2017 university of utah - subsidized graduate...
TRANSCRIPT
emihealth.com
2017 University of Utah - Subsidized Graduate Students
Corporate (801)262-7475Customer Service (800)662-5851
EMIHealth.com
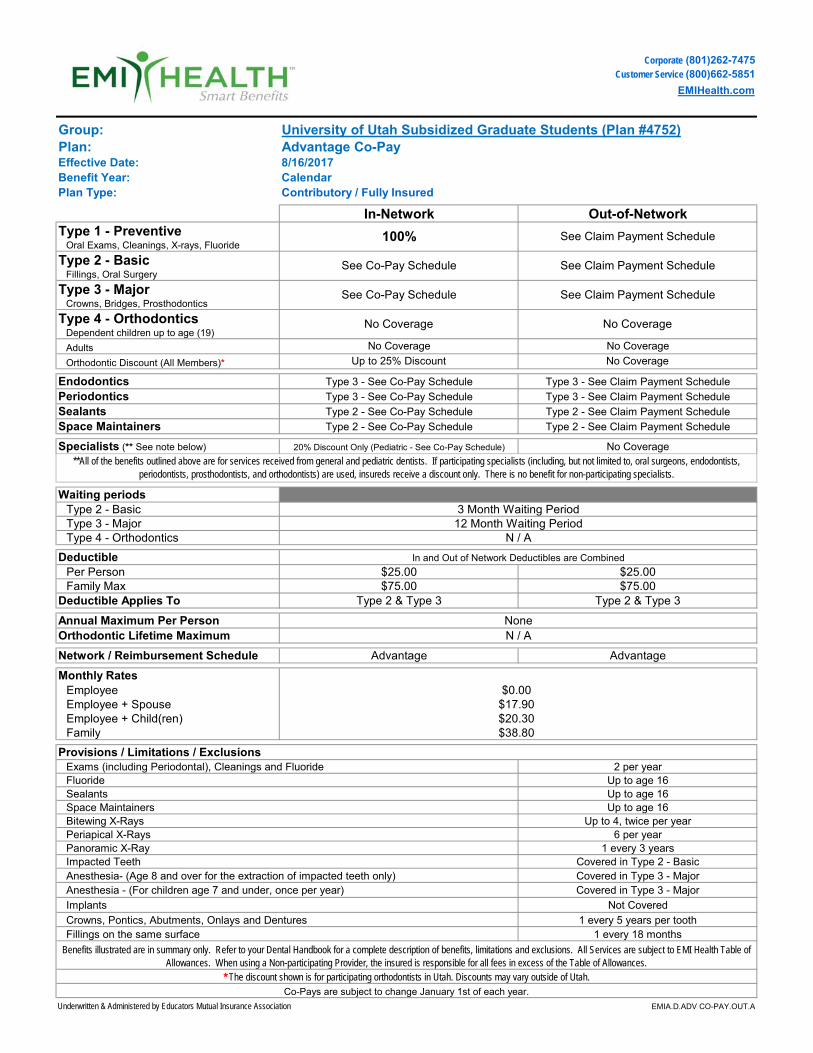
University of Utah Subsidized Graduate Students (Plan #4752)Advantage Co-Pay8/16/2017CalendarContributory / Fully Insured
Underwritten & Administered by Educators Mutual Insurance Association EMIA.D.ADV CO-PAY.OUT.A
Covered in Type 2 - BasicAnesthesia- (Age 8 and over for the extraction of impacted teeth only)
Exams (including Periodontal), Cleanings and Fluoride 2 per year
Employee + Child(ren)Family
Provisions / Limitations / Exclusions
Impacted Teeth
Implants
Sealants Up to age 16
Benefits illustrated are in summary only. Refer to your Dental Handbook for a complete description of benefits, limitations and exclusions. All Services are subject to EMI Health Table of Allowances. When using a Non-participating Provider, the insured is responsible for all fees in excess of the Table of Allowances.
$20.30
Periapical X-Rays 6 per yearPanoramic X-Ray 1 every 3 years
$38.80
Covered in Type 3 - MajorAnesthesia - (For children age 7 and under, once per year) Covered in Type 3 - Major
Not Covered
Crowns, Pontics, Abutments, Onlays and Dentures 1 every 5 years per tooth
Co-Pays are subject to change January 1st of each year.
Fillings on the same surface 1 every 18 months
* The discount shown is for participating orthodontists in Utah. Discounts may vary outside of Utah.
