38-articles-randomized clinical trial of treatments for...
TRANSCRIPT

RanSym
Conv
Arch
ABST
Objecompofficeand ofor sy
Methsymp
Main12 wposit
ResuInsufthoserespeimprocompimproOBVA
Concimpropositprede
Applan ef
Trial
INTR
ndomizemptomat
vergence Ins
Ophthalmo
TRACT
ective To cputer vergene-based vergoffice-basedymptomatic
hods In a rptomatic con
n Outcome eeks of treaive fusional
ults After 1fficiency Syme of 21.3, 24ectively (P <oved near ppared with toved outcomAT, HBPP, H
clusions Twovement in ive fusional etermined c
lication to ffective trea
l Registrati
RODUCTIO
ed Clinictic Conv
sufficiency T
l. 2008;126
ompare homnce/accommgence/accom
d placebo thc convergenc
randomized nvergence in
Measures atment. Secvergence a
12 weeks of mptom Surv4.7, and 21.
< .001). Thepoint of convthe other grome was founHBCVAT+, an
welve weekssymptoms vergence a
criteria of su
Clinical Pratment for c
ion clinicalt
N
al Trial vergence
Treatment T
6(10):1336-
me-based pemodative themmodative erapy with hce insufficie
clinical trialnsufficiency
Convergencondary outct near.
treatment, vey score (1.9 in the HBe OBVAT grovergence anoups (P .0nd in 73%, 4nd OBPT gro
s of OBVAT and clinical
and a greateccess comp
actice Offichildren with
trials.gov Id
of Treate Insuff
Trial Study G
1349.
encil push-uerapy and ptherapy withome reinfoncy.
l, 221 childry were assig
nce Insufficiecomes were
the OBVAT15.1) was stBCVAT+, HBoup also demnd positive fu005 for all c43%, 33%, oups, respec
results in ameasures o
er percentagpared with H
ce-based ve symptomat
dentifier: NC
tments fficiency
Group*
ups (HBPP),pencil push-uth home reinorcement (O
ren aged 9 tned to 1 of
ency Symptnear point
group's metatistically sBPP, and OBmonstrated usional verg
comparisonsand 35% octively.
a significantlof near pointge of patientHBPP, HBCVA
ergence accotic converge
CT00338611
Jum • Top
for in Child
home-baseups (HBCVAnforcement OBPT) as tre
to 17 years 4 treatmen
tom Survey of converge
ean Convergignificantly PT groups, a significan
gence at neas). A succesof patients in
ly greater t of convergts reaching AT+, and O
ommodativeence insuffic
1
mp to Secti
ren
ed AT+), (OBVAT),
eatments
with ts.
score after ence and
gence lower than
tly ar sful or n the
gence and the
OBPT.
e therapy isciency.
on
s

Convbinocwith headdifficreadiperioVariowith theraups pConsconsisurveprescwith
Activpurpoproxiand tdiffervergeand (whet
Until that randoStudytrialssympin priamplmorecompofficetheraimprolatteradditthera
The pused treatand pwith
impro
vergence inscular vision da variety ofaches, blurrulty concenng, and loss
ods of readinous treatmebase-in pris
apy using peplus other thensus regariderable diffeyed the ophcribed treatmsymptomat
e therapies oseful, contimity with ththeir mutuar in their (1)ence and ac(4) use of mher these d
recently, thdocument tomized cliniy Group com
s investigatinptomatic CI ism readingitudes less t
e effective thpared the efe-based placapy/orthoptioving both tr study was tion, it was sapy/orthopti
purpose of tactive treatment using pencil push-home reinfooving sympt
sufficiency (disorder1-4 tf symptoms,red vision, dtrating, movs of compreng or perfornts10, 14-23 asm reading gencil push-uherapy techrding the mferences amhthalmic coment by botic CI.24-26
for the trearolled manihe aim of nol interaction) ability to cccommodativmotor learninifferences a
here has beehe effectivecal trial, the
mpleted 2 ping the effecin children. glasses prethan twice than placeboffectiveness cebo vision tics to be mothe signs ana 19% (9 o
suggested tics regimen
this randomtments for CHBPP, hom
-ups (HBCVAorcement (Otoms and si
CI) is a comthat is often, including ediplopia, slevement of phension afteming close are commonlglasses and ps (HBPP) aniques, officost effectiveong treatmemmunity suth ophthalm
atment of sypulation of tormalizing tns.27 The varcontrol and mve demand)ng theory anffect the ou
en a scarcityeness of treae Convergenilot studies tctiveness of 28-29 In the
escribed accthe near phoo reading gla
of HBPP, oftherapy/ort
ore effectivend symptomof 47) loss that a more should have
ized clinicalCI. We come-based comAT+), officeOBVAT), andgns associa
mmon n associatedeyestrain, epiness,
print while er short activities.5-1
ly prescribedactive treat
alone, homece-based vise treatment ents in time
uggest that mologists and
ymptomatic target blur,he accommrious active manipulate ), (2) dosagnd patient fetcome of tre
y of rigorouatments for nce Insufficithat were ppassive andtrial that ev
cording to Soria),30 prismasses.28 Theffice-based vhoptics foun
e than pencims associate
o follow-up intensive hoe been inclu
trial was topared the efmputer verg-based verg
d office-baseated with sy
13 d, includingtment, suche-based thesion therapyis lacking a
e and cost. RHBPP is thed optometri
CI typicallyvergence dodative andtreatment astimulus pa
ge, (3) modeeedback. It eatment.
sly performCI. In prepaency Treatmlacebo-contd active trea
valuated theheard's critem glasses we other randvision therand office-bal push-ups od with CI.29
before treaome-based uded as a tr
o further evaffectivenessgence/accomgence/accomed placebo tmptomatic C
• Intro • Meth • Resu • Com • Conc • Auth • Refe
passive treh as home-brapy using py, and orthoand there arRecent stud most commists for youn
y involve theemand, and
d vergence sapproaches arameters (ee of adminisis unknown
med scientificaration for oment Trial (Ctrolled, randatments for e effectiveneerion (conve
were found tomized tria
apy/orthoptised vision or placebo t
9 A limitationtment compvision
reatment arm
aluate the cs of 12 weekmmodative tmmodative ttherapy (OBCI in childre
oduction hods
ults
mment
clusions
hor information
erences
eatment based pencil push-optics. re dies that monly
ng patients
e d/or target systems for CI
eg, stration, n, however,
c studies our CITT) domized
ess of base-ergence to be no l that cs, and
therapy in n of the pletion. In
m.31
commonly ks of therapy therapy
BPT) in en.
-

METH
We fothrouboardprotoguardeach
and ewas aeligibfor thInsurparenmoni
PATI
Majoexodnear vergeless tbreakwith patieincludof lesaccoma com
A referrorchan0.75 equivcycloby upfor atmet tperfo
EXAM
Eligibwas sacuitand nconveaccom
HODS
ollowed the ughout the sds of all parocol and infodian (subsestudy patie
each patientan initial cobility examinhe enrollmerance Portabnts. Study otoring comm
IENT SELEC
r eligibility ceviation at point of con
ence at nearthan twice tk), and a CIsymptomat
ents with symded in the sss than 5 diommodative mplete listin
fractive corrr or a signifige was definD or greate
valent, or 1.oplegic refrap to 1.25 D.t least 2 wethe eligibilitormed with a
MINATION
bility testingsymptomatiy at distancnear, NPC, aergence andmmodative
tenets of thstudy. The inrticipating ceormed consequently refent gave writt assented tnsent procenation follownt and randbility and Acoversight wamittee.
CTION
criteria for tnear of at lenvergence (r (PFV) (conthe near phoI Symptom ic CI often hmptomatic Cstudy. Howeopters (D) winsufficiencyg of eligibili
ection was cant changened as 1.50er of astigm.50 D or grection). For h. For myopiaeeks, eligibily criteria. Tappropriate
N PROCEDU
g included adc.12-13,32-33 O
ce and near,and positived divergenceamplitude,
he Declaratinstitutional enters approent forms. Terred to as ptten informeo participat
ess for perfowed by a secomization occountabilityas provided
the trial waseast 4 prismNPC) break
nvergence aoria]30 or mSurvey (CIShave an assCI associateever, childrewere excludy may indicaty and exclu
prescribed fe in refractiv D or greateatism, 0.75 eater of anishyperopes, ta, full correcity testing whus, the CISrefractive c
URES
dministratioOther eligibi a sensorim
e and negatie amplitudemonocular
on of Helsinreview oved the The parent oparent) of ed consent ion. There rming an cond consenof eligible pay Act authorby an indep
s being agedm diopters (
( 6 cm), implitudes) inimum PFVSS) score of ociated accod with acco
en with moned because ate an orgausion criteri
for patients ve correctioner of hyperoD or greate
sometropia ithe investigction was rewas repeatedSS and eligicorrection in
on of the CISility tests inc
motor examinive fusional es]), near steaccommoda
nki
or
nt atients into trization waspendent dat
d 9 to 17 ye) greater
insufficient (ie, failing S
V of 15 bf 16 or greatommodative
ommodative ocular accomthe severitynic etiologya.
if they had n. A significopia, 0.50 Der of anisomin any meridgator could required. Afted to determibility testinn place.
SS to identicluded bestnation (covevergence aereoacuity, ative facility
Jum • Top
• Intro • Meth • Resu • Com • Conc • Auth • Refe
the trial. Hes obtained frta and safety
ears and havthan at far,positive fusSheard's critbase-out bluter. Becausee insufficieninsufficienc
mmodative y of their . The eTable
a significancant refractivD or greater
metropia in sdian (basedreduce the per wearing t
mine if the pag were alwa
fy whether t-corrected ver testing att near [fusiomonocular (the ability
mp to Secti
oduction
hodsults
mment
clusions
hor information
erences
ealth rom y
ving a receded ional terion [PFV ur or e patients
ncy,12 cy were amplitudes
e provides
nt refractive ve error or of myopia,
spherical on prescriptionthe glasses atient still ays
the child visual t distance
onal
y to quickly
on

