97 (Martins &
Petroski, 2000).
Specific knowledge about the importance of physical
activities was evaluated by calculating the number of
correct answers in 12 questions about physical activities
related to health that were proposed by InteliHealths
Inc. (InteliHealth, 2007). The information on the
Web site has been revised and approved by health
care professionals, the editors of InteliHealth, and
academic partners from Harvard Medical School and
the Columbia University College of Dental Medicine.
The questionnaire as a whole was subjected to
a pretest to verify its adequacy for measuring the
established objectives in the study and to inves-
tigate its ease of use. The resulting observations wer
incorporated and the final questionnaire wa
composed. The 14 individuals who participated in th
pretest were excluded from the final analysis.
An alyt ic st ra tegy
Studies of diagnostic tests usually include two analytical approaches: reproducibility and accuracy analyses
The first approach seeks to determine whether a mea
surement or a technique allows for the repeated identi
fication of a specific clinical condition. In studies o
clinical indicators for nursing diagnoses, the opinion o
specialist nurses is used as a way to assess the repro
ducibility of each indicator to characterize a diagnosis
For the purpose of making diagnostic inferences, dat
collected from each patient during the interview and
the list of defining characteristics and related factor
from the sedentary lifestyle nursing diagnosis wer
evaluated by three experts (A, B, and C) selected by th
Fehring criteria. At this stage, it is important to asses
agreement among the experts to minimize misclassi
fying subjects with either the presence or the absence o
the diagnosis. In this study, using the Kappa coefficient
concordance among experts was tested in the reproduc
ibility analysis regarding the presence or the absence o
the nursing diagnosis of a sedentary lifestyle and it
clinical indicators.
In nursing diagnosis research, the accurac
analysis is related to the confidence that a nurse ha
regarding the accuracy that a specific indicator wildetermine whether a patient truly has or lacks
particular diagnosis. Unfortunately, there are n
measures or techniques to serve as a gold standard
for the identification of nursing diagnoses. Thus, afte
verifying the classification and an agreement amon
experts, we decided to use agreement among expert
as the gold standard for identifying the presence of
sedentary lifestyle. This strategy was used to minimiz
bias on behalf of an expert’s individual opinion
During this stage, the sensitivity, specificity, an
predictive values were defined for each characteristic
For the analysis of the possible predictors of th
nursing diagnosis sedentary lifestyle, variables wer
analyzed using a t test with an assumption of equa
variances for the numerical variables. Assumptions o
normality and homoskedasticity were verified befor
performing the t tests. Pearson’s w2 test was used to an
alyze the categorical variables. The variables analyzed
included age, sex, birthplace, religion, marital status
occupation, educational level, income per capita, bod
Guedes et al.: Predictors of Sedentary Lifestyle 19
8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 4/9
mass index (BMI) classification, BMI value, time of
high blood pressure diagnosis, presence of diabetes,
defining characteristics, and related factors.
In the logistic regression the following were
included: variables that demonstrated statistical
significance lower than .2: age; presence of diabetes;
the three defining characteristics demonstrates physical deconditioning, chooses a daily routine
lacking physical exercise, and verbalizes preference
for activities low in physical activity; and the four
related factors lack of training for accomplishment
of physical exercise, lack of resources, lack of
motivation, and lack of interest .
From this selection, the variables were tested
to verify their overall association in order to clarify
the occurrence of the nursing diagnosis in question.
The Wald test was applied to verify the significance
of the coefficients that encompassed the logistic
equation. The Omnibus test verified the significance
of the developed model. The Hosmer-Lemeshow test
evaluated the difference between the observed and
the expected frequencies and the Nagelkerke R2 test
estimated the determined capacity of the model.
In addition to these statistics, the final definition
of the predictors considered the reduction of the
logarithm of the maximum likelihood ratio (À2log).
Results
The age, education level, and per capita income werenonnormally distributed. The median education was
9 years, the median per capita income was US$124.79
monthly, and the median age was 56 years. The
majority of individuals were female (65.5%), from
the capital Fortaleza (86.1%), Catholic (74.5%), and
married (64.5%).
