5 sewell gi - ucsf medical education sewell gi.pdf · history"of"stricture"! ......
TRANSCRIPT
UCSF, Department of Medicine, CME
1
1
GASTROENTEROLOGY
Jus&n L. Sewell, MD, MPH, FACP Assistant Professor of Medicine Division of Gastroenterology UC San Francisco | San Francisco General Hospital
Disclosures
l No rela&onships or conflicts of interest to disclose
2

UCSF, Department of Medicine, CME
2
Agenda
l Top-‐to-‐boLom overview of GI content most per&nent to IM boards
l Cases with discussion l Addi&onal boards-‐relevant informa&on with guideline references
l Pause for ques&ons aPer each session but ask any&me
3
Case #1 l 42 year old Caucasian man with heartburn l IntermiLent retrosternal burning ~2 years
l Increasing use of antacids & OTC H2RAs, with only transient relief of symptoms
l 1-‐2 packs cigareLes QD, 1-‐2 glasses wine QHS l Regurgita&on of sour material at night, but no dysphagia
l Elevates head of bed and has lost weight without benefit
UCSF, Department of Medicine, CME
3
Case #1 – What is the most appropriate next step in management?
1. Perform upper endoscopy 2. Trial of high-‐dose PPI for 4-‐6 weeks 3. Stop all caffeine and alcohol 4. Esophageal pH tes&ng 5. Take H2RA scheduled rather than prn
5
Case #1 – What is the most appropriate next step in management?
1. Perform upper endoscopy 2. Trial of high-‐dose PPI for 4-‐6 weeks 3. Stop all caffeine and alcohol 4. Esophageal pH tes&ng 5. Take H2RA scheduled rather than prn
6

UCSF, Department of Medicine, CME
4
IndicaEons for endoscopy in GERD
Men and women with: l Alarm symptoms l GERD refractory to PPI l Severe erosive esophagi&s l Recurrent dysphagia with
history of stricture l Known BarreL’s esophagus
Men only with: l GERD>5 years AND
addi&onal risk factors for esophageal cancer (single screening EGD) l Nocturnal reflux l Obesity l Central adiposity l Smoking l Hiatal hernia
7 Shaheen NJ. Ann Intern Med 2012; 157(11):808-‐16.
8
Case #1
l Symptoms par&ally improved on PPI à EGD l EGD: 2 cm tongue of salmon colored mucosa in the distal
esophagus, otherwise unremarkable l Biopsies: intes&nal metaplasia with no dysplasia

UCSF, Department of Medicine, CME
5
9
Case #1 – Which is the most appropriate next step?
1. Repeat EGD for surveillance within 1 year
2. Test for H. pylori infec&on and treat if present
3. Radiofrequency abla&on of the BarreL’s mucosa
4. Refer to surgeon for an&-‐reflux surgery
5. Double the dose of his PPI to BID and follow symptoma&cally
10
1. Repeat EGD for surveillance within 1 year
2. Test for H. pylori infec&on and treat if present
3. Radiofrequency abla&on of the BarreL’s mucosa
4. Refer to surgeon for an&-‐reflux surgery
5. Double the dose of his PPI to BID and follow symptoma&cally
Case #1 – Which is the most appropriate next step?
UCSF, Department of Medicine, CME
6
Case #1 – BarreL’s surveillance
l Risk of progression to cancer is low (<1% per year)
l No dysplasia: EGD every 3-‐5 years l Low grade dysplasia: repeat 6 months, then annually
l High grade dysplasia: confirm by 2nd pathologist à abla&on or esophagectomy due to concomitant adenocarcinoma in 30-‐40%
11 ASGE Standards of Prac&ce CommiLee. Gastrointest Endosc 2012; 76(6):1087-‐94.
12
Case #1 – BarreL’s management
l Medical or surgical an&-‐reflux therapies do not cause regression of BarreL’s; goal is to control symptoms and minimize cancer risk
l Radiofrequency abla&on (RFA) eradicates 80-‐95% of dysplasia and reduces life&me cancer risk from 9% to 1%
l An&-‐reflux surgery reserved for failures of op&mal medical therapy or pa&ent preference
UCSF, Department of Medicine, CME
7
13
Case #1
l Eradicate H pylori when diagnosed l Reduces risk of PUD, gastric cancer
l However this does not affect progression of BarreL’s and could theore&cally worsen GERD
14
GERD
l GERD can cause chest pain but can be difficult to dis&nguish from cardiac source based on history alone l PPI trial l Cardiac tes&ng in selected pa&ents
l GERD can cause globus and dysphagia à PPI trial l Func&onal heartburn and non erosive reflux disease are
common and are less responsive to acid suppression l Esophageal pH monitoring required to diagnose
l PPI should be taken 30-‐60 minutes before ea&ng for op&mal acid suppression
UCSF, Department of Medicine, CME
8
15
GERD
l GERD can be exacerbated by l Impaired salivary flow (Sjögrens, XRT) l Esophageal dysmo&lity (scleroderma) l Gastric distension (gastroparesis, dietary habits) l Reduced LES pressure (chocolate, alcohol, nico&ne, CCBs, nitrates, an&depressants, progesterone, benzodiazepines)
l Atypical (extraesophageal) GERD manifesta&ons include: chronic cough, hoarseness, laryngi&s, asthma
16
Dysphagia
l Dysphagia: source suggested by symptoms l IntermiLent solid: Schatzki ring, eosinophilic esophagi&s l Progressive solid: stricture/achalasia (slow) or neoplasm (rapid) l Solid and liquid: dysmo&lity
l EGD usually first test though can consider esophagram l Manometry tes&ng if EGD nondiagnos&c
l Achalasia: lack of peristalsis and non-‐relaxing LES l Oropharyngeal dysphagia usually due to neuromuscular
disorders, and is associated w/ coughing, nasal regurgita&on, choking

UCSF, Department of Medicine, CME
9
17
Eosinophilic esophagiEs
l Eosinophilic esophagi&s l IntermiLent solid food dysphagia or food impac&on, M>F
l Ringed or “feline” esophagus l Eosinophilic infiltrate on biopsy l Treat with elimina&on diet, swallowed inhaled steroids, PPIs
Dellon ES. Gastroenterology 2014; 147(6):1238-‐54.
18
Case #2
l 62 y/o woman with 4 months of epigastric abdominal pain, worse post-‐prandially
l Incompletely relieved by OTC H2RAs l Occasional nausea but no vomi&ng l Mild anorexia l 5 pound weight loss l ASA 81mg/d and PRN ibuprofen for arthri&s l PEx: mild epigastric TTP, otherwise unremarkable

