2310 09 tuberculosis - amarillo college · pulmonary function test findings moderate and extensive...
TRANSCRIPT

RSPT 2310 Tuberculosis
1
Tuberculosis
RSPT 2310
Anatomic Altera8ons of the Lungs
Anatomic Altera8ons of the Lungs
• Tuberculosis (TB) is a contagious chronic bacterial infec8on – primarily affects the lungs – may involve almost any part of the body
• Clinically, TB is classified – primary tuberculosis – post-‐primary tuberculosis – disseminated tuberculosis
Primary Tuberculosis
• Progression – follows the pa8ent's first exposure to the TB pathogen, Mycobacterium tuberculosis
– begins when the inhaled bacilli implant in the alveoli
– bacilli mul8ply over a 3-‐ to 4-‐week period
– causes an inflammatory reac8on that is similar to any acute pneumonia
Primary Tuberculosis
• Progression – pulmonary capillaries dilate, the inters88um fills with fluid, the alveolar epithelium to swells from the edema fluid and alveoli become consolidated
– this phase of TB coincides with a posi8ve tuberculin reac8on—a posi8ve purified protein deriva8ve (PPD) skin test result
Primary Tuberculosis
• Early Infec8on – the lung 8ssue that surrounds the infected area produces a protec8ve cell wall called a tubercle
– this encapsulates the TB bacilli
– lesions may be seen as small, sharply defined opaci8es on radiograph

RSPT 2310 Tuberculosis
2
Primary Tuberculosis
• Later Phase – tubercles consists of a central core containing TB bacilli
– core has enlarged macrophages with an outer wall composed of fibroblasts, lymphocytes, and neutrophils
– tubercles take about 2 to 10 weeks to form • func8on of the tubercle is to contain the TB bacilli, thus preven8ng the further spread of infec8ous TB organisms
– central core of the tubercle has the poten8al to break down, especially in pa8ents with a depressed immune system
Primary Tuberculosis
• Later Phase – when this happens, the
center of the tubercle fills with necro8c 8ssue that resembles dry coTage cheese
– the tubercle is called a caseous lesion or caseous granuloma
– pa8ents are poten8ally contagious at this stage
• in most cases, however, the TB bacilli are effec8vely contained within the tubercles
Primary Tuberculosis
• Later Phase – once the bacilli are controlled—either by the pa8ent's immunologic defense system or by an8tuberculous drugs—the healing process begins
– 8ssue fibrosis and calcifica8on of the lung parenchyma slowly replace the tubercle, causing lung 8ssue retrac8on and scarring
– in some cases the calcifica8on and fibrosis cause the bronchi to distort and dilate—that is, to develop bronchiectasis
Primary Tuberculosis
• Later Phase – when the bacilli are isolated within tubercles and immunity develops, the TB bacilli may remain dormant for months, years, or life
– individuals with dormant TB (AKA latent TB) do not feel sick or have any TB-‐related symptoms
– they are s8ll infected with TB but do not have clinically ac8ve TB
Primary Tuberculosis
• Later Phase – the only indica8on of a TB infec8on is a posi8ve reac8on to the tuberculin skin test, or TB blood test, and the finding of possible residual scarring on the chest radiograph
– individuals with dormant TB are not infec8ous and cannot spread the TB bacilli to others
Post-‐primary Tuberculosis
• Post-‐primary TB – AKA reac8va8on TB, re-‐infec8on TB, or secondary TB – describes the reac8va8on of TB months or even years aVer the ini8al infec8on has been controlled
