5 important lessons learnt from australia important lessons learnt from australia disclosure...
TRANSCRIPT
Gerald Yong MBBS (Hons) FRACP FSCAI
Interventional Cardiologist
Royal Perth Hospital
Western Australia
4th APCASH – 7th September 2013
5 Important Lessons
Learnt From Australia
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial
Interest /arrangement or affiliation with the organization(s) listed below
Affiliation/Financial Relationship Company
Grant/ Research Support:
Consulting Fees/Honoraria: Edwards Lifesciences
(consultant & proctor)
Major Stock Shareholder/Equity Interest:
Royalty Income:
Ownership/Founder:
Salary:
Intellectual Property Rights:
Other Financial Benefit:

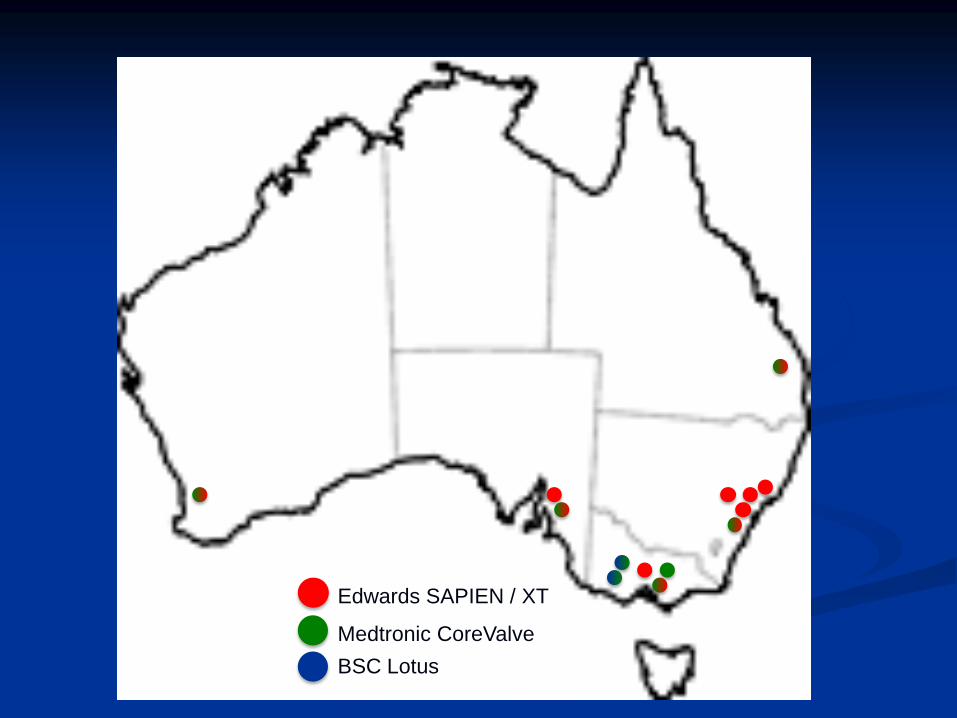
TAVR Program in Australia
Began in August 2008
Currently incorporates
Edwards SAPIEN / XT
Medtronic CoreValve
Boston-Scientific Lotus
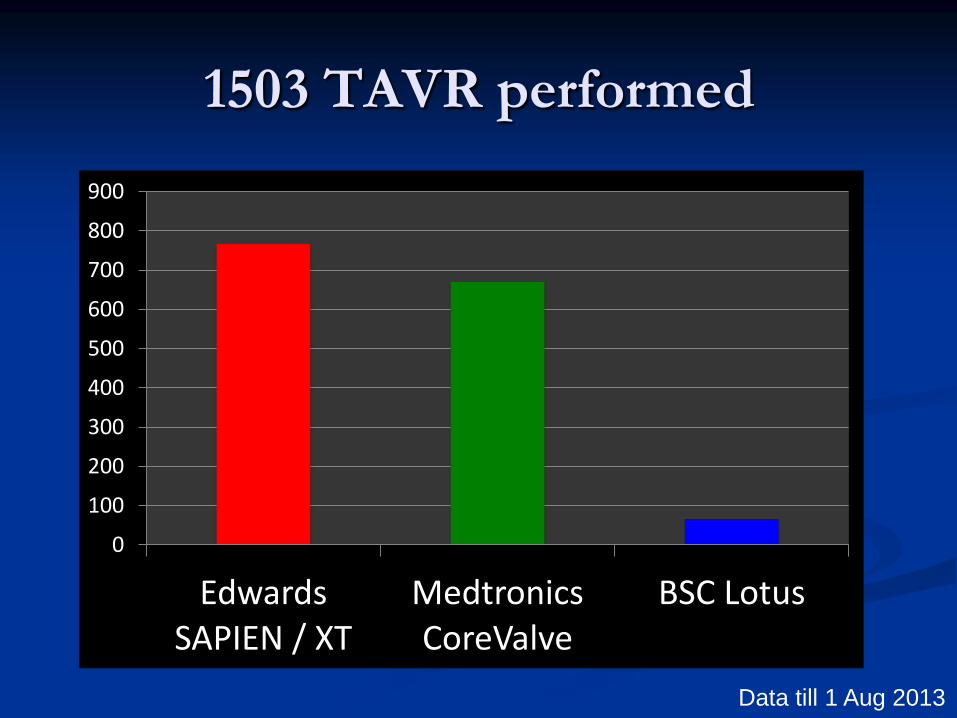
Edwards SAPIEN / XT
Medtronic CoreValve
BSC Lotus
0
100
200
300
400
500
600
700
800
900
Edwards SAPIEN / XT
Medtronics CoreValve
BSC Lotus
1503 TAVR performed
Data till 1 Aug 2013