UCSF, Department of Medicine, CME
10
19
Case #2 Which of the following is the best approach at this Eme? 1. Empiric H pylori treatment
2. H pylori tes&ng and treatment if posi&ve
3. Empiric proton pump inhibitor Rx
4. Upper endoscopy
5. Switch ibuprofen to a COX-‐2 NSAID
20
Case #2 Which of the following is the best approach at this Eme? 1. Empiric H pylori treatment
2. H pylori tes&ng and treatment if posi&ve
3. Empiric proton pump inhibitor Rx
4. Upper endoscopy
5. Switch ibuprofen to a COX-‐2 NSAID
UCSF, Department of Medicine, CME
11
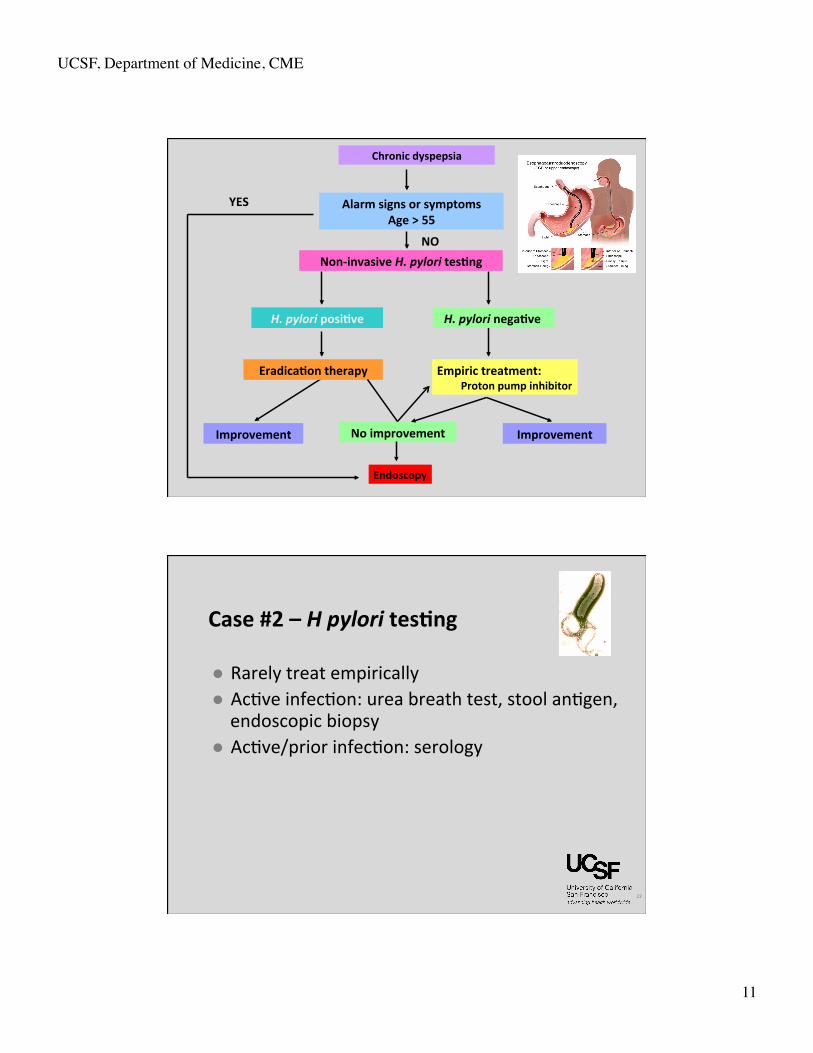
Non-‐invasive H. pylori tesEng
H. pylori negaEve
Chronic dyspepsia
H. pylori posiEve
EradicaEon therapy Empiric treatment: Proton pump inhibitor
Endoscopy
Improvement Improvement No improvement
YES
NO
Alarm signs or symptoms Age > 55
22
Case #2 – H pylori tesEng
l Rarely treat empirically l Ac&ve infec&on: urea breath test, stool an&gen, endoscopic biopsy
l Ac&ve/prior infec&on: serology

UCSF, Department of Medicine, CME
12
23
Case #2 – Empiric PPI
l Empiric acid-‐suppression has some efficacy in dyspepsia, and is reasonable in young pa&ents with no alarm symptoms
l COX-‐2 selec&ve NSAIDs have less GI toxicity l New dyspepsia in pa&ents over age 50, dyspepsia with alarm symptoms or family history of gastric cancer, should have EGD to rule out cancer
24
H pylori
l Usually acquired in childhood, person to person transmission l Inverse associa&on with socioeconomic status l OPen asymptoma&c
l 10-‐20% PUD l <0.01% gastric CA
l Treatment: l Triple: PPI, clarithromycin, amoxicillin x 10-‐14 days l Quadruple: PPI, bismuth, metronidazole, tetracycline x 10-‐14 days l Other an&bio&c op&ons include levofloxacin, rifabu&n, nitazoxanide
UCSF, Department of Medicine, CME
13
25
PepEc ulcer disease
l GUs require biopsy & repeat EGD to exclude CA l Mul&ple non-‐healing ulcers, or ulcers w/ diarrhea: suspect ZES. Best ini&al test: fas&ng serum gastrin
l Elevated gastrin seen in gastric outlet obstruc&on, PPI use, pernicious anemia, renal insufficiency, diabetes, and gastrinoma
l Gastrin levels >1000 highly suspicious for ZES; 200-‐1000 best evaluated with secre&n s&mula&on test (paradoxical rise in gastrin aPer secre&n administered)
26
UGI bleed
l High risk GIB pa&ents taking NSAIDS: l Known PUD, advanced age, warfarin l Test and treat for H pylori l Co-‐prescribe PPI
l Stress, caffeine, prednisone do not cause PUD

UCSF, Department of Medicine, CME
14
27
UGI bleed
l UGIB may present as hematochezia if brisk, and conversely, slow right-‐sided colonic bleeding may cause melena
l NG tube only 85% sensi&ve in UGIB l Most UGIB will stop spontaneously l Most UGIB can be effec&vely managed by EGD or angiography
l Surgery indicated if persistent or recurrent exsanguina&on
Common causes of upper GI bleeding
PUD (50%)
Mallory-‐Weiss tear (10%)
Varices / portal hypertension (20%)
Erosive gastri&s (10%)
UCSF, Department of Medicine, CME
15
29
UGI bleed
l Mortality risk ~10% l Increased with advance age, shock, hematochezia, cirrhosis
l EGD: diagnos&c, therapeu&c, prognos&c l IR and surgery are backup l Medical therapy with PPI bolus + con&nuous infusion
l No role for H2RA’s
30
Case #3
l 47 y/o male execu&ve admiLed with severe abdominal pain radia&ng to his back
l Drinks 2-‐3 cocktails per day, occasionally more l PEx notable for mid-‐abdominal tenderness with hypoac&ve bowel sounds
l Lipase 9,200 l Ini&al management: NPO, analgesia and hydra&on

UCSF, Department of Medicine, CME
16
Case #3
l Addi&onal labs: l WBC 11,000 l Bili 1.6, AST 95, ALT 32, AlkP 120 l Triglycerides 220 l Calcium 8.5
31
Case #3 What is the most appropriate next diagnosEc step? 1. Ultrasound of the abdomen 2. Empiric an&bio&cs 3. MRCP 4. Surgical consulta&on 5. Trend liver tests and lipase, follow exam
32

UCSF, Department of Medicine, CME
17
Case #3 What is the most appropriate next diagnosEc step? 1. Ultrasound of the abdomen 2. Empiric an&bio&cs 3. MRCP 4. Surgical consulta&on 5. Trend liver tests and lipase, follow exam
33
34
Case #3
l U/S: normal GB and CBD, pancreas is “obscured by overlying bowel gas”
l An&bio&cs not recommended l By hospital day #8, his lipase has normalized but his abdominal pain is worsening slightly, and he has developed new fevers to 101.8, with a rising WBC
Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.