Plan:Group:
Bitewing X-Rays Up to 4, twice per yearSpace Maintainers Up to age 16
Fluoride Up to age 16
Benefit Year:Plan Type:
Effective Date:
No Coverage
No Coverage
See Co-Pay Schedule
See Co-Pay Schedule See Claim Payment Schedule
See Claim Payment Schedule
Out-of-Network
Type 3 - See Co-Pay Schedule
20% Discount Only (Pediatric - See Co-Pay Schedule)
N / A
$25.00Deductible
No Coverage
No Coverage
See Claim Payment ScheduleType 3 - MajorCrowns, Bridges, Prosthodontics
Type 1 - PreventiveOral Exams, Cleanings, X-rays, Fluoride
Fillings, Oral SurgeryType 2 - Basic
100%
In-Network
No CoverageType 4 - OrthodonticsDependent children up to age (19)
Adults
Space Maintainers
Type 2 - Basic
**All of the benefits outlined above are for services received from general and pediatric dentists. If participating specialists (including, but not limited to, oral surgeons, endodontists, periodontists, prosthodontists, and orthodontists) are used, insureds receive a discount only. There is no benefit for non-participating specialists.
Type 3 - Major
Periodontics
$0.00$17.90
12 Month Waiting PeriodN / A
Orthodontic Lifetime Maximum
Deductible Applies To
Per Person $25.00In and Out of Network Deductibles are Combined
Family Max
Employee + SpouseEmployee
Network / Reimbursement Schedule
Monthly Rates
Annual Maximum Per Person
Advantage
None
Advantage
Up to 25% Discount
Specialists (** See note below)
Waiting periods
Type 3 - See Claim Payment Schedule
Type 2 & Type 3
No Coverage
Sealants Type 2 - See Co-Pay Schedule
Type 3 - See Co-Pay Schedule
Orthodontic Discount (All Members)*
Endodontics
Type 2 - See Claim Payment Schedule
Type 2 - See Co-Pay Schedule
3 Month Waiting Period
Type 3 - See Claim Payment Schedule
Type 2 & Type 3$75.00$75.00
Type 2 - See Claim Payment Schedule
Type 4 - Orthodontics
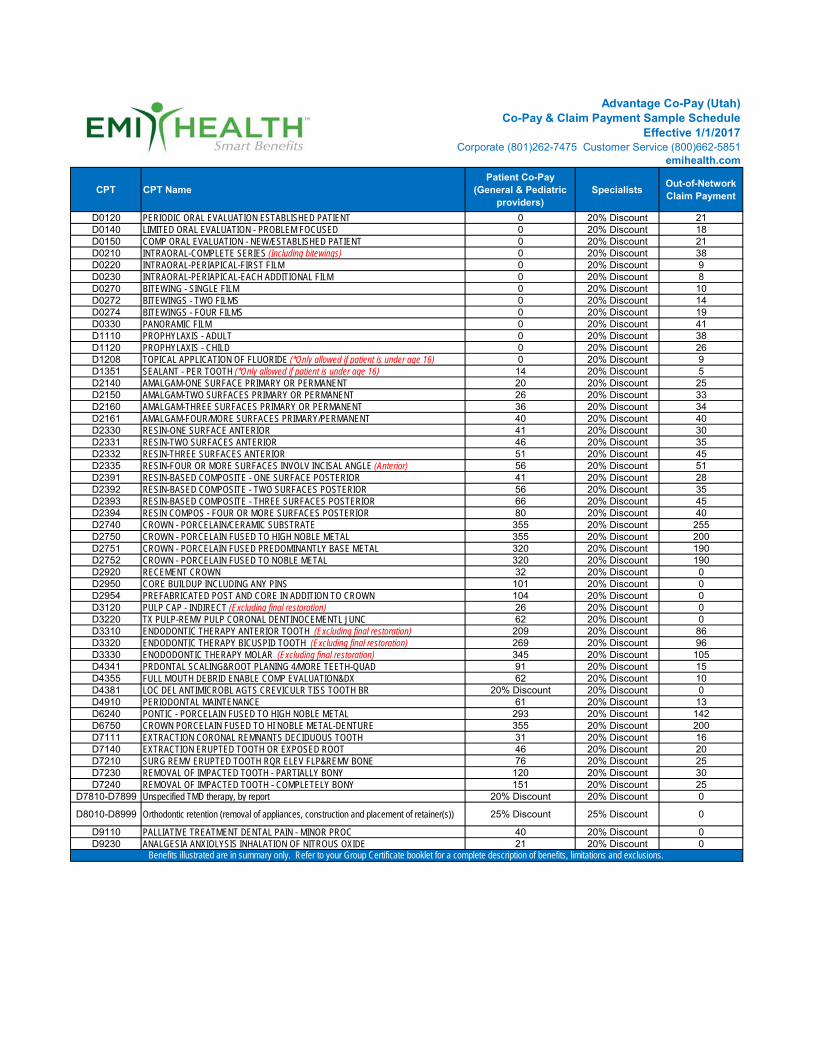
Advantage Co-Pay (Utah)Co-Pay & Claim Payment Sample Schedule
Effective 1/1/2017Corporate (801)262-7475 Customer Service (800)662-5851
emihealth.com
CPT CPT NamePatient Co-Pay
(General & Pediatric providers)
SpecialistsOut-of-Network Claim Payment
