2017 hbch company members - houstonbch.org · • ondemand client website • healthy worksite...
TRANSCRIPT

2017 HBCH Company Members

The leading resource for Houston employers dedicated to providing health care at a sustainable costwhile improving the quality and
experience in their delivery

Social Media• LinkedIn
– Search Houston Business Coalition on Health; Request to join group; Approval in 1 day
– Benefits: HBCH info, relevant news and articles input & output, upcoming events
• Twitter– Find at @Houston_bch– Articles & links in healthcare and benefits– Local and national info– HBCH news, events

Thanks Sponsors
National Alliance logoReal Appeal logo

Agenda
• 8:30-8:40 Welcome & Introductions• 8:40-9:15 Obesity as a Disease – Impact & Implications• 9:15-9:30 A Physician's Perspective• 9:30-9:50 A Health Plan’s Perspective• 9:50-10:05 Break• 10:05-10:25 A Need to Improve ICD-10 Coding• 10:25-11:00 Provider Panel Discussion• 11:00-11:30 Employer Panel Q&A• 11:30-11:50 Houston NDPP Update

Collective Influence
• eValue8 Health Plan Benchmarking• Leapfrog Group Health System Benchmarking• Specialty Pharmacy SWAT• Houston Employer NDPP


Obesity as a Disease vs. a Condition: Employer Impact and ImplicationsBRUCE SHERMAN, MD
CHIEF MEDICAL OFFICER
NATIONAL ALL IANCE OF HEALTHCARE PURCHASER COALIT IONS

Obesity trends among US adults

Obesity-related comorbidities
Nearly 21% of healthcare costs are spent on obesity-related conditions

- - - - with diabetes______ without diabetes
Annual healthcare costs by BMI and diabetes
Cawley J, et al. Pharmacoeconomics 2015

Condition-related medical cost drivers – actual client data
• Enrolled population >71,000 individuals• How well does this report capture obesity-related healthcare costs???
Clinical Condition
Client Incurred Jan. 2017 - Dec. 2017; paid thru Mar. 2018

• Obese employees have twice the number of WC claims than non-obese• WC component costs are higher for obese individuals – and increase with higher BMI
OSTBYE T, ET AL. OBESITY AND WORKERS COMPENSATION COSTS. ARCH INT MED, 2007. 6
Obesity adds to Workers Compensation costsD
olla
rs p
er c
laim
Lost workdays per claim
6000
5000
4000
3000
2000
1000
0
12
10
8
6
4
2
0<18.5 18.5-24.9 25-25.9 30-34.9 35-39.9 ≥40
Indemnity claims costsMedical claims costsLost workdays

7
Obesity – employer total cost analysis
Henke RM, et al. J Occ Environ Med, 2010.

Employer costs of obesity include more than healthcare
• Workplace accommodations for overweight/obese individuals• Hiring concerns related to physical work capabilities• Turnover issues for individuals in physically demanding jobs
8

Recognition will likely help support:• reimbursement for anti-obesity treatment• implementation of weight loss strategies• efforts to reduce risk of CV disease, diabetes and other obesity-associated comorbidities

Smoking vs. obesity – an intriguing comparisonSmoking Obesity
Behavior or disease? Behavior – with addiction potential Behavior – with addiction potential
Stress as a mediator Potentially significant Potentially significant
Social component Yes Yes
Associated medical complications
Yes Yes
Manufacturer’s role Significant contributor Significant contributor
Physician’s role Guidance – resource and pharmacotherapy support
Guidance – resource and pharmacotherapy support
Employer’s role Benefits offerings / workplace considerations
Benefits offerings / workplaceconsiderations
Community role Significant Opportunities exist

11
Employer benefits approach to obesity
As BMI increases so does the eligibility for intervention methods1,2
1. American Gastroenterological Association. 2002; 2. Wadden and Stunkard, eds. 2012.
BMI Category 18.5–24.9 25–29.9 30–34.9 35-39.9 > 40
Disease Risk Low Increased High High Very High Very High Extremely High
Nutrition Counseling ● ● ● ● ● ● ●Ensure Appropriate Physical Activity ● ● ● ● ● ● ●BehavioralWeight Management ● ● ● ● ● ●Medication ● ● ● ● ●Surgery ● ●

12
Most employers feel that current obesity management practices haven’t been particularly effective…
Employer perceptions of the overall effectiveness of their obesity management strategy
0%
10%
20%
30%
40%
50%
1 2 3 4 5 6 7 8
1 2 3 4 5 6 7 8
Not at all effective
Somewhateffective
Extremelyeffective
Don’t know
Source: ACTION Study, 2017

Source: ACTION Study, 2017 13
…and employees seem to feel the same way

14
Weight management is a community issue –needing a community-level focus

What can employers do?
15
The main points of leverage for employer impact:◦ Implement supportive benefit designs that encourage healthy
behaviors – and address well-being priorities◦ Promote a culture of health at work ◦ Provide workplace environment support for healthy lifestyles◦ Support community and family connections

