365 days of care - parliament of victoria - · pdf fileannual report 2012–2013 days of...
TRANSCRIPT

ST VINCENT’S HoSpITal, MElbourNE aNNual rEporT
2012–2013
Days of Care365
ReSPoNSiBLe BodieS deCLARATioN
In accordance with the Financial Management Act 1994, we are pleased to present the Report of Operations for St Vincent’s Hospital (Melbourne) Limited for the year ending 30 June 2013.
Mr Gary HumphrysBoard Director Dated 26th August 2013 Melbourne
Professor Patricia O’Rourke Chief Executive Officer Dated 26th August 2013 Melbourne
CoNTeNTS
Report of operations 2013 Page 8
Company directory Page 41
directors’ Report Page 42
Accountable officer’s and directors’ declaration Page 49
Auditor-General’s Report Page 50
Auditor-General’s independence declaration Page 52
Comprehensive operating Statement Year ended 30 June 2013 Page 53
Statement of Financial Position as at 30 June 2013 Page 54
Statement of Changes in equity Year ended 30 June 2013 Page 55
Cash Flow Statement Year ended 30 June 2013 Page 56
Notes to and forming part of the financial statements Page 57
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
1
Compassionaccepting people as they are, bringing to each the love and tenderness of Christ
Justicetreating all people with fairness and equality so as to transform society
Integrityacting with honesty and truth while ensuring that who we are enables others to flourish
Excellenceexcelling in all aspects of our healing ministry

2
Over the past year
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
10.00am, 20 November 2012CARDIOLABSt vincent’s Hospital invests $1.3 million to upgrade essential equipment in two cardiac catheter laboratories with leading edge technology.
10.45am, 1 JULY 2013FunDIng FOR CLInICAL SChOOL upgRADeSt vincent’s Hospital’s Clinical School is granted the funding to upgrade tutorial and examination rooms providing greater access to innovative simulation and e-learning platforms.

ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
3
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
3:00pm, 3 marCH 2013SCRuBS RunSt vincent’s Foundation holds the inaugural ‘Scrubs run’, raising $253,000 towards the cost of a new Stealth machine; an important addition to our advanced brain and spinal scan equipment.
11:00am, 3 maY 2013AuStRALIA’S FIRSt BIOFAB SuItean additive biofabrication suite with ‘3D printers’ and the potential to create regenerative muscle, nerve and other tissues is opened.
4
fOreWOrd frOm the trustees Of mary aIKenhead mInIstrIes
Congratulations to all the executives, staff, clinicians, advisory Council members and supporters of St vincent’s Hospital melbourne for the wonderful way you have continued the mission we share during the course of the last year. You all continue to build on the tradition of the Sisters of Charity of australia which began in Sydney in 1838 and then in melbourne in 1893. The Sisters of Charity transferred responsibility for their Health ministries, including St vincent’s Hospital melbourne, to the Trustees of mary aikenhead ministries, who they appointed in 2009.
Special acknowledgment is due to John Gurry who retired as Chairman of the board of St vincent’s Health australia last year. John’s contribution to St vincent’s as a clinician and then as a Director, spanned over 50 years. The Trustees also acknowledge the valuable contribution of Greg Sword who retired from the St vincent’s Health australia board during the year and welcome melbourne based professor, Suzanne Crowe am, to the board.
During the year, Sr Helen Clarke rSC and Jim russell were appointed Trustees of mary aikenhead ministries. Sister Helen is well known to many as a former Congregation Leader, former board member of St vincent’s Health australia, educator and, of course, Sister of Charity. Jim is Queensland based and a former insurance executive, former Chair of Sisters of Charity and Holy Spirit Sisters Health Services and advisor to the brisbane archdiocese.
as in past years, the Trustees hosted the leaders of all the ministries at their annual conference in brisbane with the theme “The Heart of our Service”. We focussed on Ignatian spirituality and discernment and its application to leadership and decision making. our key note speakers were Sr Una o’Neil rSC from Ireland and Fr mark raper SJ based in the philippines. They spoke of the spirituality of the present moment, the interconnectedness of the human and the holy aspects of our lives, looking for God’s presence in all things and in our activities and how we can draw on the framework of Ignatian spirituality to make decisions. The feedback from our leaders was extremely positive.
The Trustees are sincerely grateful to the many people who demonstrate great commitment to our shared values and apply their skills for the benefit of patients and each other as St vincent’s Hospital melbourne continues to bring the healing ministry of Christ to all we serve.
on behalf of the Trustees of mary aikenhead ministries I am pleased to commend to you the 2012–2013 annual report of St vincent’s Hospital melbourne.
mr David robinson Chairperson, Trustees of mary aikenhead ministries

ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
5
message frOm the bOard chaIr and ceO
It is with great pleasure that we present St vincent’s Hospital’s annual report for 2012–13.
In this historic year for our Health Service, in which we marked the 100th anniversary of St George’s Health Service and the 75th anniversary of Caritas Christi Hospice, we continue to push the boundaries of clinical excellence, education and medical research.
St vincent’s Hospital has long been at the forefront of medical research, and in 2012–13 we have strengthened collaborations with other leading research institutes to enhance our position as leaders in the field.
In 2012–13 we made significant progress towards the aikenhead Centre for medical Discovery (aCmD), signing a memorandum of Understanding with our partners, and jointly committing $60 million towards this vital project. as australia’s first biomedical engineering research and education hub, the aCmD will drive innovation in biomedical engineering, enabling us to reduce the burden of chronic disease in the community, and create jobs and new industries in a boost to victoria’s economy.
The aCmD partnership is already delivering important results, with breakthroughs during 2012–13 in muscle and limb repair, in the development of an epilepsy prediction device and australia’s first bionic eye implant. These discoveries have the potential to transform and vastly improve the quality of people’s lives.
mindful of the importance of collaborations in tackling major health problems, in april, St vincent’s Hospital became part of another significant partnership in biomedical research, the melbourne academic Centre for Health.
The new Centre was announced by the victorian Health minister, The Honourable David Davis mp, and will see St vincent’s Hospital come together with 21 organisations, including partner hospitals, medical research institutes and the University of melbourne.
This important collaboration will focus on core themes, including research and innovation, workforce capacity and training, translational programs, managed comprehensive care, primary care integration and prevention and health literacy.
In medical education, our Clinical School commenced teaching in the Doctor of medicine (mD) course. as the only australian professional entry masters level program, this course creates a new benchmark in 21st century medical education, and further enhances our position as one of australia’s leading clinical schools.
We completed renovations at our Clinical School building, and enhanced student access to e-learning and simulation platforms, both important components of the mD program.
We continued to lead the way in victoria against the National elective Surgery performance targets, and continued to invest in new strategies and models of care to improve our performance against the National emergency access Target.
We pressed ahead with our ambitious capital planning and development agenda, including planning for the rapid Care Centre, and significant capital improvements, including four new High Dependency Unit beds, a reconfigured emergency department, and an adult prevention and recovery Care service in North Fitzroy.
St vincent’s ability to consistently provide the highest standards of health care for our patients is made possible thanks to the passion and dedication of our staff. our values of compassion, justice, integrity and excellence underpin everything that we do. In this historic year, we are deeply proud of our Health Service and look forward to continuing to be a leader of the transformation in health care in australia, bringing about healthier, longer lives.
mr paul robertson board Chair St vincent’s Health australia
professor patricia o’rourke Chief executive officer St vincent’s Hospital melbourne
6
St Vincent’s Hospital, Melbourne provides medical and surgical services, sub acute care, aged care, correctional health, mental health services and a range of community and outreach services.
St vincent’s Hospital operates at 15 sites across greater melbourne, including a major teaching, research and tertiary referral centre situated in Fitzroy, sub acute care at St George’s Health Service Kew, palliative care at Caritas Christi Hospice, as well as aged care, correctional health, pathology collection centres, general practice services and dialysis satellite centres.
In 2012–13 St vincent’s Hospital treated 47,723 acute inpatients that equated to 47,762 WIeS (Weighted Inlier equivalent Separations). The hospital also recorded 96,227 public acute specialist clinic and allied health ambulatory attendances. across the sub-acute setting a total of 40,720 patient bed days were separated for rehabilitation, Gem and CraFT programs, 12,247 bed days were separated for palliative care patients and 72,571 bed days were utilised for residential, restorative and Transition Care including Transition Care at Home.
as at 30 June 2013, St vincent’s Hospital had 901 beds across all of its services.
GoVernance
St vincent’s Hospital, melbourne is part of the St vincent’s Health australia group of companies and one of the ministries of mary aikenhead ministries.
on 1 July 2009 mary aikenhead ministries was established by the Congregation of religious Sisters of Charity of australia to succeed, continue and to expand a number of the health and aged care, education and welfare ministries in which the Sisters of Charity have been engaged for over 150 years. The name is both a tribute to, and reminder of, the extraordinary work of mary aikenhead, the Foundress of the Sisters of Charity who dedicated her life to service of the poor.
St vincent’s Health australia operates under the direction of mary aikenhead ministries, providing leadership and governance of the health and aged care ministries in victoria, New South Wales and Queensland.
as a national group, St vincent’s Health australia is the nation’s largest not-for-profit Catholic health and aged care provider encompassing public, private and aged care, research and clinical education.
abOut st vIncent’s hOspItal
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
11.00am, 19 JULY 2012AwARDS FOR AuBuRn hOuSe
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
7
St vincent’s Health australia has a single national board and a group executive team. In addition, St vincent’s Hospital melbourne is led by the Ceo and an executive team.
St vincent’s melbourne reports to the national St vincent’s Health australia board. In melbourne, Queensland and New South Wales there are local advisory Councils to enable engagement with local stakeholder needs.
MiSSion
as a Catholic health and aged care service our mission is to bring God’s love to those in need through the healing ministry of Jesus. We are especially committed to people who are poor or vulnerable.
We draw on the talents of our people and collaborate with others who share our vision and values to continue the pioneering spirit of mary aikenhead and the Sisters of Charity. We are committed to providing compassionate and innovative care, enabling hope for those we serve.
OuR vISIOn
To lead transformation in health care inspired by the healing ministry of Jesus.
OuR CARe IS:
– provided in an environment underpinned by mission and values
– holistic and centred on the needs of each patient and resident
– high-quality, safe, and continuously improving to ensure best practice
– innovative and informed by current research using contemporary techniques and technology
– delivered by a team of dedicated, appropriately qualified people who are supported in a continuing development of their skills and knowledge
– committed to a respect for life in accordance with the Gospel.
ValueS
our values, which are based on the Gospel, act as a point of reference for our decision making, and are fundamental to our Catholic identity. our values underpin all we do and are demonstrated through our everyday actions, giving our mission life.
in all our activities we strive to demonstrate:
coMpaSSion
inteGrity
JuStice
excellence
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
3,854 47,723 51,572numBeR OF Fte StAFF
numBeR OF ACute InpAtIentS
tOtAL numBeR OF SepARAtIOnS
8
St GeorGe’S centenary
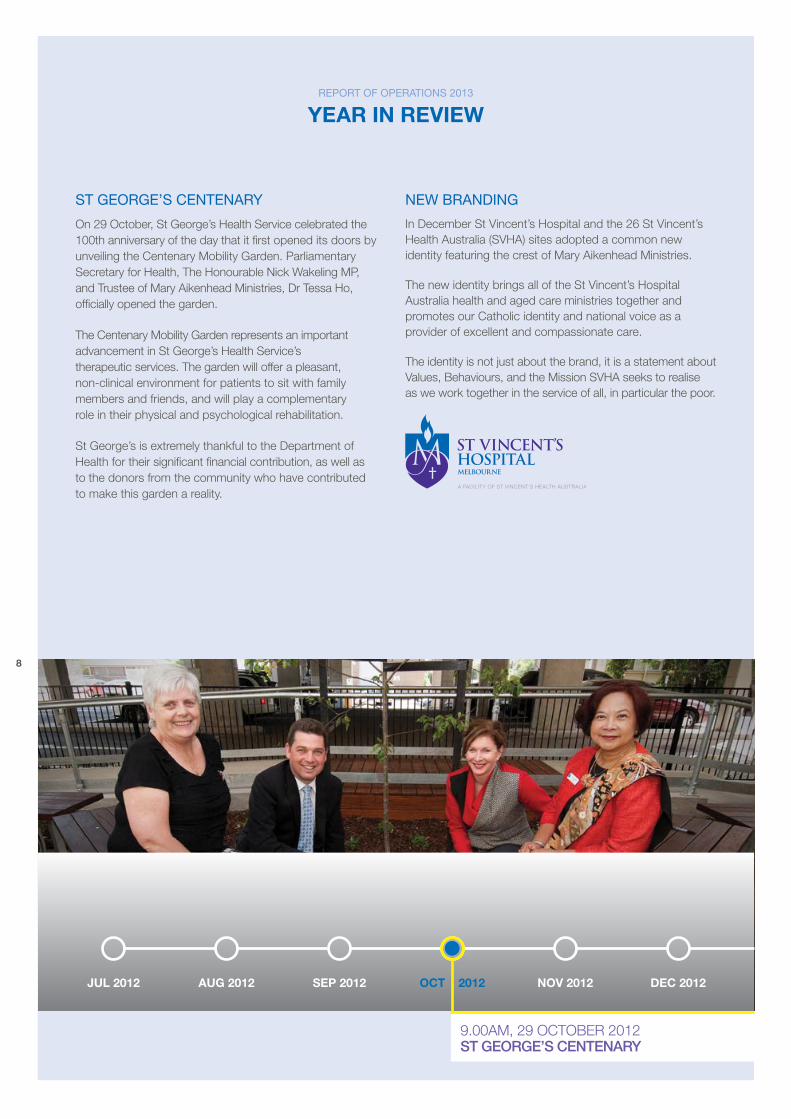
on 29 october, St George’s Health Service celebrated the 100th anniversary of the day that it first opened its doors by unveiling the Centenary mobility Garden. parliamentary Secretary for Health, The Honourable Nick Wakeling mp, and Trustee of mary aikenhead ministries, Dr Tessa Ho, officially opened the garden.
The Centenary mobility Garden represents an important advancement in St George’s Health Service’s therapeutic services. The garden will offer a pleasant, non-clinical environment for patients to sit with family members and friends, and will play a complementary role in their physical and psychological rehabilitation.
St George’s is extremely thankful to the Department of Health for their significant financial contribution, as well as to the donors from the community who have contributed to make this garden a reality.
new brandinG
In December St vincent’s Hospital and the 26 St vincent’s Health australia (SvHa) sites adopted a common new identity featuring the crest of mary aikenhead ministries.
The new identity brings all of the St vincent’s Hospital australia health and aged care ministries together and promotes our Catholic identity and national voice as a provider of excellent and compassionate care.
The identity is not just about the brand, it is a statement about values, behaviours, and the mission SvHa seeks to realise as we work together in the service of all, in particular the poor.
report of operationS 2013
year In revIeW
9.00am, 29 oCTober 2012St geORge’S CentenARy
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012

ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
9
aikenHead centre for Medical diScoVery
In an australian first, leading researchers have come together to take biomedical research on a fast track to success. The aikenhead Centre for medical Discovery (aCmD) will be the first biomedical engineering research and education centre in australia.
The aCmD will bring together research and training from hospitals, universities and medical research institutes in a purpose-built, collaborative research centre. International experience and research confirms that collaborative centres like the aCmD deliver better research outcomes while significantly reducing the time to commercialise discoveries.
Through concurrent research and Development collaborative work practices, the aCmD will reduce the burden of chronic disease in the community (such as arthritis, cancer, cardiovascular disease, diabetes, mental health, musculoskeletal disorders and dementia) through advances in biomedical engineering, and create new, world-leading industries in device creation, tissue engineering and drug design and delivery.
The unique learning and teaching environment of the aCmD will foster a culture of innovation – ‘bedside to bench to bedside’ – that brings together leading clinicians and scientists to solve clinical problems.
medical, engineering and scientific education will be fully integrated into the research environment on the hospital campus, creating a highly-skilled, well-resourced and collaborative workforce.
$1.3M for upGrade of cardio lab
St vincent’s Hospital has invested $1.3 million to upgrade essential equipment in two cardiac catheter laboratories. The Cardiac angiography Suite in Lab I and the Haemodynamic monitoring System in Lab II were replaced with leading edge technology to better suit the needs of patients.
St vincent’s Hospital provides an a1 cardiac care service and is regarded as a leader in the field of cardiac research and surgery. The equipment will support the cardiac care program and ensure that it remains at the forefront of clinical care. patient demand for procedures undertaken in catheter laboratories is expected to increase in the medium-term as developments in procedures and new mechanical devices in cardiac care continue to drive a trend towards non-invasive procedures.
The new equipment will be used to perform over 2,200 procedures each year, including coronary angiograms, stenting and pacing.
St Vincent’s Hospital provides an A1 cardiac care service and is regarded as a leader in the field of cardiac research and surgery.
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
901numBeR OF BeDS
239,290 $587.8mtOtAL
BeD DAyStOtAL
Revenue
10
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
new 3t Mri MacHine
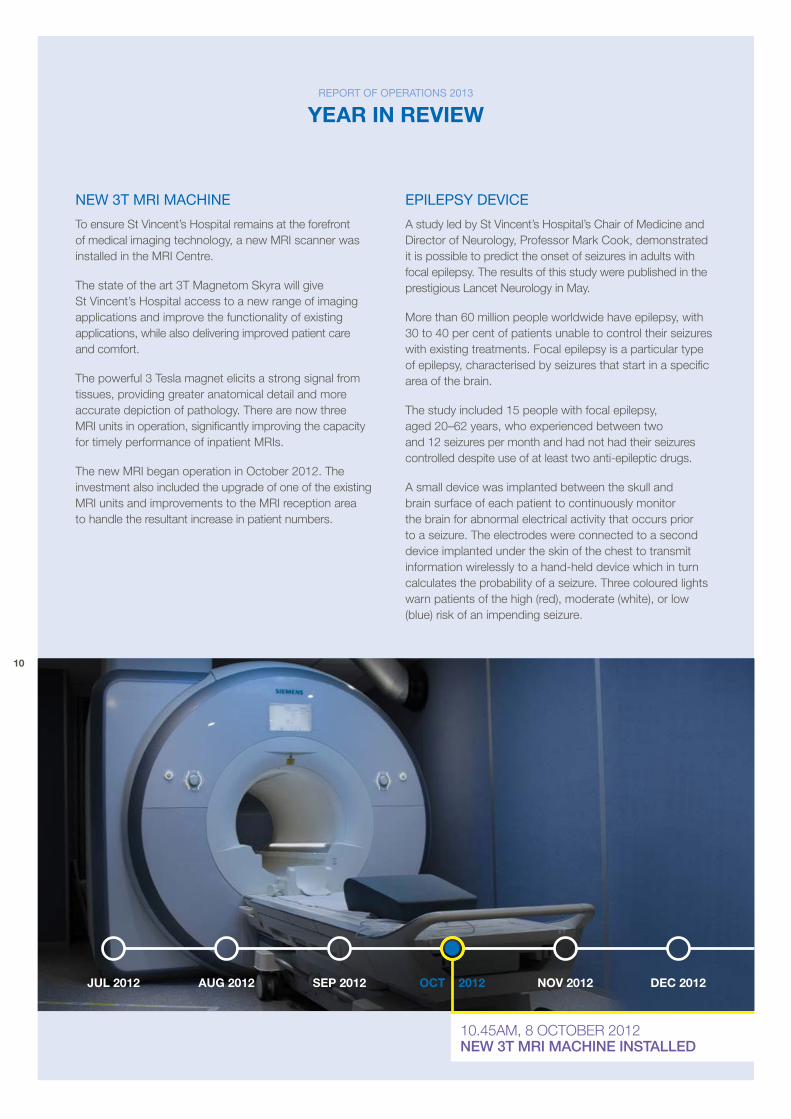
To ensure St vincent’s Hospital remains at the forefront of medical imaging technology, a new mrI scanner was installed in the mrI Centre.
The state of the art 3T magnetom Skyra will give St vincent’s Hospital access to a new range of imaging applications and improve the functionality of existing applications, while also delivering improved patient care and comfort.
The powerful 3 Tesla magnet elicits a strong signal from tissues, providing greater anatomical detail and more accurate depiction of pathology. There are now three mrI units in operation, significantly improving the capacity for timely performance of inpatient mrIs.
The new mrI began operation in october 2012. The investment also included the upgrade of one of the existing mrI units and improvements to the mrI reception area to handle the resultant increase in patient numbers.
epilepSy deVice
a study led by St vincent’s Hospital’s Chair of medicine and Director of Neurology, professor mark Cook, demonstrated it is possible to predict the onset of seizures in adults with focal epilepsy. The results of this study were published in the prestigious Lancet Neurology in may.
more than 60 million people worldwide have epilepsy, with 30 to 40 per cent of patients unable to control their seizures with existing treatments. Focal epilepsy is a particular type of epilepsy, characterised by seizures that start in a specific area of the brain.
The study included 15 people with focal epilepsy, aged 20–62 years, who experienced between two and 12 seizures per month and had not had their seizures controlled despite use of at least two anti-epileptic drugs.
a small device was implanted between the skull and brain surface of each patient to continuously monitor the brain for abnormal electrical activity that occurs prior to a seizure. The electrodes were connected to a second device implanted under the skin of the chest to transmit information wirelessly to a hand-held device which in turn calculates the probability of a seizure. Three coloured lights warn patients of the high (red), moderate (white), or low (blue) risk of an impending seizure.
10.45am, 8 oCTober 2012new 3t mRI mAChIne InStALLeD
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
11
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
In addition to accurately predicting a seizure, the device demonstrated that most participants greatly underestimated the number of seizures they were having.
professor Cook and his fellow researchers are optimistic that if the findings are replicated in larger, longer studies, this technology will improve management strategies including developing methods of preventing seizures using direct electrical stimulation or fast-acting drug therapies.
radioloGy aGreeMent witH royal eye and ear
St vincent’s Hospital’s Central melbourne medical Imaging (CmmI – now known as St vincent’s private radiology) won a tender to provide radiology services to The royal victorian eye and ear Hospital (rveeH) in east melbourne.
This new partnership will allow St vincent’s to secure further revenue and build relationships with strategic partners, in alignment with St vincent’s Strategic plan 2010–15.
CmmI will work in close partnership with rveeH to achieve an improved service delivery model and better access for patients to high quality diagnostic imaging.
St vincent’s Hospital has a long affiliation with rveeH in the provision of healthcare services to both inpatients and outpatients. a link tunnel between the sites facilitates collaboration between the two hospitals and delivers better patient care.
biofabrication Suite
a new research suite with ‘3D printers’ and equipment with the potential to create regenerative muscle, nerve and other tissues was opened in St vincent’s Hospital’s Clinical Neurosciences Department in may.
The facility is the first of its kind in an australian hospital and over time, it is hoped that it will open the way for the routine production of reparative body tissue for individual patients.
The research suite contains customised equipment capable of developing fibres for nerve and muscle regeneration, and a ‘pneumatic extrusion printer’ capable of developing three dimensional implants for muscle, nerve, cartilage and bone regeneration.
This technology is very exciting because it opens the possibility of printing joints, blood vessels, bits of bone and other structures that could potentially be made from the patient’s own tissue so that they adapt to the body more quickly.
The research suite is part of the arC Centre for electromaterials Science bionics platform collaboration between St vincent’s Hospital and the University of Wollongong’s Intelligent polymer research Institute, and is an example of the type of collaborative research that will be advanced at the aikenhead Centre for medical Discovery.

12
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
SutureleSS aortic ValVe SurGery – auStralian firSt
The Cardiothoracic Surgery team performed the first surgery in australia of a ground-breaking sutureless aortic valve replacement procedure, which uses a new class of rapid-deployment aortic valve, eliminating the need for sutures, decreasing the impact of the surgery on patients and reducing the risk of complications.
The replacement aortic valve uses a heat sensitive metal that can be folded into position, which simplifies deployment, while allowing the valve to be repositioned during the implant.
The standard method of performing a surgical aortic valve replacement is to perform a sternotomy, which involves a vertical line incision being made along the breast bone, which is then divided or cracked to provide access to the heart and lungs. The patient is placed on a heart lung machine and the heart is opened and the diseased aortic valve is removed. a new valve is then secured into position using sutures.
In the second half of 2013 the device will be used to perform aortic valve replacement operations through a small cut in the right side of the chest, avoiding the sternotomy, further reducing the invasiveness of the procedure and reducing the chance of complications. This will significantly shorten the length of time of the procedure and allow patients to recover from surgery much quicker, leave hospital sooner and return to work and normal life.
This will significantly shorten the length of time of the procedure and allow patients to recover from surgery much quicker.
11:02am, 12 DeCember 2012AuStRALIA’S FIRSt SutuReLeSS
AORtIC vALve RepLACement
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
13
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
relationSHip witH uniVerSity of Melbourne
St vincent’s Hospital Ceo, professor patricia o’rourke, University of melbourne’s vice Chancellor, professor Glynn Davis, Dean of the Faculty of medicine, professor James angus, and other representatives signed a new agreement outlining the partnership between the Hospital and the University in relation to teaching, research and academic activity.
The agreement will ensure the continued vital work of medical training and research performed by the two institutions will continue into the future.
St vincent’s acknowledges the significant support provided by professor James angus who retired from his role as the University’s Dean, Faculty of medicine, Dentistry and Health Sciences in July 2013. professor angus has been instrumental in the leadership and development of the Hospital’s and University’s shared strategic priorities, including the aikenhead Centre for medical Discovery, the victorian Comprehensive Cancer Centre and the melbourne academic Centre for Health.
150 year anniVerSary of Melbourne Medical ScHool
During 2012 the University of melbourne celebrated the 150th anniversary of the melbourne medical School. In august, Head of the School, professor Jim best, presented St vincent’s Hospital with a certificate of appreciation to commemorate the vital role of St vincent’s Hospital in training and developing doctors.
St Vincent’S openS refurbiSHed clinical ScHool
St vincent’s Clinical School received funding to upgrade simulation and e-learning facilities in 2012.
The school, which has been at its current location since 1992, now boasts three refurbished tutorial rooms, a simulation room with two examination spaces, as well as a renovated common room fit for the advances in teaching medicine in the 21st Century.
The Clinical School offers australia’s only professional entry masters level program, the University of melbourne mD program, which creates a benchmark in 21st century education.
$519,000AnnuAL OpeRAtIng
SuRpLuS
41,255 22,478emeRgenCy DepARtment
pReSentAtIOnS mentAL heALth
BeD DAyS
14
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
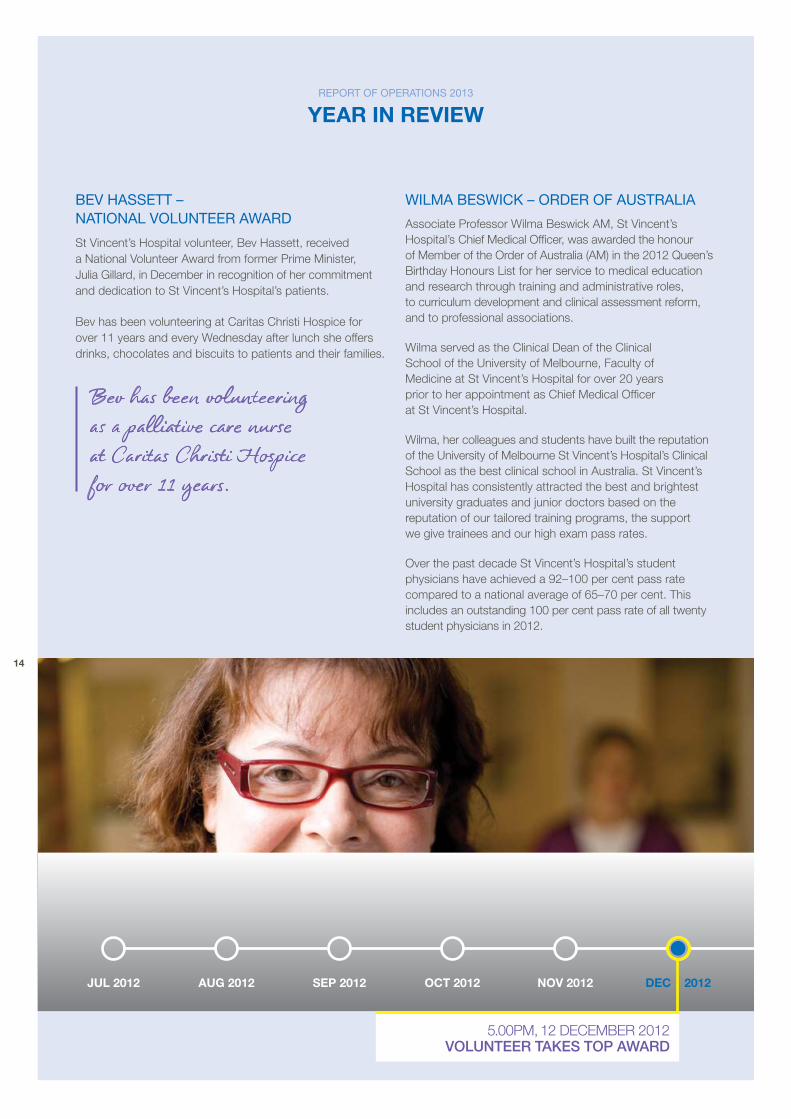
beV HaSSett – national Volunteer award
St vincent’s Hospital volunteer, bev Hassett, received a National volunteer award from former prime minister, Julia Gillard, in December in recognition of her commitment and dedication to St vincent’s Hospital’s patients.
bev has been volunteering at Caritas Christi Hospice for over 11 years and every Wednesday after lunch she offers drinks, chocolates and biscuits to patients and their families.
Bev has been volunteering as a palliative care nurse at Caritas Christi Hospice for over 11 years.
wilMa beSwick – order of auStralia
associate professor Wilma beswick am, St vincent’s Hospital’s Chief medical officer, was awarded the honour of member of the order of australia (am) in the 2012 Queen’s birthday Honours List for her service to medical education and research through training and administrative roles, to curriculum development and clinical assessment reform, and to professional associations.
Wilma served as the Clinical Dean of the Clinical School of the University of melbourne, Faculty of medicine at St vincent’s Hospital for over 20 years prior to her appointment as Chief medical officer at St vincent’s Hospital.
Wilma, her colleagues and students have built the reputation of the University of melbourne St vincent’s Hospital’s Clinical School as the best clinical school in australia. St vincent’s Hospital has consistently attracted the best and brightest university graduates and junior doctors based on the reputation of our tailored training programs, the support we give trainees and our high exam pass rates.
over the past decade St vincent’s Hospital’s student physicians have achieved a 92–100 per cent pass rate compared to a national average of 65–70 per cent. This includes an outstanding 100 per cent pass rate of all twenty student physicians in 2012.
5.00pm, 12 DeCember 2012vOLunteeR tAkeS tOp AwARD
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
15
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
inauGural ScrubS run
over 2000 participants completed the first ever annual St vincent’s Hospital Scrubs run on Sunday 3 march. The 5km course along Yarra boulevard began in burnley park, richmond. Family and friends of all ages enjoyed live music, food and a great community atmosphere in the park, before gathering to cheer on participants as they crossed the finishing line.
The St vincent’s Hospital community spirit and support culminated in a fundraising total of $253,000. all funds raised by our many enthusiastic supporters went towards a new Stealth machine. The Stealth is the latest in brain and spinal scanning technology, and offers the best in treatment for so many of our patients with head trauma, spinal injury, brain tumours and epilepsy.
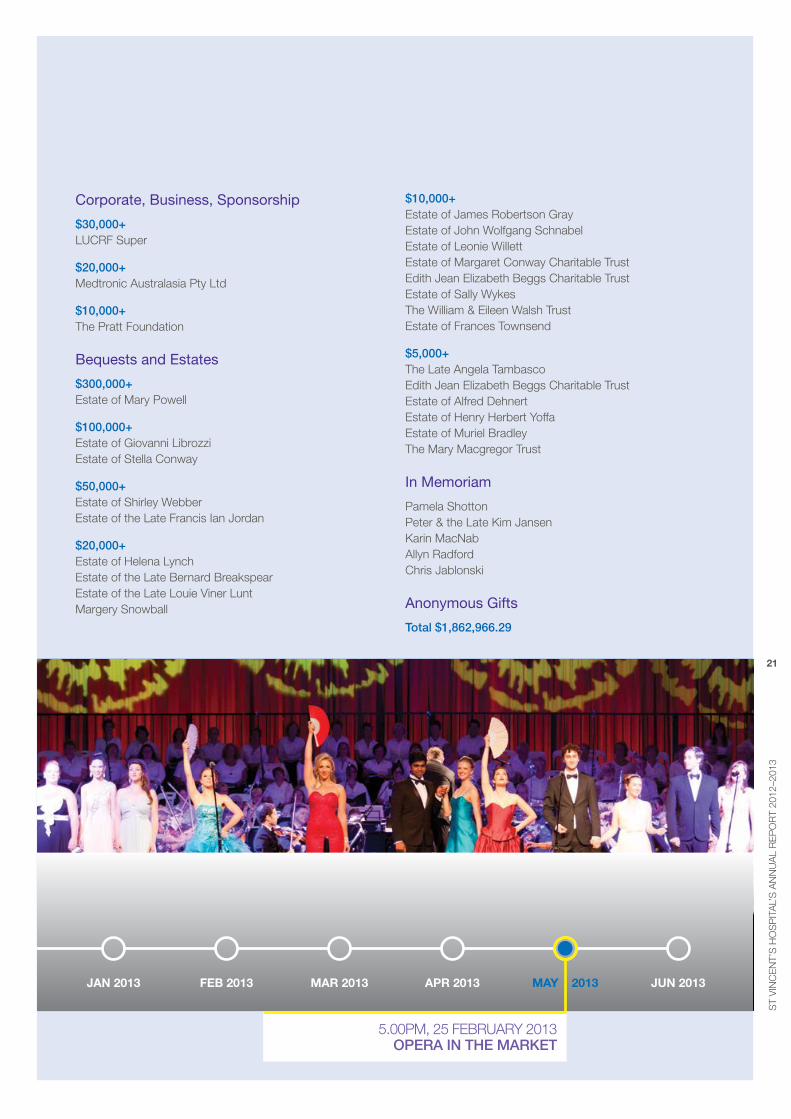
opera in tHe Market 2013
The pairing of fine food and beautiful music, combined with a mild February night, made for a spectacular opera in the market.
The event was a sell-out, with 1,700 guests attending. Celebrated soprano, Julie Lea Goodwin, acclaimed trumpeter, James morrison, and opera Scholars australia put on memorable performances, accompanied by a spectacular 100-voice choir conducted by Guy Noble.
opera in the market is one of St vincent’s Hospital’s annual fundraising events and $150,000 was raised on the night for the Home Dialysis program.
The Foundation raised $150,000 for St Vincent’s Hospital’s Home Dialysis Program at Opera in the Market.
16
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
reconciliation action plan
St vincent’s Hospital has a long history of providing care to aboriginal patients and is the largest metropolitan provider of healthcare to aboriginal adult clients in victoria.
Under the guidance of St vincent’s Health australia’s reconciliation plan, St vincent’s Hospital continues to build and grow its relationship with aboriginal people.
In 2012, thanks to ‘Closing the Gap’ funding from the victorian Department of Health, St vincent’s Hospital continued its commitment to scholarships and training for aboriginal medical, nursing and allied health students through the implementation of an aboriginal Nursing Cadetship program.
The aboriginal Nursing Cadetship program aims to increase the number of aboriginal nurses at St vincent’s Hospital by providing a cadetship as part of the bachelor of Nursing course, which in turn will improve culturally appropriate care to aboriginal patients.
The pilot program of four aboriginal cadetships provided support and paid clinical placement experience for up to 12 weeks in a variety of areas, in addition to the usual placements that are part of a bachelor of Nursing. So far, one cadet has successfully graduated at the
end of 2012 and been employed as a graduate nurse within St vincent’s Hospital, while another three will complete their studies in 2013.
To acknowledge National Sorry Day on 26 may, St vincent’s Hospital marked its ongoing commitment to reconciliation by holding smoking ceremonies at the Fitzroy and St George’s campuses, conducted by Cultural Keeper, ross morgan.
a plaque, acknowledging the traditional owners of the land, was unveiled in the courtyard by St vincent’s Ceo, professor particia o’rourke and Senior aboriginal Liaison officers, michelle Winters, amanda punch and Fay Halatanu.
St Vincent’s Hospital has a long history of providing care to Aboriginal patients.
eLeCtIve SuRgeRy ADmISSIOnS
numBeR OF SIteS
5,494 15710pALLIAtIve CARe
pAtIentS DISChARgeD

ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
17
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
aboriGinal HealtH liaiSon officerS Meet priMe MiniSter
St vincent’s Hospital’s Senior aboriginal Liaison officer, michelle Winters and aboriginal Hospital Liaison officer, mandy punch were invited to an exclusive meeting with former prime minister, Julia Gillard, while attending the reconciliation action plan showcase in Canberra in February.
The two day event was an opportunity for 40 organisations to share the work they have undertaken towards closing the gap through their reconciliation action plans. St vincent’s Hospital was proud to be the only healthcare provider invited to participate, alongside some of australia’s largest and best known corporations.
Local initiatives including our aboriginal Cultural Walking Tour, the cardiac care improvement project, the trial of an aboriginal mental Health Liaison officer and our memorandum of Understanding with the victorian aboriginal Health Service were recognised along with the work of our colleagues from Queensland and New South Wales.
auburn HouSe national award winnerS
auburn House won two 2012 better practice awards for its residents’ shed and for their tranquillity and sports garden.
The better practice awards recognise quality improvement and better practice in aged care and serve as exemplars to encourage improvement and innovation and recognise the aged care industry’s high achievers.
The residents’ shed provides auburn House patients with opportunities for engaging in familiar activities in a safe environment, while the tranquillity and sports garden provides opportunities to reconnect residents to previous life roles and skills and increase their sensory experiences.
firSt eVer MiSSion MaSterclaSS
In September, St vincent’s Hospital launched its mission master Class program with 25 participants from across the hospital. The master Class, designed and developed to be the flagship session of a wider staff formation strategy, gives participants the opportunity to spend a day immersed in the stories of the Sisters of Charity, sharing examples of our values in action, and recognising their own gifts and talents to continue to live our mission in their everyday work.
11.15am, 6 FebrUarY 2013ReCOnCILIAtIOn ACtIOn pLAn ShOwCASeD
18
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
SuStainability
St vincent’s Hospital is striving to minimise our environmental footprint by encouraging environmentally aware practice, developing energy efficient buildings and infrastructure and setting targets for improved environmental sustainability.
St vincent’s Hospital met its goal of diverting at least 29 per cent of its general waste to recycling for the 2012–13 financial year through the reduce, reuse and recycle program.
Several improvements were made to buildings and infrastructure throughout the year to reduce energy consumption and increase efficiency, including:
– introduction of LeD lighting to replace the dichroic downlights, which resulted in savings of almost $25,000pa and lower greenhouse emissions
– installation of carbon monoxide detection in the basement car park to control the exhaust system, which reduces energy consumption by up to 85%
– purchase of new Toyota prius C hybrid vehicles for St vincent’s pathology, which will improve the hospital’s environmental footprint and save thousands of dollars a year
– time scheduling of air-conditioning systems in non-patient areas
– water saving measures including installation of dual flush toilets in 25 patient areas that underwent renovation.
eMerGency departMent capital workS
In December 2012 capital refurbishments to the emergency Department (eD) were completed, including refurbishment of the fast track clinic, upgrades to cubicles and resuscitation bays and a new diagnostic lounge. With these new physical spaces operational and ongoing redesign initiatives to support improved emergency access performance, it was timely for the eD to review the patient profile, model of care and how to best manage patient flow and emergency access.
With the support of the new Service Improvement and redesign team, a new model that streams patients to four different treatment areas and care teams was developed and implemented.
This model has helped to significantly improve the utilisation of the short stay unit and further performance improvements are anticipated in 2013.
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
19
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
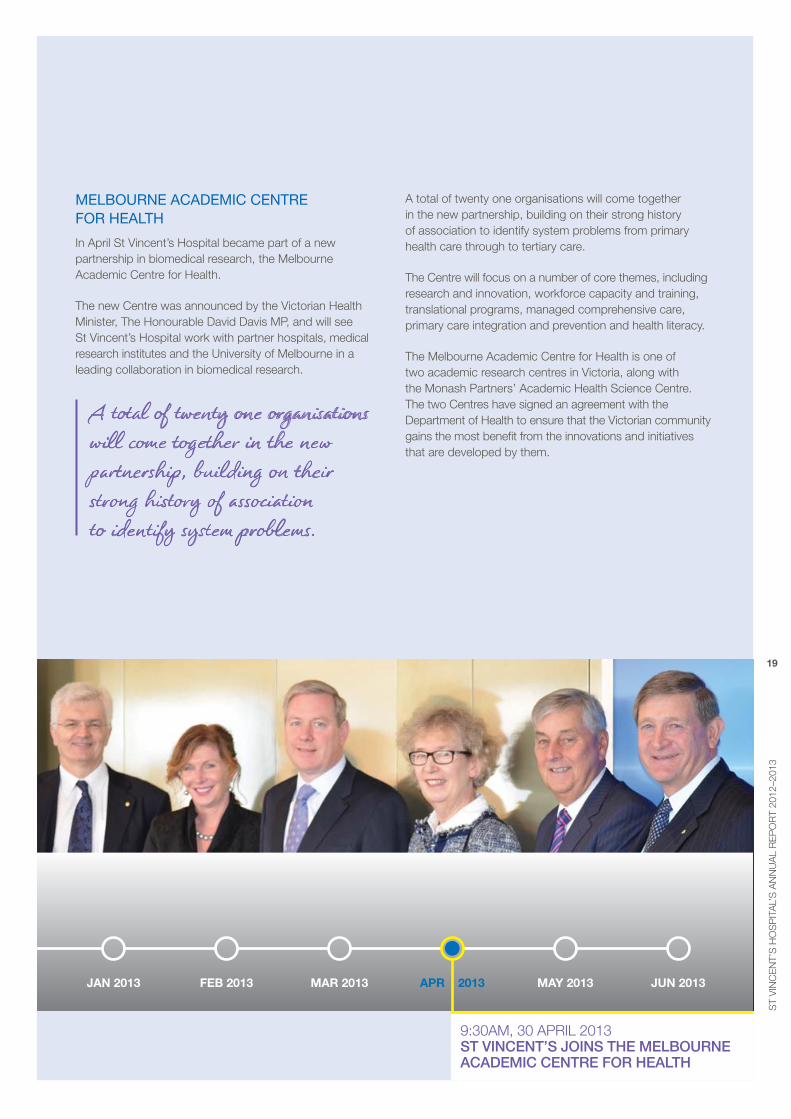
Melbourne acadeMic centre for HealtH
In april St vincent’s Hospital became part of a new partnership in biomedical research, the melbourne academic Centre for Health.
The new Centre was announced by the victorian Health minister, The Honourable David Davis mp, and will see St vincent’s Hospital work with partner hospitals, medical research institutes and the University of melbourne in a leading collaboration in biomedical research.
A total of twenty one organisations will come together in the new partnership, building on their strong history of association to identify system problems.
a total of twenty one organisations will come together in the new partnership, building on their strong history of association to identify system problems from primary health care through to tertiary care.
The Centre will focus on a number of core themes, including research and innovation, workforce capacity and training, translational programs, managed comprehensive care, primary care integration and prevention and health literacy.
The melbourne academic Centre for Health is one of two academic research centres in victoria, along with the monash partners’ academic Health Science Centre. The two Centres have signed an agreement with the Department of Health to ensure that the victorian community gains the most benefit from the innovations and initiatives that are developed by them.
