26.8.2015koage15.ppt1 disorders of haemostasis - i the new conception of coagulation lectures from...
TRANSCRIPT
19.04.2023 koage15.ppt 1
Disorders of haemostasis - IDisorders of haemostasis - IThe new conception of The new conception of
coagulationcoagulation
Disorders of haemostasis - IDisorders of haemostasis - IThe new conception of The new conception of
coagulationcoagulation
Lectures from Lectures from patpathhologicologicalal phphyyssioliolooggyy
Study materials from pathological physiology, school year 2014/2015
© Oliver Racz

19.04.2023 koage.ppt 2
System of haemostasis• Maintains blood fluidity• Local clot formation after vessel injury• Maintains vessel wall integrity• Cooperation of vessel wall cells,
thrombocytes, other blood cells, coagulation/anticoagulation factors & the fibrinolytic system
• Nonhaemostatic functions of the system
– Inflammation, immunity, glucose and lipid metabolism, angiogenesis, etc

19.04.2023 koage.ppt 3
HistoryBleeding after circumcision – TalmudSchmidt 1861 - Morawetz 1905
I. ThromboplastinII. ThrombinIII. FibrinogenIV. Calcium
1937 Quick, laboratory methods1950 – 1959 DIC, Hardaway, McKay1964 MacFarlane, Davie, Ratnoff - classic coagulation
cascade1974 The role of vitamin KXXI. century – new conception, molecular basis of
diseases
19.04.2023 koage.ppt 4
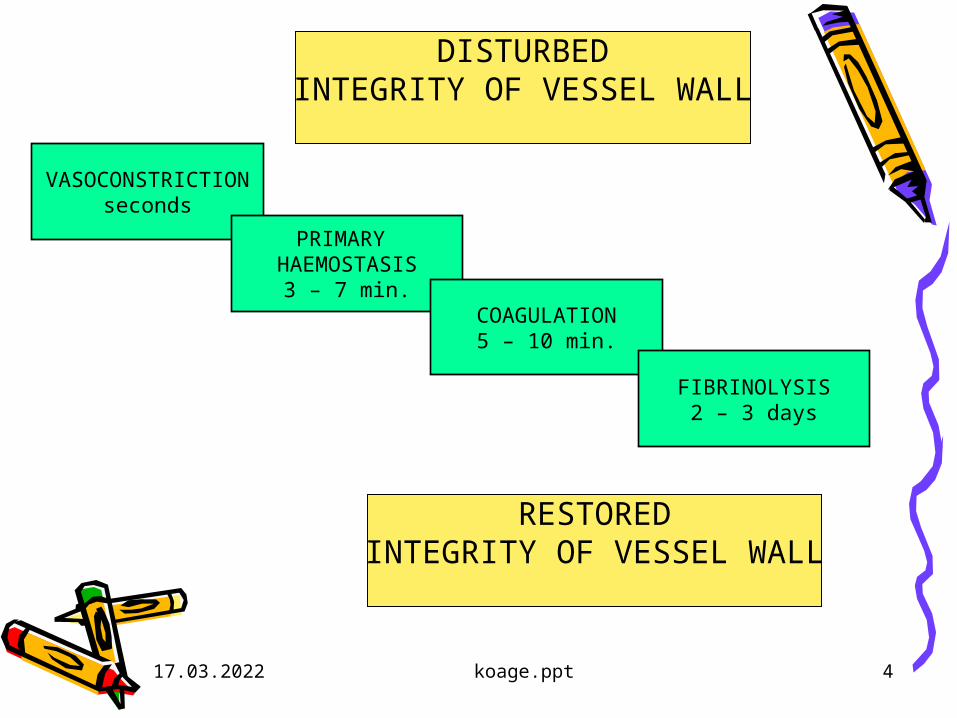
DISTURBEDINTEGRITY OF VESSEL WALL
VASOCONSTRICTIONseconds
PRIMARY HAEMOSTASIS
3 – 7 min.COAGULATION
5 – 10 min.
FIBRINOLYSIS2 – 3 days
RESTOREDINTEGRITY OF VESSEL WALL