Access Routes Used
81%
12%
5%
2%
Transfemoral
Transapical
Transaortic
Transubclavian
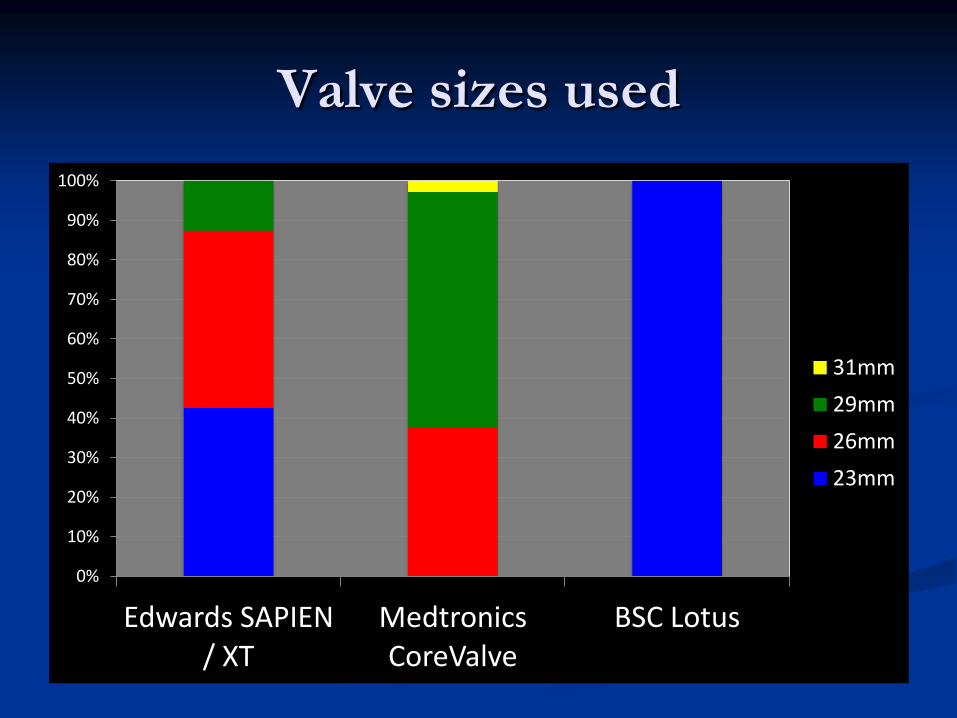
Valve sizes used
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Edwards SAPIEN / XT
Medtronics CoreValve
BSC Lotus
31mm
29mm
26mm
23mm

Clinical Trials
SOURCE-ANZ
- 2008-2010
SOLACE-AU
- 2012-current
ANZ CoreValve Trial
- 2008-current
REPRISE I
- 2011-12
REPRISE II
- 2012-13

SOURCE-
ANZ TF
(N=67)
SOURCE-
ANZ TA
(N=62)
ANZ
CoreValve
(Interim)
(N=441)
REPRISE I
(N=11)
Characteristics
Age (years) 83.7 81.7 83.9 83.0
Female (%) 34.3% 61.3% 44.9% 100%
Logistic EuroScore 26.8% 28.8% 17.3% 9.5%
Procedural Success 92.4% 87.1% 98.2% 100%
30-day Outcomes
Mortality 6.0% 9.6% 3.7% 0
Major stroke 3.0% 4.8% 3.5% 9.1%
Life threatening
bleeding
6.6% 18.2%
Major vascular
complication
4.5% 3.2% 4.1% 9.1%
Acute kidney injury 13.4% 17.7% 0
PPM 1.5% 8.1% 28.6% 36.3%
1 year Mortality 11% 18% 12% 0
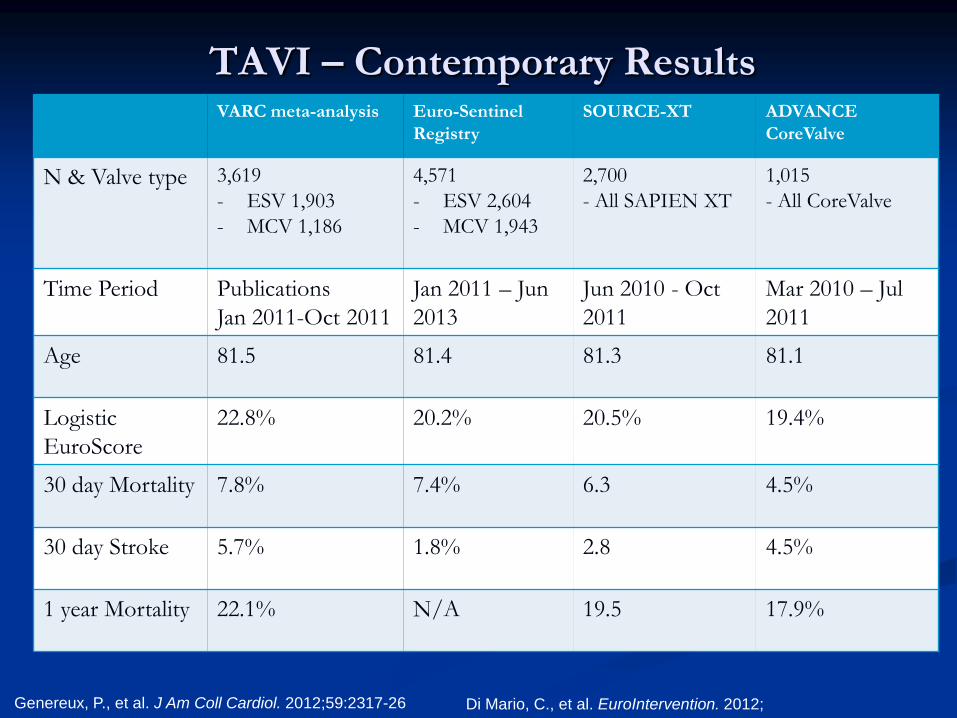
VARC meta-analysis Euro-Sentinel
Registry
SOURCE-XT ADVANCE
CoreValve
N & Valve type 3,619
- ESV 1,903
- MCV 1,186
4,571
- ESV 2,604
- MCV 1,943
2,700
- All SAPIEN XT
1,015
- All CoreValve
Time Period Publications
Jan 2011-Oct 2011
Jan 2011 – Jun
2013
Jun 2010 - Oct
2011
Mar 2010 – Jul
2011
Age 81.5 81.4 81.3 81.1
Logistic
EuroScore
22.8% 20.2% 20.5% 19.4%
30 day Mortality 7.8% 7.4% 6.3 4.5%
30 day Stroke 5.7% 1.8% 2.8 4.5%
1 year Mortality 22.1% N/A 19.5 17.9%
TAVI – Contemporary Results
Genereux, P., et al. J Am Coll Cardiol. 2012;59:2317-26 Di Mario, C., et al. EuroIntervention. 2012;