achieve clear vision while alternately viewing 20/30 print through +2 D and –2 Dlenses), a cycloplegic refraction, and an ocular health evaluation. Convergence Insufficiency Treatment Trial–trained and –certified ophthalmologists or optometrists performed all testing using a previously described standardized protocol.34 Eligible patients who consented to participate were enrolled in the study, and the measures taken at their eligibility examination were used as the study baseline measures.
RANDOMIZATION
Using a permuted block design, we randomly assigned eligible patients who consented to participate with equal probability to HBPP, HBCVAT+, OBVAT, or OBPT. Randomization was achieved using a secure Web site created and managed by the data coordinating center. To ensure approximately equal numbers of patients in
each treatment arm by site, randomization was stratified by clinical site.
TREATMENT PROTOCOLS
The therapy regimens each lasted 12 weeks. Patients were taught their assigned therapy procedures by CITT-trained and -certified therapists. Therapists were either optometrists, vision therapists, or orthoptists with at least 1 year of experience; most optometrists were residency-trained. Patients were required to demonstrate
their understanding and ability to perform home therapy procedures in the office before the therapies were prescribed for home. Instructional handouts were also provided for the home treatment procedures. Patients in all groups maintained a home therapy log and recorded their performances for each home therapy session. Monthly office visits were scheduled for those assigned to the 2 home-based therapy groups. At these visits, the therapists answered questions, reviewed home therapy procedures, and estimated adherence (compliance). In addition, the therapist contacted the patients by telephone on a weekly basis, during which time
the home therapy procedures and home logs were reviewed and attempts were made to motivate the patients to adhere to treatment. Those assigned to office-based therapy groups were scheduled for weekly office therapy visits.
All treatments included time for instruction, feedback, review of the home log, and discussion about adherence. For the office-based groups, this all occurred during the weekly office visits. For the home-based groups, these interactions occurred every 4 weeks in the office and weekly via a telephone call with the therapist. The total treatment time for each group included the time spent in therapy at home or in the office plus the contact with the therapist via the weekly phone calls (for the home-based therapy groups).
HOME-BASED PENCIL PUSH-UPS
The pencil push-ups procedure involved using a pencil with 20/60 reduced Snellen letters and a white index card placed in the background to provide a suppression check by using physiological diplopia awareness. The goal of the procedure was to move the pencil to within 2 to 3 cm of the brow, just above the nose on each push-up while trying to keep the target single and clear. Patients were instructed to perform the pencil push-ups procedure 15 minutes per day, 5 days per week. They maintained home therapy logs, recording the closest distance that they could maintain fusion after each 5 minutes of therapy.

HOME-BASED COMPUTER VERGENCE/ACCOMMODATIVE THERAPY AND PENCIL PUSH-UPS
Patients in this group were taught to perform the pencil push-up procedure as well as procedures on the Home Therapy System/Computerized Vergence System (HTS/CVS) computer software system (Computer Orthoptics, Gold Canyon, Arizona). Using this program, they performed fusional vergence and accommodative therapy procedures, including vergence base-in, vergence base-out, autoslide vergence, and jump ductions vergence programs using random-dot stereopsis
targets. The accommodative rock program was used for accommodative therapy. Much like a clinician would do at each follow-up visit, this computer program automatically modified the therapy program after each session based on the patient's performance. Patients were instructed to do pencil push-ups 5 minutes per day, 5 days per week, and the HTS software program for 15 minutes per day, 5 days per week, and to save their data on a disk provided by the study and to bring the disk to each follow-up visit.
OFFICE-BASED VERGENCE/ACCOMMODATIVE THERAPY WITH HOME REINFORCEMENT
The OBVAT group received a weekly 60-minute in-office therapy visit with additional prescribed procedures to be performed at home for 15 minutes a day, 5 days per week. The therapy procedures are described in detail elsewhere29 and those performed during the weekly OBVAT sessions are shown in the eFigure. At each
office-based therapy session, the patient performed 4 to 5 procedures with constant supervision and guidance from the therapist. There were no diagnostic tests performed during these sessions. The therapist followed a detailed and specific protocol from the CITT manual of procedures (http://optometry.osu.edu/research/CITT/4363.cfm); this document describes each procedure, amount of time procedure was performed, expected performance, and criteria for ending the procedure and advancing to a more difficult level.
OFFICE-BASED PLACEBO THERAPY
Patients in the OBPT group received therapy during a weekly 60-minute office visit and were prescribed procedures to be performed at home for 15 minutes per day, 5 days per week. The placebo therapy program consisted of 16 in-office therapy procedures and 4 home therapy procedures, which were designed to look like real vergence/accommodative therapy procedures yet not to stimulate vergence, accommodation, or fine saccadic eye movement skills beyond normal daily visual activities. The therapist followed a detailed protocol from the CITT manual of procedures. Five procedures were performed during each office therapy visit and 2 procedures were assigned for home therapy each week. Placebo procedures included traditional vergence/accommodative therapy procedures modified to be monocular rather than binocular; binocular procedures performed at 0 vergence disparity; and testing procedures that did not require significant demand on the vergence, accommodative, or fine saccadic eye movement systems. For example, in 1 placebo procedure, the patient wore the appropriate filter glasses and performed vergence therapy at 0 vergence demand on the Computer Orthopter (Computer Orthoptics). Some procedures were designed to have increasing levels of difficulty. As in real therapy, patients frequently wore filter glasses and were told that the
glasses ensured that both eyes were being used together. Objectives and goals

were established for each placebo procedure to simulate real therapy. For motivational purposes, the therapist told the patient the objective of each procedure before beginning the technique.
MASKING OF THERAPISTS AND PATIENTS
Because experienced therapists provided the treatments, it was not feasible to mask them to patients' assigned treatment. However, each therapist followed a well-defined protocol for all treatments and was instructed to interact in an identical fashion with all patients. Although patients were obviously aware of whether they were assigned to office- or home-based therapy, those receiving office-based treatment were masked regarding whether they were assigned to vergence/accommodative or placebo therapy.
To determine the effectiveness of masking, patients assigned to either of the 2 office-based treatments were asked at the completion of their treatment whether they thought they were randomized into the active or placebo treatment. To assess examiner masking, examiners were asked if they thought they could identify the patient's treatment assignment at the completion of each masked examination. In addition, at the completion of the 12-week outcome examination, examiners were asked to guess the patient's group assignment and to report a level of confidence in the response.
FOLLOW-UP EXAMINATIONS
Protocol-specified follow-up visits were conducted after 4 and 8 weeks of treatment. The primary outcome assessment was made at the visit following the 12th week of treatment. At these follow-up visits, an examiner who was masked to the patient's
treatment group administered the CISS and a sensorimotor examination that included cover testing at distance and near, NPC, PFV, accommodative amplitude, and accommodative facility testing. After the clinical testing was completed, the CISS was readministered.
TREATMENT ADHERENCE DATA
To assess adherence with home-based therapy, at each masked examination the therapist was asked, "What percent (0%, 1%-24%, 25%-49%, 50%-74%, 75%-99%, or 100%) of the time do you feel the patient adhered to the home protocol?" The therapists' estimate was based on a review of the home log, electronic data from the computer therapy program, and a discussion with the patient about home therapy. Thus, this estimate was primarily based on patient reports. The response options of 0%, 1% to 24%, 25% to 49%, and 50% to 74% were combined into 1 category (0%-74%) for data analysis because only 16% of patients were categorized into the response options below 75%.
MAINTENANCE THERAPY
Patients who demonstrated sufficient improvement on the CISS at the 12-week outcome visit were considered asymptomatic (CISS score <16) and were prescribed maintenance therapy of 15 minutes per week using home therapy procedures specific to the patient's assigned treatment group. Patients not demonstrating

suffic16)
treat
OUTC
Patie(or plesseby thconsiexamand wsomewith 15 ite(leasour pa dec
The gimprooutcoNPC basePFV, valuethan base
cient improv, were referment for th
COME MEA
nts with CI erceived to
ening or abahe CISS) as isted of 15 i
miner read thwas instructetimes, fairly4 representems were sut symptoma
previous worcrease of at
Vie
goal of treatove the patiome measurwas definedline to the 1a patient ha
e at least tw15 . Imprline to the 1
vement on trred to a noeir CI.
ASURES
who seek trbe by their tement of sthe primarytems that whe questionted to choosy often, or ating the highummed to oatic) was 0 ark,13, 32 a CIleast 10 or
ew larger vers[in this wind
[in a new win[as a PowerPoi
tment for CIient's converes. A normd as an impr12-week outad to pass S
wice the neaovement in 12-week out
the CISS, anon-CITT eye
reatment usparents), a
symptoms. Ty outcome mwere read als while the se 1 of thosealways). Eachest frequenobtain the toand the highSS score of more point
sion (59K): dow] ndow] nt slide]
I is not onlyergence abilal NPC was
rovement (dtcome examSheard's critr phoria maPFV was de
tcome exam
nd thus conscare provid
sually do so and successfThus, we usmeasure (Figoud to the cchild lookede possible ach responsency of sympotal CISS schest was 60less than 1
ts is conside
y to eliminatity. Thus, wdefined as
decrease) inmination. To terion (ie, Pgnitude) an
efined as anmination.
sidered symder to receiv
because thful treatmened symptomgure 1). Thechild by the d at a card wnswers (nev
e was scoredptom occurrecore. The low0 (most sym16 is consideered improve
Figure 1.InsufficienSurvey.
te patient sywe used NPC
less than 6 NPC of 4 cbe classifie
PFV blur or ifnd have a PFn increase of
mptomatic (Cve alternativ
hey are symnt should rem level (as me questionna examiner. Twith 5 answver, infrequd on a scaleence (ie, alwwest possib
mptomatic). ered asympted.
. Convergenncy Sympto
ymptoms, bC and PFV as
cm and an m or more fd as havingf no blur, thFV blur/breaf 10 or m
CISS score ve
ptomatic sult in a measured aire The
wer options ently,
e of 0 to 4, ways). The le score Based on tomatic and
nce m
ut also to s secondary improved from
g normal hen break ak of more ore from

