2007 annus.med.hbs+jmg 13.08.08
TRANSCRIPT



CONTENTS
FROM THE MEDICAL DIRECTOR OF HEALTH 5
I. THE DIRECTORATE OF HEALTH ............... 7
II. CLINICAL QUALITY – PATIENT SAFETY....10
III. COMMUNICABLE DISEASE CONTROL.... 15
IV. HEALTH STATISTICS ................................ 19
V. COMPLAINTS ............................................. 22
VI. PUBLIC HEALTH AND PRIMARY CARE... 23
VII. PUBLICATION ............................................ 25
ANNUS MEDICUS 2007
ICELAND
EXTRACT FROM THE ANNUAL REPORT OF
THE DIRECTORATE OF HEALTH 2007

Annus Medicus 2007 Directorate of Health Published by: Landlæknisembættið Austurströnd 5 170 Seltjarnarnes Iceland 2008 Editor: Jónína Margrét Guðnadóttir [email protected]

5
F R O M T H E M E D I C A L D I R E C T O R O F H E A L T H
Discussion of health matters in Iceland has been increasingly promi-nent in recent months and years. However, in-depth discussion, with ideas and proposals con-cerning policy and the future, has been less prominent. Hopefully, we will see changes in this regard. The most heated argument in-volves the outward as-
pects of the service, such as corporate form and working environment. The actual purpose of the service tends to get lost in the discussion, namely caring for the sick and improving public health. In comparison with other countries it is obvious that Icelanders enjoy good health. It sometimes appears that we do not appreciate this as we should. To be sure, numerous problems remain unresolved in the fields of welfare and education. Examples include the problems of the mentally disabled, the elderly, drug abusers and excessive relative poverty, to name only a few. It is difficult to appreciate fully the welfare in Iceland until one gets the opportunity to experience at close quarters the situation in the poorer regions of the world, such as Sub-Saharan Africa and South-East Asia. Living and working in circumstances of this kind for a while, as I have had an opportunity to do over the past year, is more enlightening than anything else as regards the un-equal division of resources in the world we live in and how much we can and should contribute to de-veloping countries. In that respect we could do much better. A new Medical Director of Health Act entered into force in September 2007 together with a new Health Service Act. The Directorate’s tripartite role,
i.e. advising, processing information and improving and monitoring quality, is provided for in detail in the act, as further discussed in the next chapter. In line with the new legislation, efforts are now being made to clarify the division of roles in health ad-ministration, with several tasks being transferred from the Ministry of Health to the Directorate of Health. Geriatric affairs were transferred at the close of the year to the Ministry of Social Affairs, with the exception of health services for the elderly, which will continue to be the responsibility of the Ministry of Health. The new organisation of geriatric affairs will hopefully prove to be an improvement. From the point of view of recipients, continuity and har-monisation of the services are extremely important. Sometimes we tend to organise services more on the basis of the needs of the providers than the patients. Registration of health data. The Directorate regularly issues two newsletters, Farsóttafréttir (a newsletter on communicable diseases, the English version of which is EPI-ICE) and Talnabrunnur (a newsletter in Icelandic on health statistics). These publications form a part of the regular dissemina-tion of information concerning the nation’s health. Electronic registration in the health services is be-ing enhanced, electronic patient journals being the cornerstone of all registration of national health data. Good progress has been made in developing the arrangements of data collection from hospitals and the primary health care, and the admission of data from hospitals and the contact database of the pri-mary health care are now exemplary. However, information from self-employed specialists is still limited.

6
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
the working facilities and working environment in the health services and on the other hand wages and employment terms. It should be noted that inadequate manning represents a threat to quality of service and patient safety. Public health. The University of Iceland and Reykjavik University now both have faculties of public health, and extensive research in that field is among the prerequisites of progress and increased knowledge. It should be kept in mind, however, that public health is the responsibility of the entire community, and so it should remain. Public health and discussion of public health cannot be separated from other health services. The two must go hand in hand.