Summary• Is obesity a disease or a condition? The debate continues…
• Irrespective of categorization, the health impact is significant
• Employers can derive benefit by providing meaningful resource support for weight management
• This is not an individual problem – it a major societal concern

ResourcesCenters for Disease Control and Prevention: www.cdc.gov/obesity/index.html
American Heart Association: Resources for Success www.heart.org
State of Obesity-Texas (RWJF): https://stateofobesity.org/states/tx
Novo Nordisk: www.novonordiskworks.com
Obesity Action Coalition: www.obesityaction.org

ByGary J. Sheppard, M.D.
Houston Academy of MedicineVice President

There is no single or simple solution to the obesity epidemic. It’s a complex problem and there has to be a multifaceted approach. Policy makers, state and local organizations, business and community leaders, school, childcare and healthcare professionals, and individuals must work together to create an environment that supports a healthy lifestyle.

Corpulence is not only a disease itself, but a harbinger of others Hippocrates 400 BC

DefinitionsObesity: Body Mass Index (BMI) of 30 or
higher.
Body Mass Index (BMI): A measure of an adult’s weight in relation to his or her height, calculated by using the adult’s weight in kilograms divided by the square of his or her height in meters.

¶ Prevalence estimates reflect BRFSS methodological changes started in 2011. These estimates should not be compared to prevalence estimates before 2011.
*Sample size <50 or the relative standard error (dividing the standard error by the prevalence) ≥ 30%.

Summary No state had a prevalence of obesity less than 20%. 3 states and the District of Columbia had a prevalence of
obesity between 20% and <25%. 22 states and Guam had a prevalence of obesity between
25% and <30%. 20 states, Puerto Rico, and Virgin Islands had a
prevalence of obesity between 30% and <35%. 5 states (Alabama, Arkansas, Louisiana, Mississippi, and
West Virginia) had a prevalence of obesity of 35% or greater.
¶ Prevalence estimates reflect BRFSS methodological changes started in 2011. These estimates should not be compared to prevalence estimates before 2011.
http://www.cdc.gov/obesity/data/prevalence-maps.html



What do they need? Peer support- Weight Watchers, TOPS
Convenient food choices- Jenny Craig, NutriSystem
Low-calorie, limited food options- Meal replacement (OPTIFAST, HMR, Medifast, Robard)

Treatments BMI25-26.9
BMI27-29.9
BMI 30-34.9
BMI35-39.9
BMI40+
Diet, PA, & Behavioral Therapy
WithCo-
morbidities
WithCo-morbidities
+ + +
Pharmacotherapy WithCo-morbidities
+ + +
Weight Loss Surgery With
Co-morbidities
WithCo-
morbidities
Consider pharmacotherapy only if a patient has not lost 1 pound per week after 6 months of combined lifestyle therapy.
The + represents the use of indicated treatment regardless of co-morbidities.

Listen to patient cues about hunger, satiety, and side effects to drive weight management.
Continue to encourage healthy lifestyle behaviors as weight loss medications should serve an adjunct to these.
If a patient has a superior response to medication (5-10% of total body weight loss), continue medications indefinitely.
Advise women of childbearing age about discontinuing medication prior to conception.

Just because we have an ICD-10 code, obesity treatment hasn’t been made easier.
Decrease in obesity can prevent or enhance treatment of other serious cardiovascular, metabolic and musculoskeletal conditions.
Management of obesity is a multi-factorial, chronic, individualized treatment.
Surgery is not the answer for all patients, but can be beneficial in some patients.
Insurance coverage for nutrition consultation, medications, weight programs and surgery is needed.
Always think Team Approach for obesity therapy.

A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
A Health Plan’s Perspective onObesity Challenges & OpportunitiesJUNE 12, 2018 ROBERT MORROW, MD, MBA
MARKET PRESIDENT, HOUSTON AND SOUTHEAST TEXAS
@DrBobMorrow

1 Centers for Medicare and Medicaid Services Office of the Actuary, September 2013 2 Centers for Disease Control and Prevention, 20053 2012: 17th Annual Towers Watson/National Business Group on Health Employer Survey on Purchasing Value in Health Care 4 Institute of Medicine, September 2012
Health care spending inthe United States now tops$2.9 trillion annually1
1 in 2 Americanslives with a chronic condition that is largely preventable2
Chronic conditions account for3 out of 4 U.S. dollars spent
on health care3
In one study, more than 60% of patients said they had no idea about the cost of their care until they received a bill4
2THE STATISTICS ARE DRAMATIC
@DrBobMorrow

Top 5 Most Expensive Chronic Conditions
Health Conditions
Oncology
Musculoskeletal
HeartRespiratory
Diabetes
@DrBobMorrow