UCSF, Department of Medicine, CME
18
35
Case #3 Which of the following is the best approach at this Eme? 1. Ini&ate oral feeds, as lipase is normal
2. Empiric an&bio&cs
3. Epidural catheter and PCA
4. ERCP
5. CT scan of the pancreas
36
Case #3 Which of the following is the best approach at this Eme?
1. Ini&ate oral feeds, as lipase is normal
2. Empiric an&bio&cs
3. Epidural catheter and PCA
4. ERCP
5. CT scan of the pancreas
UCSF, Department of Medicine, CME
19
37
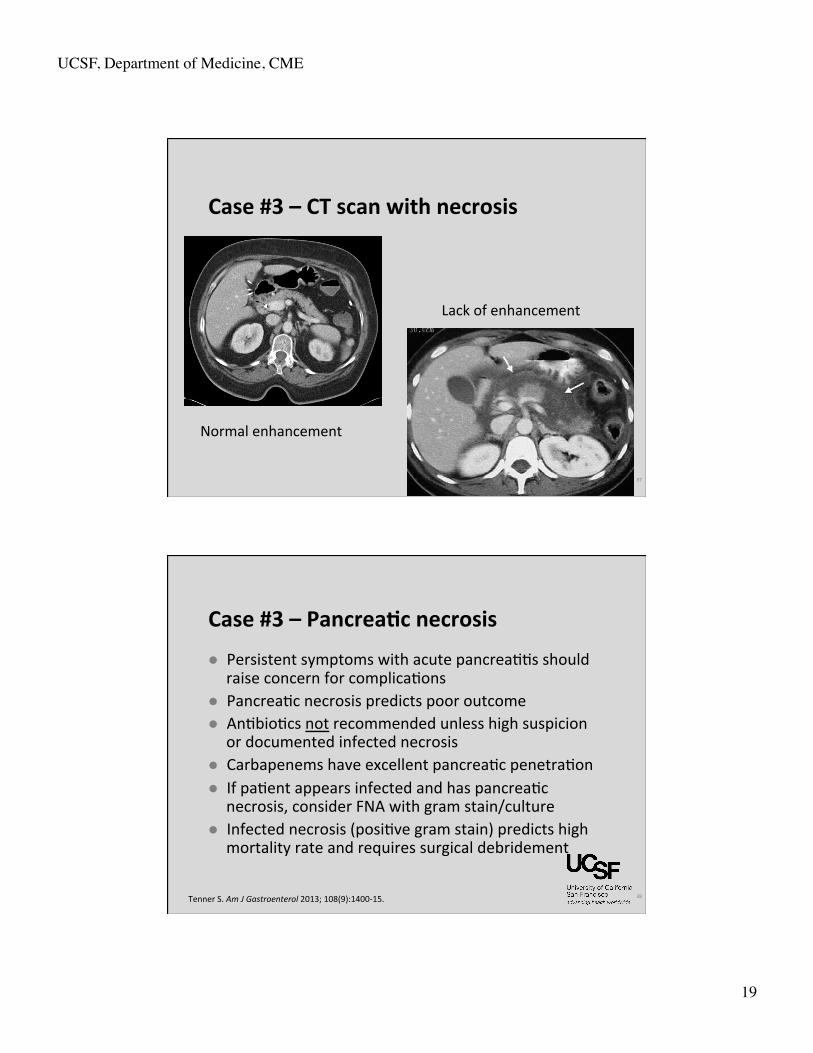
Case #3 – CT scan with necrosis
Normal enhancement
Lack of enhancement
38
Case #3 – PancreaEc necrosis
l Persistent symptoms with acute pancrea&&s should raise concern for complica&ons
l Pancrea&c necrosis predicts poor outcome l An&bio&cs not recommended unless high suspicion
or documented infected necrosis l Carbapenems have excellent pancrea&c penetra&on l If pa&ent appears infected and has pancrea&c
necrosis, consider FNA with gram stain/culture l Infected necrosis (posi&ve gram stain) predicts high
mortality rate and requires surgical debridement
Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.
UCSF, Department of Medicine, CME
20
Case #3 – ERCP for pancreaEEs
l ERCP if biliary source for pancrea&&s suspected l ALT is first to rise followed by bilirubin and alkP l Biliary dila&on (US, CT, MRCP)
l Wait for pancrea&&s to improve unless obstruc&ng CBD stone on imaging or suspected cholangi&s
39 Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.
40
Case #3 – Acute pancreaEEs management
l Can assess prognosis w/ Ranson or APACHE II l Serial amylase/lipase levels not useful in predic&ng course
l Obtain CT if severe pancrea&&s is suspected (organ failure, lack of improvement, increasing pain, fever, WBC, hypotension)
l Necrosis on CT has worst prognosis
Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.

UCSF, Department of Medicine, CME
21
41
l Prophylac&c an&bio&cs not indicated l Early studies evaluated agents with poor pancreas penetra&on and included pa&ents with mild disease
l Best therapy is good suppor&ve care and aggressive hydra&on (250-‐500 mL/hour, bolus if hypovolemic)
Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.
Case #3 – Acute pancreaEEs management
42
Case #3 – When to feed
l Pa&ents can eat when pain-‐free and hungry l Liquid diet and low-‐fat solid diet are equivalent l Post-‐duodenal enteral feeding may be appropriate in pa&ents with acute pancrea&&s but does not improve outcomes compared with on-‐demand oral feeding
Bakker OJ. New Engl J Med 2014; 371(21):1983-‐93. Tenner S. Am J Gastroenterol 2013; 108(9):1400-‐15.

UCSF, Department of Medicine, CME
22
43
Acute pancreaEEs – eEologies
l Most common e&ologies: gallstones and alcohol l Less common: hypertriglyceridemia, post‑ERCP, pregnancy, hypercalcemia, viral, hereditary, autoimmune
l Medica&ons: Erythromycin, tetracycline, 6‑MP/AZA, sulfas, 5‑ASAs, NSAIDs, estrogens, thiazides
Chronic pancreaEEs
l Exocrine and endocrine manifesta&ons l Imaging: dilated duct, calcifica&ons l Enzymes beLer for steatorrhea than pain l For pain can consider celiac plexus block, surgical op&ons
l Can cause biliary obstruc&on l Pancreas divisum: failure of fusion of dorsal and ventral glands; found in 5% of popula&on; may predispose to chronic pancrea&&s
44
UCSF, Department of Medicine, CME
23
Let’s take a detour into… radiology
l Common abdominal x-‐rays you might see on boards
45
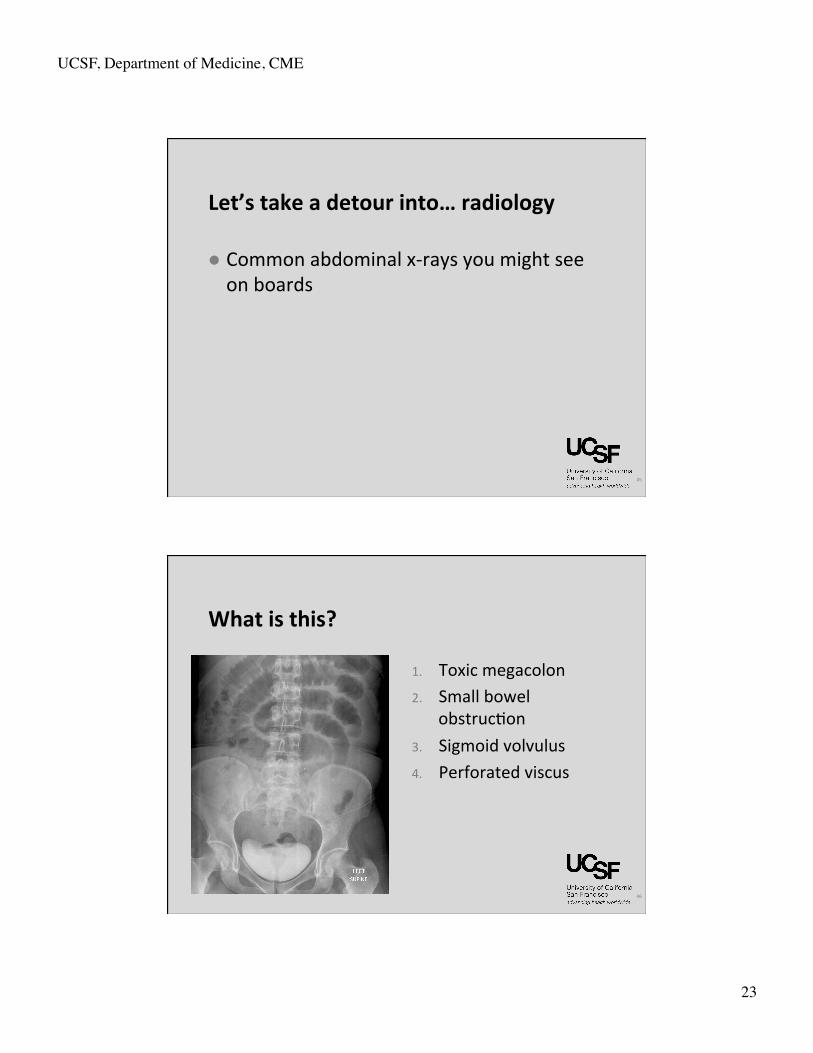
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
46