9:30am, 30 aprIL 2013St vInCent’S jOInS the meLBOuRne ACADemIC CentRe FOR heALth
20
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
tHank you to our coMMunity of SupporterS
St vincent’s Foundation expresses our sincere appreciation to all who have contributed over the past twelve months, and would like to particularly acknowledge the following generous donors:
trusts and foundations
$50,000+The Cass Foundation australian Diabetes Society The H & L Hecht Trust
$25,000+The ethel Herman Charitable Trust The edgar Foundation rp medical Fund rowe Family Foundation mazda Foundation Limited Kidney Health australia Frances and Harold abbott Foundation Ian rollo Currie estate Foundation Collier Charitable Fund aNZ Trustees: medical research & Technology In victoria
$10,000+allens arthur robinson equity Trustees: Lynne Quayle Charitable Trust Fund Irene & margaret Stewardson Charitable Trust Stepahead australia Ltd The andrews Foundation
$5,000+The Isobel Hill brown Trust The marian & e H Flack Trust The eirene Lucas Foundation Joe White bequest
Major donors
$200,000+David & Kathy mackintosh The pratt Foundation
$100,000+Fergus ryan
$50,000+Lindsay & paula Fox peter White rotary Club of balwyn
$10,000+Noel o’brien Kerry bradley Simon Quinn brenda Shanahan Dinah Krongold & Family Graduate Nurses association Kathy Kha robert Naughton Lola Cochaud max White victor Khor
$5,000+David J Keath ernest brough Karin macNab Luisa Lay Norman Ham alice vaughan bruce Walker Joseph Cappadona Les Youie order of malta Hospice Home Care (vIC) INC rae & peter Gunn Family Foundation oSK Trustees berhad
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
21
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
corporate, business, Sponsorship
$30,000+LUCrF Super
$20,000+medtronic australasia pty Ltd
$10,000+The pratt Foundation
bequests and estates
$300,000+estate of mary powell
$100,000+estate of Giovanni Librozzi estate of Stella Conway
$50,000+estate of Shirley Webber estate of the Late Francis Ian Jordan
$20,000+estate of Helena Lynch estate of the Late bernard breakspear estate of the Late Louie viner Lunt margery Snowball
$10,000+estate of James robertson Gray estate of John Wolfgang Schnabel estate of Leonie Willett estate of margaret Conway Charitable Trust edith Jean elizabeth beggs Charitable Trust estate of Sally Wykes The William & eileen Walsh Trust estate of Frances Townsend
$5,000+The Late angela Tambasco edith Jean elizabeth beggs Charitable Trust estate of alfred Dehnert estate of Henry Herbert Yoffa estate of muriel bradley The mary macgregor Trust
in Memoriam
pamela Shotton peter & the Late Kim Jansen Karin macNab allyn radford Chris Jablonski
anonymous Gifts
total $1,862,966.29
5.00pm, 25 FebrUarY 2013OpeRA In the mARket
22
Jul 2012 aug 2012 sep 2012 Oct 2012 nOv 2012 dec 2012
report of operationS 2013
year In revIeW
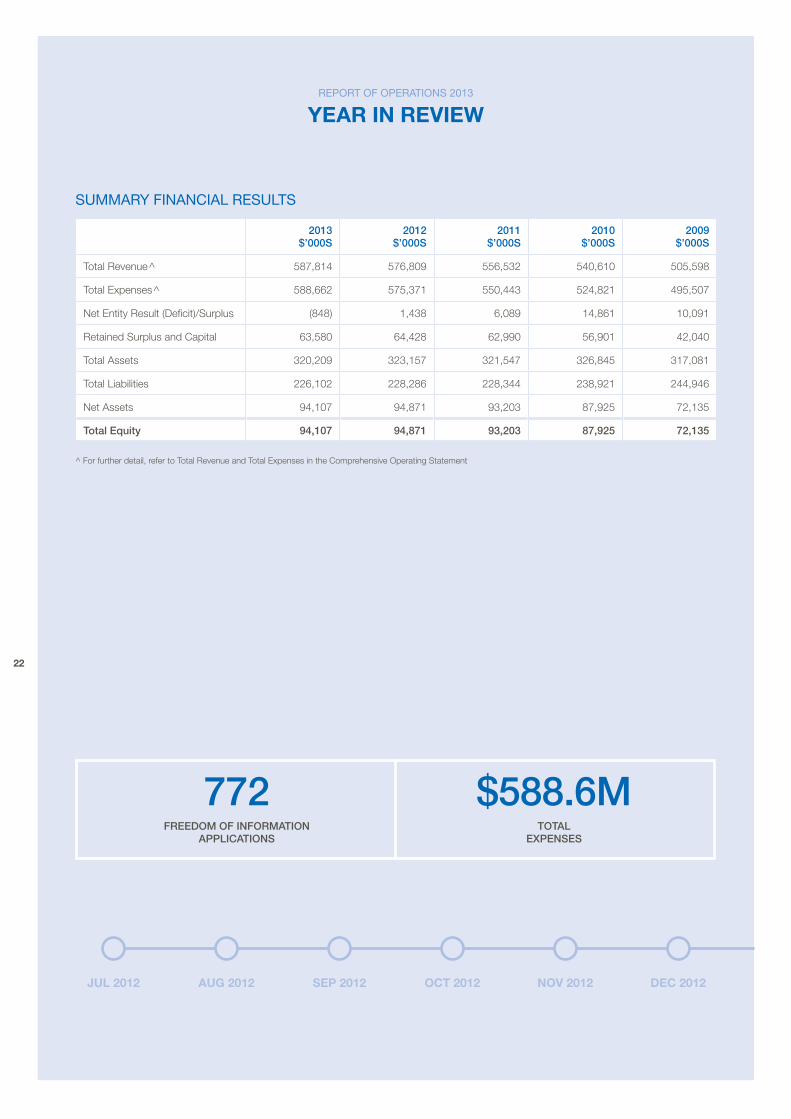
SuMMary financial reSultS
2013 $’000S
2012 $’000S
2011 $’000S
2010 $’000S
2009 $’000S
Total revenue^ 587,814 576,809 556,532 540,610 505,598
Total expenses^ 588,662 575,371 550,443 524,821 495,507
Net entity result (Deficit)/Surplus (848) 1,438 6,089 14,861 10,091
retained Surplus and Capital 63,580 64,428 62,990 56,901 42,040
Total assets 320,209 323,157 321,547 326,845 317,081
Total Liabilities 226,102 228,286 228,344 238,921 244,946
Net assets 94,107 94,871 93,203 87,925 72,135
total equity 94,107 94,871 93,203 87,925 72,135
^ For further detail, refer to Total revenue and Total expenses in the Comprehensive operating Statement
772 $588.6mFReeDOm OF InFORmAtIOn
AppLICAtIOnStOtAL
expenSeS
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
23
SuMMary of SiGnificant cHanGe in financial poSition 2013
There have been no significant changes in the Hospital’s state of affairs during the financial year.
operational and financial perforMance 2013
St vincent’s Hospital (melbourne) Limited delivered an annual operating surplus result of $519,000. after including Capital income and expenses the net entity result was a deficit of $848,000. movement in total equity includes the net equity result and a revaluation adjustment for cultural assets of $84,000 posted to equity.
SubSequent eVentS
There has been no matter or circumstance which has arisen since 30 June 2013 that has significantly affected, or may affect:
a. The operations, in financial years subsequent to 30 June 2013, of St vincent’s Hospital (melbourne) Limited, or
b. The results of those operations, or
c. The state of affairs, in financial years subsequent to 30 June 2013, of St vincent’s Hospital (melbourne).
Jan 2013 feb 2013 mar 2013 apr 2013 may 2013 Jun 2013
10.30am, 27 maY 2013COmmItment tO ReCOnCILIAtIOn
24
report of operationS 2013
year In revIeW
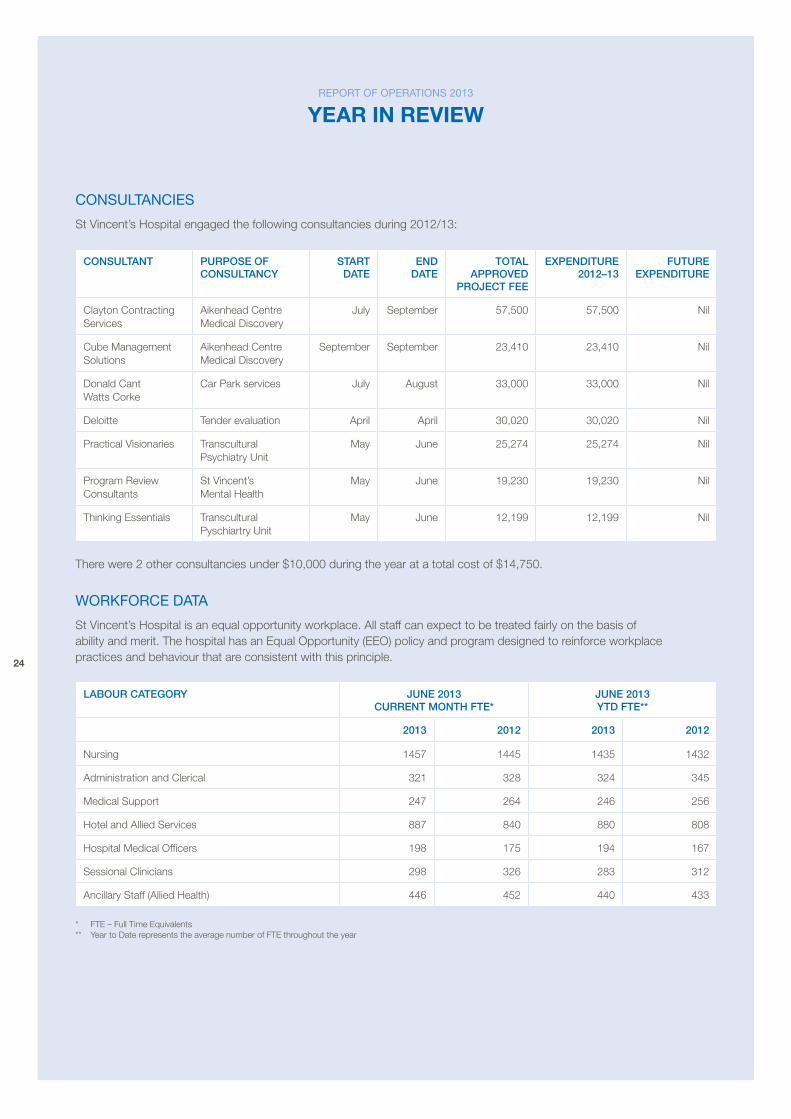
conSultancieS
St vincent’s Hospital engaged the following consultancies during 2012/13:
COnSuLtAnt puRpOSe OF COnSuLtAnCy
StARt DAte
enD DAte
tOtAL AppROveD
pROjeCt Fee
expenDItuRe 2012–13
FutuRe expenDItuRe
Clayton Contracting Services
aikenhead Centre medical Discovery
July September 57,500 57,500 Nil
Cube management Solutions
aikenhead Centre medical Discovery
September September 23,410 23,410 Nil
Donald Cant Watts Corke
Car park services July august 33,000 33,000 Nil
Deloitte Tender evaluation april april 30,020 30,020 Nil
practical visionaries Transcultural psychiatry Unit
may June 25,274 25,274 Nil
program review Consultants
St vincent’s mental Health
may June 19,230 19,230 Nil
Thinking essentials Transcultural pyschiartry Unit
may June 12,199 12,199 Nil
There were 2 other consultancies under $10,000 during the year at a total cost of $14,750.
workforce data
St vincent’s Hospital is an equal opportunity workplace. all staff can expect to be treated fairly on the basis of ability and merit. The hospital has an equal opportunity (eeo) policy and program designed to reinforce workplace practices and behaviour that are consistent with this principle.
LABOuR CAtegORy june 2013 CuRRent mOnth Fte*
june 2013 ytD Fte**
2013 2012 2013 2012
Nursing 1457 1445 1435 1432
administration and Clerical 321 328 324 345
medical Support 247 264 246 256
Hotel and allied Services 887 840 880 808
Hospital medical officers 198 175 194 167
Sessional Clinicians 298 326 283 312
ancillary Staff (allied Health) 446 452 440 433
* FTe – Full Time equivalents ** Year to Date represents the average number of FTe throughout the year
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
25
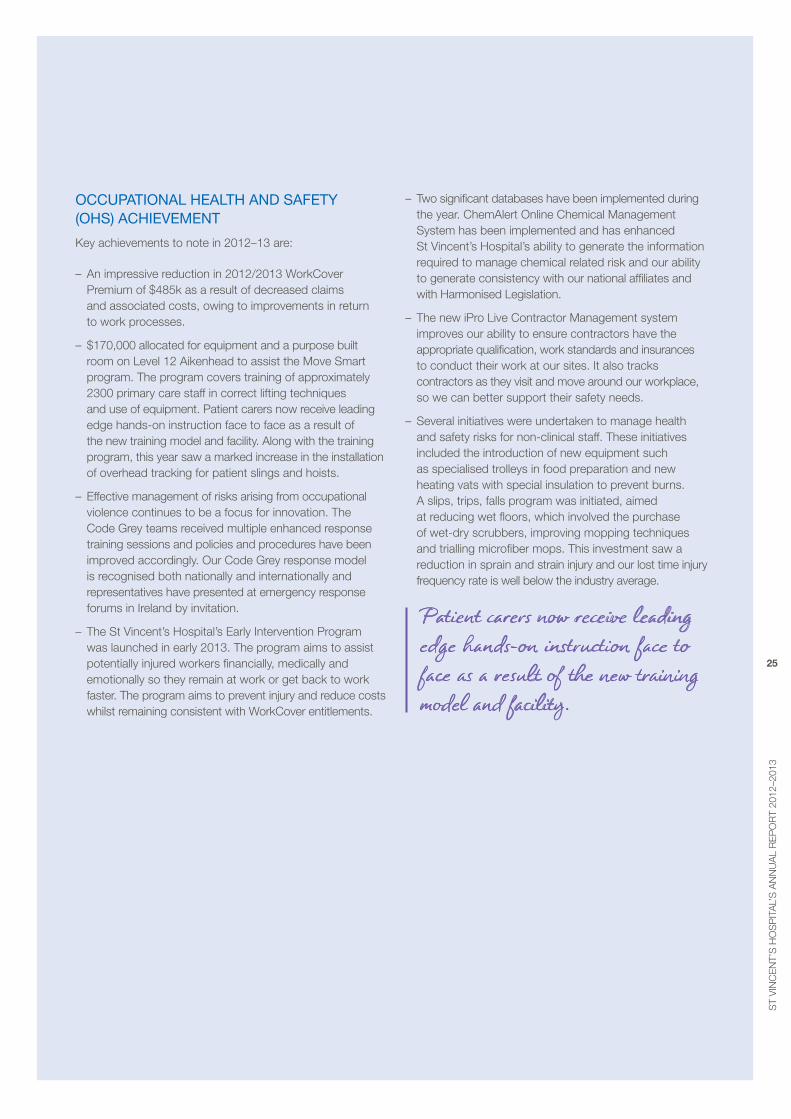
occupational HealtH and Safety (oHS) acHieVeMent
Key achievements to note in 2012–13 are:
– an impressive reduction in 2012/2013 WorkCover premium of $485k as a result of decreased claims and associated costs, owing to improvements in return to work processes.
– $170,000 allocated for equipment and a purpose built room on Level 12 aikenhead to assist the move Smart program. The program covers training of approximately 2300 primary care staff in correct lifting techniques and use of equipment. patient carers now receive leading edge hands-on instruction face to face as a result of the new training model and facility. along with the training program, this year saw a marked increase in the installation of overhead tracking for patient slings and hoists.
– effective management of risks arising from occupational violence continues to be a focus for innovation. The Code Grey teams received multiple enhanced response training sessions and policies and procedures have been improved accordingly. our Code Grey response model is recognised both nationally and internationally and representatives have presented at emergency response forums in Ireland by invitation.
– The St vincent’s Hospital’s early Intervention program was launched in early 2013. The program aims to assist potentially injured workers financially, medically and emotionally so they remain at work or get back to work faster. The program aims to prevent injury and reduce costs whilst remaining consistent with WorkCover entitlements.
– Two significant databases have been implemented during the year. Chemalert online Chemical management System has been implemented and has enhanced St vincent’s Hospital’s ability to generate the information required to manage chemical related risk and our ability to generate consistency with our national affiliates and with Harmonised Legislation.
– The new ipro Live Contractor management system improves our ability to ensure contractors have the appropriate qualification, work standards and insurances to conduct their work at our sites. It also tracks contractors as they visit and move around our workplace, so we can better support their safety needs.
– Several initiatives were undertaken to manage health and safety risks for non-clinical staff. These initiatives included the introduction of new equipment such as specialised trolleys in food preparation and new heating vats with special insulation to prevent burns. a slips, trips, falls program was initiated, aimed at reducing wet floors, which involved the purchase of wet-dry scrubbers, improving mopping techniques and trialling microfiber mops. This investment saw a reduction in sprain and strain injury and our lost time injury frequency rate is well below the industry average.
Patient carers now receive leading edge hands-on instruction face to face as a result of the new training model and facility.
26
report of operationS 2013
year In revIeW
buildinG and Maintenance coMpliance
St vincent’s Hospital complies with mandatory requirements under the building Code of australia (bCa). our building surveyors have conducted quarterly assessments and an annual audit on essential Safety measures during the last 12 months:
– each essential Safety measure is operating at the required level of performance to fulfil its purpose
– where applicable each essential Safety measure has been maintained in accordance with the occupancy permit or maintenance determination and generally fulfils its purpose
– since the last annual essential Safety measure report to the best of our knowledge, there have been no penetrations to required fire resistant construction, smoke curtains and the like, in buildings inspected other than those for which a building permit has been issued.
buildings
St vincent’s Hospital certifies the following compliance with its buildings:
– buildings are certified for approval in accordance with the building Code australia
– works under construction are subject to mandatory inspection
– all buildings receive a certificate of final inspection.
Maintenance
St vincent’s Hospital certifies that there have been no notices issued or orders to cease occupancy in relation to:
– rectification of substandard buildings requiring urgent attention
– all renovations to existing buildings comply with regulations in force at the time of construction
– there have been no orders to cease occupancy.
In 2006 and 2009 three independent reports were commissioned into the state of buildings, infrastructure and services over the Fitzroy, Caritas Christi, St George’s hospitals and other sites. These reports involved a detailed asset condition review which in particular focussed on occupational Health and Safety (oHS), fire and safety, building compliance and environmental. St vincent’s Hospital continues to invest substantial capital to address issues raised.
During the last 12 months St vincent’s Hospital has undertaken rectification projects including progressing the works identified in the Fire and oH&S reports for:
– Fitzroy ($1.6m)
– St Georges Hospital ($0.34m)
– Caritas Christi ($0.25m).
St vincent’s has also committed to a program of works to complete phase 3 and 4 of the Fitzroy Campus asset Condition review. The balance of the rectification works are planned to be addressed over the next four years.
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
27
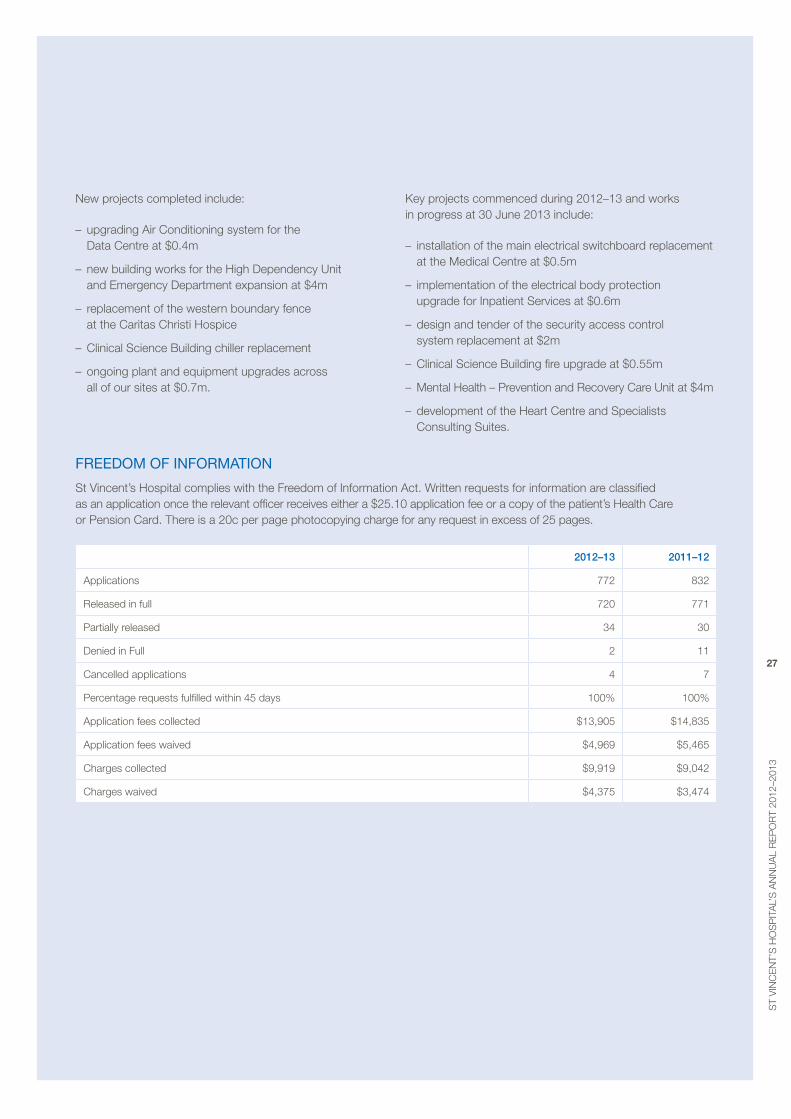
New projects completed include:
– upgrading air Conditioning system for the Data Centre at $0.4m
– new building works for the High Dependency Unit and emergency Department expansion at $4m
– replacement of the western boundary fence at the Caritas Christi Hospice
– Clinical Science building chiller replacement
– ongoing plant and equipment upgrades across all of our sites at $0.7m.
Key projects commenced during 2012–13 and works in progress at 30 June 2013 include:
– installation of the main electrical switchboard replacement at the medical Centre at $0.5m
– implementation of the electrical body protection upgrade for Inpatient Services at $0.6m
– design and tender of the security access control system replacement at $2m
– Clinical Science building fire upgrade at $0.55m
– mental Health – prevention and recovery Care Unit at $4m
– development of the Heart Centre and Specialists Consulting Suites.
freedoM of inforMation
St vincent’s Hospital complies with the Freedom of Information act. Written requests for information are classified as an application once the relevant officer receives either a $25.10 application fee or a copy of the patient’s Health Care or pension Card. There is a 20c per page photocopying charge for any request in excess of 25 pages.
2012–13 2011–12
applications 772 832
released in full 720 771
partially released 34 30
Denied in Full 2 11
Cancelled applications 4 7
percentage requests fulfilled within 45 days 100% 100%
application fees collected $13,905 $14,835
application fees waived $4,969 $5,465
Charges collected $9,919 $9,042
Charges waived $4,375 $3,474
28
report of operationS 2013
statement Of prIOrItIes
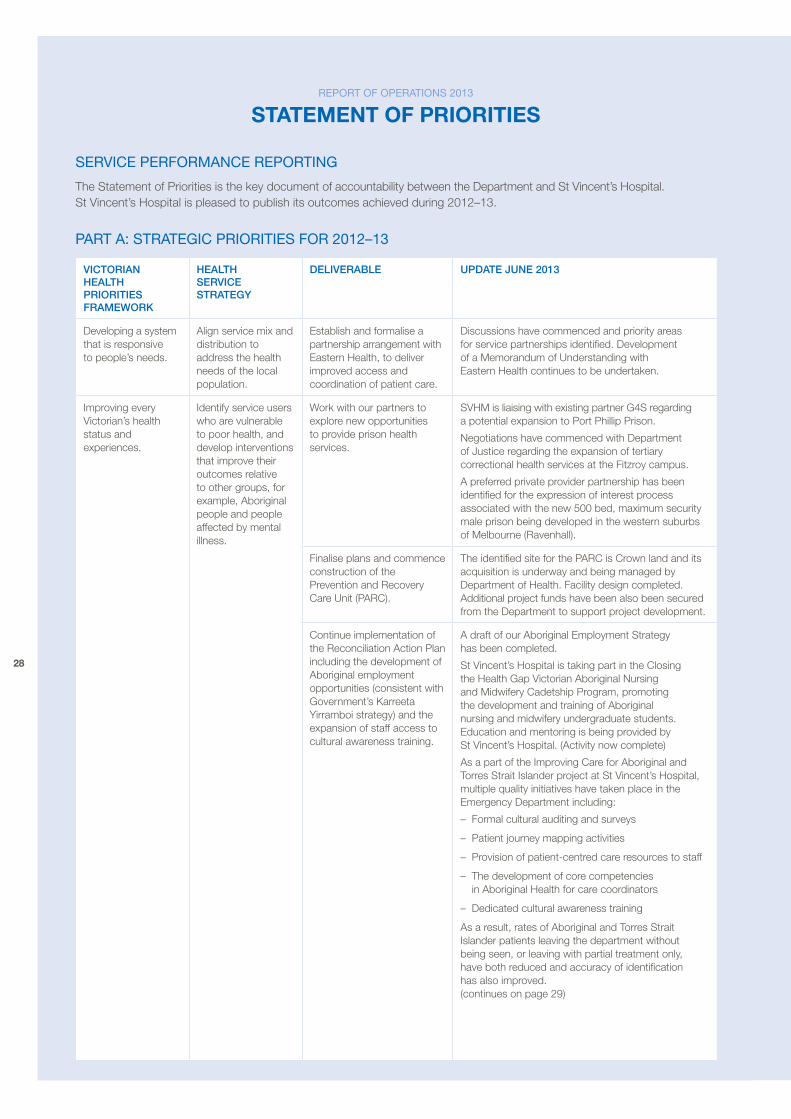
SerVice perforMance reportinG
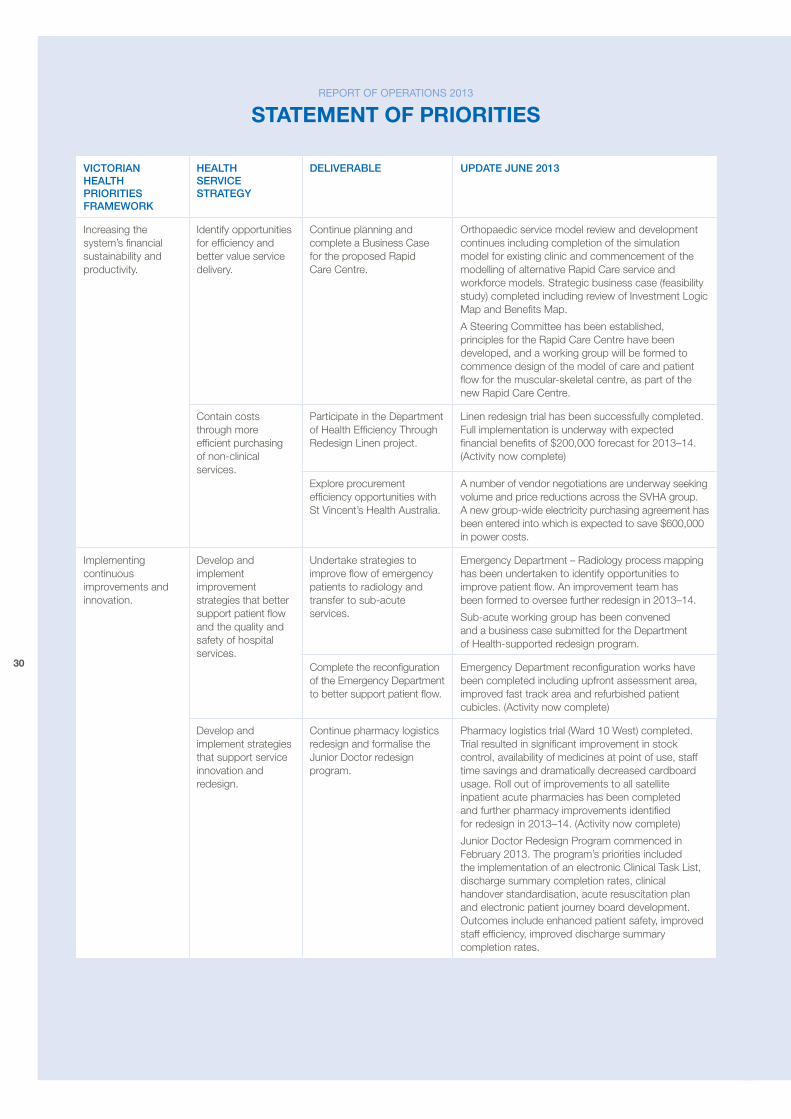
The Statement of priorities is the key document of accountability between the Department and St vincent’s Hospital. St vincent’s Hospital is pleased to publish its outcomes achieved during 2012–13.
part a: StrateGic prioritieS for 2012–13
vICtORIAn heALth pRIORItIeS FRAmewORk
heALth SeRvICe StRAtegy
DeLIveRABLe upDAte june 2013
Developing a system that is responsive to people’s needs.
align service mix and distribution to address the health needs of the local population.
establish and formalise a partnership arrangement with eastern Health, to deliver improved access and coordination of patient care.
Discussions have commenced and priority areas for service partnerships identified. Development of a memorandum of Understanding with eastern Health continues to be undertaken.
Improving every victorian’s health status and experiences.
Identify service users who are vulnerable to poor health, and develop interventions that improve their outcomes relative to other groups, for example, aboriginal people and people affected by mental illness.
Work with our partners to explore new opportunities to provide prison health services.
SvHm is liaising with existing partner G4S regarding a potential expansion to port phillip prison.
Negotiations have commenced with Department of Justice regarding the expansion of tertiary correctional health services at the Fitzroy campus.
a preferred private provider partnership has been identified for the expression of interest process associated with the new 500 bed, maximum security male prison being developed in the western suburbs of melbourne (ravenhall).
Finalise plans and commence construction of the prevention and recovery Care Unit (parC).
The identified site for the parC is Crown land and its acquisition is underway and being managed by Department of Health. Facility design completed. additional project funds have been also been secured from the Department to support project development.
Continue implementation of the reconciliation action plan including the development of aboriginal employment opportunities (consistent with Government’s Karreeta Yirramboi strategy) and the expansion of staff access to cultural awareness training.
a draft of our aboriginal employment Strategy has been completed.
St vincent’s Hospital is taking part in the Closing the Health Gap victorian aboriginal Nursing and midwifery Cadetship program, promoting the development and training of aboriginal nursing and midwifery undergraduate students. education and mentoring is being provided by St vincent’s Hospital. (activity now complete)
as a part of the Improving Care for aboriginal and Torres Strait Islander project at St vincent’s Hospital, multiple quality initiatives have taken place in the emergency Department including:
– Formal cultural auditing and surveys
– patient journey mapping activities
– provision of patient-centred care resources to staff
– The development of core competencies in aboriginal Health for care coordinators
– Dedicated cultural awareness training
as a result, rates of aboriginal and Torres Strait Islander patients leaving the department without being seen, or leaving with partial treatment only, have both reduced and accuracy of identification has also improved. (continues on page 29)
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
29
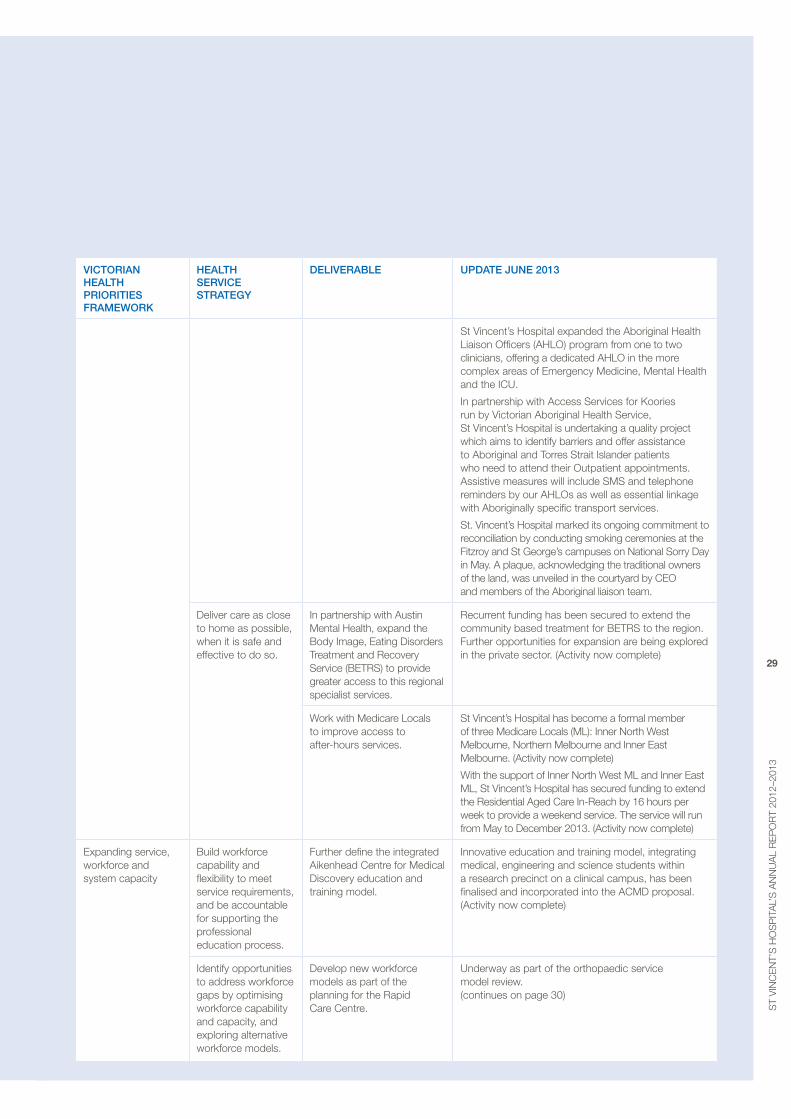
vICtORIAn heALth pRIORItIeS FRAmewORk
heALth SeRvICe StRAtegy
DeLIveRABLe upDAte june 2013
St vincent’s Hospital expanded the aboriginal Health Liaison officers (aHLo) program from one to two clinicians, offering a dedicated aHLo in the more complex areas of emergency medicine, mental Health and the ICU.
In partnership with access Services for Koories run by victorian aboriginal Health Service, St vincent’s Hospital is undertaking a quality project which aims to identify barriers and offer assistance to aboriginal and Torres Strait Islander patients who need to attend their outpatient appointments. assistive measures will include SmS and telephone reminders by our aHLos as well as essential linkage with aboriginally specific transport services.
St. vincent’s Hospital marked its ongoing commitment to reconciliation by conducting smoking ceremonies at the Fitzroy and St George’s campuses on National Sorry Day in may. a plaque, acknowledging the traditional owners of the land, was unveiled in the courtyard by Ceo and members of the aboriginal liaison team.
Deliver care as close to home as possible, when it is safe and effective to do so.
In partnership with austin mental Health, expand the body Image, eating Disorders Treatment and recovery Service (beTrS) to provide greater access to this regional specialist services.
recurrent funding has been secured to extend the community based treatment for beTrS to the region. Further opportunities for expansion are being explored in the private sector. (activity now complete)
Work with medicare Locals to improve access to after-hours services.
St vincent’s Hospital has become a formal member of three medicare Locals (mL): Inner North West melbourne, Northern melbourne and Inner east melbourne. (activity now complete)
With the support of Inner North West mL and Inner east mL, St vincent’s Hospital has secured funding to extend the residential aged Care In-reach by 16 hours per week to provide a weekend service. The service will run from may to December 2013. (activity now complete)
expanding service, workforce and system capacity
build workforce capability and flexibility to meet service requirements, and be accountable for supporting the professional education process.
Further define the integrated aikenhead Centre for medical Discovery education and training model.
Innovative education and training model, integrating medical, engineering and science students within a research precinct on a clinical campus, has been finalised and incorporated into the aCmD proposal. (activity now complete)
Identify opportunities to address workforce gaps by optimising workforce capability and capacity, and exploring alternative workforce models.
Develop new workforce models as part of the planning for the rapid Care Centre.
Underway as part of the orthopaedic service model review. (continues on page 30)
30
report of operationS 2013
statement Of prIOrItIes
vICtORIAn heALth pRIORItIeS FRAmewORk
heALth SeRvICe StRAtegy
DeLIveRABLe upDAte june 2013
Increasing the system’s financial sustainability and productivity.
Identify opportunities for efficiency and better value service delivery.
Continue planning and complete a business Case for the proposed rapid Care Centre.
orthopaedic service model review and development continues including completion of the simulation model for existing clinic and commencement of the modelling of alternative rapid Care service and workforce models. Strategic business case (feasibility study) completed including review of Investment Logic map and benefits map.
a Steering Committee has been established, principles for the rapid Care Centre have been developed, and a working group will be formed to commence design of the model of care and patient flow for the muscular-skeletal centre, as part of the new rapid Care Centre.
Contain costs through more efficient purchasing of non-clinical services.
participate in the Department of Health efficiency Through redesign Linen project.
Linen redesign trial has been successfully completed. Full implementation is underway with expected financial benefits of $200,000 forecast for 2013–14. (activity now complete)
explore procurement efficiency opportunities with St vincent’s Health australia.
a number of vendor negotiations are underway seeking volume and price reductions across the SvHa group. a new group-wide electricity purchasing agreement has been entered into which is expected to save $600,000 in power costs.
Implementing continuous improvements and innovation.
Develop and implement improvement strategies that better support patient flow and the quality and safety of hospital services.
Undertake strategies to improve flow of emergency patients to radiology and transfer to sub-acute services.
emergency Department – radiology process mapping has been undertaken to identify opportunities to improve patient flow. an improvement team has been formed to oversee further redesign in 2013–14.
Sub-acute working group has been convened and a business case submitted for the Department of Health-supported redesign program.
Complete the reconfiguration of the emergency Department to better support patient flow.
emergency Department reconfiguration works have been completed including upfront assessment area, improved fast track area and refurbished patient cubicles. (activity now complete)
Develop and implement strategies that support service innovation and redesign.
Continue pharmacy logistics redesign and formalise the Junior Doctor redesign program.
pharmacy logistics trial (Ward 10 West) completed. Trial resulted in significant improvement in stock control, availability of medicines at point of use, staff time savings and dramatically decreased cardboard usage. roll out of improvements to all satellite inpatient acute pharmacies has been completed and further pharmacy improvements identified for redesign in 2013–14. (activity now complete)
Junior Doctor redesign program commenced in February 2013. The program’s priorities included the implementation of an electronic Clinical Task List, discharge summary completion rates, clinical handover standardisation, acute resuscitation plan and electronic patient journey board development. outcomes include enhanced patient safety, improved staff efficiency, improved discharge summary completion rates.
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
31
vICtORIAn heALth pRIORItIeS FRAmewORk
heALth SeRvICe StRAtegy
DeLIveRABLe upDAte june 2013
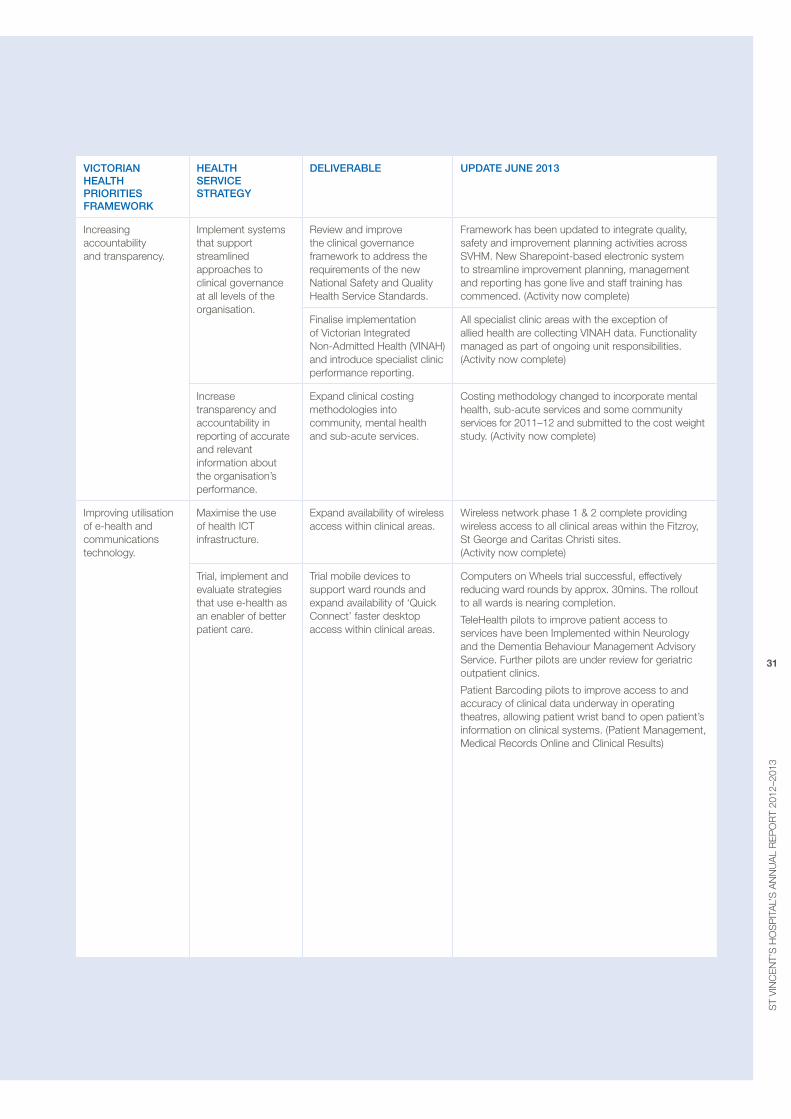
Increasing accountability and transparency.
Implement systems that support streamlined approaches to clinical governance at all levels of the organisation.
review and improve the clinical governance framework to address the requirements of the new National Safety and Quality Health Service Standards.
Framework has been updated to integrate quality, safety and improvement planning activities across SvHm. New Sharepoint-based electronic system to streamline improvement planning, management and reporting has gone live and staff training has commenced. (activity now complete)
Finalise implementation of victorian Integrated Non-admitted Health (vINaH) and introduce specialist clinic performance reporting.
all specialist clinic areas with the exception of allied health are collecting vINaH data. Functionality managed as part of ongoing unit responsibilities. (activity now complete)
Increase transparency and accountability in reporting of accurate and relevant information about the organisation’s performance.
expand clinical costing methodologies into community, mental health and sub-acute services.
Costing methodology changed to incorporate mental health, sub-acute services and some community services for 2011–12 and submitted to the cost weight study. (activity now complete)
Improving utilisation of e-health and communications technology.
maximise the use of health ICT infrastructure.
expand availability of wireless access within clinical areas.
Wireless network phase 1 & 2 complete providing wireless access to all clinical areas within the Fitzroy, St George and Caritas Christi sites. (activity now complete)
Trial, implement and evaluate strategies that use e-health as an enabler of better patient care.
Trial mobile devices to support ward rounds and expand availability of ‘Quick Connect’ faster desktop access within clinical areas.
Computers on Wheels trial successful, effectively reducing ward rounds by approx. 30mins. The rollout to all wards is nearing completion.