– most pa8ents with primary TB recover completely from a clinical standpoint, but live tubercle bacilli can remain dormant for decades
– a posi8ve tuberculin reac8on generally persists even aVer the primary infec8on stage has been controlled

RSPT 2310 Tuberculosis
3
Post-‐primary Tuberculosis
• Post-‐primary TB – TB may become reac8vated, especially in pa8ents with depressed immune systems or these risk factors • malnourished individuals • those living in ins8tu8onal housing or overcrowded condi8ons
• immunosuppressed pa8ents • human immunodeficiency virus (HIV)–infected pa8ents
• alcoholism
Post-‐primary Tuberculosis
• Post-‐primary TB – if the TB infec8on is uncontrolled, cavita8on of the caseous granuloma tubercle develops
– pa8ents progressively experience more severe symptoms • violent cough episodes • greenish or bloody sputum • low-‐grade fever • anorexia and weight loss • extreme fa8gue, night sweats
• chest pain
Post-‐primary Tuberculosis
• Post-‐Primary TB – this gradual was8ng of the
body that provided the basis for the earlier name for TB—consump(on
– pa8ents are highly contagious at this stage
– in severe cases a deep tubercle cavity may rupture and allow air and infected material to flow into the pleural space or the tracheobronchial tree
– pleural complica8ons are common in TB
Disseminated TB
• Disseminated TB – AKA extrapulmonary TB, miliary TB, and tuberculosis—disseminated
– refers to infec8on from TB bacilli that escape from a tubercle and travel to sites other throughout the body by means of the bloodstream or lympha8c system
Disseminated TB
• Disseminated TB – in general, the TB bacilli that gain entrance to the bloodstream usually gather and mul8ply in por8ons of the body that have a high 8ssue oxygen tension
– the most common loca8on is the apex of the lungs – other oxygen-‐rich areas in the body include the regional lymph nodes, kidneys, long bones, genital tract, brain, and meninges
Disseminated TB
• Disseminated TB – genital TB in males damages the prostate gland, epididymis, seminal vesicle, and testes, in females, the fallopian tubes, ovaries, and uterus
– the spine is a frequent site of TB infec8on, although the hip, knee, wrist, and elbow can also be involved
RSPT 2310 Tuberculosis
4
Disseminated TB
• Disseminated TB – tubercular meningi8s is caused by an ac8ve brain lesion seeding TB bacilli into the meninges and may cause mental deteriora8on, permanent retarda8on, blindness, and deafness
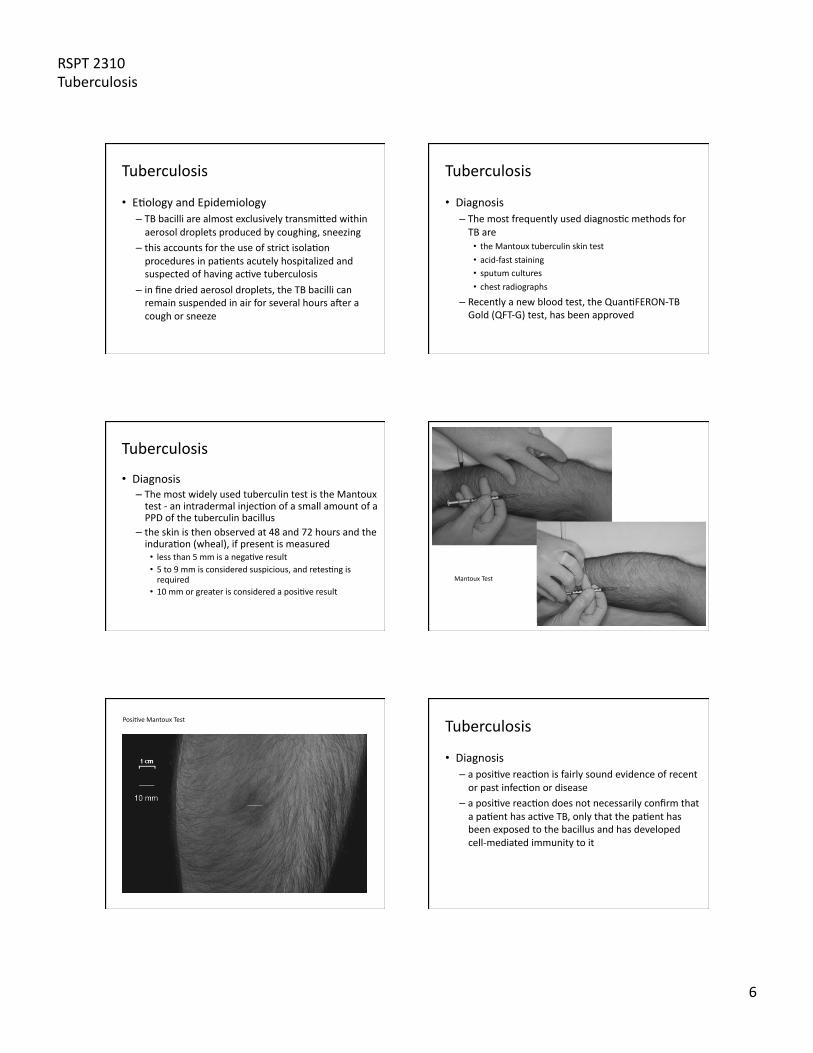
– when a large number of bacilli are freed into the bloodstream, the result can be the presence of numerous small tubercles—about the size of a pinhead—scaTered throughout the body—commonly called miliary TB
Disseminated TB
• TB is primarily a chronic restric8ve pulmonary disorder
• The major pathologic or structural changes – Alveolar consolida8on – Alveolar-‐capillary membrane destruc8on – Caseous tubercles or granulomas – Cavity forma8on – Fibrosis and secondary calcifica8on of the lung parenchyma
– Distor8on and dila8on of the bronchi – Increased bronchial secre8ons
Tuberculosis
• E8ology and Epidemiology – one of the oldest diseases known to man and remains one of the most widespread diseases in the world
– unmistakable evidence has been provided from mummies from the Stone Age, ancient Egypt, and Peru that TB is an ancient human disease
Tuberculosis
