2010 rotator cuff book.indd 1 4/19/10 11:35...
TRANSCRIPT

2010 Rotator Cuff Book.indd 1 4/19/10 11:35 AM

i
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
The Ultimate Rotator Cuff Training Guide
Brian Schiff, PT, cScS
Proven Exercises for Injury Prevention & Rehab
2010 Rotator Cuff Book.indd 1 4/19/10 11:35 AM

ii
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
The Ultimate Rotator Cuff Training GuideProven Exercises for Rehab and Injury Prevention
Copyright © 2010, 2004 by Brian Schiff and B Fit Training Systems, LLC
All rights reserved. No part of this book shall be reproduced, stored in a retrieval system, or transmitted by any means – electronic, mechanical, photocopying, recording or otherwise – without written permission from the publisher. No patent liability is assumed with respect to the use of the information contained herein. Although every precaution has been taken in preparation of this book, the publisher and author assume no responsibility for errors or omissions. Neither is any liability assumed for damages resulting from the use of information contained herein.
This book is published by B Fit Training Systems, LLC, including text, graphics and images, and is strictly intended for educational purposes. It is not intended to make any representations or warranties about the outcome of any procedure. This electronic book is not intended as a substitute for professional medical care. Only your doctor can diagnose and treat a medical problem.
2010 Rotator Cuff Book.indd 2 4/19/10 11:35 AM

iii
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
About the Author
Brian Schiff, PT, cScSgraduated from The Ohio State University in 1996 with a Bachelor of Science degree of Physical Therapy in Allied Health Professions. Since then, he has practiced as a licensed physical therapist specializing in sports medicine. Through the National Strength and Conditioning Association, Brian became a certified strength and conditioning specialist (CSCS) in 1998. He is a founding member of The American Association of Personal Trainers, and recently contributed a chapter on periodization to a fitness book entitled The Power of Champions. Schiff also co-authored a breakthrough manual on ACL injury prevention entitled Protecting the Athlete’s Knee.
Currently, he owns a private fitness studio and a performance enhancement company specializing in sport specific training programs for athletes of all sports and ages. Brian is also the former strength and conditioning coach for The Columbus Crew Major League Soccer Team. He has presented at professional conferences and coaches’ clinics on topics including training for shoulder stability, baseball specific training, soccer specific conditioning and sport specific training, ACL injury prevention and safe shoulder training.
2010 Rotator Cuff Book.indd 3 4/19/10 11:35 AM

iv
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Table of Contents
Introduction ..................................................................................... 1 Anatomy .................................................................................................. 2 History of Rotator Cuff Disease and Pathology .............................................. 4 Assessing the Shoulder .............................................................................. 5 The Role of Posture .................................................................................... 8 Injury Prevention Training/Rehab ................................................................ 9
Pendulum Warm-ups ....................................................................... 11 Forward & Backward ................................................................................ 11 Side to Side .............................................................................................. 11 Clockwise & Counterclockwise .................................................................... 12 Scapular Stabilizer Exercises ............................................................ 13 Standing Tubing Row ................................................................................. 13 Standing Dumbbell Row ............................................................................. 14 Serratus Anterior DB Punches ...................................................................... 14 Serratus Punch Push-up Progression ............................................................. 15 Prone Lower Trap Raise .............................................................................. 16 Prone Horizontal Abduction Raise ............................................................... 16 Prone Extension Raise with External Rotation ................................................. 17 Shoulder Shrugs ........................................................................................ 17 Straight Arm Pulls ...................................................................................... 18 Rotator Cuff Exercises ...................................................................... 19 Scaption .................................................................................................. 19 Internal Rotation ........................................................................................ 20 External Rotation (tubing) ........................................................................... 20 External Rotation (dumbbell) ....................................................................... 21 Horizontal External Rotation ....................................................................... 22 Standing Diagonal Raise (D2 Flextion) ......................................................... 22
Common Exercise Mistakes .............................................................. 23 Bench Press .............................................................................................. 23 Lat Pull Downs........................................................................................... 23 Military Press ............................................................................................ 23 Dips/Upright Row ..................................................................................... 24 Dumbbell Lateral Raise ............................................................................... 24
2010 Rotator Cuff Book.indd 4 4/19/10 11:35 AM

v
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Bonus Exercise Section ..................................................................... 25 Exercise #1 – Bench Press .......................................................................... 25 Exercise #2 – Push-Up ............................................................................... 26 Exercise #3 – Lat Pull Downs ...................................................................... 26 Exercise #4 – Upright Row ......................................................................... 27 Exercise #5 – Dips .................................................................................... 28 Exercise #6 – Military Press ........................................................................ 29 Exercise #7 – Dumbbell Lateral Raise ........................................................... 30
Sample Healthy Rotator Cuff Training Program ................................ 32
Injured or Inflamed Shoulder Series ................................................. 33
See Your Physician ........................................................................... 39
Table of Contents
2010 Rotator Cuff Book.indd 5 4/19/10 11:35 AM

1
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
TRAINING SYSTEMS, LLC
TM
Introduction
Have you ever experienced a dull ache or sharp pain in your shoulder or upper arm? Maybe you are unable to sleep on one side because your shoulder wakes you up at night. Perhaps you have discomfort reaching behind your back to tuck in your shirt or grab your wallet. If so, you may be suffering from a rotator cuff injury.
Most of us will experience shoulder pain of some kind in our life. Due to the excessive mobility in our shoulder joints, which allows for great versatility and function, we often place excessive stress on them in our daily life. In order for you to effectively raise and maneuver your arm, the rotator cuff must function properly.
Rotator cuff injuries, such as tendonitis, bursitis and tears, plague 20-30% of people in our population. These injuries may be caused by natural degeneration, trauma or overuse. It is important to understand general anatomy and how the rotator cuff functions so that you may gain a better appreciation for injury potential, healing time frames, and proper exercise selection.
Continued »
2010 Rotator Cuff Book.indd 1 4/19/10 11:35 AM