Challenges• Workplace environments can pose challenges.• Weight is a private and sensitive matter, which
can make outreach difficult. • Lack of obesity awareness and education can
hinder engagement levels. • Weight loss is challenging to accomplish which
requires long-term coaching and engagement. • Few physicians formally diagnose obesity through
CPT codes. • Chronic health conditions receive a greater
emphasis than obesity prevention.
4
@DrBobMorrow

OpportunitiesProactive:• Health Risk Assessments• Biometric screenings• Wellness coaching• Incentives / Disincentives• Onsite clinical nurse• Workplace assessment
Reactive:• Weight loss programs• Bariatric surgery
5
@DrBobMorrow

A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
Identifying Members Through Claims

Identify Current Member Activity using real time referrals initiated by:
• Emergency room visits• Preauthorization/notification• Self referral• Provider referrals• Human Resources staff• Pharmacy Data• 24/7 Nurseline
Proactive Identification of Members
< < < Supported by Clinical Intelligence Rules > > >
CollectClaim History with Predictive Modeling
Historical claims data is included in a scheduled predictive modeling run
1 2Member Stratification
Complex Catastrophic Care
High-Risk MultipleDiseases
Moderate-Risk
Low-Risk
Well Members
3
@DrBobMorrow

ALL GAPS MATTER – Just some of the hundreds of gaps
• Lack of immunizations, mammograms, cervical screenings, colonoscopies
• No emergency action plan in place for asthma, or condition-specific screenings done
• Member not following physician's treatment plan
• Physical inactivity / poor nutrition / BMI>=25
• Tobacco use• Abnormal cholesterol
• Positive depression screen• Inadequate financial, family
or other resources• Cultural or religious barriers
• Member does not understand need to track blood pressure readings or how to read
• Member does not know how to use peak flow meter
• No beta blocker use with Coronary Artery Disease diagnosis
• Asthmatic not on controller meds • Diabetic not taking diabetic meds
Preventive Gaps Lifestyle Gaps Condition-Specific Gaps
Psychosocial Gaps Knowledge Gaps Medication Compliance
► ► ►
►► ►

A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
Proactive Approaches for Employers

What is the most clinically and financially effective way to
manage an illness?
@DrBobMorrow
To prevent it!!

A Suite of Wellness OptionsENGAGING EVERYONE• Blue PointsSM
• ondemand client website• Healthy Worksite consultation*• Personalized member communications**• Fitness device integration
11
*Buy-up dependent **Available with BCC EnhancedSM
Blue Points Program Rules are subject to change without prior notice. See the Program Rules on the Well onTarget Member Wellness Portal at wellontarget.com for further information
CLIENT REPORTING• Weekly utilization reporting• Aggregate and member-level reporting
ASSESSING HEALTH• Health Assessment• Personal Wellness Report• Biometric screenings* • One-on-one coaching
WORKSITE WELLNESS• Events and seminars*• Health fairs*• Monthly Challenge competitions**• Wellness coordinators*
WELLNESS COACHING• Dedicated coaching• Goal-setting tools• Online and telephonic support
MEMBER WEB PORTAL• Well onTarget portal• AlwaysOn® mobile app• Self-directed courses• Trackers• Health articles• Interactive Symptom Checker• Fitness Program• Social networking• Text messaging

A Division of Health Care Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association
Solving for Obesity in the Workplace

The Mug Experiment
Source: Kahneman, Thinking Fast and Slow, 2011
Class AGiven a coffee mug at the beginning of class, and then at the end of class, offered to switch mug for a bar of Swiss chocolate.
Class BGiven a bar of Swisschocolate at the beginning of class,and then at the endof class, offered toswitch for the mug.
Class COffered the choice between a coffee mug and a bar of Swiss chocolate at the beginning of class.
@DrBobMorrow
89%Chose Coffee Mug
10%Chose Coffee Mug
59%Chose Coffee Mug

Incentive Research
• People feel loss twice as much as they feel gain.
• Reframing a question in terms of a loss instead of a gain changes the response.
14
@DrBobMorrow

@DrBobMorrow
Incentives are necessary

Chocolate vs Radish Experiment
• The set up: a room full of recently bakedchocolate chip cookies, and a basket of radishes.
• Group A: Eat Radishes (while not eating cookies)• Group B: Eat Cookies• Try to solve an unsolvable tracing puzzle

Results
Time beforegiving up
Radishes:
Attempts beforegiving up
@DrBobMorrow
Cookies:
8 minutes
19 minutes
19 attempts
34 attemptsCookies:
Radishes:

18
Diets Don’t Work.Lifestyle Changes Do.The Science of Ego Depletion
@DrBobMorrow

Weight Loss ProgramAirline Client Results 2015-2018
8 NS Classes21,786 Participants80%+ Completion
Rate
>155,000 lbs Lost So Far9 lbs Avg 10-Week Weight Loss>10,000 participants lost more
than 5% body weight
65% Lowered Diabetes Risk
39% Metabolic Syndrome (MetS) Reversal
@DrBobMorrow