TeleHealth pilots to improve patient access to services have been Implemented within Neurology and the Dementia behaviour management advisory Service. Further pilots are under review for geriatric outpatient clinics.
patient barcoding pilots to improve access to and accuracy of clinical data underway in operating theatres, allowing patient wrist band to open patient’s information on clinical systems. (patient management, medical records online and Clinical results)
32
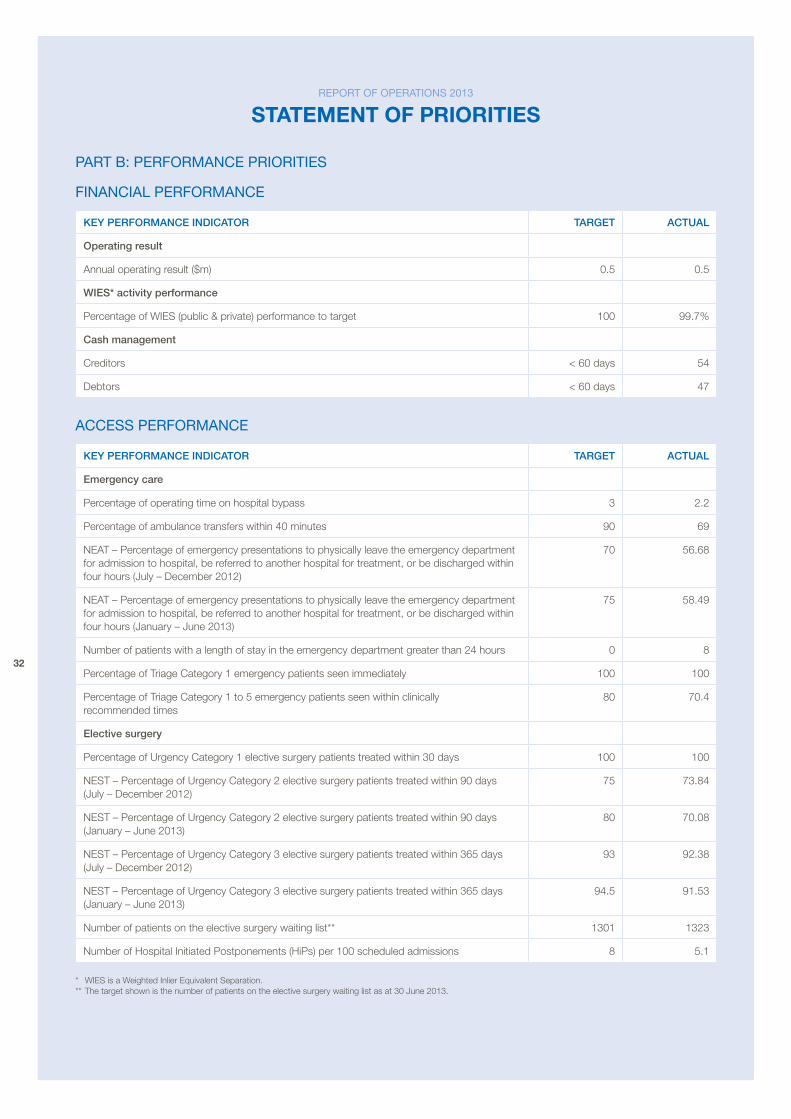
part b: perforMance prioritieS
financial perforMance
key peRFORmAnCe InDICAtOR tARget ACtuAL
Operating result
annual operating result ($m) 0.5 0.5
wIeS* activity performance
percentage of WIeS (public & private) performance to target 100 99.7%
Cash management
Creditors < 60 days 54
Debtors < 60 days 47
acceSS perforMance
key peRFORmAnCe InDICAtOR tARget ACtuAL
emergency care
percentage of operating time on hospital bypass 3 2.2
percentage of ambulance transfers within 40 minutes 90 69
NeaT – percentage of emergency presentations to physically leave the emergency department for admission to hospital, be referred to another hospital for treatment, or be discharged within four hours (July – December 2012)
70 56.68
NeaT – percentage of emergency presentations to physically leave the emergency department for admission to hospital, be referred to another hospital for treatment, or be discharged within four hours (January – June 2013)
75 58.49
Number of patients with a length of stay in the emergency department greater than 24 hours 0 8
percentage of Triage Category 1 emergency patients seen immediately 100 100
percentage of Triage Category 1 to 5 emergency patients seen within clinically recommended times
80 70.4
elective surgery
percentage of Urgency Category 1 elective surgery patients treated within 30 days 100 100
NeST – percentage of Urgency Category 2 elective surgery patients treated within 90 days (July – December 2012)
75 73.84
NeST – percentage of Urgency Category 2 elective surgery patients treated within 90 days (January – June 2013)
80 70.08
NeST – percentage of Urgency Category 3 elective surgery patients treated within 365 days (July – December 2012)
93 92.38
NeST – percentage of Urgency Category 3 elective surgery patients treated within 365 days (January – June 2013)
94.5 91.53
Number of patients on the elective surgery waiting list** 1301 1323
Number of Hospital Initiated postponements (Hips) per 100 scheduled admissions 8 5.1
* WIeS is a Weighted Inlier equivalent Separation. ** The target shown is the number of patients on the elective surgery waiting list as at 30 June 2013.
report of operationS 2013
statement Of prIOrItIes
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
33
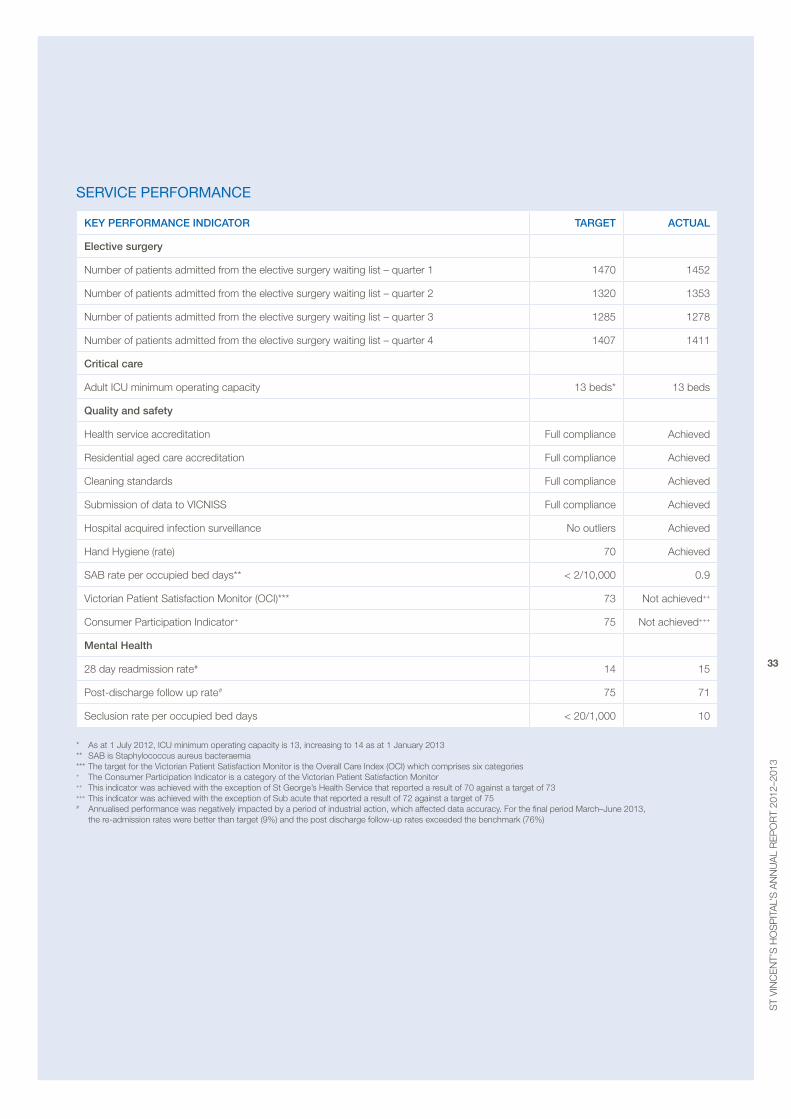
Service performance
Key performance indicator target actual
elective surgery
Number of patients admitted from the elective surgery waiting list – quarter 1 1470 1452
Number of patients admitted from the elective surgery waiting list – quarter 2 1320 1353
Number of patients admitted from the elective surgery waiting list – quarter 3 1285 1278
Number of patients admitted from the elective surgery waiting list – quarter 4 1407 1411
critical care
adult ICU minimum operating capacity 13 beds* 13 beds
Quality and safety
Health service accreditation Full compliance achieved
Residential aged care accreditation Full compliance achieved
Cleaning standards Full compliance achieved
Submission of data to VICNISS Full compliance achieved
Hospital acquired infection surveillance No outliers achieved
Hand Hygiene (rate) 70 achieved
SaB rate per occupied bed days** < 2/10,000 0.9
Victorian patient Satisfaction Monitor (oCI)*** 73 Not achieved++
Consumer participation Indicator+ 75 Not achieved+++
mental Health
28 day readmission rate# 14 15
post-discharge follow up rate# 75 71
Seclusion rate per occupied bed days < 20/1,000 10
* as at 1 July 2012, ICU minimum operating capacity is 13, increasing to 14 as at 1 January 2013 ** SaB is Staphylococcus aureus bacteraemia *** The target for the Victorian patient Satisfaction Monitor is the overall Care Index (oCI) which comprises six categories + The Consumer participation Indicator is a category of the Victorian patient Satisfaction Monitor ++ This indicator was achieved with the exception of St George’s Health Service that reported a result of 70 against a target of 73 +++ This indicator was achieved with the exception of Sub acute that reported a result of 72 against a target of 75 # annualised performance was negatively impacted by a period of industrial action, which affected data accuracy. For the final period March–June 2013,
the re-admission rates were better than target (9%) and the post discharge follow-up rates exceeded the benchmark (76%)
34
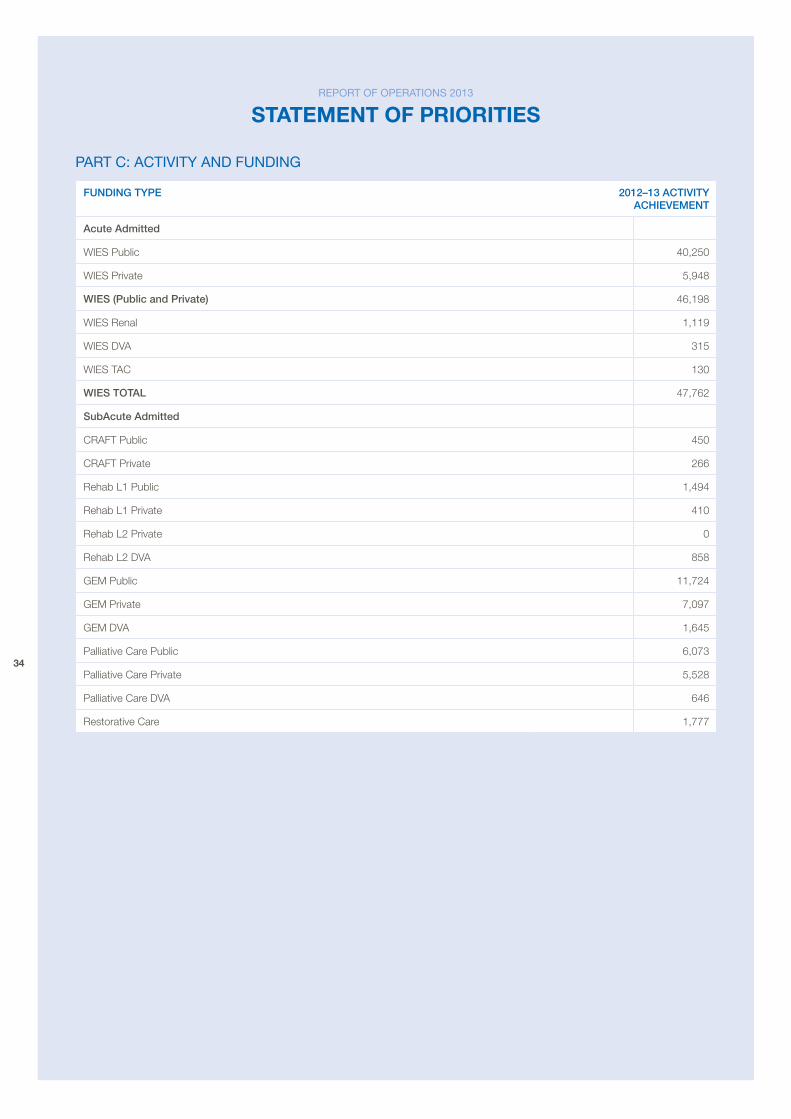
part c: actiVity and fundinG
FunDIng type 2012–13 ACtIvIty AChIevement
Acute Admitted
WIeS public 40,250
WIeS private 5,948
wIeS (public and private) 46,198
WIeS renal 1,119
WIeS Dva 315
WIeS TaC 130
wIeS tOtAL 47,762
SubAcute Admitted
CraFT public 450
CraFT private 266
rehab L1 public 1,494
rehab L1 private 410
rehab L2 private 0
rehab L2 Dva 858
Gem public 11,724
Gem private 7,097
Gem Dva 1,645
palliative Care public 6,073
palliative Care private 5,528
palliative Care Dva 646
restorative Care 1,777
report of operationS 2013
statement Of prIOrItIes
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
35
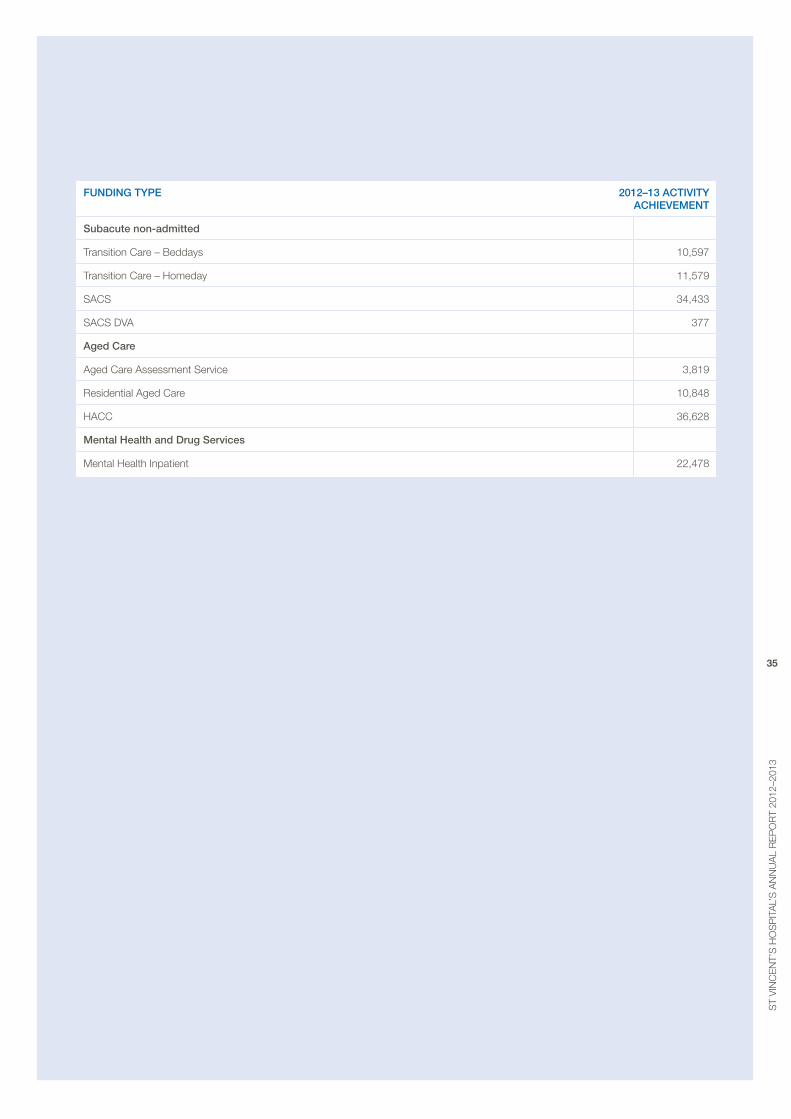
FunDIng type 2012–13 ACtIvIty AChIevement
Subacute non-admitted
Transition Care – beddays 10,597
Transition Care – Homeday 11,579
SaCS 34,433
SaCS Dva 377
Aged Care
aged Care assessment Service 3,819
residential aged Care 10,848
HaCC 36,628
mental health and Drug Services
mental Health Inpatient 22,478
36
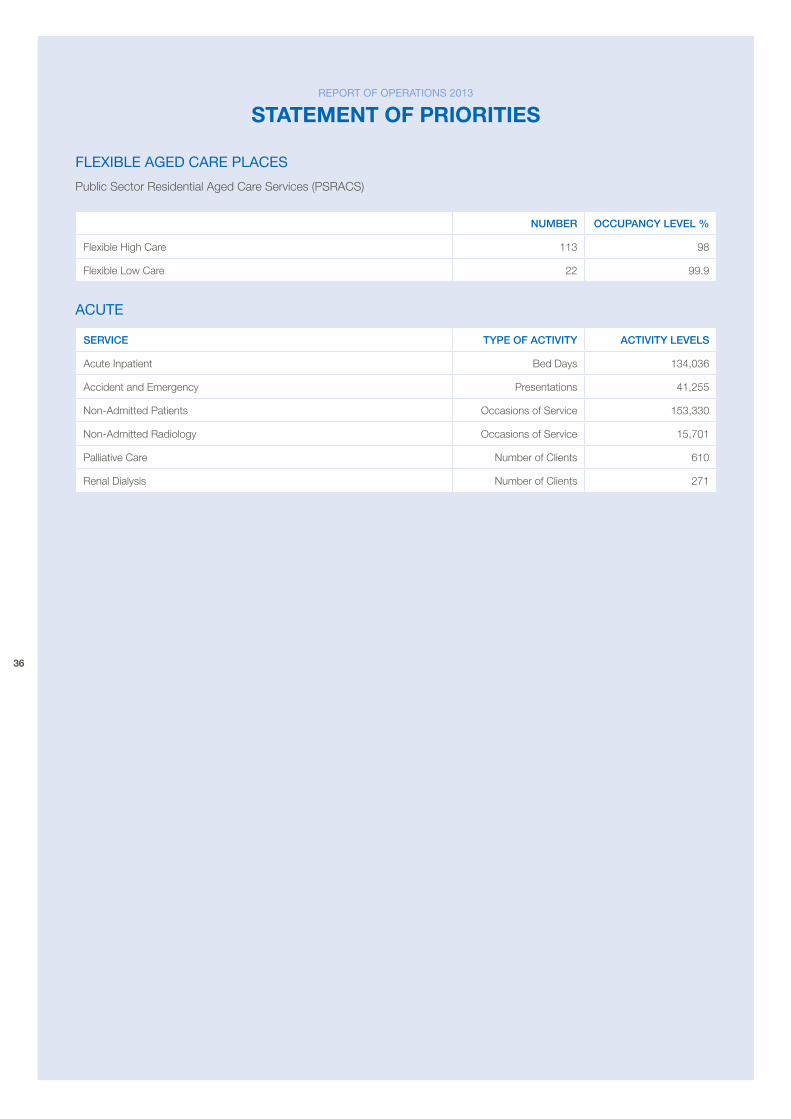
flexible aGed care placeS
public Sector residential aged Care Services (pSraCS)
numBeR OCCupAnCy LeveL %
Flexible High Care 113 98
Flexible Low Care 22 99.9
acute
SeRvICe type OF ACtIvIty ACtIvIty LeveLS
acute Inpatient bed Days 134,036
accident and emergency presentations 41,255
Non-admitted patients occasions of Service 153,330
Non-admitted radiology occasions of Service 15,701
palliative Care Number of Clients 610
renal Dialysis Number of Clients 271
report of operationS 2013
statement Of prIOrItIes
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
37
atteStation on data accuracy
I, patricia o’rourke, certify that St vincent’s Hospital (melbourne) Limited has put in place appropriate internal controls and processes to ensure that reported data reasonably reflects actual performance. St vincent’s Hospital (melbourne) Limited has critically reviewed these controls and processes during the year.
atteStation for coMpliance witH tHe MiniSterial StandinG direction 4.5.5.1 – inSurance
I, patricia o’rourke certify that St vincent’s Hospital (melbourne) Limited has complied with ministerial Direction 4.5.5.1 – Insurance, with the exception of completion of the register of indemnities for all contracts which remains in preparation.
atteStation on coMpliance witH auStralian/new Zealand riSk ManaGeMent Standard
I, patricia o’rourke certify that St vincent’s Hospital (melbourne) Limited has risk management processes in place consistent with the aS/NZS ISo 31000:2009 (or an equivalent designated standard) and an internal control system is in place that enables the executive to understand, manage and satisfactorily control risk exposures. The audit and risk Committee verifies this assurance and that the risk profile of St vincent’s Hospital (melbourne) Limited has been critically reviewed within the last 12 months.
professor patricia o’rourke Chief executive officer St vincent’s Hospital (melbourne) Limited Dated 26th august 2013
report aVailability
This report is readily available to members of parliament and the public on the St vincent’s Hospital’s website at www.svhm.org.au or by calling the office of the Ceo on 03 9288 3938 to request a copy.
38
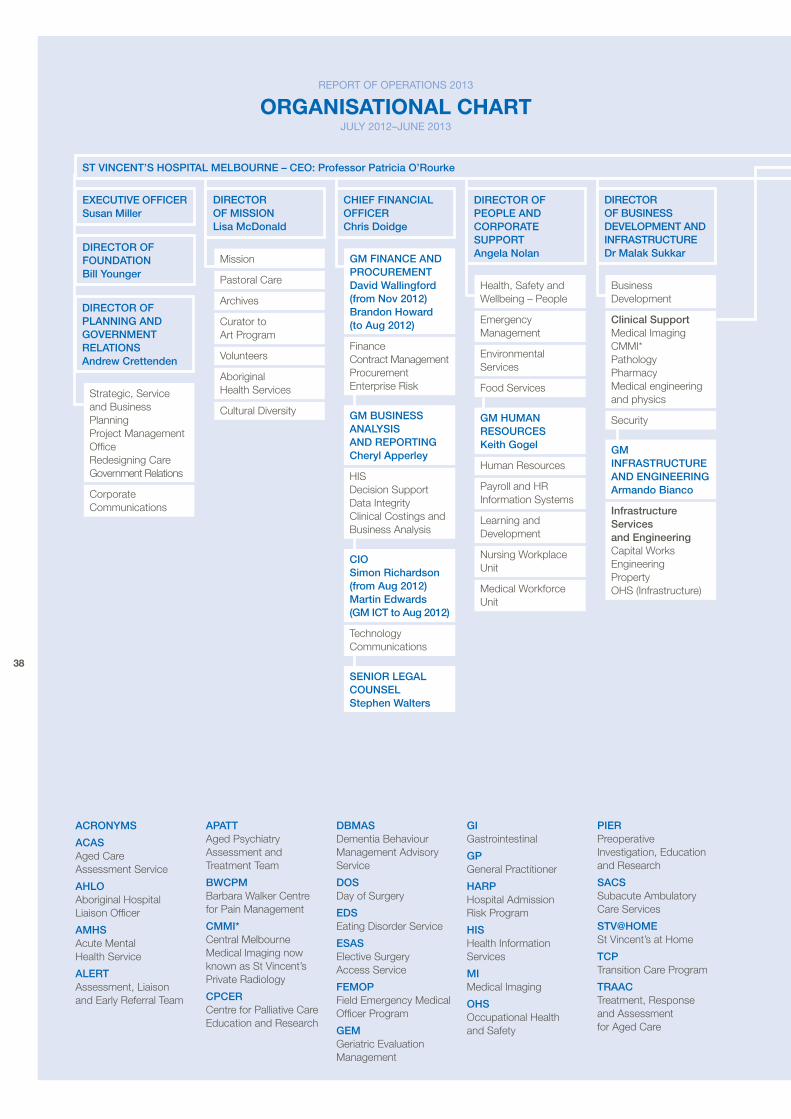
mission
pastoral Care
archives
Curator to art program
volunteers
aboriginal Health Services
Cultural Diversity
gm FInAnCe AnD pROCuRementDavid wallingford (from nov 2012) Brandon howard (to Aug 2012)
Finance Contract managementprocuremententerprise risk
Health, Safety and Wellbeing – people
emergency management
environmental Services
Food Services
business Development
Clinical Supportmedical ImagingCmmI*pathologypharmacymedical engineering and physics
Securitygm humAn ReSOuRCeSkeith gogel
Human resources
payroll and Hr Information Systems
Learning and Development
Nursing Workplace Unit
medical Workforce Unit
gm InFRAStRuCtuRe AnD engIneeRIngArmando Bianco
Infrastructure Services and engineeringCapital Worksengineering property oHS (Infrastructure)
gm BuSIneSS AnALySIS AnD RepORtIngCheryl Apperley
HISDecision SupportData Integrity Clinical Costings and business analysis
CIOSimon Richardson (from Aug 2012) martin edwards (gm ICt to Aug 2012)
Technology Communications
Strategic, Service and business planning project management office redesigning Care Government relations
Corporate Communications
DIReCtOR OF mISSIOn Lisa mcDonald
ChIeF FInAnCIAL OFFICeR Chris Doidge
DIReCtOR OF peOpLe AnD CORpORAte SuppORt Angela nolan
DIReCtOR OF BuSIneSS DeveLOpment AnD InFRAStRuCtuRe Dr malak Sukkar
exeCutIve OFFICeR Susan miller
DIReCtOR OF FOunDAtIOn Bill younger
DIReCtOR OF pLAnnIng AnD gOveRnment ReLAtIOnS Andrew Crettenden
ACROnymS
ACAS aged Care assessment Service
AhLO aboriginal Hospital Liaison officer
AmhS acute mental Health Service
ALeRtassessment, Liaison and early referral Team
ApAtt aged psychiatry assessment and Treatment Team
BwCpm barbara Walker Centre for pain management
CmmI* Central melbourne medical Imaging now known as St vincent’s private radiology
CpCeR Centre for palliative Care education and research
DBmAS Dementia behaviour management advisory Service
DOS Day of Surgery
eDS eating Disorder Service
eSAS elective Surgery access Service
FemOp Field emergency medical officer program
gem Geriatric evaluation management
gI Gastrointestinal
gp General practitioner
hARp Hospital admission risk program
hIS Health Information Services
mI medical Imaging
OhS occupational Health and Safety
pIeRpreoperative Investigation, education and research
SACS Subacute ambulatory Care Services
Stv@hOmeSt vincent’s at Home
tCp Transition Care program
tRAACTreatment, response and assessment for aged Care
SenIOR LegAL COunSeLStephen walters
report of operationS 2013
OrganIsatIOnal chart July 2012–June 2013
St vInCent’S hOSpItAL meLBOuRne – CeO: professor patricia O’Rourke
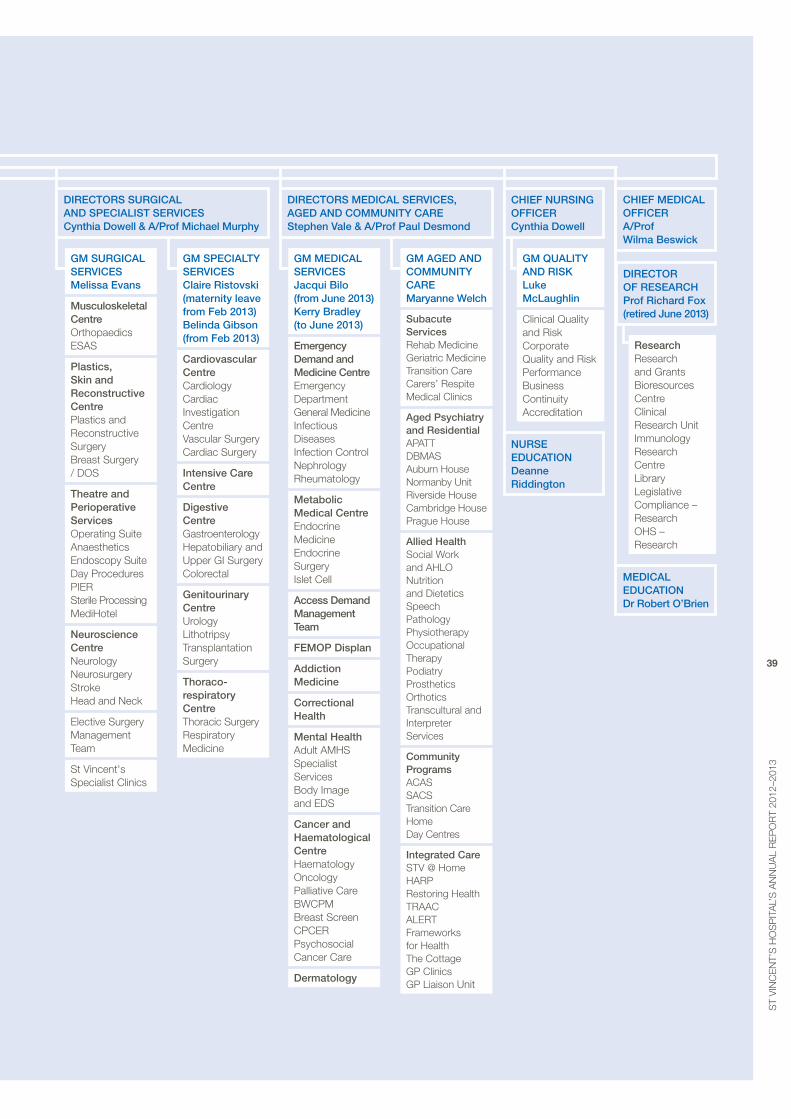
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
39
gm SuRgICAL SeRvICeSmelissa evans
musculoskeletal Centreorthopaedics eSaS
plastics, Skin and Reconstructive Centreplastics and reconstructive Surgerybreast Surgery / DoS
theatre and perioperative Servicesoperating Suiteanaesthetics endoscopy SuiteDay procedures pIerSterile processingmediHotel
neuroscience CentreNeurologyNeurosurgeryStrokeHead and Neck
elective Surgerymanagement Team
St vincent's Specialist Clinics
gm SpeCIALty SeRvICeSClaire Ristovski (maternity leave from Feb 2013) Belinda gibson (from Feb 2013)
Cardiovascular CentreCardiologyCardiac Investigation Centrevascular SurgeryCardiac Surgery
Intensive Care Centre
Digestive CentreGastroenterologyHepatobiliary and Upper GI SurgeryColorectal
genitourinary CentreUrologyLithotripsyTransplantation Surgery
thoraco-respiratory CentreThoracic Surgeryrespiratory medicine
Researchresearch and Grantsbioresources Centre Clinical research UnitImmunologyresearch Centre LibraryLegislative Compliance – researchoHS – research
gm AgeD AnD COmmunIty CARemaryanne welch
Subacute Servicesrehab medicineGeriatric medicineTransition CareCarers’ respitemedical Clinics
Aged psychiatry and ResidentialapaTT DbmaSauburn HouseNormanby Unitriverside HouseCambridge Houseprague House
Allied healthSocial Work and aHLoNutrition and DieteticsSpeech pathologyphysiotherapyoccupationalTherapypodiatryprosthetics orthoticsTranscultural and Interpreter Services
Community programsaCaSSaCSTransition Care HomeDay Centres
Integrated CareSTv @ HomeHarprestoring HealthTraaCaLerTFrameworks for HealthThe CottageGp ClinicsGp Liaison Unit
gm meDICAL SeRvICeSjacqui Bilo (from june 2013) kerry Bradley (to june 2013)
emergency Demand and medicine Centreemergency DepartmentGeneral medicineInfectious DiseasesInfection ControlNephrologyrheumatology
metabolic medical Centreendocrine medicineendocrine SurgeryIslet Cell
Access Demand management team
FemOp Displan
Addiction medicine
Correctional health
mental healthadult amHSSpecialist Servicesbody Image and eDS
Cancer and haematological CentreHaematology oncologypalliative Care bWCpmbreast Screen CpCerpsychosocial Cancer Care
Dermatology
gm QuALIty AnD RISkLuke mcLaughlin
Clinical Quality and riskCorporate Quality and riskperformance business Continuityaccreditation
ChIeF meDICAL OFFICeR A/prof wilma Beswick
St vInCent’S hOSpItAL meLBOuRne – CeO: professor patricia O’Rourke
DIReCtORS SuRgICAL AnD SpeCIALISt SeRvICeS Cynthia Dowell & A/prof michael murphy
DIReCtORS meDICAL SeRvICeS, AgeD AnD COmmunIty CARe Stephen vale & A/prof paul Desmond
nuRSe eDuCAtIOn Deanne Riddington
ChIeF nuRSIng OFFICeR Cynthia Dowell
meDICAL eDuCAtIOn Dr Robert O’Brien
DIReCtOR OF ReSeARCh prof Richard Fox (retired june 2013)
40
FInAnCIALS 2012–2013
contentS
company directory page 41
directors’ report page 42
accountable officer’s and directors’ declaration page 49
comprehensive operating Statement year ended 30 June 2013 page 53
Statement of financial position as at 30 June 2013 page 54
Statement of changes in equity year ended 30 June 2013 page 55
cash flow Statement year ended 30 June 2013 page 56
notes to and forming part of the financial Statements page 57
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
41
directorS
St vincent’s Hospital melbourne is part of the St vincent’s Health australia Limited group (‘SvHa’).
SvHa is australia’s largest not-for-profit, non-government healthcare provider and is led by board Chair mr paul robertson am and SvHa Chief executive officer Dr Tracey batten. as well as St vincent’s Hospital melbourne, SvHa comprises a number of health entities that are either operated solely by SvHa or in partnership with other Congregations.
During the period 1 July 2012 to 30 June 2013, the Trustees of mary aikenhead ministries made all appointments and reappointments to the St vincent’s Health australia board. The following persons were Directors of SvHa during the period 1 July 2012 to 30 June 2013:
mr John Gurry (resigned as Chair & board member 5 october 2012)
mr paul robertson am (appointed board Chair 5 october 2012)
Fr Frank brennan SJ ao
Sr maryanne Confoy rSC
professor Suzanne Crowe am (appointed 1 January 2013)
mr brendan earle
ms patricia Faulkner ao
mr Gary Humphrys
ms belinda Hutchinson am
mr paul mcClintock ao (appointed 1 January 2013)
professor peter Smith
mr Greg Sword am (resigned 5 october 2012)
Sr maureen Walters rSC (resigned 1 august 2013)
Secretary
mr robert beetson
chief executive officer
professor patricia o’rourke
registered office
Level 1 75 Grafton Street bondi Junction NSW 2022
auditor
UHY Haines Norton as agent of the victorian auditor General’s office
Solicitors
middletons Lawyers
bankers
australia and New Zealand banking Group Limited
National australia bank Limited
ultimate parent
St vincent’s Hospital (melbourne) Limited (the ‘Company’) is a public company limited by guarantee. The sole member of the company is St vincent’s Health australia Limited. The ultimate controlling entity of the Hospital is the Trustees of mary aikenhead ministries.
2012–2013 financial StateMentS
cOmpany dIrectOry
42
The Directors present their report on the Hospital for the financial year ended 30 June 2013. The financial statements have been prepared pursuant to the provisions of the Corporations Act 2001 (Cth) and the Financial Management Act 1994 (vic) with the exception of the application of FrD103D Non-Current physical assets and FrD114a Financial Instruments.
Mr John Gurryappointed 1 october 2010 appointed Chair 1 october 2010 resigned 5 october 2012
mr Gurry has a long and distinguished history with St vincent’s Hospital practicing as a vascular surgeon at both St vincent’s Hospital and St vincent’s & mercy private Hospital in melbourne for many years. mr Gurry is a former Director of St vincent’s Institute of medical research, and has held a number of senior roles at St vincent’s Hospital melbourne as Director of vascular Surgery, Chair of the Senior medical Staff association, member of the medical executive Committee and medical Consultative Committee. He is also the former president of the australian and New Zealand Society for vascular Surgery and served as a member of the executive Council of that society for over ten years. mr Gurry is a Fellow of the royal australasian College of Surgeons, a Fellow of the royal College of Surgeons of england, and a Fellow of the american College of Surgeons.
Mr paul robertson aMappointed 1 october 2010 appointed SvHa board Chair 5 october 2012
mr robertson has extensive experience in banking, finance and risk management. He has previously been a Director of austraclear Ltd and Sydney Futures exchange Clearing House. He is currently Chair of Social ventures australia, Chair of St Ignatius College riverview, a Trustee of St vincent’s Hospital Sydney, and founder and Director of the Financial markets Foundation for Children.
fr frank brennan SJ aoappointed 1 october 2010
a Jesuit priest and professor of Law at the australian Catholic University, Fr brennan also holds positions as adjunct professor at the australian National University College of Law and National Centre for Indigenous Studies. Fr brennan is a well-respected advocate for social justice, law and human rights in the australian community. Fr brennan is the current advocate in residence for the Society of St vincent de paul, Catholic Health australia and Catholic Social Services australia. In 2009, he chaired the australian National Human rights Consultation Committee. His many publications include acting on Conscience: How can we responsibly mix law, religion and politics?; Tampering with asylum: a universal humanitarian problem; The Wik Debate: The case for aborigines, pastoralists and miners; Legislating Liberty: a bill of rights for australia; one Land, one Nation: mabo toward 2001; Sharing the Country; Land rights Queensland style: The struggle for aboriginal self-management; and Too much order with too little law.
Sr Maryanne confoy rScappointed 6 February 2012
a Sister of Charity, Dr Confoy is professor of Spirituality and practical Theology at the Jesuit Theological College and United Faculty of Theology, past president of the United Faculty of Theology, melbourne, and a Fellow of the mCD University of Divinity. Dr Confoy has previously served as associate Dean of postgraduate Studies melbourne College of Divinity, and visiting professor at the School of Theology and ministry at boston College, USa.
publications include articles on spirituality and ministry, a biography of morris West, books on spirituality and the contemplative life, priesthood, religious life and Christian ministry, and her most recent is, “Communities visible and Invisible in oceania: Women and HIv: aids,” in Calling for Justice throughout the World: Catholic Women Theologians on the HIv: aIDS pandemic. Dr Confoy has been book review editor of pacifica, a journal of theological studies for australia and New Zealand. She has lectured and engaged in consultancy work in australia, New Zealand, in the USa, Ireland, in the pacific Islands, China, bangladesh, India, and several Latin american countries.
Dr Confoy also currently serves as a Director of Kilbride Spirituality Centre, Council member of edmund rice education australia, board member of St Columba’s College, essendon, and of The Way.
2012–2013 financial StateMentS
dIrectOrs’ repOrt
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
43
professor Suzanne crowe aMappointed 1 January 2013
professor Crowe is associate Director of the burnet Institute, principal research Fellow with the National Health medical research Council, principal Specialist in Infectious Diseases at The alfred Hospital and adjunct professor of medicine and Infectious Diseases at monash University, melbourne.
professor Crowe is Head of the international Clinical research Laboratory, burnet Institute, and the World Health organization (WHo) regional reference Laboratory for HIv resistance Testing. professor Crowe is an adviser and consultant to the WHo Global program on aIDS, has served as Deputy Chair of the board of the australian India Council (Department of Foreign affairs and Trade), as a member of the prime minister’s Science, engineering and Innovation Council asia Working Group and as president of the australasian Society for HIv medicine.
Mr brendan earleappointed 21 april 2010
mr earle is a partner with the national law firm, Herbert Smith Freehills. He is the national leader of its Healthcare practice. mr earle has over 15 years’ experience providing commercial legal advice across a range of industries and he specialises in large or strategically important negotiated transactions including acquisitions, sales, joint ventures and corporate restructuring. He also acts as a relationship partner for several clients of the firm.
mr earle has a long-standing interest in the australian healthcare industry and has advised the Commonwealth Government, private insurers, aged care providers, private consulting practices and pharmaceutical manufacturers on a diverse range of projects.
Ms patricia faulkner aoappointed 1 october 2010
ms Faulkner is Chair of the National Health performance authority as well as Chair of the boards of Jesuit Social Services, the Health and Hospitals Infrastructure Fund and Superpartners. ms Faulkner is a member of the Council of australian Governments’ reform Council and a previous member of the Commonwealth Grants Commission. ms Faulkner was previously a partner and Global Leader for Healthcare at KpmG and prior to that Secretary of the victorian Department of Human Services.
ms Faulkner has undertaken a number of roles with the victorian Government over a period of almost 20 years in the Department of Labour, Department of Community Welfare Services and the victorian public Services board. ms Faulkner is a Fellow of the Institute of public administration australia, Fellow of the Institute of public administration (victoria) and Fellow of the College of Health Service executives.
Mr Gary Humphrysappointed 1 october 2010
mr Humphrys has over 35 years’ experience in the energy and mining industries undertaking senior executive roles in a number of disciplines including finance, accounting, treasury, taxation, IT, procurement and audit. mr Humphrys is a member of the australian Institute of Chartered accountants and the australian Institute of Company Directors. In July 2005 he was appointed Chief executive officer of Stanwell Corporation, a position he held until he retired in march 2007. mr Humphrys also currently serves as a Director of ergon energy, The Holy Spirit Northside private Hospital, electricity Supply Industry Superannuation (QLD). mr Humphrys is also an alternate director for Guildford Coal Limited.
Ms belinda Hutchinson aMappointed 1 october 2010
ms Hutchinson is Chairman of Qbe Insurance Group, a Director of aGL energy and of the Centre for Independent Studies board, a member of the Salvation army Sydney advisory board, and a member of aSIC’s external advisory panel. ms Hutchinson has previously served as a Director for St vincent’s & mater Health Sydney, Telstra Corporation, Coles myer, energy australia, Tab, Crane Group, Snowy Hydro Trading and Sydney Water Corporation. ms Hutchinson is a former executive Director of macquarie Group where she was Head of macquarie Underwriting and a former vice president of Citibank australia where she was Head of the Financial Institutions Group. In February 2013 ms Hutchinson was appointed as the Chancellor of the University of Sydney.
44
Mr paul Mcclintock aoappointed 1 January 2013
mr mcClintock is previous Chairman of medibank private Limited and current Chair of Thales australia, myer Holdings Limited, I-meD Network and the Institute of virology.
From July 2000 to march 2003, mr mcClintock served as the Secretary to Cabinet and Head of the Cabinet policy Unit reporting directly to the prime minister as Chairman of Cabinet with responsibility for supervising Cabinet processes and acting as the prime minister’s most senior personal adviser on strategic directions in policy formulation.
mr mcClintocks’s former positions include Chairman of the CoaG reform Council, the expert panel of the Low emissions Technology Demonstration Fund, Intoll management Limited, Symbion Health, affinity Health, ashton mining, plutonic resources and the Woolcock Institute of medical research.
mr mcClintock was also a Director of the australian Strategic policy Institute and perpetual Limited, a Commissioner of the Health Insurance Commission and a member of the australia-malaysia Institute executive Committee.
mr mcClintock graduated in arts and Law from the University of Sydney and is an honorary fellow of the Faculty of medicine of that University, and a Life Governor of the Woolcock Institute of medical research.
professor peter Smithappointed 1 october 2010
professor peter Smith is Dean of medicine at The University of New South Wales. He specialised in paediatric clinical oncology and research following study in australia, USa and Germany. He has held senior hospital management posts in brisbane and melbourne and senior academic appointments at the Universities of Queensland, melbourne and auckland.
He is a Director of the Garvan Institute of medical research, Neuroscience research australia and a number of other research institutes. professor Smith is a Group Captain, raaFSr and Director, air Force Health reserves (NSW/aCT).He has served as a consultant to government, including as Chair of the Inquiry into vietnam veterans Cancer Incidence and mortality. He is currently vice president of medical Deans aNZ.
Mr Greg Sword aMappointed 17 october 2008 resigned 5 october 2012
mr Sword was one of the pioneers of the development of industry superannuation and is currently the Chief executive officer of LUCrF Super. He has previously held the positions of National president of the australian Labor party, vice president of the australian Council of Trade Unions (aCTU) and General Secretary of the National Union of Workers. mr Sword is a Trustee of the National Jockeys’ Trust and Trustee of the Caulfield racecourse reserve. He is a graduate of the australian Institute of Company Directors.
Sr Maureen walters rScappointed 6 February 2012 resigned 1 august 2013
a Sister of Charity, Sr maureen has held numerous roles in health leadership, governance and administration. prior to her appointment as a Director of St vincent’s Health australia, Sr maureen served on the boards of St vincent’s Hospital, melbourne; St vincents & mercy private Hospitals, melbourne; the melbourne regional board, Sisters of Charity Health Services; and the National board, Sisters of Charity Health Service.
Her contribution to the governance of the health services followed a highly successful health leadership career. Sr maureen has previously held roles as Sister administrator at St vincent’s private Hospital, Launceston; Deputy Director of Nursing, NSW prison medical Service; and Sister administrator and Director of Nursing at St vincent’s Hospital, melbourne. In her clinical nursing roles, Sr maureen worked in theatre and intensive care. Sr maureen established the post-basic operating room Nursing Course and post-basic Intensive Care Course which were approved by the NSW Nursing registration board.
Sr maureen has also served on the Council of the royal australian Nursing Federation (victorian branch), Nursing Standing Committee of the National Health and medical research Council, the australian Catholic Health Care association (as Councillor and Treasurer), St vincent’s bioethics Centre, and as a member of the Steering Committee for the transfer of victorian Catholic Schools of Nursing to the Institute of Catholic education. Sr maureen holds qualifications in Nursing, Nursing administration, Health administration and Theology.
2012–2013 financial StateMentS
dIrectOrs’ repOrt
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
45
principal actiVitieS
St vincent’s Hospital melbourne (The ‘Hospital’) provides medical and surgical services, sub-acute care, aged care, correctional health, mental health services and a range of community and outreach services. St vincent’s Hospital is a major teaching, research and tertiary referral centre.
key obJectiVeS
The Hospital has enunciated a number of key short and long term objectives in the recently issued St vincent’s Strategic plan 2010–2015. Some of the core objectives are to:
– build relationships with strategic partners
– strengthen surgery, medicine and interventional care
– deliver services of significance and value
– continue to innovate to grow a smarter business focused on the future.
The manner in which these objectives are to be achieved is set in detail in the Strategic plan 2010–2015.
The Hospital measures its performance in detailed monthly Finance and activity reports that are issued to the regional and Group executive, SvHa board and Department of Health.
tradinG reSult
The result of the company for the financial year was a deficit of $848,000 (2012 surplus of $1,438,000).
reView of operationS
a review of the operations of St vincent’s Hospital (melbourne) Limited during the financial year and the result of those operations are set out below:
2013 $’000
2012 $’000
Total revenue for the year 587,814 576,809
Net results for the year (848) 1,438
Comprehensive result (764) 1,668
revenue for the year increased, reflecting additional Department of Health (DH) funding driven by indexation and growth in both government and non-government funded activities.
Comparative increases in revenue and expenditure for the year were, in the main, related to increases in revenue indexation to support increases in pay awards and other costs in line with activity increases and increases in the treatment of complex patients
requiring additional medical and surgical inputs.
MeMberS’ Guarantee
The company is limited by guarantee. If the Company is wound up, the Constitution states that each member is required to contribute a maximum of $100 each towards meeting any outstanding obligations of the company. at 30 June 2013 the company had 1 member (2012: 1 member).
SiGnificant cHanGeS in tHe State of affairS
There were no significant changes in the State of affairs of St vincent’s Hospital (melbourne) Limited.
SubSequent eVentS
There has been no matter or circumstance, which has arisen since 30 June 2013 that has significantly affected, or may affect:
a. The operations, in financial years subsequent to 30 June 2013, of St vincent’s Hospital (melbourne) Limited, or
b. The results of those operations, or
c. The state of affairs, in financial years subsequent to 30 June 2013, of St vincent’s Hospital (melbourne) Limited,
leGiSlatiVe and enVironMental coMpliance
St vincent’s Hospital is committed to promoting a culture of legislative compliance (including environmental legislation) throughout its service. It is a core component of the organisation’s overall risk management strategy and is reported to the executive and SvHa board on an annual basis. any serious or non-compliant issues are managed in a proactive and transparent manner and at an appropriate level of seniority.
46
indeMnifyinG officer or auditor
St vincent’s Hospital (melbourne) Limited has not, during or since the end of the financial year, in respect of any person who is or has been an officer or auditor of the company or a related body corporate:
– indemnified or made any relevant agreement for indemnifying against a liability incurred as an officer, including costs and expenses in successfully defending legal proceedings; or
– paid or agreed to pay a premium in respect of a contract insuring against a liability incurred as an officer for the cost or expenses to defend legal proceedings;
With the exception of the following matter:
– during or since the end of the financial year the company has paid premiums to insure directors and officers against liabilities for costs or expenses incurred by them in defending any legal proceedings arising out of their conduct while acting in the capacity of a director or officer of the company, other than conduct involving a wilful breach of duty in relation to the company. The amount of the premium was paid as part of an overall insurance charge.
roundinG of aMountS
St vincent’s Hospital (melbourne) Limited is an entity of the kind referred to in aSIC Class order 98/0100, dated 10 July 1998, and in accordance with that Class order amounts in the Directors’ report and the financial statements are rounded to the nearest thousand dollars.
board coMMitteeS
there are five committees of the SvhA Board:
audit and risk
Finance and Investment
Quality and Safety
mission, ethics and advocacy
people and Culture
reMuneration
SvHa directors receive payment for their roles as Directors. Some directors have generously refused to accept their fee and asked that the amount due to them be retained by the Group for its charitable works, or have requested that part or all of their fees be directed to their religious order or donated to charity.
in attendance
The following members of the SvHa Group executive attended board meetings for that part of the agenda agreed by the board:
mr robert beetson, as Company Secretary
Dr Tracey batten, as Chief executive officer
mr peter Forsberg, as Chief Financial officer
mr David bryant, as Group General manager people and Culture
Dr annette pantle, as Group General manager Clinical Governance
ms marcelle mogg, as acting Group mission Leader
mr martin Day, as Chief executive officer of St vincents private Hospital melbourne
mr John Leahy, as Chief executive officer of St vincent’s Health & aged Care
professor patricia o’rourke, as Chief executive officer of St vincent’s Hospital melbourne
mr Jonathon anderson, as Chief executive officer, St vincent’s Health Network Sydney
mr robert Cusack, as Chief executive officer, St vincent’s private & mater Hospitals
2012–2013 financial StateMentS
dIrectOrs’ repOrt
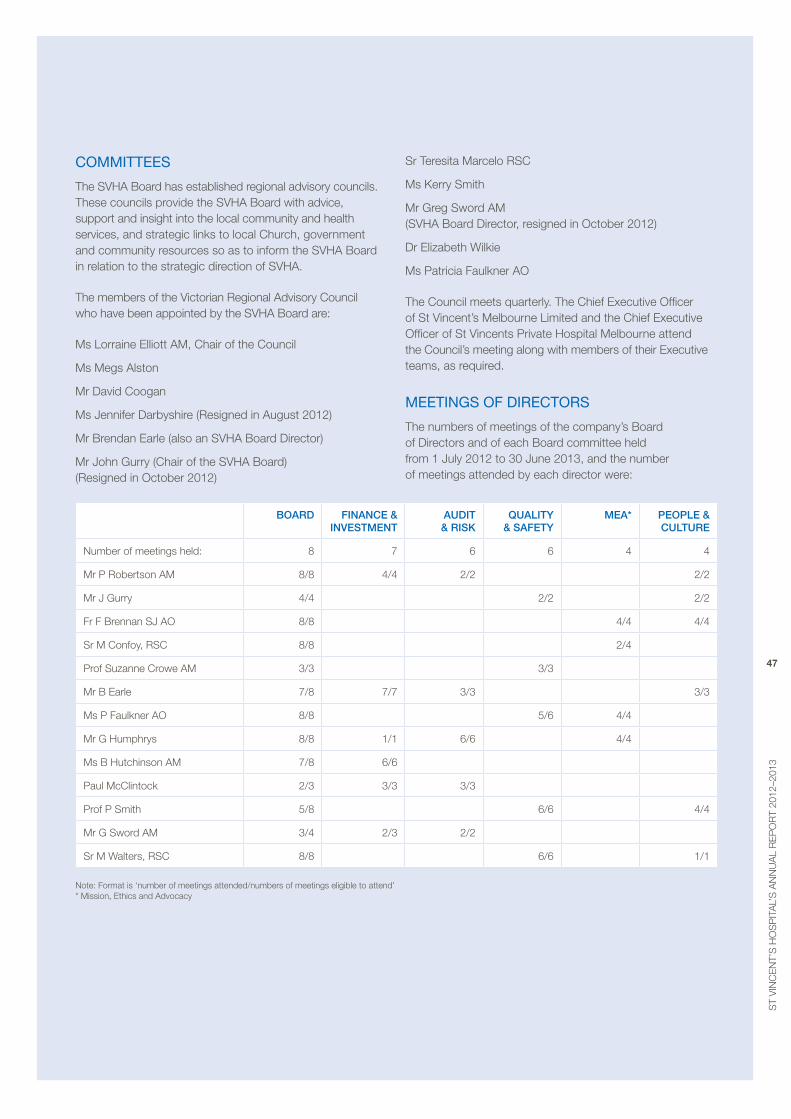
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
47
coMMitteeS
The SvHa board has established regional advisory councils. These councils provide the SvHa board with advice, support and insight into the local community and health services, and strategic links to local Church, government and community resources so as to inform the SvHa board in relation to the strategic direction of SvHa.