2
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Anatomy
The rotator cuff consists of four small muscles, which effectively form a sleeve around the shoulder and allow us to raise our arms overhead effectively. These muscles, consisting of the supraspinatus, infraspinatus, teres minor and subscapularis, oppose the action of the deltoid muscle and depress (hold down) the head of the humerus (upper arm) during shoulder elevation to prevent impingement. This allows you to effectively raise your arm and reach in certain ways without experiencing impingement of the soft tissue between the top of the shoulder blade (acromion) and the head of the humerus.
For the purposes of this book, I will not discuss in detail the origins and insertions of each particular muscle or elaborate on the nerves that innervate them. However, it is important to understand that pain in the shoulder area can also be referred from the neck. Therefore, one should not always assume that pain in the upper arm is due to rotator cuff injury or tendonitis. Weakness can be seen with neck or shoulder dysfunction. In light of this, it is always wise to consult your physician if such a problem arises.
Below, I will summarize the role of each rotator cuff muscle. One note to consider: damage to one structure may not always lead to significant functional weakness or limitation. These muscles work collectively and synergistically with the scapular muscles to produce purposeful movement. As such, the body is able to compensate for power deficiencies in many cases. These compensations may be subtle or obvious.
Supraspinatus – largely responsible for initiating elevation from 0 – 30 degrees of abduction (arm moving away from and parallel to the body) and assisting with elevation. This muscle has a poor blood supply, lies beneath the acromion and is often the most commonly affected tendon with regard to tendonitis or tears. Because of its poor blood supply, it heals slowly and is prone to recurrent bouts of inflammation.
Infraspinatus – responsible for externally rotating the arm or moving it away from the body when the arm is at the side or when cocking to throw a baseball. This muscle also helps decelerate the arm during follow through from an overhead motion (e.g., pitching).
Teres Minor – also responsible for external rotation in the same way the infraspinatus functions. In addition, it helps decelerate the arm during follow through from an overhead motion (e.g., pitching).
Subscapularis – responsible for internal rotation or pulling the arm in toward the body while at the side. This muscle also assists in follow through during throwing. Because this muscle performs the same action as that of the pectoralis major, latissimus dorsi and teres major, it is sometimes difficult to detect weakness.
2010 Rotator Cuff Book.indd 2 4/19/10 11:35 AM

3
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Equally important to the proper function of the shoulder is a group of muscles known as scapular stabilizers. These muscles have attachments to the scapula (shoulder blade) and directly contribute to shoulder motion by affecting the path of movement of the shoulder blade. You see, for every 2 degrees of shoulder abduction (arm movement away from the body in the same plane as the body), there is 1 degree of scapular elevation. The shoulder blade moves in addition to the arm to allow for the great freedom of movement we enjoy. With weakness or injury, this rhythm of movement becomes altered.
Scapular stabilizer muscles include:
• Serratus anterior - protracts or rounds the shoulder blade
• Upper trapezius - shrugs and upwardly rotates the shoulder blade
• Middle trapezius - retracts or pinches the shoulder blade inward
• Lower trapezius - depresses and upwardly rotates the shoulder blade
• Rhomboids - retract or pinch the shoulder blade inward
These muscles work synergistically (together) with the rotator cuff to ensure smooth movements without shoulder impingement.
Anatomy
The infraspinatus and teres minor muscles are not pictured as they are positioned on the back of the shoulder blade. This illustration only refers to the front of the shoulder joint.
Glenoid labrum
SupraspinatusHead of humerus
Joint capsule
Scapula
ClavicleCoracoidprocess Acromion
SupraspinatusSubscapularis
HumerusRibs
2010 Rotator Cuff Book.indd 3 4/19/10 11:35 AM
4
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Some people are predestined to have shoulder problems. Why? To a large degree, the shape of the acromion (top of the shoulder blade) plays an important role in the health of the rotator cuff tissue. There are three types of acromion: flat, hook shaped and normal. The flat and hook versions carry a higher risk of possible injury, with the hook style posing the greatest threat. If you have a flat or hook shaped acromion, there is less room for the soft tissue (muscle and tendon) to glide and move during arm motion. Over time, this naturally leads to more friction and wear and tear. This may lead to an eventual tear.
Typically, most people experience an acute onset of shoulder pain. It is often related to vigorous repetitive activities or trauma such as lifting, painting, throwing, falling, or jamming the shoulder. This type of pain is generally labeled tendonitis or bursitis. You may have pain if lying on the affected side, reaching up overhead, reaching behind the back, driving or attempting to lift with the arm out away from the body.
Tendonitis usually responds well to rest, anti-inflammatory medication, ice and rotator cuff specific strengthening. Recovery time may range from 4 weeks to several months, depending upon the compliance of the individual, the onset of symptoms prior to treatment, the age of the individual, and whether or not there are any physical changes in the tendon (structural changes including thickening or scar tissue formation are referred to as tendonosis). X-rays are important as they will reveal any arthritic change.
Rotator cuff tears present differently. The hallmark signs of a tear are nocturnal pain, loss of strength, and inability to raise the arm overhead. Also look for a “shrug sign,” in which the person uses the upper trap to raise the arm because the rotator cuff is not able to depress the humeral head effectively. Rotator cuff tears are most common in men age 65 and older. Tears and/or injury are typically related to degeneration, instability, bone spurs, trauma, overuse, and diminished strength/flexibility related to the aging process. However, youth are also at risk for injury if they are involved in repetitive overhead sports, including swimming, volleyball, baseball, softball, tennis, gymnastics, etc.
Many people can function adequately with a torn rotator cuff provided they have a low to moderate pain level. The primary reason for performing rotator cuff surgery is to alleviate pain rather than to restore function. It is common for post-surgical patients to lose some mobility/range of motion. Strength recovery is dictated by the size of tear, quality of the torn tissue at the time of surgery, time elapsed between injury and repair, and the surgeon’s ability to recreate the proper anatomical relationship.
Recovery following rotator cuff repair may take up to 18 months. However, most people are able to return to the majority of their activities of daily living in 3-6 months. Early mobilization, range of motion and progressive strengthening exercises in physical therapy are critical to regaining functional motion and strength.
History of Rotator Cuff Disease and Pathology
2010 Rotator Cuff Book.indd 4 4/19/10 11:35 AM
5
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Assessing the Shoulder
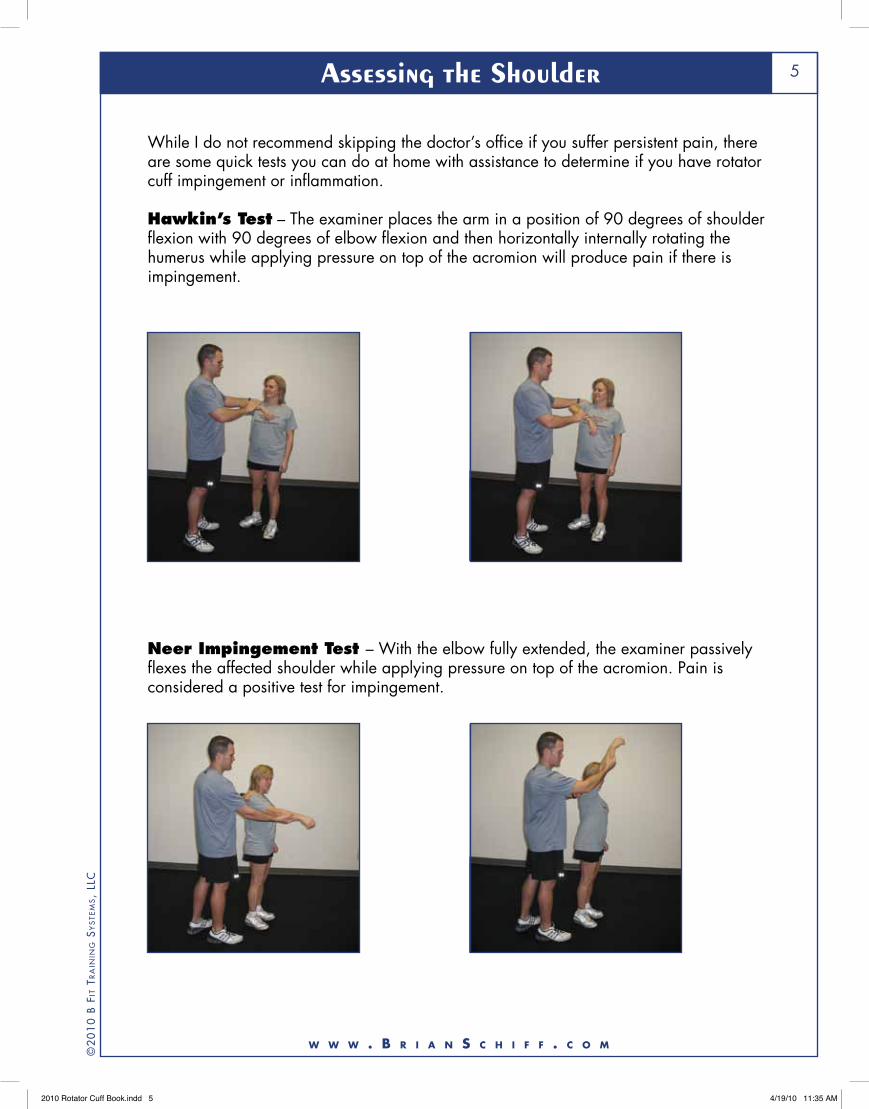
While I do not recommend skipping the doctor’s office if you suffer persistent pain, there are some quick tests you can do at home with assistance to determine if you have rotator cuff impingement or inflammation.
Hawkin’s Test – The examiner places the arm in a position of 90 degrees of shoulder flexion with 90 degrees of elbow flexion and then horizontally internally rotating the humerus while applying pressure on top of the acromion will produce pain if there is impingement.
Neer Impingement Test – With the elbow fully extended, the examiner passively flexes the affected shoulder while applying pressure on top of the acromion. Pain is considered a positive test for impingement.
2010 Rotator Cuff Book.indd 5 4/19/10 11:35 AM