19.04.2023 koage.ppt 5
Repetion of physiology• Physiology of haemostasis (factors,
thrombocytes, pathway of activation)• Biochemical characterisation of
coagulation factors and the role of vitamin K, anticoagulants
• The transformation of fibrinogen to fibrin, fibrinolysis and its regulation
19.04.2023 koage.ppt 6
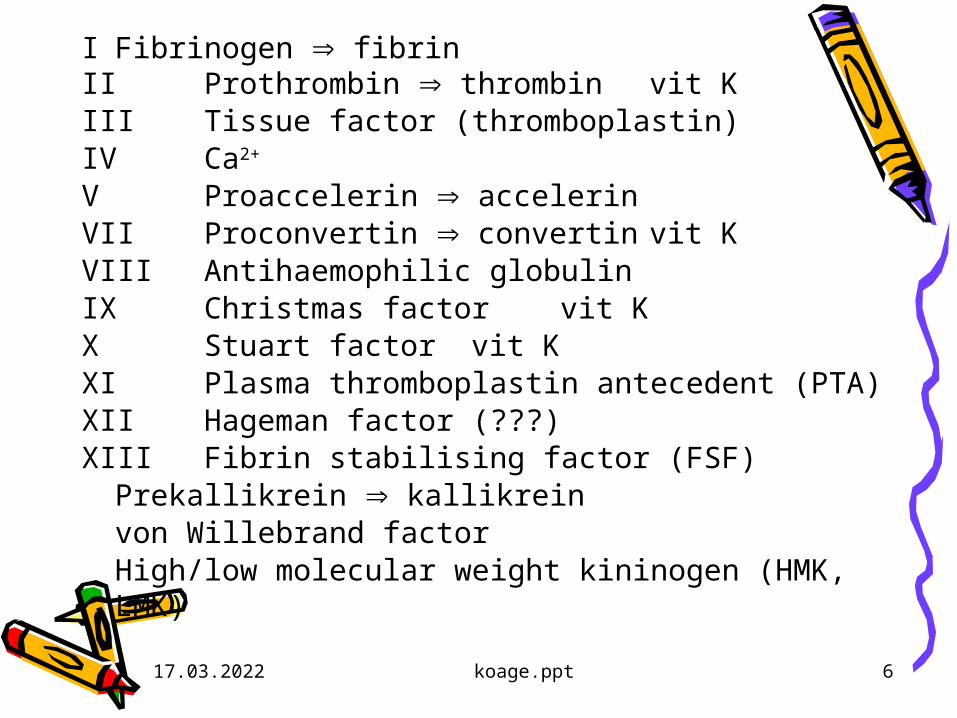
I Fibrinogen fibrinII Prothrombin thrombin vit KIII Tissue factor (thromboplastin)IV Ca2+
V Proaccelerin accelerinVII Proconvertin convertin vit KVIII Antihaemophilic globulinIX Christmas factor vit KX Stuart factor vit KXI Plasma thromboplastin antecedent (PTA)XII Hageman factor (???)XIII Fibrin stabilising factor (FSF)
Prekallikrein kallikreinvon Willebrand factorHigh/low molecular weight kininogen (HMK,
LMK)
19.04.2023 koage.ppt 7
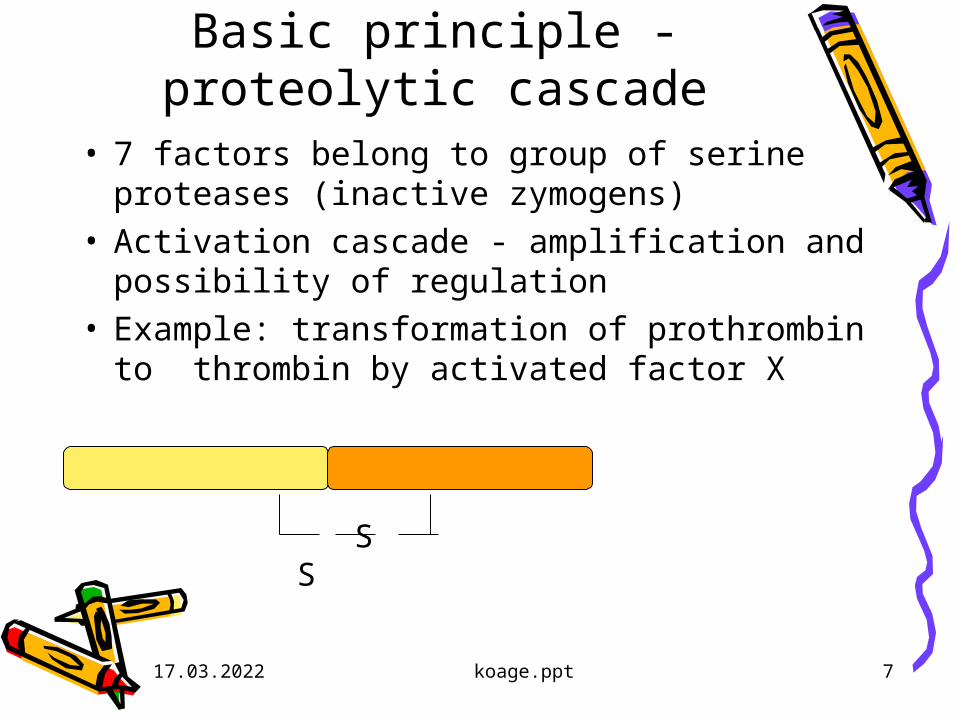
Basic principle - proteolytic cascade
• 7 factors belong to group of serine proteases (inactive zymogens)
• Activation cascade - amplification and possibility of regulation
• Example: transformation of prothrombin to thrombin by activated factor X
S S