Weight Loss ProgramSuccess at a University System (2015-2017)
@DrBobMorrow
45,000+ lbsLost and counting. Participants averaged a 10 lb. weight loss at 10 weeks in the program. 60%
MetS Reversal5,000+ Participants

Real world clinical results with employers, published in two peer-reviewed journals
Metabolic Syndrome
-50.7% Type II Diabetes
Risk
-55%
Blood PressureRisk
-50%
Losing 5%+ of bodyweight
-44%
1. Evaluation of a Voluntary Work Site Weight Loss Program on Metabolic Syndrome. Conrad P. Earnest, PhD; Timothy S. Church, MPH, MD, PhD. October Issue 2015 (N=3880)
2. Evaluation of a Voluntary Work Site Weight Loss Program on Hypertension. Conrad P. Earnest, PhD; Timothy S. Church, MPH, MD, PhD. December Issue 2016 (N=5988)
Journal of Metabolic Syndrome and Related Disorders1
Journal of Occupational and Environmental Medicine2
Weight Loss Program

Quality Bariatric Surgery
All savings results, BCBSA data; BDC+ eligible facilities vs. relevant comparison group. Results based on most recent designation cycle for each specialty. Savings based on total episode cost. To learn more about Blue Distinction Centers for Specialty Care, please visit www.bcbs.com or contact your Local Plan.
1. All quality results, BCBSA data; BDC/BDC+ eligible facilities vs. relevant comparison group; results based on most recent designation cycle for each specialty.2. AHRQ-sponsored Health Cost and Utilization Project (HCUP), 2014 (reflects all privately insured).
32% lowerER visit rate
21% lowerReadmission rate
48-73% lowerSurgical site infection rate
29% savingsoverall
$4,300 savingsgastric banding
$3,200 savingsgastric sleeve
$4,900 savingsgastric roux-en-y

23
Courcoulas, JAMA Surgery 2015
Consider Covering Bariatric Surgery
@DrBobMorrow Klein, obesity | VOLUME 19 NUMBER 3 | March 2011
Total diabetes medication costs decreased significantly
among surgery patients.
Bariatric surgery with low-level lifestyle intervention resulted in more disease
remission than did lifestyle intervention alone.

24
Follow @DrBobMorrowon Twitter

25
Client Example – Annual Wellness Exam Incentive
≈30,000Eligible Members
To increase annual wellness exam compliance, this client increased participation by offering an incentive in the form of a premium reduction.
• 13.6% of Members were diagnosed with a new condition following the exam.
21,900 (73%) Members took their annual wellness
exam
15,330 (70%) of these Members did not have an annual exam 1 year prior
@DrBobMorrow
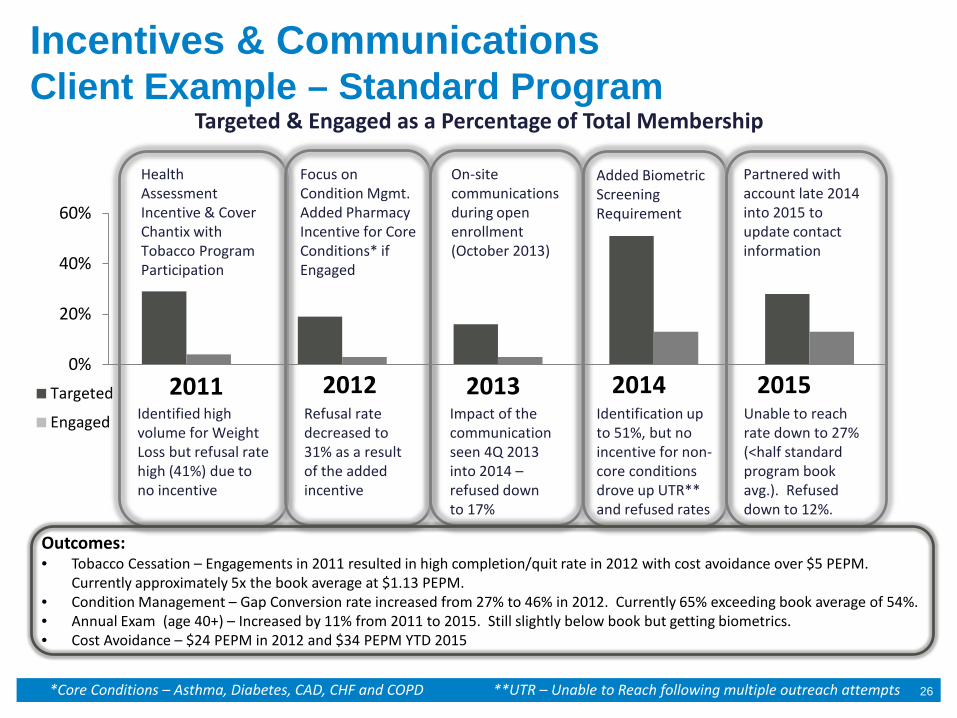
Incentives & CommunicationsClient Example – Standard Program
26
Targeted & Engaged as a Percentage of Total Membership
Targeted
Engaged
Health Assessment Incentive & Cover Chantix with Tobacco Program Participation
Focus on Condition Mgmt. Added Pharmacy Incentive for Core Conditions* if Engaged
On-site communications during open enrollment (October 2013)
Added Biometric Screening Requirement
Partnered with account late 2014 into 2015 to update contact information
Identified high volume for Weight Loss but refusal rate high (41%) due to no incentive
Refusal rate decreased to 31% as a result of the added incentive
Impact of the communication seen 4Q 2013 into 2014 –refused downto 17%
Identification up to 51%, but no incentive for non-core conditions drove up UTR** and refused rates
Unable to reach rate down to 27% (<half standard program book avg.). Refused down to 12%.
*Core Conditions – Asthma, Diabetes, CAD, CHF and COPD **UTR – Unable to Reach following multiple outreach attempts
Outcomes:• Tobacco Cessation – Engagements in 2011 resulted in high completion/quit rate in 2012 with cost avoidance over $5 PEPM.
Currently approximately 5x the book average at $1.13 PEPM.• Condition Management – Gap Conversion rate increased from 27% to 46% in 2012. Currently 65% exceeding book average of 54%.• Annual Exam (age 40+) – Increased by 11% from 2011 to 2015. Still slightly below book but getting biometrics.• Cost Avoidance – $24 PEPM in 2012 and $34 PEPM YTD 2015
0%
20%
40%
60%
2012 2013 2014 20152011