6
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Assessing the Shoulder
A-C Compression Test – This test is used to rule out an AC (acromio-clavicular joint) sprain, otherwise known as a separated shoulder or AC joint arthritis related pain. It is possible that rotator cuff tears and pain can be related to primary AC joint issues or in combination with them.
The examiner slowly stretches the affected arm across the body while stabilizing the shoulder blade. Pain past midline may indicate there is an issue with the AC joint.
Apley Internal Rotation – This self range of motion test often indicates rotator cuff inflammation or impingement if there is painful, limited motion compared to the uninvolved side.
2010 Rotator Cuff Book.indd 6 4/19/10 11:35 AM

7
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Assessing the Shoulder
The Shrug Sign – This self assessment involves actively raising the arm overhead. If there is an exaggerated shrug due to excessive upper trap action and inability to lift the arm past 90 degrees, this is a hallmark sign of a rotator cuff tear. The shrug sign indicates the rotator cuff is not able to adequately compress the head of the humerus. The picture below indicates a positive test.
2010 Rotator Cuff Book.indd 7 4/19/10 11:35 AM

8
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Reverse T Position
The Role of Posture
Did you ever wonder why you were told as a child to sit up tall? Well, it really does make a difference. Slouching allows your shoulders to protract or round forward, and this closes down the space that the rotator cuff occupies. Over time, this can contribute to compressive wear and tear on the soft tissue.
Aside from trying to maintain a more erect posture, it is important to perform strengthening exercises to reinforce posture (e.g., rows, pull downs, and reverse flies) and routine flexibility training. Given the nature of our job place today, many people sit for the majority of the day. They write or work on the computer much of the time. This encourages poor posture and necessitates stretching frequently.
The primary muscle group in need of stretching is the chest. I always recommend performing doorway stretches that include arms in a V position (sternal portion of the pecs) and reverse T or field goal post position (clavicular portion of the pecs). You can also perform single arm stretches with the arm slightly below shoulder height. It is best to hold for 20-30 seconds and repeat 2-3 times. See the pictures below.
V Position L position w/single arm
2010 Rotator Cuff Book.indd 8 4/19/10 11:35 AM