19.04.2023 koage.ppt 8
Basic principle - proteolytic cascade
• Example: transformation of prothrombin to thrombin by activated factor X
S S
Xa

19.04.2023 koage.ppt 9
Basic principle - proteolytic cascade
• Example: transformation of prothrombin to thrombin by activated factor X
S S
Xa
19.04.2023 koage.ppt 10
The role of vitamin K• Rats with vitamin K deficiency• PIVKA = protein induced in vitamin K absence• Similar to prothrombin - not active• Vitamin K is the coenzyme of glutamate
carboxylase, which converts
• glutamic acid -carboxyglutamic acid
• Two COO- s bind Ca2+
• In prothrobin there are 10 such places

19.04.2023 koage.ppt 11
O
-NH-CH-C-
CH2
CH2
COO-
O
-NH-CH-C-
CH2
CH- COO-
COO-
19.04.2023 koage.ppt 12
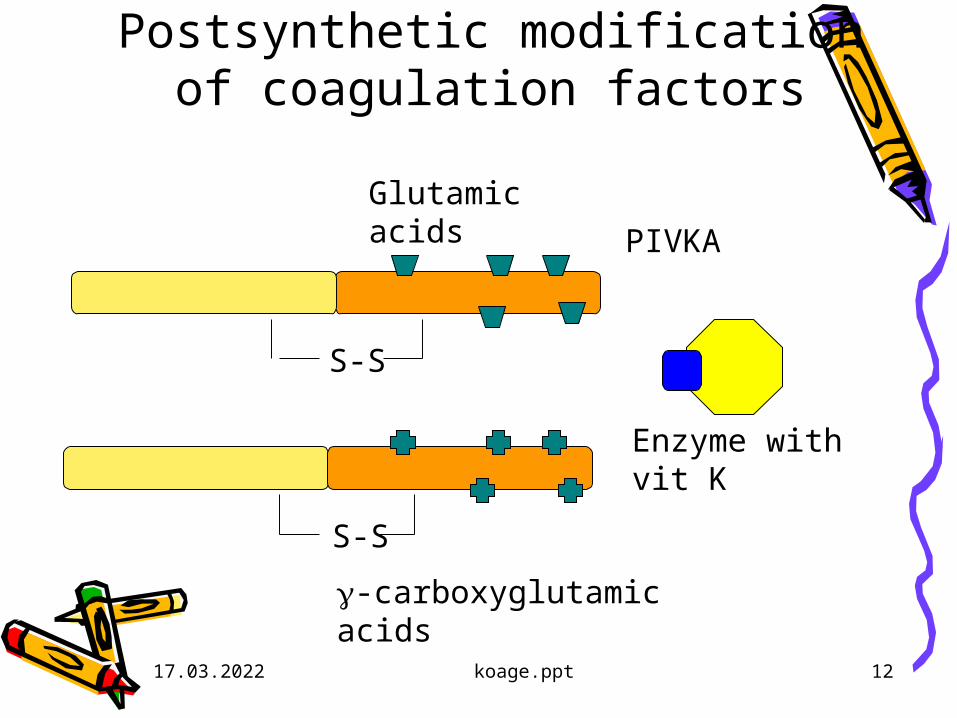
Postsynthetic modification of coagulation factors
S-S
S-S
Enzyme with vit K
Glutamic acids
-carboxyglutamic acids
PIVKA

19.04.2023 koage.ppt 13
New conception• Initiation – minimal transformation
of prothrombin to thrombin (no clot)
• Amplification• Termination• Doubts about the in vivo role of
„contact“ system (XII)
19.04.2023 koage.ppt 14
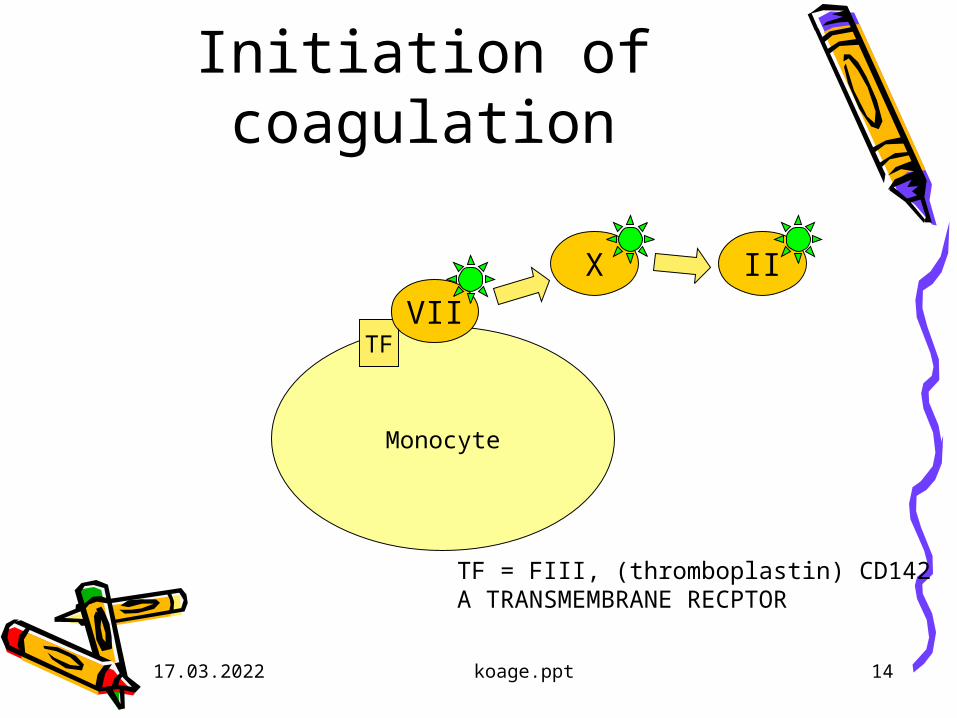
Initiation of coagulation
Monocyte
TFVII
X II
TF = FIII, (thromboplastin) CD142 A TRANSMEMBRANE RECPTOR