To evdeveoutcooutconormscorefollowan insucce
STAT
All saassumcomman escompsamp
The Cgroupon thclinicof 52varia
All daCaromeasat eaobtaiwas u
As plcovardata ensumeancovarand acollecrelatianalyfinal Tukehold modebetw
A 2 classhoc p
valuate eachloped a comome measurome was a s
mal PFV (>15e of less thawing: normacrease in PFessful treatm
TISTICAL A
ample size cming a 2-sidmon standarstimate of vpared at a tiple size was
CITT was pops, assuminhe CISS, 4 ccian expert o2 children pebles and ad
ata analyseslina). All anasures of the ach study visned from thused.
anned a pririance (ANCfrom both tring the mon comparisoriate becausall subsequected at baseionship betwyses, the leANCOVA moy's method the overall eel was also een groups
test was usified as havpairwise gro
h treatmentmposite outcres from basscore of less5 and pasn 16 or a 10al NPC, an imFV of more tment or imp
ANALYSIS
calculations ded test witrd deviationariability. Tome [6 pair-set at 0.00
owered to reng that the tcm in NPC, aopinion and er group wadjusted for a
s were perfoalyses followCISS score sit were usehe base-out
ori, a 4-groCOVA) was uthe 4-and 8-ost appropriaons. The basse our initialent values. Ieline were eween a partievel for inclodel indicatof adjustmeerror rate aused to con.
sed to compving successoup compari
t's ability to come classifseline to thes than 16 onssing the Sh0-point decrmprovementhan 10 . proved outco
were perforh 90% pow
n (SD) obtaio control forwise compa
083 (0.05/6)
eject the nutrue populatand 10 in the repeatas based on
a 10% loss t
ormed usingwed the inteand the 3 m
ed for analysto blur mea
up by 3-perused to com-week visitsate estimateseline value l pilot data sIn addition,
examined as cular outcousion in theed a significent for multt = 0.05. struct 95%
pare the percful or improsons of the
improve bofication that e 12-week en the CISS, heard's criterease in thet in NPC of Patients whome were co
rmed using er. For a givned from thr multiple coarisons]), th).
ll hypothesition differenPFV. These
ability of eacthe requiredto follow-up
g SAS, versiention-to-tremeasures ofses. Positiveasure if pres
riod repeatempare the tres maximizese of the meaof the outcoshowed a stall clinical apotential co
me measuree final ANCOcant group eiple pairwiseThe mean sconfidence
centage of poved outcompercentage
oth signs anconsidered
examinationa normal N
erion). Impre CISS scoremore than 4o did not monsidered n
PASS 2000ven outcomhe CITT pilotomparisons
he level us
is of no diffences betwee differencesch measured sample si
p.
ion 9.1 (SASeat principlef both the Ne fusional vesent; otherw
ed-measureseatment gros the degreean square eome measutrong correland demogronfounders e and treatm
OVA model weffect or groe group comsquare errointervals fo
patients in emes or as a n
in each cla
d symptomsthe change
n. A successPC (<6 cm)oved was dee, and at lea4 cm, norm
meet the criteonresponde
software35 e measure, t study29 wa(4 groups, ed for deter
erence betwn groups ars were based.13, 36 The saze for the 3
S Institute, e. The meanNPC and PFVergence at nwise, base-o
s analysis ofoups at weees of freedomrror used inre was usedation betweraphic variabof the true
ment groupwas set at 0oup x time inmparisons wor from the Aor the mean
each group wnonrespondssification w
s, we also e in all 3 ful ), and a
efined as a ast 1 of the al PFV, or eria for
ers.
and the
as used as with 2
rmining
ween re 10 points d on ample size
outcome
Cary, Northn of the 2 V obtained
near was out to break
f k 12. Using m, thus n group d as a een baselinebles
. For these
.10. If the nteraction,
was used to ANCOVA difference
who were er. Post
were
h
k

achiemeas95% exam
RESU
ENRO
Betwwereenrol(med11.8 werewerefindinnear;at nedemochildrexotrrandoin mepsychwereconfooutco
PATI
Of thoutcowere(18 oonly perce
eved using losure was incconfidence
miner's gues
ULTS
OLLMENT
ween July 20 enrolled in lled at the 9dian, 25). Thyears (SD, white, 30% Hispanic. Angs were 2; NPC breakear of 12.7 (ographics anren with conropia were eomized to eaedication ushotropic me balanced foounders werome measur
View this t[in this win
[in a new wi[as a PowerPo
IENT FOLLO
e 221 patieome examin missed. Th
of 648 visits17 were mientage of vi
ogistic regrecluded in theinterval we
ss and the p
005 and Octothe study. T
9 sites rangehe mean ag2.3 years);
% were AfricAt baseline, t
(2.8 ) ek/recovery o4.6) /8.8 nd pertinentnstant strabeligible for thach treatmesed among tedications haor these mere identifiedres.
table: ndow] ndow] int slide]
OW-UP
nts who entnation (Figurhe highest ps [2.8%]). Ossed (2.4%sits missed
ession modee regressionere used to aatient's actu
ober 2006, The numbered from 14 te of the pat 59% were an Americanthe mean (S
exodeviationof 14.2 (7.5)(4.5) . Tat clinical me
bismus werehe study anent group. Athe 4 groupsad potentialedications. B
for inclusio
Table 1. Measures
tered the trre 2). Less tercentage o
Of the 720 st). In both owas less th
els. The basn model. An assess the aual group as
221 patientr of patientsto 35 tients was female, 55%n, and 34%SD) clinical n at distance) cm/17.9 (8bl 1 provid
easures at be excluded, pd a small nu
Although thes (highest in effects on a
Based on initn in the AN
CITT Populas at Baseline
ial, 218 (99than 2% of
of missed vistudy visits s
of the home-an 1.5% (1
seline value unweightedagreement bssignment.
ts s
% %
e; 9.3 (4.48.2) cm; andes the studbaseline by tpatients witumber (4-7ere was an in the OBPT accommodatial bivariateCOVA mode
ation Demoge
9%) completall study vissits occurredscheduled in-based treat.3% of 639
Jum • Top
• Intro • Meth • Resu • Com • Conc • Auth • Refe
of each outd statistic
between the
4 ) exodevnd PFV breakdy populatiotreatment gth intermitte patients) wimbalance agroup), only
ation, and the analyses, el for any of
graphics an
ted the 12-wsits throughd in the OBPn the OBVATtment groupvisits in the
mp to Secti
oduction
hods
ultsmment
clusions
hor information
erences
tcome and the
e
viation at k/recovery
on
roup. Whileent were at baseline y he groups no
f the 3
d Clinical
week h week 12 PT group T group, ps, the e HBPP
on

group
TREA
At 12the hgroupgroupnot aor PF
MAS
p and 1.4%
Vie
ATMENT AD
2 weeks, thehome therapp, 84.9% inp (Table 2).affect the reFV (data not
View this t[in this win
[in a new wi[as a PowerPo
KING
of 636 visit
ew larger vers[in this wind
[in a new win[as a PowerPoi
DHERENCE
e percentagpy protocol a the HBPP g Accountingsults of the t shown).
table: ndow] ndow] int slide]
ts in the HB
sion (52K): dow] ndow] nt slide]
E DATA
e of CITT paat least 75%group, 87% g for the obs
treatment g
Table 2. With HomTime
CVAT+ grou
atients rated% of the timin the OBPT
served differgroup comp
Patients Ratme Therapy
up).
Figure 2.randomizeConvergeTreatmenindicates computer vergence/therapy aHBPP, hompush-up toffice-baswith homeand OBVAvergence/therapy wreinforcemvisit.
d by therape was 67.3%T group, andrences in esparisons for
ted by TherProtocol at
. Flowchart ed, clinical nce Insuffict Trial. HBChome-based
/accommodnd pencil pume-based ptherapy; OBsed placebo e reinforcemAT, office-ba/accommod
with home ment. *One
pists as comp% in the HBd 91.4% in stimated adsymptom sc
rapist as CoLeast 75%
of the
ciency CVAT+ d
ative ush-ups;
pencil BPT,
therapy ment; ased ative
missed
pliant with BCVAT+ the OBVAT herence did core, NPC,
mpliant of the