9
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injury PrevenTion Training / rehaB
In the following section, I will outline specific exercises that are designed to prevent and/or rehabilitate shoulder injuries to the rotator cuff. Keep in mind that these exercises are not meant to serve as a substitute to medical care from a physician or physical therapist if you are currently experiencing shoulder pain. But, they provide a good blueprint for healthy shoulder exercises and should reduce the likelihood of a future injury.
The key to avoiding rotator cuff injury is performing adequate conditioning prior to stressing it with vigorous activities. Many weekend warriors try to pick up the softball, baseball, football, etc. and begin throwing repetitively and forcefully without properly warming up. In addition, they are not likely to condition before the season like competitive athletes.
This often leads to excessive strain on the rotator cuff and swelling. The inevitable result is soreness, especially with overhead movement or reaching behind the back. The act of throwing is the most stressful motion on the shoulder. The rotator cuff is forced to decelerate the humerus during follow through at speeds up to 7000 degrees/second.
Without proper strength and conditioning, the shoulder easily becomes inflamed. Since the rotator cuff muscles are small, it is best to utilize lower resistance and higher repetitions to sufficiently strengthen them. Gradually increasing the intensity and volume of activity is critical to avoiding an overuse injury (particularly common among young throwing athletes).
Remember, these are not bodybuilding type muscles. You will not use heavy loads or expect to see great muscle hypertrophy. The payoff comes in performance and injury prevention. Who wants to miss any playing time? The answer is obvious, but rotator cuff pain will restrict most overhead athletes, and it often necessitates some rest in competitive overhead athletes.
The following exercises should be performed at least 6-8 weeks prior to preseason for overhead athletes such as swimmers, pitchers, volleyball players and quarterbacks. For position players in baseball and softball, I generally recommend that they condition the cuff at least 4 weeks prior to preseason drills begin. It is also important for throwing athletes to use an interval throwing program in the preseason to condition the shoulder for repetitive throwing at different distances and velocities.
During the in-season, each of the aforementioned athletes should perform routine maintenance rotator cuff strengthening 1-2x/week for continued injury prevention. With regard to the general fitness client, I recommend using rotator cuff training at least 1-2x/week, especially if you have any pre-existing condition or history of injury. If you have a current issue, perhaps doing these exercises three times per week with a day of rest in between would be best.
2010 Rotator Cuff Book.indd 9 4/19/10 11:35 AM

10
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injury PrevenTion Training & rehaB C
ha
pter 1
The exercises should not cause pain at any time. Performing them in a pain free range of motion is an absolute must! Certainly, pain does not equal gain here. Generally, it is best not to use loads greater than 4% of your body weight (guideline advocated by Charles Neer, M.D.). I can not emphasize enough that these are small relatively weak muscles that are neglected by most of you in the gym. Lighter weight and higher reps is definitely the way to go.
Below you will find a list of appropriate scapular stabilizer and rotator cuff exercises. These exercises are designed to improve posture, correct muscular imbalances, and strengthen the rotator cuff. They are not intended to build lean muscle. Keeping strict form and performing these exercises in a safe, pain free range of motion is essential.
While there is no definitive order in which to perform these exercises, I generally suggest that you do the scapular exercises first since they are the larger muscle group.
2010 Rotator Cuff Book.indd 10 4/19/10 11:35 AM

11
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Pendulum warm-uPS
Using a light dumbbell (2-5#) you can prepare the shoulder for exercise doing pendulum arm swings. The goal is to initiate the movement with the body and allow the arm to follow the path of motion. This can be done forward/backward, side to side and in a clockwise/counterclockwise direction. You may do 15-25 repetitions in each direction.
Forward & Backward
Side to Side
2010 Rotator Cuff Book.indd 11 4/19/10 11:35 AM

12
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Pendulum warm-uPS (conTinued)
Using a light dumbbell (2-5#) you can prepare the shoulder for exercise doing pendulum arm swings. The goal is to initiate the movement with the body and allow the arm to follow the path of motion. This can be done forward/backward, side to side and in a clockwise/counterclockwise direction. You may do 15-25 repetitions in each direction.
Note: Remember to allow the arm to hang freely and glide in response to the movement initiated by the body. It should feel as if it is simply dangling in the air.
Clockwise & Counterclockwise (clockwise pictured below)
2010 Rotator Cuff Book.indd 12 4/19/10 11:35 AM

13
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
1 2
Standing Tubing Row
ScaPular STaBilizer exerciSeS
This strengthens the middle trapezius, posterior deltoid and rhomboids. Using a pole or door, position the tubing so that the handles are even. Stand with the feet shoulder width apart and the knees slightly bent (relaxed). Beginning with some resistance (tube is taut) pull toward the body, squeezing the shoulder blades together and keeping the elbows at your side. Pause for 1-2 seconds and then return to the starting position. Perform 2-3 sets of 10-15 repetitions. This can also be done with a machine. An alternate method is keeping the elbows out with the arms abducted ~ 90 degrees. This positioning places more emphasis on the posterior deltoid, rhomboids and middle trap, as compared to greater assistance from the latissimus dorsi with the low row.
Low Row
High Row1 2
2010 Rotator Cuff Book.indd 13 4/19/10 11:35 AM

14
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
1 2
1 2
Standing Dumbbell Row
Serratus Anterior DB Punches
ScaPular STaBilizer exerciSeS
This can serve as an alternative exercise to the tubing rows if you do not have tubing on hand or wish to mix it up a bit. Position the left leg forward (split stance) while holding the dumbbell in the right hand. Keeping your back flat, lift the weight up in a rowing motion. Pause at the top and lower back down. Repeat 10-15 times and repeat on the other side. Perform 2-3 sets on each side.
This strengthens the serratus anterior, a muscle which helps to stabilize the shoulder blade during arm elevation. Lying on the back with the knees bent and feet flat, press the dumbbells toward the ceiling making sure to keep the elbows straight. The shoulder blades will round forward and lift off the floor. Pause at the top of the movement, and lower with control to the starting position. Perform 2 sets of 15 repetitions.
2010 Rotator Cuff Book.indd 14 4/19/10 11:35 AM

15
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Serratus Punch Push-up Progression
ScaPular STaBilizer exerciSeS
Lying face down with your body weight supported by the forearms and knees (or toes), push the upper body up toward the ceiling (rounding the shoulder blades). Pause at the top and then slowly return to the start position. Perform 2 sets of 15 repetitions in place of the previous exercise.
1 2
On the knees
On the toes (advanced version)
1 2
2010 Rotator Cuff Book.indd 15 4/19/10 11:35 AM

16
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
ScaPular STaBilizer exerciSeS
Prone Horizontal Abduction Raise This strengthens the middle trapezius and rhomboids, which promote good posture. Using a stability ball, raise the arms out away from the body until they are near parallel to the floor. Keep the palms down and pinch the shoulder blades together at the top of the motion. Lower slowly to the starting position. It is also acceptable to do this exercise lying face down on a benchor the edge of your bed with only the affected side. Perform 2 sets of 15 repetitions.
1 2
Prone Lower Trap Raise This strengthens the lower trap, which is often weak and fatigues quickly. This muscle depresses the shoulder blade and prevents impingement. Using a stability ball, raise the arms up in a 45 degree angle as far as the shoulders allow without discomfort. Pause at the top, and lower slowly to the starting position. This is an awkward motion, and it is best to use a light weight and focus on controlling the motion. It is also acceptable to do this exercise lying face down on a bench or the edge of your bed with only the affected side. Perform 2 sets of 15 repetitions.
1 2
2010 Rotator Cuff Book.indd 16 4/19/10 11:35 AM