19.04.2023 koage.ppt 15
Amplification of coagulation IActivation of thrombocytes
II vWfVIII
X
XI
IX
V
thrombocyte
flip-flop of
phospholipids

19.04.2023 koage.ppt 16
Amplification of coagulation II
Internal amplification loop
XI
II VIIIvWf
VX
IX

19.04.2023 koage.ppt 17
Amplification of coagulation IIIActivation of IX/VIII, formation of tenase
XIIX/VIII
II vWf
VX

19.04.2023 koage.ppt 18
Amplification of coagulation IVformation of prothrombinase
XI
X/V
IX/VIII
II
vWf

19.04.2023 koage.ppt 19
Amplification & termination
• Activation of thrombocytes, flip-flop of phospholipids
• Activation of XI – amplification loop• Activation of IX and VIII → TENASE• Tenase activates X and V – PROTHOROMBINASE• production of huge amounts of thrombin• Transformation of fibrinogen to fibrin → CLOT• Formation of crosslinks in fibrin network (XIII) →
STABLE CLOT

19.04.2023 koage.ppt 20
Revision of „contact“ system
• John Hageman (deficiency of XII) died in 1968 on thrombembolic disease after a trauma
• He probably did not read the textbooks of physiology!
• According to current opinion the system has rather nonhaemostatic functions

19.04.2023 koage.ppt 21
Structure of fibrinogen
6 chains, 2*
Proteolytic removal of peptides A,B
Polymerisation

19.04.2023 koage.ppt 22
Polymerisation of fibrinogen
19.04.2023 koage.ppt 23
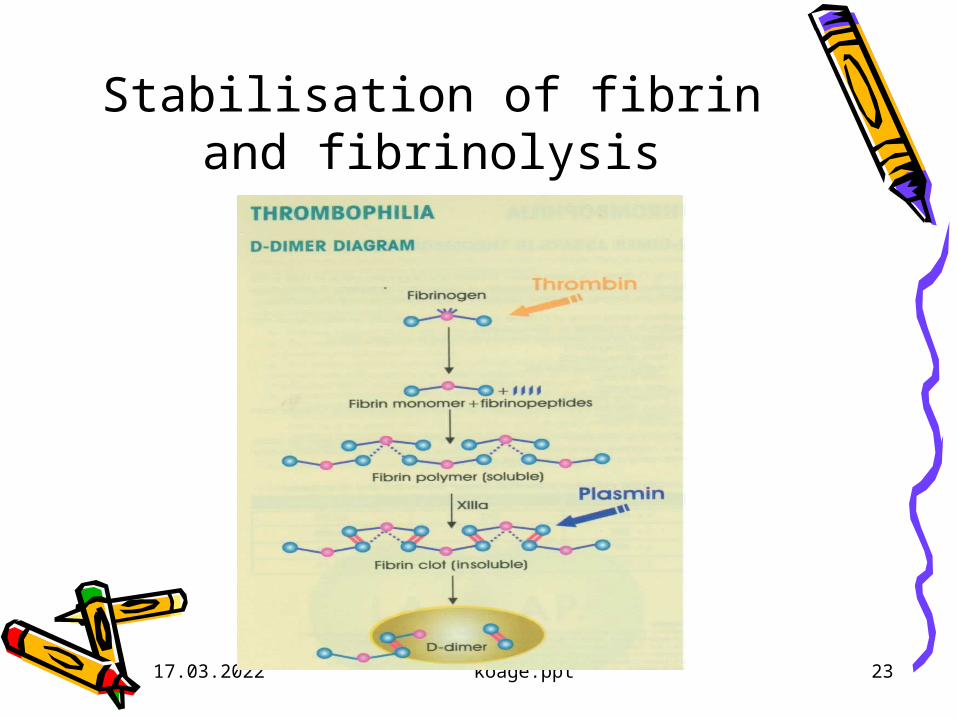
Stabilisation of fibrin and fibrinolysis