The members of the victorian regional advisory Council who have been appointed by the SvHa board are:
ms Lorraine elliott am, Chair of the Council
ms megs alston
mr David Coogan
ms Jennifer Darbyshire (resigned in august 2012)
mr brendan earle (also an SvHa board Director)
mr John Gurry (Chair of the SvHa board) (resigned in october 2012)
Sr Teresita marcelo rSC
ms Kerry Smith
mr Greg Sword am (SvHa board Director, resigned in october 2012)
Dr elizabeth Wilkie
ms patricia Faulkner ao
The Council meets quarterly. The Chief executive officer of St vincent’s melbourne Limited and the Chief executive officer of St vincents private Hospital melbourne attend the Council’s meeting along with members of their executive teams, as required.
MeetinGS of directorS
The numbers of meetings of the company’s board of Directors and of each board committee held from 1 July 2012 to 30 June 2013, and the number of meetings attended by each director were:
BOARD FInAnCe & InveStment
AuDIt & RISk
QuALIty & SAFety
meA* peOpLe & CuLtuRe
Number of meetings held: 8 7 6 6 4 4
mr p robertson am 8/8 4/4 2/2 2/2
mr J Gurry 4/4 2/2 2/2
Fr F brennan SJ ao 8/8 4/4 4/4
Sr m Confoy, rSC 8/8 2/4
prof Suzanne Crowe am 3/3 3/3
mr b earle 7/8 7/7 3/3 3/3
ms p Faulkner ao 8/8 5/6 4/4
mr G Humphrys 8/8 1/1 6/6 4/4
ms b Hutchinson am 7/8 6/6
paul mcClintock 2/3 3/3 3/3
prof p Smith 5/8 6/6 4/4
mr G Sword am 3/4 2/3 2/2
Sr m Walters, rSC 8/8 6/6 1/1
Note: Format is ‘number of meetings attended/numbers of meetings eligible to attend’ * mission, ethics and advocacy
48
auditorS’ independence declaration
a copy of the auditor’s independence declaration as required under section 307C of the Corporations Act 2001 is attached. Dated at melbourne on 26th august 2013 in accordance with a resolution of the board.
mr Gary Humphrys board Director St vincent’s Hospital (melbourne) Limited Dated 26 august 2013
2012–2013 financial StateMentS
dIrectOrs’ repOrt
patricia Faulkner ao board Director St vincent’s Hospital (melbourne) Limited Dated 26 august 2013
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
49
We declare that:
The Financial report comprising the Comprehensive operating Statement, Statement of Financial position, Statement of Changes in equity, Cash Flow Statement and notes to and forming part of the financial statements are in accordance with the Corporations Act 2001, including;
a. Giving a true and fair view of St vincent’s Hospital (melbourne) Limited’s financial position as at 30 June 2013 and of its performance for the year ended on that date: and
b. Complying with accounting Standards, Corporation regulations 2001 and other mandatory professional reporting requirements.
There are reasonable grounds to believe that St vincent’s Hospital (melbourne) Limited will be able to pay its debts as and when they become due and payable.
The Directors have been given the declarations by the Chief executive officer and Chief Financial officer required under section 295a of the Corporations Act 2001.
We certify that the attached financial report for St vincent’s Hospital (melbourne) Limited have been prepared in accordance with part 4.2 of the Standing Directions of the minister for Finance under the Financial Management Act 1994, applicable Financial reporting Directions (with the exception of FrD103D physical Non-Current assets and FrD114a Financial Instruments), australian accounting Standards and other mandatory professional reporting requirements.
We are not aware of any circumstance which would render any particulars included in the financial statements to be misleading or inaccurate.
This declaration is made in accordance with a resolution of the Directors and the accountable officer.
mr Gary Humphrys board Director St vincent’s Hospital (melbourne) Dated 26 august 2013
accOuntable OffIcer’s and dIrectOrs’ declaratIOn
patricia Faulkner ao board Director St vincent’s Hospital (melbourne) Dated 26 august 2013
professor patricia o’rourke Chief executive St vincent’s Hospital (melbourne) Dated 26 august 2013
50
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
51
cOntent tO be supplIed
52
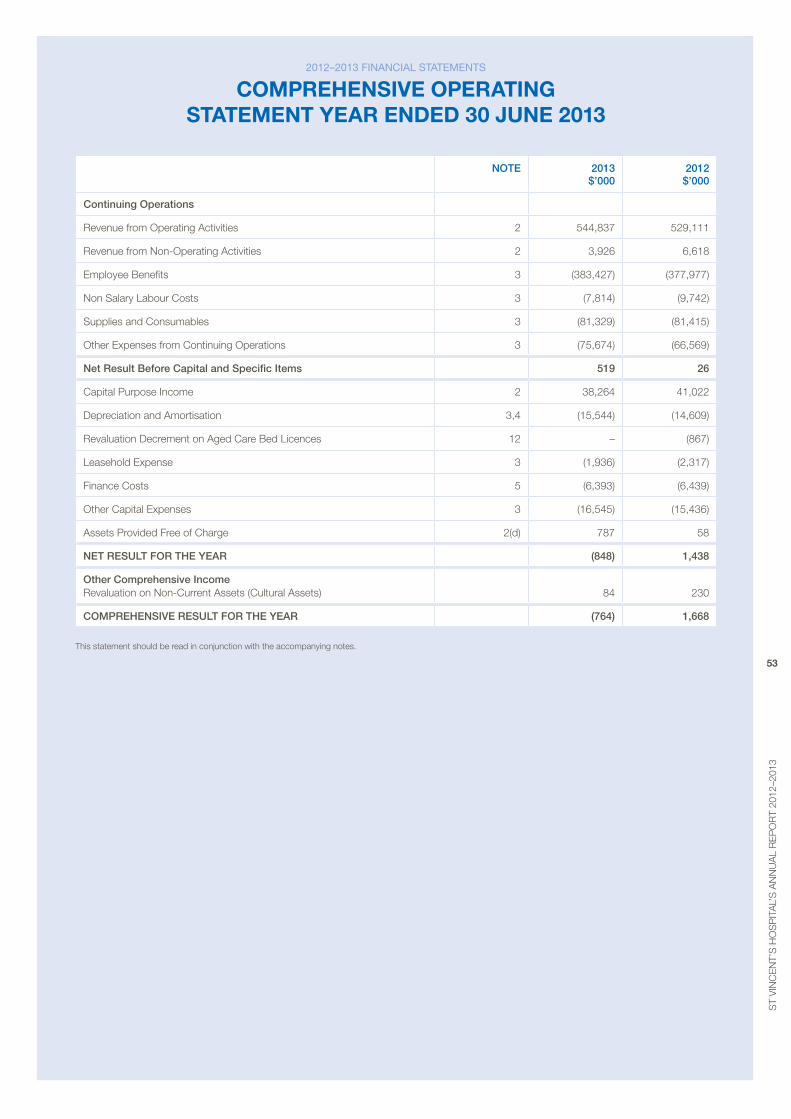
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
53
nOte 2013 $’000
2012 $’000
Continuing Operations
revenue from operating activities 2 544,837 529,111
revenue from Non-operating activities 2 3,926 6,618
employee benefits 3 (383,427) (377,977)
Non Salary Labour Costs 3 (7,814) (9,742)
Supplies and Consumables 3 (81,329) (81,415)
other expenses from Continuing operations 3 (75,674) (66,569)
net Result Before Capital and Specific Items 519 26
Capital purpose Income 2 38,264 41,022
Depreciation and amortisation 3,4 (15,544) (14,609)
revaluation Decrement on aged Care bed Licences 12 – (867)
Leasehold expense 3 (1,936) (2,317)
Finance Costs 5 (6,393) (6,439)
other Capital expenses 3 (16,545) (15,436)
assets provided Free of Charge 2(d) 787 58
net ReSuLt FOR the yeAR (848) 1,438
Other Comprehensive Income revaluation on Non-Current assets (Cultural assets)
84
230
COmpRehenSIve ReSuLt FOR the yeAR (764) 1,668
This statement should be read in conjunction with the accompanying notes.
2012–2013 financial StateMentS
cOmprehensIve OperatIng statement year ended 30 June 2013
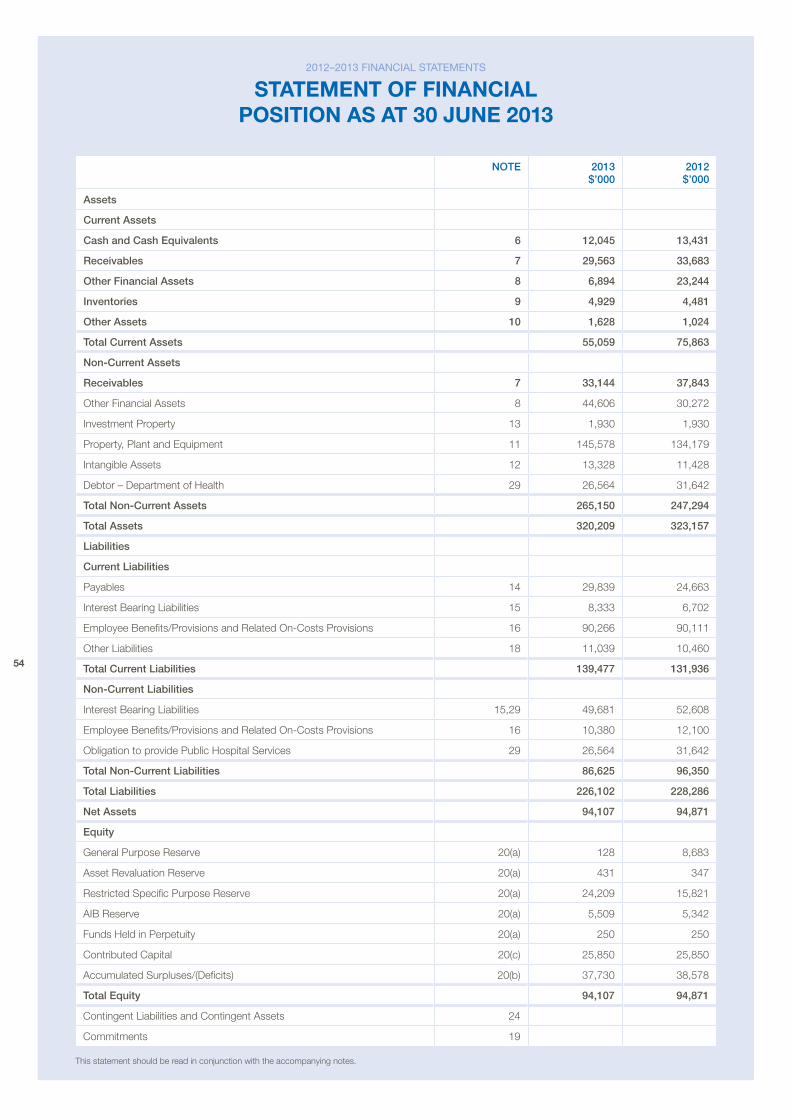
54
nOte 2013 $’000
2012 $’000
Assets
Current Assets
Cash and Cash equivalents 6 12,045 13,431
Receivables 7 29,563 33,683
Other Financial Assets 8 6,894 23,244
Inventories 9 4,929 4,481
Other Assets 10 1,628 1,024
total Current Assets 55,059 75,863
non-Current Assets
Receivables 7 33,144 37,843
other Financial assets 8 44,606 30,272
Investment property 13 1,930 1,930
property, plant and equipment 11 145,578 134,179
Intangible assets 12 13,328 11,428
Debtor – Department of Health 29 26,564 31,642
total non-Current Assets 265,150 247,294
total Assets 320,209 323,157
Liabilities
Current Liabilities
payables 14 29,839 24,663
Interest bearing Liabilities 15 8,333 6,702
employee benefits/provisions and related on-Costs provisions 16 90,266 90,111
other Liabilities 18 11,039 10,460
total Current Liabilities 139,477 131,936
non-Current Liabilities
Interest bearing Liabilities 15,29 49,681 52,608
employee benefits/provisions and related on-Costs provisions 16 10,380 12,100
obligation to provide public Hospital Services 29 26,564 31,642
total non-Current Liabilities 86,625 96,350
total Liabilities 226,102 228,286
net Assets 94,107 94,871
equity
General purpose reserve 20(a) 128 8,683
asset revaluation reserve 20(a) 431 347
restricted Specific purpose reserve 20(a) 24,209 15,821
aIb reserve 20(a) 5,509 5,342
Funds Held in perpetuity 20(a) 250 250
Contributed Capital 20(c) 25,850 25,850
accumulated Surpluses/(Deficits) 20(b) 37,730 38,578
total equity 94,107 94,871
Contingent Liabilities and Contingent assets 24
Commitments 19
This statement should be read in conjunction with the accompanying notes.
2012–2013 financial StateMentS
statement Of fInancIal pOsItIOn as at 30 June 2013
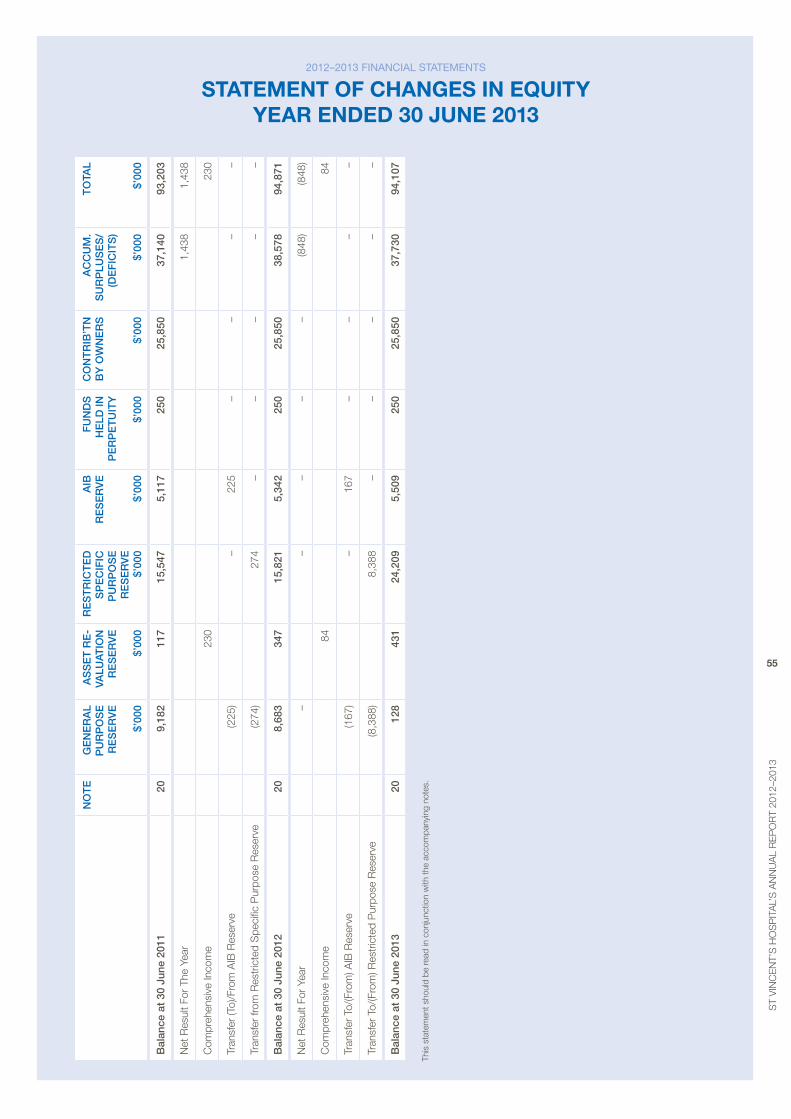
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
55
nO
te
ge
ne
RA
L p
uR
pO
Se
R
eS
eR
ve
$’
000
AS
Se
t R
e-
vALu
AtIO
n
Re
Se
Rv
e
$’00
0
Re
St
RIC
te
D
Sp
eC
IFIC
p
uR
pO
Se
R
eS
eR
ve
$’
000
AIB
R
eS
eR
ve
$’
000
Fu
nD
S
he
LD In
p
eR
pe
tu
Ity
$’
000
CO
nt
RIB
’tn
B
y O
wn
eR
S
$’00
0
AC
Cu
m.
Su
Rp
LuS
eS
/ (D
eF
ICIt
S)
$’00
0
tO
tAL
$’00
0
Bal
ance
at
30 j
une
2011
209,
182
117
15,5
475,
117
250
25,8
5037
,140
93,2
03
Net
res
ult F
or T
he Y
ear
1,4
38
1,4
38
Com
preh
ensi
ve In
com
e23
023
0
Tran
sfer
(To)
/Fro
m a
Ib r
eser
ve (2
25)
–
225
–
–
–
–
Tran
sfer
from
res
tric
ted
Spe
cific
pur
pose
res
erve
(274
) 2
74 –
–
–
–
–
Bal
ance
at
30 j
une
2012
208,
683
347
15,8
215,
342
250
25,8
5038
,578
94,8
71
Net
res
ult F
or Y
ear
–
–
–
–
–
(848
)(8
48)
Com
preh
ensi
ve In
com
e84
84
Tran
sfer
To/
(Fro
m) a
Ib r
eser
ve(1
67)
–
167
–
–
–
–
Tran
sfer
To/
(Fro
m) r
estr
icte
d p
urpo
se r
eser
ve(8
,388
)8,
388
–
–
–
–
–
Bal
ance
at
30 j
une
2013
2012
843
1 2
4,20
9 5,
509
250
25,
850
37,7
30 9
4,10
7
This
sta
tem
ent s
houl
d be
read
in c
onju
nctio
n w
ith th
e ac
com
pany
ing
note
s.
2012–2013 financial StateMentS
statement Of changes In equIty year ended 30 June 2013
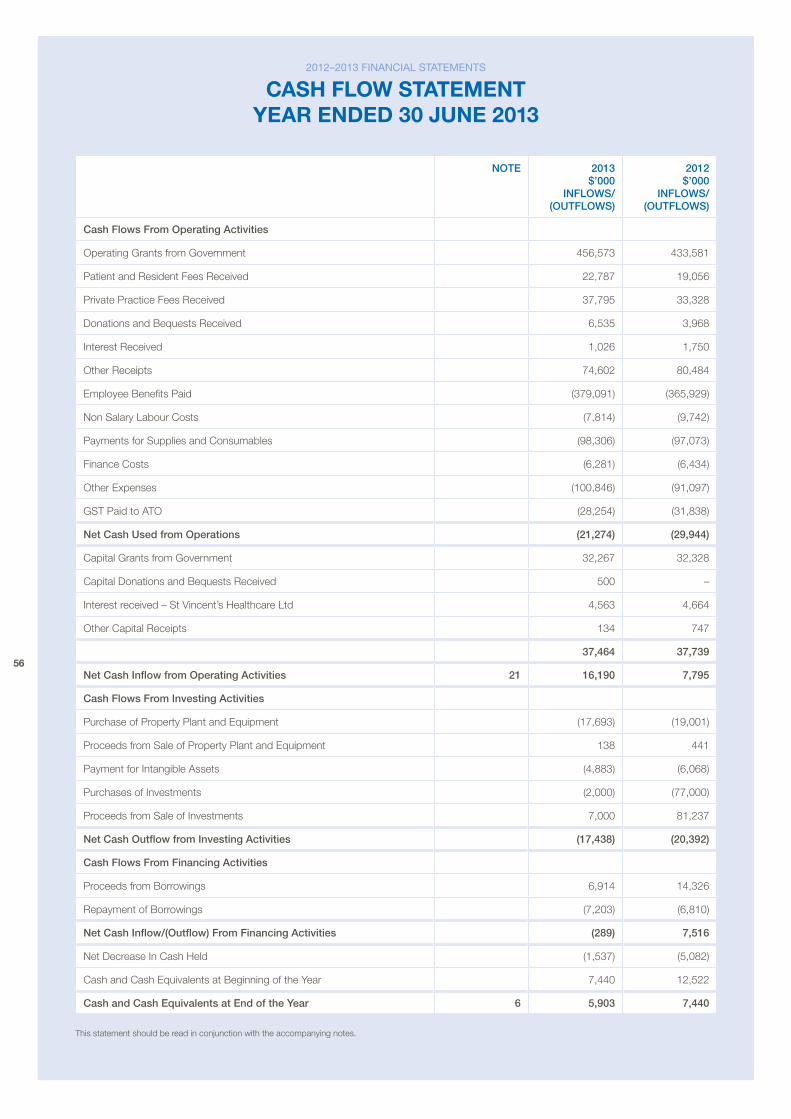
56
nOte 2013 $’000
InFLOwS/ (OutFLOwS)
2012 $’000
InFLOwS/ (OutFLOwS)
Cash Flows From Operating Activities
operating Grants from Government 456,573 433,581
patient and resident Fees received 22,787 19,056
private practice Fees received 37,795 33,328
Donations and bequests received 6,535 3,968
Interest received 1,026 1,750
other receipts 74,602 80,484
employee benefits paid (379,091) (365,929)
Non Salary Labour Costs (7,814) (9,742)
payments for Supplies and Consumables (98,306) (97,073)
Finance Costs (6,281) (6,434)
other expenses (100,846) (91,097)
GST paid to aTo (28,254) (31,838)
net Cash used from Operations (21,274) (29,944)
Capital Grants from Government 32,267 32,328
Capital Donations and bequests received 500 –
Interest received – St vincent’s Healthcare Ltd 4,563 4,664
other Capital receipts 134 747
37,464 37,739
net Cash Inflow from Operating Activities 21 16,190 7,795
Cash Flows From Investing Activities
purchase of property plant and equipment (17,693) (19,001)
proceeds from Sale of property plant and equipment 138 441
payment for Intangible assets (4,883) (6,068)
purchases of Investments (2,000) (77,000)
proceeds from Sale of Investments 7,000 81,237
net Cash Outflow from Investing Activities (17,438) (20,392)
Cash Flows From Financing Activities
proceeds from borrowings 6,914 14,326
repayment of borrowings (7,203) (6,810)
net Cash Inflow/(Outflow) From Financing Activities (289) 7,516
Net Decrease In Cash Held (1,537) (5,082)
Cash and Cash equivalents at beginning of the Year 7,440 12,522
Cash and Cash equivalents at end of the year 6 5,903 7,440
This statement should be read in conjunction with the accompanying notes.
2012–2013 financial StateMentS
cash flOW statement year ended 30 June 2013
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
57
note 1: SuMMary of SiGnificant accountinG policieS
These general-purpose statements have been prepared in accordance with the Corporations Act 2001, the Financial Management Act 1994 (with the exception of FrD103D – Non-Current physical assets and FrD114a Financial Instruments) and accounting Standards issued by the australian accounting Standards board. accounting standards include australian accounting Standards (aaS’s) and Interpretations.
The principal accounting policies adopted in the preparation of the financial statement have been consistently applied to all the years presented unless otherwise stated.
basis of preparation
The financial statements are prepared on an accrual basis and in accordance with the historical cost convention, except for the revaluation of certain non-current assets and financial instruments, as noted. Cost is based on the fair value of the consideration given in exchange for assets.
The financial statements have been prepared on a going concern basis as the Directors’ are satisfied that the Hospital can meet it’s cash operating costs and its debts as and when due for the foreseeable future.
In the application of australian accounting Standards management is required to make judgments, estimates and assumptions about carrying values of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and various other factors that are believed to be reasonable under the circumstance, the results of which form the basis of making the judgments. actual results may differ from these estimates.
The estimates and underlying assumptions are reviewed on an ongoing basis. revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods.
accounting policies are selected and applied in a manner which ensures that the resulting financial information satisfies the concepts of relevance and reliability, thereby ensuring that the substance of the underlying transactions or other events is reported.
The accounting policies set out below have been applied in preparing the financial statements for the year ended 30 June 2013 and the comparative information presented in these financial statements for the year ended 30 June 2012.
a. reporting entity
The financial statements include all the controlled activities of the St vincent’s Hospital (melbourne) Limited (the ‘Hospital’). The Hospital is a not-for-profit company and therefore applies the additional australian paragraphs applicable to ‘not-for-profit’ entities under the accounting standards.
Its principal place of business is:
St vincent’s Hospital (melbourne) Limited 41 victoria parade Fitzroy victoria 3065
b. rounding of amounts
St vincent’s is a company referred to in class order 98/100 issued by the australian Securities and Investment Commission relating to the ‘rounding off’ of amounts in financial statements. amounts in the financial statements have been rounded off in accordance with that class order to the nearest thousand dollars.
c. cash and cash equivalents
Cash and cash equivalents comprise cash on hand and in the banks and investments in money market instruments, which can be readily converted to cash.
d. receivables
Trade receivables are initially recognised at fair value and are due for settlement within 30 days from the date of recognition. Collectability of trade debtors is reviewed on an ongoing basis. Debts which are known to be uncollectible are written off. a provision for doubtful receivables is established when there is objective evidence that the Hospital will not be able to collect all amounts due according to the original terms of receivables. bad debts are written off when identified.
e. inventories
Inventories include goods held for distribution at no or nominal cost in the ordinary course of business operations. It excludes depreciable assets. Inventories held for distribution are measured at the lower of cost and net realisable value. Cost for all inventories is measured on the basis of weighted average cost.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
58
f. other financial assets
Initial recognition and measurementFinancial assets are recognised when the entity becomes a party to the contractual provisions of the instrument being equivalent to the date that the company commits itself to either purchase or sell the asset (i.e. trade date accounting is adopted).
Financial assets are initially measured at fair value plus transaction costs, except where the instrument is classified ‘at fair value through profit or loss’ in which case transaction costs are expensed to profit or loss immediately.
Dividend revenue is recognised on a receivable basis. Interest revenue is recognised on a time proportionate basis that takes into account the effective yield on the financial asset.
Classification and subsequent measurementFinancial instruments are subsequently measured at either fair value, amortised cost using the effective interest rate method or cost. Fair value represents the amount for which an asset could be exchanged or a liability settled, between knowledgeable, willing parties. Where available, quoted prices in an active market are used to determine fair value. In other circumstances, valuation techniques are adopted.
amortised cost is calculated as: (i) the amount at which the financial asset or financial liability is measured at initial recognition; (ii) less principal repayments; (iii) plus or minus the cumulative amortisation of the difference, if any, between the amount initially recognised and the maturity amount calculated using the effective interest method; and (iv) less any reduction for impairment.
The effective interest method is used to allocate interest income or interest expense over the relevant period and is equivalent to the rate that exactly discounts estimated future cash payments or receipts (including fees, transaction costs and other premiums or discounts) through the expected life (or when this cannot be reliably predicted, the contractual term) of the financial instrument to the net carrying amount of the financial asset or financial liability. revisions to expected future net cash flows will necessitate an adjustment to the carrying value with a consequential recognition of an income or expense in profit or loss.
(i) Financial assets at fair value through profit or lossFinancial assets are classified at ‘fair value through profit or loss’ when they are either held for trading for the purpose of short-term profit taking, derivatives not held for hedging purposes, or when they are designated as such to avoid an accounting mismatch or to enable performance evaluation where a group of financial assets is managed by key management personnel on a fair value basis in accordance with a documented risk management or investment strategy. Such assets are subsequently measured at fair value with changes in carrying value being included in profit or loss.
(ii) Loans and receivablesLoans and receivables are non-derivative financial assets with fixed or determinable payments that are not quoted in an active market and are subsequently measured at amortised cost.
Loans and receivables are included in current assets, except for those which are not expected to mature within 12 months after the end of the reporting period, which will be classified as non-current assets.
(iii) Held-to-maturity investmentsHeld-to-maturity investments are non-derivative financial assets that have fixed maturities and fixed or determinable payments, and it is the Hospital’s intention to hold these investments to maturity. They are subsequently measured at amortised cost.
Held-to-maturity investments are included in non-current assets, except for those which are expected to mature within 12 months after the end of the reporting period, which will be classified as current assets.
If during the period the Hospital sold or reclassified more than an insignificant amount of the held-to-maturity investments before maturity, the entire category of held-to-maturity investments would be tainted and would be reclassified as available-for-sale.
Fair value Fair value is determined based on current bid prices for all quoted investments. valuation techniques are applied to determine the fair value for all unlisted securities, including recent arm’s length transactions, reference to similar instruments and option pricing models.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
59
Impairmentat the end of each reporting period, the Hospital assesses whether there is objective evidence that a financial instrument has been impaired. In the case of available-for-sale financial instruments, a prolonged decline in the value of the instrument is considered to determine whether an impairment has arisen. Impairment losses are recognised in the statement of comprehensive income.
DerecognitionFinancial assets are derecognised where the contractual rights to receipt of cash flows expire or the asset is transferred to another party whereby the entity no longer has any significant continuing involvement in the risks and benefits associated with the asset. Financial liabilities are derecognised where the related obligations are either discharged, cancelled or expire. The difference between the carrying value of the financial liability extinguished or transferred to another party and the fair value of consideration paid, including the transfer of non-cash assets or liabilities assumed, is recognised in profit or loss.
g. intangible assets
Intangible assets represent identifiable non-monetary assets without physical substance such as aged Care bed licences, computer software and development costs. Intangible assets are recognised at cost. Costs incurred subsequent to initial acquisition are capitalised when it is expected that additional future economic benefits will flow to the Hospital.
amortisation is allocated to intangible assets with finite useful lives on a systematic basis over the asset’s useful life. amortisation begins when the asset is available for use, that is, when it is in the location and condition necessary for it to be capable of operating in the manner intended by management. The amortisation period and the amortisation method for an intangible asset with a finite useful life is reviewed at least at the end of each annual reporting period. In addition, an assessment is made at each reporting date to determine whether there are indicators that the intangible asset concerned is impaired. If so, the assets concerned are tested as to whether their carrying value exceeds their recoverable amount.
Intangible assets with indefinite useful lives are not amortised. The useful lives of intangible assets that are not being amortised are reviewed each period to determine whether events and circumstances continue to support an indefinite useful life assessment for that asset. In addition, the Hospital tests all intangible assets with indefinite useful lives for impairment by comparing their recoverable amounts with their carrying amounts:
– annually, and
– whenever there is an indication that the intangible asset may be impaired.
any excess of the carrying amount over the recoverable amount is recognised as an impairment loss.
h. property, plant and equipment
plant, equipment and vehicles are measured at cost less accumulated depreciation and impairment losses. Cultural assets are initially measured at cost and subsequently valued at fair value with increments and decrements being reflected through a reserve where decrements have not previously been recognised through the profit and loss. Decrements that offset previous increments in the same class of asset are charged against an asset revaluation reserve directly in equity and other decreases are charged to the profit and loss.
i. depreciation and amortisation
assets with a cost in excess of $1,000 are capitalised and depreciation or amortisation has been provided on depreciable assets so as to allocate their cost (or valuation) over their estimated useful lives using the straight-line method. estimates of the remaining useful lives and depreciation method for all assets are reviewed at least annually. This depreciation charge is not funded by the Department of Health of victoria.
The following table indicates the expected useful lives of non-current assets on which the depreciation charges are generally based.
2013 2012
Leasehold Improvements 10 to 40 years 10 to 40 years
plant and equipment 4 to 10 years 4 to 10 years
medical equipment 4 to 10 years 4 to 10 years
Computers and Communications
4 to 10 years 4 to 10 years
motor vehicles 6.6 years 6.6 years
Furniture and Fittings 6 to 18 years 6 to 18 years
Leased assets 4 to 10 years 4 to 10 years
Computer Software 4 to 10 years 4 to 10 years
60
The basis for leasehold improvements amortisation is determined in accordance with the receipt of letters from:
i) the parent company advising of extension of the ground lease, and
ii) Department of Health advising of the proposed usage of the Hospital for public hospital services beyond 2017 has allowed continuing application of the above expected useful lives of non-current assets.
j. impairment of assets
Intangible assets that have indefinite useful life are not subject to amortisation and are tested annually for impairment or more frequently if events or changes in circumstances indicate that they may be impaired. all other assets are reviewed for indications of impairment except for:
– inventories, and
– financial instrument assets.
If there is an indication of impairment, the assets concerned are tested as to whether their carrying value exceeds their recoverable amount. Where an asset’s carrying value exceeds its recoverable amount, the difference is written-off by a charge to the operating statement except to the extent that the write-down can be debited to an asset revaluation reserve amount applicable to that class of asset.
an impairment loss is recognised for the amount by which the asset’s carrying amount exceeds its recoverable amount. The recoverable amount is measured at the higher of an asset’s fair value less costs to sell and depreciated replacement cost. recoverable amount for assets held primarily to generate net cash inflows is measured at the higher of the present value of future cash flows expected to be obtained from the asset and fair value less costs to sell.
For the purposes of assessing impairment, assets are grouped at the lowest level for which there are separately identifiable cash inflows which are largely independent of the cash inflows from other assets or group of assets (cash-generating units). Where there are indicators of impairment and an asset’s carrying value exceeds its recoverable amount, the difference is written-off by a charge to the operating statement except to the extent that the write-down can be debited to an asset revaluation reserve amount applicable to that class of asset.
The recoverable amount for most assets is measured at the higher of depreciated replacement cost and fair value less costs to sell. recoverable amount for assets held primarily to generate net cash inflows is measured at the higher of the present value of future cash flows expected to be obtained from the asset and fair value less costs to sell. It is deemed that, in the event of the loss of an asset, the future economic benefits arising from the use of the asset will be replaced unless a specific decision to the contrary has been made.
k. investment properties
Investment properties represent properties held to earn rentals or for capital appreciation or both. Investment properties exclude properties held to meet service delivery objectives of the State of victoria.
Investment properties are initially recognised at cost. Costs incurred subsequent to initial acquisition are capitalised when it is probable that future economic benefits in excess of the originally assessed performance of the asset will flow to the Hospital.
Subsequent to initial recognition at cost, investment properties are re-valued to fair value with changes in the fair value recognised as revenue or expenses in the period that they arise. The properties are not depreciated.
The Gertrude Street Investment property is held for long-term capital gain and is not occupied by the Hospital.
rental revenue from the leasing of Gertrude Street is recognised in the Statement of Comprehensive Income in the periods in which it is receivable, as this represents the pattern of service rendered through the provision of the property.
l. payables
These amounts represent liabilities for goods and services provided prior to the end of the financial year and which were unpaid at that date. The amounts are unsecured and normal credit terms are within 30 days of recognition.
m. resources provided and received free of charge or nominal consideration
resources provided or received free of charge or for nominal consideration are recognised at their fair value when the Hospital receives control over them regardless of any restrictions or conditions imposed over their use. Contributions in the form of services are only recognised when a fair value can be reliably determined and the services would have been purchased if not donated.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
61
n. interest bearing liabilities
Interest bearing liabilities in the Statement of Financial position are recognised at fair value upon initial recognition. Subsequent to initial recognition, all financial liabilities are recognised at amortised cost using the effective interest method.
o. functional and presentation currency
The presentation currency of the Hospital is the australian dollar, which has also been identified as the functional currency of the Hospital.
p. Goods and Services tax (GSt)
Income, expenses and assets are recognised net of the amount of associated GST, unless the GST incurred is not recoverable from the taxation authority. In this case it is recognised as part of the cost of acquisition of the asset or as part of the expense.
receivables and payables are stated inclusive of the amount of GST receivable or payable. The net amount of GST recoverable from, or payable to, the taxation authority is included with other receivables or payables in the Statement of Financial position.
Cash flows in the Cashflow Statement are presented on a gross basis. The GST components of cash flows arising from investing or financing activities which are recoverable from, or payable to the taxation authority, are presented as operating cash flow.
q. employee benefits wages and Salaries, annual leave, Sick leave and accrued days off
Liabilities for wages and salaries, including non-monetary benefits, annual leave and accrued days off expected to be settled within 12 months of the reporting date are recognised in the provision for employee benefits in respect of employee’s services up to the reporting date, classified as current liabilities and measured at nominal values.
Those liabilities that the Hospital does not expect to settle within 12 months are recognised in the provision for employee benefits as current liabilities, measured at present value of the amounts expected to be paid when the liabilities are settled using the remuneration rate expected to apply at the time of settlement.
long Service leave
Current Liability — unconditional LSL (representing 10 or more years of continuous service) is disclosed as a current liability regardless whether or not the Hospital expects to settle the liability within 12 months, as it does not have the unconditional right to defer the settlement of the entitlement should an employee decide to take leave.
The components of this current LSL liability are measured at:
– present value — component that the Hospital does not expect to settle within 12 months; and
– nominal value — component that the Hospital expects to settle within 12 months.
Non-Current Liability — conditional LSL (representing less than 10 years of continuous service) is disclosed as a non-current liability. There is an unconditional right to defer the settlement of the entitlement until 10 years of service has been completed by an employee. Conditional LSL is required to be measured at present value.
Consideration is given to expected future wage and salary levels, experience of employee departures and periods of service. expected future payments are discounted using interest rates of Commonwealth Government guaranteed securities in australia.
62
Superannuation
employees of the Hospital are entitled to receive superannuation benefits and the Hospital contributes to both the defined benefit and defined contribution plans. The defined benefit plan(s) provide benefits based on years of service and final average salary.
Contributions to defined superannuation plans are expensed when incurred. The Hospital has no liability in respect of these plans.
The amount charged to the Income Statement in respect of defined benefit superannuation plans represents the contributions made by the Hospital to the superannuation plan in respect of the services of current company staff. Superannuation contributions are made to the plans based on the relevant rules of each plan.
The Hospital does not recognise any defined benefit liability in respect of the superannuation plans because the Hospital has no legal or constructive obligation to pay future benefits relating to its employees; its only obligation is to pay superannuation contributions as they fall due. The Department of Treasury and Finance of the State of victoria administers and discloses the State’s defined benefit liabilities in its financial statements.
termination BenefitsTermination benefits are payable when employment is terminated before the normal retirement date or when an employee accepts voluntary redundancy in exchange for these benefits.
Liabilities for termination benefits are recognised when a detailed plan for the termination has been developed and a valid expectation has been raised with those employees affected that the terminations will be carried out. The liabilities for termination benefits are recognised in other creditors unless the amount or timing of the payments is uncertain, in which case they are recognised as a provision.
On-Costsemployee benefit on-costs are recognised and included in employee benefit liabilities and costs when the employee benefits to which they relate are recognised as liabilities.
r. finance costs
Finance costs are recognised as expenses in the period in which they are incurred. Finance costs include:
– interest on bank overdrafts and short-term and long-term borrowings
– amortisation of discounts or premiums relating to borrowings
– amortisation of ancillary costs incurred in connection with the arrangement of borrowings
– finance charges in respect of finance leases recognised in accordance with AASB 117 Leases.
s. leases
Leases of property, plant and equipment are classified as finance leases whenever the terms of the lease transfer substantially all the risks and rewards of ownership to the lessee. all other leases are classified as operating leases.
operating lease payments, including any contingent rentals, are recognised as an expense in the Statement of Comprehensive Income on a straight line basis over the lease term, except where another systematic basis is more representative of the time pattern of the benefits derived from the use of the leased asset.
t. revenue recognition
revenue is recognised in accordance with aaSb 118 revenue and is recognised as revenue to the extent it is earned. Unearned income at reporting dates is reported as income received in advance. amounts disclosed as revenue are, where applicable, net of returns, allowances and duties and taxes.
government grantsGrants are recognised as revenue when the Hospital gains control of the underlying assets as prescribed in AASB 1004 Contributions. Where grants are reciprocal, revenue is recognised as performance occurs under the grant. Non-reciprocal grants are recognised as revenue when the grant is received or receivable. Conditional grants may be reciprocal or non-reciprocal depending on the terms of the grant.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
63
Indirect Contributions from the Department of health (Doh)Long Service Leave (LSL) – revenue is recognised upon finalisation of movements in LSL liability in line with the arrangements set out in the victorian Department of Health Hospital Circular 05/2013.
patient Feespatient fees are recognised as revenue at the time invoices are raised.
private practice Feesprivate practice fees are recognised as revenue at the time invoices are raised.
Donations and BequestsDonations and bequests are recognised as revenue when received. If donations are for a special purpose they may be appropriated to a reserve, such as specific restricted purpose reserve.
InterestInterest revenue is recognised on a time proportionate basis that takes into account the effective yield of the financial asset.
DividendsDividend revenue is recognised when the right to receive payment is obtained.
u. fund accounting
The Hospital operates on a fund accounting basis and maintains three funds: operating, Specific purpose and Capital Funds. The Hospital’s Capital and Specific purpose Funds include unspent capital donations and receipts from fund-raising activities conducted solely in respect of these funds. Funds held in perpetuity reflect the initial investment into the Health Service by St vincent’s Health australia Limited upon establishment of the Hospital.
v. Services Supported by Health Services agreement and Services Supported by Hospital and community initiatives
activities classified as Services Supported by Health Services Agreement (HSa) are substantially funded by the Department of Health for the provision of public Hospital Services and includes residential aged Care Services (raCS), while Services Supported by Hospital and Community Initiatives (Non HSa) are funded by the Hospital’s own activities or commercial/business unit activities and/or the Commonwealth.
w. Specific restricted purpose reserve
a specific restricted purpose reserve is established where the Hospital has possession or title to the funds but has no discretion to amend or vary the restriction and/or condition underlying the funds received.
x. net result from continuing operations before capital and Specific items
The subtotal entitled ‘Net result before Capital and Specific Items’ is included in the Statement of Comprehensive Income to enhance the understanding of the financial performance of the Hospital. This subtotal reports the result excluding items such as capital grants, assets received or provided free of charge, depreciation, and items of unusual nature and amount such as specific income (Note 2) and expenses (Note 3). The exclusion of these items is made to enhance matching of income and expenses so as to facilitate the comparability and consistency of results between years and victorian public Health Services.
The Net result before Capital and Specific Items is used by the management of the Hospital, the Department of Health and the victorian Government to measure the ongoing result of health services in operating hospital services.
Capital and specific items, which are excluded from this sub-total, comprise:
– Capital purpose income, which comprises all tied grants, donations and bequests received for the purpose of acquiring non-current assets, such as capital works, plant and equipment. It also includes donations of plant and equipment. Consequently the recognition of revenue as capital purpose income is based on the intention of the provider of the revenue at the time the revenue is provided
– Specific income/expenses comprise the following items, where material:
i ) Depreciation and amortisation, as described in Note 1(i)
ii ) assets provided free of charge, as described in Note 1(m).
64
y. category Groups
The Hospital has used the following category groups for reporting purposes for the current and previous financial years. However it should be noted that allocations across category groups are limited by both the Hospital’s common chart of account coverage and the inclusion of the activities of St George’s Health Service, Caritas Christ Hospice and prague House.
Admitted Patient Services (Admitted Patients) comprises all recurrent health revenue/expenditure on admitted patient services, where services are delivered in public hospitals, or free standing day hospital facilities, or palliative care facilities, or rehabilitation facilities, or alcohol and drug treatment units.
Mental Health Services (Mental Health) comprises all recurrent health revenue/expenditure on specialised mental health services (child and adolescent, general and adult, community) managed or funded by the state or territory health administrations, and includes: admitted patient services, outpatient services, emergency department services (where it is possible to separate emergency department mental health services), community-based services, residential and ambulatory services.
Outpatient Services (Outpatients) comprises all recurrent health revenue/expenditure on public hospital type outpatient services, where services are delivered in public hospital outpatient clinics, or free standing day hospital facilities, or rehabilitation facilities, or alcohol and drug treatment units, or outpatient clinics specialising in ophthalmic aids or palliative care.
Emergency Department Services (EDS) comprises all recurrent health revenue/expenditure on emergency department services that are available free of charge to public patients.
Ambulatory comprises all recurrent health revenue/expenditure on public hospital type services, provided the following are delivered/received outside a hospital campus, services which have moved from a hospital to a community setting since June 1998, services which fall within the agreed scope of inclusions under the new system, which have been delivered with hospitals, i.e. in rural/remote areas.