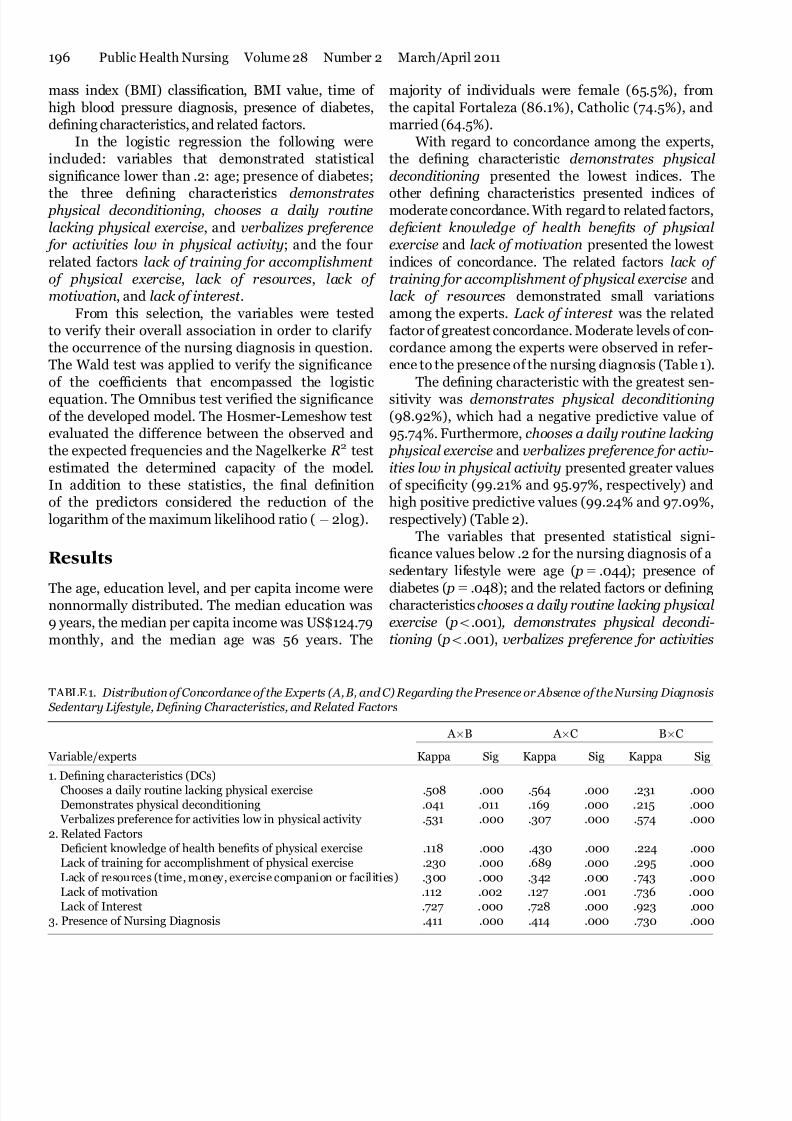
With regard to concordance among the experts,
the defining characteristic demonstrates physical
deconditioning presented the lowest indices. The
other defining characteristics presented indices of moderate concordance. With regard to related factors,
deficient knowledge of health benefits of physical
exercise and lack of motivation presented the lowest
indices of concordance. The related factors lack of
training for accomplishment of physical exercise and
lack of resources demonstrated small variations
among the experts. Lack of interest was the related
factor of greatest concordance. Moderate levels of con-
cordance among the experts were observed in refer-
ence to the presence of the nursing diagnosis (Table 1).
The defining characteristic with the greatest sen-
sitivity was demonstrates physical deconditioning
(98.92%), which had a negative predictive value of
95.74%. Furthermore, chooses a daily routine lacking
physical exercise and verbalizes preference for activ-
ities low in physical activity presented greater values
of specificity (99.21% and 95.97%, respectively) and
high positive predictive values (99.24% and 97.09%,
respectively) (Table 2).