17
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
ScaPular STaBilizer exerciSeS
Shoulder Shrugs This strengthens the upper trapezius. Standing with the arms resting at the side of the body, shrug the shoulders straight up toward the ceiling. Pause at the top for 1-2 seconds. Slowly lower the weight to the starting position. It is important not to roll the shoulders forward or backward as this may cause grating of the scapula on the chest wall, not to mention the upper trap muscle’s primary action is shoulder elevation. With this exercise, it is okay to use loads heavier than 4% of body weight. Perform 2-3 sets of 10-15 repetitions.
1 2
Prone Extension Raise with External Rotation This strengthens the posterior deltoid and latissimus dorsi, in addition to the posterior rotator cuff muscles. Using a stability ball, raise the arms along the side of the body until they are even with the body. It is important to keep the palms facing down during this exercise (this position externally rotates the shoulder) as this creates greater rotator cuff activation. It is also acceptable to do this exercise lying face down on a bench or the edge of your bed with only the affected side. Pause at the top, and slowly lower to the starting position. Perform 2 sets of 15 repetitions.
1 2
2010 Rotator Cuff Book.indd 17 4/19/10 11:35 AM

18
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
ScaPular STaBilizer exerciSeS
Straight Arm Pulls This strengthens the lats, posterior deltoid and middle/lower trapezius. In standing with elbows straight (palms down) and knees slightly bent, pull the arms back toward the hips. Pause for 1-2 seconds and return to the start position. Keep the back flat throughout. Stand far enough back to have tension during the entire movement. This exercise can be substituted for the pull downs referenced in the scapular stabilizer exercise section of the program. Perform 2-3 sets of 10-15 repetitions.
Note: The scapular stabilizer exercises should generally be performed first in the program as they are larger muscle groups, not to mention the fact they form the foundation for normal rotator cuff function. Adjust weight as tolerated keeping in mind that form should never be compromised, nor should you feel pain at any time as you increase resistance.
1 2
2010 Rotator Cuff Book.indd 18 4/19/10 11:35 AM

19
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
2
2
2
2
Start
Finish
Mid - Position
Side View
roTaTor cuff exerciSeS
Scaption This strengthens the supraspinatus muscle, the most commonly affected rotator cuff muscle and slowest to heal. Stand with the knees slightly bent (relaxed) holding the dumbbells in such a way that your thumbs are up or on top of the dumbbells. Keep the arms approximately 30-45 degrees forward from being perpendicular or straight out away from the body (scapular plane) and raise the arms up to shoulder height. Pause at the top and slowly lower to the starting position. Keep the elbows straight throughout the entire movement. Avoid any part of the range of motion that causes pain. Perform 2 sets of 15-20 repetitions.
2010 Rotator Cuff Book.indd 19 4/19/10 11:35 AM

20
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
roTaTor cuff exerciSeS
External Rotation (tubing) This strengthens the infraspinatus and teres minor muscles. In standing with the knees relaxed, hold tubing and begin with the arm positioned at the side (neutral) with light tension on the tubing. Place a small rolled towel between the upper arm and body. Now, pull the arm away from the body, while keeping the elbow close to your side. Do not allow the shoulder to rotate backward. Perform 2 sets of 15-20 repetitions.
Internal Rotation This strengthens the subscapularis muscle, as well as the chest muscles. In standing with the knees relaxed, hold tubing and begin with the arm positioned at the side (neutral) with light tension on the tubing. Place a small rolled towel between the upper arm and body. Now pull the arm across the body to the stomach, while keeping the elbow at your side. Do not allow the shoulder to rotate forward. Perform 2 sets of 15-20 repetitions.
1 2
1 2
Start
Start
Finish
Finish
2010 Rotator Cuff Book.indd 20 4/19/10 11:35 AM

21
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
roTaTor cuff exerciSeS
External Rotation (Dumbbell) This too strengthens the infraspinatus and teres minor. I prefer this exercise over tubing if you have an inflamed rotator cuff. The reason for this is that the dumbbell provides consistent resistance throughout the range of motion with respect to gravity, whereas, the resistance with tubing actually increases as the muscle becomes less able to generate tension. Even though the tubing eliminates gravity, it still provides a force loading vs. force generation mismatch, which tends to aggravate the rotator cuff. As such, it is generally best to use a light dumbbell in this case.
Begin in a side lying position with the elbow at the side of the body and the arm in neutral. Place a small rolled towel between the upper arm and body. Slowly raise the dumbbell through a full pain free range of motion, while keeping the elbow at your side and then slowly return to the starting position. Perform 2 sets of 15-20 repetitions.
NotesYou do not need to do both tubing and dumbbell external rotation. Choose one method. However, if you are experiencing ongoing pain or inflammation, I recommend using a dumbbell or no resistance at all in the side lying position. The key difference is that the tubing offers increasing resistance throughout the exercise as the muscle’s ability to generate force declines.
In contrast, a dumbbell offers consistent resistance throughout the exercise. With a dumbbell, the ability to lift the weight is dependent upon raising the dumbbell up against gravity at the beginning of the motion. This does not require added tension or effort at the end of the movement, whereas the tubing does.
You may also choose to place a small rolled towel between the inside of the elbow and the side of your body to emphasize keeping the elbow in and avoiding compensatory motion from the shoulder blade.
1 2
2010 Rotator Cuff Book.indd 21 4/19/10 11:35 AM

22
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
roTaTor cuff exerciSeS
Horizontal External Rotation This strengthens the infrapsinatus, teres minor and posterior deltoid. It also works the shoulder in a more functional plane. Sitting on a stability ball (or bench), begin with arm 90 degrees away from the body with the palm of the hand facing the floor. Raise the dumbbell up to 90 degrees and slowly return to the starting position. Perform 2 sets of 15-20 repetitions.
Standing Diagonal Raise (D2 Flexion) This is a more advanced exercise that strengthens the entire rotator cuff. It also maximally stresses the cuff as it places it in an overhead position. Begin in standing with relaxed knees and with the palm against the opposite thigh. Slowly raise the dumbbell up and overhead. As the arm elevates, you will allow the forearm to rotate out and the thumb to move from a downward to an upward position (hitchhiking position). Lower slowly to the starting position. Perform 2 sets of 15-20 repetitions.
1 2 3
1 2 3
Beginning
Beginning
Mid - Position
Mid - Position
Finish
Finish
2010 Rotator Cuff Book.indd 22 4/19/10 11:35 AM

