2007 ucsf stanford current issues in anatomic … ucsf stanford current issues in anatomic pathology...
TRANSCRIPT
Cartilage tumors of bone
2007 UCSF Stanford Current Issues in Anatomic Pathology
Andrew Horvai M.D. Ph.D.
Outline• Principles: Definitions, radiology, treatment • Common intramedullary tumors
– Chondroblastoma– Enchondroma– Conventional chondrosarcoma– Dedifferentiated chondrosarcoma– Variants: clear cell & mesenchymal chondrosarcoma
• Current issues and controversies– Grading– Malignant transformation– Cartilage tumors of small bones of hands and feet
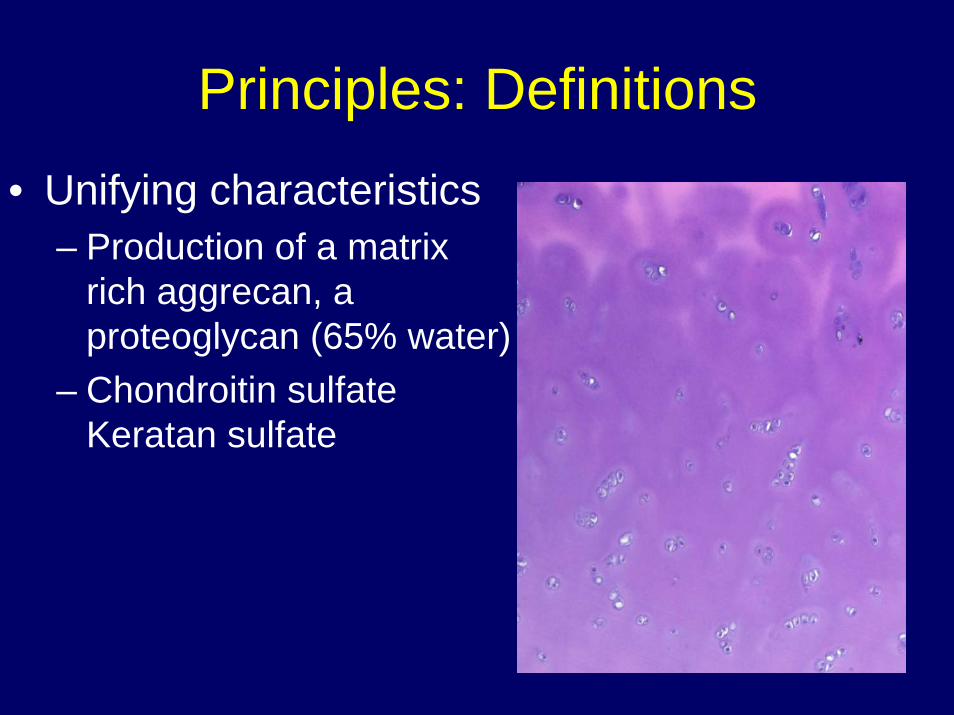
Principles: Definitions• Unifying characteristics
– Production of a matrix rich aggrecan, a proteoglycan (65% water)
– Chondroitin sulfate Keratan sulfate
Principles: Radiology• Opacity
– Lytic– Sclerotic– Mixed
• Border– Marginated– Circumscribed– Moth eaten– Permeative
• Periosteum– Solid: Thickened cortex– Elevated: Codman’s triangle– Spiculated: New bone at right angles to cortex– Onion skin: New bone parallel to cortex
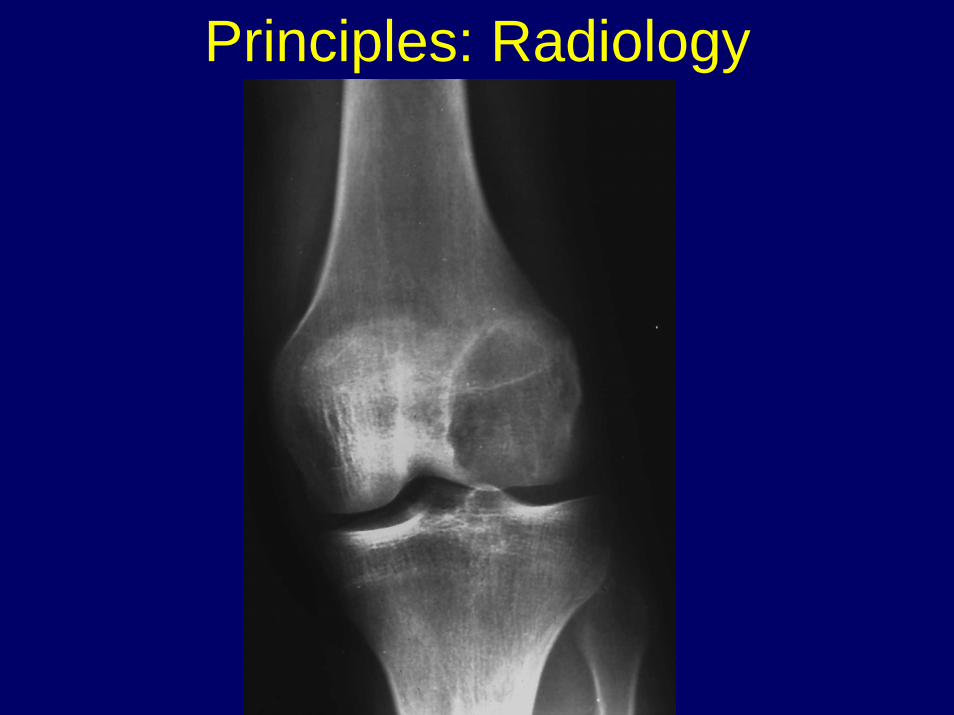
Principles: Radiology

Principles: Radiology

Principles: Radiology
Ring-like calcifications
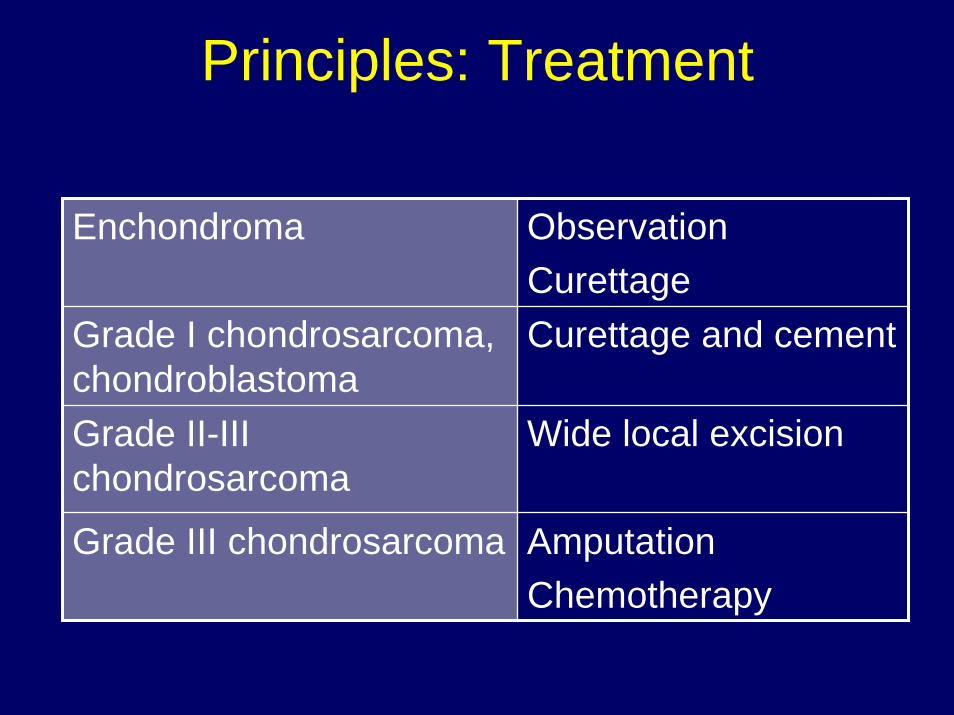
Principles: Treatment
Enchondroma ObservationCurettage
Grade I chondrosarcoma, chondroblastoma
Curettage and cement
Grade II-III chondrosarcoma
Wide local excision
Grade III chondrosarcoma AmputationChemotherapy
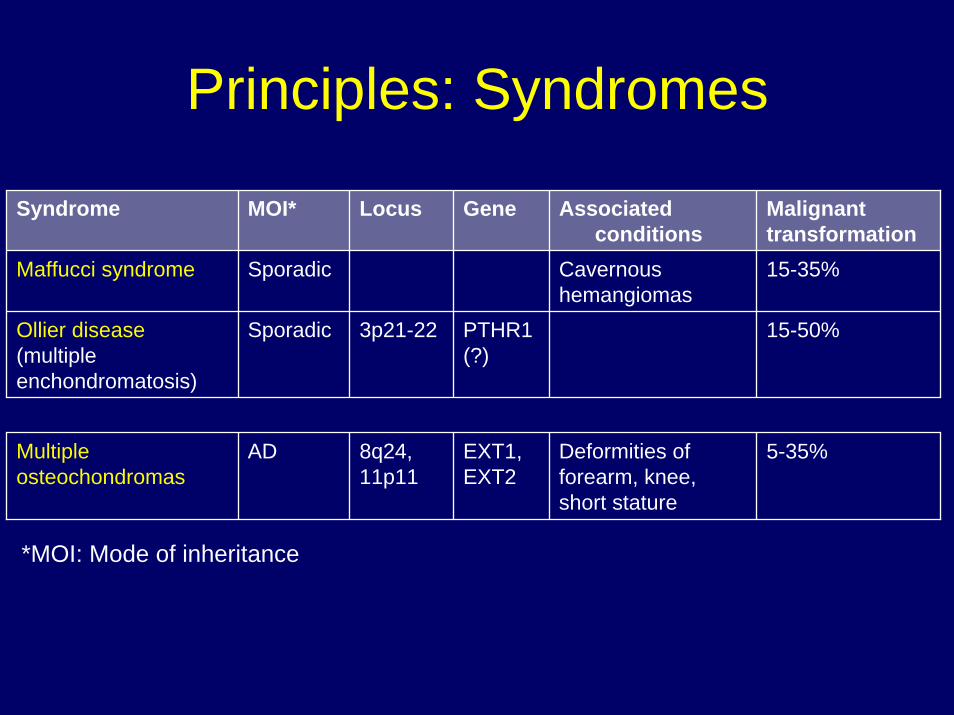
Principles: Syndromes
Syndrome MOI* Locus Gene Associated conditions
Malignanttransformation15-35%
15-50%
5-35%
Maffucci syndrome Sporadic Cavernous hemangiomas
Ollier disease(multiple enchondromatosis)
Sporadic 3p21-22 PTHR1(?)