Quality development. In essence, the moni-toring function of the Directorate of Health fo-cuses on the enhancement of service quality. Specific quality indicators have been defined, which also serve as measures of health services and health trends, and work is in progress on developing minimum service quality require-ments. Until now, attention has predominantly been focused on competition for lower costs, when the focal point should be the quality and results of the service. Shortage of human resources. The shortage of nurses is acute and the limited recruitment in their ranks is a matter of concern. This problem is even greater in the case of nursing assistants. Nurses point out two reasons: on the one hand
Sigurður Guðmundsson Medical Director of Health

7
Changes in framework and administration A milestone was passed in 2007 with the enact-ment of special legislation on the Medical Director of Health, Act No. 41/2007, which entered into force on 1 September 2007. Provisions relating to the Medical Director of Health and the Directorate used to form part of the Health Service Act and a separate government regulation, but in the course of the revision of the Health Service Act it was con-sidered necessary to enact a separate code on the Directorate of Health.
The Act contains more precise provisions on the status and role of the Directorate of Health as a monitoring and administrative organisation, includ-ing the task of the Medical Director of Health of maintaining professional surveillance of the opera-tion of health services and various aspects of the work of health care practitioners, including the pre-scription of medicinal products. The Act also con-tains provisions on the role of the Medical Director of Health in gathering data and preparing reports in the field of health and on the required recording and reporting of health care facilities and health care professionals in the case of any incidents in the course of providing health services. Further-more, the Act contains provisions on the responsi-bilities of the Medical Director of Health in quality development in the health services. A new feature of the legislation is that parties intending to launch the operation of a health service are required to notify the Directorate of Health, which will then confirm whether the service meets the minimum professional standards for the operation of health services set by the Directorate.
Concurrently with the entry into force of the new act three new regulations were signed: a regulation on health districts, a regulation on the Directorate of Health’s monitoring of the operation of health services and minimum professional standards and,
finally, a regulation on primary health care centres. Additionally, a new Act amending the Communica-ble Diseases Act No. 43/2007 entered into force in March 2007, widening the scope of the replaced legislation, as well as two government regulations, as further discussed in Chapter III. Finally, a new Health Service Act entered into force on 1 Septem-ber, supplanting earlier legislation, the bulk of which dated back to 1973. All these changes effec-tively constitute a virtual transformation of the regulatory framework of the Directorate of Health.
For most of the year Dr. Matthías Halldórsson, who has held the post of Deputy Medical Director of Health for several years, served as acting Medical Director of Health in the absence of the appointed Medical Director of Health, Dr. Sigurður Guðmunds-son, who took a one year’s leave of absence while working in Malawi in the service of the Icelandic International Development Agency (ICEIDA). Dr. Guðmundsson returned to his former post at the end of October.
The current organisation chart for the Directorate of Health was introduced at the beginning of 2006. According to the chart, the activities of the Direc-torate are divided into four professional and admin-istrative divisions. Each division is headed by a gen-eral manager who, together with the Medical Direc-tor of Health and the Deputy Director of Health, form the Executive Board of the institution.
Employees In the course of the year, the Directorate of Health had 34 employees, nine men and 25 women, in just short of 26 full-time equivalent positions, in addition to three contractors and a few temporary employees.
I . T H E D I R E C T O R A T E O F H E A L T H

8
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
design of the website was concluded and the site was re-launched with a new appearance and layout on 30 March. In addition to the thorough face-lift, all the contents of the website have been revised. Two working groups within the Directorate were responsible for the revision of the website under the supervision of the webmaster. In addition, vir-tually the entire staff played some part in the pro-ject. Information to the public concerning health issues and diseases In September the Directorate opened access on its website to health information for the general public concerning various diseases and minor health is-sues. The website now features a selection of links to international and Icelandic data on the Internet, selected by the Directorate on the basis of certain professional guidelines. Influensa.is On 7 December an independent web site, www.influensa.is, was launched on the Director-ate’s web site for the purpose of educating and informing the general public and professionals about seasonal and avian influenza and the poten-tial influenza pandemic. This web site is a joint undertaking of the Chief Epidemiologist, the Civil Protection Department of the National Commissioner of the Icelandic Police, the Icelandic Food and Veterinary Authority and the Environment Agency, the organisations that need to co-ordinate their actions in the event of an influ-enza pandemic.