19.04.2023 koage.ppt 24
The anticoagulant system
• Serpins – inhibitors of proteases– Inhibitor of initiation - TFPI– Antithrombin (III)
• Protein C together with S are the most important inhibitors of amplification – proteolytic degradation of V and VIII

19.04.2023 koage.ppt 25
The fibrinolytic – plasminogen system
• PLASMINOGEN – 92 kDa glykoprotein• Two step activation to active form, PLASMIN by
tissue PLASMINOGEN ACTIVATOR - tPA• Plasmin degrades fibrin clot (and has a lot of
nonhaemostatic functions)• The process is inhibited by PAI – 1, an
antagonist of tPA Important – the activities of tPA and PAI are
oscillating in a broad range – effects of stress, adrenaline, antidiuretic hormone, obesity (!) and gene polymorphism

19.04.2023 koage.ppt 26
FIBRIN CLOT
PLASMINOGEN
PLASMIN
FDP
D-DIMERS
PAI-1tPA- +

19.04.2023 koage.ppt 27
Disorders of haemostasis - IIDisorders of haemostasis - IIPrinciples of diagnosticsPrinciples of diagnostics
Disorders of haemostasis - IIDisorders of haemostasis - IIPrinciples of diagnosticsPrinciples of diagnostics
Lectures from Lectures from patpathhologicologicalal phphyyssioliolooggyy
Study materials from pathological physiology, school year 2005/2006
© Oliver Racz, 12. 2. 2006

19.04.2023 koage.ppt 28
Diagnostics IRumpel-Leede, test of capillary fragility Bleeding time (standardized methods!)
normal: 4 - 6 min.; pathological: > 10 min.Whole blood coagulation time (Lee-White) normal: 4 - 8 min.Platelet count (automatic analyzers)
norm: 140 - 440*109/l100*109/l thrombocytopenia50*109/l risk of longer bleeding after an injury or
surgery40*109/l spontaneous bleeding (or not)10*109/l danger of fatal bleeding (GIT, NS)
19.04.2023 koage.ppt 29
Diagnostics IIprinciple of coagulation tests
• Step 1: Anticoagulated blood (Ca2+ binding by citrate);• Step 2: Removal of RBC, LE, TH (centrifugation)• Step 3: Addition of surplus Ca2+ & activators to plasma• Step 4: Measurement of time until the first fibrin filaments
are formed• Expression of results
A. In seconds (international standardized calibrators, QC)B. In relative units compared to norm (time patient/control)
C. INR = International Normalized Ratio

19.04.2023 koage.ppt 30
Diagnostics IIIcoagulation tests - examples
Prothrombin time - QuickOral anticoagulant therapy control (OAC)
Plasma + Ca2++ tissue thromboplastinNorm: 11 - 15 secNecessary factors: VII, X, V, II
APTT = activated partial thromboplastin timePlasma + Ca2+ + caolin (negat. charge) + phospholipid Norm: 35 - 45 sec.Necessary factors: XII, XI, IX, and VII, X, V, II

19.04.2023 koage.ppt 31
Prothrombin and APTT assay
Prothrombin (Quick)
APTT

19.04.2023 koage.ppt 32
Diagnostics IV - other assays
• Fibrinogen concentration (2 - 4 g/l)• Fibrin & fibrinogen degradation products
– D-dimer, degradation product of fibrin clot by plasmin
diagnostics of DIC
exclusion of deep venous thrombosis and pulmonary embolism (limit 500 g/l)
• Special assays – aggregometry, adhaesion of thrombocytes
• Direct measurement of factors
•Assays of polymorphisms, mutations

19.04.2023 koage.ppt 33
Disorders of haemostasis - IDisorders of haemostasis - IIIIIThe most important diseasesThe most important diseasesDisorders of haemostasis - IDisorders of haemostasis - IIIIIThe most important diseasesThe most important diseases
Lectures from Lectures from patpathhologicologicalal phphyyssioliolooggyy
Study materials from pathological physiology, school year 2005/2006
© Oliver Racz, 12. 2. 2006