Multiple osteochondromas
AD 8q24,11p11
EXT1, EXT2
Deformities of forearm, knee, short stature
*MOI: Mode of inheritance
Malignant transformation
• Chondroblastoma– Case reports (correct diagnosis?)– Benign metastasizing chondroblastoma
• Solitary Enchondroma– Case reports
• Sporadic Osteochondroma– 1-8%
Case 1
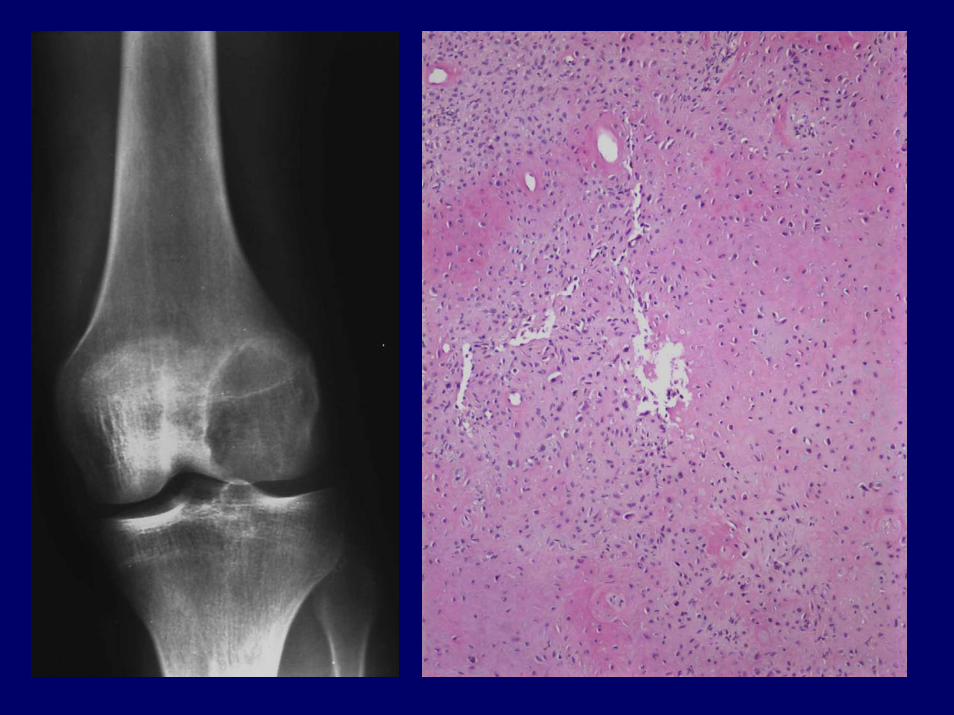
• 17 year old girl, injured her left knee playing soccer and has had persistent pain at the site prompting X-Rays
Clinical Radiology Histology Ddx
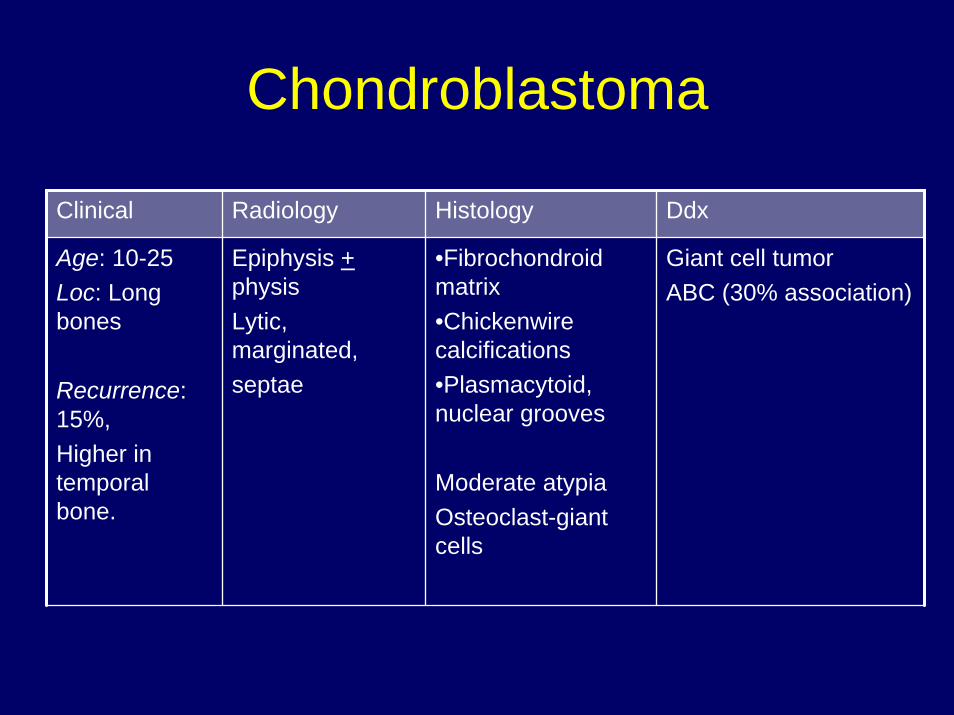
Age: 10-25Loc: Long bones
Recurrence: 15%, Higher in temporal bone.
Epiphysis +physisLytic, marginated,septae
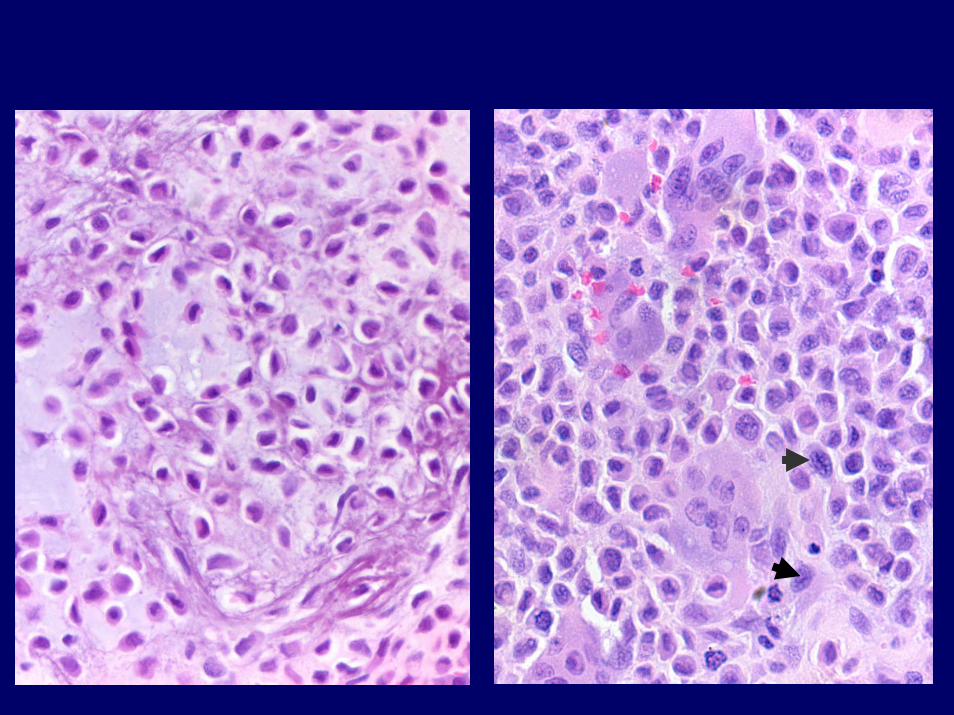
•Fibrochondroid matrix•Chickenwire calcifications•Plasmacytoid, nuclear grooves
Moderate atypiaOsteoclast-giant cells
Giant cell tumorABC (30% association)
Chondroblastoma

Case 2
• 20 year old woman with history of “lesion”in right tibia.
• No pain, no palpable mass.