D0120 PERIODIC ORAL EVALUATION ESTABLISHED PATIENT 0 20% Discount 21D0140 LIMITED ORAL EVALUATION - PROBLEM FOCUSED 0 20% Discount 18D0150 COMP ORAL EVALUATION - NEW/ESTABLISHED PATIENT 0 20% Discount 21D0210 INTRAORAL-COMPLETE SERIES (Including bitewings) 0 20% Discount 38D0220 INTRAORAL-PERIAPICAL-FIRST FILM 0 20% Discount 9D0230 INTRAORAL-PERIAPICAL-EACH ADDITIONAL FILM 0 20% Discount 8D0270 BITEWING - SINGLE FILM 0 20% Discount 10D0272 BITEWINGS - TWO FILMS 0 20% Discount 14D0274 BITEWINGS - FOUR FILMS 0 20% Discount 19D0330 PANORAMIC FILM 0 20% Discount 41D1110 PROPHYLAXIS - ADULT 0 20% Discount 38D1120 PROPHYLAXIS - CHILD 0 20% Discount 26D1208 TOPICAL APPLICATION OF FLUORIDE (*Only allowed if patient is under age 16) 0 20% Discount 9D1351 SEALANT - PER TOOTH (*Only allowed if patient is under age 16) 14 20% Discount 5D2140 AMALGAM-ONE SURFACE PRIMARY OR PERMANENT 20 20% Discount 25D2150 AMALGAM-TWO SURFACES PRIMARY OR PERMANENT 26 20% Discount 33D2160 AMALGAM-THREE SURFACES PRIMARY OR PERMANENT 36 20% Discount 34D2161 AMALGAM-FOUR/MORE SURFACES PRIMARY/PERMANENT 40 20% Discount 40D2330 RESIN-ONE SURFACE ANTERIOR 41 20% Discount 30D2331 RESIN-TWO SURFACES ANTERIOR 46 20% Discount 35D2332 RESIN-THREE SURFACES ANTERIOR 51 20% Discount 45D2335 RESIN-FOUR OR MORE SURFACES INVOLV INCISAL ANGLE (Anterior) 56 20% Discount 51D2391 RESIN-BASED COMPOSITE - ONE SURFACE POSTERIOR 41 20% Discount 28D2392 RESIN-BASED COMPOSITE - TWO SURFACES POSTERIOR 56 20% Discount 35D2393 RESIN-BASED COMPOSITE - THREE SURFACES POSTERIOR 66 20% Discount 45D2394 RESIN COMPOS - FOUR OR MORE SURFACES POSTERIOR 80 20% Discount 40D2740 CROWN - PORCELAIN/CERAMIC SUBSTRATE 355 20% Discount 255D2750 CROWN - PORCELAIN FUSED TO HIGH NOBLE METAL 355 20% Discount 200D2751 CROWN - PORCELAIN FUSED PREDOMINANTLY BASE METAL 320 20% Discount 190D2752 CROWN - PORCELAIN FUSED TO NOBLE METAL 320 20% Discount 190D2920 RECEMENT CROWN 32 20% Discount 0D2950 CORE BUILDUP INCLUDING ANY PINS 101 20% Discount 0D2954 PREFABRICATED POST AND CORE IN ADDITION TO CROWN 104 20% Discount 0D3120 PULP CAP - INDIRECT (Excluding final restoration) 26 20% Discount 0D3220 TX PULP-REMV PULP CORONAL DENTINOCEMENTL JUNC 62 20% Discount 0D3310 ENDODONTIC THERAPY ANTERIOR TOOTH (Excluding final restoration) 209 20% Discount 86D3320 ENDODONTIC THERAPY BICUSPID TOOTH (Excluding final restoration) 269 20% Discount 96D3330 ENODODONTIC THERAPY MOLAR (Excluding final restoration) 345 20% Discount 105D4341 PRDONTAL SCALING&ROOT PLANING 4/MORE TEETH-QUAD 91 20% Discount 15D4355 FULL MOUTH DEBRID ENABLE COMP EVALUATION&DX 62 20% Discount 10D4381 LOC DEL ANTIMICROBL AGTS CREVICULR TISS TOOTH BR 20% Discount 20% Discount 0D4910 PERIODONTAL