Meetings and events hosted by the Director-ate of Health The Directorate of Health sponsored 17 confer-ences, meetings, courses and other events during 2007, either alone or in partnership with other insti-tutions and organisations.
Visits The Minister of Health and Social Security, Guðlau-gur Þór Þórðarson, visited the Directorate of Health in September with his assistant and the Secretary General of his Ministry for the purpose of acquaint-ing himself with the activities and role of the Direc-torate of Health, especially with regard to the points of focus in the new legislation on the Medical Director of Health.
Nearly a third of the employees of the Directorate of Health took part in the campaign “Let’s cycle to work”, organised by the National Olympic and Sports Association of Iceland. Members of the team travelled over 400 km during the campaign, which lasted just over two weeks.
Activities in 2007 Formal reports on bills and regulations The Directorate of Health gives opinions on parlia-mentary bills and proposals for parliamentary reso-lutions which concern health issues and other is-sues within the scope of the Directorate. The Direc-torate is also asked to comment on government regulations. In 2007, this aspect of the Director-ate's work was unusually extensive, as substantial reforms were made to laws and regulations in the course of the year as outlined above. Information and Education Activities General educational role Education and lectures form a part of the work of some of the Directorate’s employees, as well as the supply of information to the media. The Director-ate’s employees are also involved in the formal in-struction of various groups and professions, par-ticularly in the health services, both in the course of their regular studies at universities and other edu-cational institutions and in courses organised by the Directorate itself. Redesign of the Directorate’s website A large part of our educational and promotional activities consists in the operation of an informa-tional website at www.landlaeknir.is. The impor-tance of the website as a channel for information from the Directorate is growing continually, and there has been a steady increase in visits in recent years. At the beginning of the year a complete re-

9
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
amounting to ISK 2,500,000, which will in part be used for the survey. Study of the health of Icelanders Late in 2007, an extensive study was carried out relating to the health, wellbeing and welfare of Ice-landers from 18–79 years of age. The study cov-ered 10,000 randomly chosen participants. It was carried out by the Public Health Institute of Iceland in collaboration with the Directorate of Health and other parties. Studies based on the Pharmaceuticals Data Bank (PDB) A study was conducted on the use of methylpheni-date (Ritalin and related medicinal products) in chil-dren in Iceland from 1989–2006 and the results were published in the Icelandic Medical Journal (Læknablaðið). Another study, based on the PDB and other data, was carried out to demonstrate the increased risk of cardiovascular disease in individu-als using the pharmaceutical rofecoxib or Vioxx. Collaboration with the University of Iceland In October 2006 a collaboration agreement was signed between the Directorate of Health and the University of Iceland concerning teaching and re-search at the newly founded Faculty of Public Health Sciences at the University of Iceland. The purpose of the agreement is to enhance co-operation between the two organisations in order to make the best possible use of the expertise, re-sources and facilities available.
International co-operation The Directorate of Health co-operates extensively with organisations and associations in the Nordic countries, Europe and internationally. The Director-ate participates in the work of the World Health Organisation (WHO) in addition to various interna-tional collaboration projects where representatives of the Directorate participate in the relevant work-ing groups and committees. There is an established tradition of collaboration with corresponding or-ganisations in the Nordic countries and co-operation with institutions of the EU is also quite extensive. A meeting of the Nordic Medical Directors of Health was held in Sigtuna in Sweden on 21–23 August 2007, and on 20–21 September a Nordic meeting on medical devices was held in Iceland. Further-more, the Directorate participates in Nordic co-operation on quality indicators.