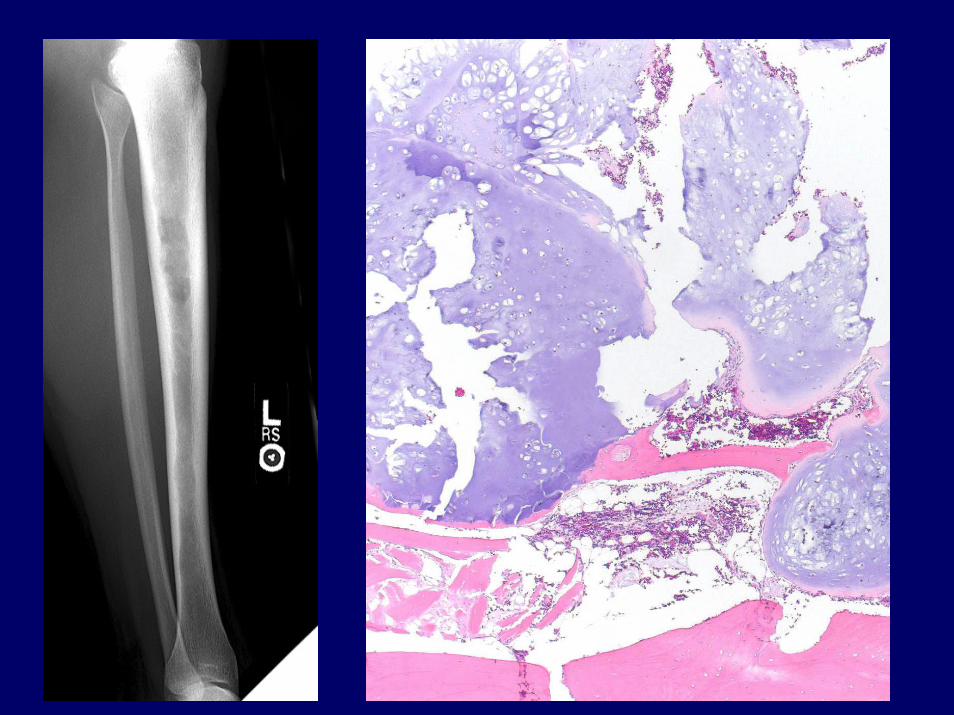
Clinical Radiology Histology Ddx
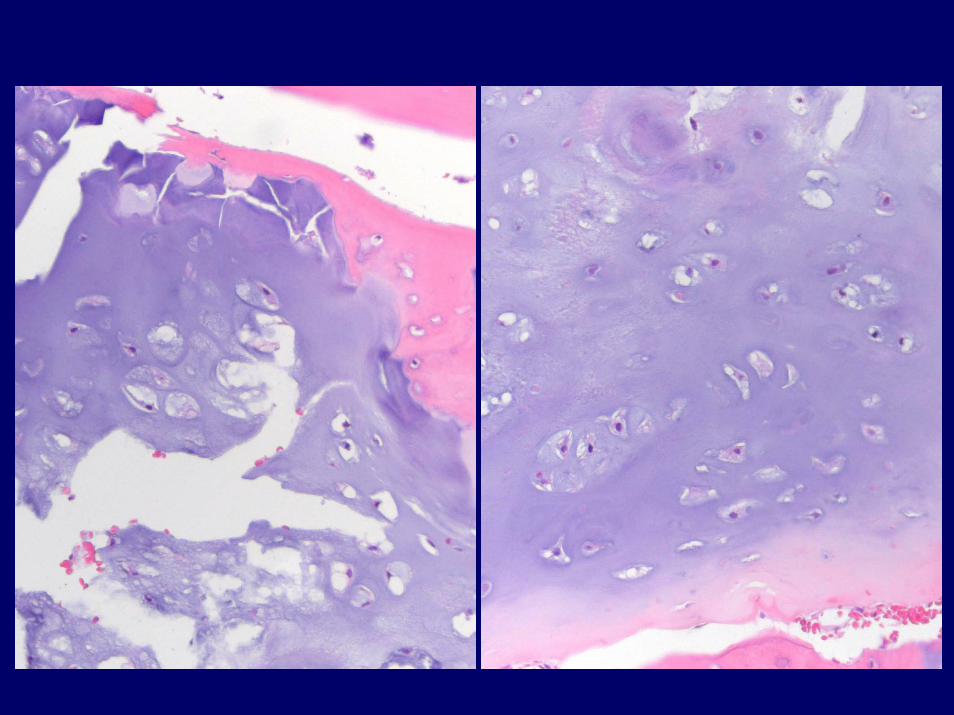
Age: AllLoc: Hands/feet, long tubular bones
MetaphysisLytic, lobularRing calcificationsIntact cortex
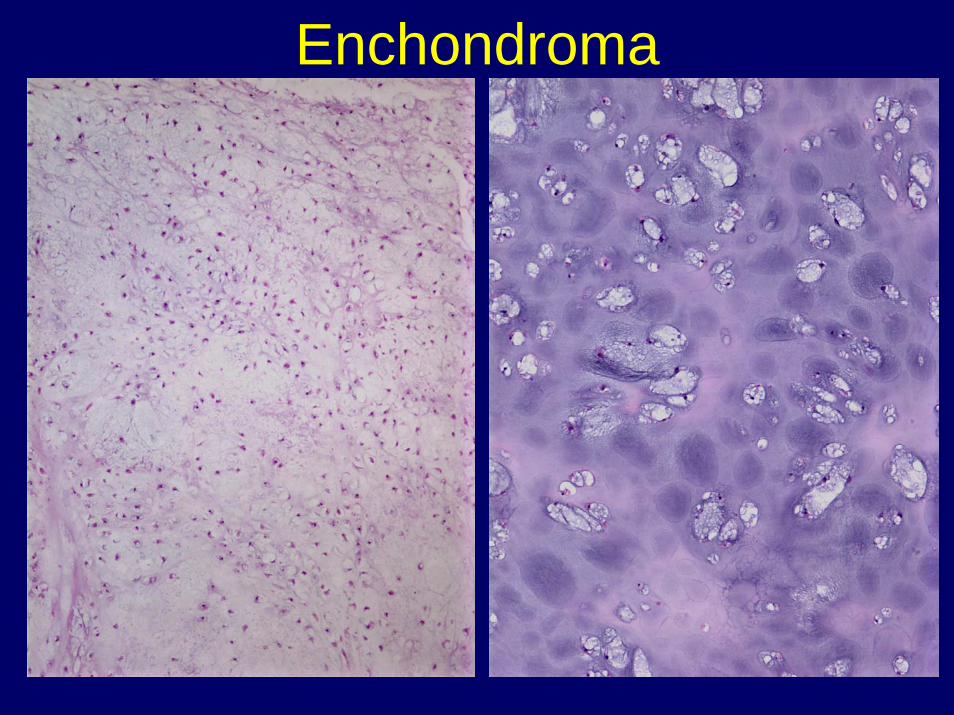
LobularPeripheral ossificationNo permeationLow cellularityNo atypia/mitoses
Grade I Chondrosarcoma
Enchondroma
Enchondroma
Case 3
• 53 year old woman with “hip” pain x 2 months
• Needle biopsy performed of hip mass
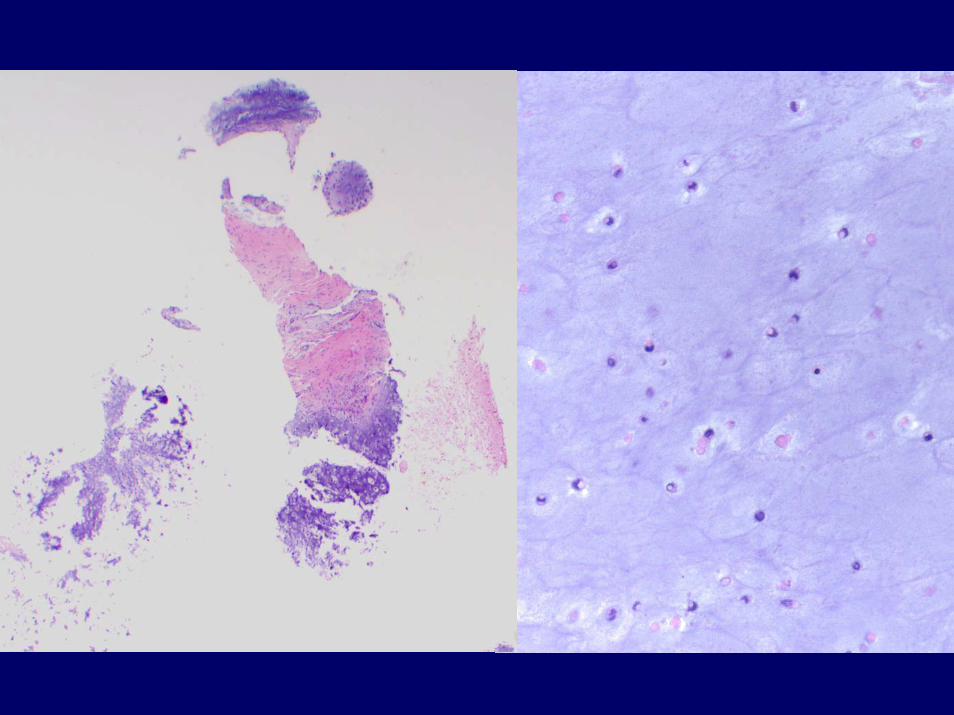
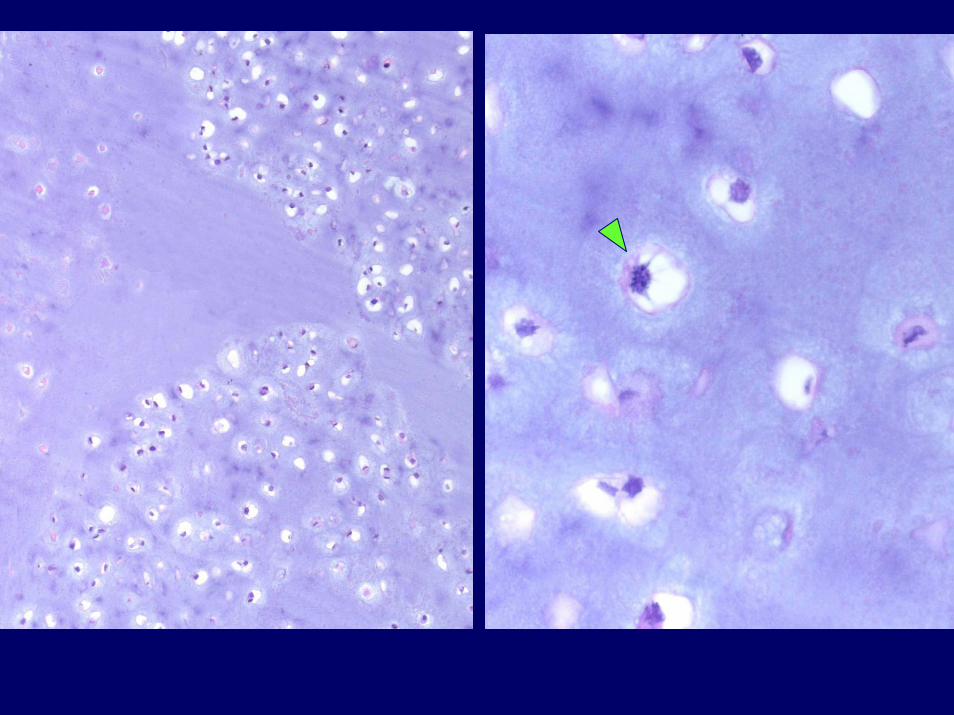

Enchondroma or Grade I chondrosarcoma?
• Enchondroma: “Multiple nodules of hyaline cartilage separated by normal marrow (and) plates of lamellar bone that conform to the irregular shapes of cartilage lobules.”
• Chondrosarcoma: “Single confluent mass of cartilage… trapping host lamellar bone or invasion into Haversian or Volkman systems.”
- J. Mirra (1985)
• Pitfalls– Small biopsy– Curettage– Small bones of hands and feet
Mirra JM et al. Clin Ortho Rel Res 1985 201:214-237
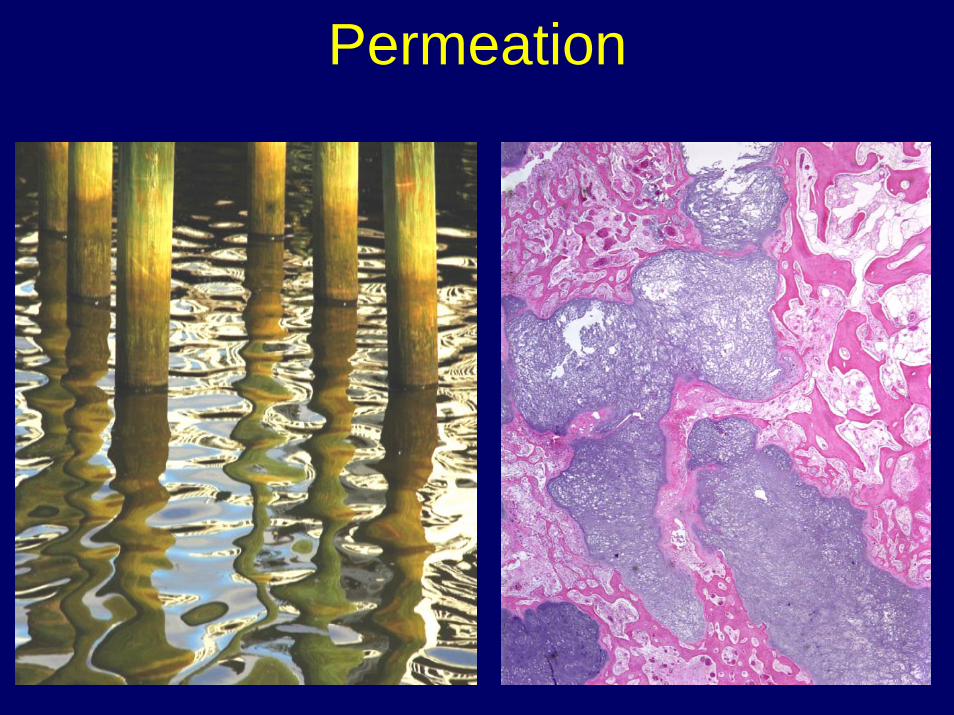
Permeation
Enchondroma or Grade I chondrosarcoma?