Aged Care comprises revenue/expenditure from Home and Community Care (HaCC) programs, allied Health, aged Care assessment and support services.
Residential Aged Care (RAC) including Mental Health referred to in the past as psychogeriatric residential services, comprises those Commonwealth-licensed residential aged care services in receipt of supplementary funding from DoH under the mental health program. It excludes all other residential services funded under the mental health program, such as mental health funded community care units (CCUs) and secure extended care units (SeCs).
Primary Health comprises revenue/expenditure for Community Health Services including health promotion and counselling, physiotherapy, speech therapy, podiatry and occupational therapy.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
65
z. new accounting Standards and interpretations
Certain new accounting standards and interpretations have been published that are not mandatory for the year ended 30 June 2013. The Hospital’s assessment of the impact of those new standards and interpretations which are applicable to the Hospital is set out below.
StAnDARD/InteRpRetAtIOn
SummARy AppLICABLe FOR AnnuAL RepORtIng peRIODS BegInnIng On
ImpACt On the hOSpItAL’S FInAnCIAL StAtementS
aaSb 9 Financial instruments
This standard simplifies requirements for the classification and measurement of financial assets resulting from phase 1 of the IaSb’s project to replace IaS 39 Financial Instruments: Recognition and Measurement (aaSb 139 Financial Instruments: Recognition and Measurement).
1 Jan 2015 Subject to aaSb’s further modifications to aaSb 9, together with the anticipated changes resulting from the staged projects on impairments and hedge accounting, details of impacts will be assessed.
aaSb 10 Consolidated Financial Statements
This Standard forms the basis for determining which entities should be consolidated into an entity’s financial statements. aaSb 10 defines ‘control’ as requiring exposure or rights to variable returns and the ability to affect those returns through power over an investee, which may broaden the concept of control for public sector entities.
The aaSb has issued an exposure draft eD 238 Consolidated Financial Statements – Australian Implementation Guidance for Not-for-Profit Entities that explains and illustrates how the principles in the Standard apply from the perspective of not-for-profit entities in the private and public sectors.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date.
The Standard is not expected to apply.
aaSb 11 Joint Arrangements
This Standard deals with the concept of joint control, and sets out a new principles-based approach for determining the type of joint arrangement that exists and the corresponding accounting treatment. The new categories of joint arrangements under aaSb 11 are more aligned to the actual rights and obligations of the parties to the arrangement.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date.
Subject to aaSb’s final deliberations and any modifications made to aaSb 11 for not-for-profit entities, the entity will need to assess the nature of arrangements with other entities in determining whether a joint arrangement exists in light of aaSb 11.
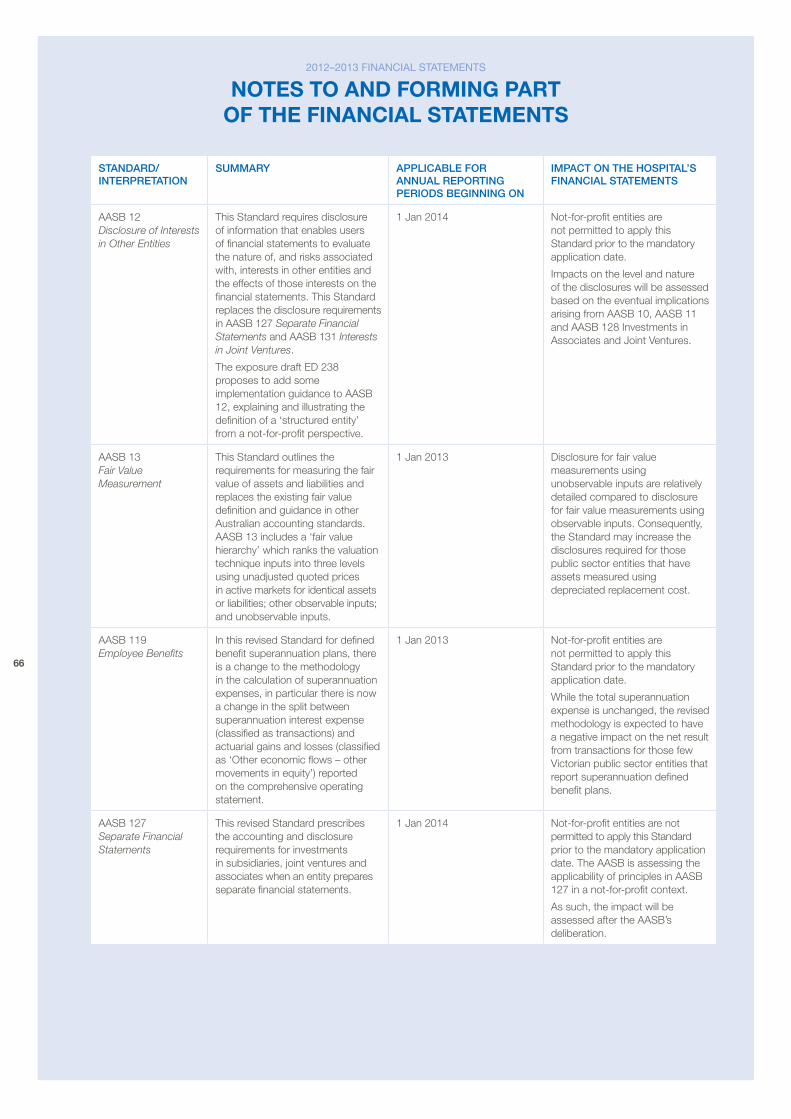
66
StAnDARD/InteRpRetAtIOn
SummARy AppLICABLe FOR AnnuAL RepORtIng peRIODS BegInnIng On
ImpACt On the hOSpItAL’S FInAnCIAL StAtementS
aaSb 12 Disclosure of Interests in Other Entities
This Standard requires disclosure of information that enables users of financial statements to evaluate the nature of, and risks associated with, interests in other entities and the effects of those interests on the financial statements. This Standard replaces the disclosure requirements in aaSb 127 Separate Financial Statements and aaSb 131 Interests in Joint Ventures.
The exposure draft eD 238 proposes to add some implementation guidance to aaSb 12, explaining and illustrating the definition of a ‘structured entity’ from a not-for-profit perspective.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date.
Impacts on the level and nature of the disclosures will be assessed based on the eventual implications arising from aaSb 10, aaSb 11 and aaSb 128 Investments in associates and Joint ventures.
aaSb 13 Fair Value Measurement
This Standard outlines the requirements for measuring the fair value of assets and liabilities and replaces the existing fair value definition and guidance in other australian accounting standards. aaSb 13 includes a ‘fair value hierarchy’ which ranks the valuation technique inputs into three levels using unadjusted quoted prices in active markets for identical assets or liabilities; other observable inputs; and unobservable inputs.
1 Jan 2013 Disclosure for fair value measurements using unobservable inputs are relatively detailed compared to disclosure for fair value measurements using observable inputs. Consequently, the Standard may increase the disclosures required for those public sector entities that have assets measured using depreciated replacement cost.
aaSb 119 Employee Benefits
In this revised Standard for defined benefit superannuation plans, there is a change to the methodology in the calculation of superannuation expenses, in particular there is now a change in the split between superannuation interest expense (classified as transactions) and actuarial gains and losses (classified as ‘other economic flows – other movements in equity’) reported on the comprehensive operating statement.
1 Jan 2013 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date.
While the total superannuation expense is unchanged, the revised methodology is expected to have a negative impact on the net result from transactions for those few victorian public sector entities that report superannuation defined benefit plans.
aaSb 127 Separate Financial Statements
This revised Standard prescribes the accounting and disclosure requirements for investments in subsidiaries, joint ventures and associates when an entity prepares separate financial statements.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date. The aaSb is assessing the applicability of principles in aaSb 127 in a not-for-profit context.
as such, the impact will be assessed after the aaSb’s deliberation.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
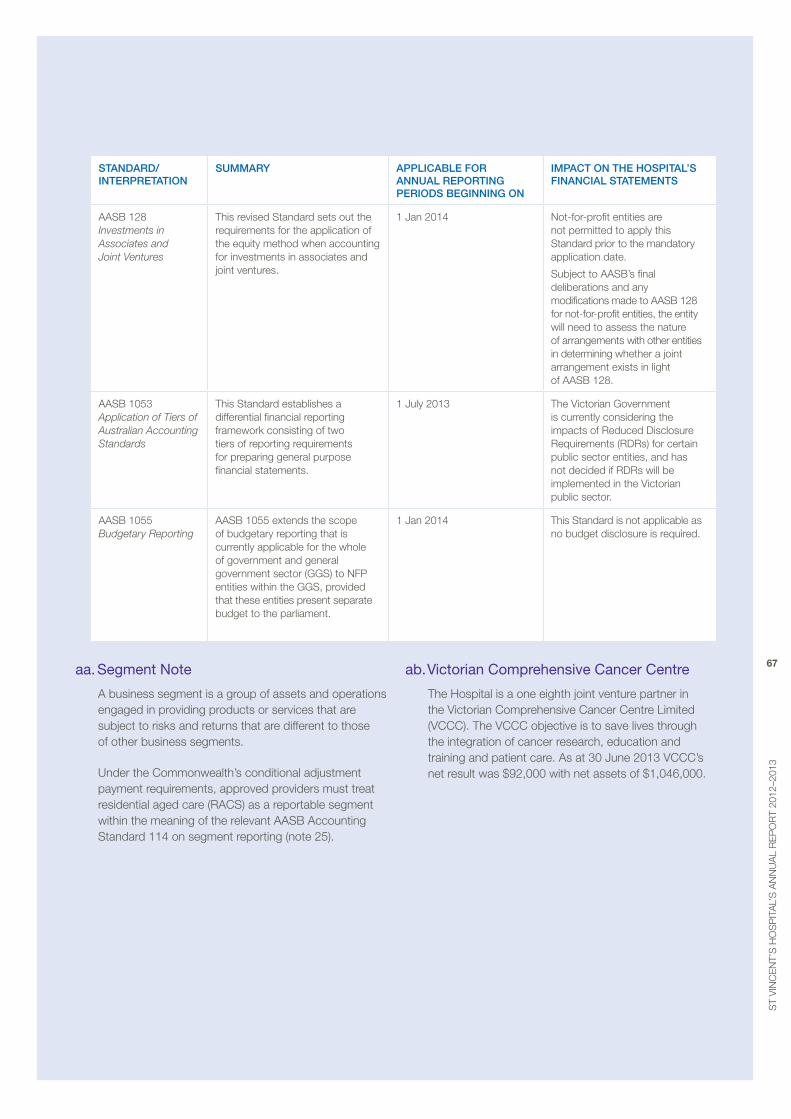
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
67
StAnDARD/InteRpRetAtIOn
SummARy AppLICABLe FOR AnnuAL RepORtIng peRIODS BegInnIng On
ImpACt On the hOSpItAL’S FInAnCIAL StAtementS
aaSb 128 Investments in Associates and Joint Ventures
This revised Standard sets out the requirements for the application of the equity method when accounting for investments in associates and joint ventures.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date.
Subject to aaSb’s final deliberations and any modifications made to aaSb 128 for not-for-profit entities, the entity will need to assess the nature of arrangements with other entities in determining whether a joint arrangement exists in light of aaSb 128.
aaSb 1053 Application of Tiers of Australian Accounting Standards
This Standard establishes a differential financial reporting framework consisting of two tiers of reporting requirements for preparing general purpose financial statements.
1 July 2013 The victorian Government is currently considering the impacts of reduced Disclosure requirements (rDrs) for certain public sector entities, and has not decided if rDrs will be implemented in the victorian public sector.
aaSb 1055 Budgetary Reporting
aaSb 1055 extends the scope of budgetary reporting that is currently applicable for the whole of government and general government sector (GGS) to NFp entities within the GGS, provided that these entities present separate budget to the parliament.
1 Jan 2014 This Standard is not applicable as no budget disclosure is required.
aa. Segment note
a business segment is a group of assets and operations engaged in providing products or services that are subject to risks and returns that are different to those of other business segments.
Under the Commonwealth’s conditional adjustment payment requirements, approved providers must treat residential aged care (raCS) as a reportable segment within the meaning of the relevant aaSb accounting Standard 114 on segment reporting (note 25).
ab. Victorian comprehensive cancer centre
The Hospital is a one eighth joint venture partner in the victorian Comprehensive Cancer Centre Limited (vCCC). The vCCC objective is to save lives through the integration of cancer research, education and training and patient care. as at 30 June 2013 vCCC’s net result was $92,000 with net assets of $1,046,000.
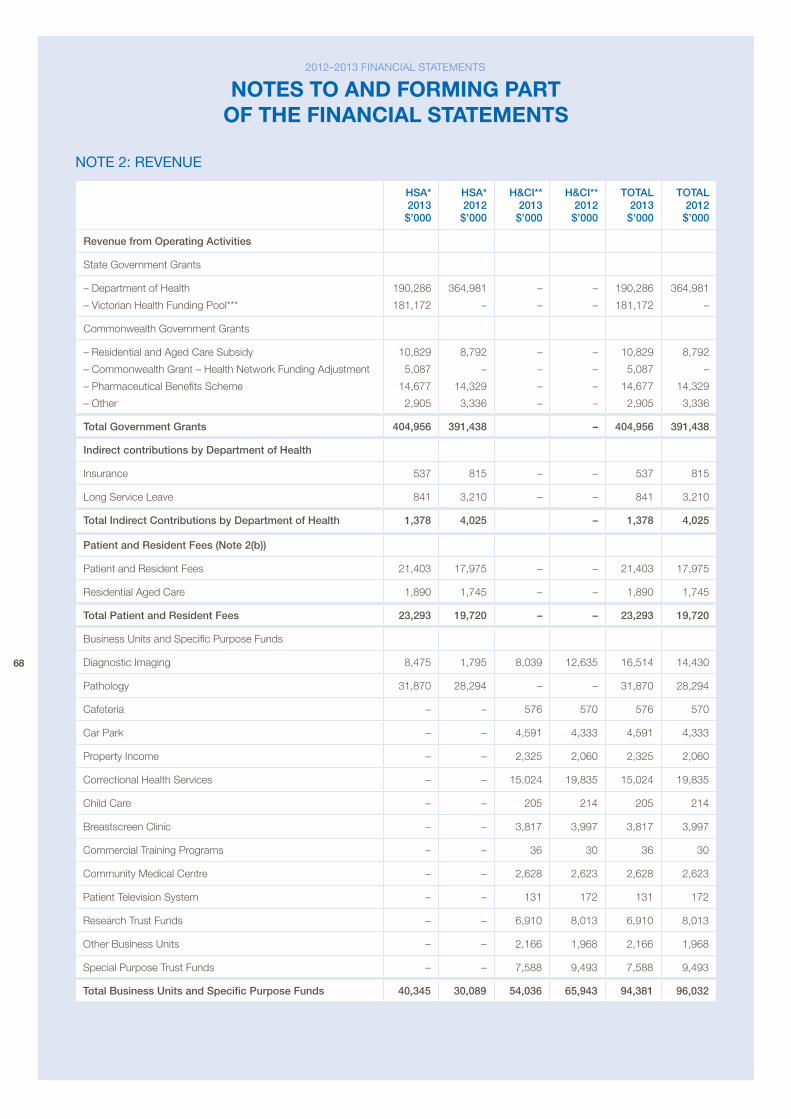
68
note 2: reVenue
hSA* 2013 $’000
hSA* 2012 $’000
h&CI** 2013 $’000
h&CI** 2012 $’000
tOtAL 2013 $’000
tOtAL 2012 $’000
Revenue from Operating Activities
State Government Grants
– Department of Health
– victorian Health Funding pool***
190,286
181,172
364,981
–
–
–
–
–
190,286
181,172
364,981
–
Commonwealth Government Grants
– residential and aged Care Subsidy
– Commonwealth Grant – Health Network Funding adjustment
– pharmaceutical benefits Scheme
– other
10,829
5,087
14,677
2,905
8,792
–
14,329
3,336
–
–
–
–
–
–
–
–
10,829
5,087
14,677
2,905
8,792
–
14,329
3,336
total government grants 404,956 391,438 – 404,956 391,438
Indirect contributions by Department of health
Insurance 537 815 – – 537 815
Long Service Leave 841 3,210 – – 841 3,210
total Indirect Contributions by Department of health 1,378 4,025 – 1,378 4,025
patient and Resident Fees (note 2(b))
patient and resident Fees 21,403 17,975 – – 21,403 17,975
residential aged Care 1,890 1,745 – – 1,890 1,745
total patient and Resident Fees 23,293 19,720 – – 23,293 19,720
business Units and Specific purpose Funds
Diagnostic Imaging 8,475 1,795 8,039 12,635 16,514 14,430
pathology 31,870 28,294 – – 31,870 28,294
Cafeteria – – 576 570 576 570
Car park – – 4,591 4,333 4,591 4,333
property Income – – 2,325 2,060 2,325 2,060
Correctional Health Services – – 15,024 19,835 15,024 19,835
Child Care – – 205 214 205 214
breastscreen Clinic – – 3,817 3,997 3,817 3,997
Commercial Training programs – – 36 30 36 30
Community medical Centre – – 2,628 2,623 2,628 2,623
patient Television System – – 131 172 131 172
research Trust Funds – – 6,910 8,013 6,910 8,013
other business Units – – 2,166 1,968 2,166 1,968
Special purpose Trust Funds – – 7,588 9,493 7,588 9,493
total Business units and Specific purpose Funds 40,345 30,089 54,036 65,943 94,381 96,032
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
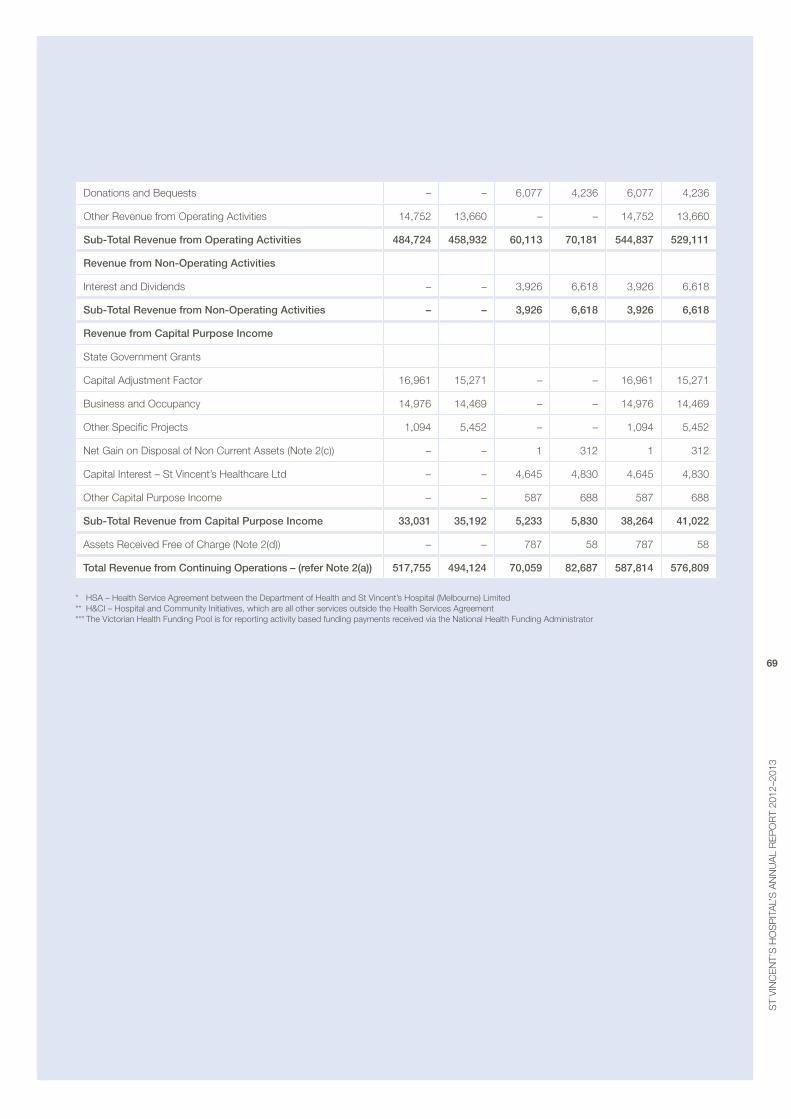
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
69
Donations and bequests – – 6,077 4,236 6,077 4,236
other revenue from operating activities 14,752 13,660 – – 14,752 13,660
Sub-total Revenue from Operating Activities 484,724 458,932 60,113 70,181 544,837 529,111
Revenue from non-Operating Activities
Interest and Dividends – – 3,926 6,618 3,926 6,618
Sub-total Revenue from non-Operating Activities – – 3,926 6,618 3,926 6,618
Revenue from Capital purpose Income
State Government Grants
Capital adjustment Factor 16,961 15,271 – – 16,961 15,271
business and occupancy 14,976 14,469 – – 14,976 14,469
other Specific projects 1,094 5,452 – – 1,094 5,452
Net Gain on Disposal of Non Current assets (Note 2(c)) – – 1 312 1 312
Capital Interest – St vincent’s Healthcare Ltd – – 4,645 4,830 4,645 4,830
other Capital purpose Income – – 587 688 587 688
Sub-total Revenue from Capital purpose Income 33,031 35,192 5,233 5,830 38,264 41,022
assets received Free of Charge (Note 2(d)) – – 787 58 787 58
total Revenue from Continuing Operations – (refer note 2(a)) 517,755 494,124 70,059 82,687 587,814 576,809
* HSa – Health Service agreement between the Department of Health and St vincent’s Hospital (melbourne) Limited ** H&CI – Hospital and Community Initiatives, which are all other services outside the Health Services agreement *** The victorian Health Funding pool is for reporting activity based funding payments received via the National Health Funding administrator
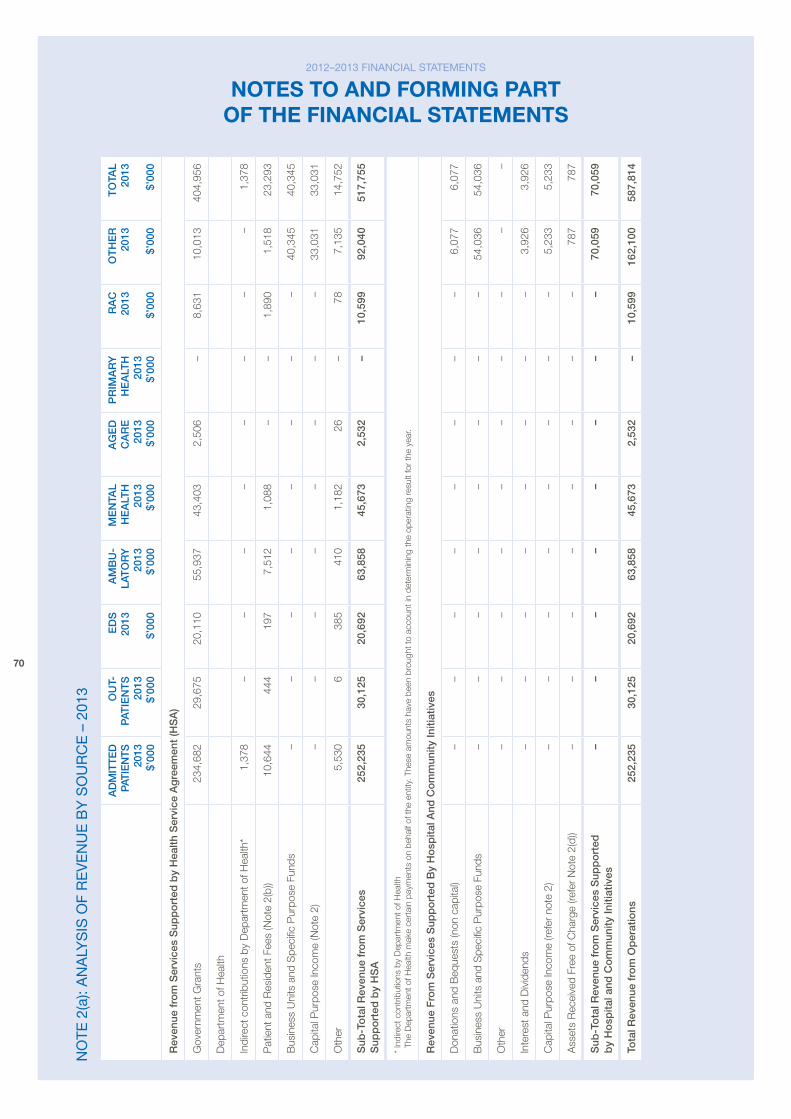
70
no
te 2
(a):
an
aly
SiS
of
re
Ve
nu
e b
y S
ou
rc
e –
201
3
AD
mIt
teD
pA
tIe
ntS
20
13
$’00
0
Ou
t-p
AtIe
nt
S
2013
$’
000
eD
S
2013
$’
000
Am
Bu
-LA
tO
Ry
20
13
$’00
0
me
ntA
L h
eA
Lth
20
13
$’00
0
Ag
eD
C
AR
e
2013
$’
000
pR
ImA
Ry
h
eA
Lth
20
13
$’00
0
RA
C
2013
$’
000
Ot
he
R
2013
$’
000
tO
tAL
2013
$’
000
Rev
enue
fro
m S
ervi
ces
Sup
po
rted
by
hea
lth S
ervi
ce A
gre
emen
t (h
SA
)
Gov
ernm
ent G
rant
s23
4,68
2 2
9,67
5 2
0,11
0 5
5,93
743
,403
2,50
6 –
8
,631
1
0,01
3 4
04,9
56
Dep
artm
ent o
f Hea
lth
Indi
rect
con
trib
utio
ns b
y D
epar
tmen
t of H
ealth
* 1
,378
–
–
–
–
–
–
–
–
1
,378
pat
ient
and
res
iden
t Fee
s (N
ote
2(b)
) 1
0,64
4 4
44
197
7
,512
1
,088
–
–
1
,890
1
,518
2
3,29
3
bus
ines
s U
nits
and
Spe
cific
pur
pose
Fun
ds
–
–
–
–
–
–
–
–
40,
345
40,
345
Cap
ital p
urpo
se In
com
e (N
ote
2) –
–
–
–
–
–
–
–
3
3,03
1 3
3,03
1
oth
er 5
,530
6
3
85
410
1
,182
2
6 –
7
8 7
,135
1
4,75
2
Sub
-to
tal R
even
ue f
rom
Ser
vice
s S
upp
ort
ed b
y h
SA
2
52,2
35
30,
125
20,
692
63,
858
45,
673
2,5
32
–
10,
599
92,
040
517
,755
* In
dire
ct c
ontr
ibut
ions
by
Dep
artm
ent o
f Hea
lth
The
Dep
artm
ent o
f Hea
lth m
ake
cert
ain
paym
ents
on
beha
lf of
the
entit
y. T
hese
am
ount
s ha
ve b
een
brou
ght t
o ac
coun
t in
dete
rmin
ing
the
oper
atin
g re
sult
for
the
year
.
Rev
enue
Fro
m S
ervi
ces
Sup
po
rted
By
ho
spita
l And
Co
mm
unity
Initi
ativ
es
Don
atio
ns a
nd b
eque
sts
(non
cap
ital)
–
–
–
–
–
–
–
–
6,0
77
6,0
77
bus
ines
s U
nits
and
Spe
cific
pur
pose
Fun
ds –
–
–
–
–
–
–
–
5
4,03
6 5
4,03
6
oth
er –
–
–
–
–
–
–
–
–
–
Inte
rest
and
Div
iden
ds –
–
–
–
–
–
–
–
3
,926
3
,926
Cap
ital p
urpo
se In
com
e (re
fer
note
2)
–
–
–
–
–
–
–
–
5,2
33
5,2
33
ass
ets
rec
eive
d Fr
ee o
f Cha
rge
(refe
r N
ote
2(d)
) –
–
–
–
–
–
–
–
7
87
787
Sub
-to
tal R
even
ue f
rom
Ser
vice
s S
upp
ort
ed
by
ho
spita
l and
Co
mm
unity
Initi
ativ
es –
–
–
–
–
–
–
–
7
0,05
9 7
0,05
9
tota
l Rev
enue
fro
m O
per
atio
ns 2
52,2
35
30,
125
20,
692
63,
858
45,
673
2,5
32
–
10,
599
162
,100
587
,814
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
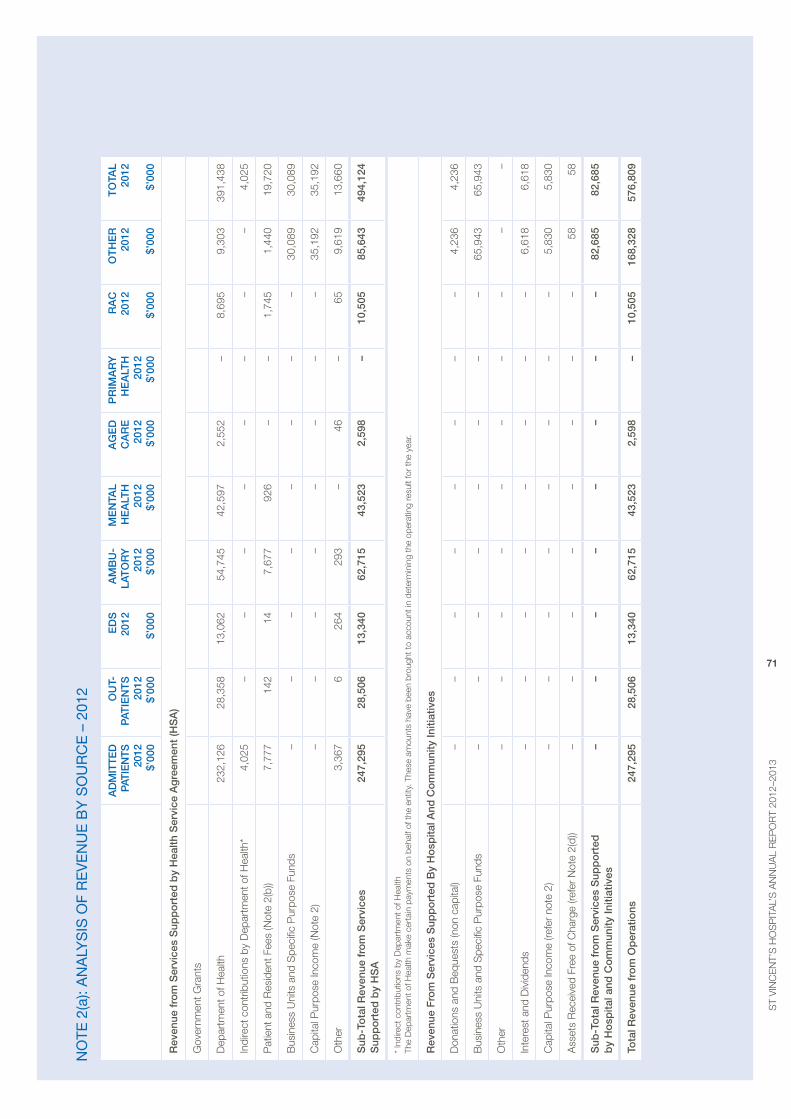
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
71
no
te 2
(a):
an
aly
SiS
of
re
Ve
nu
e b
y S
ou
rc
e –
201
2
AD
mIt
teD
pA
tIe
ntS
20
12
$’00
0
Ou
t-p
AtIe
nt
S
2012
$’
000
eD
S
2012
$’
000
Am
Bu
-LA
tO
Ry
20
12
$’00
0
me
ntA
L h
eA
Lth
20
12
$’00
0
Ag
eD
C
AR
e
2012
$’
000
pR
ImA
Ry
h
eA
Lth
20
12
$’00
0
RA
C
2012
$’
000
Ot
he
R
2012
$’
000
tO
tAL
2012
$’
000
Rev
enue
fro
m S
ervi
ces
Sup
po
rted
by
hea
lth S
ervi
ce A
gre
emen
t (h
SA
)
Gov
ernm
ent G
rant
s
Dep
artm
ent o
f Hea
lth 2
32,1
26 2
8,35
8 1
3,06
2 5
4,74
5 4
2,59
7 2
,552
–
8
,695
9
,303
3
91,4
38
Indi
rect
con
trib
utio
ns b
y D
epar
tmen
t of H
ealth
* 4,
025
–
–
–
–
–
–
–
–
4,02
5
pat
ient
and
res
iden
t Fee
s (N
ote
2(b)
) 7
,777
1
42
14
7,6
77
926
–
–
1
,745
1
,440
1
9,72
0
bus
ines
s U
nits
and
Spe
cific
pur
pose
Fun
ds
–
–
–
–
–
–
–
–
30,
089
30,
089
Cap
ital p
urpo
se In
com
e (N
ote
2) –
–
–
–
–
–
–
–
3
5,19
2 3
5,19
2
oth
er 3
,367
6
2
64
293
–
4
6 –
6
5 9
,619
1
3,66
0
Sub
-to
tal R
even
ue f
rom
Ser
vice
s S
upp
ort
ed b
y h
SA
2
47,2
95 2
8,50
6 1
3,34
0 6
2,71
5 4
3,52
3 2
,598
–
1
0,50
5 8
5,64
3 4
94,1
24
* In
dire
ct c
ontr
ibut
ions
by
Dep
artm
ent o
f Hea
lth
The
Dep
artm
ent o
f Hea
lth m
ake
cert
ain
paym
ents
on
beha
lf of
the
entit
y. T
hese
am
ount
s ha
ve b
een
brou
ght t
o ac
coun
t in
dete
rmin
ing
the
oper
atin
g re
sult
for
the
year
.
Rev
enue
Fro
m S
ervi
ces
Sup
po
rted
By
ho
spita
l And
Co
mm
unity
Initi
ativ
es
Don
atio
ns a
nd b
eque
sts
(non
cap
ital)
–
–
–
–
–
–
–
–
4,2
36
4,2
36
bus
ines
s U
nits
and
Spe
cific
pur
pose
Fun
ds –
–
–
–
–
–
–
–
6
5,94
3 6
5,94
3
oth
er –
–
–
–
–
–
–
–
–
–
Inte
rest
and
Div
iden
ds –
–
–
–
–
–
–
–
6
,618
6
,618
Cap
ital p
urpo
se In
com
e (re
fer
note
2)
–
–
–
–
–
–
–
–
5,8
30
5,83
0
ass
ets
rec
eive
d Fr
ee o
f Cha
rge
(refe
r N
ote
2(d)
) –
–
–
–
–
–
–
–
58
58
Sub
-to
tal R
even
ue f
rom
Ser
vice
s S
upp
ort
ed
by
ho
spita
l and
Co
mm
unity
Initi
ativ
es –
–
–
–
–
–
–
–
8
2,68
5 82
,685
tota
l Rev
enue
fro
m O
per
atio
ns 2
47,2
95
28,
506
13,
340
62,
715
43,
523
2,5
98
–
10,
505
168
,328
576,
809
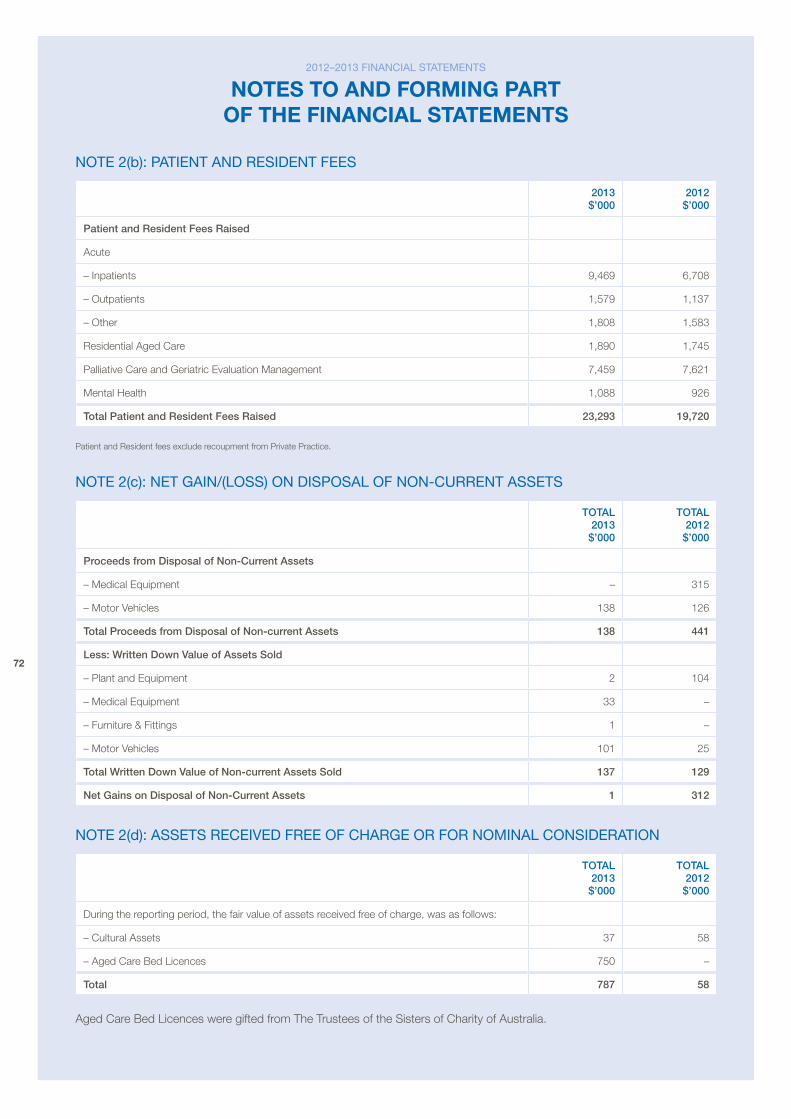
72
note 2(b): patient and reSident feeS
2013 $’000
2012 $’000
patient and Resident Fees Raised
acute
– Inpatients 9,469 6,708
– outpatients 1,579 1,137
– other 1,808 1,583
residential aged Care 1,890 1,745
palliative Care and Geriatric evaluation management 7,459 7,621
mental Health 1,088 926
total patient and Resident Fees Raised 23,293 19,720
patient and resident fees exclude recoupment from private practice.