The variables that presented statistical signi-
ficance values below .2 for the nursing diagnosis of a
sedentary lifestyle were age ( p5 .044); presence of
diabetes ( p5 .048); and the related factors or definingcharacteristics chooses a daily routine lacking physical
exercise ( po.001), demonstrates physical decondi-
tioning ( po.001), verbalizes preference for activities
TABLE 1. Distribution of Concordance of the Experts (A, B, and C) Regarding the Presence or Absence of the Nursing Diagnosis Sedentary Lifestyle, Defining Characteristics, and Related Factors
Variable/experts
A ÂB A ÂC BÂC
Kappa Sig Kappa Sig Kappa Sig
1. Defining characteristics (DCs)
Chooses a daily routine lacking physical exercise .508 .000 .564 .000 .231 .000Demonstrates physical deconditioning .041 .011 .169 .000 .215 .000 Verbalizes preference for activities low in physical activity .531 .000 .307 .000 .574 .000
2. Related FactorsDeficient knowledge of health benefits of physical exercise .118 .000 .430 .000 .224 .000Lack of training for accomplishment of physical exercise .230 .000 .689 .000 .295 .000
Lack of resources (time, money, exercise companion or facilities) .300 .000 .342 .000 .743 .000Lack of motivation .112 .002 .127 .001 .736 .000Lack of Interest .727 .000 .728 .000 .923 .000
3. Presence of Nursing Diagnosis .411 .000 .414 .000 .730 .000
196 Public Health Nursing Volume 28 Number 2 March/April 2011

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 5/9
low in physical activity ( po.001), lack of training for
accomplishment of physical exercise ( po.001), lack of
resources ( po.001), lack of motivation ( po.001), and
lack of interest ( po.001).
Among these variables, demonstrates physical
deconditioning, verbalizes preference for activities
low in physical activity, and lack of training for
accomplishment of physical exercise were identified
as significant predictive indicators. The logistic model
developed was statistically significant according to
the Omnibus test ( po.001), and it enabled the iden-
tification of the presence of the diagnosis from
these three variables of the model. No significant
differences were identified among the observed and
expected frequencies in the final model ( p5 .202).
The coefficients of each variable included in the model
demonstrated statistical significance according to the
Wald test ( po.05). The determination coefficient
of the model was .852; this coefficient implied that
the variables included in the model explained 85.2%
of the occurrence of the nursing diagnosis of a seden-tary lifestyle in patients with high blood pressure. This
fact was confirmed through the reduction of the
maximum likelihood ratio (À2 log) (Table 3).
Discussion
Studies have shown that the problem of physical
inactivity is a worldwide concern and indicated that a
large segment of the population does not follow current
recommendations regarding the practice of physica
activities (Altieri et al., 2004; Bernstein et al., 2001)
Worldwide inactivity justifies the creation and us
of the defining characteristic chooses a daily routin
lacking physical exercise (Hallal et al., 2005). Con
versely, a previous study has demonstrated that regula
physical exercise was associated with a significan
reduction in cardiovascular morbidity and mortalit
as well as an improvement in the cardiac illness reha
bilitation process (Lee & Skerrett, 2001).
A study comparing active and sedentary banker
found a relationship between the defining character
istics chooses a daily routine lacking physica
exercise and verbalizes preference for activities low
in physical activity. In the study, the active group
perceived regular physical exercise as a source o
pleasure because it afforded them the opportunit
to forget work-related problems. Conversely, thos
who were considered sedentary verbally reporte
preferring activities with little physical exercise du
to a lack of motivation. Instead, they opted for activities that were calming and less physically strenuou
(Andrade et al., 2005).
The fact that the defining characteristic demon
strates physical deconditioning was the greates
sensitivity measure for the sedentary lifestyle diagno
sis is likely due to the simplicity and clarity of the
individual self-evaluation tool. The findings should b
viewed with caution because effective physical fitnes
depends on the thorough execution of well-planned
TABLE 2. Sensitivity Value (SE), Specificity Value (SP), Positive Predictive Value (PPV), and Negative Predictive Value (NPV for the Defining Characteristics of the Sedentary Lifestyle
Defining characteristics SE (%) SP (%) PPV (%) NPV (%
Chooses a daily routine lacking physical exercise 69.35 99.21 99.24 68.51Demonstrates physical deconditioning 98.92 36.29 69.96 95.74 Verbalizes preference for activities low in physical activity 89.78 95.97 97.09 86.23
TABLE 3. Logistic Regression for the Predictive Factors of the Presence of the Nursing Diagnosis of a Sedentary Lifestyle
Predictors OMN HL R2À2 log Wald
o.001 .202 .852 219.511Demonstrates physical deconditioning .00 Verbalizes preference for activities low in physical activity o.00Lack of training for accomplishment of physical exercise o.00Constant o.00
Note. OMN5Omnibus test; HL 5Hosmer and Lemeshow test; R25Nagelkerke R2; 2log5Logarithm of likelihood ratio
Wald5 Wald test.
