4th cranial nerve
TRANSCRIPT
ANATOMY & CLINICAL SIGNIFICANCE OF 4TH
CRANIAL NERVE
Dr.Ashok Kumar Valuroutu

Free Template from www.brainybetty.com 2
TROCHLEAR NERVE
Free Template from www.brainybetty.com 3
FUNCTIONAL COMPONENTS
• SOMATIC EFFERENT-concerned with movement of eye ball through SO.
• GENERAL SOMATIC AFFERENT-carries proprioceptive impulses from SO which are relayed in the mesencephalic nucleus of 5 th nerve.

Free Template from www.brainybetty.com 4
COURSE AND DISTRIBUTION
1)Fascicular part
2)Pre cavernous part
3)Intra cavernous part
4)Intra orbital part

Free Template from www.brainybetty.com 5
• SITUATION: at the level of inferior colliculus in the ventromedial part of central gray metter of midbrain dorsal to medial longitudinal bundle.
• Caudal & continous with 3rd nucleus complex.

Free Template from www.brainybetty.com 6

Free Template from www.brainybetty.com 7

Free Template from www.brainybetty.com 8
FASCICULAR PART:
• axons leave the nucleus
• curve posteriorly around the aquiduct in the central greymatter
• decussate in the anterior medullary velum.
Free Template from www.brainybetty.com 9

Free Template from www.brainybetty.com 10
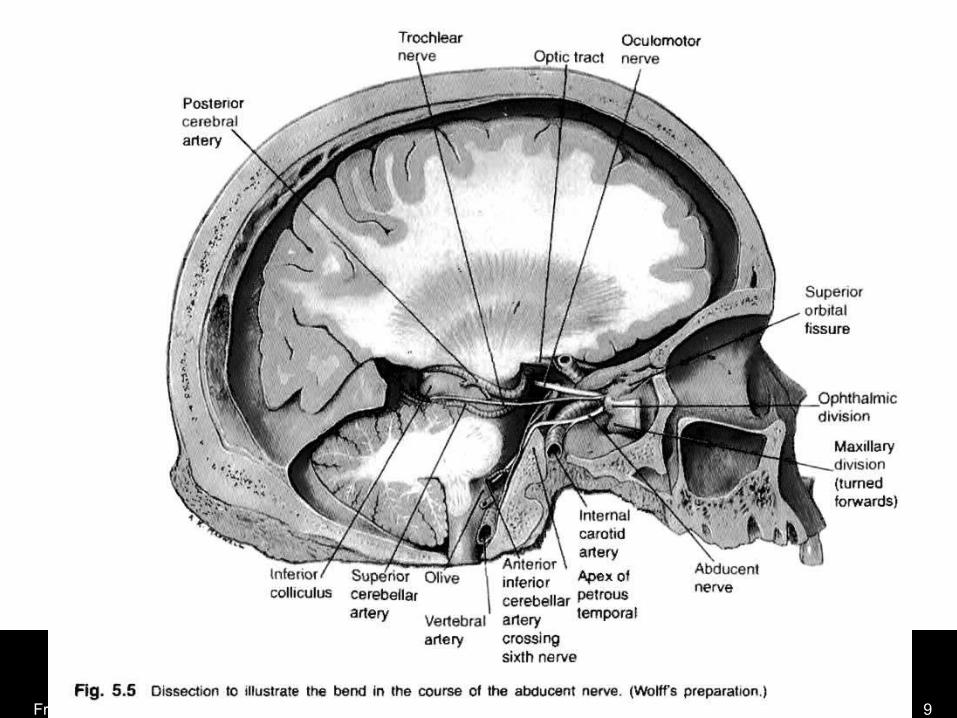
PRECAVERNOUS PART: leaves the brainstem on the dorsal surface
just caudal to inferior colliculus winds around brainstem runs forwards beneath the free edge of
tentorium pierces the dura on the posterior corner of
the roof of cavernous sinus to enter in to it.

Free Template from www.brainybetty.com 11
INTRACAVERNOUS PART:
Runs forwards in the lateral wall of the sinus,lying below 3rd nerve and above the 1st division of 5th nerve.
In the anterior part of the sinus, it rises,
crosses over the 3rd nerve
passes through the superior orbital fissure, above and lateral to annulus of zinn.