Edwards SAPIEN / XT
Medtronic CoreValve
BSC Lotus

WA FIRST TRANSFEMORAL TAVR
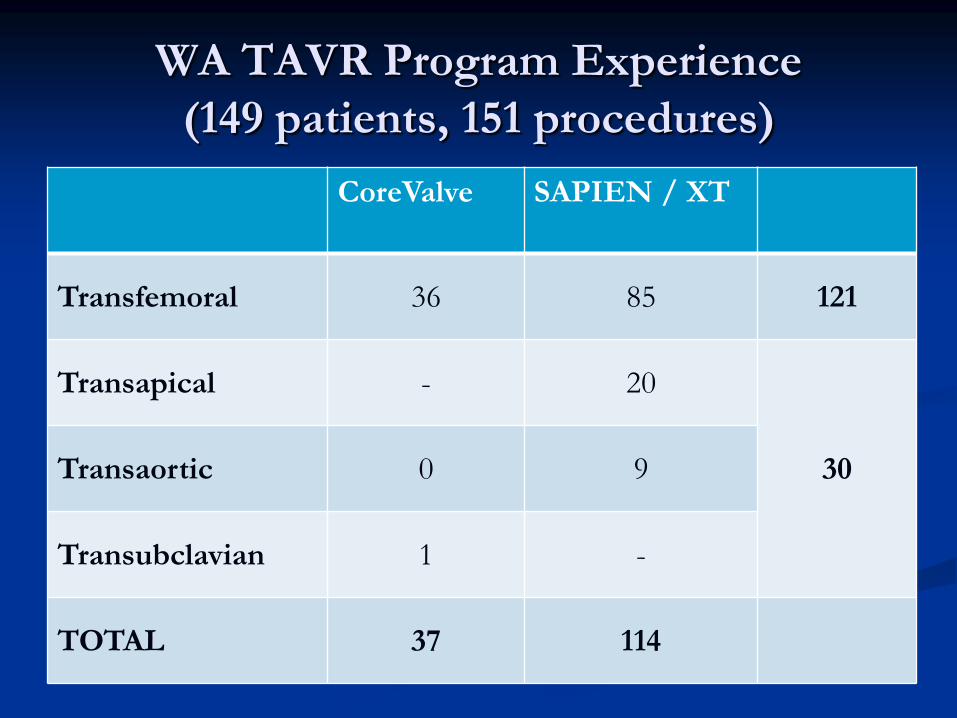
WA TAVR Program Experience
(149 patients, 151 procedures)
CoreValve SAPIEN / XT
Transfemoral 36 85 121
Transapical - 20
30 Transaortic 0 9
Transubclavian 1 -
TOTAL 37 114
WA TAVR Program
Procedural Success
Procedural success – 98.0%
3 failures
1x TF SAPIEN – failure to advance 24Fr sheath
1x TF SAPIEN XT – embolised valve converted to SAVR
1x TA SAPIEN – apical tear procedural death

TOTAL Transfemoral Hybrid
Characteristics
Age (years) 85.3 85.6 84.2
Female (%) 40.7% 40.8% 40.1%
Logistic EuroScore 23.8% 23.1% 27.1%
Procedural Success 98.0% 98.3% 96.7%
30-day Outcomes
Mortality 4.7% 2.0% 16.7%
Major stroke1 2.4% 2.0% 4.3%
Life threatening
bleeding1 8.8% 8.8% 8.7%
Major vascular
complication1 8.8% 8.8% 8.7%
Acute kidney injury1 8.0% 6.9% 13.0%
PPM1 17.6% 16.7% 17.7%
1 year Mortality1 14.8% 10.1% 35.8%
1 Based on patients to 2012 (N=125)