23
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Common Exercise Mistakes
All too often I see people in the gym performing exercises incorrectly. This may not lead to an immediate injury, but over time it will cause tendonitis, pain, and lost time from working out. Aside from lifting improperly, many exercise enthusiasts attempt to lift too much weight. This combination is a proven recipe for injury. Below, I will discuss some common exercises that offer potential risk for injury when performed improperly. With a few simple modifications, these exercises deliver maximum results without posing any danger to your health.
Bench Press – This is a popular exercise chosen to build the chest, along with the anterior deltoid and triceps. Most teach taking the bar down until it lightly touches the chest. However, I believe this is unsafe because it exposes the anterior shoulder capsule to excessive load, in addition to compressing the soft tissue of the rotator cuff between the humerus and the acromion. Over time, with repeated bouts and heavy loads, the rotator cuff becomes inflamed. Individuals with any anterior shoulder laxity (looseness) or history of subluxation, dislocation or instability are also at increased risk for rotator cuff injury or labral (shoulder cartilage) damage. Furthermore, you also have the potential to rupture the pectoralis tendon (chest) with full range pressing during heavy loads. The safe answer is to lower the bar until the upper arm is parallel to the floor (elbow bent to 90 degrees). This prevents the shoulder joint from moving into the unsafe range. The same advice applies to push-ups and dumbbell flies.
Lat Pull Downs – This is a good exercise to strengthen the back, but when done behind the head it can cause problems. Like the bench press, pulling the bar down behind the head positions the humerus in such a way that the rotator cuff can be pinched. This may depend on other factors, including the shape of a person’s acromion and degree of any present arthritis, but I still believe the risk outweighs any benefit. Not to mention that keeping the bar in front of the head still accomplishes the same movement for the target muscle, while eliminating the risk of shoulder injury. Remember not to sway during the movement, and position the body in a slightly reclined position (20-30 degrees), while pulling the bar toward the sternum. Another unrelated reason not to do behind the neck pull downs is that it places undue stress on the cervical spine.
Military Press – This exercise, when performed behind the neck with a bar, positions the shoulder in the aforementioned unfavorable position. Done repeatedly, the rotator cuff can become inflamed. Similar to behind the neck pull downs, you also expose your neck to unnecessary stress. It is safer to perform the exercise in front of the head or utilize dumbbells and work in the scapular plane (a position about 30-45 degrees forward of the plane of the body). You must watch to avoid arching the low back, and it is best to use a bench with back support to prevent this.
2010 Rotator Cuff Book.indd 23 4/19/10 11:35 AM

24
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Dips/Upright Row – As before, the key mistake made with these exercises is allowing the shoulder to move beyond 90 degrees relative to a position parallel to the floor or perpendicular to the body. I always recommend stopping at 90 degrees to protect the shoulder capsule and the rotator cuff. These are also not exercises I recommend to those just beginning to work out. It is best served to incorporate them after developing a base level of strength and mastering basic lifting movements. People with A-C (acromio-clavicular) joint arthritis should probably avoid dips, as this joint undergoes much stress.
Dumbbell Lateral Raise – I believe this exercise is often done incorrectly. The mistakes include lifting too much weight, keeping the arms straight, and raising the arms out away from the body in the plane of the body. The force on the rotator cuff reaches 90% of your body weight when the arms are raised to 90 degrees with the arms straight and in the plane of the body. That is a lot of force on four relatively small rotator cuff muscles. The target muscle is the lateral deltoid, but the rotator cuff is extremely active, and it functions to allow you to raise the arm by depressing the humerus so that it passes under the acromion during active elevation. When heavy loads are introduced in the wrong plane of motion, disaster usually occurs. I am fanatical about performing this exercise correctly. The proper way to execute a lateral raise is to keep the elbows comfortably flexed (20-30 degrees) and raise the arm to no higher than parallel to the floor. The arm should be in the scapular plane of motion (approximately 30-45 degrees forward from the plane of the body) and the weight should be relatively light. Once you feel you have to shrug or use momentum to raise the weight, you need to rest or lower the weight. I feel this is absolutely one of the worst exercises for the shoulder if done incorrectly.
In summary, I want to emphasize that good intentions may spell bad results for the shoulder if proper form is lacking. The rotator cuff and shoulder joint is extremely vulnerable to heavy loads and repetitive bouts of exercise. Gradually, it may become inflamed and hinder or limit your workout altogether. Be sure to master form before increasing weight, and do not attempt to work through pain, as this often perpetuates the problem. Remember to assess risk and reward at all times, and rest assured that these modifications will not hinder your gains. Instead, they will prevent missed time in the gym and produce happier, healthier shoulders!
Common Exercise Mistakes
2010 Rotator Cuff Book.indd 24 4/19/10 11:35 AM

25
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
BonuS exerciSe SecTion
Exercise # 1 – Bench PressWith my background in physical therapy, and having experienced severe rotator cuff tendonitis firsthand, I can tell you how harmful this exercise truly is when done improperly. So, what is improper form? I always recommend limiting the range of motion on descent to the point where the upper arm is parallel to the floor. Lowering past this plane places excessive stress on the front of the shoulder joint.
With heavy loads or repetitive loading, you expose the ligaments, cartilage and rotator cuff to wear and tear. Additionally, you may even be at risk for rupturing the pectoralis (chest) muscle. While some purists in the strength and conditioning field will argue that limiting motion affects strength gains, I would argue that the risk of injury outweighs any benefit gained from the additional range of motion. Not to mention the fact that I have not lost strength on the bench after performing this modified version for over 10 years.
In this section, I will outline some additional shoulder/upper body exercises that are often done incorrectly in the gym. When these particular exercises are done with poor form and excessive loads, the results can be disastrous. Even with lighter loads, over time repetitive lifting with faulty alignment will lead to overuse injuries and probably tendonitis.
2010 Rotator Cuff Book.indd 25 4/19/10 11:35 AM