Guedes et al.: Predictors of Sedentary Lifestyle 19

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 6/9
activities and is influenced by the initial level of cardio-
vascular fitness of the individual as well as the type,
velocity, frequency, duration, and intensity of the
fitness session (Mcardle et al., 2006). In the present
study, a demonstrates physical deconditioning defin-
ing characteristic was tied to a chooses a daily routine
lacking physical exercise characteristic, which may result in an individual’s preference for activities with
little physical exertion.
Despite the low indices of concordance for deficient
knowledge of health benefits of physical exercise
among the experts, the literature highlights the fact that
a knowledge deficit about exercising, the purpose of
exercise, the limitations of some populations (as well as
distorted perceptions), and the benefits of movement is
one reason why individuals have sedentary lifestyles.
Conversely, increasing knowledge about physical
activity can prevent an increase in sedentarism
(Domingues & Araujo, 2004). Patients’ knowledge
about their health conditions, therapeutic treatments,
and prevention can facilitate adherence to regimens
and to maintenance of or improvement in well-being.
Additionally, patients can avoid changes in overall
health due to uncontrollable blood pressure levels.
Finally, lack of knowledge, motivation, and interest
in physical activity were also considered important
elements in understanding the adherence of high
blood pressure patients to physical activity programs
(Chummun, 2009).
Another topic that merits discussion is a relatedfactor: lack of training for the accomplishment of
physical exercise. This variable is an important etiologic
factor when considering the diagnosis of a sedentary
lifestyle in patients with high blood pressure. After a
period of training, patients with slight-to-moderately
high blood pressure who regularly perform dynamic
exercise can achieve a significant decrease in their
diastolic and systolic pressures during periods of both
rest and stress (Chobanian et al., 2003; Pitt et al., 2003).
These data may suggest the promotion of activities that
do not require training, such as walking.
In addition, regular training programs also pro-
vide better physical fitness for individuals and create
sustainable mechanisms for maintaining daily physi-
cal exercise routines (thereby increasing activity).
This relationship was demonstrated in this study,
in that the characteristics or factors chooses a daily
routine lacking physical exercise, demonstrates
physical deconditioning, and lack of training for
accomplishment of physical exercise increased the
probability that patients with high blood pressure
would develop a sedentary lifestyle.
With regard to the related factor lack of resources,
the findings demonstrated that interference from
family, friends, health care professionals, climate,
structure, time availability, and financial resources
influenced adherence to physical fitness regimens.Stimulation of patients with high blood pressure to
develop a more active lifestyle represents a valuable
tool for improving health standards. To become more
active, patients need to be educated and receive
adequate information and motivators. They also need
to belong to physical fitness groups and have access to
favorable conditions (e.g., financial resources, free time,
and nearby fitness locations). In the present study, the
factor lack of resources was not predictive, but it is
important in clinical practice. In the institution where
the study was developed, patients received all medi-
cations and had free access to all services; this may have
influenced our results.
In addition, analyses of the sensitivity and speci-
ficity of the defining characteristics in this investigation
indicated that demonstrates physical deconditioning
was the most sensitive variable; in contrast, chooses a
daily routine lacking physical exercise and verbalizes
preference for activities low in physical activity were
the most specific variables for the nursing diagnosis
under study.
Of the proposed characteristics for the diagnosis
of sedentarism, a previous study demonstrated thatverbal expression of the family of having a sedentary
lifestyle and verbalizing a preference for activities
with low or no physical activity yielded scores with a
diagnostic content validation superior than or equal
to 80; these scores were considered critical or specific
(Guirao-Goris et al., 2000). Conversely, the charac-
teristics realizes exclusively operational activities
of daily living and diminished capacity to execute
physical activity: poor physical conditioning (COOP/
WONCA score ! 3) had scores lower than 80 and
were classified as minor defining characteristics.
In a similar investigation by Guirao-Goris
and Duarte-Climents (2007), no characteristic had a
diagnostic content validation greater than 80. In
contrast, the characteristics verbal expression from
the family and/or a person of having a sedentary
lifestyle, verbalizes preference for activities with low
or no physical activity, and the presence of a COOP /
WONCA score ! 3 received higher scores of 70, 74,
and 73, respectively.