• E8ology and Epidemiology – In early wri8ngs, the disease was called “consump8on,” “Captain of the Men of Death,” and “white plague”
– in the nineteenth century, the disease was named tuberculosis, a term that derives mainly from the tubercle forma8ons found during postmortem examina8ons of vic8ms of the disease
Tuberculosis
• E8ology and Epidemiology – In 2010, a total of 11,181 tuberculosis (TB) cases were reported in the United States • 3.6 cases per 100,000 popula8on • a decline of 3.9% from 2009 • the lowest rate recorded since na8onal repor8ng began in 1953
Tuberculosis
• E8ology and Epidemiology – the number of TB cases reported annually in the United States dropped 74% between 1953 and 1985 (84,304 to 22,201)
– star8ng in 1986, however, the incidence of TB trended upward each year in the United States, with a peak of 26,673 reported cases in 1992

RSPT 2310 Tuberculosis
5
Tuberculosis
• E8ology and Epidemiology – the resurgence of TB during this period is well correlated with • increased immigra8on from endemic areas
• the sudden rise of the HIV infec8on epidemic • the increased use of immunosuppressive drugs
– from 1994 to 2010 the yearly incidence of TB again trended downward to its lowest level of 11,181
Tuberculosis
• E8ology and Epidemiology – the decline of TB in the United States is believed to be the result of • new TB medica8ons
• beTer understanding of the disease • beTer public health educa8on
Tuberculosis
• E8ology and Epidemiology – the mortality rate from TB in the United States is currently 0.6 deaths per 100,000, which represents approximately 1700 deaths per year
– in 1953 the mortality rate was 12.5 deaths per 100,000 per year
Tuberculosis
• E8ology and Epidemiology – globally, in 2010
• 8.8 million cases of TB • 1.1 million deaths from TB among HIV-‐nega8ve people
• 350,000 deaths from HIV-‐associated TB
Tuberculosis
• E8ology and Epidemiology – in humans, TB is primarily caused by M. tuberculosis
• mycobacteria are long, slender, straight or curved rods • the organism enters humans via three routes
– the respiratory tract – the gastrointes8nal tract – an open wound in the skin
– most TB infec8ons are contracted via the airborne route
Tuberculosis
• E8ology and Epidemiology – TB bacilli are highly aerobic organisms and thrive best in areas of the body with high oxygen tension(e.g. apex of the lung)
– when stained, the hard outer layer of the tubercle bacilli resists decoloriza8on by acid or alcohol(acid-‐fast bacilli)
– the hard outer coat of the tubercle bacillus also protects the organism against killing and diges8on by phagocytes and renders the bacilli more resistant to an8tuberculous drugs
RSPT 2310 Tuberculosis
6
Tuberculosis
• E8ology and Epidemiology – TB bacilli are almost exclusively transmiTed within aerosol droplets produced by coughing, sneezing
– this accounts for the use of strict isola8on procedures in pa8ents acutely hospitalized and suspected of having ac8ve tuberculosis
– in fine dried aerosol droplets, the TB bacilli can remain suspended in air for several hours aVer a cough or sneeze
Tuberculosis
• Diagnosis – The most frequently used diagnos8c methods for TB are • the Mantoux tuberculin skin test
• acid-‐fast staining • sputum cultures
• chest radiographs – Recently a new blood test, the Quan8FERON-‐TB Gold (QFT-‐G) test, has been approved
Tuberculosis
• Diagnosis – The most widely used tuberculin test is the Mantoux test -‐ an intradermal injec8on of a small amount of a PPD of the tuberculin bacillus