Eightassigto thpatieexamthe erespoassigExamassigcorreassigconfi
PRIM
Figurthe 4outcolower(Tabl6.8 p3.4-1and Hdiffer11.9;differP .
ty-five percegned to verge active the
ents' group aminer felt thaexaminers reonded that hgned to HBPPminers, whengnment onlyect vs incorrgnment and dence interv
MARY OUTC
re 3 displays4 treatment ome examinr mean symle 3). The mpoints lower 10.3; P < .0HBPP grouprence in me; P < .001),rences were38 for all).
Vie
ent of the pagence/accomerapy groupassignment at he could esponded thhe/she was P, and 21%n asked to g
y 34% of therect, P < .00the examinval, 0.04-0.
COME MEA
s the cumulgroups at b
nation, patieptom level c
mean CISS sthan that in
001). A meas (95% conan symptom, observed be observed a
ew larger vers[in this wind
[in a new win
atients assigmmodative t. None of that the 4- oridentify the
hat their patassigned to said their pguess, weree time, whic01). There wer's guess o20).
ASURE
ative distribbaseline andents assignecompared wscore at 12 wn patients an differencefidence inte
m level was between theamong the H
sion (48K): dow] ndow]
gned to plactherapy beliee examiners
r 8-week mae group assigtient was aso HBCVAT+, patient was e correct in ich is less thawas low agreof assigned
bution plots d after 12 wed to the OB
with patientsweeks in passigned to O
e of 7.9 poinerval, 4.4-118.4 points (
e OBVAT andHBPP, HBCV
cebo therapeved that ths felt that thasked examgnment at o
ssigned to th 21% said tassigned toidentifying tan is expecteement betwtreatment g
of the meaneeks of trea
BVAT group s in the 3 otatients in theOBPT (95% nts was foun1.4; P < .00(95% confidd HBCVAT+ VAT+, and O
Figure 3.distributioInsufficienSurvey scduring theexaminatimasked e12. HBCVhome-basvergence/therapy aHBPP, hompush-up toffice-baswith homeand OBVAvergence/therapy w
py and 93% hey had beehey could id
minations, anoutcome. Onhe OBVAT gtheir patiento the OBPT gthe patient'sted by chancween the acgroup ( = 0
n symptom atment. At treported a sther treatmee OBVAT groconfidence
nd between 01). The largdence interv
groups. NoOBPT groups
. Cumulativeon of Convency Symptocores collecte eligibility ion and at t
examination VAT+ indicatsed compute/accommodnd pencil pume-based ptherapy; OBsed placebo e reinforcemAT, office-ba/accommod
with home
of those en assigned dentify the nd only 1 ne-third of roup, 24% t was group. s group ce (ie, 50%
ctual group 0.11, 95%
level for he 12-weeksignificantlyent groups oup was interval, the OBVAT
gest val, 4.9-o significants (pairwise
e rgence m ted
he at week
tes er ative ush-ups;
pencil BPT,
therapy ment; ased ative
%
k y

As seasymat thwith P = .consibased
We asymptreatchanwouldscorethe OobseHBCVamon
SECO
NPC
View this t[in this win
[in a new wi[as a PowerPo
een in Tablemptomatic (ie outcome ethe other tr004). Thereidered asymd groups (p
View this t[in this win
[in a new wi[as a PowerPo
also used anptom score oment if impce that patid be classifiee was withinOBVAT grourved in any VAT+, P < .ng the latter
ONDARY O
Break
[as a PowerPoi
table: ndow] ndow] int slide]
e 4, the perce, CISS scoexaminationeatment groe was no sigmptomatic oairwise P >
table: ndow] ndow] int slide]
n alternate dof less thanrovement wents with CIed as achiev
n the normap met this cof the other001; 35% ir 3 treatmen
UTCOME M
nt slide]
Table 3. Each Out
centage of pore <16) or in) was signifoups (HBPPgnificant diffr improved
.60 for all).
Table 4. Converge
definition of 16 were on
was 10 or mISS scores tving successl variability
criterion, whr treatment n OBPT, P =nt groups (p
MEASURES
Means and tcome by Tr
patients in eimproved (ieficantly high, P = .013; ference in thbetween the
Improvemeence Insuffic
success in wnly considerore points (that just mesful treatmeof the surve
hich was signgroups (38
= .001); thepairwise P >
reinforcem
95% Confidreatment Gr
each group we, change inher in the OHBCVAT+,
he percentage OBPT grou
ent in Signs ciency by T
which patiered to have hTable 4). Th
et the eligibient when they. Sixty-sixnificantly gr
8% in HBPP,ere were no > .50 for all)
ment.
dence Intervroup and Tim
who were con score of BVAT groupP < .001; Oge of patienup and the 2
and Symptoherapy Grou
nts who achhad successhis eliminateility criterion
he change inx percent ofreater than , P = .003; 3statistical d
).
vals for me
onsidered 10 points
p compared OBPT, nts 2 home-
oms of up
hieved a sful ed the n ( 16) the CISS f patients inthat 33% in differences
n
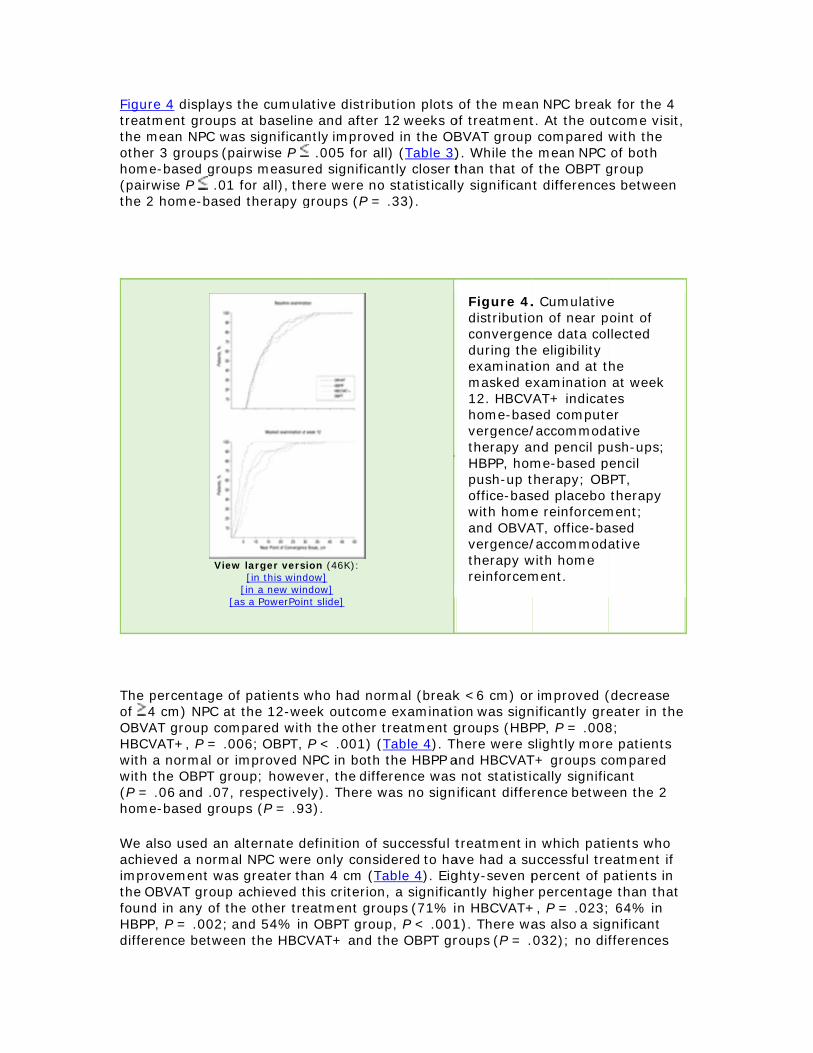
Figurtreatthe motherhome(pairwthe 2
The pof 4OBVAHBCVwith with (P = home
We aachieimprothe OfoundHBPPdiffer
re 4 displaysment group
mean NPC wr 3 groups (e-based growise P .0
2 home-base
Vie
percentage 4 cm) NPC aAT group coVAT+, P = .a normal orthe OBPT g.06 and .07
e-based gro
also used aneved a normovement wa
OBVAT groupd in any of tP, P = .002;rence betwe
s the cumulps at baselinwas significapairwise P
oups measur1 for all), thed therapy g
ew larger vers[in this wind
[in a new win[as a PowerPoi
of patients at the 12-wempared wit006; OBPT, r improved Nroup; howe
7, respectiveoups (P = .9
n alternate dmal NPC weras greater thp achieved tthe other tre and 54% in
een the HBC
ative distribne and after ntly improve .005 for a
red significahere were nogroups (P =
sion (46K): dow] ndow] nt slide]
who had noeek outcomeh the other P < .001) (
NPC in bothver, the diffely). There w3).
definition of e only conshan 4 cm (Tthis criterioneatment gron OBPT grouCVAT+ and t
bution plots 12 weeks o
ed in the OBll) (Table 3)
antly closer to statisticall
= .33).
ormal (breake examinatitreatment g
(Table 4). T the HBPP a
ference was was no sign
successful tidered to ha
Table 4). Eign, a significaoups (71% iup, P < .001the OBPT gr
of the meanof treatmentBVAT group). While thethan that ofy significan
Figure 4.distributioconvergenduring theexaminatimasked e12. HBCVhome-basvergence/therapy aHBPP, hompush-up toffice-baswith homeand OBVAvergence/therapy wreinforcem
k <6 cm) orion was signgroups (HBPhere were s
and HBCVAT not statistiificant diffe
treatment inave had a sughty-seven pantly highern HBCVAT+1). There waroups (P = .
n NPC breakt. At the out compared
e mean NPC f the OBPT gt difference
. Cumulativeon of near pnce data cole eligibility ion and at t
examination VAT+ indicatsed compute/accommodnd pencil pume-based ptherapy; OBsed placebo e reinforcemAT, office-ba/accommod
with home ment.
r improved (nificantly grePP, P = .008slightly moreT+ groups cocally significrence betwe
n which patiuccessful trepercent of pr percentage+, P = .023;as also a sig032); no dif
k for the 4 tcome visit, with the of both
group s between
e point of llected
he at week
tes er ative ush-ups;
pencil BPT,
therapy ment; ased ative
(decrease eater in the 8; e patients ompared cant een the 2
ients who eatment if patients in e than that ; 64% in gnificant fferences