MAINTENANCE 61 20% Discount 13D6240 PONTIC - PORCELAIN FUSED TO HIGH NOBLE METAL 293 20% Discount 142D6750 CROWN PORCELAIN FUSED TO HI NOBLE METAL-DENTURE 355 20% Discount 200D7111 EXTRACTION CORONAL REMNANTS DECIDUOUS TOOTH 31 20% Discount 16D7140 EXTRACTION ERUPTED TOOTH OR EXPOSED ROOT 46 20% Discount 20D7210 SURG REMV ERUPTED TOOTH RQR ELEV FLP&REMV BONE 76 20% Discount 25D7230 REMOVAL OF IMPACTED TOOTH - PARTIALLY BONY 120 20% Discount 30D7240 REMOVAL OF IMPACTED TOOTH - COMPLETELY BONY 151 20% Discount 25
D7810-D7899 Unspecified TMD therapy, by report 20% Discount 20% Discount 0
D8010-D8999 Orthodontic retention (removal of appliances, construction and placement of retainer(s)) 25% Discount 25% Discount 0
D9110 PALLIATIVE TREATMENT DENTAL PAIN - MINOR PROC 40 20% Discount 0D9230 ANALGESIA ANXIOLYSIS INHALATION OF NITROUS OXIDE 21 20% Discount 0
Benefits illustrated are in summary only. Refer to your Group Certificate booklet for a complete description of benefits, limitations and exclusions.
Corporate (801)262-7475Customer Service (800)662-5851
EMIHealth.com
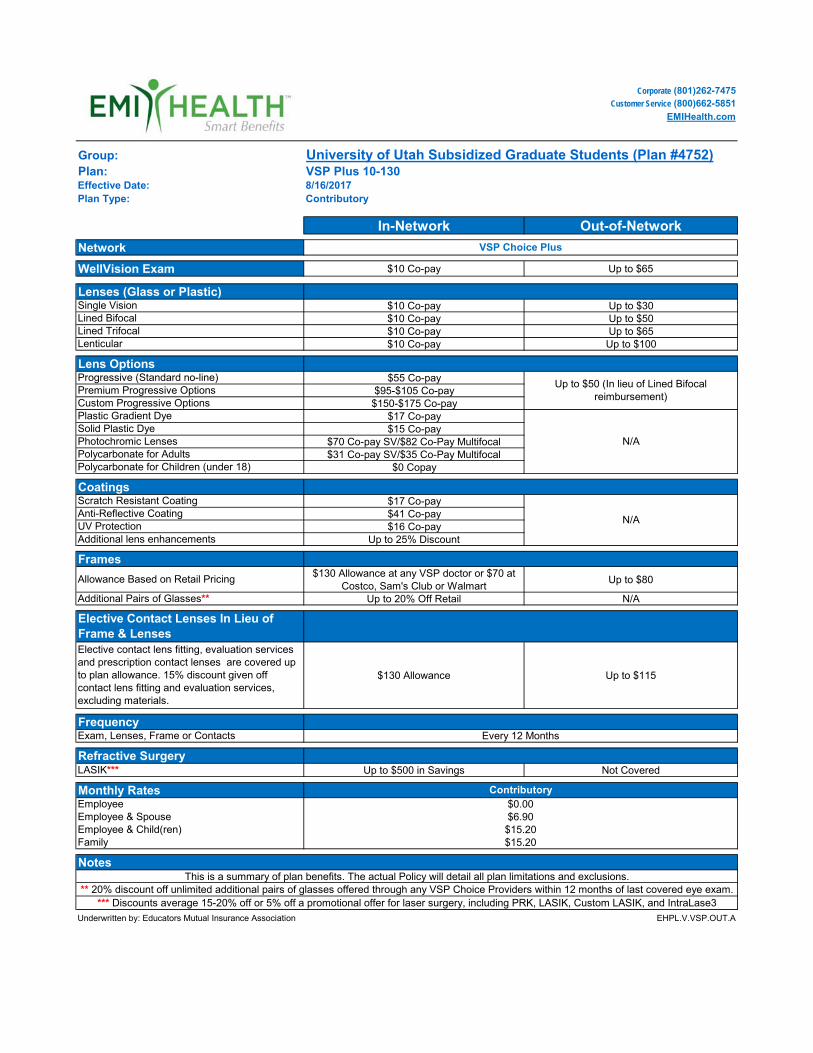
Group: University of Utah Subsidized Graduate Students (Plan #4752)Plan: VSP Plus 10-130
8/16/2017Plan Type: Contributory
In-Network Out-of-Network
$10 Co-pay Up to $65
$10 Co-pay Up to $30$10 Co-pay Up to $50$10 Co-pay Up to $65$10 Co-pay Up to $100
$55 Co-pay$95-$105 Co-pay$150-$175 Co-pay
$17 Co-pay$15 Co-pay
$70 Co-pay SV/$82 Co-Pay Multifocal$31 Co-pay SV/$35 Co-Pay Multifocal
$0 Copay
$17 Co-pay$41 Co-pay$16 Co-pay
Up to 25% Discount
$130 Allowance at any VSP doctor or $70 at Costco, Sam's Club or Walmart
Up to $80
Up to 20% Off Retail N/A
$130 Allowance Up to $115
Up to $500 in Savings Not Covered
Underwritten by: Educators Mutual Insurance Association EHPL.V.VSP.OUT.A
Contributory$0.00$6.90 $15.20 $15.20
Up to $50 (In lieu of Lined Bifocal reimbursement)
Effective Date:
Progressive (Standard no-line)
Network VSP Choice Plus
WellVision Exam
Lenses (Glass or Plastic)Single VisionLined Bifocal Lined Trifocal
Lens Options
Premium Progressive OptionsCustom Progressive OptionsPlastic Gradient DyeSolid Plastic DyePhotochromic LensesPolycarbonate for Adults
N/A
Polycarbonate for Children (under 18)
Exam, Lenses, Frame or Contacts Every 12 Months
CoatingsScratch Resistant Coating
N/AAnti-Reflective CoatingUV ProtectionAdditional lens enhancements
Additional Pairs of Glasses**