Free Template from www.brainybetty.com 12

Free Template from www.brainybetty.com 13
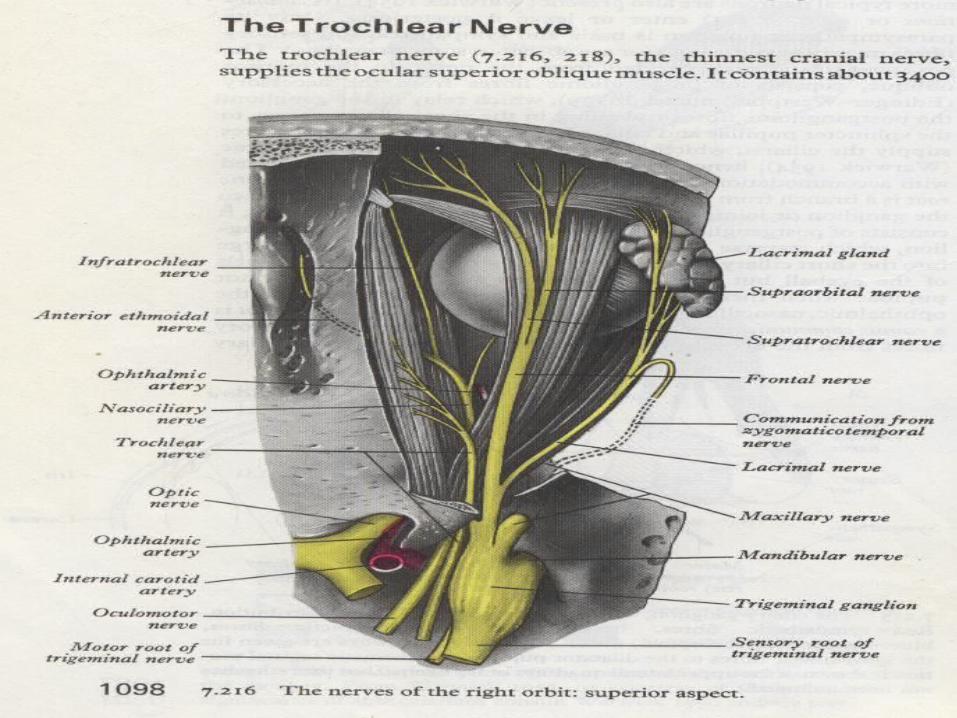
INTRA ORBITITAL PART:
• Enters the orbit through lateral part of SOF
• Frontal & lacrimal nerves laterally, ophthalmic vein inferiorly.
• Divides in to fan shaped manner into 3 or 4 branches
• Ends by supplying SO on its orbital surface near lateral border.

Free Template from www.brainybetty.com 14

Free Template from www.brainybetty.com 15
Free Template from www.brainybetty.com 16

Free Template from www.brainybetty.com 17
CONNECTIONS:
1)Cerebral cortex
Motor cortex - cortico nuclear tracts
Visual cortex - supeior colliculus & tactobulbar Frontal eye field. tracts.
2)Nuclei of 3rd ,6th&8th -MLF
3)Superior colliculi -descending predorsal bundle
4)Vertical & torsional gaze centres
5)Cerebellum - vestibular nuclei.
Free Template from www.brainybetty.com 18
UNIQUE CHARACTERS
• Only cranial nerve to emerge from dorsal aspect of brain.
• Only crossed cranial nerve
• Longest Intra cranial course(about 75 mm)& thinnest of all cranial nerves