• “Diagnosis should be based on what the tumor is doing to the patient” - Dr. Kempson– Progression over time– Radiology
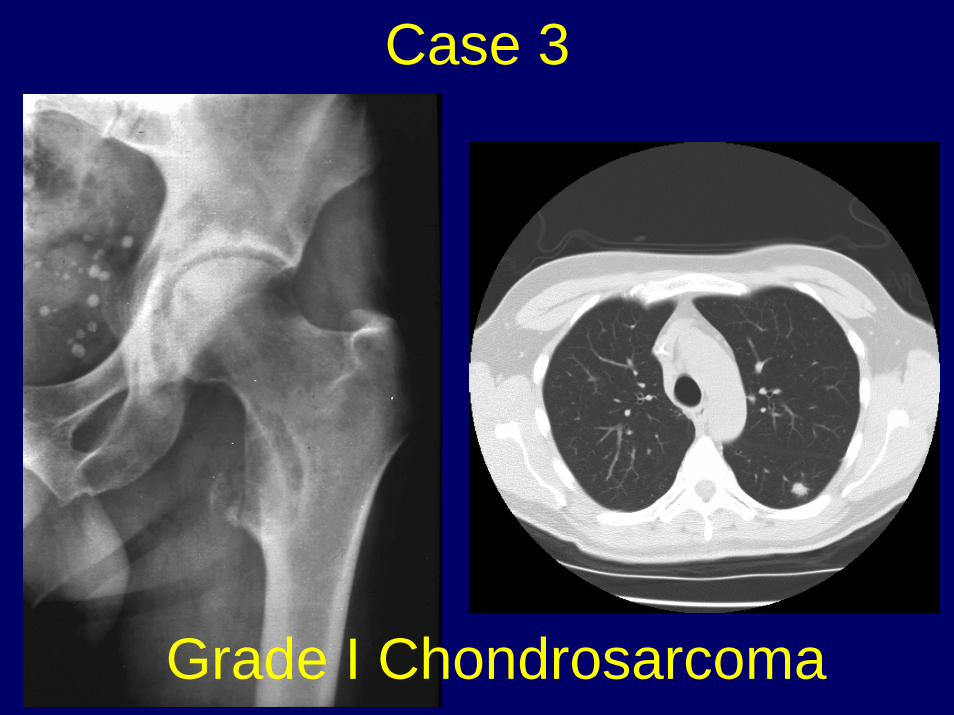
Case 3
Grade I Chondrosarcoma
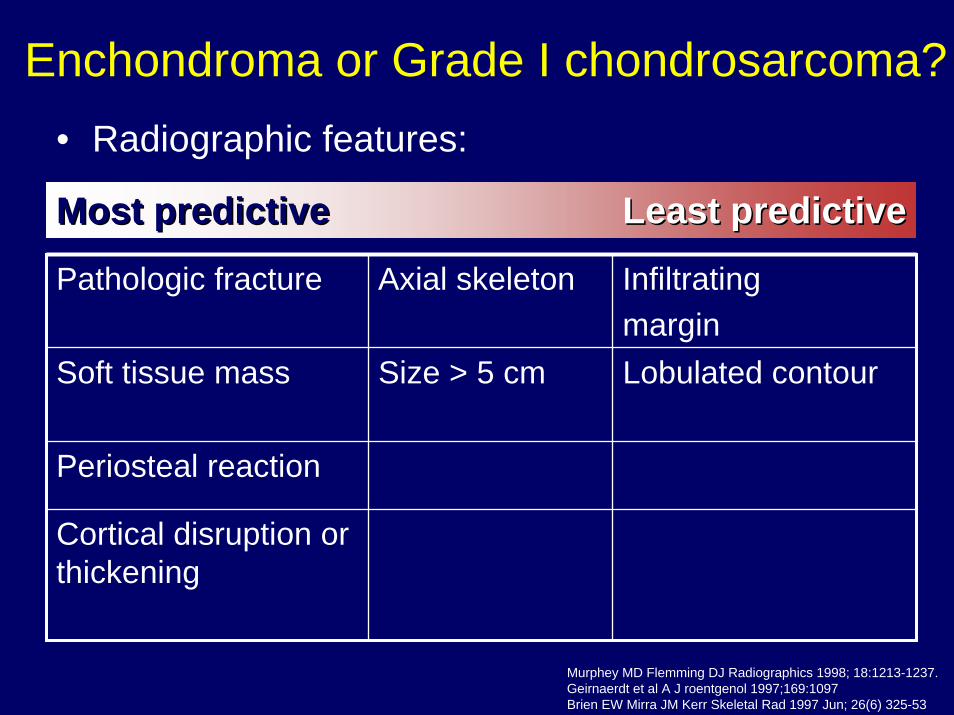
Enchondroma or Grade I chondrosarcoma?• Radiographic features:
Most predictiveMost predictive Least predictiveLeast predictive
Pathologic fracture Axial skeleton Infiltratingmargin
Soft tissue mass Size > 5 cm Lobulated contour
Periosteal reaction
Cortical disruption or thickening
Murphey MD Flemming DJ Radiographics 1998; 18:1213-1237.Geirnaerdt et al A J roentgenol 1997;169:1097Brien EW Mirra JM Kerr Skeletal Rad 1997 Jun; 26(6) 325-53
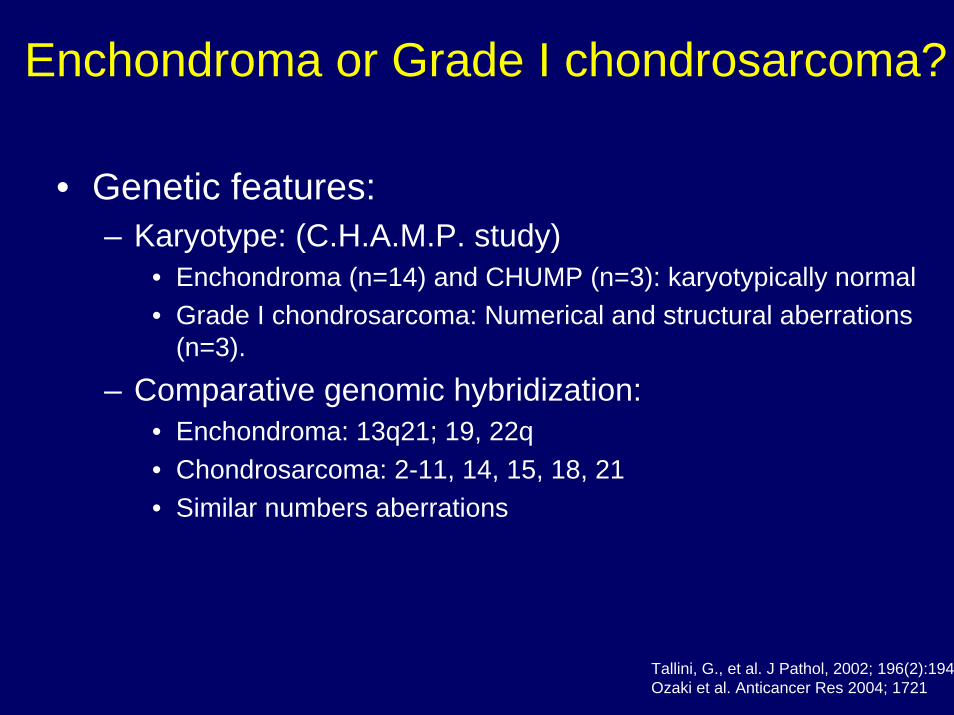
• Genetic features:– Karyotype: (C.H.A.M.P. study)
• Enchondroma (n=14) and CHUMP (n=3): karyotypically normal• Grade I chondrosarcoma: Numerical and structural aberrations
(n=3).
– Comparative genomic hybridization:• Enchondroma: 13q21; 19, 22q• Chondrosarcoma: 2-11, 14, 15, 18, 21• Similar numbers aberrations
Enchondroma or Grade I chondrosarcoma?