A view of the crowded hall during the Directorate’s symposium on patient safety at Hotel Nordica in February. In addition to over 200 participants, nearly 300 people followed the events of the symposium through direct webcasting. As always, various foreign guests visited the Direc-torate. Visitors arrived from Health Canada, the United Kingdom, Sudan, the Czech Parliament, the European Centre for Disease Prevention and Con-trol in Stockholm, nurses from Scotland and schol-ars from the University of Minnesota. Every year, the Directorate’s employees also visit various local institutions, either to conduct their regulatory monitoring of health care facilities or to familiarise themselves with their activities as needed. Monitoring visits were paid to 16 institu-tions, in addition to visits to other institutions for informational purposes.
Collaboration on research and education HOUPE study Collaboration on the HOUPE study (study of Health and Organisation among University Physicians in four Eurpean countries) in Iceland was continued in 2007. Our collaborators in Norway, Sweden and Italy are currently processing data from the first part of the study and are aiming for the preparation of its second part. A more detailed description of the HOUPE Study is available on the project web-site (see http://www.houpe.no). Processing of the study in Iceland progressed well during the year. Survey of services to women with breast conditions The Directorate of Health assumed the role of con-sultant in a study called “Future vision of women diagnosed with breast conditions and their relatives of desirable specialised services.” At the beginning of 2007 the survey received a grant from the Budget Committee of the Icelandic parliament

10
The Directorate of Health emphasises the enhance-ment of quality and safety in the health services. In 2007, the Directorate, together with the Ministry of Health and Social Security, published the Quality Policy of the Health Authorities to the Year 2010, which focuses on projects pertaining to the health authorities rather than the formal quality develop-ment of individual health care facilities. The new quality policy is based, among other things, on the objectives of the Icelandic National Health Plan to the year 2010 and the guidelines of the World Health Organisation, with further reference to the quality policy of health authorities in the other Nor-dic countries. Patient safety is the main focus of the revised quality policy. Safety in the health services Symposium on patient safety The Directorate hosted a symposium on safety in the health services on 8 February. Sir Liam Donaldson, the UK Chief Medical Officer and man-
ager of a WHO project titled World Alliance for Patient Safety, attended the symposium as a guest and keynote speaker. At the symposium Siv Friðleifsdóttir, the Minister of Health at the time, signed an agreement on Iceland’s partici-pation in an international project titled “Clean Care is Safer Care”. This placed Iceland in the ranks of approximately 50 other states who have undertaken to implement measures to reduce the frequency of infections in the health services.
Research and recording of incidents in the health services No information is available on the frequency of unforeseen adverse events in the Icelandic health services, but by extrapolating from the results of foreign studies, some 50–100 inci-dents of this kind may be estimated to prove fatal in the national health services every year.
The Directorate of Health has participated in studies of safety practises in the health system in co-operation with Landspitali University Hos-
pital (LUH) and the Faculty of Nursing of the University of Iceland, focusing on nurses and nursing assistants at LUH to-gether with professionals from the same groups at the surgical and medical wards of four Icelandic hospitals.
Advisory board on patient safety The Directorate of Health is advised by an advisory board on patient safety, which was appointed late in the year 2006. In addition to representatives from the Direc-torate itself, the members include repre-sentatives of Landspitali University Hospital, one health institution outside the capital area, the primary health care service and a geriatric institution.
I I . C L I N I C A L Q UA L I T Y A N D PA T I E N T S A F E T Y
From the symposium on patient safety. Sir Liam Donaldson, UK Chief Medi-cal Officer and manager of the project World Alliance for Patient Safety, attended the symposium as a guest and keynote speaker. From the left: Sir Liam Donaldson, Matthías Halldórsson, Anna Björg Aradóttir and Laura Scheving Thorsteinsson.