198 Public Health Nursing Volume 28 Number 2 March/April 2011

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 7/9
Consequently, we believe that the differences
between specificity and sensitivity, which are influenced
by the diagnostic prevalence, directly depend on the
characteristics of the studied population. There is a
need to further investigate this hypothesis in diverse
population contexts to better clarify this question. For
Tanner and Hugles (1984), the relationship betweenthe clinical indicators and diagnosis could only be
validated after repeated and systematic observations
that required the development of new research with
additional subjects.
Although the classification of the physical activity
level by the IPAQ has the advantage of offering
an evaluation of physical activity in diverse contexts,
it is necessary to consider the potential recall bias
of the participants. Because of the length and detail
of the questionnaire with regard to the number and
period of executed activities, we concluded that
participants at times only estimated these values. This
estimation made it difficult to capture reliable infor-
mation fundamental for the development of the study.
Regarding the validity and reliability of these mea-
sures, we used standard techniques and calibrated
instruments for our clinical assessment. Moreover,
observation and evaluation biases are usually present
in studies of this nature. These biases can be associated
with different levels of experience and knowledge, the
omission of clinical data, lack of attention, and prema-
ture inferences. Despite the experience and selection
criteria used, one cannot guarantee that bias will not be present. In addition, it is necessary explain that
cross-sectional studies cannot show direction or cause.
Thus, the results should be considered in the context of
their limitations.
Unfortunately, data related to levels of hyperten-
sion and the use of medications were not investigated
because the study institution primarily serves indi-
viduals with severe hypertension (SBP4179 and/or
DBP4109). This limitation should be considered when
generalizing the results, and further studies investi-
gating the relationship between a sedentary lifestyle
with these variables are encouraged.
Another point to consider is the lack of studies
regarding the nursing diagnosis sedentary lifestyle.
This dearth made it difficult to compare and discuss
findings relevant to this research. This fact increases
the importance of developing new studies that involve
this nursing diagnosis.
The defining characteristic with greatest sensitivity
for the sedentary lifestyle diagnosis was demonstrates
physical deconditioning. The characteristics chooses a
daily routine lacking physical exercise and verbalize
preference for activities low in physical activit
showed the greatest specificity values. The indicator
identified as predictors of sedentary lifestyle wer
demonstrates physical deconditioning, verbalizes pref
erence for activities low in physical activity, and lacof training for accomplishment of physical exercise.
This study serves as a guide for the diagnosti
efficiency of clinical indicators for the sedentar
lifestyle diagnosis and contributes to improving diag
nostic accuracy by determining sensitivity, specificity
and positive and negative predictive factors. We cal
attention to the fact that the accuracy in question ha
not been sufficiently investigated in studies regardin
nursing diagnoses. We recognize the need to develop
studies examining the sedentary lifestyle diagnosis
Such studies are fundamental in order to better delin
eate the defining characteristics, develop more accurat
measurement instruments, and conduct clinical vali
dation in other contexts.
References
Altieri, A., Tavani, A., Gallus, S., & Vecchia, L. A(2004). Occupational and leisure time physicaactivity and the risk of nonfatal myocardiainfarction in Italy. Annals of Epidemiology14(7), 461–466.
Andrade, A., Back, A., Vasconcellos, D. I. C., & VianaM. S. (2005). Auto-evaluation of the healthstress and productivity in the work of activand sedentary bank clerks. Journal of Sporand Exercise Psychology, 27 (suppl), s31.
Benedetti, T. R. B., Antunes, P. C., Anez, C. R. R.Mazo, G. Z., & Petroski, E. L. (2007). Reproducibility and validity of the InternationaPhysical Activity Questionnaire (IPAQ) ielderly men. Revista Brasileira de Medicindo Esporte, 13(1), 11–16.
Bernstein, M. S., Costanza, M. C., & Morabia, A(2001). Physical activity of urban adults: A
general population survey in Geneva. Sozia Praventivmedizin, 46(1), 49–59.
Chang, B. L., Uman, G. C., & Hirsch, M. (1998)Predictive power of clinical indicators for selfcare deficit. Nursing Diagnosis, 9(2), 71–82.
Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman W. C., Green, L. A., Izzo, J. L., et al. (2003). Thseventh report of the Joint National Committeon Prevention, Detection, Evaluation, and Treatment of high blood pressure: The JNC 7 report
Guedes et al.: Predictors of Sedentary Lifestyle 19

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 8/9
Journal of the American Medical Association,289(19), 2560–2572.
Chummun, H. (2009). Hypertension—a contem-porary approach to nursing care. British
Journal of Nursing, 18(13), 784–789.Damewood, B. M., & Carlson-Catalano, J. (2000).
Physical activity deficit: A proposed nursingdiagnosis. Nursing Diagnosis, 11(1), 24–31.
Domingues, M. R., & Araujo, C. L. P. (2004). Knowl-edge and perceptions of physical exercise in anadult urban population in Southern Brazil.Cadernos de Saude Publica, 20(1), 204–215.
Guirao-Goris, J. A., & Duarte-Climents, G. (2007).The expert nurse profile and diagnostics con-tent validity of sedentary lifestyle: The Spanish
validation. International Journal of NursingTerminologies and Classifications, 18(3), 84–92.
Guirao-Goris, J. A., Pina, M. P., & Campo, P. M. (2000).
Validacion del contenido diagnostico de la etiqu-eta diagnostica enfermera ‘‘sedentarismo’’.
Enfermerıa Clınica, 11(4), 135–140.Hallal, P. C., Matsudo, S. M., Matsudo, V. K., Araujo,
T. L., Andrade, D. R., & Bertoldi, A. D. (2005).Physical activity in adults from two Brazilianareas: Similarities and differences. Cadernosde Saude Publica, 21(2), 573–580.
International Physical Activity Questionnaire [IPAQ].(2005). Research Committee. Guidelines for data processing and analysis of the Interna-tional Physical Activity Questionnaire: Short and long form. Retrieved from http://www.ipaq.ki.se
InteliHealth. (2007). Fitness. Exercise. Retrievedfrom http://www.intelihealth.com/IH/ihtIH/
WSIHW000/7165/24439/335060.html?d=dmtContent
Lee, I. M., & Skerrett, P. J. (2001). Physical activity and all-cause mortality: What is the dose
response relation? Medicine and Sciencein Sports and Exercise, 33(Suppl. 6), S459–S471.
Lunney, M. (2001). Critical thinking & nursing diag-noses: Case studies & analyses. Philadelphia,PA: NANDA.
Martins, M. O., & Petroski, E. L. (2000). Perception of physical activities barriers measurement: Aninstrument proposition. Brazilian Journal of
Kinanthropometry and Human Performance,2(1), 58–65.
Mcardle, W. D., Katch, F. I., & Katch, V. L. (2006). Exercise physiology: Energy, human perfor-mance. Philadelphia, PA: Lippincott Williams& Wilkins.
Murphy, E. S., Krummel, D. A., Morrison, N., &Gordon, P. M. (2005). Environmental percep-tions related to physical activity in high- andlow-risk counties. Health Promotion Practice,
6(1), 57–63.NANDA International [NANDA-I]. (2009). Nursing
diagnoses: Definitions & classification,2009–2011. Oxford, U.K.: Wiley-Blackwell.
Parker, L., & Lunney, M. (1998). Moving beyond con-tent validation of nursing diagnosis. Nursing
Diagnosis, 9(4), 144–150.Pitt, B., Remme, W., & Zannad, F. (2003). Eplerenome, a
selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarc-tion. New England Journal of Medicine, 348,1309–1321.
Tanner, C.A, & Hugles, A. M. (1984). Nursing diagnosis:Issues in clinical practice research. Clinical
Nursing, 5 (4), 30–38.Tudela, L. L., & Ferrer, A. R. (2002). Adaptacion
transcultural de una medida de la calidad de vida relacionada con la salud: la version espa-nola de las vinetas COOP/WONCA. Atencion
Primaria, 24(2), 75–82.
200 Public Health Nursing Volume 28 Number 2 March/April 2011

8/2/2019 58633929
http://slidepdf.com/reader/full/58633929 9/9
Copyright of Public Health Nursing is the property of Wiley-Blackwell and its content may not be copied or
emailed to multiple sites or posted to a listserv without the copyright holder's express written permission.
However, users may print, download, or email articles for individual use.