26
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
BonuS exerciSe SecTion
1 2
Exercise # 3 – Lat Pull DownsThis exercise is designed to strengthen the back, specifically the latissimus dorsi. In the past, many have done this exercise behind the head. In addition to placing unnecessary stress on the neck, this positioning puts added stress on the shoulders. Pulling the bar behind the head forces the humerus into the top of the shoulder blade and can compress the rotator cuff. In light of this, I suggest pulling the bar to the sternum. Recline the body approximately 20-30 degrees and lower the bar in front of the head, squeezing the shoulder blades down and together.
Exercise # 2 – Push-up
1 2
This is a great upper body strengthening exercise. However, much like the bench press, moving beyond 90 degrees with the shoulders on the descent places undue stress on the shoulders. For this reason, it is not advisable to lower beyond this point.
2010 Rotator Cuff Book.indd 26 4/19/10 11:35 AM

27
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
BonuS exerciSe SecTion
Exercise # 4 – Upright RowThis exercise is a popular method of strengthening the shoulders and adding muscle mass to the lateral deltoids and upper traps. It may be done with dumbbells, tubing or with a cable attachment. The key to avoiding damage with this exercise is to stop the movement once the arms reach 90 degrees, or are parallel to the ground. Going above this position will lead to impingement of the rotator cuff. Remember to lead with the elbows and allow the hands to follow in a natural path of motion.
2010 Rotator Cuff Book.indd 27 4/19/10 11:35 AM

28
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
1 2
Exercise # 5 – DipsDips are difficult for people to do and place a lot of stress on the shoulder complex. In addition to placing high demands on the shoulder joint and rotator cuff itself, the clavicle and acromio-clavicular joint is also exposed to significant loads during this exercise. Dips are designed to strengthen the upper body, more specifically the chest, shoulders, and triceps. This exercise is similar to the upright row with regard to shoulder positioning.
Whether using a dip apparatus, assisted dip machine or flat bench, it is important not to lower the body past a point where the upper arms are parallel to the floor. I do not recommend this activity (even when done properly) for people with current rotator cuff injuries, A-C joint arthritis, shoulder instability, or those with partial/complete rotator cuff tears or prior surgery to repair a tear.
As a general rule, I use this exercise infrequently for clientele over the age of 40 as it tends to add repetitive stress to the AC joint and may lead to overuse injuries.
2010 Rotator Cuff Book.indd 28 4/19/10 11:35 AM

29
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
BonuS exerciSe SecTion
Exercise # 6 – Military PressThis is by far one of the most popular and effective means to build shapely shoulders. For the same reasons explained earlier with the lat pull downs, I again recommend not performing shoulder presses behind the head. Additionally, it is important not to lower the bar or dumbbells below the point where the upper arms are parallel to the floor (shoulder height) to avoid compressive forces on the cuff. I also suggest keeping the arms in the scapular plane throughout the movement (30-45 degrees forward of the plane of the body). Lastly, keep your back pressed firmly against the bench during the exercise. If the back begins to arch, this typically means the weight is too heavy or you are becoming fatigued. This exercise should not be done if you are experiencing pain with overhead motion.
1 1
Start - Front Finish - Side
2010 Rotator Cuff Book.indd 29 4/19/10 11:35 AM

30
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
Perhaps, this is one of the most common shoulder exercises I see routinely done incorrectly. It is a great way to strengthen the lateral deltoid, but when done with improper technique, it often leads to rotator cuff tendonitis.
The most common mistake I see is performing this activity with the arms completely straight and moving them out directly away from the side. Keeping the arms straight provides a long lever and places a high amount of torque on the joint and rotator cuff. With this alignment, you also encourage shoulder impingement. It is essential to keep the shoulders in the scapular plane throughout.
The second major mistake is using too much weight. Heavier loads require using momentum and other larger muscles to accomplish the lift (such as the low back and hip extensors). Men are generally the biggest offenders on this point. Remember, the movement should be slow, and you should be able to pause momentarily at the top of the lift.
Next, I often witness people raising their arms above shoulder height. Although the cuff functions most from 70 – 120 degrees of elevation, I have found that raising the arm above 90 degrees encourages impingement in a loaded shoulder and often aggravates a person’s symptoms. Sometimes, it is necessary to limit the range of motion further based on pain. This is okay. As a matter of fact, you should only perform the exercise with a weight and range of motion that does not increase pain.
BonuS exerciSe SecTion
Exercise # 7 – Dumbbell Lateral Raise
2010 Rotator Cuff Book.indd 30 4/19/10 11:35 AM

31
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
BonuS exerciSe SecTion
Exercise # 7 – Dumbbell Lateral Raise (continued)The final error is related to set-up position. Many simply stand erect with their feet too close together during this exercise. A better method is to stand with the feet shoulder width apart and the knees slightly bent. This will prevent cheating by using momentum and engage the core muscles throughout the exercise. It is important to maintain a flat back or the natural curve of your spine in this athletic position.
This exercise is similar to scaption, but places a greater load on the lateral deltoid due to the different hand position (palm down). If you are unable to do lateral raises without pain, scaption will also activate the lateral deltoid and serve as a good precursor to returning to lateral raises.
I generally recommend avoiding lateral raises with bands or tubing as the load continually increases, while the muscle’s ability to generate force decreases. With repetition, this approach to training leads to a sore shoulder. Performing this exercise on a cable also provides a significant challenge in terms of controlling the movement and should only be done occasionally with lighter weight and perfect form.
2
Side View – Finish
1 2
Start Finish
2010 Rotator Cuff Book.indd 31 4/19/10 11:35 AM

32
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
SamPle healThy roTaTor cuff Training Program
Healthy Shoulder Series (2x/week)
Scapular Stabilizer MusclesDumbbell or Tubing Rows (p. 14) – 3 sets of 10-15 repsLat Pull Downs (or Straight Arm Pulls) (p. 26) – 3 sets of 10-15 repsSerratus Dumbbell Punches (p. 14) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsSeated Dumbbell Horizontal External Rotation (p. 22) – 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #1
Scapular Stabilizer MusclesProne Lower Trap Dumbbell Raise (p. 16) – 2 sets of 15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation w/Arm at Side (tubing or dumbbell) (p. 20-21) – 2 sets of 15-20 repsStanding Diagonal Dumbbell Raise (p. 22) – 2 sets of 15-20 reps
Day #2
2010 Rotator Cuff Book.indd 32 4/19/10 11:35 AM

