36 pleural effusion with otherwise normal appearing chest
TRANSCRIPT
36 Pleural Effusion with Otherwise Normal-Appearing Chest
CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
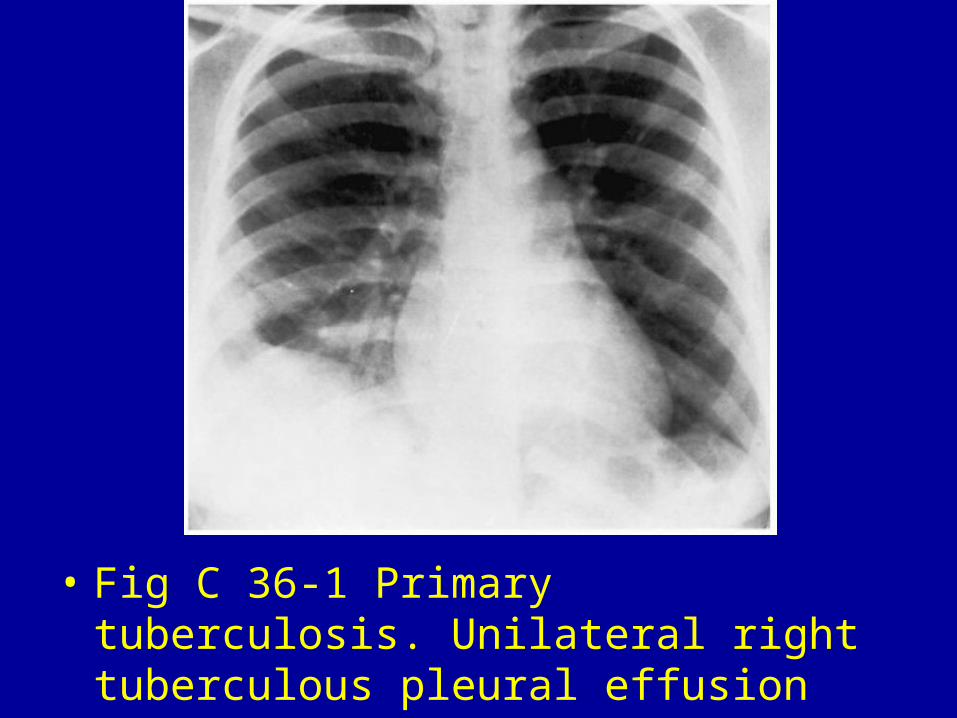
• Fig C 36-1 Primary tuberculosis. Unilateral right tuberculous pleural effusion without parenchymal or lymph node involvement.
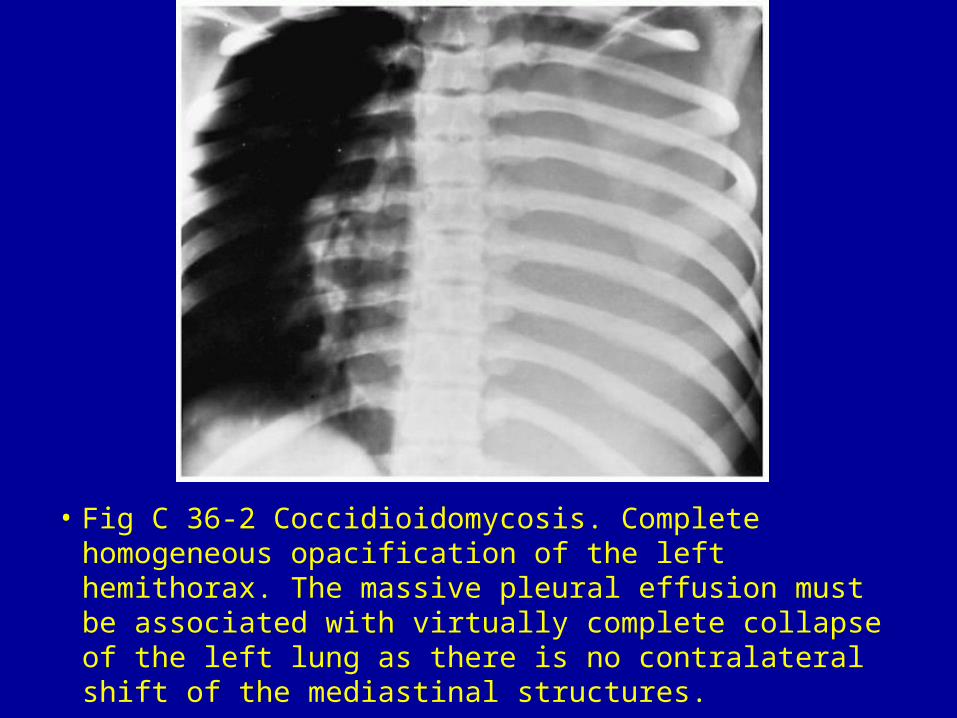
• Fig C 36-2 Coccidioidomycosis. Complete homogeneous opacification of the left hemithorax. The massive pleural effusion must be associated with virtually complete collapse of the left lung as there is no contralateral shift of the mediastinal structures.