11
DIRECTORATE OF HEALTH ANNUS MEDICUS 2007
Clinical quality Quality indicators In recent years there has been increasing emphasis on the use of quality indicators as a measure for monitoring and assessing the quality of health care services. These indicators are also used internation-ally to compare health services provided in different institutions and different countries and to increase transparency. The Nordic Council of Ministers has appointed two working groups on quality indica-tors; the first submitted its report in 2003 and the second in 2007. The Directorate of Health has par-ticipated in this Nordic project, the OECD’s work in this field and also the efforts of the Nordic Nurses’ Federation (SSN). It is important to develop quality indicators for the various fields of health services, which can subsequently be used for monitoring and for the determination of minimum professional standards in the operation of health services.
Clinical quality advisory boards A geriatric nursing clinical advisory board was at work over the year and completed the preparation of guidelines for nursing-home care. Also, a clinical advisory board of midwives administering at-home care worked on clinical guidelines for at-home care provided by midwives; preparations were well un-der way by the close of the year.
Operation of the health services Clinical quality monitoring and minimum professional standards According to law, the Directorate of Health has been responsible for the professional monitoring of the activities of health care facilities and the work-ing conditions of health care workers over the past decades. The new Medical Director of Health Act of 2007 reaffirms this role and in fact widens the Di-rectorate’s scope of monitoring to include self-employed specialists in all fields of the health ser-vices. According to a new government regulation, parties intending to launch the operation of a health service are required to notify the Medical Director of Health and obtain confirmation that cer-tain professional standards have been met.
In recent years, monitoring of health care facilities has been carried out in a standardised manner, involving the assessment of the operations of the facilities based on data available at the Directorate, information on operations and employment issues obtained from managers of the relevant facilities,
opinions of employees surveyed by the Directorate by means of questionnaires and, finally, a service survey submitted to recipients of the service. Sub-sequently, the facilities in question are visited and the managers and employees consulted. The Direc-torate also uses other methods of monitoring based, among other things, on the quality guide-lines of the World Health Organisation.
Some 350 health care units operating in Iceland fall within the scope of this monitoring system and in the autumn of 2007 confirmed data on over 300 self-employed physicians had been gathered at the Directorate of Health. Clinical quality monitoring audits were performed in thirteen health care facili-ties in western Iceland and three in other parts of the country. Monitoring of facilities for the elderly RAI assessment Resident Assessment Instrument (RAI) 2.0 in nurs-ing homes for the elderly A regulation issued by the Ministry of Health calls for regular assessment of the accommodation and health of residents in facilities for the elderly based on an international instrument, the Resident As-sessment Instrument (RAI). In Iceland, the Direc-torate of Health monitors the RAI assessment un-der the supervision of a project manager. In 2007, seven courses were held for nurses and nursing assistants involved in the RAI assessment, both in Reykjavík and in other parts of the country.
The RAI 2.0 is an extensive standardised tool de-signed to assess the strength, health conditions and need for care of the elderly in nursing homes. Among other things, the tool makes it possible to extract quality indicators, RAPs (Resident Assess-ment Protocols) and RUG (Resource Utilization Group) staffing intensity categories. The results are subsequently used to assess the professional ser-vice of health care facilities. The RAI assessment also gives managers of facilities and the health au-thorities the opportunity to compare the success of different wards and institutions, making funding more transparent and fair.
RAI assessment can be used at various levels of care. The tool has already been put to use to some extent for at-home care in Reykjavík and in the course of the year it was implemented for geriatric and psychiatric wards.

12
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
Preadmission nursing-home assessment (PNHA) At the end of the year a new regulation was issued by the Minister of Health on PNHA for permanent care in nursing homes. The regulation entrusts the Medical Director of Health with the supervision of the application of PNHA in Iceland. By the end of the year preparations for assuming this new task on 1 January 2008 were in progress.