UCSF, Department of Medicine, CME
24
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
47
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
48

UCSF, Department of Medicine, CME
25
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
49
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
50

UCSF, Department of Medicine, CME
26
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
51
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
52

UCSF, Department of Medicine, CME
27
What is this?
1. Toxic megacolon 2. Small bowel
obstruc&on 3. Sigmoid volvulus 4. Perforated viscus
53
54
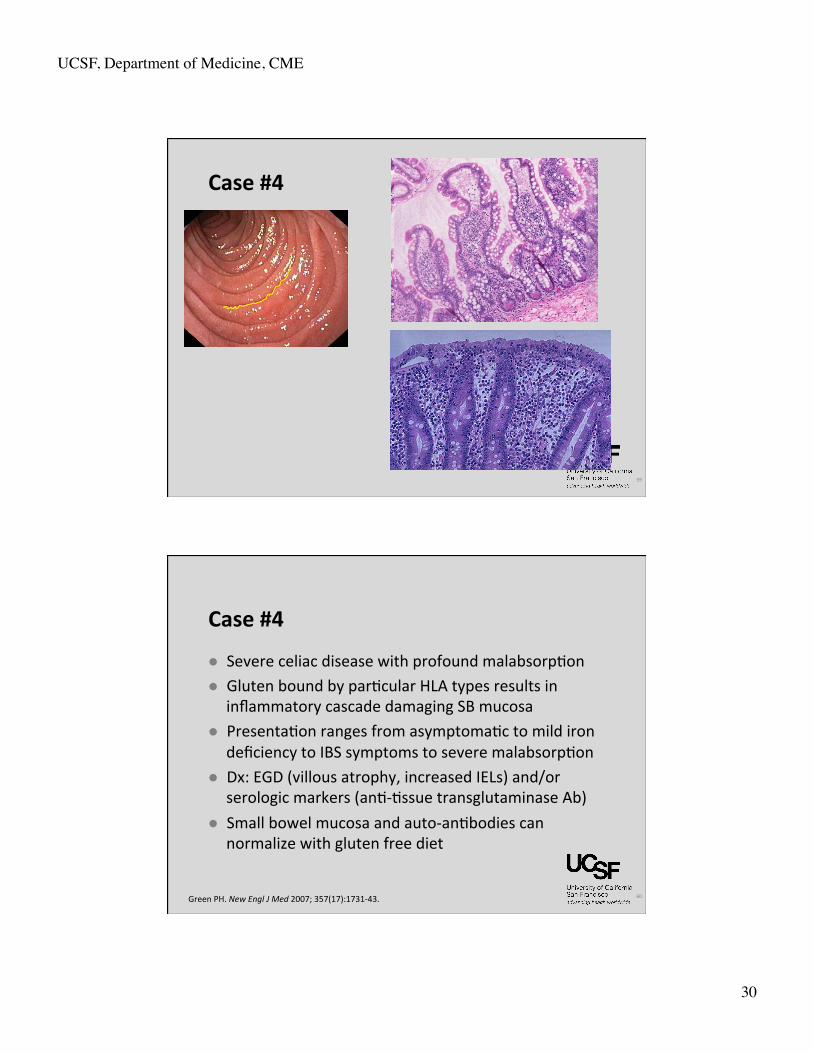
Case #4
l 22 y/o man c/o 1 year of worsening bloa&ng & gas l Frequent malodorous, floa&ng, greasy stools l 20 lb weight loss in 6 months l Denies abdominal pain, but has decreased food intake as it provokes diarrhea
l He also complains of an itchy rash on his knees and elbows

UCSF, Department of Medicine, CME
28
55
Case #4
l Pex: short stature, mucosal pallor, angular cheilosis, scaLered papules and vesicles with excoria&on over the knees and elbows, and mild pre&bial edema
l Lab tests are significant for microcy&c anemia and a low serum albumin
56
GI rashes you need to know…
Derma&&s Herpe&formis E. nodosum Pyoderma
UCSF, Department of Medicine, CME
29
57
Case #4 Which of the following is the most likely cause of this paEent’s syndrome and malnutriEon?
1. Whipple’s Disease
2. Crohn’s Disease
3. Celiac Disease
4. Pancrea&c exocrine insufficiency
5. Small bowel bacterial overgrowth
58
Case #4 Which of the following is the most likely cause of this paEent’s syndrome and malnutriEon?
1. Whipple’s Disease
2. Crohn’s Disease
3. Celiac Disease
4. Pancrea&c exocrine insufficiency
5. Small bowel bacterial overgrowth
UCSF, Department of Medicine, CME
30
Case #4
59
60
Case #4
l Severe celiac disease with profound malabsorp&on l Gluten bound by par&cular HLA types results in
inflammatory cascade damaging SB mucosa l Presenta&on ranges from asymptoma&c to mild iron
deficiency to IBS symptoms to severe malabsorp&on l Dx: EGD (villous atrophy, increased IELs) and/or
serologic markers (an&-‐&ssue transglutaminase Ab) l Small bowel mucosa and auto-‐an&bodies can
normalize with gluten free diet
Green PH. New Engl J Med 2007; 357(17):1731-‐43.

UCSF, Department of Medicine, CME
31
61
Case #4 l Tx : gluten-‐free diet l New agent = larazo&de (prevents &ght junc&on opening à decreased gluten uptake)
l Long-‐term complica&ons include elevated risk of SB CAs (AdenoCA, lymphoma) and osteoporosis
l Associa&on with other autoimmune diseases, such as RA and thyroid disease
l Whipple’s disease, bacterial overgrowth, Crohn’s disease & pancrea&c insufficiency can also cause malabsorp&on
Green PH. New Engl J Med 2007; 357(17):1731-‐43.
62
Case #5
l 48 year old man complains of watery diarrhea of 4 months’ dura&on
l He has 4-‐6 large volume watery movements daily
l He has required hospitaliza&on twice for dehydra&on
l On each admission, exam, labs, cultures unrevealing
UCSF, Department of Medicine, CME
32
63
Case #5 Which of the following studies would provide the strongest evidence for a secretory eEology for his diarrhea?
1. The presence of fecal leukocytes
2. A history of recent an&bio&c use
3. A history of lactose intolerance
4. High stool osmolar gap
5. A fas&ng fecal volume >2.5L / 24 hours
64
1. The presence of fecal leukocytes
2. A history of recent an&bio&c use
3. A history of lactose intolerance
4. High stool osmolar gap
5. A fas&ng fecal volume >2.5L / 24 hours
Case #5 Which of the following studies would provide the strongest evidence for a secretory eEology for his diarrhea?