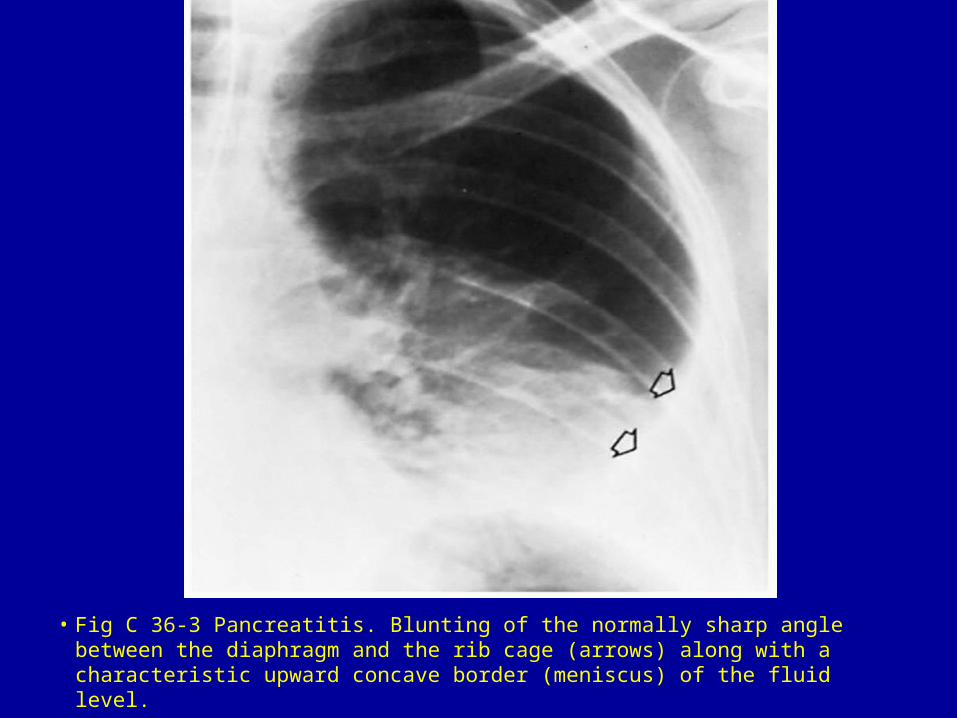
• Fig C 36-3 Pancreatitis. Blunting of the normally sharp angle between the diaphragm and the rib cage (arrows) along with a characteristic upward concave border (meniscus) of the fluid level.
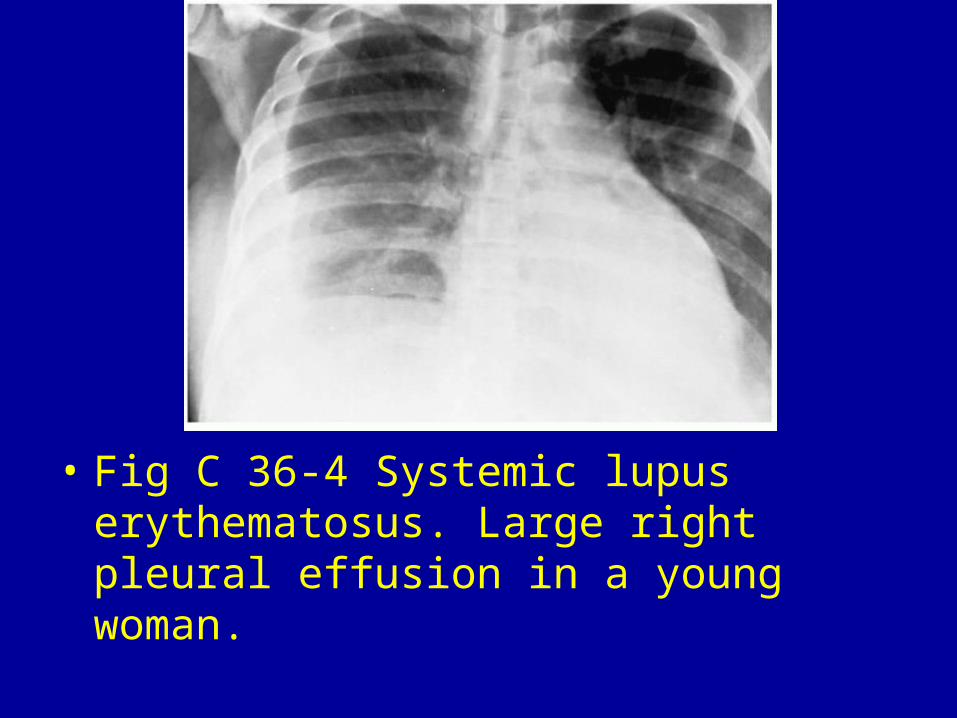
• Fig C 36-4 Systemic lupus erythematosus. Large right pleural effusion in a young woman.