were(P = wouldbase
PFV
FigurtreatexamgreatHBCVOBPTand O
As seoutcootherThereimpro
As wwhichsucce
found betw.20) groupsd be consideline, which i
at Near
re 5 displaysment group
mination, theter than all oVAT+ groupT (P = .008)OBPT group
Vie
een in Tableome examinr treatment e were no soved PFV in
ith CISS scoh patients wessful treatm
ween the HBs. This consered to havemproves to
s the cumulps at baseline mean PFV other group was signific) groups. Ths (P = .57).
ew larger vers[in this wind
[in a new win[as a PowerPoi
e 4, the percnation was sgroups (HBignificant di the latter 3
ore and NPCwho achievement outcom
PP group anervative este had clinica 3.5 cm).
ative distribne and after
for patientss (pairwise cantly bette
here was no .
sion (45K): dow] ndow] nt slide]
centage of psignificantly PP, P = .00fferences in
3 treatment
C break, an d a normal me if improv
nd either thetimate woulally successf
bution plots 12 weeks o
s in the OBVP < .001 fo
er (higher) tsignificant
patients withhigher in th2; HBCVAT+ the percengroups (pai
alternate dePFV were on
vement was
e HBCVAT+d not includful treatmen
of the meanof treatmentVAT group wor all). The mhan in the Hdifference in
Figure 5.distributiofusional vcollected dexaminatimasked e12. HBCVhome-basvergence/therapy aHBPP, hompush-up toffice-baswith homeOBVAT, overgence/therapy wreinforcemdiopter.
h normal orhe OBVAT gr+, P = .007
ntage of patiirwise P > .
efinition of snly consider greater tha
+ (P = .37) ode some patnt (eg, a 7 c
n PFV at neat. At the outwas significamean PFV inHBPP (P = .n response
. Cumulativeon of positivvergence datduring the eion and at t
examination VAT+ indicatsed compute/accommodnd pencil pume-based ptherapy; OBsed placebo e reinforcemffice-based /accommod
with home ment; and
improved Proup compa
7; OBPT, P <ients with n10 for all).
success wasred to have an 10 (Ta
or OBPTients who cm NPC at
ar for the 4 tcome antly n the 037) and in the HBPP
e ve ta eligibility he at week
tes er ative ush-ups;
pencil BPT,
therapy ment;
ative
, prism
PFV at the ared with all< .001). ormal or
s used in had a ble 4).
P

Sevesignifin theOBPTHBCVweresomenear
Succ
UsingPFV, outcogroupgrouppatie(33%class
Seco
Previimproand 2respeachiegroupcompcomp
Atte
Childhighetheregroupmeanbetwbetw
ADV
Six aand fto th
COM
nty-three peficantly highe HBCVAT+T group, P <VAT+ and O detected (Pe patients wwith a PFV
cessful, Im
g the compothe proport
ome in the Ops (P < .002p (73%) ha
ents in the H%), and just
ified.
ondary Mea
ous studiesovements o22% of patiectively, acheved both a p compared parison). Noparison).
ntion-Defic
ren with paer on the CIe were slightps at baselinn treatmenteen ADHD aeen ADHD,
ERSE EVEN
dverse evenfurther evale study trea
MENT
ercent of paher percenta group, P =
< .001). TheOBPT groupsP > .10 for a
who would beat near of 1
proved, an
osite outcomtion of patieOBVAT grou2 for all). Wd either suc
HBPP group more than
asures Com
have assesccurred in bents in the hieved both normal NPCwith the ot
o other grou
cit/Hypera
rent-reporteSS at baselt differencesne. Howevedifferences
and treatmetreatment,
NTS
nts that incluations deteatment.
atients in theage than tha .02; 40% i
ere was alsos (P = .007)all). Again, te considered16 at base
nd Nonresp
me classificants found to
up was signihile nearly t
ccessful or im(43%), oneone-third in
mbined
ssed treatmeboth NPC anOBVAT, HBPa normal N
C and a normher treatmep difference
activity Dis
ed attentionine than chs in the distr, ADHD was among theent (P = .93and time an
uded eyes oermined tha
e OBVAT grat in any of n the HBPP a significan; however, this conservd clinically seline, which
ponder Crit
ation, which o have had ficantly greathree-quartmproved ou
e-third of then the placeb
ent effectivend PFV. SevePP, HBCVATPC and PFV
mal PFV wasent groups (es were sign
sorder
n-deficit/hypildren withoribution of ts not a conf
e groups. Th3). We examnd found no
or vision weat none of th
roup achievethe other trgroup, P<
nt differenceno other sigvative estimsuccessful (eimproves t
teria
combines ssuccessful tater than thers of patie
utcomes, lese patients ino group (35
eness by eventy-three pT+, and OBP. The perces significant(P < .001 fonificant (P >
peractivity dut parent-rethese childrfounder and
here was alsmined the 3-
significant
ere reportedhe events w
ed this critereatment gr.001; and 2e between thgnificant diff
mate would neg, 10 exo 25 ).
symptoms, Ntreatment ohat in any ofnts in the Oss than half n the HBCVA5%) were si
valuating whpercent, 40%PT groups, ntage of patly higher inor each pairw .11 for eac
disorder (ADeported ADHen among td did not affso no interacway interaceffect (P =
d. All were uwere serious
rion, a roups (52% 26% in the he ferences not include
xophoria at
NPC, and r improved f the other
OBVAT
the AT+ group milarly
hether %, 37%,
tients who the OBVATwise ch pairwise
DHD) scoredHD, and treatment fect the ction ction .26).
nexpected or related
T
d

We ctherasympvergereinfoHBPPsympsympthe 2no m
We efrom outcosympmeaspropowhenof all
The fwas dinto ctreatBasestudyno grCISSvariathe C
In thpointrangetreatUsingmediet al3meancan bclinicpointon eftreatissue
The sdifferimproOBVAHBCV
ompared thapy approacptomatic CI.ence/accomorcement wP, HBCVAT+ptoms and cptomatic CI.2 home-base
more effectiv
established 4this study:
ome, (2) theptom score osures, NPC, ortion of patn using the c 3 outcome
first criteriondifficult to eclinical pracment regimd on the groy,29 the CITTroup mean d score was bility in CIS
CITT Study G
e present stts on the CIed from 7 toment groupg Cohen’s37 um, 0.8 is l
38 contend thningful diffebe disregardcally meanints change beffect size, thment effect
e.
second criterences amonoved symptAT met this VAT+, and 4
he effectivenches in 221 c. Office-base
mmodative thas significan
+, and OBPTlinical signs. Although sed therapiesve in improv
4 criteria, a (1) the sco
e proportionon the CISSand PFV (cotients classicomposite omeasures).
n, the treatmestablish a ptice, and, coens that indoup mean dT was desigdifferences i10 points. T
SS scores obGroup, trans
tudy, we didSS. Insteado 8.5 pointsps. This tranguidelines farge), the ghat an effecrence that i
ded. Thus, gngful, thoughetween grouhe 10-point . Further stu
erion used tong treatmenom level oncriterion, in
43% assigne
ness of 3 actchildren wited herapy with ntly more ef
T in improvins associated ymptoms ds, these treaving sympto
priori, to deore differencn of childrenS at outcomeonvergence ified as havioutcome clas.
ment grouppriori. Our suonsequentlydicated clinidifferences foned to haveif the true pThis differenbtained fromslates into a
d not find a , we found
s between thslates to anfor interpretgroup differect size of 0.5s scientifica
group differeh they are leups. Lookingdifference wudy and refi
o assess clinnt groups inn the CISS. A contrast toed to OBPT.
tive vision h
home ffective thanng both the with id improve iatments werms than off
etermine thces on the C who achieve, (3) the champlitudes
ing had succssification (c
difference urvey instru
y, the magncal relevancound for the
e 90% powepopulation dnce of 10 pom 3 separatean effect size
difference istatistically
he OBVAT gr effect size tation of effeences we fo5 is a conseally supportaences observess than theg retrospectwas a signifiinement of t
nical relevan patients' aAfter treatm
o 47% assigChanging t
n
in re fice-based p
e clinical relISS betweeved a normahange in secs) at outcomcessful or imcombining t
in the CISSument had nitude of thece had not be CISS in ouer to reject tifference be
oints, along we randomizee of greater
in group mesignificant group and eathat rangesect size (0.2und are conrvative estimable and unlved in this se a priori estively and recant overesthe CISS wi
nce was whebility to ach
ment, 73% oned to HBPthe criterion
Jum • Top
• Intro • Meth • Resu • Com • Conc • Auth • Refe
lacebo thera
levance of ten treatmenal or improvcondary out
me, and (4) tmproved outthe treatme
score at ounot been ince difference been establiur previous the null hypetween grouwith data on
ed trials conr than 1 SD.
eans of 10 ogroup differach of the ots from 0.77 2 is small, 0nsidered largmate of a cllikely to be study are costimate of a eviewing thestimate of thill help clarif
ether there ieve a norm
of patients aP, 39% assi
n to require t
mp to Secti
oduction
hods
ults
mmentclusions
hor information
erences
apy.
the data t groups at
ved tcome
the tcomes nt effects
utcome, corporated between 2
shed. pilot
pothesis of ups in the n the ducted by .
r more rences that ther 3 to 0.94 SD.
0.5 is ge. Sloan linically
one that onsidered 10 or more
e literature he potentialfy the
were mal or assigned to igned to that
on
.
e