UCSF, Department of Medicine, CME
33
65
Case #5
l Main diarrhea mechanisms are secretory, osmoEc / malabsorpEve, inflammatory, funcEonal
l Differen&ate on analysis of stool for fat and WBC, response to fas&ng, stool osmolar gap
l Osmolar gap
66
Case #5
l Secretory diarrhea is typically large volume (>1L/d) and does not diminish with fas&ng
l Causes of secretory diarrhea: l Bacterial and parasi&c infec&ons l Bile salt malabsorp&on from ileal resec&on l Medica&ons l Small intes&nal bacterial overgrowth (SIBO) l Hormone secre&ng tumors l Microscopic coli&s

UCSF, Department of Medicine, CME
34
67
Diarrhea
l Celiac disease can cause both secretory and osmo&c (malabsorp&ve) diarrhea
l Osmo&c diarrhea: lactose intolerance, magnesium intake
l Inflammatory diarrhea: usually due to bacterial coli&s or IBD
68
Steatorrhea
l Elevated fecal fat suggests maldiges&on or malabsorp&on
l FaLy diarrhea can be due to defec&ve: l Lipolysis (pancrea&c insufficiency) l Micellariza&on (bile salt insufficiency) l Absorp&on (intes&nal epithelium) l Delivery (lympha&cs)
+ à
UCSF, Department of Medicine, CME
35
69
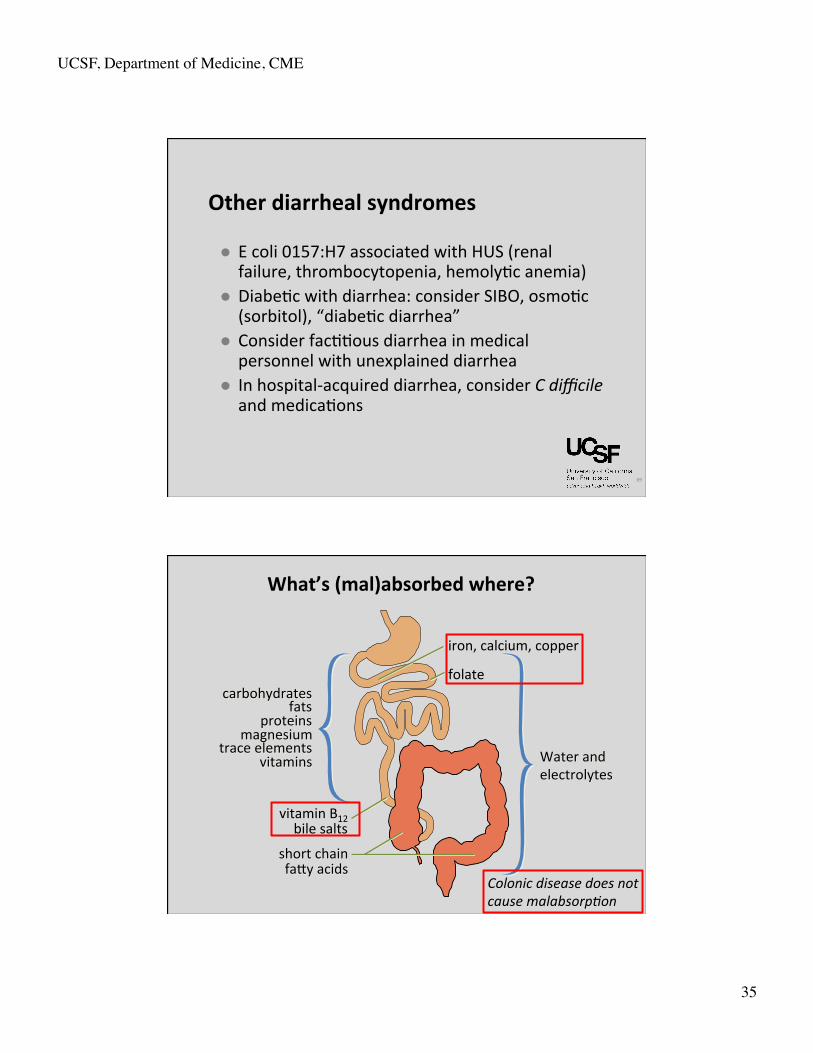
Other diarrheal syndromes
l E coli 0157:H7 associated with HUS (renal failure, thrombocytopenia, hemoly&c anemia)
l Diabe&c with diarrhea: consider SIBO, osmo&c (sorbitol), “diabe&c diarrhea”
l Consider fac&&ous diarrhea in medical personnel with unexplained diarrhea
l In hospital-‐acquired diarrhea, consider C difficile and medica&ons
carbohydrates fats
proteins magnesium
trace elements vitamins Water and
electrolytes
short chain faLy acids
iron, calcium, copper folate
vitamin B12 bile salts
Colonic disease does not cause malabsorp@on
What’s (mal)absorbed where?