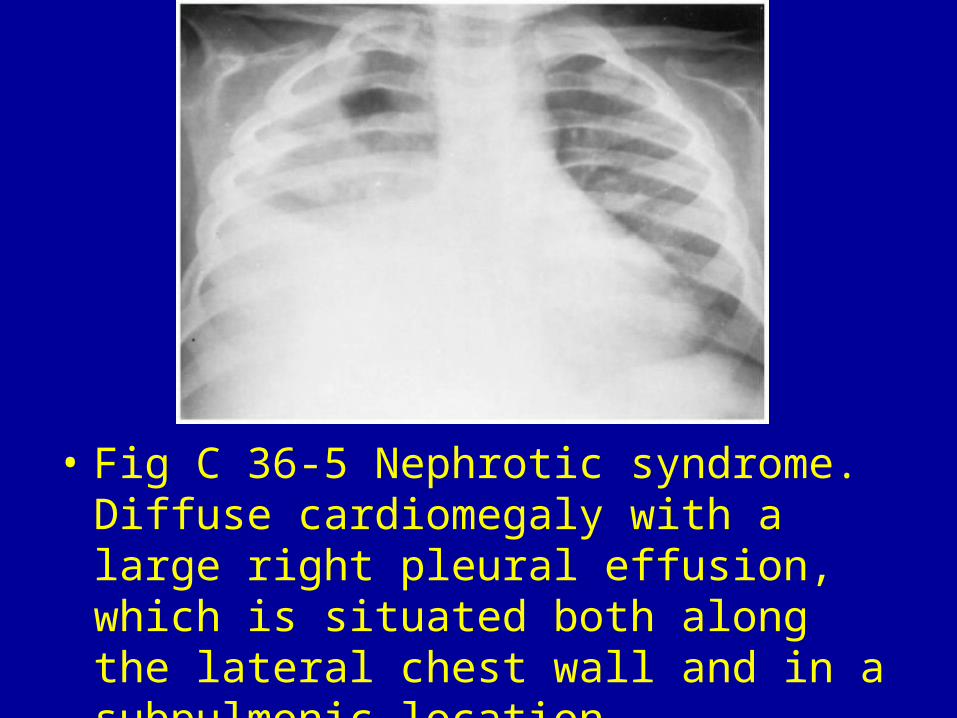
• Fig C 36-5 Nephrotic syndrome. Diffuse cardiomegaly with a large right pleural effusion, which is situated both along the lateral chest wall and in a subpulmonic location.
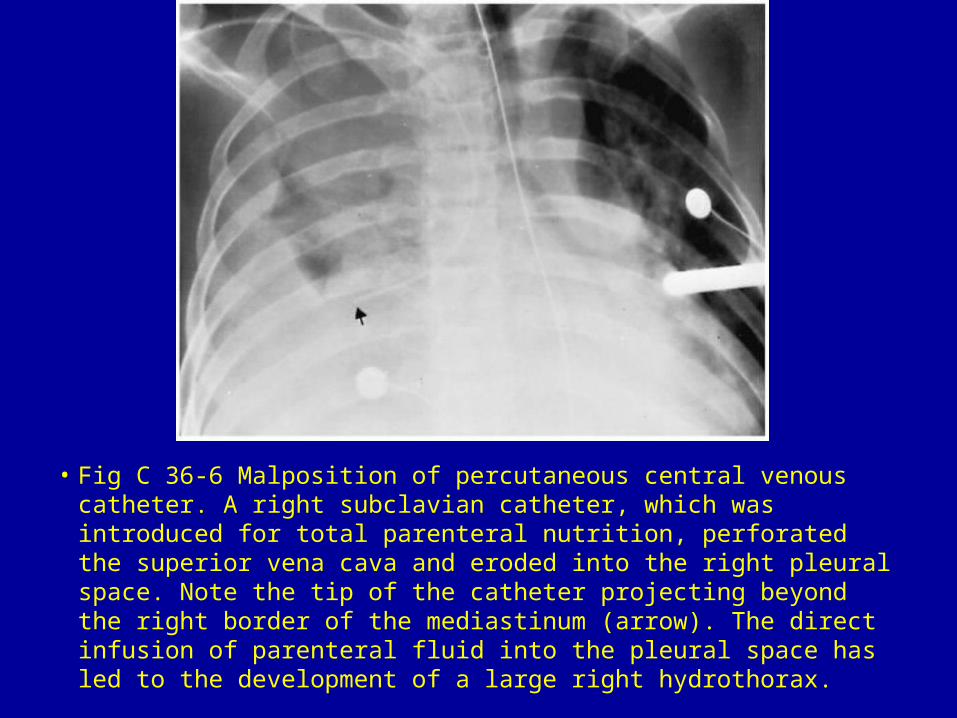
• Fig C 36-6 Malposition of percutaneous central venous catheter. A right subclavian catheter, which was introduced for total parenteral nutrition, perforated the superior vena cava and eroded into the right pleural space. Note the tip of the catheter projecting beyond the right border of the mediastinum (arrow). The direct infusion of parenteral fluid into the pleural space has led to the development of a large right hydrothorax.