patients achieved both a score of less than 16 and a change of 10 or more points on the CISS resulted in lower success rates for all groups, but the differences among treatment groups remained the same.
The third criterion used was an evaluation of the secondary outcome measures, NPC and PFV (convergence amplitudes), as they are often used clinically to determine treatment success for CI. The proportion of patients who achieved a clinically normal level for both measures was 73% in the OBVAT group compared with no more than 40% in each of the other 3 treatment groups.
The fourth a priori criterion for determining clinical significance was the proportion of patients classified as having successful or improved outcomes when using the composite outcome classification (combining the treatment effects of all 3 outcomes). A significantly higher proportion of children assigned to OBVAT (73%) compared with the 3 other treatment groups was classified as having successful treatment or improved outcome. No significant differences were observed between the 2 home-based groups and the placebo therapy group. Thus, based on the analysis of all 4 a priori criteria, we conclude that there are both statistically significant and clinically meaningful differences between the groups.
The results of this large, randomized clinical trial are similar to those from the only previous randomized trial of vision therapy/orthoptics for CI in children29 in which 3 treatment groups were studied: HBPP, office-based vision therapy/orthoptics, and OBPT. In that pilot study, only the OBVAT group experienced a significant
improvement in symptoms, NPC, and PFV.
The current study was not designed to show the maximal possible improvement with treatment. Longer treatment may have resulted in additional changes in signs and symptoms. Office-based vergence/accommodative therapy programs for CI often include 12 to 24 office visits.19-21 Our 12-week treatment program was based on the assumption that this represented the maximum length of time that a symptomatic patient who was not improving would stay on the assigned treatment. Because our 12-week treatment program is at the low end of the range of time recommended for office-based CI therapy, it is possible that OBVAT might have been effective in more patients had the treatment program been longer. Likewise, a longer treatment program may have resulted in additional improvements by those
assigned to the home-based treatment groups. It is also possible that using more home-based therapy procedures or prescribing longer periods of daily home-based therapy may have produced different results. Answers to these questions will have to await further study.
While a placebo effect could be associated with any of the 4 treatments owing to the patient's expectation that the treatment would be effective, office-based therapy might be more susceptible to this effect owing to the enthusiasm, caring, and compassion of a therapist who spends 60 minutes per week with the patient.39
However, this is the second randomized trial of OBVAT that was designed to control for the effect of the therapist as a placebo40; placebo therapy was designed to simulate bona fide therapy procedures and therapists were trained to behave identically for patients in both of the office-based therapy groups. The data reportedherein confirm that we were successful in achieving this objective, as 85% of the patients assigned to OBPT believed they had been assigned to the actual OBVAT group. This compares well with our previous pilot study in which 90% of the

patients assigned to placebo therapy believed they had been assigned to actual therapy.29 A no treatment group was not included; therefore, it is not known whether any improvements were due to regression to the mean or natural history of the disease. However, this should have affected all treatment groups similarly because there were no statistically significant or clinically relevant differences in any primary or secondary outcome measure among the treatment groups at baseline. Therefore, the observed differences in effectiveness between the OBVAT and placebo therapy groups are most likely attributable to treatment effect.
The OBVAT used in this study represents a typical approach used in clinical practice.21 We conclude that this specific therapy protocol was successful in this study and should be applicable to children with similar clinical findings. A better understanding of which procedures were most effective will require additional research.
While this study was not designed to determine which factors within a particular group contributed to the outcome, the procedures that comprise the OBVAT provide therapists with the greatest ability to control and manipulate stimulus parameters (eg, vergence amplitude and accommodative demand) and to incorporate motor
learning theory (eg, modeling and demonstration, transfer of training, patient feedback). The weekly visits with the therapist during OBVAT also permit the inclusion of a variety of procedures that stress convergence and accommodative abilities not typically addressed in home therapy programs. There were also differences among the treatment groups in time spent performing therapy and interacting with the therapist. The 2 office-based groups had a mean prescribed therapy time of 135 minutes per week; the HBCVAT+ group averaged 115 minutes; and the HBPP group averaged 90 minutes, which included weekly telephone calls with the therapist. However, this study was not designed to equalize time spent
performing therapy and/or interacting with a therapist; rather, it was designed as an effectiveness study to evaluate 3 clinical treatments typically provided in clinical practice. It is possible that the difference in treatment effect found in this study
could be related to the OBVAT group having been prescribed more minutes of therapy per day than the home-based groups. However, having a patient perform a greater amount of daily home-based therapy, particularly pencil push-ups, is likely impractical.
There are limited data in the literature that suggest there is a relationship between CI and ADHD.41-42 Although we asked parents whether their child had ADHD (ie, parental report), this study was not designed to assess this relationship and was not powered for such subgroup analyses, nor was the diagnosis of ADHD definitive. However, investigation of this possible association is of interest and merits additional research.
We could not identify any other sources of bias or confounding factors to explain our findings. Accounting for slight differences in the distribution of baseline factors between groups in the analyses did not alter the interpretation of the results. The
follow-up visit rate was excellent and almost identical in all 4 groups. The investigators performing the 4-, 8-, and 12-week examinations were masked to the treatment group, and the patients in the 2 office-based treatment groups were effectively masked as well. We did have slight differences in adherence among the
groups, however, and accounting for these differences in estimated adherence did not affect the results of the treatment group comparisons for the CISS score, NPC,

or PF
Whenrecogagedsuggtheraof thenorm
With in thiwith calledofficeeffecweekresulphonwere
It is eits sipatie(4 vistreatis wo
Theretime.betwbasedthey have chaneffecenconot kcan bof thetherasustatreatcond
CON
FV. The plac
n translatinggnize that th 9 to 17 yeaested by ou
apy/orthoptie treatment
malization of
regards to is study for considerabld on a weeke visits evertive if presc
kly telephonts of the CITe calls, prov classified a
easy to undmplicity and
ents in a shosits for homment). Whi
orthwhile to
e are a num. It is possibeen the thed treatmentwere depena placebo h
ges found int. It is possiurage adher
know which be modified e synergisticapist interacained over tment must ucting.
CLUSIONS
ebo effect w
g these studhey can onlyars. Adults wr pilot studyics we used,ts we studieor improve
home-basedthe HBPP gy closer follo
kly basis by ry fourth wecribed accore calls fromTT pilot studvide some ss having su
erstand thed cost-effectort time and
me-based trele our studyexplore in f
mber of interble that therrapist and tt groups' resndent on pathome-basedn the 2 homible that diffrence wouldprocedures to make it mc role of thection. It is aime. Therefawait the re
S
was account
dy results iny be appliedwith symptoy.43 Our find, OBVAT wit
ed in this triaement in sym
d therapy, iroup were dow-up than a therapist,
eek. It is posding to usua a therapistdy, in whichsupport for tccessful or
e clinical poptiveness. Borequire few
eatments coy was not defuture resea
resting clinicre may be pthe patient tsults differetient-therapd therapy gr
me-based groferent protod affect the were most
more effectie active homlso not knowfore, a conclesults of the
ed for by in
nto clinical pd to childrenomatic CI mdings indicatth home reial, with aboumptoms and
t is importaderived from
is typical in, completedssible that thal clinical prt and often hh the HBPP gthis hypotheimproved o
pularity of hoth HBPP anwer follow-uompared witesigned to crch.
cal questionpsychologicathat could afntially (if thpist contact roup and thuoups are duocols that moutcomes. Feffective or ive. This inc
me treatmenwn whether lusion aboute 12-month
corporating
practice, it isn with symptay respond te that the snforcementut 75% of p
d signs withi
ant to note tm a therapy n clinical prad a home loghis treatmeractice, whichas less freqgroup did noesis, as noneutcomes.29
home-basedd HBCVAT+p visits thanth 12 visits fonduct a co
ns that cannal effects froffect the off
hese effects time). In thus, do not ke to a real oore closely For the OBVr whether thcludes undent componen
the treatmet the long-tefollow-up st
Jum • Top
g the OBPT g
s important tomatic CI wdifferently,
specific form, is the mos
patients achin 12 weeks
hat the dataprogram de
actice. Patieg, and returnt would bech does not quent followot receive we of the 11
treatment b+ can be taun office-basfor office-baost-utility an
ot be answeom the interfice-based awere prese
his study, weknow whetheor placebo tmonitor and
VAT regimenhe treatmenrstanding thnt as well asent effect werm benefit tudy we are
mp to Secti
group.
to who are as
m of vision st effective ieving
s.
a reported esigned ents were
ned for e less include
w-up. The weekly patients
because of ught to ed therapy
ased nalysis, this
ered at this action
and home-nt, and if e did not er the treatment d n, we do t protocol he nature s the
will be of
e
on

This trial odemowith 12-wsymp
AUTH
CorrPennAve,
Submfinal 5, 20
FinaintereHBCV
FundNatio
Th
Cli
Sitnuareexa
BasMDMD(VT(SC
StaDr Frie
large-scale of treatmenonstrates thhome reinfo
week programptoms and s
HOR INFOR
espondencsylvania CoPhiladelphia
mitted for revision rec
008.
ncial Discloest in CompVAT+ group
ding/Suppoonal Institut
e CITT Stu
nical Sites
es are listedmber of pate listed as Paminer, and
scom PalmeD (E); Mark D (E); KathrT); Ronda SC); and Elia
ate UniversiCooper (PI)edman, OD
multi-centets for childr
hat a 12-weeorcement is m of HBPP oigns associa
RMATION
ce: Mitchell llege of Opta, PA 19141
Publicationeived June
osure: Dr Cputer Orthop.
ort: This stues of Health
udy Group
s
d in order ofients in pareI for princip
d VT for visio
er Eye InstitDunbar, ODyn Nelson,
Singh, OD (Vs Silverman
ity of New Y); Audra Ste(VT); Steve
er, randomizen with symek regimen more effect
or HBCVAT+ated with CI
Scheiman, tometry, 1201 (mscheima
n: Decembe4, 2008; ac
Cooper has aptics, the co
udy was suph, Departme
f the numbeentheses af
pal investigaon therapist
tute, Miami, D (E); Craig OD (E); VicVT); Eva Olin (SC).
York College einer, OD (Een Ritter, OD
zed clinical mptomatic Cof OBVAT tive than a
+ in improviI.
OD, 00 W [email protected]
er 11, 2007;ccepted June
a financial mpany that
pported by tent of Health
er of patientfter the site ator, SC for
t.
Florida (35)McKeown, ky Fischer, Ovares (SC);
of OptometE, Co-PI); MD (E); Lily Z
CI
ng
ey u).
; e
t sells the pr
the Nationah and Huma
ts enrolled iname and lsite coordin
5): Dr TamkMD (co-PI);OD (VT); Ad Ana Rosa (
try, New YorMarta BrunelZhu, OD (E)
• Intro • Meth • Resu • Com • Conc • Auth • Refe
Jum • Top
• Intro • Meth • Resu • Com • Conc • Auth • Refe
rogram use
l Eye Instituan Services.
n the studylocation. Per
nator, E for
ins (PI); Hild; Arlanna Modam Perlma(SC); Nidia
rk, New Yorli (VT); Stac; Lyndon W
oduction
hods
ults
mment
clusions hor information
erences
mp to Secti
oduction
hods
ults
mment
clusions
hor information erences
d for the
ute of the
, with the rsonnel
da Capo, oshfeghi, an, OD Rosado
rk (28): cy
Wong, OD
on