Tallini, G., et al. J Pathol, 2002; 196(2):194Ozaki et al. Anticancer Res 2004; 1721
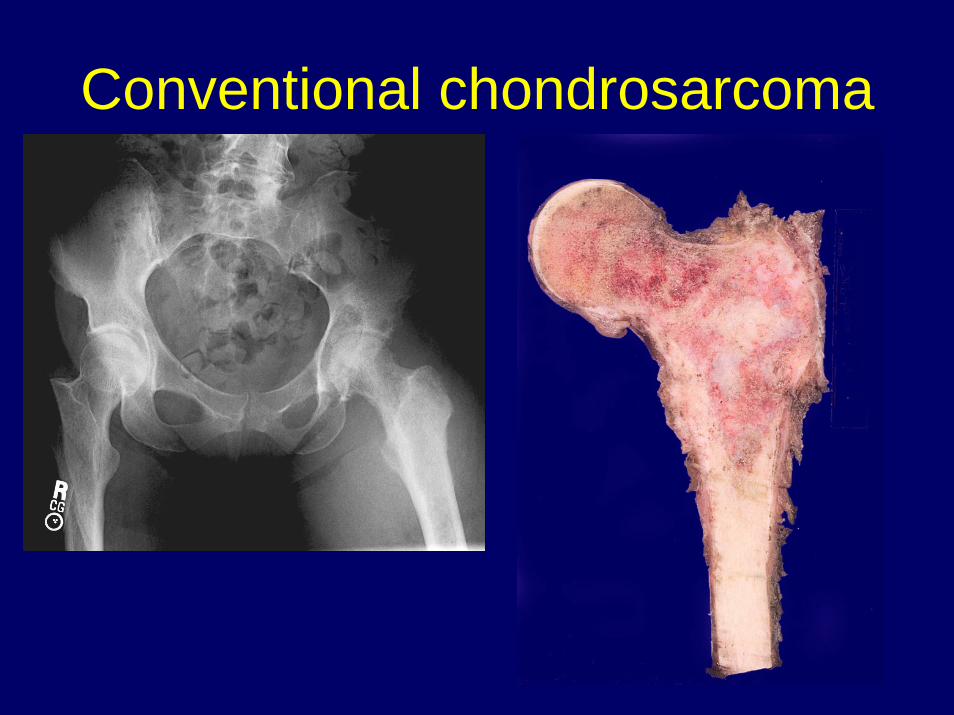
Conventional chondrosarcoma

Conventional chondrosarcomaClinical Radiology Histology Ddx
Age: 50+Loc:
Central: pelvis, meta-diaphysis long bones
Peripheral: osteochondroma
Large (> 5 cm)Cortical disruptionEndosteal scallopingSoft tissue extensionRing calcifications
Permeates viable, lamellar boneHypercellularMyxoid changeAtypia NecrosisMitoses
EnchondromaClear cell chondrosarcomaChondroblastic OGS
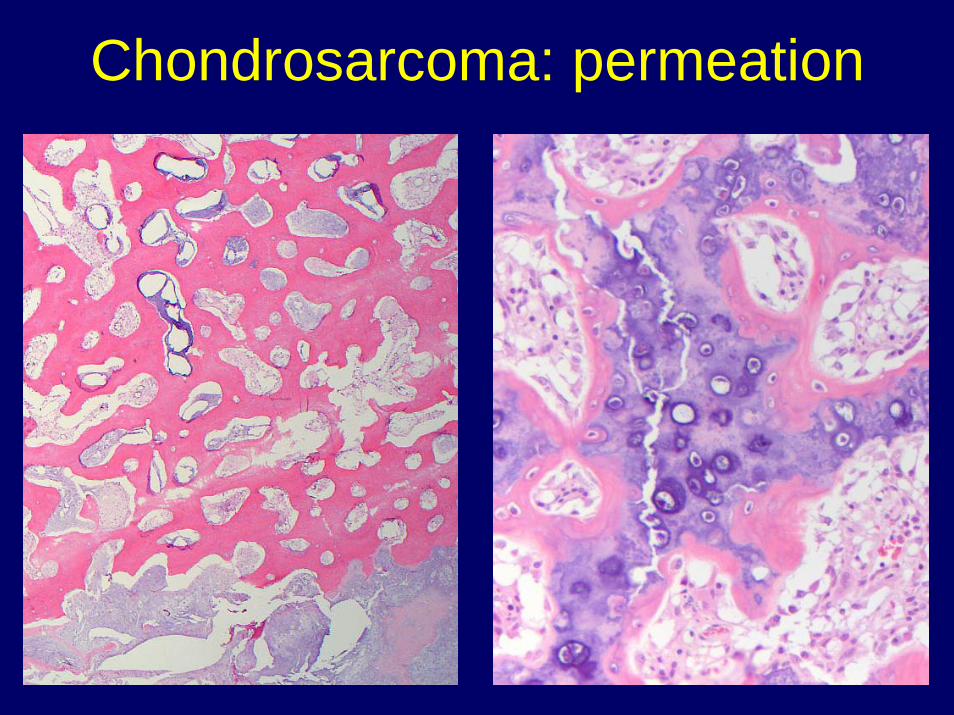
Chondrosarcoma: permeation
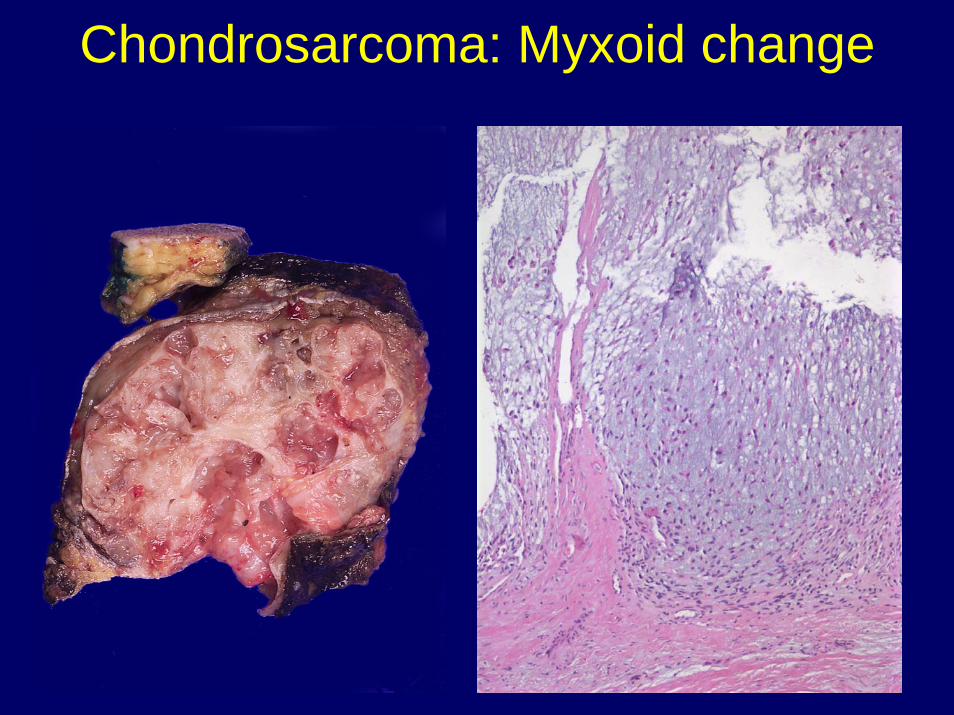
Chondrosarcoma: Myxoid change

Chondrosarcoma: GradingPROGNOSTIC FACTORS IN CHONDROSARCOMA
OF BONE A Clinicopathologic Analysis with Emphasis on Histologic Grading
HARRY L. EVANS, M.D.* ALBERTO G. AYALA, MD
AND MARVIN M. ROMSDAHL, MD, PHD
Cancer 40:818-831, 1977.
Histology 5 year survival
10 year survival
90
81
43
Grade I Hypercellular, uniform but hyperchromatic nuclei, nuclear detail not visible
83
Grade II Diffusely hypercellular, nuclei paler with visible intranuclear detail
64
Grade III Sheets of cells, larger nuclei, mitotic activity > 2mf/10 hpf
29
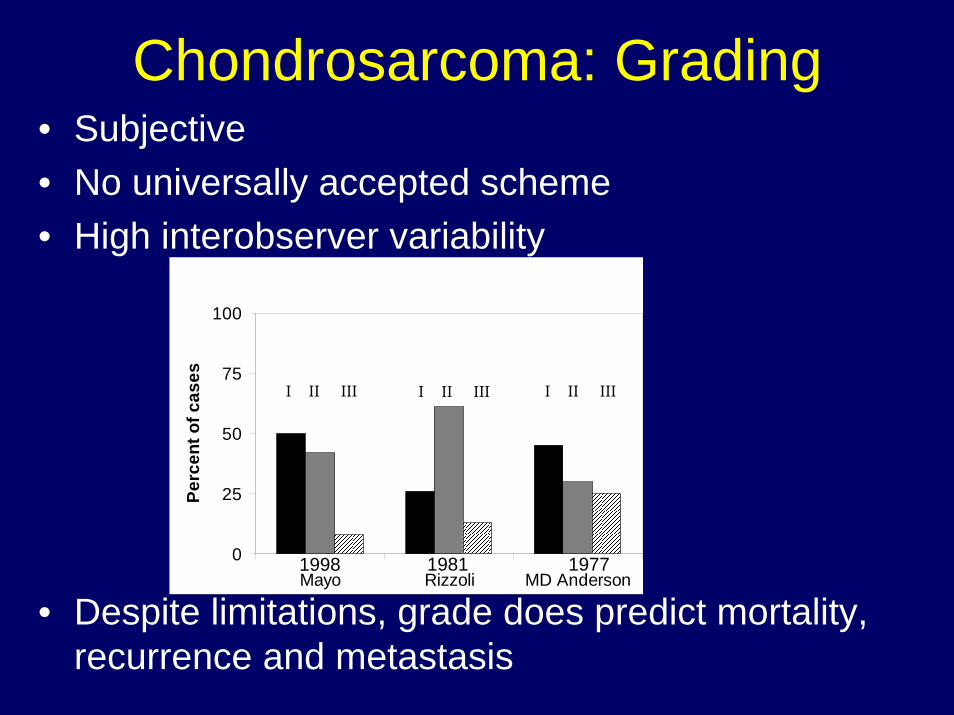
Chondrosarcoma: Grading• Subjective• No universally accepted scheme• High interobserver variability
• Despite limitations, grade does predict mortality, recurrence and metastasis
0
25
50
75
100
Mayo Rizzoli MD Anderson
Perc
ent o
f cas
es
I II III I II III I II III
1998 1981 1977