19.04.2023 koage.ppt 34
Syllabus1. Classification2. Symptomatology3. Disorders of primary haemostasis -
thrombocytopenia & thrombocytopathy4. Coagulation disorders5. Vascular purpuras6. Disseminated intravascular coagulation -
DIC7. Thrombembolic conditions
19.04.2023 koage.ppt 35
ClassificationA. HAEMORRHAGIC DIATHESES
A1. PLATELET DISORDERS A2. COAGULOPATHIES A3. DISORDERS OF THE VESSEL WALL
(In each group inherited and acquired conditions)
B. THROMBEMBOLIC CONDITIONS Congenital thrombophilia and othersThe association betweeen coagulation & atherosclerosis
C. DISSEMINATED INTRAVASCULAR COAGULATION
19.04.2023 koage.ppt 36
ThrombocytopeniaThree mechanisms:• A. Insufficient production of
megakaryocytes• B. Increased destruction of
thrombocytes• C. Abnormal distribution of
thrombocytes
19.04.2023 koage.ppt 37
ThrombocytopeniaA. Insufficient production of
megakaryocytes• Bone marrow damage: drugs,
toxins, radiation, infection, tumors, leukaemia, fibrosis
• Congenital insufficiency• Cobalamin and folic acid deficiency

19.04.2023 koage.ppt 38
Thrombocytopenia
B. Increased destruction– Idiopathic thrombocytopenic purpura
(ITP) - autoimmune disease– Rh group incompatibility– DIC– Arteficial heart valves
C. DistributionSplenomegalia and hypersplenism

19.04.2023 koage.ppt 39
Thrombocytopathy• A. Congenital
– thrombastenia - m. Glanzman AR– insufficient aggregation of platetelets
• B. Acquired– Acetylsalicylic acid, phenylbutasone– Uremia
19.04.2023 koage.ppt 40
Hereditary disorders of coagulation
• Hemophilia A (1/10 000)– Unexpected fluctuation of clinical
symptomatology– Long repeated bleedings– Internal bleedings– Intracranial bleeding (can be fatal)– Chronic anaemia, icterus– Severe damage of joints
• Hemophilia B (IX- XR) C (XI - AR), less severe

19.04.2023 koage.ppt 41
f. VIII concentration and symptoms
Concentration, g/l Symptoms
100 – 50
50 - 30 Intensive and long lastingbleeding after big trauma
30 – 5 Long bleeding after surgery andminor trauma
5 – 1 Intensive/long bleeding afterminor trauma
< 1 Spontaneous bleeding
19.04.2023 koage.ppt 42
von Willebrand disease
• In the past considered as a moderate form of hemophilia
• Von Willebrand factor = big multimeric protein • Synthesised in endothel and megakaryocytes• Function – contact of damaged endothel and
platelets, mutual interaction of thromobocytes• stabilisation of factor VIII. • Concentration in people with blood group AB > 0
19.04.2023 koage.ppt 43
von Willebrand
• Deficiency is probably common (1-3 %) mostly asymptomatic
• Together with other factors can manifest (acetylsalicylic acid, OAC therapy) as mucosal bleeding, bleeding after tooth extraction, menorrhagia
• Type I, IIa, IIb, III
19.04.2023 koage.ppt 44
Acquired coagulation disorders
• Vitamin K deficiency– Newborns, malabsorbtion, obstructve
icterus, etc.
• Anticoagulant drugs– Dicumarols (antivitamin K);– Heparin (activator of antithrombin,
inactivation of X, IX & XI)– Streptokinase
• Liver disease
19.04.2023 koage.ppt 45
Vascular purpura
• Relatively common condition• skin eruption in infectious diseases in
children• senile purpura• scorbut, scurvy - deficiency of vitamin
C– Disorder of collagen synthesis (proline -
hydroxyproline) and abnormal platelet function. Perifollicular skin, gingival, mucosa muscle, GIT bleeding, hematuria. Skin hyperkeratosis.

19.04.2023 koage.ppt 46
Hereditary disordes of vessel wall
Hereditary haemorrhagic teleangiectasy (m. Osler-Weber-Rendu), AD, Epistaxis, teleangiectasy Anaemia, DIC, liver cirrhosis Lack of elastic fibers in vessel wall
Other hereditary collagen diseasesMarfan - Lincoln, Ehlers-Danlos - Paganini
19.04.2023 koage.ppt 47
Disseminated intravascular coagulation,
DIC
• Consumption coagulopathy• Life threating disorder (Death Is
Coming !)• Generalised activation of
haemostasis• Thrombosis and bleeding at the
same time, tissue hypoxia

19.04.2023 koage.ppt 48
DIC - causes
Complications of gravidity. Amniotic fluid embolisation. Preeclampsia, eclampsia
Sepsis & septic shock G- infections (endotoxin), meningococci, pneumococci, plasmodium malariaeSy Waterhouse-Friederichsen as a
consequence of meningitis
Neoplastic disease: Lung, gastric, breast, prostata Ca, leukaemia