(E); Ida Chung, OD (E); and Kaity Colon (SC).
University of Alabama at Birmingham School of Optometry, Birmingham (28): Dr Hopkins (PI); Marcela Frazier, OD, MPH (E); Janene Sims, OD (E); Marsha Swanson, OD (E); Katherine Weise, OD, MBA (E); Adrienne Broadfoot, MS, OTR/L (VT, SC); Michelle Anderson, OD (VT); and Catherine Baldwin (SC).
Nova Southeastern University, Ft Lauderdale, Florida (27): Dr Coulter (PI); Deborah Amster, OD (E); Gregory Fecho, OD (E); Tanya Mahaphon, OD (E); Jacqueline Rodena, OD (E); Mary Bartuccio, OD (VT); Yin Tea, OD (VT); and Annette Bade, OD (SC).
Pennsylvania College of Optometry, Philadelphia (25): Dr Gallaway (PI); Brandy
Scombordi, OD (E); Mark Boas, OD (VT); Tomohiko Yamada, OD (VT); Ryan Langan (SC), Ruth Shoge, OD (E); and Lily Zhu, OD (E).
The Ohio State University College of Optometry, Columbus (24): Dr Kulp (PI); Michelle Buckland, OD (E); Michael Earley, OD, PhD (E); Gina Gabriel, OD, MS (E); Aaron Zimmerman, OD (E); Kathleen Reuter, OD (VT); Andrew Toole, OD, MS (VT); Molly Biddle, MEd (SC); and Nancy Stevens, MS, RD, LD (SC).
Southern California College of Optometry, Fullerton (23): Dr Cotter (PI); Eric Borsting, OD, MS (E); Dr Rouse (E); Carmen Barnhardt, OD, MS (VT); Raymond Chu, OD, MS (VT); Susan Parker (SC); Rebecca Bridgeford (SC);
Jamie Morris (SC); and Javier Villalobos (SC).
University of California–San Diego Ratner Children's Eye Center, San Diego (17): Dr Granet (PI); Lara Hustana, OD (E); Shira Robbins, MD (E); Erica Castro (VT); and Cintia Gomi, MD (SC).
Mayo Clinic, Rochester, Minnesota (14): Dr Mohney (PI); Jonathan Holmes, MD (E); Melissa Rice, OD (VT); Virginia Karlsson, BS, CO (VT); Becky Nielsen (SC); Jan Sease, COMT, BS (SC); and Tracee Shevlin (SC).
CITT Study Chair
Dr Scheiman (study chair); Karen Pollack (study coordinator); Dr Cotter (vice chair); Dr Hertle (vice chair); and Dr Rouse (consultant).
CITT Data Coordinating Center
Ms Mitchell (PI); Tracy Kitts (project coordinator); Melanie Bacher
(programmer); Linda Barrett (data entry); Loraine Sinnott, PhD
(biostatistician); Kelly Watson (student worker); and Pam Wessel (office associate).
National Eye Institute, Bethesda, MD

Dr
CIT
Dr
Ro
Da
MaMDMa
*AutInsufresulMitchand M(alphDavidSusa
REFE
1. Lérelatischoo1979
2. Léelem
3. PopopuWEB O
4. RoamonOF SCI
5. Da22. W
Redford; an
TT Executi
Scheiman; use.
ata and Saf
arie Diener-WD; Ron D. Haanny, OD, Ph
thors/Writfficiency Trets: Lead au
hell, MAS; MMaryann Rehabetical): Jd Granet, Mnna Tamkin
ERENCES
étourneau JEionship betwol achievem
9;56(1):18-2
étourneau JEentary scho
orcar E, Martlation of un
OF SCIENCE | P
ouse MW, Bong fifth and IENCE | PUBME
aum KM. CoWEB OF SCIENC
nd Paivi Misk
ve Commit
Ms Mitchell;
fety Monito
West, PhD (ays, PhD; AhD.
ing Commeatment Triathors: Mitch
Marjean Kulpdford, DDS,effrey CoopD; Kristine
ns, OD.
E, Lapierre Nween conver
ment. Am J O22. WEB OF SC
E, Ducic S. Pool children.
tinez-Palomiversity stud
PUBMED
orsting E, Hsixth grade
ED
onvergence E | PUBMED
kala, PhD.
ttee
; Dr Cotter;
oring Comm
chair); Rev rgye Hillis,
ittee: The fal Study Grohell Scheimap, OD, MS; M, MPH. Addi
per, MS, ODHopkins, OD
N, Lamont Argence insufOptom PhysiCIENCE | PUBM
Prevalence o Can J Opto
mera A. Prevdents. Opto
yman L; et ers. Optom V
insufficiency
Dr Hertle;
mittee
Andrew CosPhD (throug
following meoup take autan, OD; SusMichael Routional writin; Rachel CoD, MSPH; B
A. The fficiency andiol Opt. MED
of convergeom. 1988;50
alence of gem Vis Sci. 1
al. FrequenVis Sci. 199
y. Am J Opt
Dr Kulp; Dr
stello, CSsRgh March 20
embers of ththorship ressan Cotter, Ouse, OD, MEng committeulter, OD; Mrian G. Moh
d
nce insuffic0:194-197.
eneral binoc1997;74(2):
ncy of conve9;76(9):64
tom Physiol
Jum • Top
• Intro • Meth • Resu • Com • Conc • Auth • Refe
r Redford; a
R; William V006); and Ru
he Convergsponsibility OD, MS; G.
Ed; Richard ee membersMichael Gallhney, MD; a
iency amon
cular dysfun:111-113. F
ergence insu3-649. FULL
Opt. 1984;6
mp to Secti
oduction
hods
ults
mment
clusions
hor information
erences
nd Dr
. Good, uth
ence for the Lynn
Hertle, MD;s away, OD; nd
g
nctions in a ULL TEXT |
ufficiency TEXT | WEB
61(1):16-
on

6. Cotreat
7. Keperso
8. Podisab
9. Ma1971
10. DSyste
11. POpht
12. Bconve2003
13. BconveSci. 2
14. vof Str
15. ALiving
16. CPhila
17. PYork,
18. vLouis
19. GBosto
20. P1997
21. SAccomand W
22. HParal
23. Gtreat2002
24. Cconve
25. SconveSCIEN
ooper J, Ducment. J Am
ent PR, Steeonnel and re
oynter HL, Sbility. Am J O
azow ML. Th1;8:243-244
Duke-Elder Sem of Ophth
Pickwell LD, thalmic Phys
Borsting E, Rergence and
3;74(1):25-3
Borsting EJ, ergence ins2003;80(12
von Noordenrabismus. S
Abrams D. Dgstone; 199
Cibis G, Tongdelphia, PA
Pratt-Johnso, NY: Thiem
von Noordens, MO: Mosb
Griffin JR, Gon, MA: But
Press LJ. App7.
Scheiman Mmmodative Wilkins; 200
Hugonnier Rlysis. St Lou
Gallaway M, ment for co
2;79(4):265
Chin FH, Faiergence ins
Scheiman Mergence insCE | PUBMED
ckman R. Co Optom Ass
eve JH. Convelief by orth
Schor C, HayOptom Phys
he converge4.
S, Wybar K.halmology. S
Hampshire siol Opt. 198
Rouse MW, d accommod34. PUBMED
Rouse MW,ufficiency sy):832-838.
n GK. BinocuSt Louis, MO
Duke-Elder's93.
gue A, Stas: Mosby-Yea
on JA, Tillsone Medical P
n G, Helvestby-Year Boo
risham JD. Btterworth-He
plied Concep
, Wick B. Cland Eye Mo
02.
R, Clayette-Huis, MO: CV
Scheiman Monvergence i-267. FULL TE
bish B, Hisaufficiency. J
, Cooper J, ufficiency. O
onvergence soc. 1978;49
vergence insoptic metho
ynes HM, Hisiol Opt. 198
ence insuffic
Ocular motSt Louis, MO
R. The sign81;1(1):13-
Deland PN; dative insuff
Mitchell GLymptom surFULL TEXT | W
ular Vision aO: Mosby; 19
s Practice of
s-Isern M. Dar Book; 19
n G. Manageublishers; 2
ton E. Strabk; 1994.
Binocular Aneinemann; 2
pts in Vision
linical Managovement Dis
Hugonnier CMosby; 196
M, MalhotrainsufficiencyEXT | WEB OF
aka C, Thal LJ Beh Optom
Mitchell GL;Optom Vis S
insufficienc9(6):673-68
sufficiency: ods. Mil Surg
rsch J. Ocul82;59(2):11
ciency syndr
tility and strO: Mosby; 1
nificance of i-18. WEB OF S
et al. Assocficiency in s
L; et al. Valirvey in childWEB OF SCIENC
and Ocular M996.
f Refraction.
Decision Ma93.
ement of St2001.
ismus: A De
nomalies: D2002.
n Therapy. S
gement of Bsorders. Phi
C. Strabismu69.
K. The effey: a pilot stuSCIENCE | PUB
L, Tsuda K. m. 1995;6:9
; et al. A suSci. 2002;79
cy: incidence80. WEB OF SC
incidence arg. 1953;112
lomotor fun16-127. WEB
rome. J Pedi
rabismus. In1973.
inadequate SCIENCE | PUB
ciation of syschool-age c
dity and reldren aged 9CE | PUBMED
Motility: The
Edinburgh,
king in Pedi
trabismus an
ecision Maki
Diagnosis an
St Louis, MO
Binocular Visladelphia, P
us, Heteroph
ectiveness oudy. OptomBMED
A survey of91-92, 109.
rvey of trea9(3):151-15
e, diagnosisCIENCE | PUBM
among milita2(3):202-20
ctions in reaB OF SCIENCE |
iatr Ophthal
n: Duke-Eld
convergencBMED
ymptoms anchildren. Op
iability of th-18 years. O
eory and Ma
, Scotland:
iatric Ophth
nd Amblyop
king Approac
nd Vision Th
O: Mosby-Ye
sion: HeteroPA: Lippinco
horia and O
of pencil pusm Vis Sci.
f the treatm
atment mod57. FULL TEXT
s, and MED
ary 05. PUBMED
ading PUBMED
lmol.
der S, ed.
ce.
nd ptometry.
he revised Optom Vis
anagement
Churchill-
halmology.
pia. New
ch. St
erapy.
ear Book;
ophoric, tt, Williams
cular Motor
shups
ment of
alities for | WEB OF
r