Health care professionals Applications for licences to practice The Directorate of Health has for a long time been responsible for giving formal opinions on applica-tions for licences to practice in most health care professions, i.e. 26 out of the 32 health care pro-fessions. In 2007, a total of 331 licence applications were processed at the Directorate, 115 of which were from physicians, 31 from paramedics, the same number from physiotherapists and 33 from a new health care profession, alcohol and drug con-sultants. With the legislative amendments of 2007 it was clear that this would change in 2008, making the Directorate itself responsible for licensing of all health care professionals.
Threats to health care professionals A working group was appointed by the Directorate of Health, the Administration of Safety and Health in Iceland, the Icelandic Medical Association and the Icelandic Nurses’ Association to analyse the optimal responses to threats to health care profes-sionals in the course of their work and to develop proposals on measures. The working group pub-lished a report on its results in October. In co-operation with the Administration of Occupational Safety and Health in Iceland a leaflet was also dis-tributed stressing the obligation of employers to guarantee a safe and healthy working environment for their staff. The report contained a specific re-minder to health care institutions that physical as-sault is categorised as a reportable incident to be recorded in the same manner as any other occupa-tional accident. Shortage of human resources in the health services Shortage of health care professionals, particularly nursing assistants and nurses, was the subject of considerable discussion during the year. The num-ber of actively employed nursing assistants is ap-proximately 2000, with 90–100 nursing assistants graduating on a yearly basis. The estimated need is approximately 300 per year. The shortage of nurses is estimated at approximately 600 for just over 400 full-time equivalent positions. The short-age extends to hospitals, the primary health care services and nursing homes. In 2007, the Icelandic parliament approved a special allocation which en-abled the enrolment of 153 first-year nursing stu-dents at the Universities of Iceland and Akureyri. Clinical guidelines Work on the preparation of clinical guidelines was started at the Directorate of Health in January 2000. Since that time, guidelines on some 37 sub-jects have been published, five of which have al-ready been revised. The clinical guidelines were presented at meetings in Iceland and abroad and courses based on the guidelines have now become a permanent feature of the studies of physicians, nurses and pharmacists, the aim being to empha-sise their role as a teaching tool even further in the future.
There has been extensive collaboration with similar committees at LUH in Reykjavík, both as regards co-operation with working groups and presenta-tions. During the year productive co-operation has

13
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
groups predominantly abusing morphine the use has decreased and the number of addicts undergo-ing treatment has fallen. In co-operation with the Icelandic Medicines Control Agency a list intended for physicians was developed to indicate the pharmaceuticals recommended as the first choice for common diseases with regard to efficacy, adverse effects and pricing. The Director-ate issued a recommendation stating that certain pharmaceuticals should not be used in prisons ex-cept in case of emergency or with the approval of more than one physician when justified in excep-tional circumstances. It is important to limit the use of these pharmaceuticals among prisoners to the extent possible.
Shortage of pharmaceuticals Shortages of certain pharmaceuticals in the market are becoming increasingly evident, even products registered in Iceland; frequently the shortages in-volve pharmaceuticals that return small profits but which are nevertheless necessary for patients. Shortages of some pharmaceuticals can cause sig-nificant discomfort and harm to patients. New institute for pharmaceutical issues The Research Institute for Pharmaceutical Out-comes and Policy was launched on 25 April 2007, with the purpose of serving as a venue for pharma-ceutical research with special regard to studies re-lating to sound decisions on pharmaceutical use. The Directorate of Health is one of the founders of the Institute together with several other public enti-ties.
also been maintained with the primary health care services, the Regional Hospital in Akureyri, the Ma-ternity Care Centre in Reykjavík and the Public Health Institute of Iceland. Partner institutions abroad include the Scottish Intercollegiate Guideline Network (SIGN) in Scotland, NICE in Great Britain, NZGG in New Zealand, NHMRC in Australia and SBU in Sweden. In addition, co-operation with EUnetHTA (www.eunethta.net) was formalised at the beginning of 2007 with the editor of the clinical guidelines participating in four working groups which are engaged in developing tools for institu-tion health technology assessment (HTA). Participa-tion in the Cochrane Collaboration continued.