INSIDE Obesity Management
Houston Business Coalition on Health
Luigi Meneghini, MD, MBAProfessor, UT Southwestern Medical Center
Executive Director, Global Diabetes Program, Parkland Health & Hospital System

• Baseline data collection & analysis from EMR• Quality Improvement (QI) training & education• Three regional CME/CE conducted by ADA, KOL & clinical site faculty• Patient education• Ongoing data collection & analysis• Publications & presentations
INSIDEQuality Improvement Project
Program Overview: Improve the clinical management of patients with obesity

Agreed with sponsoring partners to focus attention on overweight/obese patients with pre-diabetes
RATIONALE• Intervention on weight directly impacts risk of developing type 2 diabetes• Diabetes Prevention Program (DPP) proven intervention for delaying type 2 diabetes through
weight loss & lifestyle modifications• Delaying type 2 diabetes can have beneficial impact on morbidity & fiscal burden of disease
Challenge: Most patients with pre-diabetes have not been identified
Baseline data collection & analysis

Analyzed 91,574 patients with 454k encounters over 36 months
• Lack data on • Diet, exercise, patient adherence
• Some data/exclusion criteria incomplete, unhelpful, or un-curatedLimitations
Care Quality: EHR Landscape Survey
Age, gender Height, weight, BMIMedications ICD codesHbA1c, glucose, OGTTNephropathy screening
BP, lipid panel, LFTsEthnicity/race, education
Population sample: Age 18-89 with PCP visit < 18 months AND BMI c/w overweight OR Age≥45

Population Demographics
Min: 19
Max: 90+
Median: 53Mean: 52
35% Male / 65% Female
• Seen: 2014-2016 for 1-65 visits, median 4• 56% Hispanic white, 27% Black, 10% Non-
Hispanic white, 4% Asian
AgeInsurance65%
14%8% 7% 5%
Charity Medicare Medicaid Commercial Self Pay

ICD Diagnoses Associated with Obesity (BMI≥30)
65%35%
43%
29% 28%
23%
5%2%
Only 5% have ICD prediabetes codes6%
Only 6% have ICD obesity codes
28% have prediabetes by lab tests

ADA Criteria for Prediabetes/Diabetes Testing in Undiagnosed Adults
79%
21%
% testing in undiagnosed, eligible patients
97% of undiagnosed sample eligible for testing; 79% tested
65%35%
% prediabetes in all undiagnosed patients
23%14,598
23% of undiagnosed sample meets ADA criteria for prediabetes

Diabetes Screening at Parkland• Approximately 61% of Parkland COPC patients without diagnosed
diabetes/prediabetes have been screened in the past 2 years• We are doing BETTER than the National average (53%)
• Of Parkland patients screened Diabetes:• 49% normal glycemic status• 38% Prediabetes• 13% Diabetes
• Although we are doing a good job, nearly half (46%) of COPC patients we have not screened in clinical practice have either prediabetes or diabetes
• Determined by inviting COPC patients in for a screening study