19.04.2023 koage.ppt 49
DIC - causes
Liver failureHaemolysis (incompatible transfusion)Trauma (haemorrhagic shock, burns)Rejection of transplanted organsTropical snake toxins
19.04.2023 koage.ppt 50
Pathogenesis of DICA. Generalised activation of coagulationB. Thrombosis
Microthrombi in circulation;Deposits of microthrombi in tissues and
their damageC. Decreased haemostasis
Decrease of platelet number, factor concentration
Activation of fibrinolysisD. BleedingE. Disorder of nonhaemostatic functions
of the system

19.04.2023 koage.ppt 51
BLEEDING
GENERALISED ACTIVATION OF COAGULATION
MICROTHROMBI
DECREASE OF PLATELETS & COAGULATION FACTORS
ACTIVATION OF FIBRINOLYSIS
EMBOLISATION

19.04.2023 koage.ppt 52
BLEEDING
GENERALISED ACTIVATION OF COAGULATION
MICROTHROMBS
DECREASE OF PLATELETS & COAGULATION FACTORS
ACTIVATION OF FIBRINOLYSIS
EMBOLISATION
19.04.2023 koage.ppt 53
Symptoms and forms tissue ischaemia, gangrena of fingers bleeding (after injections); kidney failure, anuria; haemorrhagic necrosis of adrenal cortex - sy
Waterhouse-Friderichsen; haemolytic anaemia, haemoglobinuria;Beginning acute or subacuteStages: Compensated, decompensated and
manifest
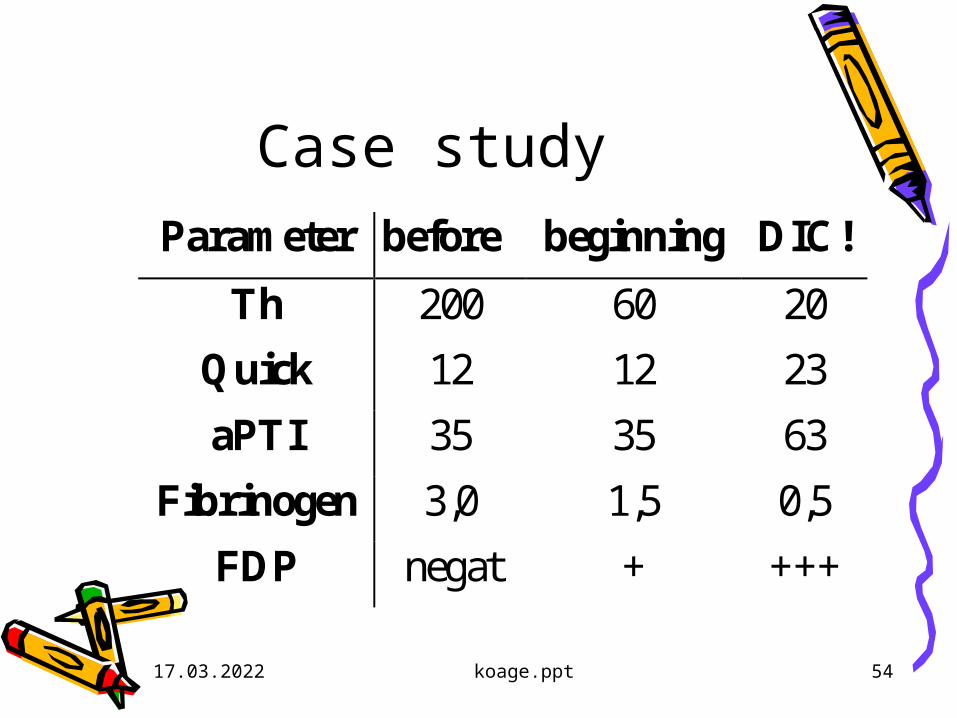
19.04.2023 koage.ppt 54
Case studyParameter before beginning DIC!
Th 200 60 20
Quick 12 12 23
aPTI 35 35 63
Fibrinogen 3,0 1,5 0,5
FDP negat + +++

19.04.2023 koage.ppt 55
Our case study• As an editor of a medical journal I
visited our publisher, a cca 50 y old lady.
• Complaining about respiratory condition, therapy resistant
• And also swelling of the legs• Nothing serious?

19.04.2023 koage.ppt 56
Our case study• Complaining about respiratory
condition, therapy resistant• And also swelling of the legs• Nothing serious?• Immediately sent to hospital:
– D-dimers extremely high– X-ray repeated small embolisation