Finally, the Directorate published two guidelines at the close of the year in co-operation with the steer-ing group for clinical guidelines covering procedures in the assessment and treatment of attention-deficit hyperactivity disorder (ADHD) and the use of CAT scanning of the coronary arteries.
Pharmaceuticals and pharmaceutical regulation Pharmaceuticals Data Bank
The Directorate of Health began the operation of a Pharmaceuticals Data Bank (PDB) in 2005, in accor-dance with Act 89/2003 amending the Medicinal Products Act, for the purpose of monitoring pre-scriptions issued by physicians, in particular for ad-dictive drugs, as well as monitoring trends in the use of pharmaceuticals.
For slightly less than a year, until the autumn of 2007, a project manager for the Pharmaceuticals Data Bank was engaged at the Directorate to su-pervise and develop special projects and studies based on data from the bank. One such study fo-cused on the use of methylphenidate (Ritalin and related products) in children in Iceland in 1989–2006. Another study concerned the increased risk of cardiovascular disease in individuals using the medicinal product rofecoxib or Vioxx.
Choice and use of pharmaceuticals Monitoring of addictive drug prescriptions was tightened even further during the year. The Chief Physician of SÁÁ, the National Centre of Addiction Medicine, is of the opinion that the Pharmaceuticals Data Base already has significant preventive ef-fects; for example, the use of amphetamines de-creased by 25% from 2003 to 2006, and in the age

14
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
mendation stating that certain pharmaceuticals should not be used in prisons except in case of emergency, as recounted earlier. Immigrants The Government worked on devising a policy on immigrant affairs and the Directorate participated in this work. The Directorate also co-operated with other organisations to improve the information and services available to immigrants. Sale of hearing aids – Recommendation of the Medical Director of Health to operating licence holders According to a new regulation issued by the Minis-ter of Health, the Medical Director of Health is re-sponsible for monitoring holders of operating li-cences to sell hearing aids. The Medical Director of Health is granted access to all data regarded as necessary to conduct the surveillance. In addition to the National Hearing and Speech Institute of Iceland, three undertakings currently hold licenses to sell hearing aids. Psychological support and trauma treatment The Directorate of Health continued its work on the organisation of psychological support and trauma treatment in co-operation with the Icelandic Red Cross, the Landspitali University Hospital (LUH), the Civil Protection Department of the National Com-missioner of the Icelandic Police and the Icelandic Bishop’s office. The work focuses on informing the public, the media and others on the pivotal role of family and friends in the face of unexpected and traumatic events.
Civil protection According to law, the Directorate of Health is re-sponsible for various aspects of civil protection. As in recent years, the most prominent features in-clude participation in exercises and the organisation of health services in the event of catastrophes.
Numerous exercises were held with the participa-tion of the Directorate’s crew. A bus accident in eastern Iceland showed that exercises of this sort return results with regard to co-ordinated response. Work progressed on the organisation of psychologi-cal support and trauma treatment and the coordi-nation of response plans in health care facilities.
Medical devices According to a law, the Directorate of Health is the competent authority in matters concerning medical devices, and in that capacity is responsible for pol-icy making, inspection and market surveillance of medical devices in Iceland.
In 2007, the Directorate received a total of 1993 notifications and other documents concerning medical devices. Notifications of defects in medical devices were 710 in total, of which 544 were notifi-cations from competent authorities in other coun-tries and 166 were notifications from Eudamed (European Database on Medical Devices). The Di-rectorate also received 186 notifications concerning devices and methods marketed in Europe for the assessment of biological samples in vitro. Other notifications, queries etc. on various aspects of medical devices totalled 799.
Nordic collaboration meetings on medical devices are conducted annually, and this year the meeting was held in Iceland on 20–21 September.