LESSONS LEARNT ON:
PATIENT SELECTION
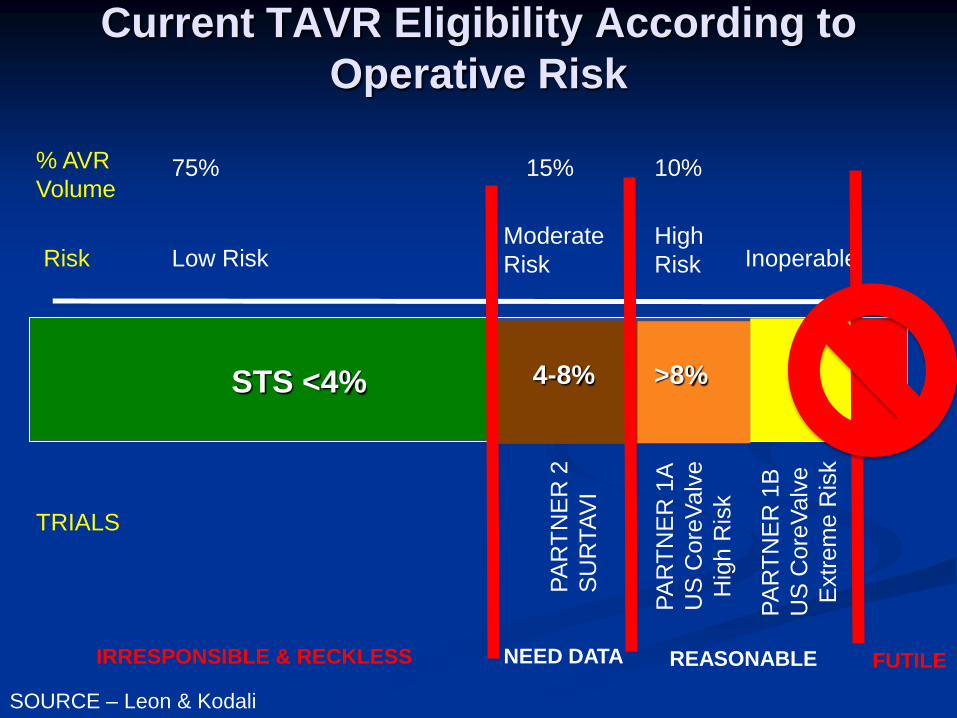
Current TAVR Eligibility According to
Operative Risk
STS <4%
>8%
4-8%
Inoperable Low Risk Moderate
Risk
High
Risk
PA
RT
NE
R 2
SU
RTA
VI
PA
RT
NE
R 1
A
US
Core
Valv
e
H
igh R
isk
PA
RT
NE
R 1
B
US
Core
Valv
e
E
xtr
em
e R
isk
75% 10% 15% % AVR
Volume
Risk
TRIALS
FUTILE REASONABLE NEED DATA IRRESPONSIBLE & RECKLESS
SOURCE – Leon & Kodali

Risk Scores
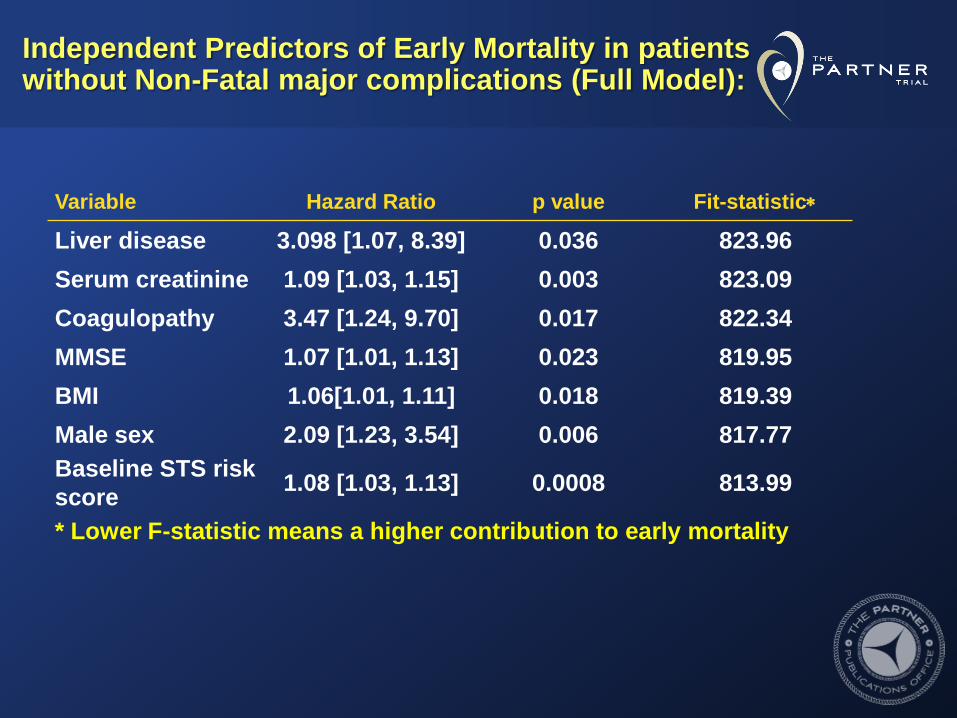
Independent Predictors of Early Mortality in patients without Non-Fatal major complications (Full Model):
Variable Hazard Ratio p value Fit-statistic
Liver disease 3.098 [1.07, 8.39] 0.036 823.96
Serum creatinine 1.09 [1.03, 1.15] 0.003 823.09
Coagulopathy 3.47 [1.24, 9.70] 0.017 822.34
MMSE 1.07 [1.01, 1.13] 0.023 819.95
BMI 1.06[1.01, 1.11] 0.018 819.39
Male sex 2.09 [1.23, 3.54] 0.006 817.77
Baseline STS risk
score 1.08 [1.03, 1.13] 0.0008 813.99
* Lower F-statistic means a higher contribution to early mortality
Frailty
Syndrome of multisystem impairment
associated with aging that results in
decreased physiologic reserve and
increased vulnerability to stressors.
Fried J Gerontol A Biol Sci Med Sci. 2001 Mar;56(3)

Frailty Domain Measure Frailty Score
Slowness
15 foot walk gait speed (m/s) Quartiles (0-3)
Weakness Grip strength (kg) Gender based quartiles
(0-3)
Wasting and
malnutrition
Serum albumin (g/dl) Quartiles (0-3)
Inactivity Katz ADLs (dress, bath, transfer,
feed, toilet, continence)
Any dependence=3,
Independence=0
Mental Faculty MMSE
Frailty Components
Kappetein, A. P., et al. J Am Coll Cardiol. 2012;60:1438-54 Stortecky, S., et al. JACC Cardiovasc Interv. 2012;5:489-96