note 2(c): net Gain/(loSS) on diSpoSal of non-current aSSetS
tOtAL 2013 $’000
tOtAL 2012 $’000
proceeds from Disposal of non-Current Assets
– medical equipment – 315
– motor vehicles 138 126
total proceeds from Disposal of non-current Assets 138 441
Less: written Down value of Assets Sold
– plant and equipment 2 104
– medical equipment 33 –
– Furniture & Fittings 1 –
– motor vehicles 101 25
total written Down value of non-current Assets Sold 137 129
net gains on Disposal of non-Current Assets 1 312
note 2(d): aSSetS receiVed free of cHarGe or for noMinal conSideration
tOtAL 2013 $’000
tOtAL 2012 $’000
During the reporting period, the fair value of assets received free of charge, was as follows:
– Cultural assets 37 58
– aged Care bed Licences 750 –
total 787 58
aged Care bed Licences were gifted from The Trustees of the Sisters of Charity of australia.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
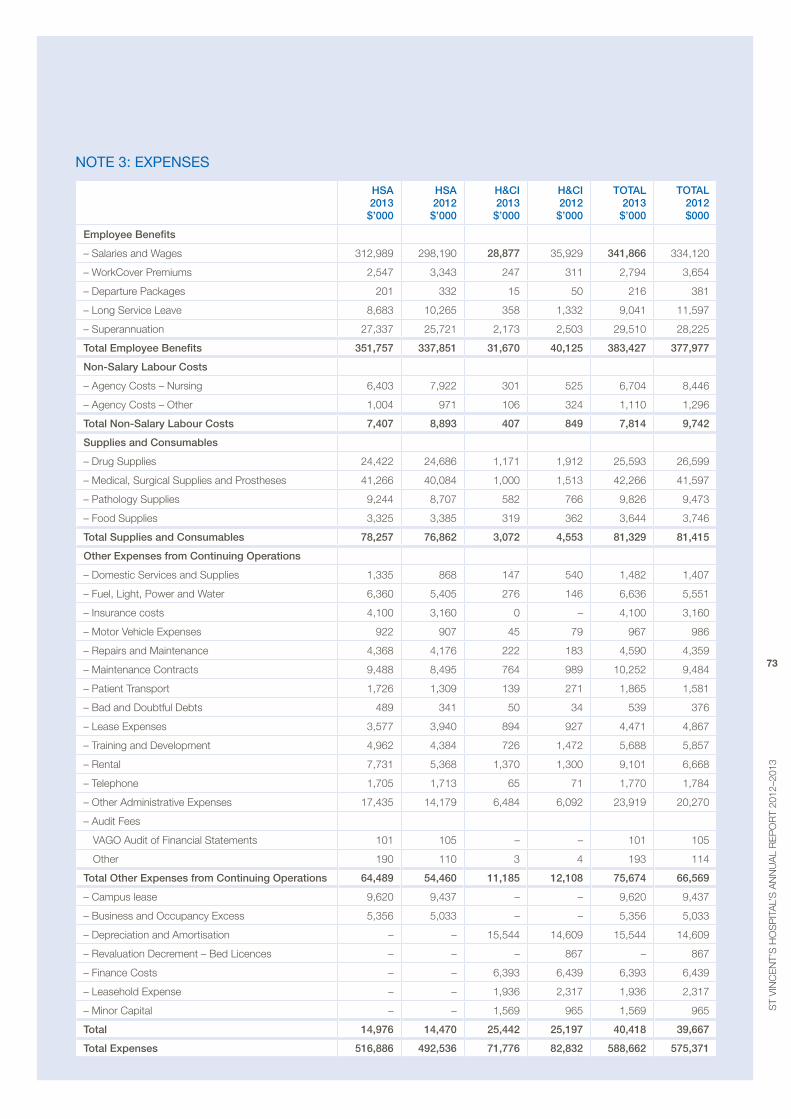
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
73
note 3: expenSeS
hSA 2013 $’000
hSA 2012 $’000
h&CI 2013 $’000
h&CI 2012 $’000
tOtAL 2013 $’000
tOtAL 2012 $000
employee Benefits
– Salaries and Wages 312,989 298,190 28,877 35,929 341,866 334,120
– WorkCover premiums 2,547 3,343 247 311 2,794 3,654
– Departure packages 201 332 15 50 216 381
– Long Service Leave 8,683 10,265 358 1,332 9,041 11,597
– Superannuation 27,337 25,721 2,173 2,503 29,510 28,225
total employee Benefits 351,757 337,851 31,670 40,125 383,427 377,977
non-Salary Labour Costs
– agency Costs – Nursing 6,403 7,922 301 525 6,704 8,446
– agency Costs – other 1,004 971 106 324 1,110 1,296
total non-Salary Labour Costs 7,407 8,893 407 849 7,814 9,742
Supplies and Consumables
– Drug Supplies 24,422 24,686 1,171 1,912 25,593 26,599
– medical, Surgical Supplies and prostheses 41,266 40,084 1,000 1,513 42,266 41,597
– pathology Supplies 9,244 8,707 582 766 9,826 9,473
– Food Supplies 3,325 3,385 319 362 3,644 3,746
total Supplies and Consumables 78,257 76,862 3,072 4,553 81,329 81,415
Other expenses from Continuing Operations
– Domestic Services and Supplies 1,335 868 147 540 1,482 1,407
– Fuel, Light, power and Water 6,360 5,405 276 146 6,636 5,551
– Insurance costs 4,100 3,160 0 – 4,100 3,160
– motor vehicle expenses 922 907 45 79 967 986
– repairs and maintenance 4,368 4,176 222 183 4,590 4,359
– maintenance Contracts 9,488 8,495 764 989 10,252 9,484
– patient Transport 1,726 1,309 139 271 1,865 1,581
– bad and Doubtful Debts 489 341 50 34 539 376
– Lease expenses 3,577 3,940 894 927 4,471 4,867
– Training and Development 4,962 4,384 726 1,472 5,688 5,857
– rental 7,731 5,368 1,370 1,300 9,101 6,668
– Telephone 1,705 1,713 65 71 1,770 1,784
– other administrative expenses 17,435 14,179 6,484 6,092 23,919 20,270
– audit Fees
vaGo audit of Financial Statements 101 105 – – 101 105
other 190 110 3 4 193 114
total Other expenses from Continuing Operations 64,489 54,460 11,185 12,108 75,674 66,569
– Campus lease 9,620 9,437 – – 9,620 9,437
– business and occupancy excess 5,356 5,033 – – 5,356 5,033
– Depreciation and amortisation – – 15,544 14,609 15,544 14,609
– revaluation Decrement – bed Licences – – – 867 – 867
– Finance Costs – – 6,393 6,439 6,393 6,439
– Leasehold expense – – 1,936 2,317 1,936 2,317
– minor Capital – – 1,569 965 1,569 965
total 14,976 14,470 25,442 25,197 40,418 39,667
total expenses 516,886 492,536 71,776 82,832 588,662 575,371
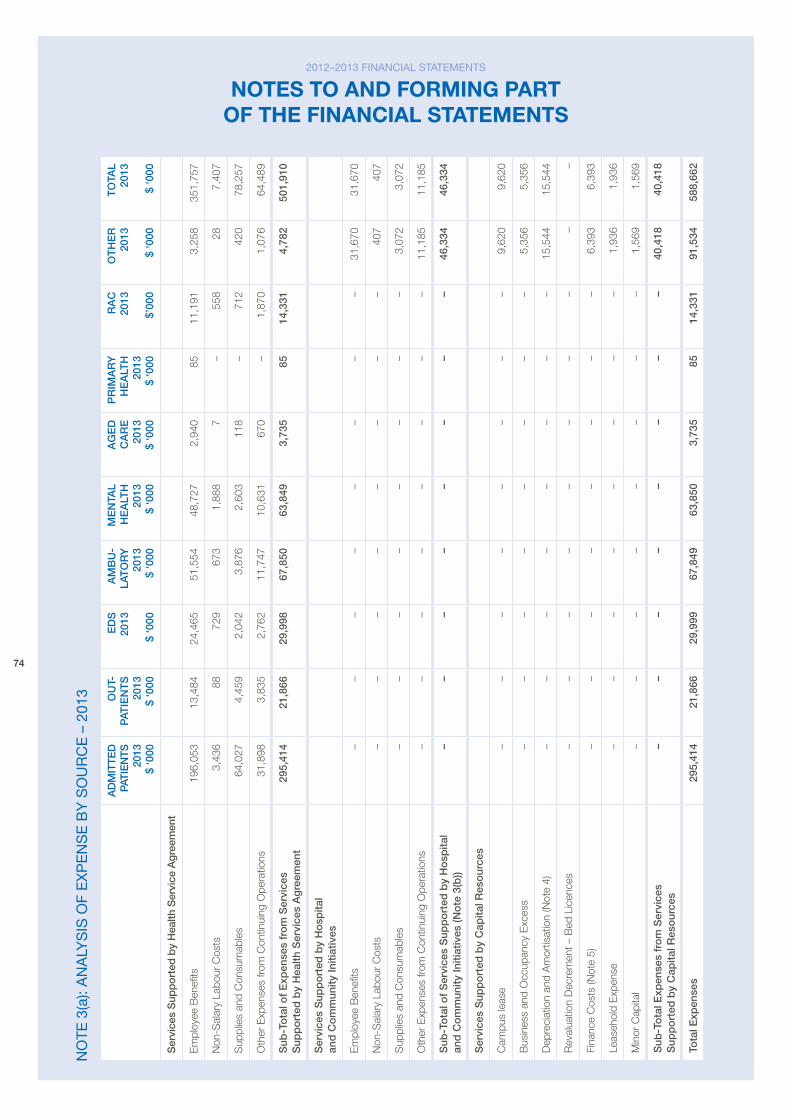
74
no
te 3
(a):
an
aly
SiS
of
ex
pe
nS
e b
y S
ou
rc
e –
201
3
AD
mIt
teD
pA
tIe
ntS
20
13
$ ‘0
00
Ou
t-p
AtIe
nt
S
2013
$
‘000
eD
S
201
3 $
‘000
Am
Bu
-LA
tO
Ry
20
13
$ ‘0
00
me
ntA
L h
eA
Lth
20
13
$ ‘0
00
Ag
eD
C
AR
e
2013
$
‘000
pR
ImA
Ry
h
eA
Lth
20
13
$ ‘0
00
RA
C
2013
$’
000
Ot
he
R
2013
$
‘000
tO
tAL
2013
$
‘000
Ser
vice
s S
upp
orte
d b
y h
ealth
Ser
vice
Agr
eem
ent
em
ploy
ee b
enefi
ts19
6,05
313
,484
24,4
6551
,554
48,7
272,
940
8511
,191
3,25
835
1,75
7
Non
-Sal
ary
Labo
ur C
osts
3,43
688
729
673
1,88
87
–
558
287,
407
Sup
plie
s an
d C
onsu
mab
les
64,0
274,
459
2,04
23,
876
2,60
311
8 –
71
242
078
,257
oth
er e
xpen
ses
from
Con
tinui
ng o
pera
tions
31,8
983,
835
2,76
211
,747
10,6
3167
0 –
1,
870
1,07
664
,489
Sub
-to
tal o
f e
xpen
ses
fro
m S
ervi
ces
Sup
po
rted
by
hea
lth S
ervi
ces
Ag
reem
ent
295,
414
21,8
6629
,998
67,8
5063
,849
3,73
585
14,3
314,
782
501,
910
Ser
vice
s S
upp
ort
ed b
y h
osp
ital
and
Co
mm
unity
Initi
ativ
es
em
ploy
ee b
enefi
ts –
–
–
–
–
–
–
–
31
,670
31,6
70
Non
-Sal
ary
Labo
ur C
osts
–
–
–
–
–
–
–
–
407
407
Sup
plie
s an
d C
onsu
mab
les
–
–
–
–
–
–
–
–
3,07
23,
072
oth
er e
xpen
ses
from
Con
tinui
ng o
pera
tions
–
–
–
–
–
–
–
–
11,1
8511
,185
Sub
-to
tal o
f S
ervi
ces
Sup
po
rted
by
ho
spita
l an
d C
om
mun
ity In
itiat
ives
(no
te 3
(b))
–
–
–
–
–
–
–
–
46,3
3446
,334
Ser
vice
s S
upp
ort
ed b
y C
apita
l Res
our
ces
Cam
pus
leas
e –
–
–
–
–
–
–
–
9,
620
9,62
0
bus
ines
s an
d o
ccup
ancy
exc
ess
–
–
–
–
–
–
–
–
5,35
65,
356
Dep
reci
atio
n an
d a
mor
tisat
ion
(Not
e 4)
–
–
–
–
–
–
–
–
15,5
4415
,544
rev
alua
tion
Dec
rem
ent –
bed
Lic
ence
s –
–
–
–
–
–
–
–
–
–
Fina
nce
Cos
ts (N
ote
5) –
–
–
–
–
–
–
–
6,
393
6,39
3
Leas
ehol
d e
xpen
se –
–
–
–
–
–
–
–
1,
936
1,93
6
min
or C
apita
l –
–
–
–
–
–
–
–
1,
569
1,56
9
Sub
-to
tal e
xpen
ses
fro
m S
ervi
ces
Sup
po
rted
by
Cap
ital R
eso
urce
s –
–
–
–
–
–
–
–
40
,418
40,4
18
tota
l exp
ense
s 2
95,4
14
21,
866
29,
999
67,
849
63,
850
3,7
35
85
14,
331
91,5
3458
8,66
2
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
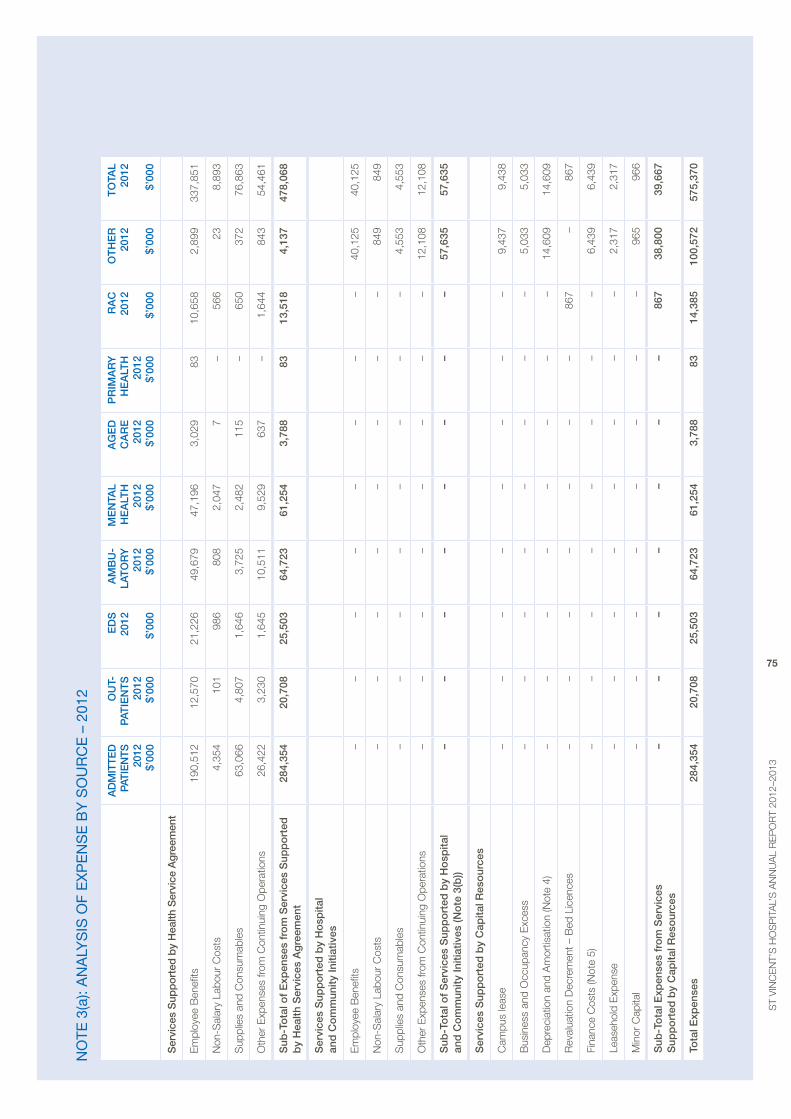
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
75
no
te 3
(a):
an
aly
SiS
of
ex
pe
nS
e b
y S
ou
rc
e –
201
2
AD
mIt
teD
pA
tIe
ntS
20
12
$’00
0
Ou
t-p
AtIe
nt
S
2012
$’
000
eD
S
2012
$’
000
Am
Bu
-LA
tO
Ry
20
12
$’00
0
me
ntA
L h
eA
Lth
20
12
$’00
0
Ag
eD
C
AR
e
2012
$’
000
pR
ImA
Ry
h
eA
Lth
20
12
$’00
0
RA
C
2012
$’
000
Ot
he
R
2012
$’
000
tO
tAL
2012
$’
000
Ser
vice
s S
upp
orte
d b
y h
ealth
Ser
vice
Agr
eem
ent
em
ploy
ee b
enefi
ts 1
90,5
12
12,
570
21,
226
49,
679
47,
196
3,0
29
83
10,
658
2,8
99
337
,851
Non
-Sal
ary
Labo
ur C
osts
4,3
54
101
9
86
808
2
,047
7
–
5
66
23
8,8
93
Sup
plie
s an
d C
onsu
mab
les
63,
066
4,8
07
1,6
46
3,7
25
2,4
82
115
–
6
50
372
7
6,86
3
oth
er e
xpen
ses
from
Con
tinui
ng o
pera
tions
26,
422
3,2
30
1,6
45
10,
511
9,5
29
637
–
1
,644
8
43
54,
461
Sub
-to
tal o
f e
xpen
ses
fro
m S
ervi
ces
Sup
po
rted
b
y h
ealth
Ser
vice
s A
gre
emen
t 2
84,3
54
20,
708
25,
503
64,
723
61,
254
3,7
88
83
13,
518
4,1
37
478
,068
Ser
vice
s S
upp
ort
ed b
y h
osp
ital
and
Co
mm
unity
Initi
ativ
es
em
ploy
ee b
enefi
ts –
–
–
–
–
–
–
–
4
0,12
5 4
0,12
5
Non
-Sal
ary
Labo
ur C
osts
–
–
–
–
–
–
–
–
849
8
49
Sup
plie
s an
d C
onsu
mab
les
–
–
–
–
–
–
–
–
4,5
53
4,5
53
oth
er e
xpen
ses
from
Con
tinui
ng o
pera
tions
–
–
–
–
–
–
–
–
12,
108
12,
108
Sub
-to
tal o
f S
ervi
ces
Sup
po
rted
by
ho
spita
l an
d C
om
mun
ity In
itiat
ives
(no
te 3
(b))
–
–
–
–
–
–
–
–
57,
635
57,
635
Ser
vice
s S
upp
ort
ed b
y C
apita
l Res
our
ces
Cam
pus
leas
e –
–
–
–
–
–
–
–
9
,437
9
,438
bus
ines
s an
d o
ccup
ancy
exc
ess
–
–
–
–
–
–
–
–
5,0
33
5,0
33
Dep
reci
atio
n an
d a
mor
tisat
ion
(Not
e 4)
–
–
–
–
–
–
–
–
14,
609
14,
609
rev
alua
tion
Dec
rem
ent –
bed
Lic
ence
s –
–
–
–
–
–
–
86
7–
867
Fina
nce
Cos
ts (N
ote
5) –
–
–
–
–
–
–
–
6,4
39
6,4
39
Leas
ehol
d e
xpen
se –
–
–
–
–
–
–
–
2
,317
2
,317
min
or C
apita
l –
–
–
–
–
–
–
–
9
65
966
Sub
-to
tal e
xpen
ses
fro
m S
ervi
ces
Sup
po
rted
by
Cap
ital R
eso
urce
s –
–
–
–
–
–
–
86
738
,800
39,6
67
tota
l exp
ense
s 2
84,3
54
20,
708
25,
503
64,
723
61,
254
3,7
88
83
14,
385
100
,572
5
75,3
70
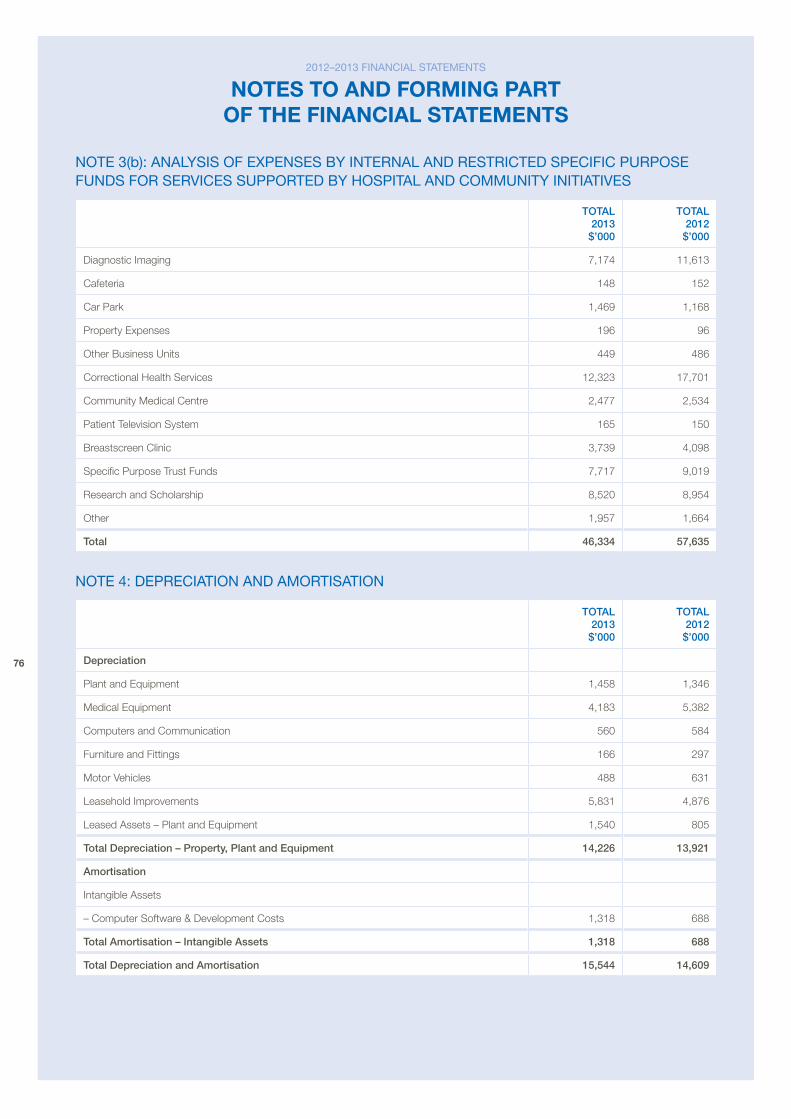
76
note 3(b): analySiS of expenSeS by internal and reStricted Specific purpoSe fundS for SerViceS Supported by HoSpital and coMMunity initiatiVeS
tOtAL 2013 $’000
tOtAL 2012 $’000
Diagnostic Imaging 7,174 11,613
Cafeteria 148 152
Car park 1,469 1,168
property expenses 196 96
other business Units 449 486
Correctional Health Services 12,323 17,701
Community medical Centre 2,477 2,534
patient Television System 165 150
breastscreen Clinic 3,739 4,098
Specific purpose Trust Funds 7,717 9,019
research and Scholarship 8,520 8,954
other 1,957 1,664
total 46,334 57,635
note 4: depreciation and aMortiSation
tOtAL 2013 $’000
tOtAL 2012 $’000
Depreciation
plant and equipment 1,458 1,346
medical equipment 4,183 5,382
Computers and Communication 560 584
Furniture and Fittings 166 297
motor vehicles 488 631
Leasehold Improvements 5,831 4,876
Leased assets – plant and equipment 1,540 805
total Depreciation – property, plant and equipment 14,226 13,921
Amortisation
Intangible assets
– Computer Software & Development Costs 1,318 688
total Amortisation – Intangible Assets 1,318 688
total Depreciation and Amortisation 15,544 14,609
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
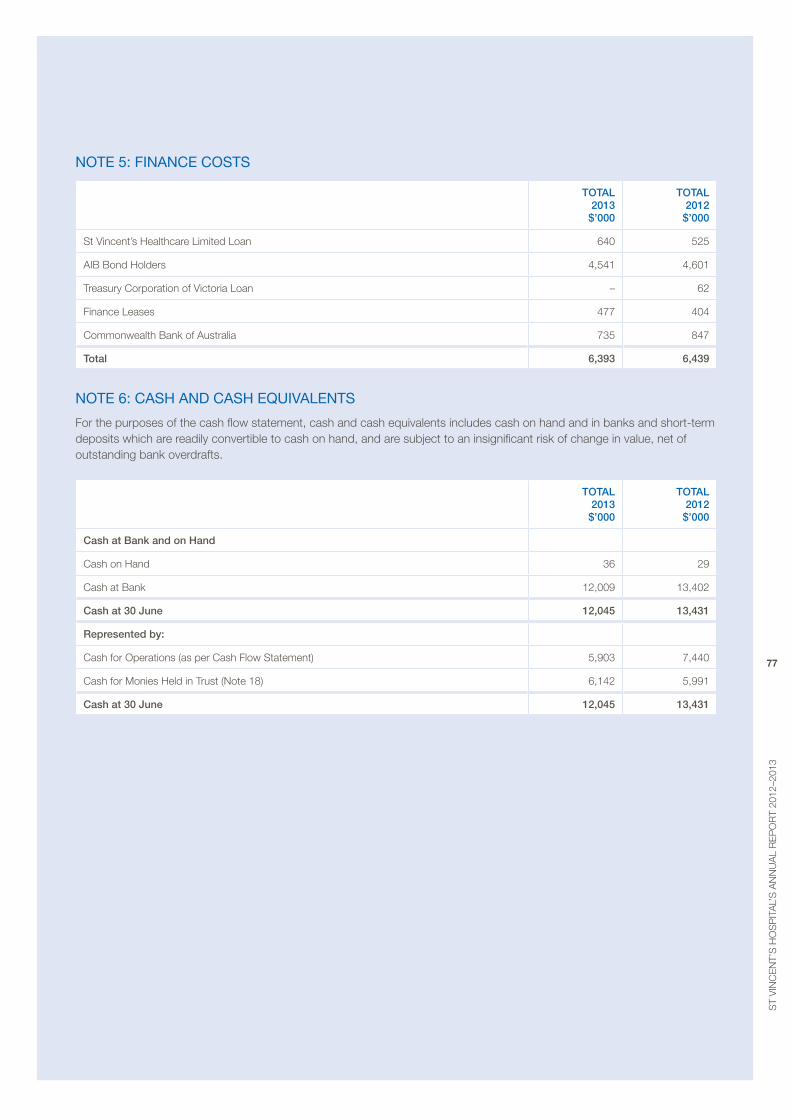
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
77
note 5: finance coStS
tOtAL 2013 $’000
tOtAL 2012 $’000
St vincent’s Healthcare Limited Loan 640 525
aIb bond Holders 4,541 4,601
Treasury Corporation of victoria Loan – 62
Finance Leases 477 404
Commonwealth bank of australia 735 847
total 6,393 6,439
note 6: caSH and caSH equiValentS
For the purposes of the cash flow statement, cash and cash equivalents includes cash on hand and in banks and short-term deposits which are readily convertible to cash on hand, and are subject to an insignificant risk of change in value, net of outstanding bank overdrafts.
tOtAL 2013 $’000
tOtAL 2012 $’000
Cash at Bank and on hand
Cash on Hand 36 29
Cash at bank 12,009 13,402
Cash at 30 june 12,045 13,431
Represented by:
Cash for operations (as per Cash Flow Statement) 5,903 7,440
Cash for monies Held in Trust (Note 18) 6,142 5,991
Cash at 30 june 12,045 13,431
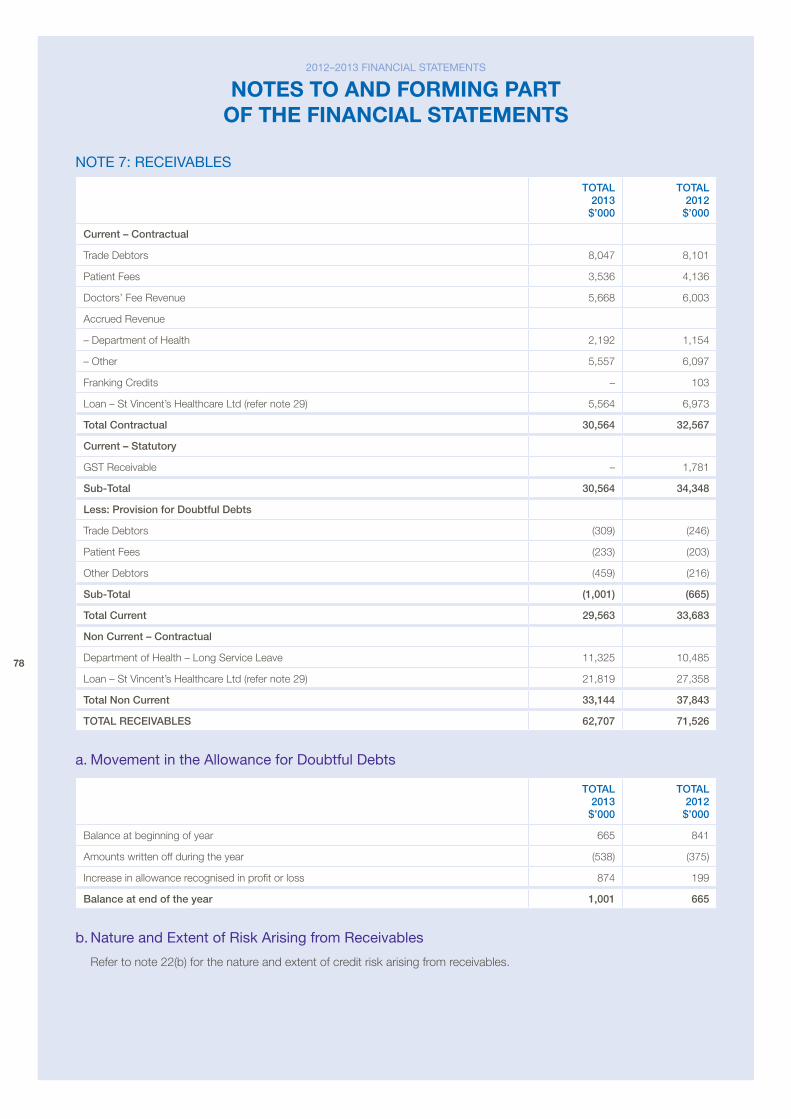
78
note 7: receiVableS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current – Contractual
Trade Debtors 8,047 8,101
patient Fees 3,536 4,136
Doctors’ Fee revenue 5,668 6,003
accrued revenue
– Department of Health 2,192 1,154
– other 5,557 6,097
Franking Credits – 103
Loan – St vincent’s Healthcare Ltd (refer note 29) 5,564 6,973
total Contractual 30,564 32,567
Current – Statutory
GST receivable – 1,781
Sub-total 30,564 34,348
Less: provision for Doubtful Debts
Trade Debtors (309) (246)
patient Fees (233) (203)
other Debtors (459) (216)
Sub-total (1,001) (665)
total Current 29,563 33,683
non Current – Contractual
Department of Health – Long Service Leave 11,325 10,485
Loan – St vincent’s Healthcare Ltd (refer note 29) 21,819 27,358
total non Current 33,144 37,843
tOtAL ReCeIvABLeS 62,707 71,526
a. Movement in the allowance for doubtful debts
tOtAL 2013 $’000
tOtAL 2012 $’000
balance at beginning of year 665 841
amounts written off during the year (538) (375)
Increase in allowance recognised in profit or loss 874 199
Balance at end of the year 1,001 665
b. nature and extent of risk arising from receivables
refer to note 22(b) for the nature and extent of credit risk arising from receivables.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
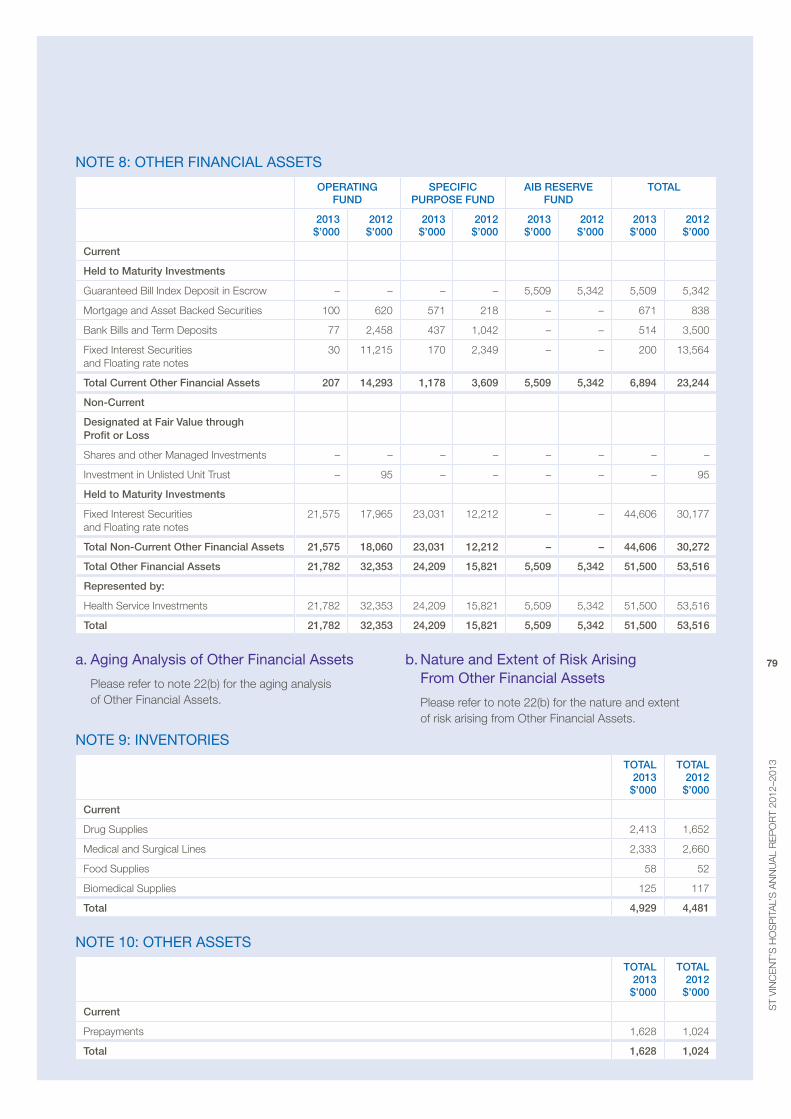
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
79
note 8: otHer financial aSSetS
OpeRAtIng FunD
SpeCIFIC puRpOSe FunD
AIB ReSeRve FunD
tOtAL
2013 $’000
2012 $’000
2013 $’000
2012 $’000
2013 $’000
2012 $’000
2013 $’000
2012 $’000
Current
held to maturity Investments
Guaranteed bill Index Deposit in escrow – – – – 5,509 5,342 5,509 5,342
mortgage and asset backed Securities 100 620 571 218 – – 671 838
bank bills and Term Deposits 77 2,458 437 1,042 – – 514 3,500
Fixed Interest Securities and Floating rate notes
30 11,215 170 2,349 – – 200 13,564
total Current Other Financial Assets 207 14,293 1,178 3,609 5,509 5,342 6,894 23,244
non-Current
Designated at Fair value through profit or Loss
Shares and other managed Investments – – – – – – – –
Investment in Unlisted Unit Trust – 95 – – – – – 95
held to maturity Investments
Fixed Interest Securities and Floating rate notes
21,575 17,965 23,031 12,212 – – 44,606 30,177
total non-Current Other Financial Assets 21,575 18,060 23,031 12,212 – – 44,606 30,272
total Other Financial Assets 21,782 32,353 24,209 15,821 5,509 5,342 51,500 53,516
Represented by:
Health Service Investments 21,782 32,353 24,209 15,821 5,509 5,342 51,500 53,516
total 21,782 32,353 24,209 15,821 5,509 5,342 51,500 53,516
a. aging analysis of other financial assets
please refer to note 22(b) for the aging analysis of other Financial assets.
b. nature and extent of risk arising from other financial assets
please refer to note 22(b) for the nature and extent of risk arising from other Financial assets.
note 9: inVentorieS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current
Drug Supplies 2,413 1,652
medical and Surgical Lines 2,333 2,660
Food Supplies 58 52
biomedical Supplies 125 117
total 4,929 4,481
note 10: otHer aSSetS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current
prepayments 1,628 1,024
total 1,628 1,024
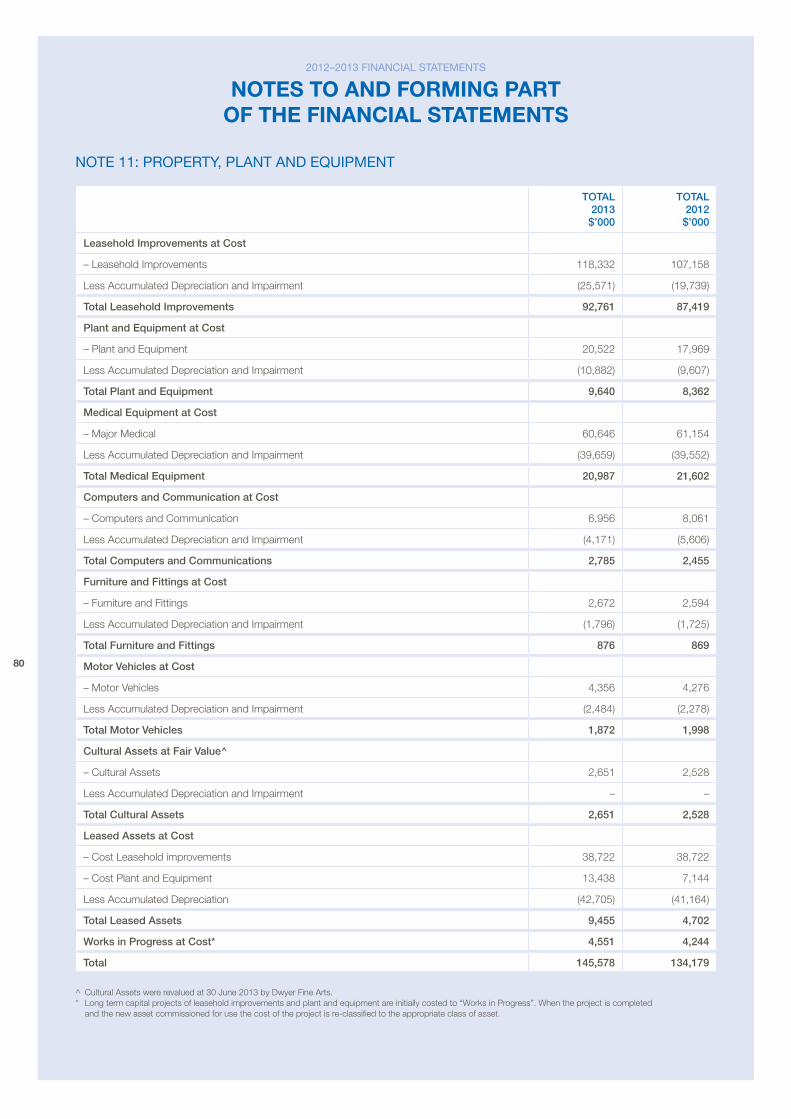
80
note 11: property, plant and equipMent
tOtAL 2013 $’000
tOtAL 2012 $’000
Leasehold Improvements at Cost
– Leasehold Improvements 118,332 107,158
Less accumulated Depreciation and Impairment (25,571) (19,739)
total Leasehold Improvements 92,761 87,419
plant and equipment at Cost
– plant and equipment 20,522 17,969
Less accumulated Depreciation and Impairment (10,882) (9,607)
total plant and equipment 9,640 8,362
medical equipment at Cost
– major medical 60,646 61,154
Less accumulated Depreciation and Impairment (39,659) (39,552)
total medical equipment 20,987 21,602
Computers and Communication at Cost
– Computers and Communication 6,956 8,061
Less accumulated Depreciation and Impairment (4,171) (5,606)
total Computers and Communications 2,785 2,455
Furniture and Fittings at Cost
– Furniture and Fittings 2,672 2,594
Less accumulated Depreciation and Impairment (1,796) (1,725)
total Furniture and Fittings 876 869
motor vehicles at Cost
– motor vehicles 4,356 4,276
Less accumulated Depreciation and Impairment (2,484) (2,278)
total motor vehicles 1,872 1,998
Cultural Assets at Fair value^
– Cultural assets 2,651 2,528
Less accumulated Depreciation and Impairment – –
total Cultural Assets 2,651 2,528
Leased Assets at Cost
– Cost Leasehold improvements 38,722 38,722
– Cost plant and equipment 13,438 7,144
Less accumulated Depreciation (42,705) (41,164)
total Leased Assets 9,455 4,702
works in progress at Cost* 4,551 4,244
total 145,578 134,179
^ Cultural assets were revalued at 30 June 2013 by Dwyer Fine arts. * Long term capital projects of leasehold improvements and plant and equipment are initially costed to “Works in progress”. When the project is completed
and the new asset commissioned for use the cost of the project is re-classified to the appropriate class of asset.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
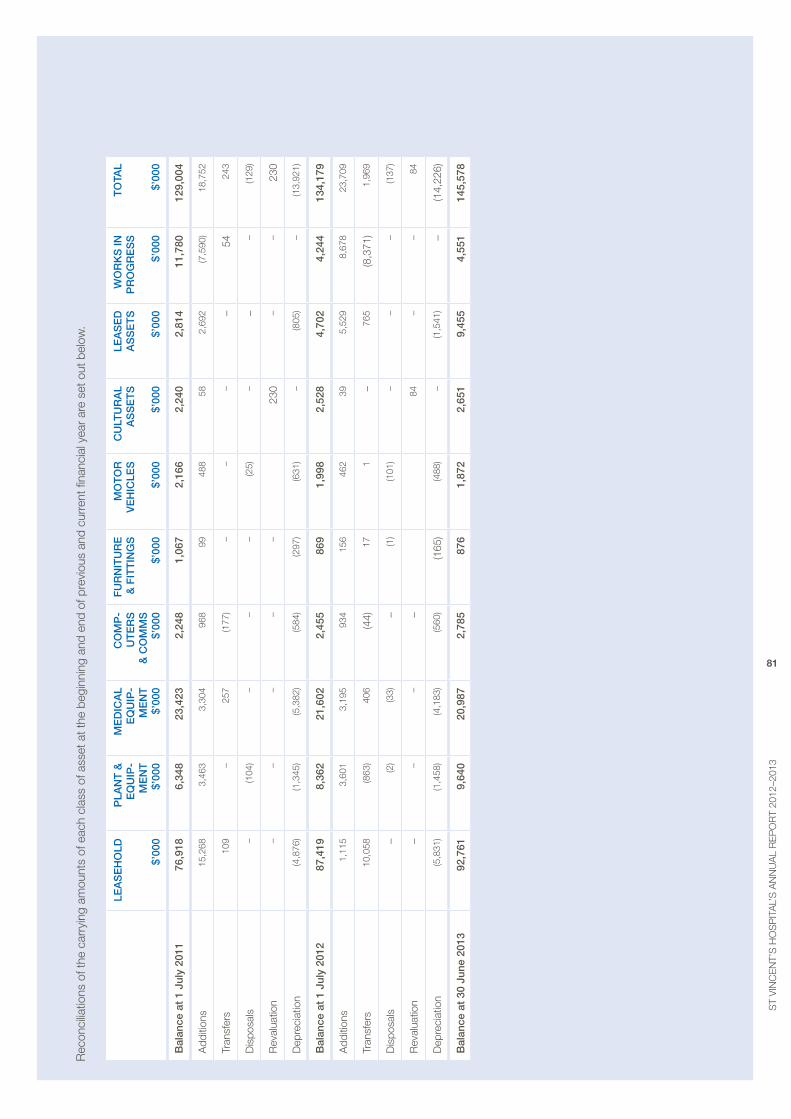
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
81
rec
onci
liatio
ns o
f the
car
ryin
g am
ount
s of
eac
h cl
ass
of a
sset
at t
he b
egin
ning
and
end
of p
revi
ous
and
curr
ent fi
nanc
ial y
ear
are
set o
ut b
elow
.
LeA
Se
hO
LD
$’00
0
pLA
nt
&
eQ
uIp
-m
en
t
$’00
0
me
DIC
AL
eQ
uIp
-m
en
t
$’00
0
CO
mp
-u
te
RS
&
CO
mm
S
$’00
0
Fu
Rn
Itu
Re
&
FIt
tIn
gS
$’
000
mO
tO
R
ve
hIC
LeS
$’
000
Cu
Ltu
RA
L A
SS
et
S
$’00
0
LeA
Se
D
AS
Se
tS
$’
000
wO
Rk
S In
p
RO
gR
eS
S
$’00
0
tO
tAL
$’00
0
Bal
ance
at
1 ju
ly 2
011
76,9
186,
348
23,4
232,
248
1,06
72,
166
2,24
02,
814
11,7
8012
9,00
4
add
ition
s15
,268
3,46
33,
304
968
9948
858
2,69
2(7
,590
)18
,752
Tran
sfer
s10
9–
257
(177
)–
––
–54
243
Dis
posa
ls–
(104
)–
––
(25)
––
–(1
29)
rev
alua
tion
––
––
–23
0–
–23
0
Dep
reci
atio
n(4
,876
)(1
,345
)(5
,382
)(5
84)
(297
)(6
31)
–(8
05)
–(1
3,92
1)
Bal
ance
at
1 ju
ly 2
012
87,4
198,
362
21,6
022,
455
869
1,99
82,
528
4,70
24,
244
134,
179
add
ition
s 1
,115
3,6
01
3,1
95
934
1
56
462
3
9 5
,529
8
,678
2
3,70
9
Tran
sfer
s 1
0,05
8 (8
63)
406
(4
4) 1
7 1
– 7
65
(8,3
71)
1,9
69
Dis
posa
ls–
(2)
(33)
– (1
) (1
01)
––
– (1
37)
rev
alua
tion
––
––
84–
– 8
4
Dep
reci
atio
n (5
,831
) (1
,458
) (4
,183
) (5
60)
(165
) (4
88)
–
(1,5
41)
–(1
4,22
6)
Bal
ance
at
30 j
une
2013
92,
761
9,6
40
20,
987
2,7
85 8
76
1,8
72
2,6
51
9,4
55
4,5
51
145
,578
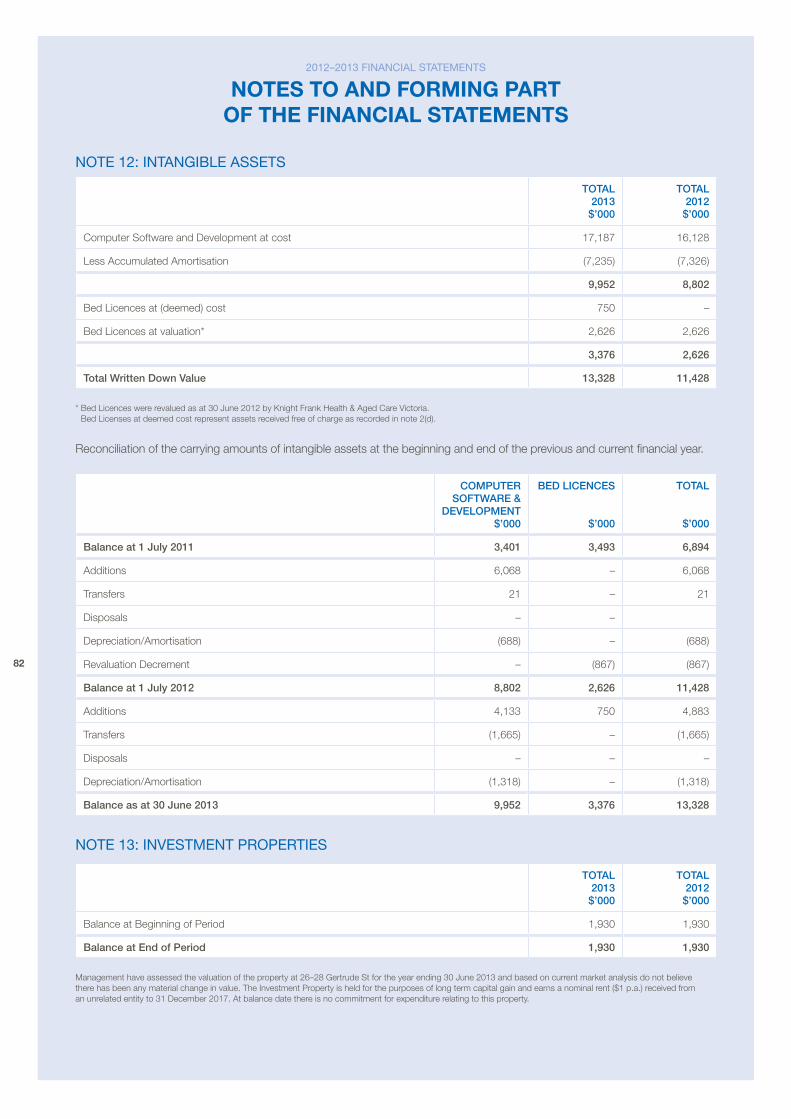
82
note 12: intanGible aSSetS
tOtAL 2013 $’000
tOtAL 2012 $’000
Computer Software and Development at cost 17,187 16,128
Less accumulated amortisation (7,235) (7,326)
9,952 8,802
bed Licences at (deemed) cost 750 –
bed Licences at valuation* 2,626 2,626
3,376 2,626
total written Down value 13,328 11,428
* bed Licences were revalued as at 30 June 2012 by Knight Frank Health & aged Care victoria. bed Licenses at deemed cost represent assets received free of charge as recorded in note 2(d).
reconciliation of the carrying amounts of intangible assets at the beginning and end of the previous and current financial year.
COmputeR SOFtwARe &
DeveLOpment $’000
BeD LICenCeS
$’000
tOtAL
$’000
Balance at 1 july 2011 3,401 3,493 6,894
additions 6,068 – 6,068
Transfers 21 – 21
Disposals – –
Depreciation/amortisation (688) – (688)
revaluation Decrement – (867) (867)
Balance at 1 july 2012 8,802 2,626 11,428
additions 4,133 750 4,883
Transfers (1,665) – (1,665)
Disposals – – –
Depreciation/amortisation (1,318) – (1,318)
Balance as at 30 june 2013 9,952 3,376 13,328
note 13: inVeStMent propertieS
tOtAL 2013 $’000
tOtAL 2012 $’000
balance at beginning of period 1,930 1,930
Balance at end of period 1,930 1,930
management have assessed the valuation of the property at 26–28 Gertrude St for the year ending 30 June 2013 and based on current market analysis do not believe there has been any material change in value. The Investment property is held for the purposes of long term capital gain and earns a nominal rent ($1 p.a.) received from an unrelated entity to 31 December 2017. at balance date there is no commitment for expenditure relating to this property.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
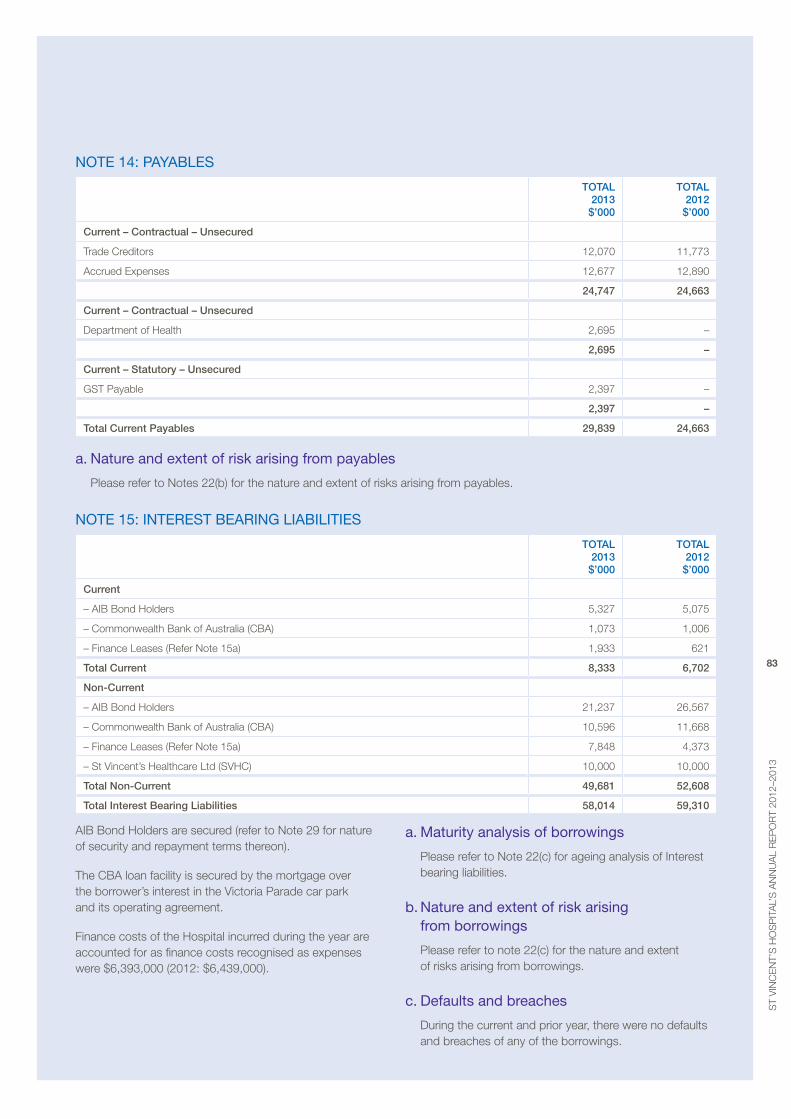
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
83
note 14: payableS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current – Contractual – unsecured
Trade Creditors 12,070 11,773
accrued expenses 12,677 12,890
24,747 24,663
Current – Contractual – unsecured
Department of Health 2,695 –
2,695 –
Current – Statutory – unsecured
GST payable 2,397 –
2,397 –
total Current payables 29,839 24,663
a. nature and extent of risk arising from payables
please refer to Notes 22(b) for the nature and extent of risks arising from payables.
note 15: intereSt bearinG liabilitieS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current
– aIb bond Holders 5,327 5,075
– Commonwealth bank of australia (Cba) 1,073 1,006
– Finance Leases (refer Note 15a) 1,933 621
total Current 8,333 6,702
non-Current
– aIb bond Holders 21,237 26,567
– Commonwealth bank of australia (Cba) 10,596 11,668
– Finance Leases (refer Note 15a) 7,848 4,373
– St vincent’s Healthcare Ltd (SvHC) 10,000 10,000
total non-Current 49,681 52,608
total Interest Bearing Liabilities 58,014 59,310
aIb bond Holders are secured (refer to Note 29 for nature of security and repayment terms thereon).