Elective Contact Lenses In Lieu of Frame & LensesElective contact lens fitting, evaluation services and prescription contact lenses are covered up to plan allowance. 15% discount given off contact lens fitting and evaluation services, excluding materials.
Frequency
Lenticular
NotesThis is a summary of plan benefits. The actual Policy will detail all plan limitations and exclusions.
** 20% discount off unlimited additional pairs of glasses offered through any VSP Choice Providers within 12 months of last covered eye exam.*** Discounts average 15-20% off or 5% off a promotional offer for laser surgery, including PRK, LASIK, Custom LASIK, and IntraLase3
LASIK***
Monthly RatesEmployeeEmployee & Spouse Employee & Child(ren)Family
Refractive Surgery
Frames
Allowance Based on Retail Pricing
Detach Cards Here
MR TEST 100 S ROOSEVELT ST MURRAY, UT 84107
Dear Insured:
Welcome to EMI Health. We are pleased to provide you with your new identification cards. Please present this card to your provider each time you receive services.
Providers may use either your social security number or the member ID number on your card when submitting claims. All correspondence from EMI Health, including your Explanations of Benefits (EOBs), will reference your social security number.
If you have any questions or concerns, or if you have terminated your employment, please call the EMI Health Enrollment Department at (801) 262-7475 within the Salt Lake area, or toll free at (800) 662-5851 in other areas of Utah.
Sincerely,
EMI Health
000222XXEMIHFI
EMI.M
KTG.
OE-S
IGNU
P.011
7.013
2
852 EAST ARROWHEAD LANE, MURRAY, UTAH 84107TOLL FREE 800 662 5850 CORPORATE 801 262 7476 FAX 801 270 3016
emihealth.com
Sign Up For Your My EMI Health Account Today
We are pleased to offer My EMI Health, an online services system for viewing benefit, eligibility, and claims information. Getting started with My EMI Health is easy and only takes a few minutes.
1. Go to www.emihealth.com. 2. Click on the green login button, and select My EMI Health. 3. Click on "Register Now" under "Not Registered Yet." 4. Select "Member" as the type of account. 5. Enter the information requested to identify yourself, and click "Continue."
Please note:
• You will need the Member ID number found on your EMI Health identification card.
• For your security, the password must be at least six characters, including a special character.