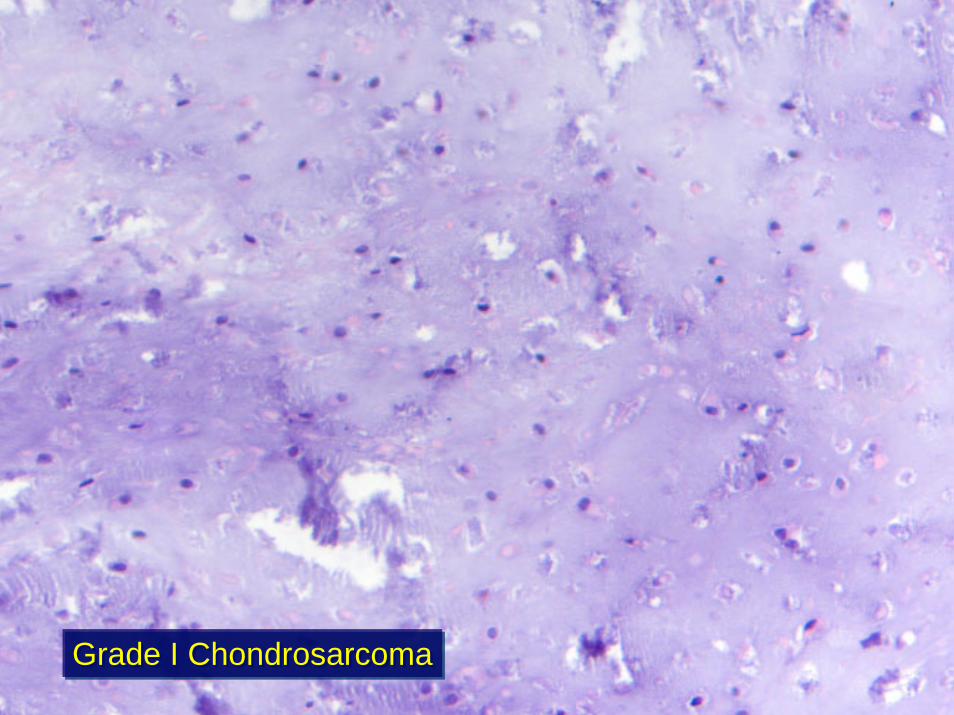
Grade I ChondrosarcomaGrade I Chondrosarcoma
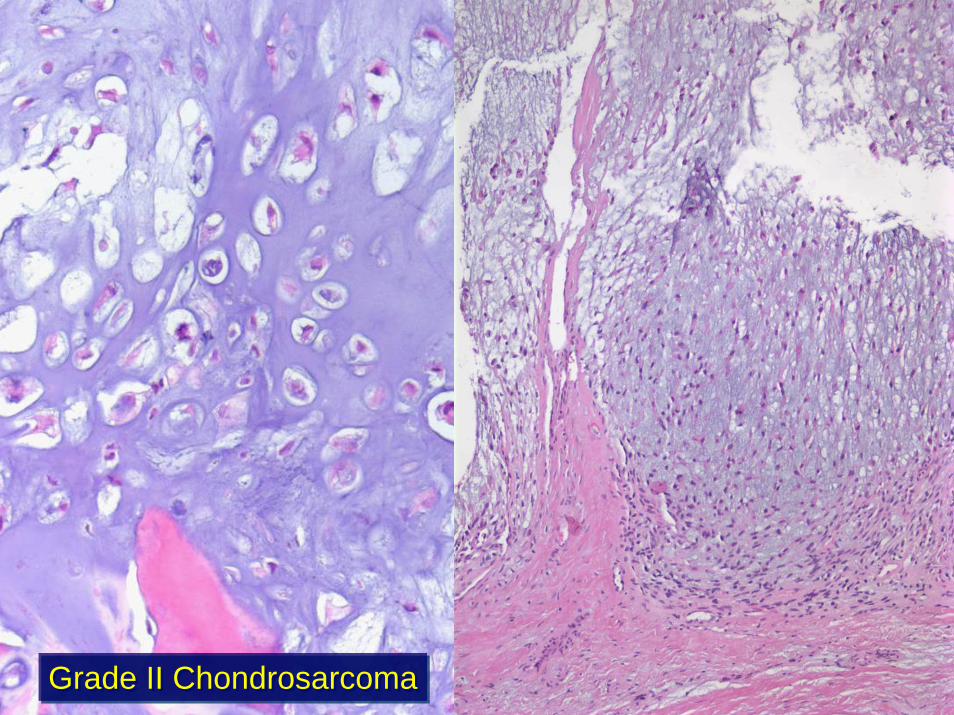
Grade II ChondrosarcomaGrade II Chondrosarcoma
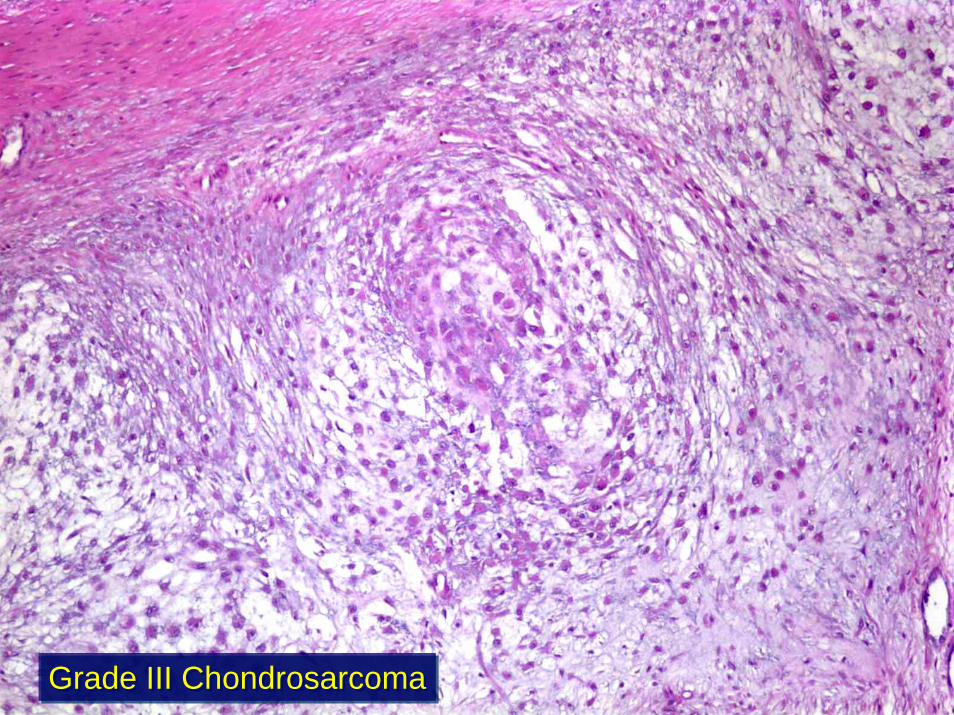
Grade III ChondrosarcomaGrade III Chondrosarcoma
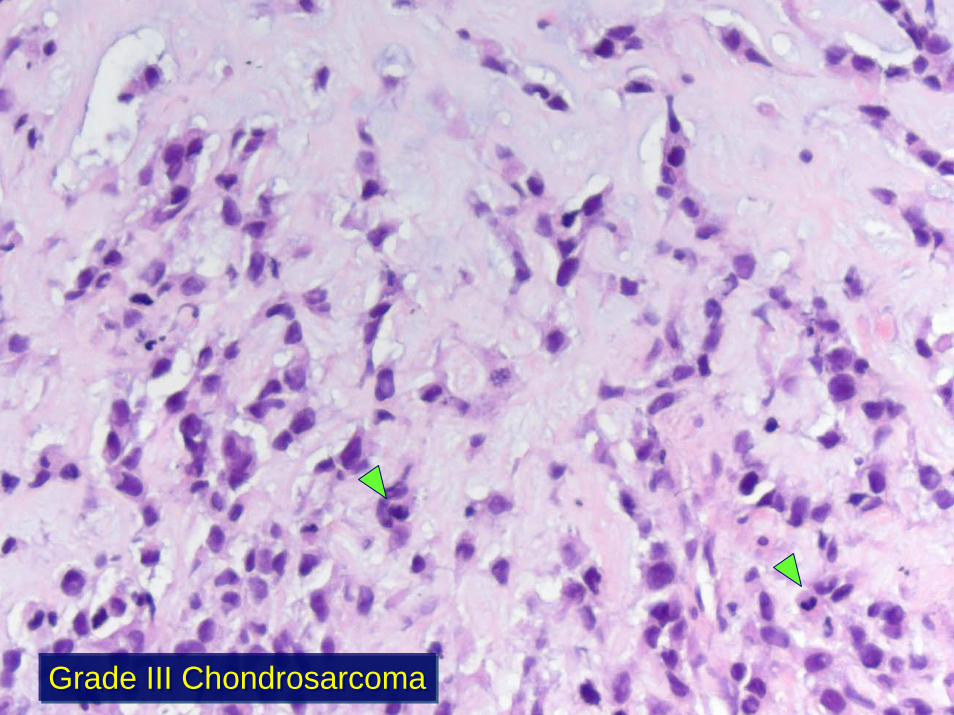
Grade III ChondrosarcomaGrade III Chondrosarcoma

Chondrosarcoma of small bones of hands and feet
• Enchondromas of hands and feet– Clinical: Very common site (~30%), painful,
pathologic fracture common– Radiographs: Cortical erosion common– Histology: Hypercellular, myxoid change,
nuclear hyperchromasia, permeation within medulla
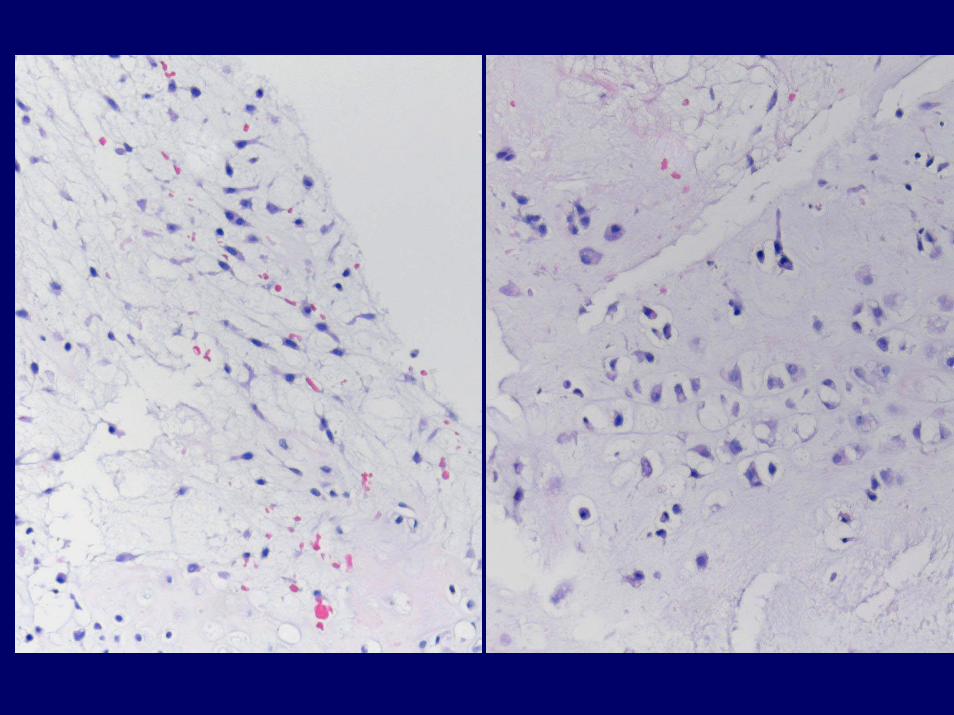
• Mayo Clinic: (n=163) 12/70 metastasized– Radiographs: Permeative pattern, cortical
destruction, soft tissue mass– Histology: Permeation through cortex into soft
tissue (“sweating”)• Baylor (n=15) 0/8 metastasized.• Leiden (phalanges only, n=35) 0/28
metastasized
Chondrosarcoma of small bones of hands and feet
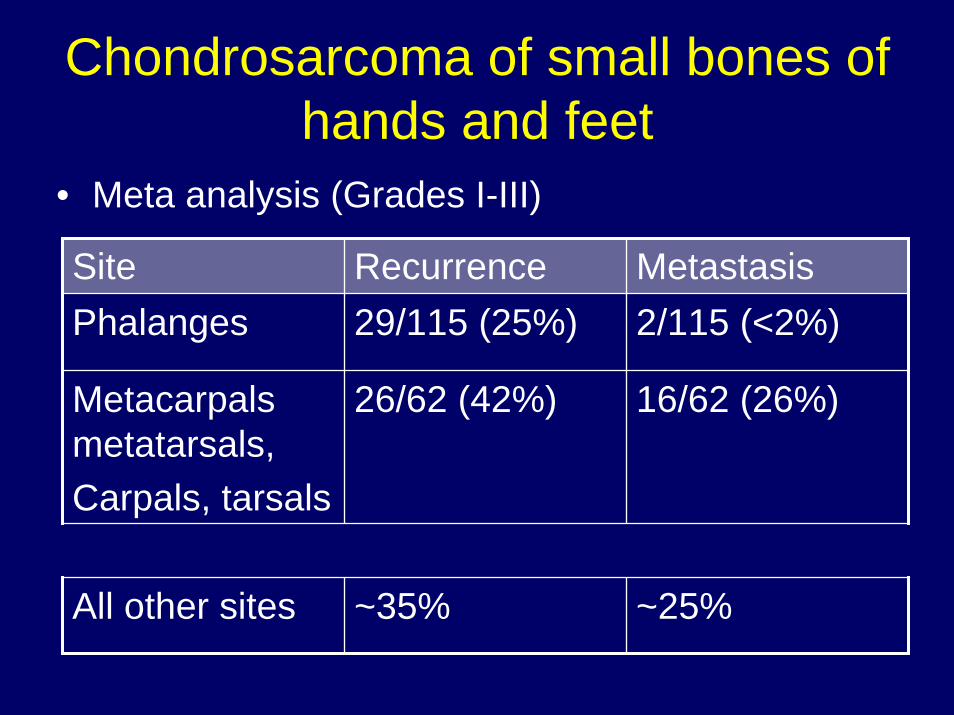
• Meta analysis (Grades I-III)
Site Recurrence MetastasisPhalanges 29/115 (25%) 2/115 (<2%)
Metacarpals metatarsals,Carpals, tarsals
26/62 (42%) 16/62 (26%)
All other sites ~35% ~25%
Chondrosarcoma of small bones of hands and feet
• Metacarpals, metatarsals, wrist and ankle:– Diagnosis requires either grade III cytology if
equivocal radiology or evidence of soft tissue involvement
• Phalanges:– Probably does exist but with a metastatic rate
that is very low– Local resection is favored over amputation
whenever possible.