PRE-DIABETES REGISTRY
HIGH RISK Pool
Is patient part of
Diabetes Registry?
Provider Order
NO
Order screening test(Random A1C or fasting
plasma glucose)
Automated result
reporting to ordering
provider
Pre-DM
Diabetes Prevention Program Intervention
(Education materials, local COPC intervention, community program
[YMCA])
No further action
Alert COPC provider &
staff
Diabetes Normal
Assign appropriate ICD10 code (R73.09 for PDM) (E66.x for obesity)
[automated] to Problem List
12
3
45
6
7 8
PHHS EPIC Population
Does patient have pre-DM
by labs (A1C/FPG) &
is not on anti-DM meds*
&/or obesity by BMI?
* With the exception of metformin, GLP-1 RA, pioglitazone or acarbose
YES
Glycemic Risk Surveillance (Bowen Risk Tool)
LOW RISK Pool
Visit-Based DM Screening BPA
(Garland)
Population Health DM Screening (Vickery)
Screening Outreach by Population Health Team
DIABETES REGISTRY
Glycemic Risk Surveillance/ Re-screening (Bowen Tool)
OBESITYREGISTRY

Challenges with ICD coding of obesity & pre-diabetes population• No automated option for patients identified with condition
• ICD code entry would need to be manually entered
• Pre-diabetes & overweight/obesity are dynamic conditions• Will probably change over time making the prior ICD code incorrect
• Establishing registries for the condition based on A1C scores (pre-diabetes) and BMI category makes sense
• Registries can be periodically updated to add/remove patients

• Laboratory-based A1C within past 2 years (5.7-6.4%)• Exclude use of FPG or OGTT
• Exclude anyone in the diabetes registry• No antidiabetic medications with exception of metformin
Preliminary Pre-Diabetes Registry Stand-Up


PRE-DIABETES REGISTRY
OBESITY REGISTRY MODIFIED OBESITY REGISTRY
Is patient part of
Diabetes Registry?
Has patient had PCP visit
in past 18 months?
Identify high DM risk patients (EPIC tool, ADA questionnaire,
Bowen study)
YES
NO
Order screening test(Random A1C or fasting
plasma glucose)
Is patient at high risk for DM or pre-
DM?
Interpret test result
Pre-DM
Diabetes Prevention Program Intervention(Education materials, local COPC intervention,
community program [YMCA])
No further actionAlert COPC provider & staff
Diabetes Normal
YES
Assign appropriate ICD10 code (R73.09)

June 12, 2018

2
What is your “Why?”

of U.S. adults are overweight or obese1
7x higher medical claims
than fit coworkers2
in estimated health care costs directly related to excess pounds
in 20303
$957B Being overweight can drive significant medical costs:
Being overweight increases the risk of developing diseases4 like:
Heart Disease Type 2 Diabetes Hypertension High Blood Pressure Sleep Apnea Musculoskeletal Strain Depression
America’s weight problem is dangerous and expensive
1. Flegal et al., “Prevalence of obesity and trends in the distribution of body mass index among U.S. adults”; Journal of American Medical Association; 2012 2. Finklestein et al., “Obesity and Severe Obesity Forecast through 2030”; American Journal of Preventative Medicine; 2012 3. American Heart Association; “Overweight and Obesity: 2012 Statistical Fact Sheet”; January 2012 4. Centers for Disease Control and Prevention (CDC); “Vital Signs: Adult Obesity”; August 2010
69%
3

of the U.S. population already has diabetes.
10%
Diabetes looms large and real, in every American community.
4 4
of the U.S. adults are prediabetic.
40%

5
It’s about health.
The health of
your company,
your community,
your country.
Source: Centers for Disease Control and Prevention. (2014). National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States, 2014. Atlanta, GA: US Department of Health and Human Services.
$176 billion
$69 billion in direct medical expenses.
in disability, work loss and premature death.
$245 billion PER YEAR.
Total direct and indirect cost of diabetes:
The costly expense of diabetes:

6
You can help.
You can actually prevent chronic disease and save lives.
In fact, you can do more than help.
6

7
87% of Real Appeal participants are considered “at risk” for developing a chronic disease like diabetes.
U.S. Department of Health and Human Services National Institutes of Health, National Diabetes Information Clearinghouse (2006). Diabetes Prevention Program (DPP).
reduction in the risk for pre-diabetic individuals to develop type 2 diabetes by participating in a structured lifestyle-change program.
58% Market to the Willing Impact Those at Risk
Our approach
7

8
We’ve changed the conversation by taking…
20 years of weight loss research
Transformation support
Engaging entertainment
and transforming them into one
personalized & motivating program.
+ + =