That's all there is to it. You can then log in to My EMI Health to manage your medical, dental, and vision plans:
• View benefit descriptions • Access the Smart Cost Calculator • Check claims status • Review eligibility/enrollment status • Order ID cards • Manage prescription benefits • View EOBs
8:00 am to 6:00 pm MST Monday through FridayCustomer Service and Benefit Inquires call(Local)(801)262-7475(Toll Free)(800)662-5851(Fax)(801)269-9734
Customer Service
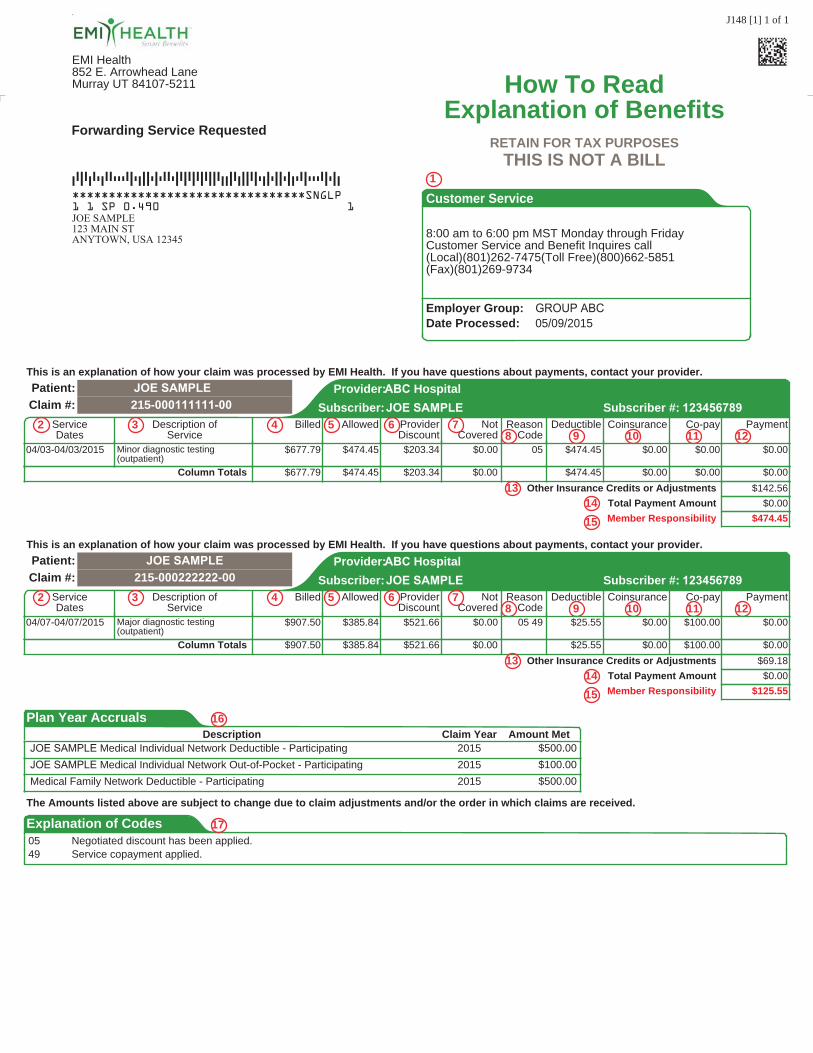
How To ReadExplanation of Benefits
RETAIN FOR TAX PURPOSESTHIS IS NOT A BILL
Employer Group: GROUP ABC Date Processed: 05/09/2015
1
ABC Hospital
ServiceDates
PaymentSubscriber:
NotCovered
DeductibleReasonCode
Billed Co-pay
Patient: JOE SAMPLEClaim #:
Provider:
AllowedJOE SAMPLE
Coinsurance
215-000111111-00 Subscriber #: 123456789Description of
Service
This is an explanation of how your claim was processed by EMI Health. If you have questions about payments, contact your provider.
ProviderDiscount
2 3 4 5 78 9 10 11 12
6
04/03-04/03/2015 $677.79 $0.00 05 $474.45 $0.00$0.00$474.45 $0.00Minor diagnostic testing(outpatient)
$203.34
Column Totals
Other Insurance Credits or Adjustments
Total Payment Amount
Member Responsibility
$0.00$677.79 $474.45 $0.00 $474.45 $0.00 $0.00$203.34
$0.00$142.56
$474.45
1314
15
ABC Hospital
ServiceDates
PaymentSubscriber:
NotCovered
DeductibleReasonCode
Billed Co-pay
Patient:
Claim #:Provider:
AllowedJOE SAMPLE
Coinsurance
JOE SAMPLE 215-000222222-00 Subscriber #: 123456789
Description ofService
This is an explanation of how your claim was processed by EMI Health. If you have questions about payments, contact your provider.
ProviderDiscount
2 3 4 5 78 9 10 11 12
6
04/07-04/07/2015 $907.50 $0.00 05 49 $25.55 $0.00$100.00$385.84 $0.00Major diagnostic testing(outpatient)
$521.66
Column Totals
Other Insurance Credits or Adjustments
Total Payment Amount
Member Responsibility
$0.00$907.50 $385.84 $0.00 $25.55 $0.00 $100.00$521.66
$0.00$69.18
$125.55
1314
15
Plan Year AccrualsClaim Year Amount MetDescription
16
JOE SAMPLE Medical Individual Network Deductible - Participating 2015 $500.00JOE SAMPLE Medical Individual Network Out-of-Pocket - Participating 2015 $100.00Medical Family Network Deductible - Participating 2015 $500.00
The Amounts listed above are subject to change due to claim adjustments and/or the order in which claims are received.