UCSF, Department of Medicine, CME
36
71
C difficile
l Risk factors: hospitaliza&on, an&bio&cs, chemotherapy, immune suppression, PPIs
l Community acquired C. difficile increasingly common
l C. difficile spores are hardy and highly infec&ous l Have a high index of suspicion in the elderly, immunosuppressed, immunocompromised, and pa&ents with IBD
Case #6
l 87 y/o man with history of AFib, HTN, CAD, and DM presents to ER with 1 day of crampy leP lower quadrant abdominal pain and bloody stool
l PEx: BP 106/75, pulse 112, mild LLQ TTP, and maroon stool on rectal exam
l Hct 36%, WBC 12K l CT Abd shows leP colon wall thickening l The pa&ent is admiLed to the hospital and gentle fluid resuscita&on is ini&ated
UCSF, Department of Medicine, CME
37
73
Case #6 Which of the following is the most appropriate next step?
1. Visceral angiogram
2. Flexible sigmoidoscopy
3. Thromboly&c therapy
4. Renal dose dopamine
5. Stool for C difficile toxin
74
Case #6 Which of the following is the most appropriate next step?
1. Visceral angiogram
2. Flexible sigmoidoscopy
3. Thromboly&c therapy
4. Renal dose dopamine
5. Stool for C difficile toxin
UCSF, Department of Medicine, CME
38
75
76
Case #6
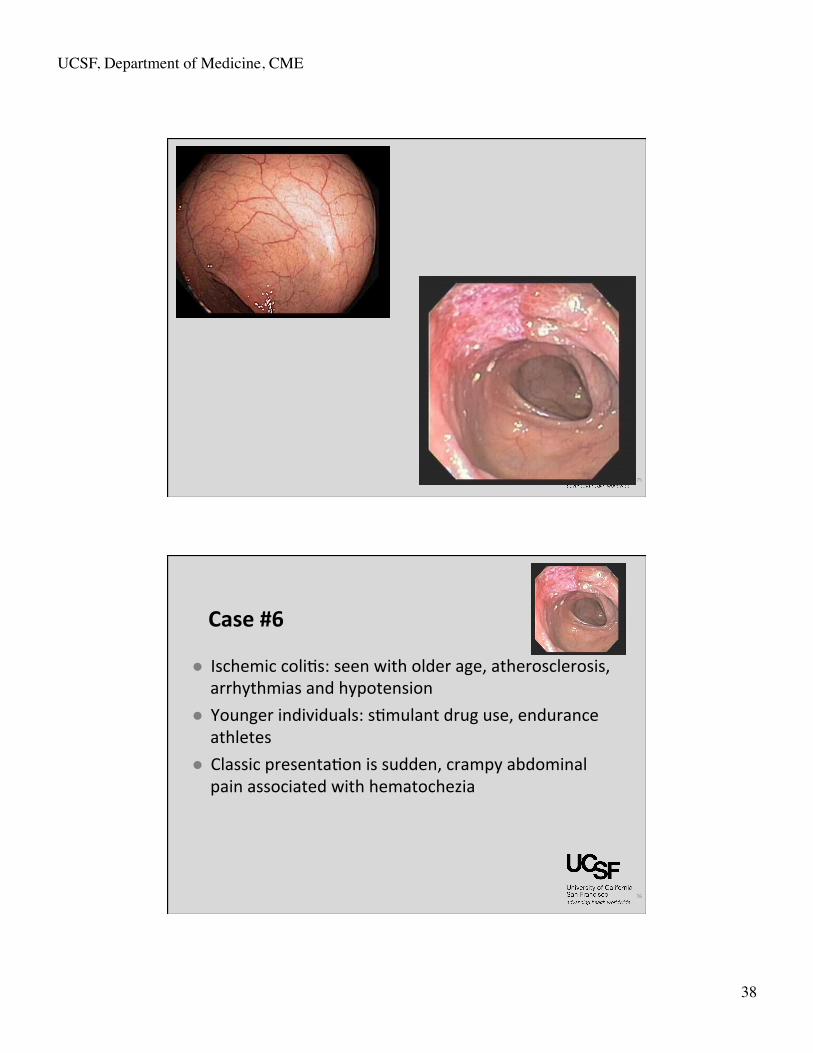
l Ischemic coli&s: seen with older age, atherosclerosis, arrhythmias and hypotension
l Younger individuals: s&mulant drug use, endurance athletes
l Classic presenta&on is sudden, crampy abdominal pain associated with hematochezia
UCSF, Department of Medicine, CME
39
77
Case #6
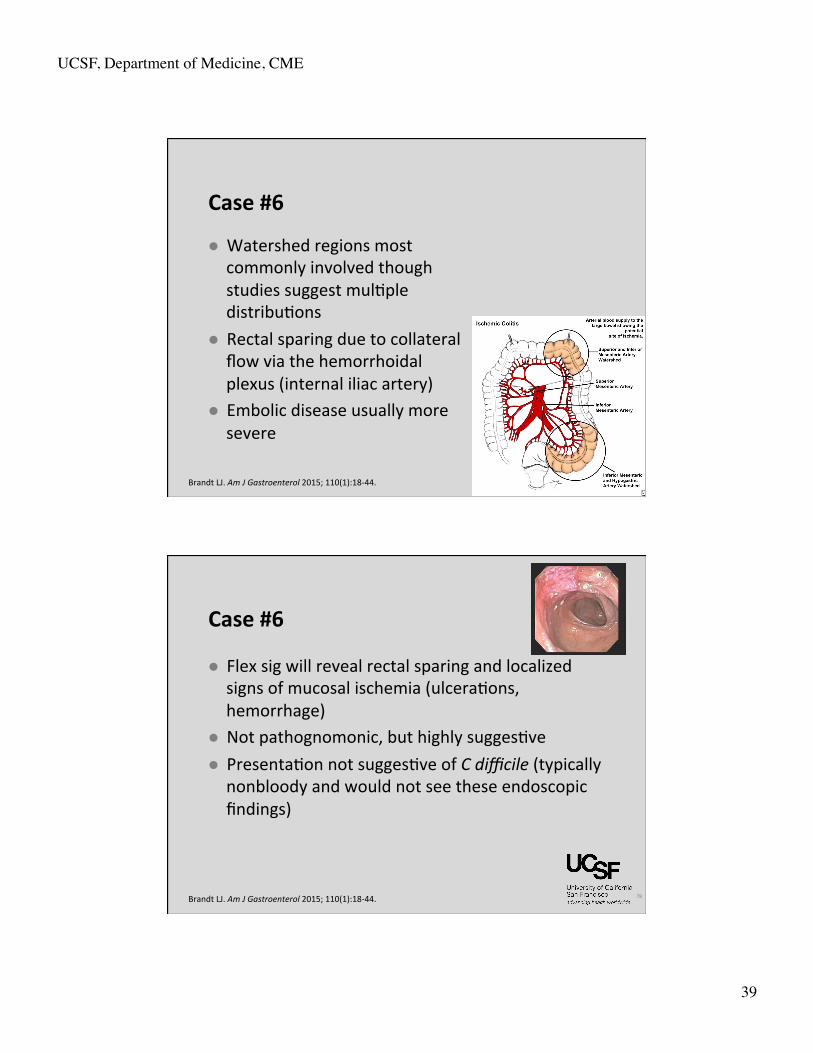
l Watershed regions most commonly involved though studies suggest mul&ple distribu&ons
l Rectal sparing due to collateral flow via the hemorrhoidal plexus (internal iliac artery)
l Embolic disease usually more severe
Brandt LJ. Am J Gastroenterol 2015; 110(1):18-‐44.
78
Case #6
l Flex sig will reveal rectal sparing and localized signs of mucosal ischemia (ulcera&ons, hemorrhage)
l Not pathognomonic, but highly sugges&ve l Presenta&on not sugges&ve of C difficile (typically nonbloody and would not see these endoscopic findings)
Brandt LJ. Am J Gastroenterol 2015; 110(1):18-‐44.