33
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
During this program, it is generally best to avoid overhead lifting. Once most of the pain or discomfort resolves, you can gradually resume overhead training.
At the completion of the initial 4 weeks, you should notice improved strength, more range of motion and less discomfort with shoulder movements and function. Throughout this time, none of the exercises should cause any discomfort or pain. If you can not perform an exercise without pain, it is best to limit the range of motion or discontinue it altogether.
If you are making progress with the exercises, then you can progress to the final phase of this 6 week program. In the final phase, more emphasis is placed on transitioning back to overhead positions and functional movements. Less emphasis is placed on shrugs and serratus punches, as sufficient stabilization strength should have been attained in the initial month of training. Again, it is critical to make sure the exercise is completely pain free!
Training Notes
2010 Rotator Cuff Book.indd 33 4/19/10 11:35 AM

34
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
Scapular Stabilizer MusclesLow Row (or Dumbbell Rows) (p. 13) – 2-3 sets of 10-15 repsSerratus Dumbbell Punches (p. 14) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #1 (Week 1 & 2)
Scapular Stabilizer MusclesLat Pull Downs (or Straight Arm Pulls) (p. 26) – 3 sets of 10-15 repsSerratus Dumbbell Punches (p. 14) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #2 (Week 1 & 2)
Scapular Stabilizer MusclesHigh Row (or Dumbbell Row) (p. 13-14) – 3 sets of 10-15 repsSerratus Dumbbell Punches (p. 14)– 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #3 (Week 1 & 2)
2010 Rotator Cuff Book.indd 34 4/19/10 11:35 AM

35
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
Scapular Stabilizer MusclesLow Row (or Dumbbell Rows) (p. 13) – 2-3 sets of 10-15 repsSerratus Push-ups (p. 15) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #1 (Week 3 & 4)
Scapular Stabilizer MusclesHigh Row (or Dumbbell Rows) (p. 13-14) – 3 sets of 10-15 repsSerratus Push-ups (p. 15) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsSeated Dumbbell Horizontal External Rotation (p. 22) – 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 reps
Day #2 (Week 3 & 4)
2010 Rotator Cuff Book.indd 35 4/19/10 11:35 AM

36
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
Scapular Stabilizer MusclesLat Pull Downs (or Straight Arm Pulls) (p. 26) – 3 sets of 10-15 repsSerratus Pushups (p. 15) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsSeated Dumbbell Horizontal External Rotation (p. 22) – 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 22) – 2 sets of 15-20 reps
Day #3 (Week 3 & 4)
2010 Rotator Cuff Book.indd 36 4/19/10 11:35 AM

37
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
Scapular Stabilizer MusclesLow Row (or Dumbbell Rows) (p. 13) – 2-3 sets of 10-15 repsProne Lower Trap Dumbbell Raise (p. 16) – 2 sets of 15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsExternal Rotation (Dumbbell) (p. 21) - 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 22) – 2 sets of 15-20 repsSeated Dumbbell Horizontal External Rotation (p. 22) – 2 sets of 15-20 reps
Day #1 (Week 5 & 6)
Scapular Stabilizer MusclesHigh Row (or Dumbbell Rows) (p. 13-14) – 2-3 sets of 10-15 repsProne Lower Trap Dumbbell Raise (p. 16) – 2 sets of 15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 repsSerratus Dumbbell Punches (p. 14) – 2 sets of 15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 20) – 2 sets of 15-20 repsStanding Diagonal Dumbbell Raise (p. 22) – 2 sets of 15-20 reps
Day #2 (Week 5 & 6)
2010 Rotator Cuff Book.indd 37 4/19/10 11:35 AM

38
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
injured or inflamed Shoulder SerieS 6 Week Program (3x/week)
Scapular Stabilizer MusclesLat Pull Downs (or Straight Arm Pulls) (p. 26) – 3 sets of 10-15 repsProne Lower Trap Dumbbell Raise (p. 16) – 2 sets of 15 repsProne Horizontal Abduction Raise (p. 16) – 2 sets of 10-15 repsProne Extension Raise w/External Rotation (p. 17) – 2 sets of 15 repsDumbbell Shoulder Shrugs (p. 17) – 2-3 sets of 10-15 reps
Rotator Cuff MusclesScaption (p. 19) – 2 sets of 15-20 repsSeated Dumbbell Horizontal External Rotation (p. 22) – 2 sets of 15-20 repsInternal Rotation w/Tubing (p. 22) – 2 sets of 15-20 repsStanding Diagonal Dumbbell Raise (p. 22) – 2 sets of 15-20 reps
Day #3 (Week 5 & 6)
2010 Rotator Cuff Book.indd 38 4/19/10 11:35 AM

39
w w w . B r i a n S c h i f f . c o m
©2
01
0 B
Fit
tr
ain
ing
Sy
Ste
mS,
LLC
See your PhySician
The previous exercise program is not intended to replace professional medical care by a physician or physical therapist. It is simply designed to strengthen the rotator cuff and scapular stabilizer muscles, correct muscular imbalances and improve shoulder function. If you suffer from chronic shoulder pain, experience an acute onset of significant shoulder pain, or notice gross weakness and limitation with activities of daily living, it is recommended that you see your physician for a complete evaluation.
After completing the six week program, you may not be pain free. In this case, I generally recommend continuing with week 5 and 6 exercises for several more weeks until your symptoms resolve. Chronic pain often takes longer to respond to treatment. If you do not experience improvement with the program, it is recommended that you seek professional medical evaluation and treatment.
With that said, I hope the information in this book will enable you to train more safely and efficiently in the future. At the very least, the techniques described here will allow you to avoid many common exercise pitfalls that lead to compressive wear and tear on the rotator cuff itself. While it is not absolutely necessary to perform rotator cuff strengthening on a weekly basis, I highly recommend incorporating the training modifications as outlined earlier with respect to the bonus exercises. In addition, keep in mind the importance of posture, flexibility and rotator cuff strengthening in relation to proper shoulder function.
For more information regarding my training or consulting services you can e-mail me at [email protected] and www.brianschiff.com.
2010 Rotator Cuff Book.indd 39 4/19/10 11:35 AM

2010 Rotator Cuff Book.indd 40 4/19/10 11:35 AM