19.04.2023 koage.ppt 57
Thrombosis, thrombembolia, thrombophilia
• Factors– endothel (aterosclerosis, inflammatio)– thrombocytes– coagulation pro & contra, fibrinolysis
(tPA/PAI!)– circulation (stasis)
• Forms– venous thrombosis– arterial (MI)– intracardial (mitral stenosis)– diffuse (DIC)
• Occlusive – nonocclusive clots•Embolia – lung, brain, paradox,
microembolisation
19.04.2023 koage.ppt 58
Trombophiliacomplex disease
• Immobilisation• Stasis• Varices• Gravidity, hormonal
anticonception• Trauma, burns• Malignant tumors• ATHEROSCLEROSIS
• DEFICIENCY OF ANTICOAGULANT FACTORSANTITHROMBIN, 1965PROTEIN C, 1981
• INCREASED ACTIVITY OF PROCOAGULANT FACTORS (VII)
• DECREASED FIBRINOLYSIS
19.04.2023 koage.ppt 59
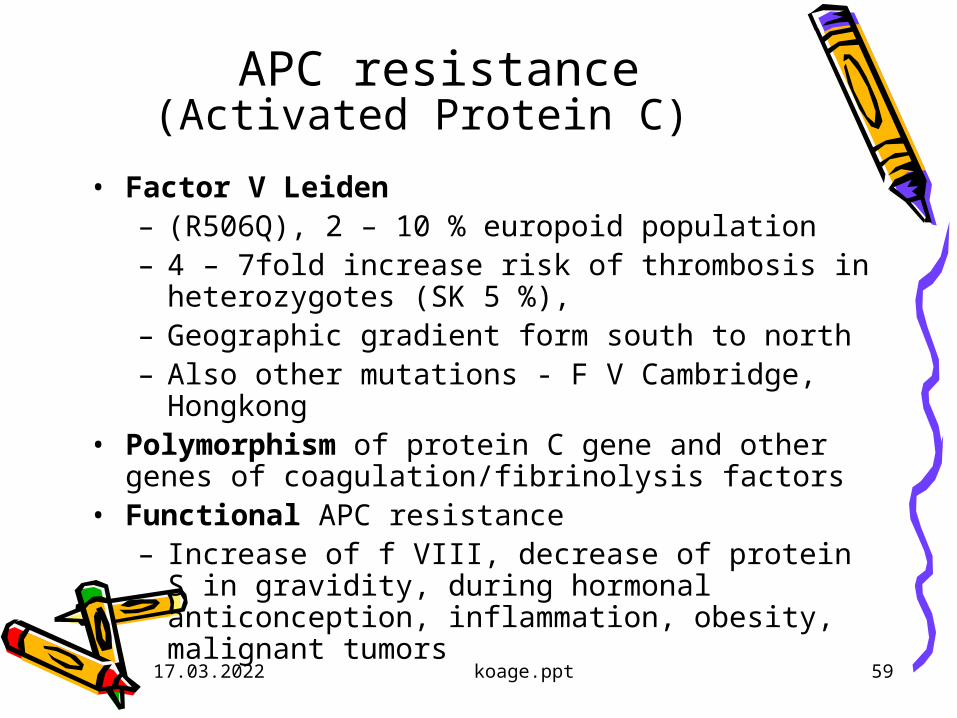
APC resistance(Activated Protein C)
• Factor V Leiden – (R506Q), 2 – 10 % europoid population– 4 – 7fold increase risk of thrombosis in
heterozygotes (SK 5 %), – Geographic gradient form south to north– Also other mutations - F V Cambridge,
Hongkong• Polymorphism of protein C gene and other genes
of coagulation/fibrinolysis factors• Functional APC resistance
– Increase of f VIII, decrease of protein S in gravidity, during hormonal anticonception, inflammation, obesity, malignant tumors

12.2.2006 koage.ppt 18
Amplifi cation of coagulation I Vf ormation of prothrombinase
XI
X/V
IX/VIII
II
vWf
12.2.2006 koage.ppt 18
Amplifi cation of coagulation I Vf ormation of prothrombinase
XI
X/V
IX/VIII
II
vWf
X/V Leiden
APC
19.04.2023 koage.ppt 61
Trombophiliacomplex disease
• Immobilisation• Stasis• Varices• Gravidity, hormonal
anticonception• Trauma, burns• Malignant tumors• ATHEROSCLEROSIS
• DEFICIENCY OF ANTICOAGULANT FACTORSANTITHROMBIN, 1965PROTEIN C, 1981
• INCREASED ACTIVITY OF PROCOAGULANT FACTORS
• DECREASED FIBRINOLYSIS
19.04.2023 koage.ppt 62
Bleeding vs clotting !
• Haemophilia: 1 in 10 000 (Sk 400)• Other bleeding disorders (Th) not so
rare or clinically silent (vWd)• Thrombophilia 1 in 10 or even more
in older, obese, sick people!!!• In EU more than 540 000 deaths,
often nondiagnosed!!!

19.04.2023 koage.ppt 63
Bleeding vs clotting !
• Thrombophilia 1 in 10 or even more in older, obese, sick people!!!
• (ATRIAL FIBRILLATION, MALIGNANCIES, BURNS, DIABETES, INFECTIONS, POST SURGERY…..
• Both in DIC• Both in MI secondary prevention –
anticoagulant treatment – WALKING THE TIGHTROPE