Frailty predicts long term outcome
Stortecky, S., et al. JACC Cardiovasc Interv. 2012;5:489-96
Review of symptoms & indication for intervention
History and comorbidities
Objective functional assessment
Katz ADL assessment
Lowton & Brody instrumented ADL assessment
Canadian Study of Health and Aging Frailty assessment
Mini Mental State Examination
Formal assessment by geriatrics physician in bordeline
cases (ADL<6/6, iADL<6/8, MMSE<26/30)
Expectations – patient and family
Assess patient wish for intervention
Complete Global Clinical Assessment

2009-10 2011 2012
Age (years) 84.5 85.5 85.8
Logistic EuroScore 23.8% 23.0% 21.7%
30-day Mortality 5.6% 7.7%% 5.7%
Length of Stay 9.0 6.7 5.4
The IDEAL TAVR Patient
Elderly
High surgical risk
BUT…
LESSONS LEARNT IN:
VALVE SIZING


Predictors of Paravalvular Regurgitation
Severe calcification – Agaston calcium score on CT
Low implantation depth
Markers of valve undersizing
Small cover index
Large annulus
“Prosthesis / annulus mismatch”
Athappan, G., et al. J Am Coll Cardiol. 2013;61:1585-95

Traditional Imaging for Annulus Sizing
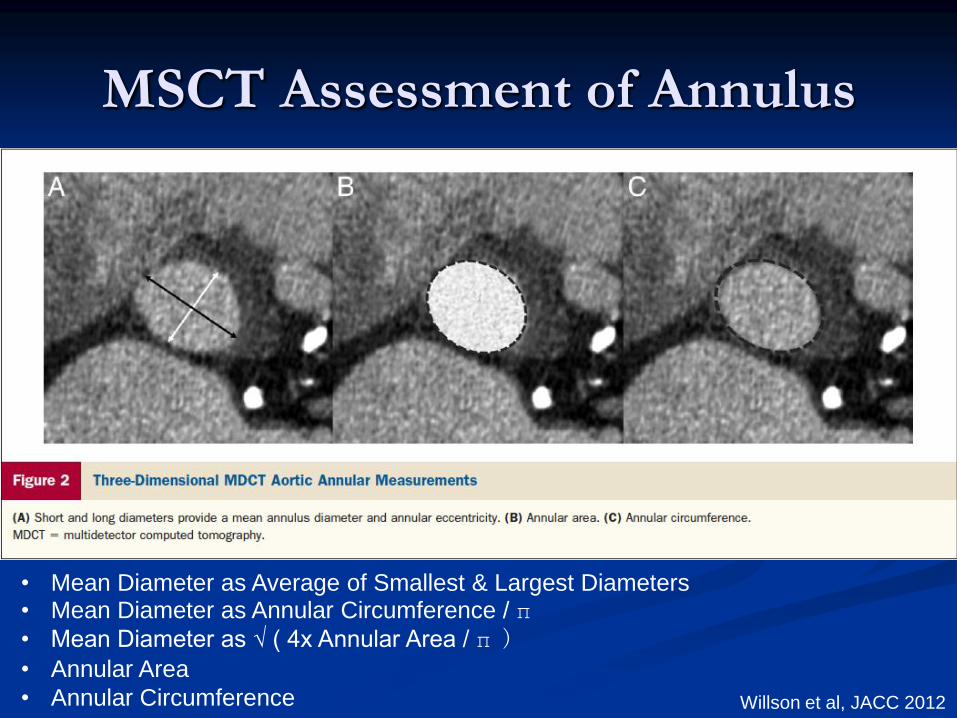
MSCT Assessment of Annulus
• Mean Diameter as Average of Smallest & Largest Diameters • Mean Diameter as Annular Circumference / π • Mean Diameter as √ ( 4x Annular Area / π )
• Annular Area
• Annular Circumference
Willson et al, JACC 2012
Multimodality Imaging with 3D TEE or MSCT
important in sizing
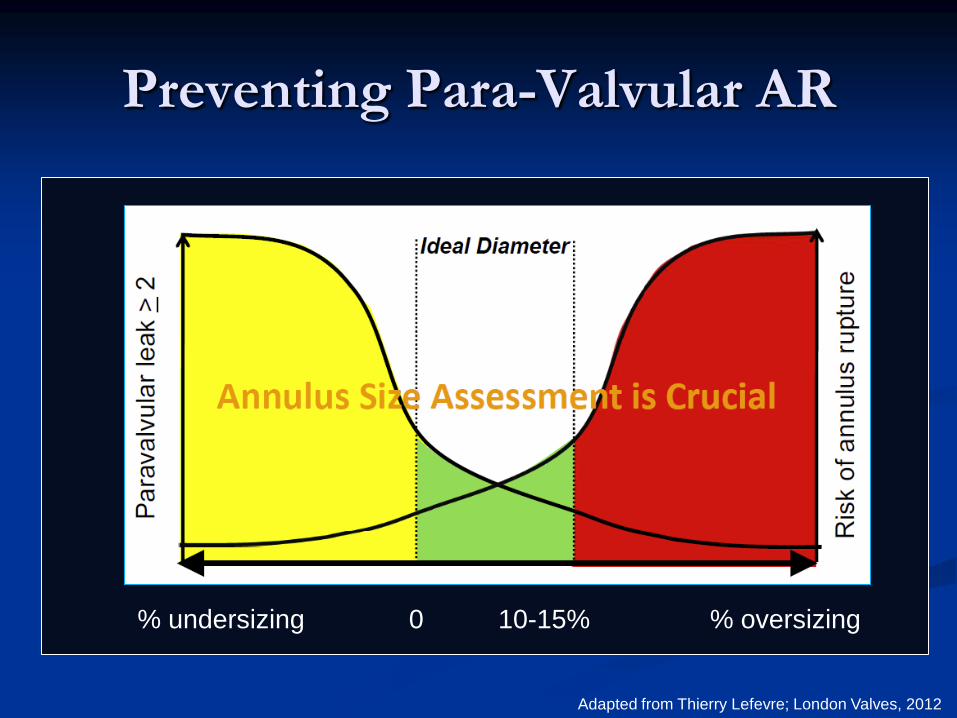
Preventing Para-Valvular AR
% oversizing % undersizing 10-15% 0
Adapted from Thierry Lefevre; London Valves, 2012
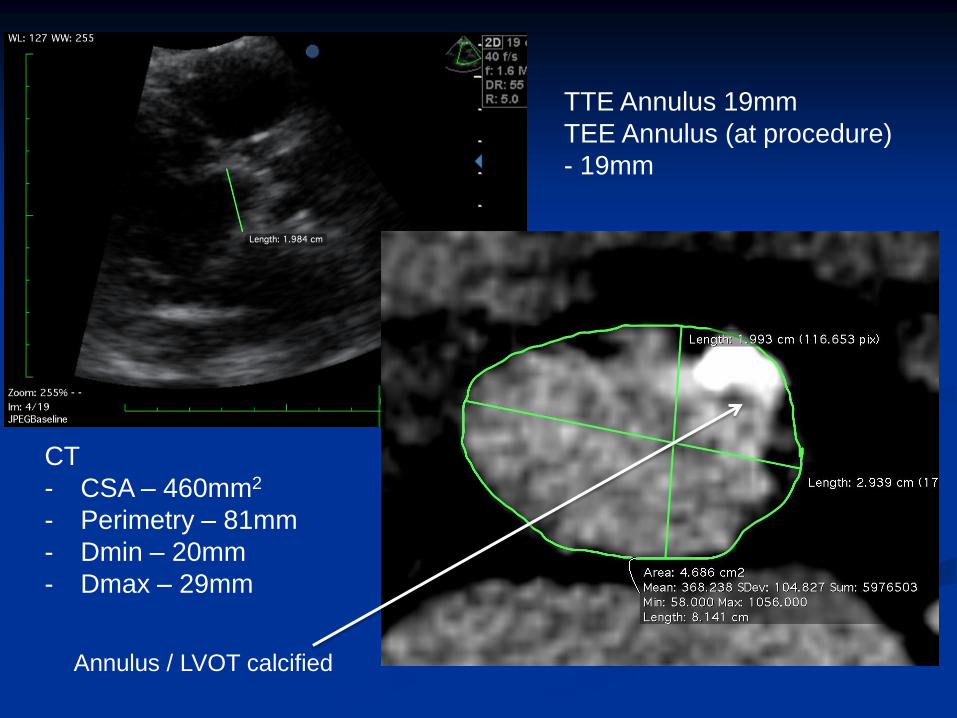
TTE Annulus 19mm
TEE Annulus (at procedure)
- 19mm
CT
- CSA – 460mm2
- Perimetry – 81mm
- Dmin – 20mm
- Dmax – 29mm
Annulus / LVOT calcified
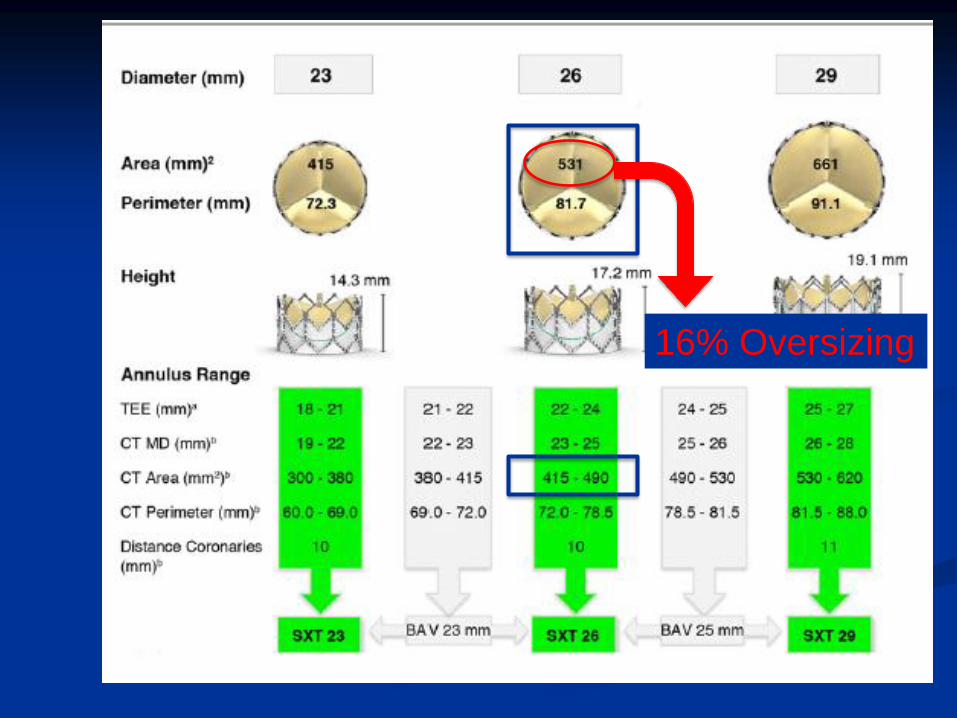
16% Oversizing
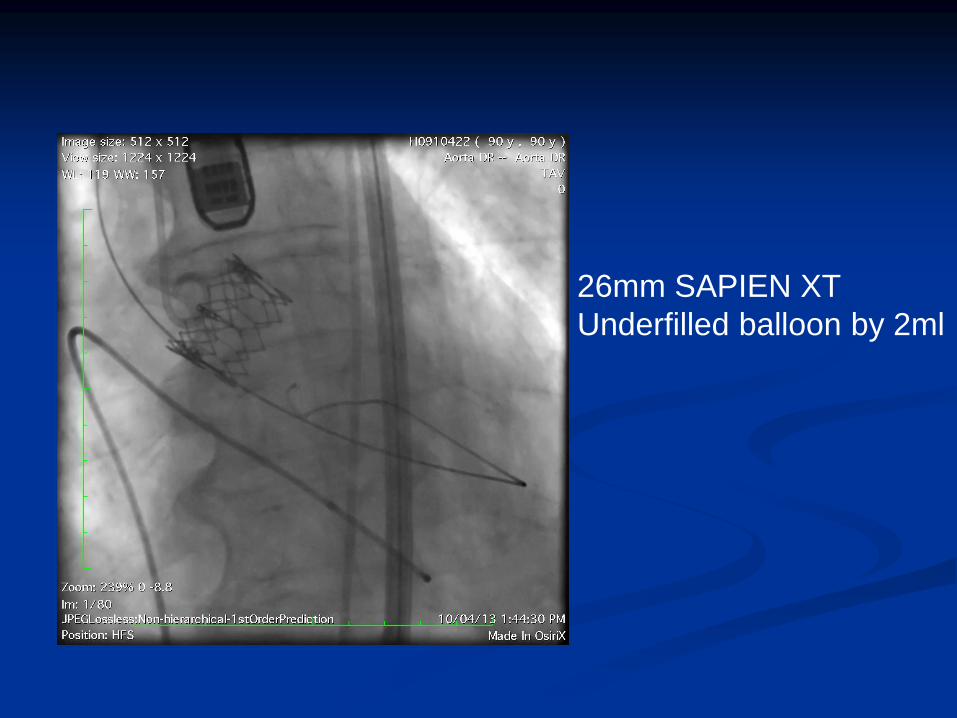
26mm SAPIEN XT
Underfilled balloon by 2ml