Explanation of Codes 17
05 Negotiated discount has been applied.49 Service copayment applied.
EMI Health852 E. Arrowhead LaneMurray UT 84107-5211
J148 [1] 1 of 1
Forwarding Service Requested
********************************SNGLP
DAFADATDAATTTAFTDFFTFTAATFAFAFAFAFFADDFADFFAFTDFTFFTFDTAFTTTAFTFD
1 1 SP 0.490JOE SAMPLE123 MAIN STANYTOWN, USA 12345
1
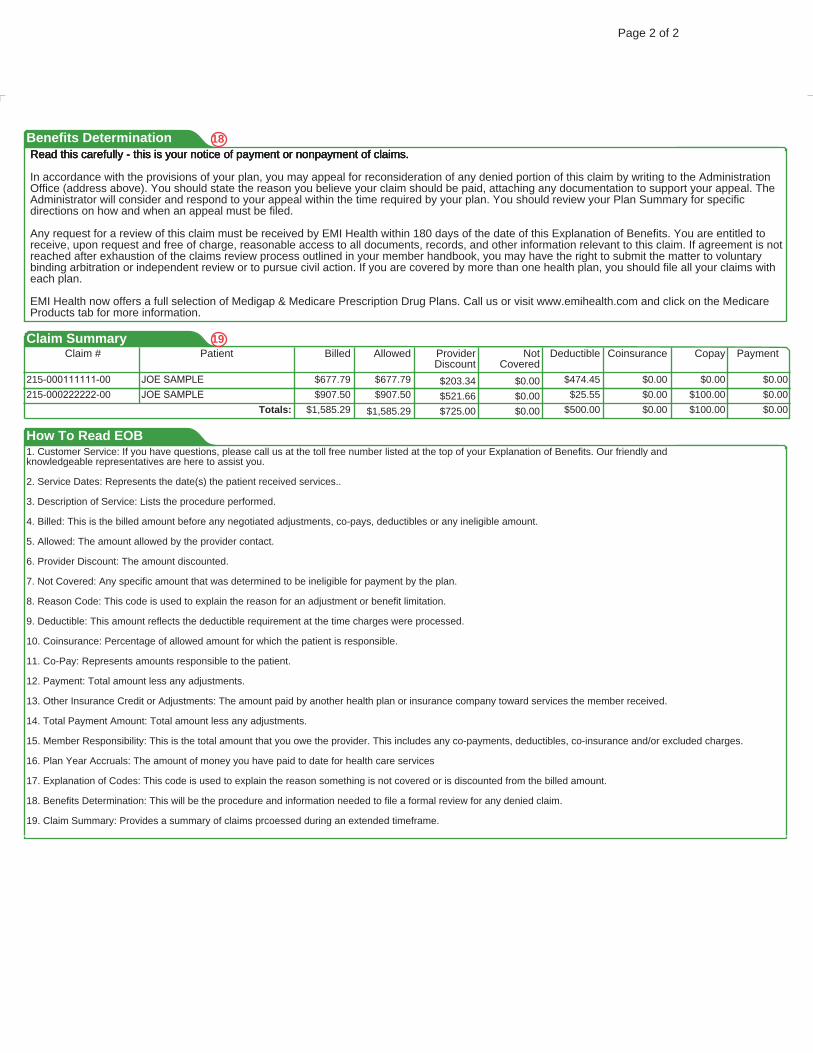
Page 2 of 2
Benefits Determination 18Read this carefully - this is your notice of payment or nonpayment of claims.Read this carefully - this is your notice of payment or nonpayment of claims.Read this carefully - this is your notice of payment or nonpayment of claims.Read this carefully - this is your notice of payment or nonpayment of claims.
In accordance with the provisions of your plan, you may appeal for reconsideration of any denied portion of this claim by writing to the AdministrationOffice (address above). You should state the reason you believe your claim should be paid, attaching any documentation to support your appeal. TheAdministrator will consider and respond to your appeal within the time required by your plan. You should review your Plan Summary for specificdirections on how and when an appeal must be filed.
Any request for a review of this claim must be received by EMI Health within 180 days of the date of this Explanation of Benefits. You are entitled toreceive, upon request and free of charge, reasonable access to all documents, records, and other information relevant to this claim. If agreement is notreached after exhaustion of the claims review process outlined in your member handbook, you may have the right to submit the matter to voluntarybinding arbitration or independent review or to pursue civil action. If you are covered by more than one health plan, you should file all your claims witheach plan.