Summary: chondrosarcoma of small bones of hands and feet

Case 4
• 44 year old man• Thigh pain for 3 years
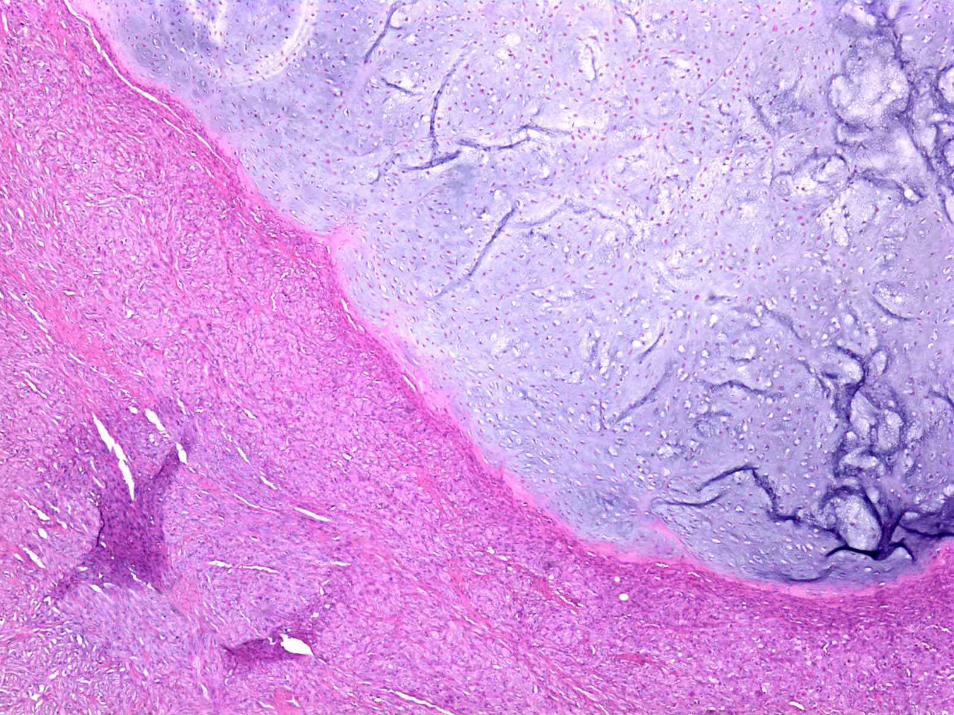
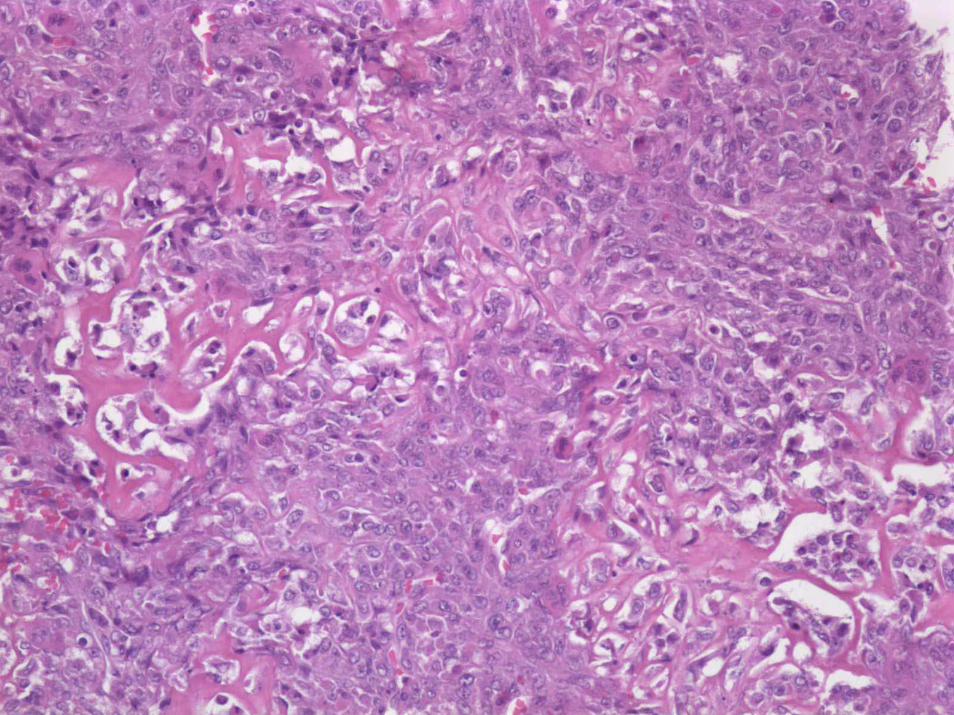
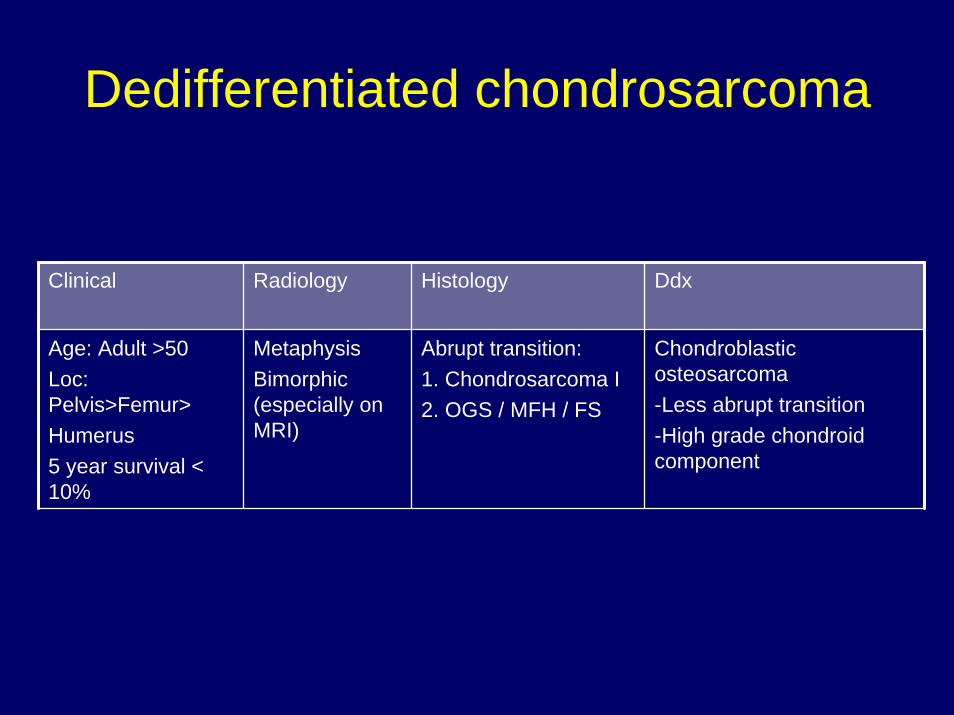
Dedifferentiated chondrosarcoma
Clinical Radiology Histology Ddx
Age: Adult >50Loc: Pelvis>Femur>Humerus5 year survival < 10%
MetaphysisBimorphic (especially on MRI)
Abrupt transition:1. Chondrosarcoma I2. OGS / MFH / FS
Chondroblastic osteosarcoma-Less abrupt transition-High grade chondroid component
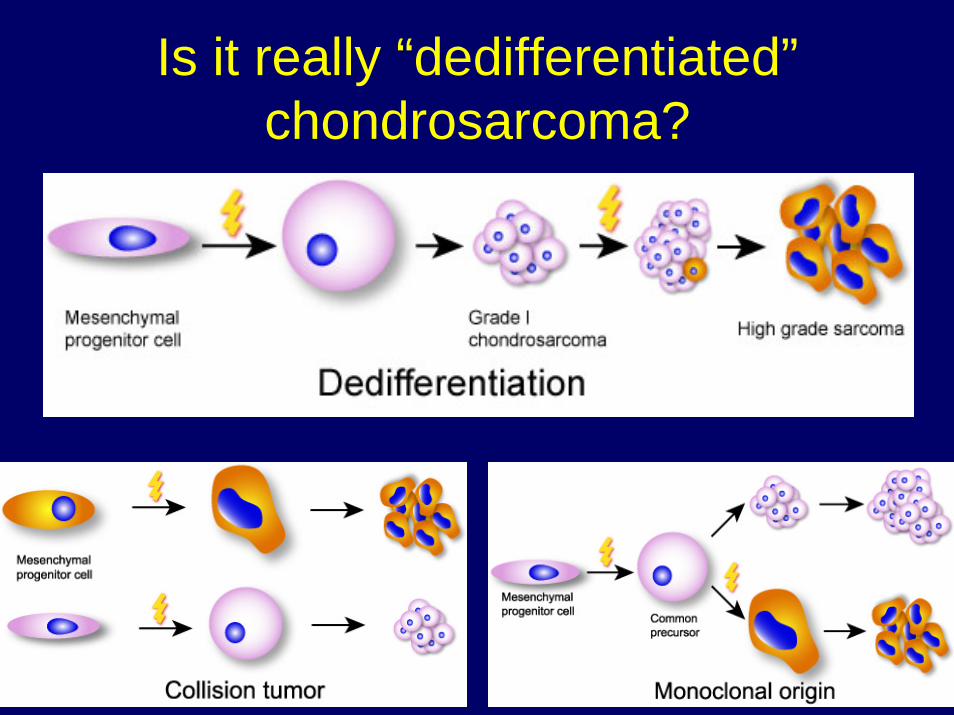
Is it really “dedifferentiated”chondrosarcoma?