The Cba loan facility is secured by the mortgage over the borrower’s interest in the victoria parade car park and its operating agreement.
Finance costs of the Hospital incurred during the year are accounted for as finance costs recognised as expenses were $6,393,000 (2012: $6,439,000).
a. Maturity analysis of borrowings
please refer to Note 22(c) for ageing analysis of Interest bearing liabilities.
b. nature and extent of risk arising from borrowings
please refer to note 22(c) for the nature and extent of risks arising from borrowings.
c. defaults and breaches
During the current and prior year, there were no defaults and breaches of any of the borrowings.
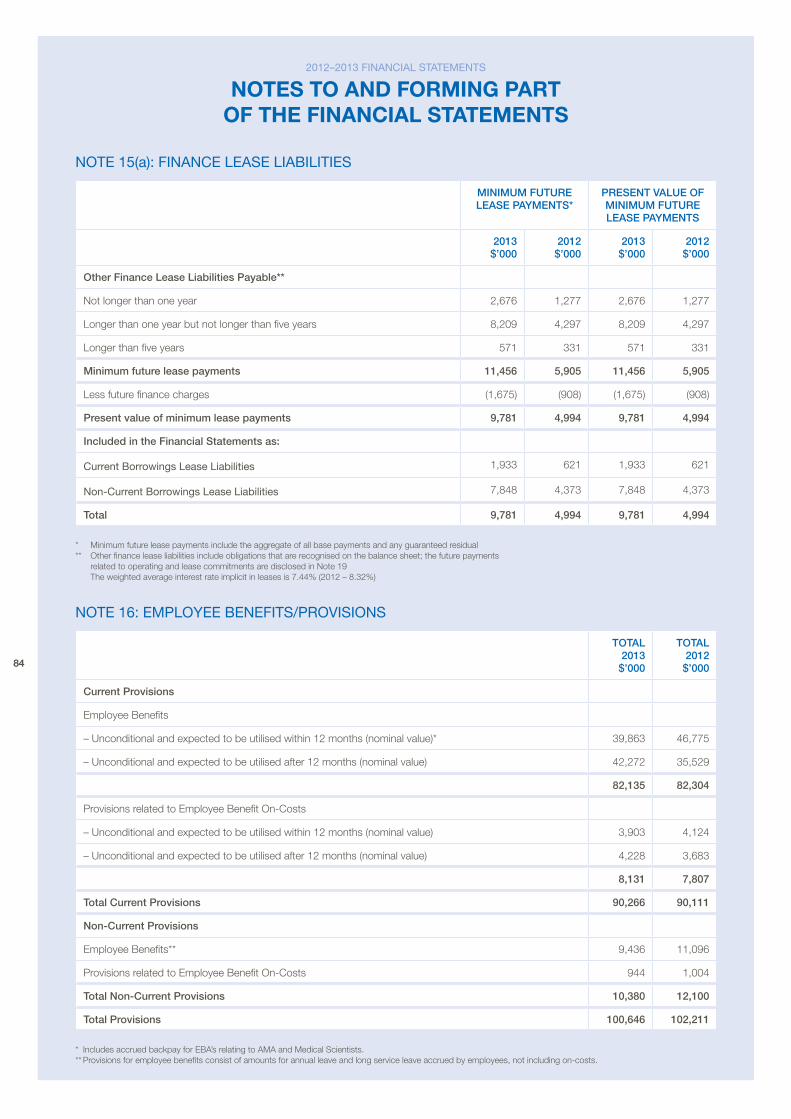
84
note 15(a): finance leaSe liabilitieS
mInImum FutuRe LeASe pAymentS*
pReSent vALue OF mInImum FutuRe LeASe pAymentS
2013 $’000
2012 $’000
2013 $’000
2012 $’000
Other Finance Lease Liabilities payable**
Not longer than one year 2,676 1,277 2,676 1,277
Longer than one year but not longer than five years 8,209 4,297 8,209 4,297
Longer than five years 571 331 571 331
minimum future lease payments 11,456 5,905 11,456 5,905
Less future finance charges (1,675) (908) (1,675) (908)
present value of minimum lease payments 9,781 4,994 9,781 4,994
Included in the Financial Statements as:
Current Borrowings Lease Liabilities 1,933 621 1,933 621
Non-Current Borrowings Lease Liabilities 7,848 4,373 7,848 4,373
total 9,781 4,994 9,781 4,994
* minimum future lease payments include the aggregate of all base payments and any guaranteed residual ** other finance lease liabilities include obligations that are recognised on the balance sheet; the future payments
related to operating and lease commitments are disclosed in Note 19 The weighted average interest rate implicit in leases is 7.44% (2012 – 8.32%)
note 16: eMployee benefitS/proViSionS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current provisions
employee benefits
– Unconditional and expected to be utilised within 12 months (nominal value)* 39,863 46,775
– Unconditional and expected to be utilised after 12 months (nominal value) 42,272 35,529
82,135 82,304
provisions related to employee benefit on-Costs
– Unconditional and expected to be utilised within 12 months (nominal value) 3,903 4,124
– Unconditional and expected to be utilised after 12 months (nominal value) 4,228 3,683
8,131 7,807
total Current provisions 90,266 90,111
non-Current provisions
employee benefits** 9,436 11,096
provisions related to employee benefit on-Costs 944 1,004
total non-Current provisions 10,380 12,100
total provisions 100,646 102,211
* Includes accrued backpay for eba’s relating to ama and medical Scientists. ** provisions for employee benefits consist of amounts for annual leave and long service leave accrued by employees, not including on-costs.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
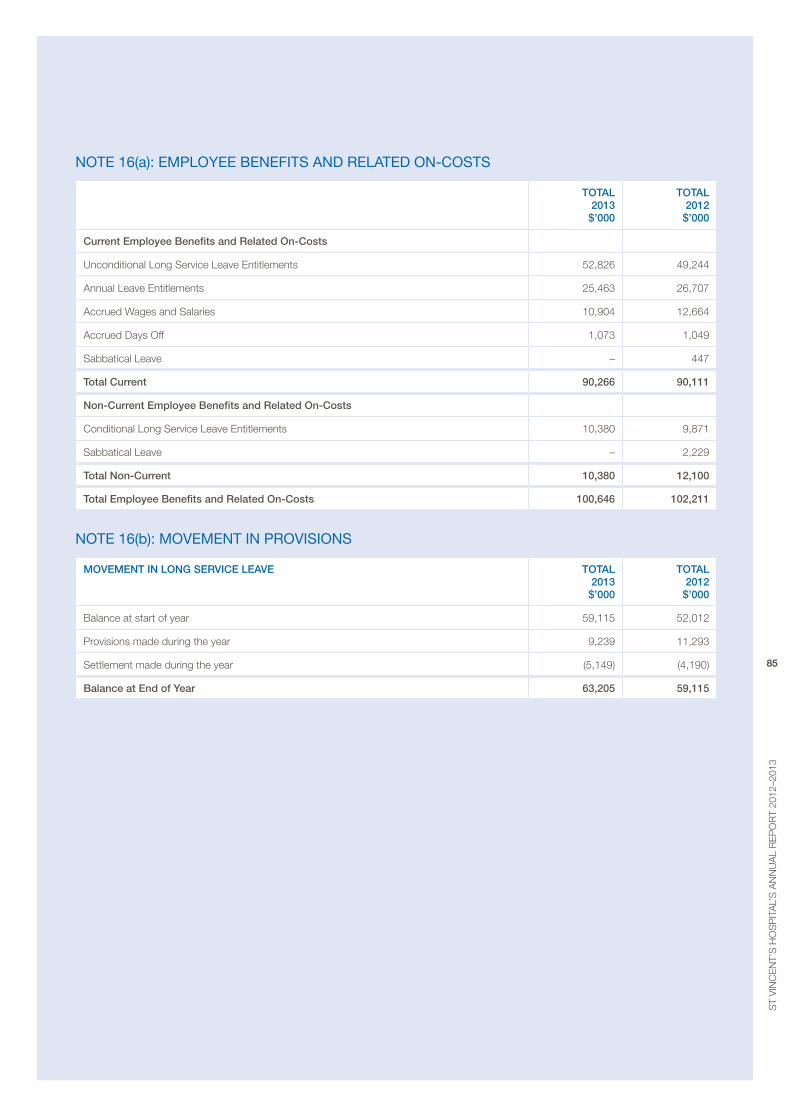
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
85
note 16(a): eMployee benefitS and related on-coStS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current employee Benefits and Related On-Costs
Unconditional Long Service Leave entitlements 52,826 49,244
annual Leave entitlements 25,463 26,707
accrued Wages and Salaries 10,904 12,664
accrued Days off 1,073 1,049
Sabbatical Leave – 447
total Current 90,266 90,111
non-Current employee Benefits and Related On-Costs
Conditional Long Service Leave entitlements 10,380 9,871
Sabbatical Leave – 2,229
total non-Current 10,380 12,100
total employee Benefits and Related On-Costs 100,646 102,211
note 16(b): MoVeMent in proViSionS
mOvement In LOng SeRvICe LeAve tOtAL 2013 $’000
tOtAL 2012 $’000
balance at start of year 59,115 52,012
provisions made during the year 9,239 11,293
Settlement made during the year (5,149) (4,190)
Balance at end of year 63,205 59,115
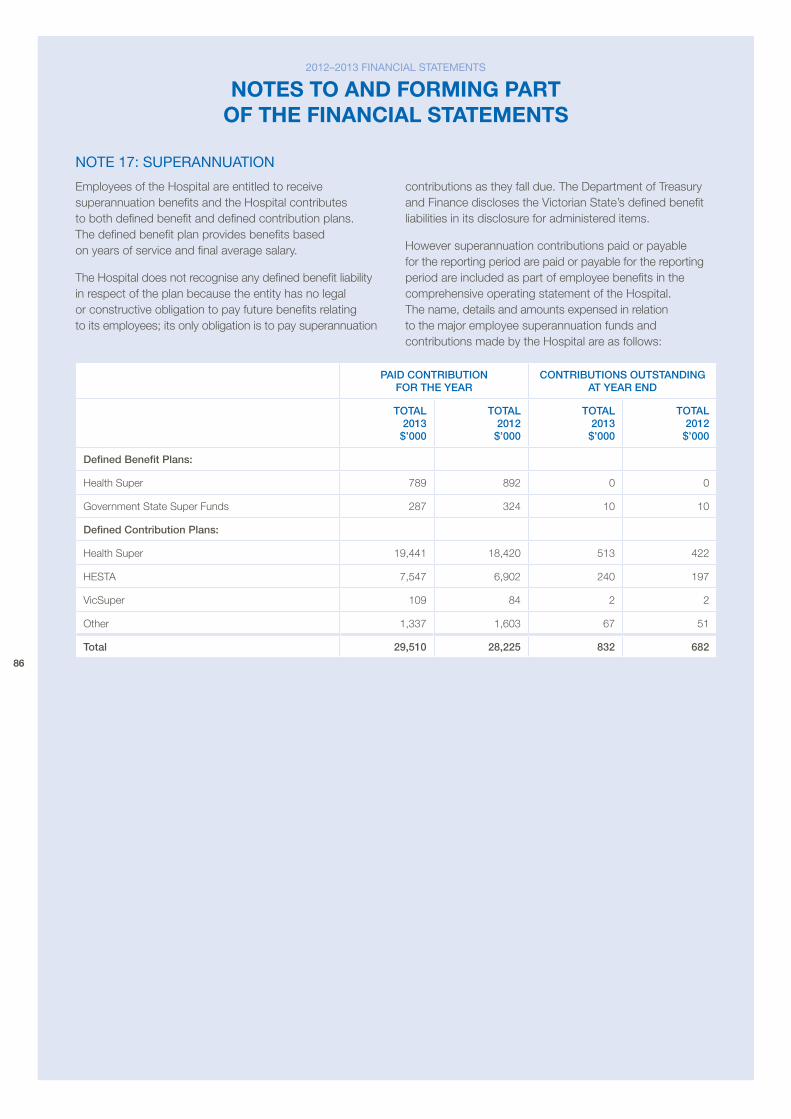
86
note 17: Superannuation
employees of the Hospital are entitled to receive superannuation benefits and the Hospital contributes to both defined benefit and defined contribution plans. The defined benefit plan provides benefits based on years of service and final average salary.
The Hospital does not recognise any defined benefit liability in respect of the plan because the entity has no legal or constructive obligation to pay future benefits relating to its employees; its only obligation is to pay superannuation
contributions as they fall due. The Department of Treasury and Finance discloses the victorian State’s defined benefit liabilities in its disclosure for administered items.
However superannuation contributions paid or payable for the reporting period are paid or payable for the reporting period are included as part of employee benefits in the comprehensive operating statement of the Hospital. The name, details and amounts expensed in relation to the major employee superannuation funds and contributions made by the Hospital are as follows:
pAID COntRIButIOn FOR the yeAR
COntRIButIOnS OutStAnDIng At yeAR enD
tOtAL 2013 $’000
tOtAL 2012 $’000
tOtAL 2013 $’000
tOtAL 2012 $’000
Defined Benefit plans:
Health Super 789 892 0 0
Government State Super Funds 287 324 10 10
Defined Contribution plans:
Health Super 19,441 18,420 513 422
HeSTa 7,547 6,902 240 197
vicSuper 109 84 2 2
other 1,337 1,603 67 51
total 29,510 28,225 832 682
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
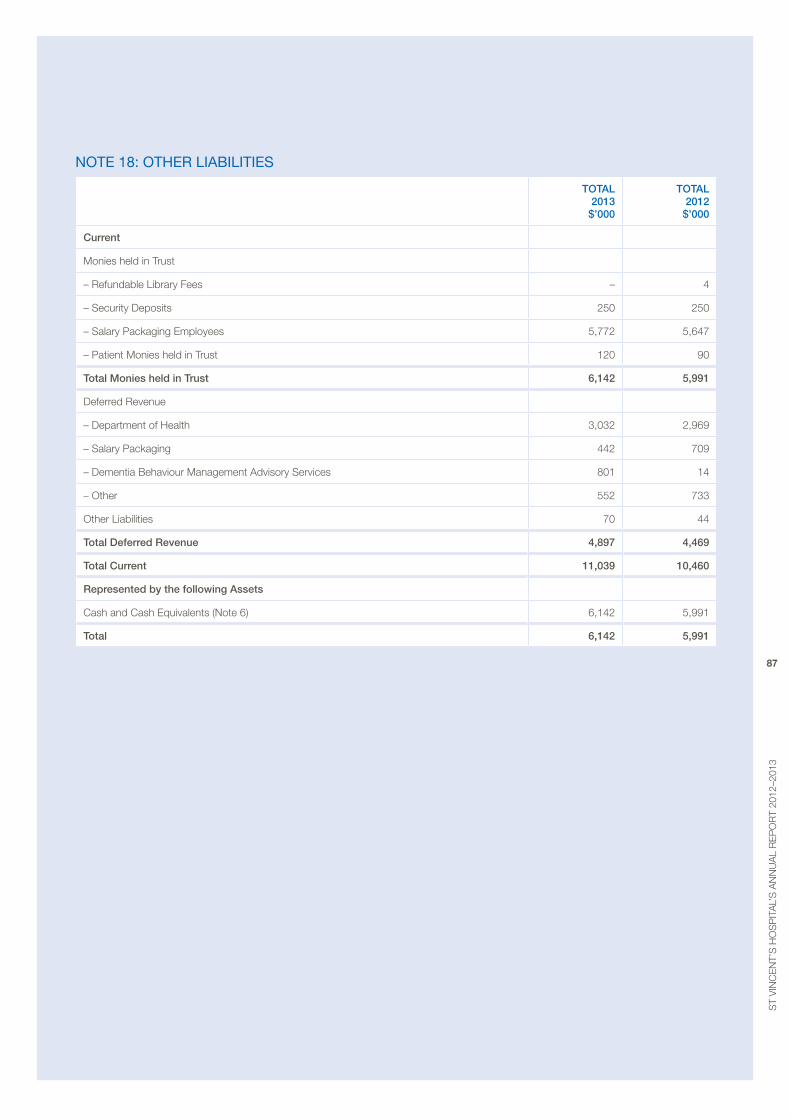
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
87
note 18: otHer liabilitieS
tOtAL 2013 $’000
tOtAL 2012 $’000
Current
monies held in Trust
– refundable Library Fees – 4
– Security Deposits 250 250
– Salary packaging employees 5,772 5,647
– patient monies held in Trust 120 90
total monies held in trust 6,142 5,991
Deferred revenue
– Department of Health 3,032 2,969
– Salary packaging 442 709
– Dementia behaviour management advisory Services 801 14
– other 552 733
other Liabilities 70 44
total Deferred Revenue 4,897 4,469
total Current 11,039 10,460
Represented by the following Assets
Cash and Cash equivalents (Note 6) 6,142 5,991
total 6,142 5,991
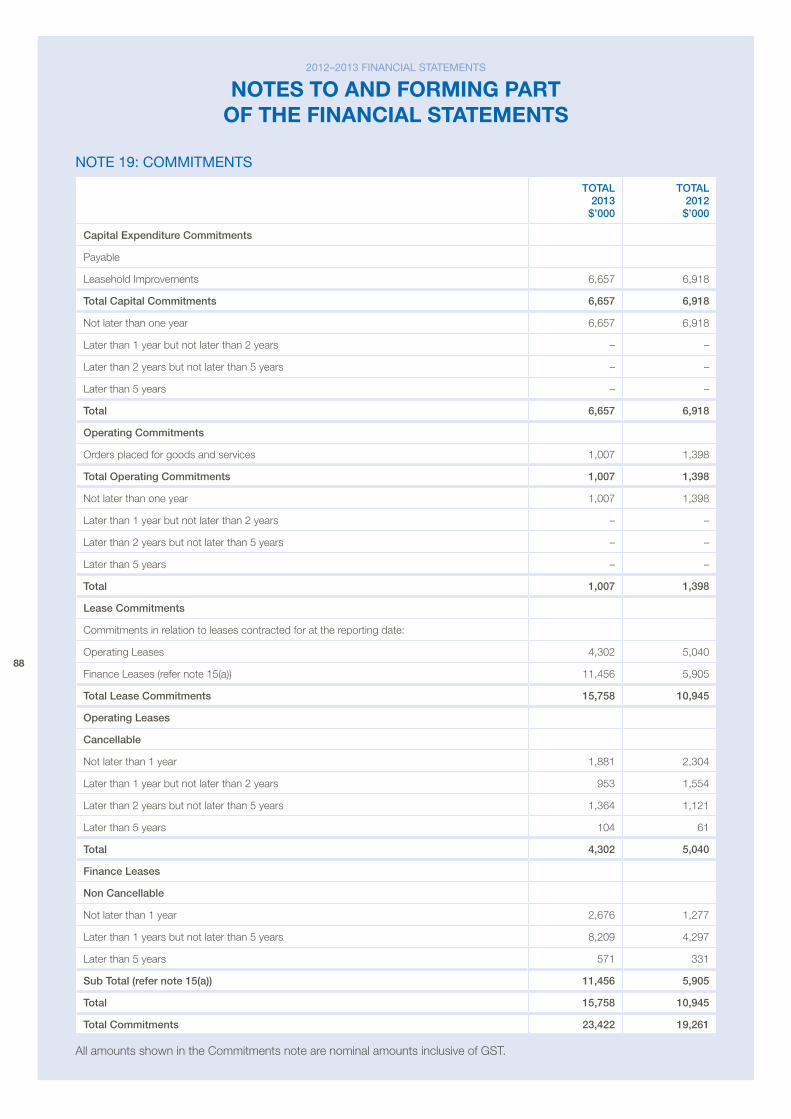
88
note 19: coMMitMentS
tOtAL 2013 $’000
tOtAL 2012 $’000
Capital expenditure Commitments
payable
Leasehold Improvements 6,657 6,918
total Capital Commitments 6,657 6,918
Not later than one year 6,657 6,918
Later than 1 year but not later than 2 years – –
Later than 2 years but not later than 5 years – –
Later than 5 years – –
total 6,657 6,918
Operating Commitments
orders placed for goods and services 1,007 1,398
total Operating Commitments 1,007 1,398
Not later than one year 1,007 1,398
Later than 1 year but not later than 2 years – –
Later than 2 years but not later than 5 years – –
Later than 5 years – –
total 1,007 1,398
Lease Commitments
Commitments in relation to leases contracted for at the reporting date:
operating Leases 4,302 5,040
Finance Leases (refer note 15(a)) 11,456 5,905
total Lease Commitments 15,758 10,945
Operating Leases
Cancellable
Not later than 1 year 1,881 2,304
Later than 1 year but not later than 2 years 953 1,554
Later than 2 years but not later than 5 years 1,364 1,121
Later than 5 years 104 61
total 4,302 5,040
Finance Leases
non Cancellable
Not later than 1 year 2,676 1,277
Later than 1 years but not later than 5 years 8,209 4,297
Later than 5 years 571 331
Sub total (refer note 15(a)) 11,456 5,905
total 15,758 10,945
total Commitments 23,422 19,261
all amounts shown in the Commitments note are nominal amounts inclusive of GST.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
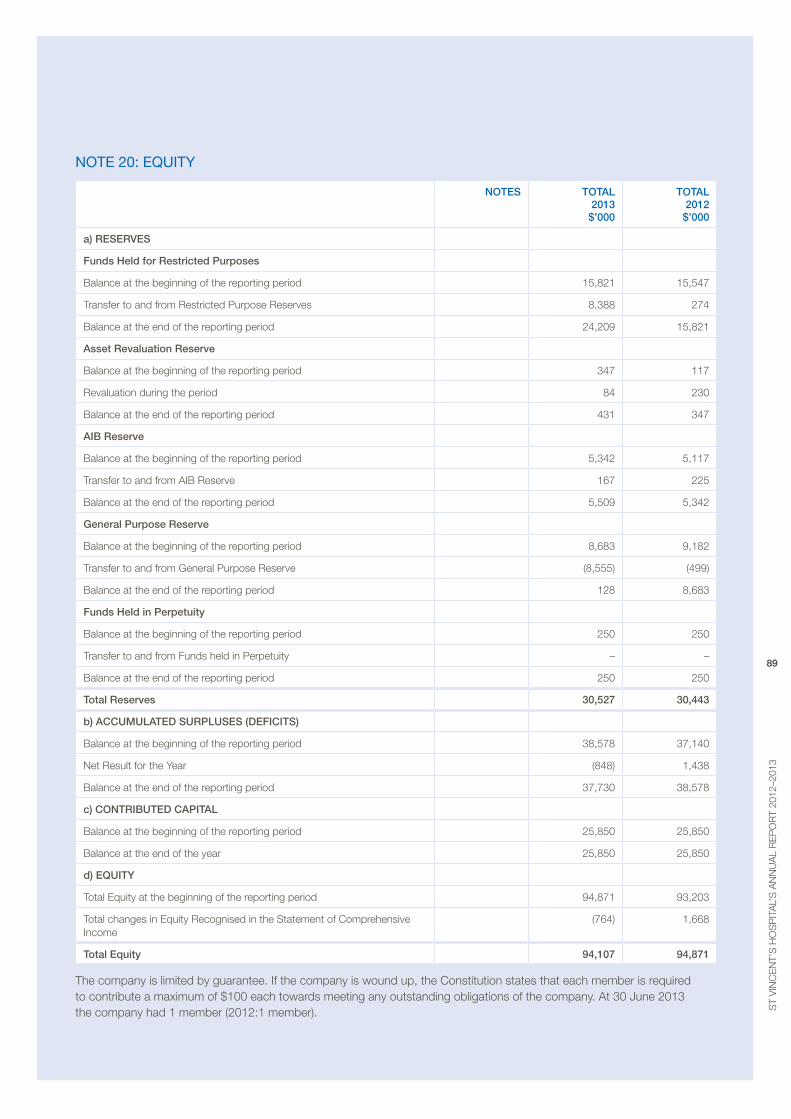
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
89
note 20: equity
nOteS tOtAL 2013 $’000
tOtAL 2012 $’000
a) ReSeRveS
Funds held for Restricted purposes
balance at the beginning of the reporting period 15,821 15,547
Transfer to and from restricted purpose reserves 8,388 274
balance at the end of the reporting period 24,209 15,821
Asset Revaluation Reserve
balance at the beginning of the reporting period 347 117
revaluation during the period 84 230
balance at the end of the reporting period 431 347
AIB Reserve
balance at the beginning of the reporting period 5,342 5,117
Transfer to and from aIb reserve 167 225
balance at the end of the reporting period 5,509 5,342
general purpose Reserve
balance at the beginning of the reporting period 8,683 9,182
Transfer to and from General purpose reserve (8,555) (499)
balance at the end of the reporting period 128 8,683
Funds held in perpetuity
balance at the beginning of the reporting period 250 250
Transfer to and from Funds held in perpetuity – –
balance at the end of the reporting period 250 250
total Reserves 30,527 30,443
b) ACCumuLAteD SuRpLuSeS (DeFICItS)
balance at the beginning of the reporting period 38,578 37,140
Net result for the Year (848) 1,438
balance at the end of the reporting period 37,730 38,578
c) COntRIButeD CApItAL
balance at the beginning of the reporting period 25,850 25,850
balance at the end of the year 25,850 25,850
d) eQuIty
Total equity at the beginning of the reporting period 94,871 93,203
Total changes in equity recognised in the Statement of Comprehensive Income
(764) 1,668
total equity 94,107 94,871
The company is limited by guarantee. If the company is wound up, the Constitution states that each member is required to contribute a maximum of $100 each towards meeting any outstanding obligations of the company. at 30 June 2013 the company had 1 member (2012:1 member).
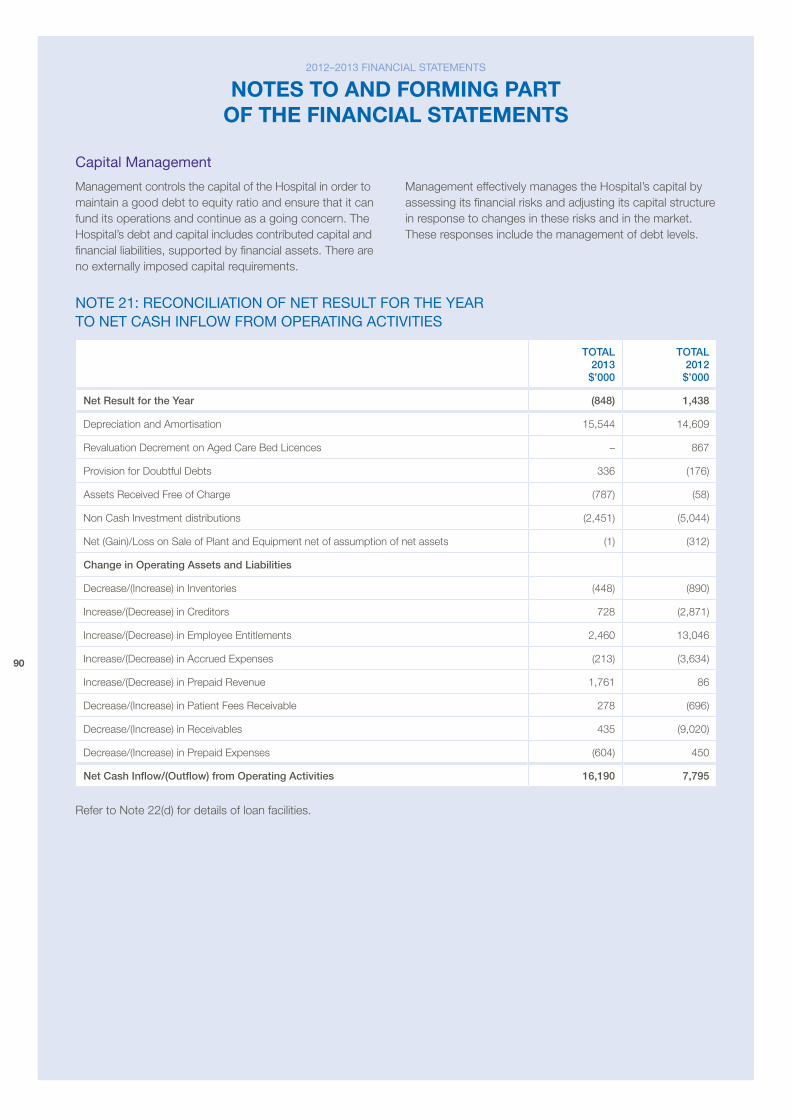
90
capital Management
management controls the capital of the Hospital in order to maintain a good debt to equity ratio and ensure that it can fund its operations and continue as a going concern. The Hospital’s debt and capital includes contributed capital and financial liabilities, supported by financial assets. There are no externally imposed capital requirements.
management effectively manages the Hospital’s capital by assessing its financial risks and adjusting its capital structure in response to changes in these risks and in the market. These responses include the management of debt levels.
note 21: reconciliation of net reSult for tHe year to net caSH inflow froM operatinG actiVitieS
tOtAL 2013 $’000
tOtAL 2012 $’000
net Result for the year (848) 1,438
Depreciation and amortisation 15,544 14,609
revaluation Decrement on aged Care bed Licences – 867
provision for Doubtful Debts 336 (176)
assets received Free of Charge (787) (58)
Non Cash Investment distributions (2,451) (5,044)
Net (Gain)/Loss on Sale of plant and equipment net of assumption of net assets (1) (312)
Change in Operating Assets and Liabilities
Decrease/(Increase) in Inventories (448) (890)
Increase/(Decrease) in Creditors 728 (2,871)
Increase/(Decrease) in employee entitlements 2,460 13,046
Increase/(Decrease) in accrued expenses (213) (3,634)
Increase/(Decrease) in prepaid revenue 1,761 86
Decrease/(Increase) in patient Fees receivable 278 (696)
Decrease/(Increase) in receivables 435 (9,020)
Decrease/(Increase) in prepaid expenses (604) 450
net Cash Inflow/(Outflow) from Operating Activities 16,190 7,795
refer to Note 22(d) for details of loan facilities.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
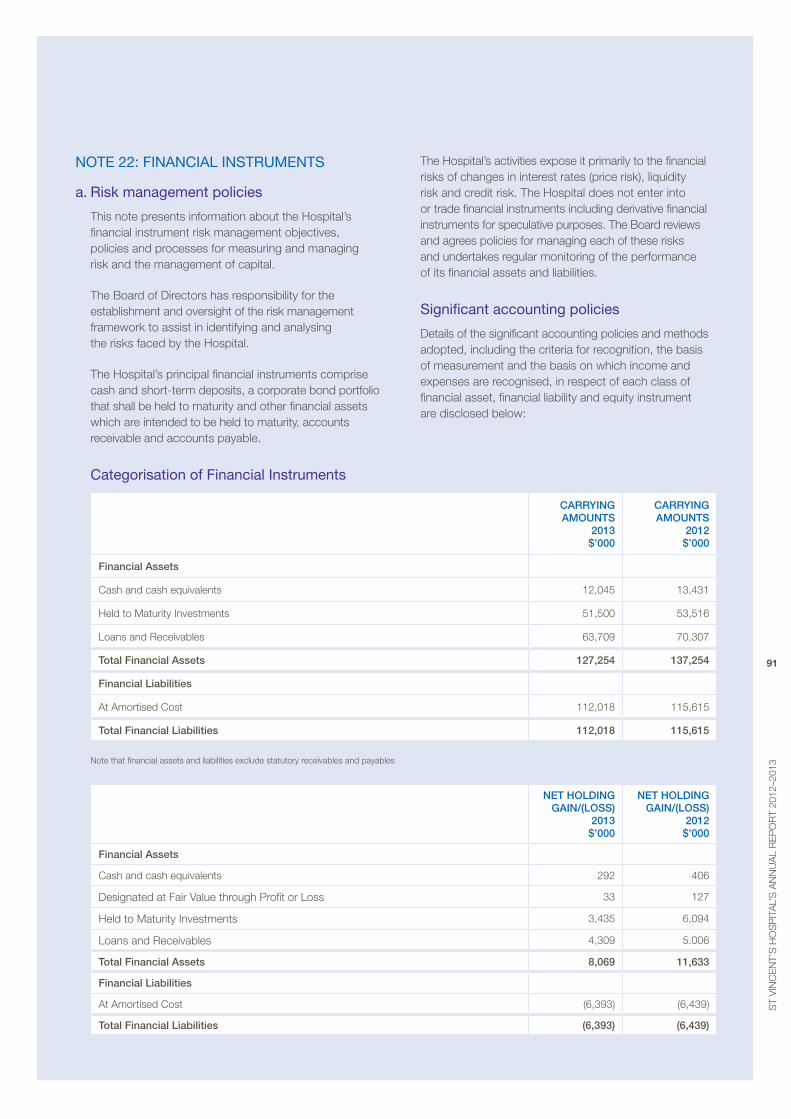
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
91
note 22: financial inStruMentS
a. risk management policies
This note presents information about the Hospital’s financial instrument risk management objectives, policies and processes for measuring and managing risk and the management of capital.
The board of Directors has responsibility for the establishment and oversight of the risk management framework to assist in identifying and analysing the risks faced by the Hospital.
The Hospital’s principal financial instruments comprise cash and short-term deposits, a corporate bond portfolio that shall be held to maturity and other financial assets which are intended to be held to maturity, accounts receivable and accounts payable.
The Hospital’s activities expose it primarily to the financial risks of changes in interest rates (price risk), liquidity risk and credit risk. The Hospital does not enter into or trade financial instruments including derivative financial instruments for speculative purposes. The board reviews and agrees policies for managing each of these risks and undertakes regular monitoring of the performance of its financial assets and liabilities.
Significant accounting policies
Details of the significant accounting policies and methods adopted, including the criteria for recognition, the basis of measurement and the basis on which income and expenses are recognised, in respect of each class of financial asset, financial liability and equity instrument are disclosed below:
categorisation of financial instruments
CARRyIng AmOuntS
2013 $’000
CARRyIng AmOuntS
2012 $’000
Financial Assets
Cash and cash equivalents 12,045 13,431
Held to maturity Investments 51,500 53,516
Loans and receivables 63,709 70,307
total Financial Assets 127,254 137,254
Financial Liabilities
at amortised Cost 112,018 115,615
total Financial Liabilities 112,018 115,615
Note that financial assets and liabilities exclude statutory receivables and payables
net hOLDIng gAIn/(LOSS)
2013 $’000
net hOLDIng gAIn/(LOSS)
2012 $’000
Financial Assets
Cash and cash equivalents 292 406
Designated at Fair value through profit or Loss 33 127
Held to maturity Investments 3,435 6,094
Loans and receivables 4,309 5.006
total Financial Assets 8,069 11,633
Financial Liabilities
at amortised Cost (6,393) (6,439)
total Financial Liabilities (6,393) (6,439)
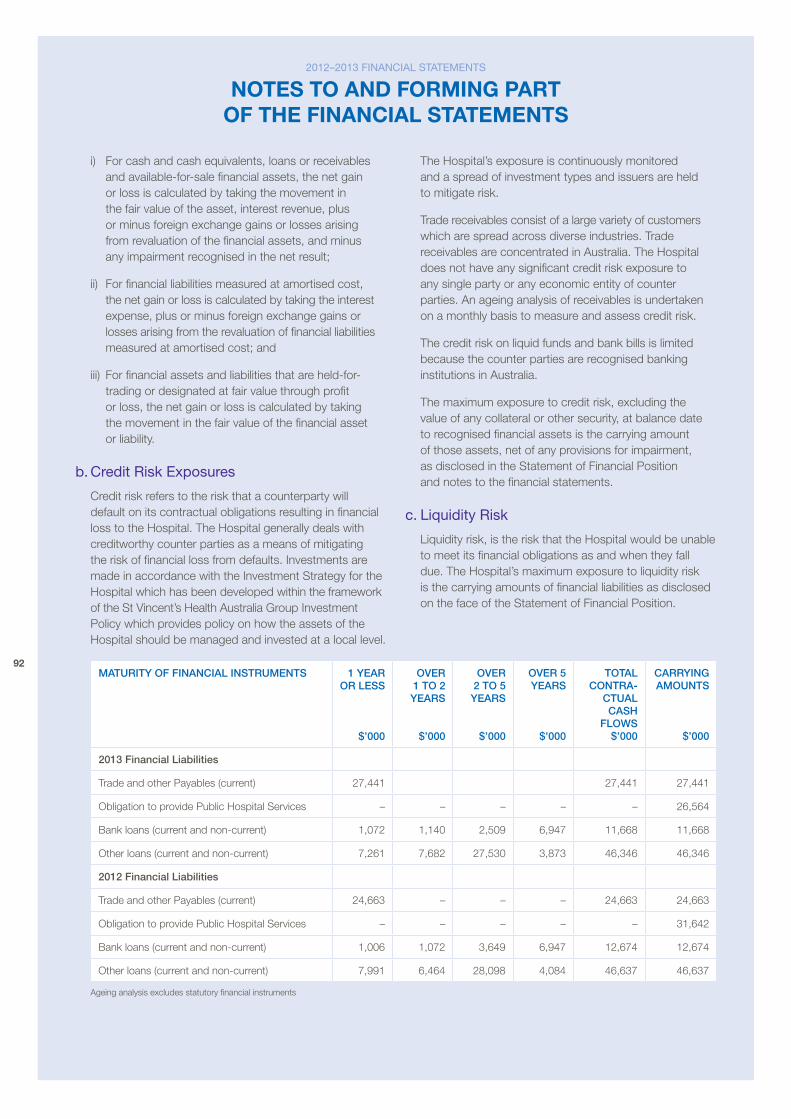
92
i) For cash and cash equivalents, loans or receivables and available-for-sale financial assets, the net gain or loss is calculated by taking the movement in the fair value of the asset, interest revenue, plus or minus foreign exchange gains or losses arising from revaluation of the financial assets, and minus any impairment recognised in the net result;
ii) For financial liabilities measured at amortised cost, the net gain or loss is calculated by taking the interest expense, plus or minus foreign exchange gains or losses arising from the revaluation of financial liabilities measured at amortised cost; and
iii) For financial assets and liabilities that are held-for-trading or designated at fair value through profit or loss, the net gain or loss is calculated by taking the movement in the fair value of the financial asset or liability.
b. credit risk exposures
Credit risk refers to the risk that a counterparty will default on its contractual obligations resulting in financial loss to the Hospital. The Hospital generally deals with creditworthy counter parties as a means of mitigating the risk of financial loss from defaults. Investments are made in accordance with the Investment Strategy for the Hospital which has been developed within the framework of the St vincent’s Health australia Group Investment policy which provides policy on how the assets of the Hospital should be managed and invested at a local level.
The Hospital’s exposure is continuously monitored and a spread of investment types and issuers are held to mitigate risk.
Trade receivables consist of a large variety of customers which are spread across diverse industries. Trade receivables are concentrated in australia. The Hospital does not have any significant credit risk exposure to any single party or any economic entity of counter parties. an ageing analysis of receivables is undertaken on a monthly basis to measure and assess credit risk.
The credit risk on liquid funds and bank bills is limited because the counter parties are recognised banking institutions in australia.
The maximum exposure to credit risk, excluding the value of any collateral or other security, at balance date to recognised financial assets is the carrying amount of those assets, net of any provisions for impairment, as disclosed in the Statement of Financial position and notes to the financial statements.
c. liquidity risk
Liquidity risk, is the risk that the Hospital would be unable to meet its financial obligations as and when they fall due. The Hospital’s maximum exposure to liquidity risk is the carrying amounts of financial liabilities as disclosed on the face of the Statement of Financial position.
mAtuRIty OF FInAnCIAL InStRumentS 1 yeAR OR LeSS
$’000
OveR 1 tO 2 yeARS
$’000
OveR 2 tO 5 yeARS
$’000
OveR 5 yeARS
$’000
tOtAL COntRA-
CtuAL CASh
FLOwS $’000
CARRyIng AmOuntS
$’000
2013 Financial Liabilities
Trade and other payables (current) 27,441 27,441 27,441
obligation to provide public Hospital Services – – – – – 26,564
bank loans (current and non-current) 1,072 1,140 2,509 6,947 11,668 11,668
other loans (current and non-current) 7,261 7,682 27,530 3,873 46,346 46,346
2012 Financial Liabilities
Trade and other payables (current) 24,663 – – – 24,663 24,663
obligation to provide public Hospital Services – – – – – 31,642
bank loans (current and non-current) 1,006 1,072 3,649 6,947 12,674 12,674
other loans (current and non-current) 7,991 6,464 28,098 4,084 46,637 46,637
ageing analysis excludes statutory financial instruments
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
93
at the reporting date St vincent’s Hospital (melbourne) Limited has no access to any undrawn credit facilities.
Ultimate responsibility for liquidity risk management rests with the board of Directors, which has in place a framework to manage the Hospital’s short, medium and long term funding and liquidity. The Hospital manages the liquidity risk by maintaining adequate cash reserves and by continuously monitoring forecast and actual cash flows by matching the maturity profiles of financial assets and liabilities. Given the current surplus cash assets, liquidity risk is considered to be minimal.
d. Market risk
The Hospital’s exposures to market risk are primarily through interest rate risk with only insignificant exposure to foreign currency and other price risks. objectives, policies and processes used to manage each of these risks are disclosed in the paragraph below.
interest rate risk exposure
The Hospital’s exposure to interest rate risk, which is the risk that a financial instrument’s value will fluctuate as a result of changes in market interest rates and the effective weighted average interest rates on classes of financial assets and financial liabilities, is limited to assets and liabilities bearing variable interest rates. St vincent’s Hospital (melbourne) Limited does not enter into interest rate swaps.
The Hospital’s major long term financial liabilities are effectively protected from interest rate risk as indicated below:
– Cba car-park loan facility of $15,000,000 (residual as at year end: $11,668,000) $10.5m fixed interest at 7.05% and $4.5m variable facility capped at 7.05%
– aIb facility for development of hospital building (IpS) effectively relates to Inflation Indexed bonds where the loan repayments are entirely underwritten by a Government Grant and accordingly no interest rate risk is borne by St vincent’s Hospital (melbourne) Limited
– finance leases on fixed terms totalling $9,781,000 at year end are currently being amortised
– a facility with St vincent’s Healthcare Ltd (SvHC)was fully drawn down in the year. The interest rate is variable but is currently 5.3% with interest only over the first three years and with the principal to be paid off over the following four years.
The Hospital also holds a number of term investments and bonds with fixed interest rates, which are intended to be generally held to maturity. The Hospital’s intention is to maintain a combination of fixed and variable rates for both liabilities and financial assets to ensure that in aggregate interest rate risk is minimised. This is illustrated in the table below.