UCSF, Department of Medicine, CME
40
79
Case #6
l Suppor&ve management with goal of euvolemia, normotension
l Pressors may worsen visceral vasoconstric&on l Worsening abdominal exam with peritoneal signs, lac&c acidosis suggest toxic megacolon and/or perfora&on à requires urgent surgical evalua&on
l Prognosis is generally good l 80% resolve, 15% chronic ischemia, 5% fulminant
Brandt LJ. Am J Gastroenterol 2015; 110(1):18-‐44.
80
Vascular bowel disease
Ischemic coliEs Acute mesenteric ischemia
Chronic mesenteric ischemia
Bowel site Colon Small bowel Small bowel
Onset Acute Acute Chronic/recurrent
Typical pathophysiology
Hypoperfusion Embolism Thrombosis
Atherosclerosis
PresentaEon Acute cramping and hematochezia
Acute, severe pain “out of propor&on to examina&on”
Recurrent post-‐prandial pain “food fear”
Natural course 80% resolves 15% chronic 5% fulminant
Death if not rapidly treated
Gradual chronic worsening
Treatment Conserva&ve Emergent surgery Elec&ve surgical or endovascular therapy
UCSF, Department of Medicine, CME
41
ColiEs
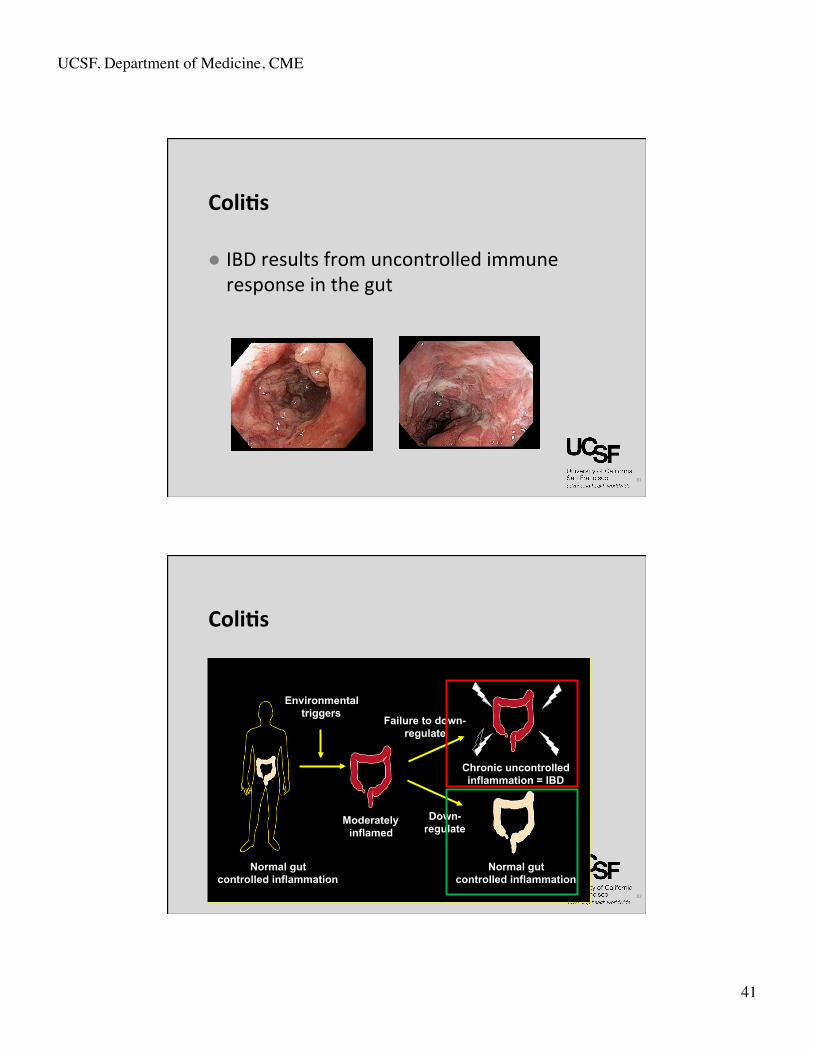
l IBD results from uncontrolled immune response in the gut
81
ColiEs
82
Environmental triggers
Moderately inflamed
Failure to down- regulate
Chronic uncontrolled inflammation = IBD
Down- regulate
Normal gut controlled inflammation
Normal gut controlled inflammation
UCSF, Department of Medicine, CME
42
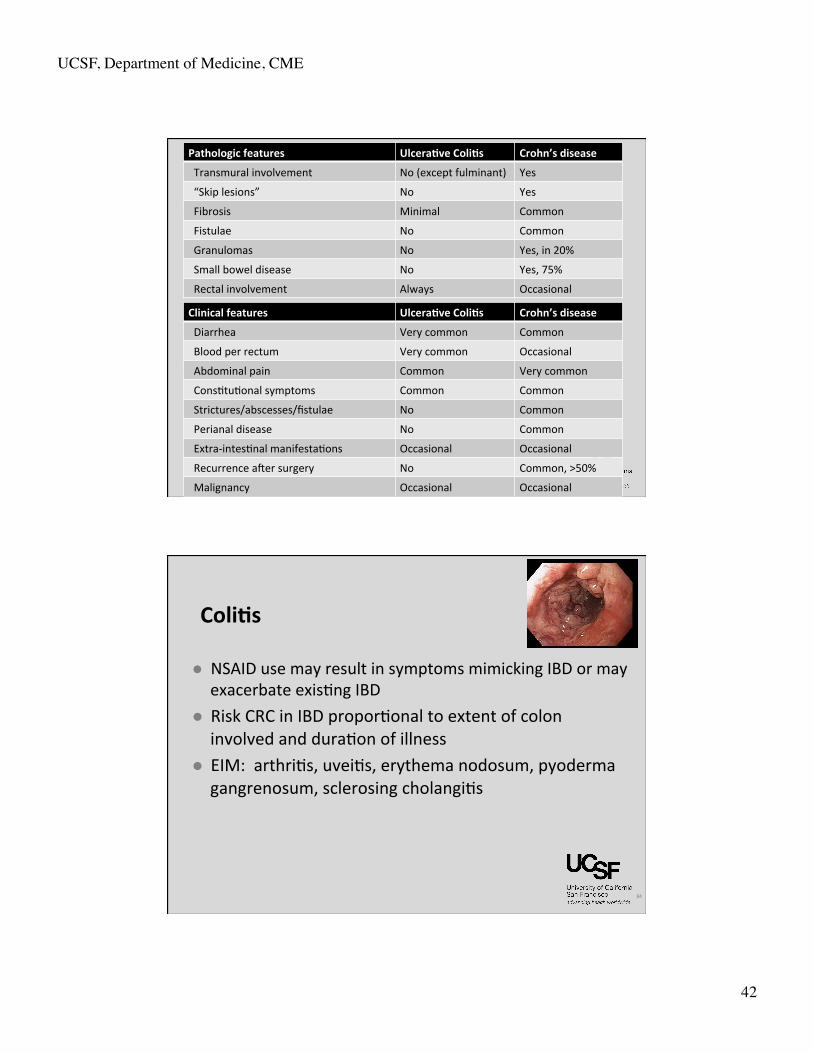
Pathologic features UlceraEve ColiEs Crohn’s disease
Transmural involvement No (except fulminant) Yes
“Skip lesions” No Yes
Fibrosis Minimal Common
Fistulae No Common
Granulomas No Yes, in 20%
Small bowel disease No Yes, 75%
Rectal involvement Always Occasional
Clinical features UlceraEve ColiEs Crohn’s disease
Diarrhea Very common Common
Blood per rectum Very common Occasional
Abdominal pain Common Very common
Cons&tu&onal symptoms Common Common
Strictures/abscesses/fistulae No Common
Perianal disease No Common
Extra-‐intes&nal manifesta&ons Occasional Occasional
Recurrence aPer surgery No Common, >50%
Malignancy Occasional Occasional
84
ColiEs
l NSAID use may result in symptoms mimicking IBD or may exacerbate exis&ng IBD
l Risk CRC in IBD propor&onal to extent of colon involved and dura&on of illness
l EIM: arthri&s, uvei&s, erythema nodosum, pyoderma gangrenosum, sclerosing cholangi&s
UCSF, Department of Medicine, CME
43
Medical therapy
5ASA
An&bio&cs
Steroids
Immuno-‐modulators
Biologics
Suppor&ve agents
Cancer screening in IBD
l Ulcera&ve coli&s proximal to the rectum or Crohn’s disease with significant colonic involvement
l Disease dura&on > 8 years l Colonoscopy q1-‐2 years with targeted biopsies plus random biopsies OR chromoendoscopy
86 Laine L. Gastrointest Endosc 2015; 81(3):489-‐501.
UCSF, Department of Medicine, CME
44
87
Lower GIB
l 10% w/ hematochezia have UGI source l >80% LGIB stops spontaneously, 25% recur l Diver&culosis most common cause l Tagged RBC scan (blood loss 0.1 cc/min, 6 cc/hr) l Angiography (blood loss 0.5 cc/min, 30 cc/hr) l Colonoscopy can be pursued but requires rapid prep
DiverEcular disease
l Common in elderly l No treatment indicated l Complica&ons: LGIB and diver&culi&s l Diagnosis of diver&culi&s warrants future colonoscopy to rule out cancer
l Consider surgery if recurrent diver&culi&s
88
UCSF, Department of Medicine, CME
45
89
Case 7
l A 62 y/o man has a posi&ve FOBT collected via digital rectal exam
l Takes a daily low-‐dose ASA for cardioprotec&on l Reports occasional BRB when he wipes with toilet paper for years, especially with straining
l No family history of colorectal cancer l No other GI symptoms
90
Case 7 Which of the following is the best approach at this Eme?
1. Repeat FOBT on spontaneously defecated stool
2. Colonoscopy
3. Flexible Sigmoidoscopy
4. Barium Enema
5. CT colonography
UCSF, Department of Medicine, CME
46
91
Case 7 Which of the following is the best approach at this Eme?
1. Repeat FOBT on spontaneously defecated stool
2. Colonoscopy
3. Flexible Sigmoidoscopy
4. Barium Enema
5. CT colonography
92