Caroline Apulian, M.D., FACP, FACN • Professor of Medicine & Pediatrics; Endocrinology,
Diabetes, Nutrition; Boston University School of Medicine
• Director, Nutrition and Weight Management Center; Boston Medical Center;
• Director, Nutrition and Support Service; Boston Medical Center
Louis J. Arnone, M.D., FACP • Weill Professor of Metabolic Research; Weill-Cornell
Medical College • Medical Director, Center for Weight Management and
Metabolic Clinical Research • Adjunct Associate Professor of Clinical Medicine;
Columbia University
David Afterburner, M.D., M.P.H. • Associate Investigator, Group Health Research Institute
(GHRI) • Group Health Physician, Internal Medicine • Affiliate Associate Professor, Department of Medicine,
University of Washington
Donna Ryan, M.D. • Professor Emeritus, Pennington Biomedical Research
Center • Investigator, Diabetes Prevention Program (DPP)
Steven R. Smith, M.D. • Professor, Metabolic Disease Program, Sanford-
Burnham Medical Research Institute • Scientific Director, Translational Research Institute for
Metabolism and Diabetes • Chief Scientific Officer, Florida Hospital
Thomas A. Wadden, Ph.D. • Albert J. Stunkard Professor of Psychology in Psychiatry,
Perelman School of Medicine, University of Pennsylvania
• Director, Center for Weight and Eating Disorders
Rena R. Wing, Ph.D. • Professor of Psychiatry and Human Behavior, Brown
Medical School • Director, Weight Control & Diabetes Research Center,
The Miriam Hospital
Clinical Advisory Board Guiding Design

1 2 3 4 5 6
Qualify When your employees enroll online, they disclose health and insurance information
which qualifies them for Real Appeal.
Enroll Your employees are invited to
enroll in Real Appeal.
Receive kit A program toolkit including a scale, workout DVDs, session
guides and more is sent to your employee’s home.
Attend weekly sessions Courses led by specially trained coaches
inspire and inform employees.
Access digital tools A suite of digital tools supports
employees and tracks progress to encourage them forward.
Find lasting change
Through these tools and methods, healthy, smart habits will start to form a
different future for your employees.
How Real Appeal works for your employees.
10

Real Appeal Success Kit

Real Appeal Program Tiers
12
At-Risk Intensive Lifestyle Intervention (ILI)
Not At-Risk Self-Directed
Definition An intensive lifestyle intervention experience for individuals who will benefit from clinically relevant weight
loss. Participate in up to 52 weeks of engaging, intensive, customized lifestyle support.
A self-directed experience for individuals who are primarily healthy and do not medically
qualify, but looking to lose a few pounds and maintain a healthy weight.
Qualifications BMI ≥ 30 OR * BMI 25 to 29.9 with qualifying comorbidity BMI 23-29.9 with no qualifying comorbidity
Coaching • Live group Welcome Session • Group sessions with a live virtual coach and videos (20-
30 class size) • Customized 1:1 live coaching, telephone, secure
messaging • Real Appeal Answer Center
• Live group Welcome Session • Group sessions with a live virtual coach
• Messaging with coach • View videos in the online library or DVD
• Real Appeal Answer Center
Supporting Tools • 24/7 access to the secure portal • Tips and tools for healthier living
• Online tracking tools (syncs with RA app, Jawbone, Fitbit)
• Box of supportive tools – Blender, scale, food scale, portion plate, session guide, nutrition guide, workout
DVD
• 24/7 access to the secure portal • Tips and tools for healthier living • Online tracking tools (syncs with RA app,
Jawbone, Fitbit) • Box of supportive tools – Blender, scale, food
scale, portion plate, session guide, nutrition guide, workout DVD

The difference is real. Investing in the wellness of employees is a long-term approach,
continually improving your cost per member over time.
And for these particularly vulnerable individuals, the difference you can make is profound.
13