– the skin is then observed at 48 and 72 hours and the indura8on (wheal), if present is measured • less than 5 mm is a nega8ve result • 5 to 9 mm is considered suspicious, and retes8ng is required
• 10 mm or greater is considered a posi8ve result
Mantoux Test
Posi8ve Mantoux Test Tuberculosis
• Diagnosis – a posi8ve reac8on is fairly sound evidence of recent or past infec8on or disease
– a posi8ve reac8on does not necessarily confirm that a pa8ent has ac8ve TB, only that the pa8ent has been exposed to the bacillus and has developed cell-‐mediated immunity to it

RSPT 2310 Tuberculosis
7
Tuberculosis
• Diagnosis – Acid-‐Fast Staining
• since M. tuberculosis has an unusual, waxy coa8ng on the cell surface, which makes the cells impervious to staining, an acid-‐fast bacteria (AFB) test (also called a sputum smear) is performed instead
• several varia8ons of the acid-‐fast stain are currently in use – the frequently used Ziehl-‐Neelsen stain reveals bright red acid-‐fast bacilli against a blue background
– another popular technique involves a fluorescent acid-‐fast stain that reveals luminescent yellow-‐green bacilli against a dark background
– the fluorescent acid-‐fast stain is becoming the acid-‐fast test of choice because it is easier to read and provides a striking contrast
Tuberculosis
• Diagnosis – Sputum Culture
• used to differen8ate the different strains of mycobacterium
• cultures can also iden8fy drug-‐resistant bacilli and their sensi8vity to an8bio8c therapy
• not necessarily the diagnos8c test of choice because M. tuberculosis grows very slowly -‐ it takes up to 6 weeks for colonies to appear in culture
M. tuberculosis in culture
Tuberculosis
• Diagnosis – Quan8FERON-‐TB Gold Test
• approved by FDA in 2005, QFT-‐G is a whole-‐blood test used for diagnosing M. tuberculosis infec8on, including latent TB infec8on
– samples of the pa8ent's blood are mixed with an8gens of two M. tuberculosis proteins
– the mixture incubates for 16 to 24 hours – aVer this period the mixture is measured for the presence of interferon-‐gamma (IFN-‐gamma)
Overview of the Cardiopulmonary Clinical Manifesta8ons Associated with Tuberculosis

RSPT 2310 Tuberculosis
8
Clinical Data Obtained at the Pa8ent’s Bedside
The Physical Examination
The Physical Examination The Physical Examination
Chest Assessment Findings Increased tactile and vocal fremitus Dull percussion note Bronchial breath sounds Crackles, rhonchi, and wheezing Pleural friction rub
• if process extends to pleural surface Whispered pectoriloquy

RSPT 2310 Tuberculosis
9
Clinical Data Obtained from Laboratory Tests and Special Procedures
Pulmonary Function Test Findings Moderate and Extensive Cases (Restrictive Lung Pathophysiology)
Forced Expiratory Flow Rate Findings
Pulmonary Function Test Findings Moderate and Extensive Cases (Restrictive Lung Pathophysiology)
Lung Volume & Capacity Findings
Arterial Blood Gases Moderate Tuberculosis
Acute Alveolar Hyperventilation with Hypoxemia (Acute Respiratory Alkalosis)
pH PaCO2 HCO3 PaO2 ↑ ↓ ↓ (slightly) ↓
PaO2 and PaCO2 trends during acute alveolar hyperven8la8on.
Arterial Blood Gases Extensive Tubeculosis with Pulmonary Fibrosis
Chronic Ventilatory Failure with Hypoxemia (Compensated Respiratory Acidosis)
pH PaCO2 HCO3 PaO2 N ↑ ↑ (Slightly) ↓

RSPT 2310 Tuberculosis
10
PaO2 and PaCO2 trends during acute or chronic ven8latory failure.