Free Template from www.brainybetty.com 19
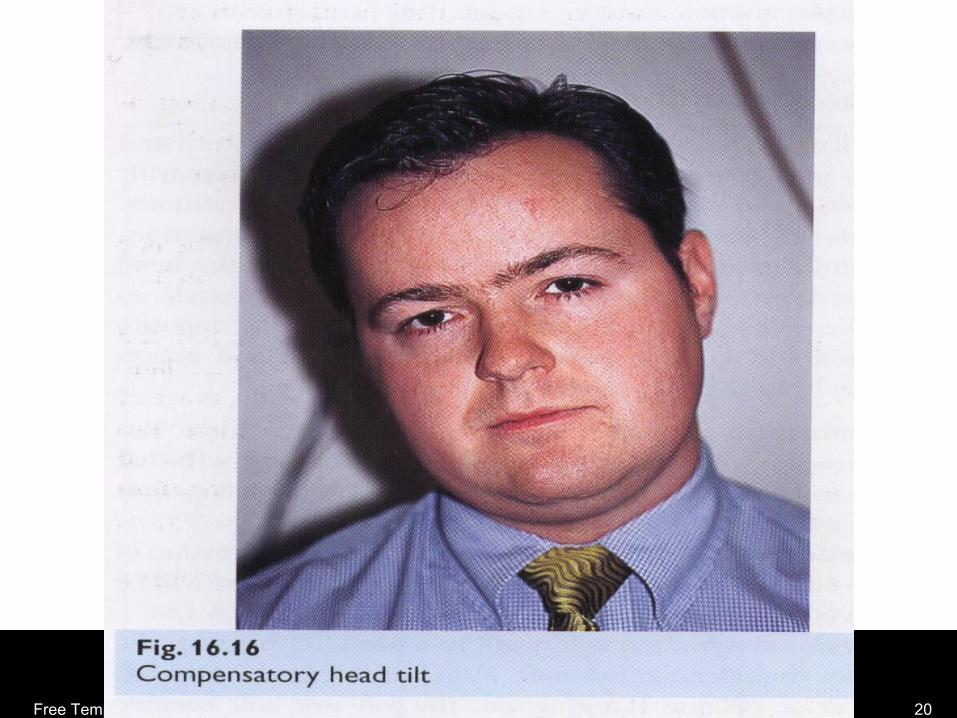
CLINICAL FEATURESSYMPTOMS:• Ac.onset of double vision,• Difficulty in going downstairs,• VertigoSIGNS: • Hyperdeviation ,limitation of depression in adduction,• Extorsion, vertical diplopia,• Hypertropia on opposite gaze• Charecteristic head posture- head tilted to opposite side face turned towards opposite side chin depressed
Free Template from www.brainybetty.com 20

Free Template from www.brainybetty.com 21
SPECIAL TESTS
Free Template from www.brainybetty.com 22
PARK’S 3 STEP TEST:
STEP 1: Identify the HYPERTROPIC EYE in primary position.
depressors of hypertropic eye- SO,IR.
elevators of hypotropic eye-SR,IO.
STEP 2: Determine whether hypertropia is greater in Rt or Lt gaze.
on Lt gaze Lt SR, Rt.SO
on Rt gaze Rt IR, Lt IO
Free Template from www.brainybetty.com 23
STEP 3: Tilt the head towards each shoulder, look for vertical sqint.
BEILSCHOWSKY HEAD TILT TEST: same principle as the 3rd step of PARK TEST Pt fixates, head tilted Rt &Lt of Lt hypertropia on Lt head tilt- Lt SO of Lt hypertropia on Rt head tilt- Lt IR

Free Template from www.brainybetty.com 24

Free Template from www.brainybetty.com 25
DOUBLE MADDOX ROD TEST :
For measuring the degree of cyclodeviation.
In unilateral palsy – cyclodeviation <10 deg
In bilateral palsy – cyclodeviation >10 deg

Free Template from www.brainybetty.com 26

Free Template from www.brainybetty.com 27
Differential Diagnosis of Vertical Binocular Diplopia• Superior Oblique Palsy• Thyroid Ophthalmopathy• Myasthenia Gravis• Brown Syndrome• Orbital fracture with entrapment• Cyclovertical paresis or overaction• Skew Deviation/Ocular Tilt• Dissociated Vertical Deviation
Free Template from www.brainybetty.com 28
Isolated Superior Oblique Palsy
• Most common etiologies are congenital and traumatic
• Also vascular; less commonly tumor, demyelinating
• In absence of other neurological symptoms and presence of vascular risk factors, reasonable to observe
Free Template from www.brainybetty.com 29
TREATMENT• CONGENITAL:large hypertropia in PP treated by
SO tucking• ACQUIRED:
SMALL- ipsilateral IO weakening.
MODERATE- ipsilateral IO weakening with ipsilateral SR weakening .
PURE EXCYCLOTROPIA: without hypertropia –HARADA- Ito procedure
Splitting & ALT OF lateral half of SO tendon.