26. SrandoFULL T
27. Cnons2002
28. Seffecsymp2005
29. Sof tre2005
30. S
31. KOpht
32. BinsufInsufFULL T
33. MconveOF SCI
34. TConvOpht
35. H2000
36. Rused 2002
37. CEarlb
38. Squest2005
39. BIn: HCamb
40. MWEB O
41. Bsympprelim
42. Gconve
Scheiman Momized cliniTEXT Ciuffreda KJtrabismic ac
2;73(12):73
Scheiman Mtiveness of ptomatic con5;89(10):13
Scheiman Meatments fo5;123(1):14
Sheard C. Zo
Kushner BJ. thalmol. 200
Borsting E, Rfficiency andfficiency andTEXT | WEB OF
Mitchell G, Sergence insIENCE | PUBME
The Convergvergence Insthalmic Epid
Hintze J. NC0.
Rouse MW, Hin the class
2;79(4):254
Cohen J. Stabaum Associ
Sloan JA, Cetionnaire da
5;58(12):12
Brody H. TheHarrington Abridge, MA:
Margo CE. TOF SCIENCE | P
Borsting E, Rptomatic accminary stud
Granet DB, Gergence ins
, Mitchell GLcal trial [rep
. The scientccommodati5-762. PUBM
, Cotter S, Rbase-in prisnvergence in18-1323. FR
, Mitchell GLr convergen-24. FREE FU
ones of ocul
The treatm05;123(1):1
Rouse MW, d normal bind Reading S SCIENCE | PU
Scheiman M,ufficiency pED
gence Insuffsufficiency Tdemiol. 2008
SS and PAS
Hyman L, Hsification of -264. FULL TE
atistical Powates; 1988.
ella D, Hays ata: another17-1219. FU
e doctor as A, ed. The Pl
Harvard Un
he placebo PUBMED
Rouse M, Chcommodativy. Optomet
Gomi CF, Veufficiency a
L, Cotter S;ply]. Arch O
ific basis foive and bino
MED
Rouse M; etsm reading nsufficiencyREE FULL TEXT
L, Cotter S;nce insufficieLL TEXT
lar comfort.
ent of conve100-101. FRE
De Land PNnocular childStudy (CIRS)UBMED
, Borsting Eatients. Opt
ficiency TreaTreatment T8;15(1):24-
SS. Kaysville
ussein M. RconvergencEXT | WEB OF
wer Analyses.
RD. Clinicar step towarULL TEXT | WEB
a therapeutlacebo Effecniversity Pre
effect. Surv
hu R. Measuve dysfunctitry. 2005;76
entura R, Mind ADHD. S
et al. ConvOphthalmol.
r and efficacocular vision
t al. Randomglasses vers
y in children
et al. A ranency in child
Am J Optom
ergence insEE FULL TEXT
. Prospectivdren on CIR) group. Op
; et al. Evaltom Vis Sci.
atment TrialTrial: design36. FULL TEXT
e, UT: Numb
Reliability of ce insufficienSCIENCE | PUB
s for the Beh
l significancrd consensuB OF SCIENCE
tic agent: a ct: An Interdess; 1997.
v Ophthalmo
uring ADHD on or conve6(10):588-5
iller-ScholteStrabismus.
vergence ins2005;123(
cy of optomn disorders.
mised clinicasus placebo. Br J Ophth
ndomized trdren. Arch O
m. 1930;7:
ufficiency [e
ve comparisS symptom
ptom Vis Sci
luation of a 2001;78(1
l (CITT) Stun, methods, T | WEB OF SC
ber Crunche
binocular vncy. Optom BMED
havioral Scie
ce of patientus. J Clin Epi| PUBMED
placebo effdisciplinary
ol. 1999;44(
behaviors inergence insu592. PUBMED
e A. The rela2005;13(4)
sufficiency: 12):1760-1
metric vision Optometry
al trial of theo reading glahalmol.
rial of the efOphthalmol.
9-25.
editorial]. A
on of conve surveys. Coi. 1999;76(4
symptom s2S):37. FUL
udy Group. Tand baselin
CIENCE | PUBM
er Statistica
ision measuVis Sci.
ences. Hillsd
t-reported idemiol.
fect researchExploration
(1):31-44. F
n children wufficiency: a
ationship be):163-168.
761. FREE
therapy in y.
e asses for
ffectiveness .
Arch
ergence onvergence4):221-228.
survey for L TEXT | WEB
The ne data. ED
l Systems;
urements
dale, NH:
h agenda. .
FULL TEXT |
with a
etween FULL TEXT |
e .

PUBME
43. StherainsufSCIEN
SECT
Cit
Techno
RELA
EviscCrimRalphC. LloArch EXTR
The NishaRevaArch EXTR
RELA
RespSusaMichaExecArch EXTR
TreaDavidArch EXTR
THIS
ED Scheiman Mapy/orthoptifficiency in yCE | PUBMED
TION EDITO
teULike C
orati Twi
ATED LETT
ceration ofme—Reply h C. Eagle, Joyd, III, andOphthalmo
RACT | FULL
Steroid Coa R. Acharyathi RajaramOphthalmo
RACT | FULL
ATED ARTI
ponse to Edn Cotter, Mael Rouse, autive CommOphthalmo
RACT | FULL
tment Optd K. WallaceOphthalmo
RACT | FULL
S ARTICLE
, Mitchell GLics versus pyoung adults
R: ROY W.
Connotea
tter What's
ERS
f Blind, Pai
Jr, Hans E. d Robert Fol. 2009;127
L TEXT
ontroversy a, Muthiah S
man, Michael. 2009;127
L TEXT
CLES
ditorial Aboarjean Kulpand for the C
mittee l. 2009;127
L TEXT
tions for Sye l. 2008;126
L TEXT
HAS BEEN
L, Cotter S;pencil pushus. Optom Vi
BECK, MD,
Delicious
this?
inful Eyes W
Grossniklaulberg
7(9):1229.
in BacteriaSrinivasan, l Zegans, St
7(9):1231.
out the Co, Mitchell ScConvergenc
7(9):1229-1
ymptomati
6(10):1455-
CITED BY
et al. A ranps for the tris Sci. 2005
PhD
Digg
With Occul
s, Nasreen
al KeratitisJeena Masctephen McLe
nvergencecheiman, Rice Insufficien
230.
c Converge
1456.
OTHER AR
ndomized clreatment of;82(7):583-
lt Uveal Me
A. Syed, R.
s carenhas, Meeod, and Th
e Insufficiechard Hertlency Treatme
ence Insuf
RTICLES
inical trial of convergen-595. FULL TE
elanoma N
Nick Hogan
eenakshi Rahomas M. Li
ency Treatme, G. Lynn Ment Trial (CI
fficiency
of vision ce EXT | WEB OF
ot a
n, William
avindran, etman
ment TrialMitchell, ITT)

LearHandPediaABST
VisioShainAmerABST
Resp-RepWallaArch FULL
RespCotteArch FULL
LearAmerPediaABST
Effecof VeKulp IOVSABST
DoesKarlsAmerABST
TreaWallaArch FULL
�
rning Disabdler et al. atrics 2011;TRACT | FUL
on Therapynberg r. Orthoptic TRACT
ponse to Edply ace OphthalmoTEXT
ponse to Eder et al. OphthalmoTEXT
rning Disabrican Acadeatrics 2009;TRACT | FUL
ctiveness oergence/Aet al.
S 2009;50:2TRACT | FUL
s Nonsurgisson r. Orthoptic TRACT
tment Optace OphthalmoTEXT
bilities, Dys
127:e818-eLL TEXT
y and Ortho
Jrnl. 2010;
ditorial Abo
l 2009;127:
ditorial Abo
l 2009;127:
bilities, Dysmy of Pedia124:837-84
LL TEXT
of Placebo ccommoda
2560-2566. LL TEXT
cal Treatm
Jrnl. 2009;
tions for Sy
l 2008;126:
slexia, and
e856.
optics
60:28-32.
out the Co
:1230-1231
out the Co
:1229-1230
slexia, andatrics, Sectio44.
Therapy foative Thera
ment of Exo
59:18-25.
ymptomati
:1455-1456
d Vision
nvergence
.
nvergence
.
d Vision on on Ophth
or Maintainapy
odeviations
c Converge
.
e Insufficie
e Insufficie
hal et al.
ning Maski
s Work?
ence Insuf
ency Treatm
ency Treatm
ng in a Clin
fficiency
ment Trial-
ment Trial
nical Trial
-