UCSF, Department of Medicine, CME
47
93
Case #7
l Could be false posi&ve FOBT due to DRE or hemorrhoids, but a posi&ve test always requires a complete colonoscopy
l No role for “confirmatory” retes&ng
94
Colorectal cancer screening
l Approved CRC screening methods: l Colonoscopy (q 10 years) l Flexible sigmoidoscopy (q 5 years) l CT colonography (q 5 years) l FOBT/FIT (annually) l BE has fallen out of favor (q 5 years)
l Any posi&ve exam à colonoscopy l CEA not used for screening l Fecal DNA not widely used
Levin B. Gastroenterology 2008; 134(5):1570-‐95.
UCSF, Department of Medicine, CME
48
95
Polyps & colorectal cancer
l Increased CRC risk l Personal or family history of polyps or cancer
l 10 years before age of affected family member or age 40, whichever is earlier
l IBD l APer 8-‐10 years of disease
l Subsequent colonoscopy intervals if average risk l 10 years if no polyps l 5 years is < 2 small adenomas l 3 years if >2 small, or any large (10mm+) adenomas
Lieberman DA. Gastroenterology 2012; 143(3):844-‐57.
96
Cancer syndromes
l Familial Adenomatous Polyposis: AD, 1/3 new muta&ons, cancer in 30s w/o colectomy
l Gardner's = FAP w/ extracolonic osteomas, desmoid tumors, congenital hypertrophy of the pigmented re&nal epithelium
l Both caused by same muta&on (APC), a tumor suppresser gene
l Main cause of death in FAP and Gardner’s pa&ents s/p colectomy is periampullary neoplasia; next are desmoid tumors
UCSF, Department of Medicine, CME
49
97
l Turcot's = FAP w/ CNS malignancies l Lynch Syndrome = Hereditary Non-‐Polyposis Colorectal Cancer (HNPCC). AD, incomplete penetrance, R-‐sided CRCs, beLer prognosis than FAP l Increased risk of ovarian, endometrial, breast, gastric,
ampullary CA l Caused by muta&ons in DNA mismatch-‐repair genes
Cancer syndromes
98
CASE #8
l 59 y/o Chinese woman recently immigrated to US with 4 months of progressive dyspepsia, described as a periumbilical gnawing or fullness
l 12 lb weight loss and early sa&ety l EGD reveals diffuse gastric atrophy and a 1.5cm ulcer in the fundus with exophy&c edges l Ulcer biopsies – granula&on &ssue l Gastric body biopsies – organisms consistent with H
pylori
UCSF, Department of Medicine, CME
50
99
CASE #8 Which of the following is the best approach at this Eme?
1. Treat for H pylori, then repeat EGD
2. Treat for H pylori, repeat EGD if symptoms persist
3. Treat for H pylori, check UGIS if symptoms persist
4. Treat for H pylori, no need to repeat EGD
5. PPI BID, no need to treat for H pylori if symptoms resolve
100
1. Treat for H pylori, then repeat EGD
2. Treat for H pylori, repeat EGD if symptoms persist
3. Treat for H pylori, check UGIS if symptoms persist
4. Treat for H pylori, no need to repeat EGD
5. PPI BID, no need to treat for H pylori if symptoms resolve
CASE #8 Which of the following is the best approach at this Eme?
UCSF, Department of Medicine, CME
51
101
102
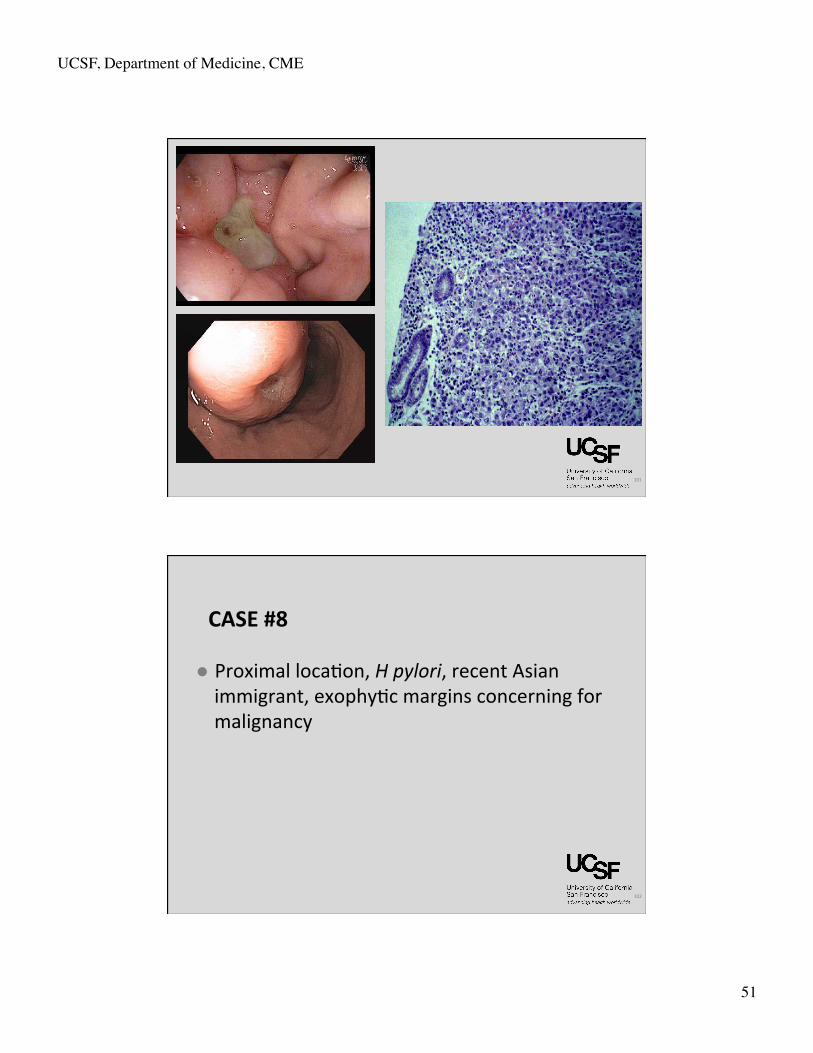
CASE #8
l Proximal loca&on, H pylori, recent Asian immigrant, exophy&c margins concerning for malignancy
UCSF, Department of Medicine, CME
52
103
CASE #8
l All gastric ulcers require repeat endoscopy aPer medical treatment to confirm healing and exclude neoplasia
l Pa&ent with mul&ple, small, antral ulcers, especially with known risk factors (such as NSAIDs) is the excep&on
l Repeat EGD not required for typical duodenal ulcers, as cancer risk is very low
ASGE Standards of Prac&ce CommiLee. Gastrointest Endosc 2010; 71(4): 663-‐8.
104
Gastric cancer
l Risk factors: H pylori, achlorhydria (par&al gastrectomy, atrophic gastri&s), intes&nal metaplasia, adenomatous gastric polyps, smoking, alcohol abuse
l Majority is adenocarcinoma l Gastric lymphoma is the most common site of extranodal lymphoma
l MALT lymphoma: related to H pylori, can oPen be cured with HP eradica&on alone
UCSF, Department of Medicine, CME
53
105
Esophageal cancer
l Esophageal adenocarcinoma risk factors: male gender, Caucasian, BarreL’s, smoking, obesity, alcohol abuse
l Squamous cell esophageal cancer risk factors: alcohol abuse, smoking, caus&c inges&on, achalasia, tylosis, dietary nitrates
l Stage with CT scan à endoscopic ultrasound if no mets on CT
106
l Very uncommon, but can include adenocarcinoma, carcinoid, GIST, lymphoma
l Risk factors: celiac disease, Crohn’s disease, familial polyposis, HIV (lymphoma)
Small bowel cancer
UCSF, Department of Medicine, CME
54
107
PancreaEc cancer
l Incidence increasing, now the 4th leading cause of cancer death in US (lung, colon, breast)
l Risk factors: smoking, alcohol abuse, chronic pancrea&&s
l Mainly adenocarcinoma, 70% in pancrea&c head l Systemic manifesta&ons of Panc CA: polyarthri&s, subcutaneous fat necrosis, migratory thrombophlebi&s
108
Other pancreaEc cancers
l IPMN, cystadenocarcinoma, neuroendocrine l Islet cell tumors:
l insulinomas → hypoglycemia l glucagonomas → hyperglycemia & rash (necroly&c migratory erythema)
l gastrinoma → pep&c ulcer disease, diarrhea l VIPoma → watery diarrhea, hypokalemia
UCSF, Department of Medicine, CME
55
PancreaEc cysts
l Serous cystadenoma (or carcinoma), mucinous cystadenoma (or carcinoma), IPMN, pseudocysts
l Common incidentalomas
109
PancreaEc cysts – new guidelines
l High risk features: >3 cm in size, solid component, dilated PD
l 0-‐1 high-‐risk feature: MRI in 1 year then q2 years x 2
l >1 high-‐risk feature: EUS with FNA l If EUS without concerning features à MRI l If lesion in tail, easier to resect surgically
110 Vege SS. Gastroenterology 2015; 148(4):819-‐22.
UCSF, Department of Medicine, CME
56
The End
111