Arterial Blood Gases
Acute Ventilatory Changes Superimposed On Chronic Ventilatory Failure
Oxygenation Indices Moderate to Severe Stages
QS/QT DO2 VO2 C(a-v)O2 O2ER SvO2
↑ ↓ N N ↑ ↓
Hemodynamic Indices Severe Stage
CVP RAP PA PCWP CO SV
↑ ↑ ↑ N N N
SVI CI RVSWI LVSWI PVR SVR N N ↑ N ↑ N
Abnormal Laboratory Tests and Procedures
Positive tuberculosis skin test (PPD) Positive sputum acid-fast bacillus (AFB) stain test Positive sputum culture
Radiologic Findings
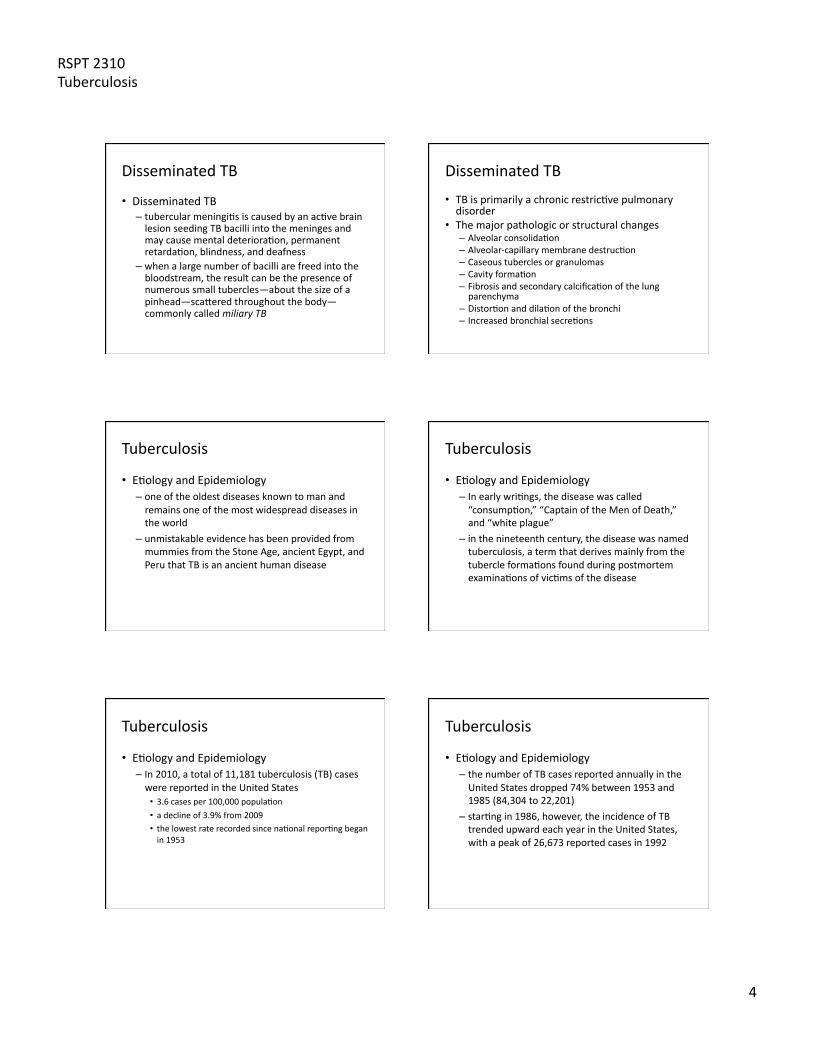
Chest Radiograph Increased opacity Ghon nodule Ghon complex Cavity formation Cavity lesion containing an air-fluid level (see Figure 16-2) Pleural effusion Calcification and fibrosis Retraction of lung segments or lobe Right ventricular enlargement
RSPT 2310 Tuberculosis
11
Figure 17-‐5. Cavitary reac8va8on tuberculosis showing a leV upper lobe cavity and localized pleural thickening. Figure 17-‐6. Miliary tuberculosis showing widespread uniformly distributed fine nodula8on of the lung.
General Management
• Pharmacologic Agents – 2-‐4 drugs for 6 to 9 months
• 6 month protocol – For the first 2 months (call the induc8on phase), the pa8ent takes a daily dose of isoniazid (INH), rifampin, pyrazinamide, and either ethambutol or streptomycin
– For the next 4 months, the pa8ent takes isoniazid and rifampin daily or twice weekly
General Management
• Pharmacologic Agents – 9 month protocol
• For the first 1 to 2 months, the pa8ent takes a daily dose of isoniazid and rifampin
• Followed by twice-‐weekly isoniazid and rifampin un8l the full 9 month period is completed
General Management
• Isoniazid (INH) and rifampin (Rifadin) – First-‐line agents prescribed for the en8re 9 months
• Isoniazid is considered to be the most effec8ve first-‐line an8tuberculosis agent
• Rifampin is bactericidal and is most commonly used with isoniazid
RC Treatment Protocols
• Oxygen Therapy Protocol
• Bronchopulmonary Hygiene Therapy Protocol
• Mechanical Ven8la8on Protocol