EMI Health now offers a full selection of Medigap & Medicare Prescription Drug Plans. Call us or visit www.emihealth.com and click on the MedicareProducts tab for more information.
Claim #Claim Summary
Patient Allowed NotCovered
Copay PaymentCoinsuranceBilled DeductibleProviderDiscount
19
$677.79 $677.79 $0.00 $0.00$0.00$474.45215-000111111-00 JOE SAMPLE $0.00$203.34$907.50 $907.50 $0.00 $100.00$0.00$25.55215-000222222-00 JOE SAMPLE $0.00$521.66
$0.00Totals: $1,585.29 $0.00 $100.00$0.00$500.00$1,585.29 $725.00
How To Read EOB1. Customer Service: If you have questions, please call us at the toll free number listed at the top of your Explanation of Benefits. Our friendly andknowledgeable representatives are here to assist you.
2. Service Dates: Represents the date(s) the patient received services..
3. Description of Service: Lists the procedure performed.
4. Billed: This is the billed amount before any negotiated adjustments, co-pays, deductibles or any ineligible amount.
5. Allowed: The amount allowed by the provider contact.
6. Provider Discount: The amount discounted.
7. Not Covered: Any specific amount that was determined to be ineligible for payment by the plan.
8. Reason Code: This code is used to explain the reason for an adjustment or benefit limitation.
9. Deductible: This amount reflects the deductible requirement at the time charges were processed.
10. Coinsurance: Percentage of allowed amount for which the patient is responsible.
11. Co-Pay: Represents amounts responsible to the patient.
12. Payment: Total amount less any adjustments.
13. Other Insurance Credit or Adjustments: The amount paid by another health plan or insurance company toward services the member received.
14. Total Payment Amount: Total amount less any adjustments.
15. Member Responsibility: This is the total amount that you owe the provider. This includes any co-payments, deductibles, co-insurance and/or excluded charges.
16. Plan Year Accruals: The amount of money you have paid to date for health care services
17. Explanation of Codes: This code is used to explain the reason something is not covered or is discounted from the billed amount.
18. Benefits Determination: This will be the procedure and information needed to file a formal review for any denied claim.
19. Claim Summary: Provides a summary of claims prcoessed during an extended timeframe.
EMI.M
KTG.
OE-F
INDP
ROV.1
014.0
133
852 EAST ARROWHEAD LANE, MURRAY, UTAH 84107TOLL FREE 800 662 5850 CORPORATE 801 262 7476 FAX 801 270 3016
emihealth.com
Finding Participating Providers
Using participating providers is an important part of ensuring that you make the most of your health plan benefits. You can confirm that your provider is part of the EMI Health network, or locate a new participating provider, online at emihealth.com:
1. Click on the "Provider Search" link on the upper right-hand side of the page.
2. Select the type of network (medical, dental, or vision).
3. Select your plan (as identified on your ID card) and your state.
4. To narrow your search, select one or more of the additional criteria listed.
5. Click "Search."
Not all plans have participating provider benefits outside of your state of residence. To confirm your benefits, or if you have any questions, please contact EMI Health's customer service department toll free at 800.662.5851.
Manage your EMI Health plans on the go!
With the EMI Health mobile app, you have secure access to your important health plan information on your smart phone or tablet:
wView or email your ID card
wView your plan documents and benefit summaries
wSearch for participating medical, dental, and vision providers
The free EMI Health mobile app is available now from the Apple App Store and the Google Play store. Download the app and log in using your My EMI Health username and password. If you haven't registered your account yet, you can do so in the app or online at www.emihealth.com.
852 EAST ARROWHEAD LANE, MURRAY, UTAH 84107TOLL FREE 800 662 5850 CORPORATE 801 262 7476 FAX 801 270 3016
emihealth.com
EMI.M
KTG
.MO
BILE
APP
.121
6.01
43
[Grab your reader’s attention with a great quote from the document or use this space to emphasize a
key point. To place this text box anywhere on the page, just drag it.]
[Grab your reader’s attention with a great quote from the document or use this space to emphasize a
key point. To place this text box anywhere on the page, just drag it.]
VSP Vision Easy to Use Benefits!
No claim forms or paperwork for your members
Members simply choose a VSP provider and provide their EMI ID number and VSP does the rest
Choice Plus Network (Plans include Exams & Hardware)
VSP Choice Network Costco Wal-Mart Sam’s Club ShopKo Visionworks Eye Masters
Member
contacts VSP
provider
Member
receives careProvider bills
VSP
TM
emihealth.com