Post-dilate – fully-filled
deployment balloon

Final Result

LESSONS LEARNT IN:
COMPLICATIONS

Be Prepared for All Emergencies
Pre-defined & discussed protocol....
What to do when BP falls
What to do if peripheral
perforation
What to do if pre-closure fail
What to do if coronary occlusion
What to do if severe AR from
valve malposition
Bail out equipment list... And
know where to find them...
Etc...
Hypotension
Consider circumstances
At sheath insertion / removal
Peripheral perforation
Early angiography
After stiff wire passage to LV
Severe MR; Tamponade
Echo
Post-BAV
Severe AR; Tamponade
Echo, Aortogram
Post-THV deployment
Severe AR (valvular / paravalvular); Coronary occlusion; Tamponade
Echo & Aortogram, then coronary angiogram
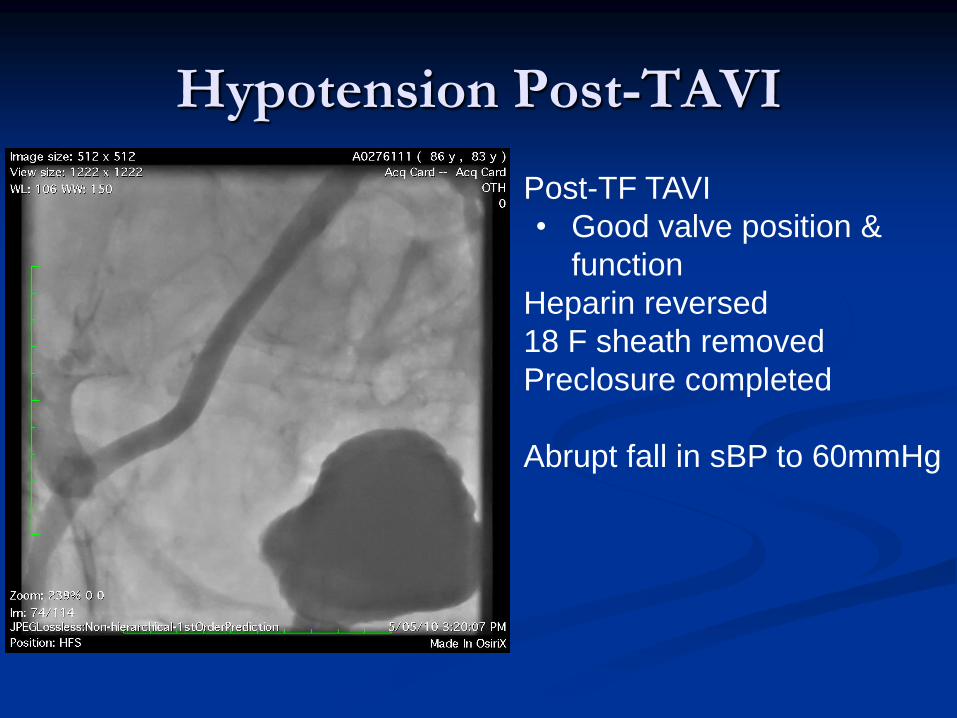
Hypotension Post-TAVI
• Post-TF TAVI
• Good valve position &
function
• Heparin reversed
• 18 F sheath removed
• Preclosure completed
• Abrupt fall in sBP to 60mmHg
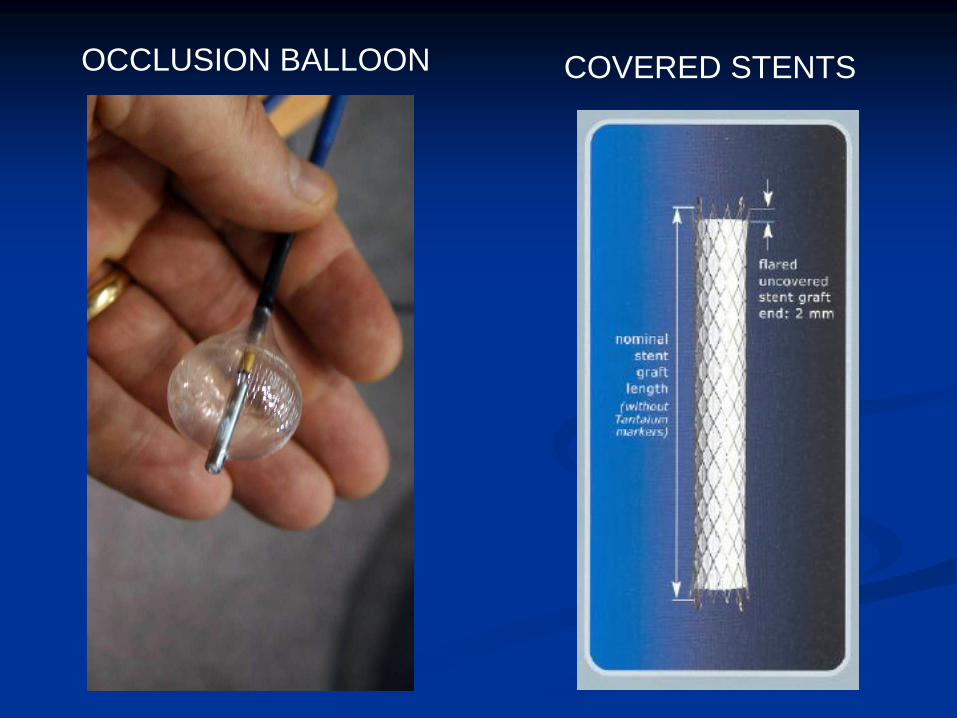
OCCLUSION BALLOON COVERED STENTS
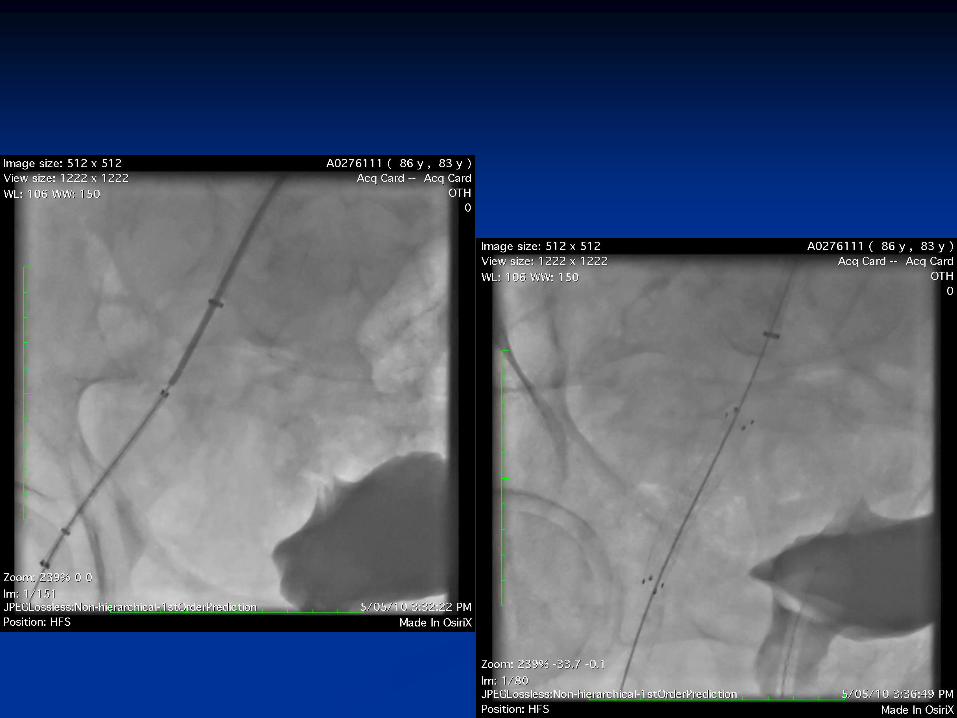

Hypotension post-TAVI
• Post-TF TAVI
• Heparin reversed with
protamine
• 18Fr Sheath removed
successfully & hemostasis
confirmed
10 minutes post sheath removal
• Severe hypotension
• CVP


LESSONS LEARNT IN
TEAM WORK

Interventional cardiology Cardiac surgery
Cardiac Imaging
Cardiac Anesthetist Vascular Surgery
Cardiac cathlab
Hybrid OR
Wards – ICU / CCU /
Cadiac / CTS ward
TAVR Program
Geriartrician Nephrologist
Intensivist
Program Co-ordinator
Need for Multi-Disciplinary Team Involvement
Conclusions
Well-established TAVR programs in Australia since 2008
Despite no formal regulatory approval for use of TAVR
Results are comparable to contemporary international
outcomes
30-day mortality 4-8%
30-day stroke
Patient selection important contributor to outcomes
Risk profile bordering on intermediate risk
My personal lessons learnt in running
WA TAVR Program
Patient selection important
Co-morbidities
Frailty
Paravalvular regurgitation is an important limitation of TAVR
Proper device sizing is important step to reducing incidence
Meticulous attention to procedural details is important,
especially well developed plan to treat complications
Multidisciplinary team-work in patient selection and
management of this group of high risk patients with low
reserve is extremely important

THANK YOU… POST TAVR #100
18TH APRIL 2012