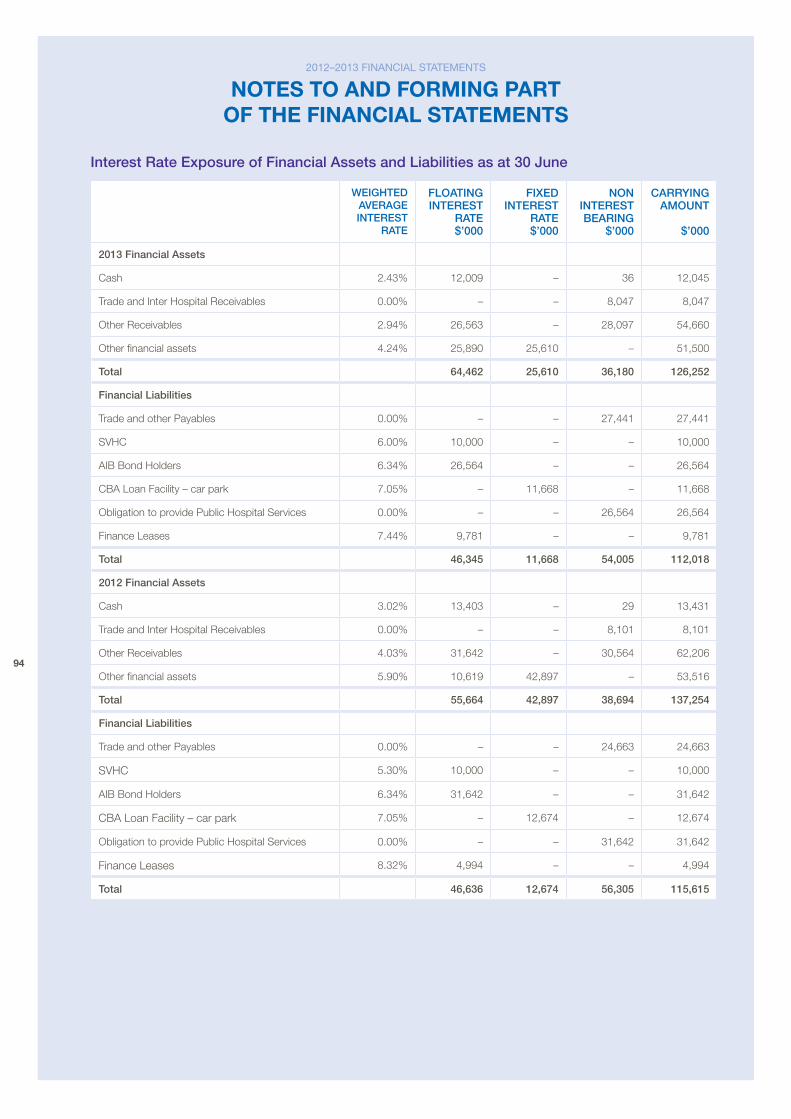
94
Interest Rate exposure of Financial Assets and Liabilities as at 30 june
weIghteD AveRAge InteReSt
RAte
FLOAtIng InteReSt
RAte $’000
FIxeD InteReSt
RAte $’000
nOn InteReSt BeARIng
$’000
CARRyIng AmOunt
$’000
2013 Financial Assets
Cash 2.43% 12,009 – 36 12,045
Trade and Inter Hospital receivables 0.00% – – 8,047 8,047
other receivables 2.94% 26,563 – 28,097 54,660
other financial assets 4.24% 25,890 25,610 – 51,500
total 64,462 25,610 36,180 126,252
Financial Liabilities
Trade and other payables 0.00% – – 27,441 27,441
SvHC 6.00% 10,000 – – 10,000
aIb bond Holders 6.34% 26,564 – – 26,564
Cba Loan Facility – car park 7.05% – 11,668 – 11,668
obligation to provide public Hospital Services 0.00% – – 26,564 26,564
Finance Leases 7.44% 9,781 – – 9,781
total 46,345 11,668 54,005 112,018
2012 Financial Assets
Cash 3.02% 13,403 – 29 13,431
Trade and Inter Hospital receivables 0.00% – – 8,101 8,101
other receivables 4.03% 31,642 – 30,564 62,206
other financial assets 5.90% 10,619 42,897 – 53,516
total 55,664 42,897 38,694 137,254
Financial Liabilities
Trade and other payables 0.00% – – 24,663 24,663
SvHC 5.30% 10,000 – – 10,000
aIb bond Holders 6.34% 31,642 – – 31,642
Cba Loan Facility – car park 7.05% – 12,674 – 12,674
obligation to provide public Hospital Services 0.00% – – 31,642 31,642
Finance Leases 8.32% 4,994 – – 4,994
total 46,636 12,674 56,305 115,615
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
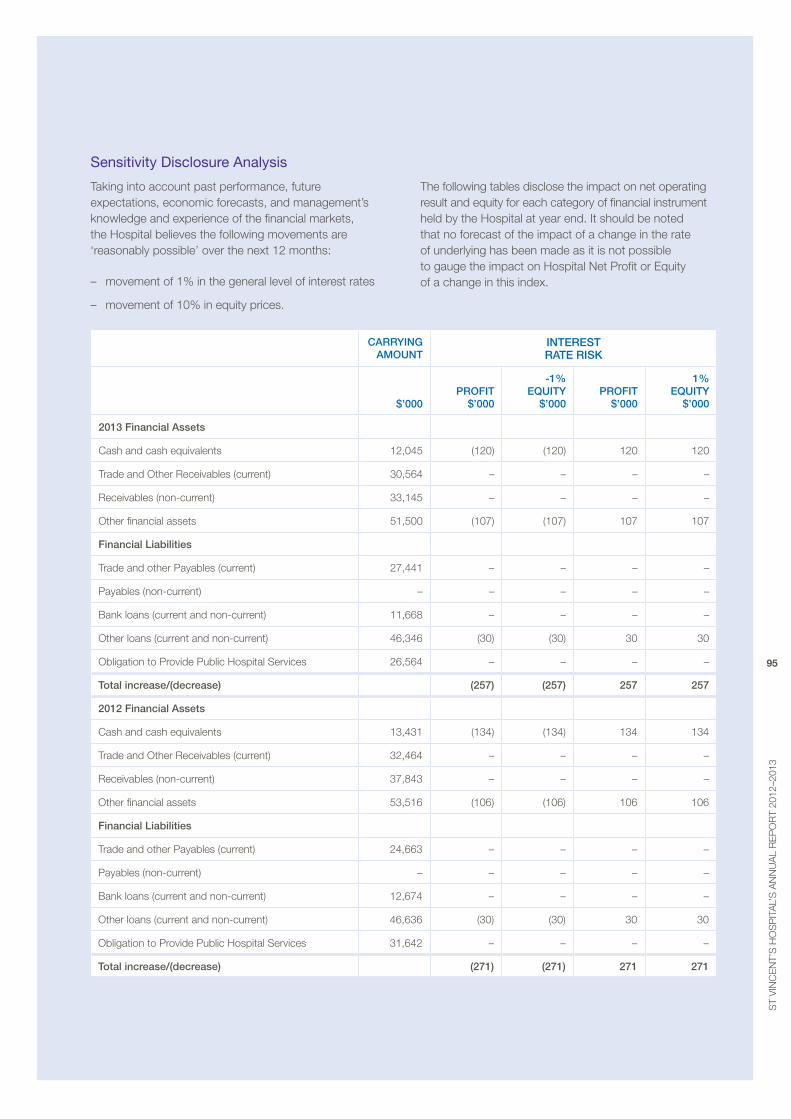
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
95
Sensitivity disclosure analysis
Taking into account past performance, future expectations, economic forecasts, and management’s knowledge and experience of the financial markets, the Hospital believes the following movements are ‘reasonably possible’ over the next 12 months:
– movement of 1% in the general level of interest rates
– movement of 10% in equity prices.
The following tables disclose the impact on net operating result and equity for each category of financial instrument held by the Hospital at year end. It should be noted that no forecast of the impact of a change in the rate of underlying has been made as it is not possible to gauge the impact on Hospital Net profit or equity of a change in this index.
CARRyIng AmOunt
InteReSt RAte RISk
$’000
pROFIt
$’000
-1% eQuIty
$’000
pROFIt
$’000
1% eQuIty
$’000
2013 Financial Assets
Cash and cash equivalents 12,045 (120) (120) 120 120
Trade and other receivables (current) 30,564 – – – –
receivables (non-current) 33,145 – – – –
other financial assets 51,500 (107) (107) 107 107
Financial Liabilities
Trade and other payables (current) 27,441 – – – –
payables (non-current) – – – – –
bank loans (current and non-current) 11,668 – – – –
other loans (current and non-current) 46,346 (30) (30) 30 30
obligation to provide public Hospital Services 26,564 – – – –
total increase/(decrease) (257) (257) 257 257
2012 Financial Assets
Cash and cash equivalents 13,431 (134) (134) 134 134
Trade and other receivables (current) 32,464 – – – –
receivables (non-current) 37,843 – – – –
other financial assets 53,516 (106) (106) 106 106
Financial Liabilities
Trade and other payables (current) 24,663 – – – –
payables (non-current) – – – – –
bank loans (current and non-current) 12,674 – – – –
other loans (current and non-current) 46,636 (30) (30) 30 30
obligation to provide public Hospital Services 31,642 – – – –
total increase/(decrease) (271) (271) 271 271
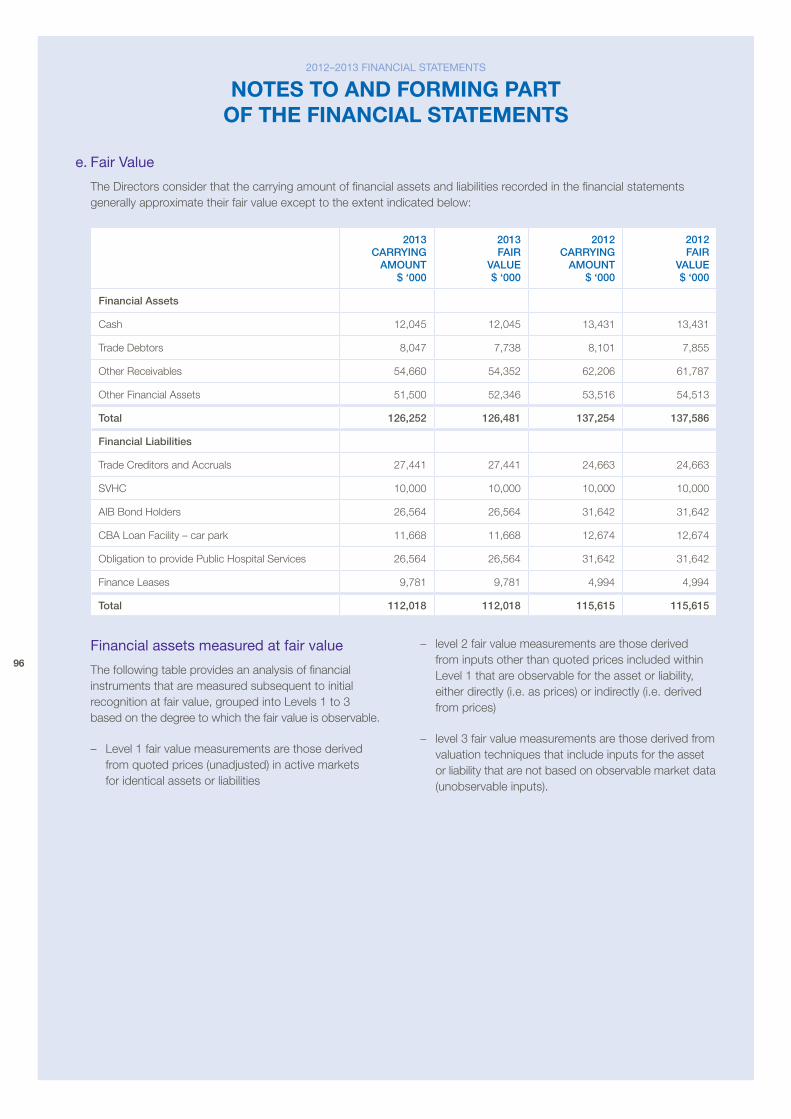
96
e. fair Value
The Directors consider that the carrying amount of financial assets and liabilities recorded in the financial statements generally approximate their fair value except to the extent indicated below:
2013 CARRyIng
AmOunt $ ‘000
2013 FAIR
vALue $ ‘000
2012 CARRyIng
AmOunt $ ‘000
2012 FAIR
vALue $ ‘000
Financial Assets
Cash 12,045 12,045 13,431 13,431
Trade Debtors 8,047 7,738 8,101 7,855
other receivables 54,660 54,352 62,206 61,787
other Financial assets 51,500 52,346 53,516 54,513
total 126,252 126,481 137,254 137,586
Financial Liabilities
Trade Creditors and accruals 27,441 27,441 24,663 24,663
SvHC 10,000 10,000 10,000 10,000
aIb bond Holders 26,564 26,564 31,642 31,642
Cba Loan Facility – car park 11,668 11,668 12,674 12,674
obligation to provide public Hospital Services 26,564 26,564 31,642 31,642
Finance Leases 9,781 9,781 4,994 4,994
total 112,018 112,018 115,615 115,615
financial assets measured at fair value
The following table provides an analysis of financial instruments that are measured subsequent to initial recognition at fair value, grouped into Levels 1 to 3 based on the degree to which the fair value is observable.
– Level 1 fair value measurements are those derived from quoted prices (unadjusted) in active markets for identical assets or liabilities
– level 2 fair value measurements are those derived from inputs other than quoted prices included within Level 1 that are observable for the asset or liability, either directly (i.e. as prices) or indirectly (i.e. derived from prices)
– level 3 fair value measurements are those derived from valuation techniques that include inputs for the asset or liability that are not based on observable market data (unobservable inputs).
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
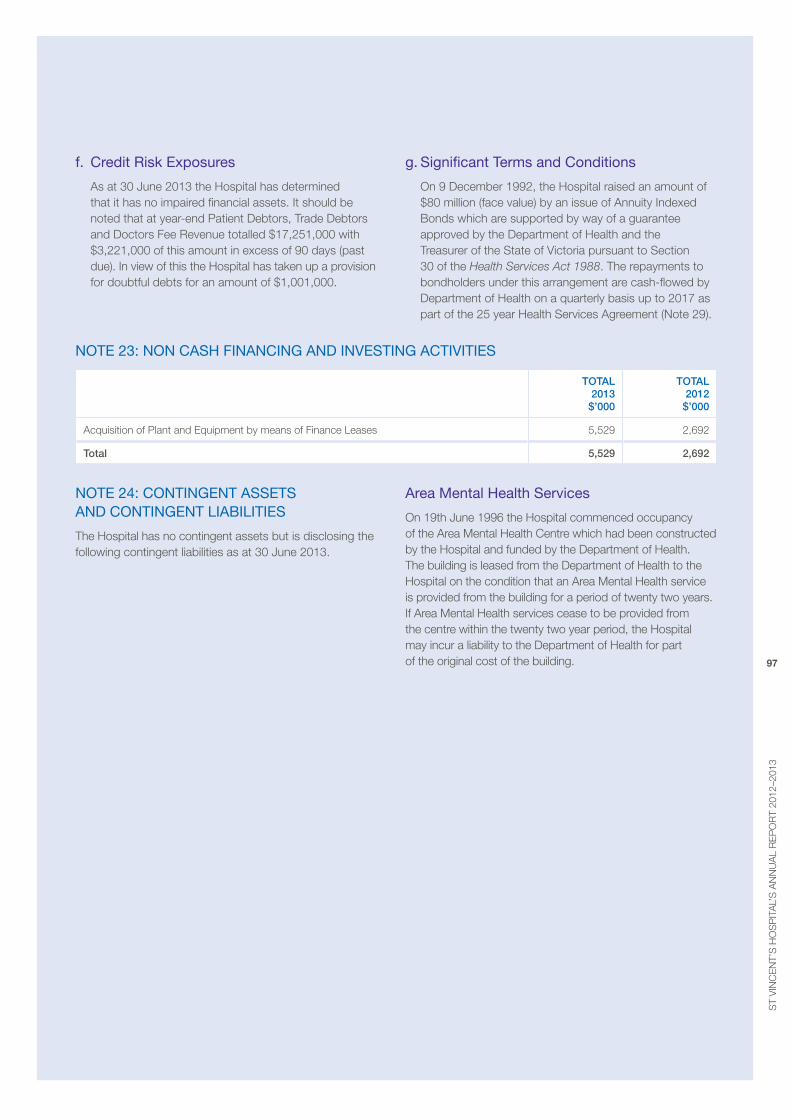
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
97
f. credit risk exposures
as at 30 June 2013 the Hospital has determined that it has no impaired financial assets. It should be noted that at year-end patient Debtors, Trade Debtors and Doctors Fee revenue totalled $17,251,000 with $3,221,000 of this amount in excess of 90 days (past due). In view of this the Hospital has taken up a provision for doubtful debts for an amount of $1,001,000.
g. Significant terms and conditions
on 9 December 1992, the Hospital raised an amount of $80 million (face value) by an issue of annuity Indexed bonds which are supported by way of a guarantee approved by the Department of Health and the Treasurer of the State of victoria pursuant to Section 30 of the Health Services Act 1988. The repayments to bondholders under this arrangement are cash-flowed by Department of Health on a quarterly basis up to 2017 as part of the 25 year Health Services agreement (Note 29).
note 23: non caSH financinG and inVeStinG actiVitieS
tOtAL 2013 $’000
tOtAL 2012 $’000
acquisition of plant and equipment by means of Finance Leases 5,529 2,692
total 5,529 2,692
note 24: continGent aSSetS and continGent liabilitieS
The Hospital has no contingent assets but is disclosing the following contingent liabilities as at 30 June 2013.
area Mental Health Services
on 19th June 1996 the Hospital commenced occupancy of the area mental Health Centre which had been constructed by the Hospital and funded by the Department of Health. The building is leased from the Department of Health to the Hospital on the condition that an area mental Health service is provided from the building for a period of twenty two years. If area mental Health services cease to be provided from the centre within the twenty two year period, the Hospital may incur a liability to the Department of Health for part of the original cost of the building.
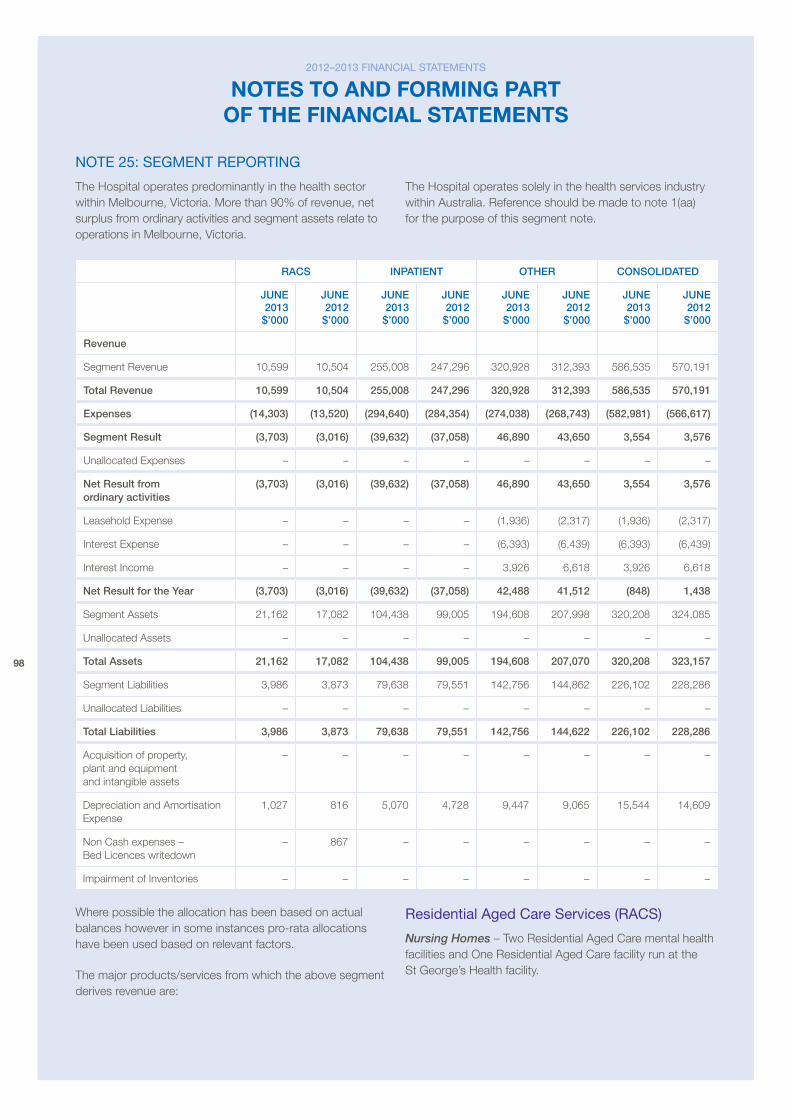
98
note 25: SeGMent reportinG
The Hospital operates predominantly in the health sector within melbourne, victoria. more than 90% of revenue, net surplus from ordinary activities and segment assets relate to operations in melbourne, victoria.
The Hospital operates solely in the health services industry within australia. reference should be made to note 1(aa) for the purpose of this segment note.
RACS InpAtIent OtheR COnSOLIDAteD
june 2013 $’000
june 2012 $’000
june 2013 $’000
june 2012 $’000
june 2013 $’000
june 2012 $’000
june 2013 $’000
june 2012 $’000
Revenue
Segment revenue 10,599 10,504 255,008 247,296 320,928 312,393 586,535 570,191
total Revenue 10,599 10,504 255,008 247,296 320,928 312,393 586,535 570,191
expenses (14,303) (13,520) (294,640) (284,354) (274,038) (268,743) (582,981) (566,617)
Segment Result (3,703) (3,016) (39,632) (37,058) 46,890 43,650 3,554 3,576
Unallocated expenses – – – – – – – –
net Result from ordinary activities
(3,703) (3,016) (39,632) (37,058) 46,890 43,650 3,554 3,576
Leasehold expense – – – – (1,936) (2,317) (1,936) (2,317)
Interest expense – – – – (6,393) (6,439) (6,393) (6,439)
Interest Income – – – – 3,926 6,618 3,926 6,618
net Result for the year (3,703) (3,016) (39,632) (37,058) 42,488 41,512 (848) 1,438
Segment assets 21,162 17,082 104,438 99,005 194,608 207,998 320,208 324,085
Unallocated assets – – – – – – – –
total Assets 21,162 17,082 104,438 99,005 194,608 207,070 320,208 323,157
Segment Liabilities 3,986 3,873 79,638 79,551 142,756 144,862 226,102 228,286
Unallocated Liabilities – – – – – – – –
total Liabilities 3,986 3,873 79,638 79,551 142,756 144,622 226,102 228,286
acquisition of property, plant and equipment and intangible assets
– – – – – – – –
Depreciation and amortisation expense
1,027 816 5,070 4,728 9,447 9,065 15,544 14,609
Non Cash expenses – bed Licences writedown
– 867 – – – – – –
Impairment of Inventories – – – – – – – –
Where possible the allocation has been based on actual balances however in some instances pro-rata allocations have been used based on relevant factors.
The major products/services from which the above segment derives revenue are:
residential aged care Services (racS)
Nursing Homes – Two residential aged Care mental health facilities and one residential aged Care facility run at the St George’s Health facility.
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
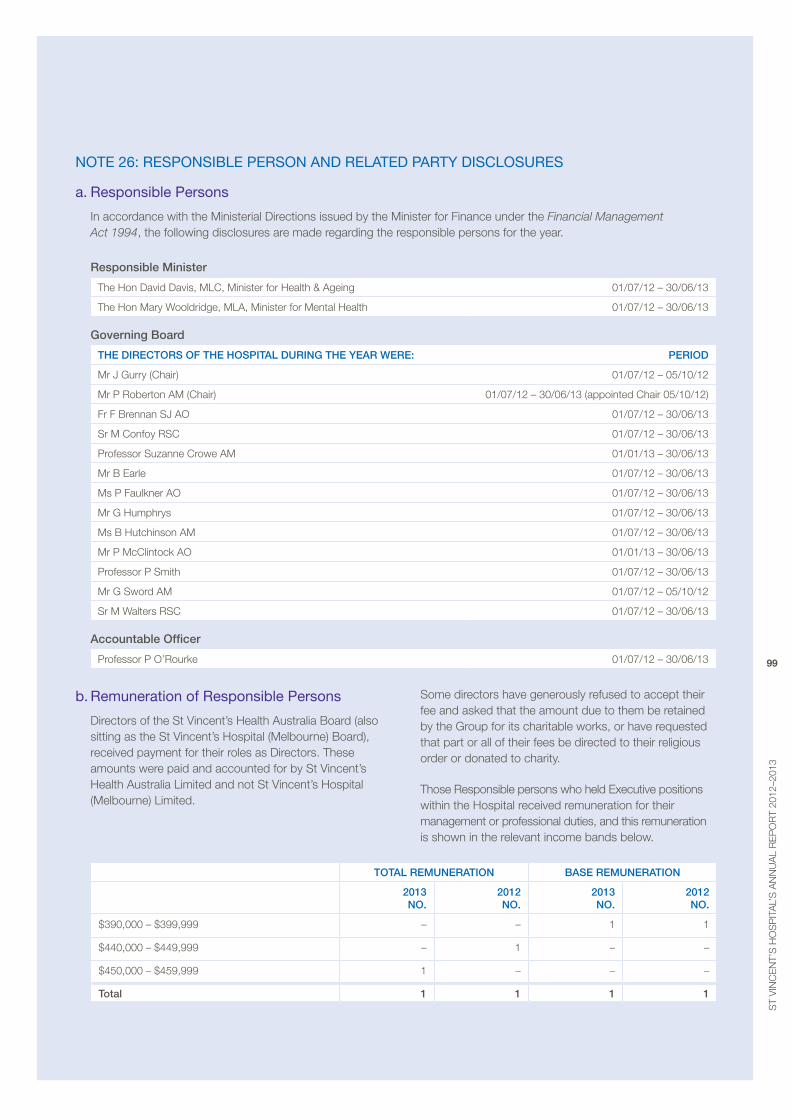
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
99
note 26: reSponSible perSon and related party diScloSureS
a. responsible persons
In accordance with the ministerial Directions issued by the minister for Finance under the Financial Management Act 1994, the following disclosures are made regarding the responsible persons for the year.
Responsible minister
The Hon David Davis, mLC, minister for Health & ageing 01/07/12 – 30/06/13
The Hon mary Wooldridge, mLa, minister for mental Health 01/07/12 – 30/06/13
governing Board
the DIReCtORS OF the hOSpItAL DuRIng the yeAR weRe: peRIOD
mr J Gurry (Chair) 01/07/12 – 05/10/12
mr p roberton am (Chair) 01/07/12 – 30/06/13 (appointed Chair 05/10/12)
Fr F brennan SJ ao 01/07/12 – 30/06/13
Sr m Confoy rSC 01/07/12 – 30/06/13
professor Suzanne Crowe am 01/01/13 – 30/06/13
mr b earle 01/07/12 – 30/06/13
ms p Faulkner ao 01/07/12 – 30/06/13
mr G Humphrys 01/07/12 – 30/06/13
ms b Hutchinson am 01/07/12 – 30/06/13
mr p mcClintock ao 01/01/13 – 30/06/13
professor p Smith 01/07/12 – 30/06/13
mr G Sword am 01/07/12 – 05/10/12
Sr m Walters rSC 01/07/12 – 30/06/13
Accountable Officer
professor p o’rourke 01/07/12 – 30/06/13
b. remuneration of responsible persons
Directors of the St vincent’s Health australia board (also sitting as the St vincent’s Hospital (melbourne) board), received payment for their roles as Directors. These amounts were paid and accounted for by St vincent’s Health australia Limited and not St vincent’s Hospital (melbourne) Limited.
Some directors have generously refused to accept their fee and asked that the amount due to them be retained by the Group for its charitable works, or have requested that part or all of their fees be directed to their religious order or donated to charity.
Those responsible persons who held executive positions within the Hospital received remuneration for their management or professional duties, and this remuneration is shown in the relevant income bands below.
tOtAL RemuneRAtIOn BASe RemuneRAtIOn
2013 nO.
2012 nO.
2013 nO.
2012 nO.
$390,000 – $399,999 – – 1 1
$440,000 – $449,999 – 1 – –
$450,000 – $459,999 1 – – –
total 1 1 1 1
100
c. remuneration of responsible persons
There was no other remuneration paid in connection with responsible persons of St vincent’s Hospital (melbourne) Limited.
d. retirement benefits of responsible persons
There were no retirement benefits paid by the Hospital in connection with the retirement of responsible persons of St vincent’s Hospital (melbourne) Limited.
e. other transactions of responsible persons and their related parties
There were no other transactions of responsible persons and their related parties.
f. transactions with entities in the wholly-owned group
St vincent’s Hospital (melbourne) Limited is part of a wholly owned group. Transactions between St vincent’s Hospital (melbourne) Limited and other entities in the wholly owned group during the year ended 30 June 2013 consist of:
i) recoveries by St vincent’s Hospital (melbourne) Limited for the provision of management and administrative services
ii) recoveries by St vincent’s Hospital (melbourne) Limited for the provision of other health services at cost
iii) payment to St vincent’s Health australia Limited Group levy and other service costs
iv) repayment of loans (including interest) and payment of a car park lease to St vincent’s Healthcare Limited (SvHC).
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
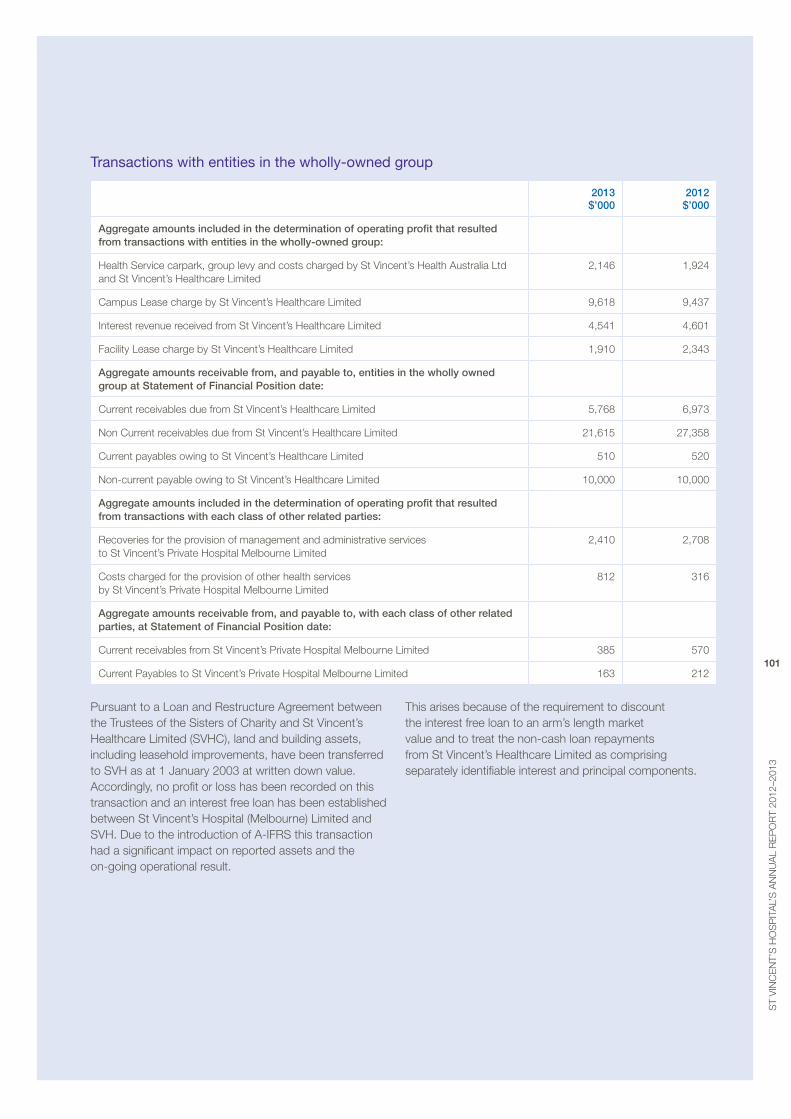
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
101
transactions with entities in the wholly-owned group
2013 $’000
2012 $’000
Aggregate amounts included in the determination of operating profit that resulted from transactions with entities in the wholly-owned group:
Health Service carpark, group levy and costs charged by St vincent’s Health australia Ltd and St vincent’s Healthcare Limited
2,146 1,924
Campus Lease charge by St vincent’s Healthcare Limited 9,618 9,437
Interest revenue received from St vincent’s Healthcare Limited 4,541 4,601
Facility Lease charge by St vincent’s Healthcare Limited 1,910 2,343
Aggregate amounts receivable from, and payable to, entities in the wholly owned group at Statement of Financial position date:
Current receivables due from St vincent’s Healthcare Limited 5,768 6,973
Non Current receivables due from St vincent’s Healthcare Limited 21,615 27,358
Current payables owing to St vincent’s Healthcare Limited 510 520
Non-current payable owing to St vincent’s Healthcare Limited 10,000 10,000
Aggregate amounts included in the determination of operating profit that resulted from transactions with each class of other related parties:
recoveries for the provision of management and administrative services to St vincent’s private Hospital melbourne Limited
2,410 2,708
Costs charged for the provision of other health services by St vincent’s private Hospital melbourne Limited
812 316
Aggregate amounts receivable from, and payable to, with each class of other related parties, at Statement of Financial position date:
Current receivables from St vincent’s private Hospital melbourne Limited 385 570
Current payables to St vincent’s private Hospital melbourne Limited 163 212
pursuant to a Loan and restructure agreement between the Trustees of the Sisters of Charity and St vincent’s Healthcare Limited (SvHC), land and building assets, including leasehold improvements, have been transferred to SvH as at 1 January 2003 at written down value. accordingly, no profit or loss has been recorded on this transaction and an interest free loan has been established between St vincent’s Hospital (melbourne) Limited and SvH. Due to the introduction of a-IFrS this transaction had a significant impact on reported assets and the on-going operational result.
This arises because of the requirement to discount the interest free loan to an arm’s length market value and to treat the non-cash loan repayments from St vincent’s Healthcare Limited as comprising separately identifiable interest and principal components.
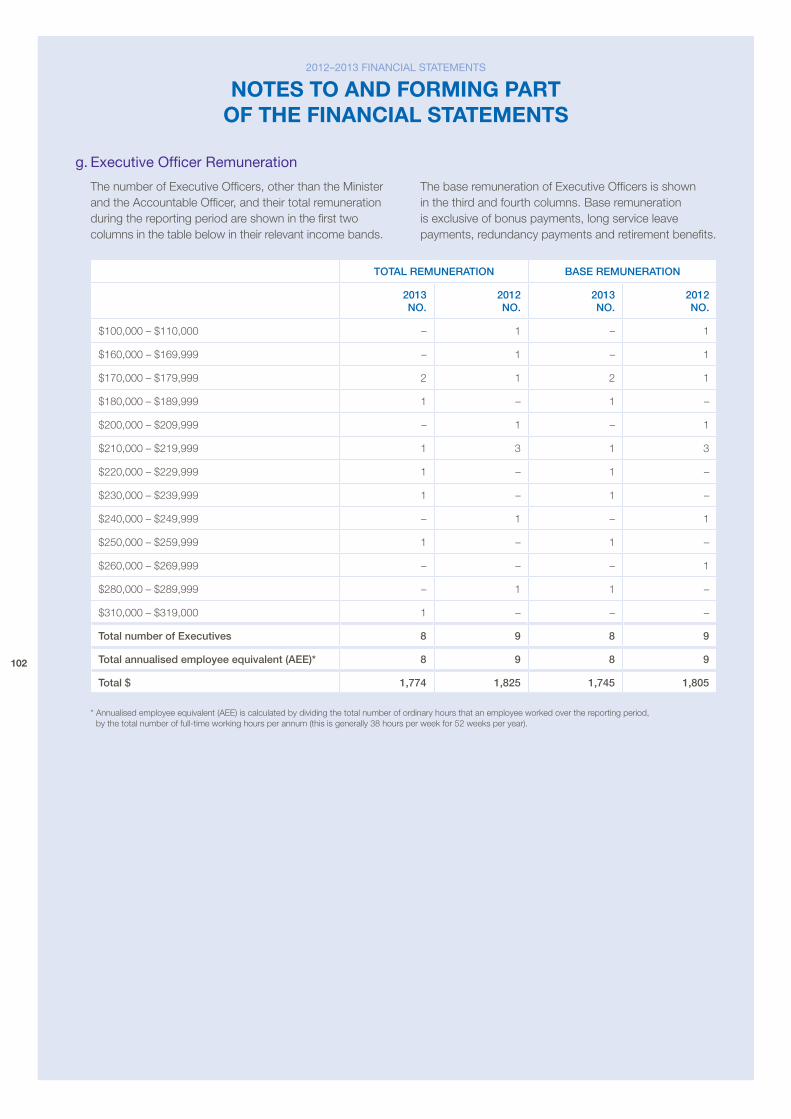
102
g. executive officer remuneration
The number of executive officers, other than the minister and the accountable officer, and their total remuneration during the reporting period are shown in the first two columns in the table below in their relevant income bands.
The base remuneration of executive officers is shown in the third and fourth columns. base remuneration is exclusive of bonus payments, long service leave payments, redundancy payments and retirement benefits.
tOtAL RemuneRAtIOn BASe RemuneRAtIOn
2013 nO.
2012 nO.
2013 nO.
2012 nO.
$100,000 – $110,000 – 1 – 1
$160,000 – $169,999 – 1 – 1
$170,000 – $179,999 2 1 2 1
$180,000 – $189,999 1 – 1 –
$200,000 – $209,999 – 1 – 1
$210,000 – $219,999 1 3 1 3
$220,000 – $229,999 1 – 1 –
$230,000 – $239,999 1 – 1 –
$240,000 – $249,999 – 1 – 1
$250,000 – $259,999 1 – 1 –
$260,000 – $269,999 – – – 1
$280,000 – $289,999 – 1 1 –
$310,000 – $319,000 1 – – –
total number of executives 8 9 8 9
total annualised employee equivalent (Aee)* 8 9 8 9
total $ 1,774 1,825 1,745 1,805
* annualised employee equivalent (aee) is calculated by dividing the total number of ordinary hours that an employee worked over the reporting period, by the total number of full-time working hours per annum (this is generally 38 hours per week for 52 weeks per year).
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements
ST
VIN
CEN
T’S
Ho
Sp
ITa
l’S
aN
NU
al
REp
oR
T 20
12–2
013
103
note 27: reMuneration of auditorS
2013 $’000
2012 $’000
audit fees paid or payable to the victorian auditor-General’s office for audit of the St vincent’s Hospital (melbourne) Limited’s financial statements
paid as at 30 June 51 43
payable as at 30 June 50 62
total paid and payable 101 105
note 28: eVentS occurrinG after reportinG date
There have been no significant events occurring after the reporting date that has any material impact on the results of the Hospital as reported in these financial statements.
note 29: redeVelopMent of tHe HoSpital (1996)
Hospital development agreement
The Hospital agreed with Nba Leasing proprietary Limited to develop a minimum 350 bed inpatient facility for the sum of $146 million in accordance with the agreed plans and specifications. The agreement provided that the Hospital should fund from its own resources any sum by which the Construction Cost exceeded the agreed redevelopment Cost of $135.3 million. In June 1996 the development was completed. Total costs for the development were $144.3 million. The following financial arrangements were entered into to fund the development of the hospital facility.
borrowings
The Hospital issued Inflation Indexed annuities of $80.0 million (face value) on 9 December 1992. payments are by quarterly instalments over a 25 year period with the first instalment made on 20 February 1993. The annuity has a quarterly base payment of $1,414,400 which is adjusted quarterly by the movement in the Consumer price Index. The total payment made to the annuity holders represents a progressive repayment of their loans plus interest. repayments are secured by a guarantee given by the Treasurer of the State of victoria under Section 30 of the Health Services Act and are funded by the twenty five year Health Services agreement. at 30 June 2013, the amount outstanding under this agreement is $26,564,000 (2012: $31,642,000) which has a corresponding receivable asset of $26,564,000 (2012: $31,642,000).
a Finance lease was entered into between the Trustees of the Sisters of Charity of australia and Nba Leasing proprietary Limited to fund the building fit out and equipment. The Hospital recognised this Finance Lease obligation in its accounts. excluded from the Finance Lease obligation is the value of a Zero Coupon bond purchased on 15 December 1992 by the Trustees of the Sisters of Charity of australia which was scheduled to mature in December 2008 with a value of $28 million. The proceeds of the bond were to be utilised to meet the final borrowing obligations to Nba Leasing proprietary Limited.
on 24th December 2001 the financial obligations to Nba Leasing proprietary Limited were extinguished by the payment of the Compensation amount of $153,669,755. This amount was funded by the Trustees of the Sisters of Charity of australia repaying their loan of $80,082,041, drawing down funds from the aIb reserve account of $7,926,816, sale of the Zero Coupon bond of $19,530,840, and a loan from Treasury Corporation of victoria of $46,130,058. There is no specific funding stream under the Health Service agreement to repay this loan to Treasury Corporation of victoria. repayments have been sourced from commercial returns and productivity savings achieved on an annual basis. The Treasury Corporation of victoria loan was fully repaid in December 2011.
campus lease
The Hospital has leased from the Trustees of the Sisters of Charity of australia the Hospital campus for a period of twenty five years commencing on 11th august, 1992. The Hospital is obliged to pay one hundred quarterly rental payments (part a rent) for the land commencing on 8 February 1993 and pay rent on building and equipment (part b rent) from the date of completion of the new hospital building. The part b rent under the Campus Lease was the sum required to allow the Trustees of the Sisters of Charity of australia to meet their obligations to Nba Leasing proprietary Limited under the Lease. The part b rent ceased on 24 December 2001 with the payment of the compensation amount (refer above), whilst part a rent continues.
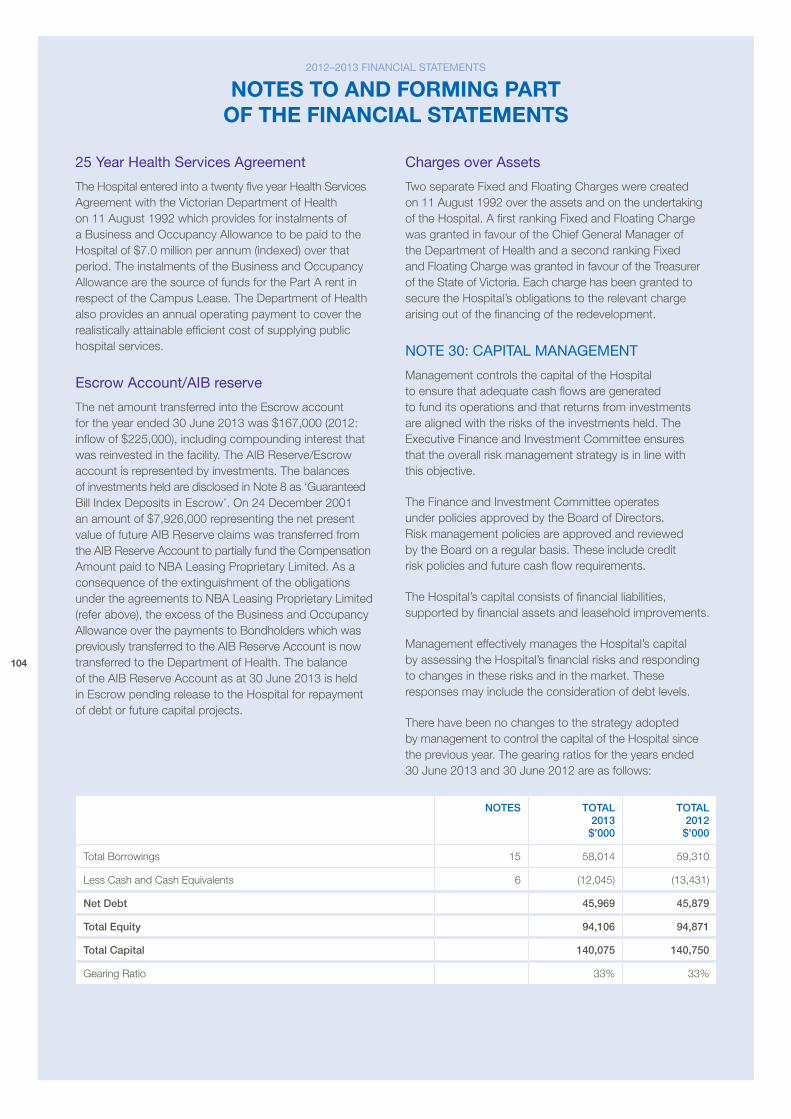
104
25 year Health Services agreement
The Hospital entered into a twenty five year Health Services agreement with the victorian Department of Health on 11 august 1992 which provides for instalments of a business and occupancy allowance to be paid to the Hospital of $7.0 million per annum (indexed) over that period. The instalments of the business and occupancy allowance are the source of funds for the part a rent in respect of the Campus Lease. The Department of Health also provides an annual operating payment to cover the realistically attainable efficient cost of supplying public hospital services.
escrow account/aib reserve
The net amount transferred into the escrow account for the year ended 30 June 2013 was $167,000 (2012: inflow of $225,000), including compounding interest that was reinvested in the facility. The aIb reserve/escrow account is represented by investments. The balances of investments held are disclosed in Note 8 as ‘Guaranteed bill Index Deposits in escrow’. on 24 December 2001 an amount of $7,926,000 representing the net present value of future aIb reserve claims was transferred from the aIb reserve account to partially fund the Compensation amount paid to Nba Leasing proprietary Limited. as a consequence of the extinguishment of the obligations under the agreements to Nba Leasing proprietary Limited (refer above), the excess of the business and occupancy allowance over the payments to bondholders which was previously transferred to the aIb reserve account is now transferred to the Department of Health. The balance of the aIb reserve account as at 30 June 2013 is held in escrow pending release to the Hospital for repayment of debt or future capital projects.
charges over assets
Two separate Fixed and Floating Charges were created on 11 august 1992 over the assets and on the undertaking of the Hospital. a first ranking Fixed and Floating Charge was granted in favour of the Chief General manager of the Department of Health and a second ranking Fixed and Floating Charge was granted in favour of the Treasurer of the State of victoria. each charge has been granted to secure the Hospital’s obligations to the relevant charge arising out of the financing of the redevelopment.
note 30: capital ManaGeMent
management controls the capital of the Hospital to ensure that adequate cash flows are generated to fund its operations and that returns from investments are aligned with the risks of the investments held. The executive Finance and Investment Committee ensures that the overall risk management strategy is in line with this objective.
The Finance and Investment Committee operates under policies approved by the board of Directors. risk management policies are approved and reviewed by the board on a regular basis. These include credit risk policies and future cash flow requirements.
The Hospital’s capital consists of financial liabilities, supported by financial assets and leasehold improvements.
management effectively manages the Hospital’s capital by assessing the Hospital’s financial risks and responding to changes in these risks and in the market. These responses may include the consideration of debt levels.
There have been no changes to the strategy adopted by management to control the capital of the Hospital since the previous year. The gearing ratios for the years ended 30 June 2013 and 30 June 2012 are as follows:
nOteS tOtAL 2013 $’000
tOtAL 2012 $’000
Total borrowings 15 58,014 59,310
Less Cash and Cash equivalents 6 (12,045) (13,431)
net Debt 45,969 45,879
total equity 94,106 94,871
total Capital 140,075 140,750
Gearing ratio 33% 33%
2012–2013 financial StateMentS
nOtes tO and fOrmIng part Of the fInancIal statements


St Vincent’s Hospital acknowledges the traditional owners of this land, the Wurundjeri people and all the members of the Kulin nations. We pay our respects to their Elders, past and present. St Vincent’s Hospital is Victoria’s largest metropolitan provider of Aboriginal and Torres Strait Islander healthcare. We continue to develop our relationship with the Aboriginal and Torres Strait Islander communities and are proud to be acknowledged as a centre of excellence in healthcare for Indigenous Australians.
St Vincent’s Hospital (Melbourne) acknowledges the support of the Victorian Government.
St Vincent’s Hospital (Melbourne) LimitedACN 052 110 755ABN 22 052 110 75541 Victoria ParadeFitzroy Victoria 3065Telephone 03 9288 2211Facsimile 03 9288 3399