Real Appeal members have collectively lost more than 1 million pounds.
15
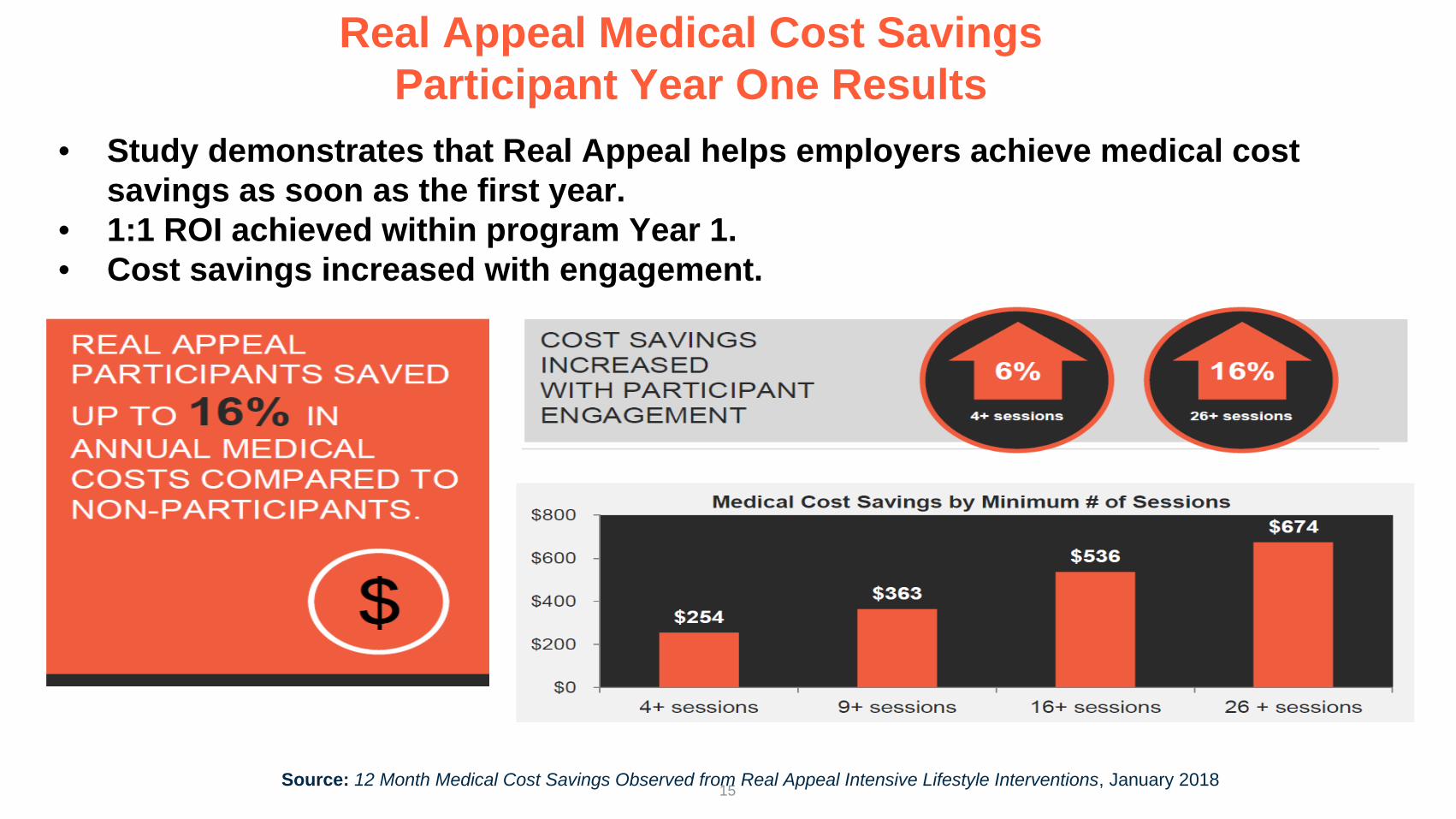
Real Appeal Medical Cost Savings Participant Year One Results
Source: 12 Month Medical Cost Savings Observed from Real Appeal Intensive Lifestyle Interventions, January 2018
• Study demonstrates that Real Appeal helps employers achieve medical cost savings as soon as the first year.
• 1:1 ROI achieved within program Year 1. • Cost savings increased with engagement.

16
I’ve lost 147 lbs. with Real Appeal! When I went into the doctor’s office, he could not believe that I had not had surgery, that I had lost 45% of my body mass the healthy way. Thank you! Brooke J.
When I joined Real Appeal, I could see the results right away. I’ve lost 80 lbs.! I look better, I feel better and I’m no longer pre-diabetic. I changed my life forever! Rochelle W.
I was in denial about being overweight, and there’s a family history of diabetes so I knew I had to make some changes. I lost 60 lbs. with Real Appeal! I’m pretty confident that I’ve scared diabetes from coming anywhere near me. Sandra L.
Real words about true change.
16

Thank you!

Appendix

19
5%
28% 67% 52% 33%
5% 2%
34 Average
85% are pre-diabetic or
obese
Participant BMI Breakdown
Participant Condition Breakdown
BMI over 30
BMI under 25
BMI between 25-
29.9
Pre-Diabetic Obese
Healthy
Diabetic
Engaging those who need prevention most.

20
44 Average
Average Participant Age
Engaging those who need prevention most.
20-29 years
30-39 years
40-49 years
50+ years
11%
27%
29%
33%

21 *Real Appeal Book of Business, results through December 2016; 4-session attendance meets CDC definition of “active participant”, Cohort represents participants at-risk, in program 26+ weeks, attend 4+ ILIs
10 lbs.
20% Engagement
46%
82%
200,000 + enrolled participants*
is the average pounds lost per participant*
of participants have lost at least 5% of their body weight*
of participants have lost weight*
the average engagement compared to other programs*
Real Appeal’s overall success

22
Quantifying the Value of Prevention

23
Implementation
Program set up, claims readiness, and more.
Activation Develop communications plan and provide materials to generate awareness and participation.
Ongoing Support Track participation, measure successes, optimize and report outcomes.
Our Team:
• Completes the customer setup. • Hosts meetings to optimize engagement. • Provides an activation plan and timeline. • Develops awareness campaigns. • Provides engagement and outcomes reporting.
Your Real Appeal team does the heavy lifting.
Our dedicated team supports prevention at scale.
23