Take-home messages• Correlation of radiologic, clinical and histologic features
critical, especially in low-grade lesions• Permeation is the most sensitive histologic criterion
separating enchondroma from chondrosarcoma.• Chondrosarcoma of small bones of the hands and feet
should be diagnosed with caution. • Grade is most important prognostic indicator for
chondrosarcoma• Chondrosarcomas are predominantly locally aggressive,
but local disease can be fatal even in the absence of metastases
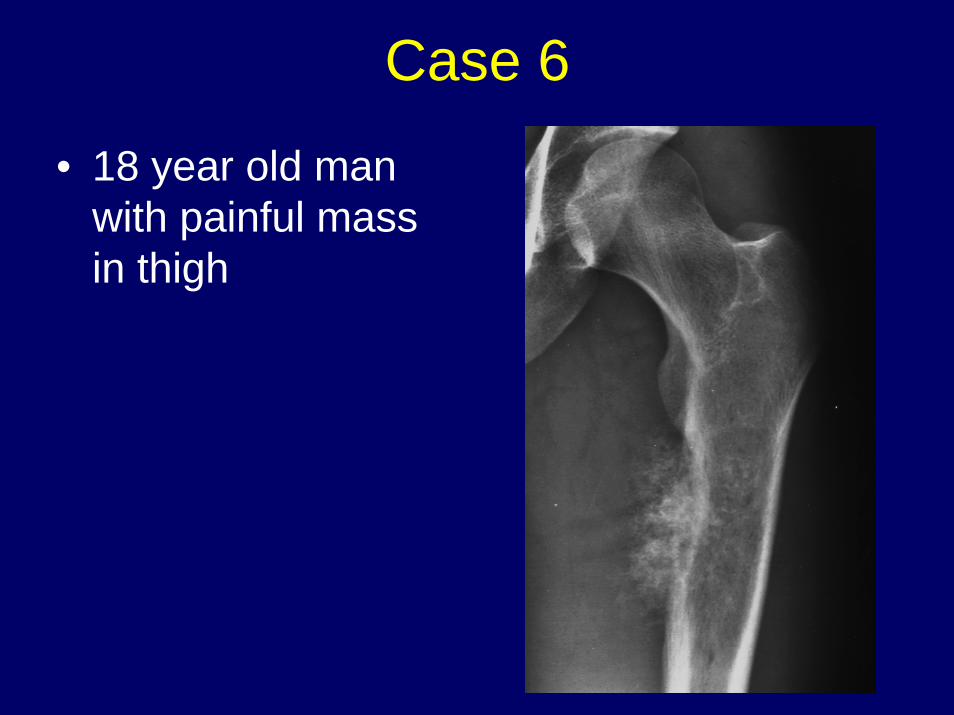
Case 6
• 18 year old man with painful mass in thigh
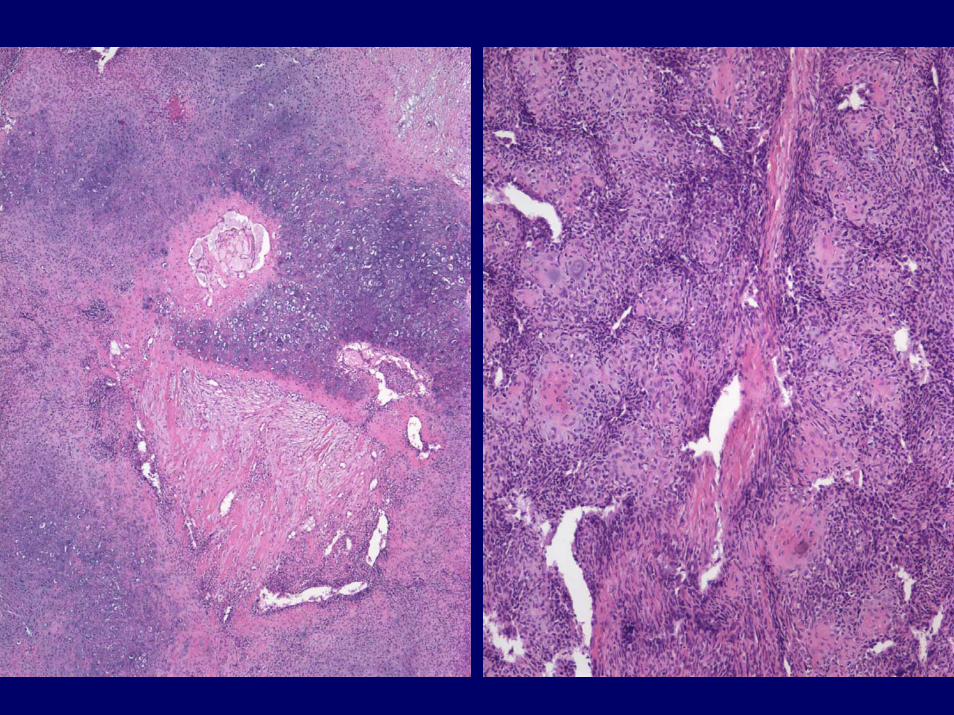
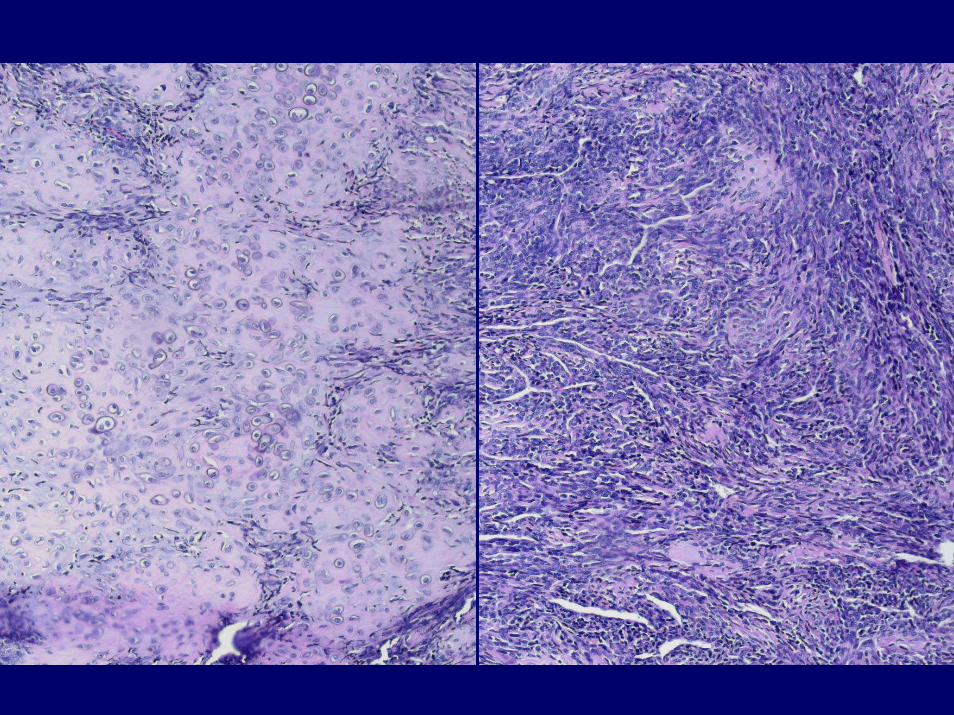
Mesenchymal chondrosarcomaClinical Radiology Histology Ddx
Age: 20-30Loc: Jaw, rib, pelvis, soft tissueMultifocal
10yr survival 25% Variable course
LyticRing calcificationsRarely circumscribed
1. Benign cartilage islands/perivascular2. Small round blue cell tumorHPC-ish vessels common
Ewing sarcoma (CD99)Dediff chondrosarc (abrupt)Small cell osteosarcoma

Case 4
• 28 year old man with shoulder discomfort

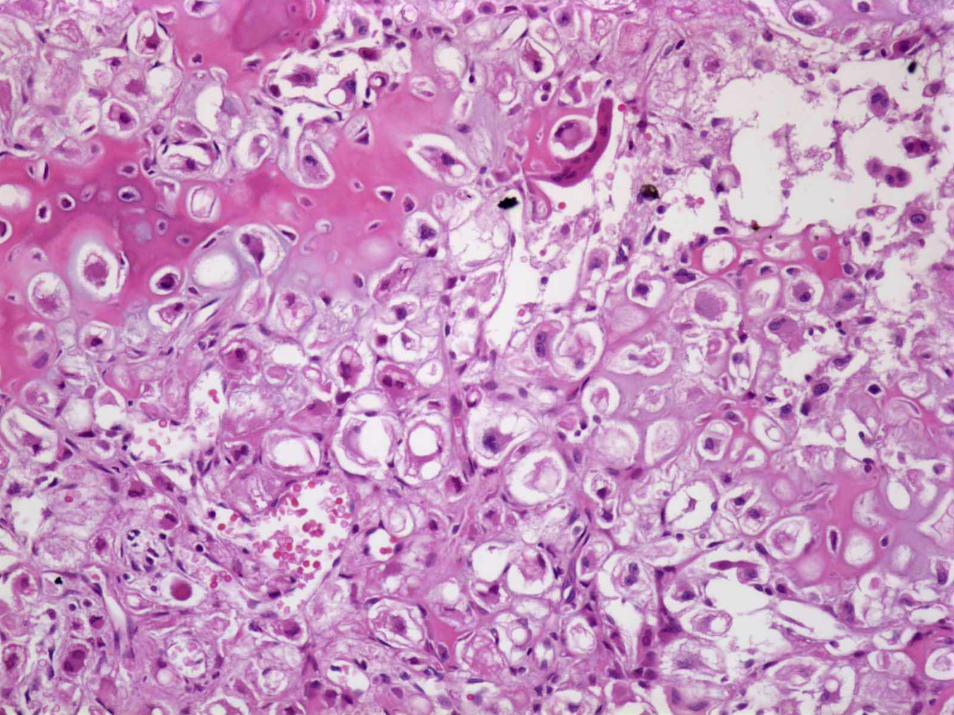
Clear cell chondrosarcomaClinical Radiology Histology Ddx
Age: 25-50 M>FLoc: Proximal femurSkull, rib, spineSlow growing~25% Metastasize~15% mortality
EpiphysisCircumscribedEarly: lytic, septaeLate: sclerotic
Permeates Osteogenic “No” hyaline cartilageClear cells, well defined membrane, macronucleoli (S100+)
Chondroblastic osteosarcomaOsteoblastoma
Chondroblastoma (radiology Ddx)