Medical treatment and health care services Anorexia The work of the Forma Association, an organisation to counteract anorexia, came under some discus-sion during the year. The Directorate emphasised that the treatment of anorexia should be left to health care professionals, as anorexia is a complex mental disorder, the treatment of which calls for professional expertise. Future vision in geriatrics An interesting symposium on a future vision for geriatrics was held on 24 October 2007. The Direc-torate declared its readiness to work with profes-sional bodies for the further elaboration of propos-als on the organisation of geriatric issues. The guideline underlying this work is to enable the eld-erly to live in their homes for as long as possible. For this to be possible, it is necessary for primary health care services, hospitals, nursing homes, the social services and associations of the elderly to collaborate on proposals for solutions. Health care in prisons The Directorate of Health participates in a consulta-tion group on prisoners’ affairs to promote im-proved services to prisoners. In co-operation with prison physicians, the Directorate issued a recom-

15
Response and preparedness plans against pandemic influenza In the past two years, extensive preparations have been made for a national pandemic response and preparedness plan in co-operation with the Civil Protection Department of the National Commis-sioner of the Icelandic Police. As discussed earlier, the Chief Epidemiologist, the Agricultural Authority of Iceland, the Environment Agency of Iceland and the Civil Protection Department of the National Commissioner of the Icelandic Police co-operated on a common web site, www.influensa.is, which was opened in the beginning of December. On 10 December 2007, an extensive exercise was con-ducted involving responses to pandemic influenza.
Communicable diseases Reportable diseases The obligation to report on so-called reportable communicable diseases refers to the obligation to submit data to the Chief Epidemiologist on these diseases without information on personal identity or on contact tracing. The reporting on these dis-eases, however, is far from complete and some primary health care centres do not submit any such reports. Influenza The annual influenza outbreak in Iceland usually peaks in the period from October to March. In 2007, the influenza began in January and peaked in early March. In the same period the influenza A diagnosed belonged mostly to the strain H3N1, but at the beginning of the epidemic the cases of influ-enza A diagnosed all belonged to the H1N1 strain. There was an equal number of cases of influenza A and B. The influenza outbreak in 2007 was not se-vere in Iceland.
At the close 2007, 10 years had passed since the current Communicable Diseases Act No. 19/1997 entered into force. Since then a number of unex-pected events, both in Iceland and elsewhere, have required the attention of the Chief Epidemiologist. Outside Iceland, the European Union (EU) has en-hanced communicable disease control by launching the European Centre for Disease Prevention and Control – ECDC and an institution under the aus-pices of the European Commission, the Health Se-curity Committee, for the purpose of responding to health threats. Furthermore, the World Health As-sembly has adopted the International Health Regu-lations (IHR), which became a legally binding inter-national agreement after its entry into force on 15 June 2007.
Legal framework of communicable dis-ease control and new regulations In 2007, amendments were made to the Communi-cable Diseases Act based on the provisions of the International Health Regulations (IHR). Following the amendments in 2007, the Act now also covers the impact on health of radioactive and toxic mate-rials and all unexpected events posing a potential global threat to public health. The Act is now called Act on Health Security and Communicable Disease Control.
Two new government regulations were adopted during the year under the amended Act. The first regulation entrusts the Chief Epidemiologist with supervising emergency inventories of pharmaceuti-cals and other necessary equipment in the country to address health threats, such as epidemics and other emergencies, and publish procedures con-cerning medical examinations of immigrants to Ice-land. The other regulation divides the country into eight communicable disease control districts, each of which features a designated head physician of the primary health care services who serves as dis-trict epidemiologist.
I I I . C O M M U N I C A B L E D I S E A S E C O N T R O L

16
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
Notifiable diseases The obligation to notify certain diseases involves submitting identifiable data to the Chief Epidemiolo-gist. This information is very reliable, as it is based on data from both physicians and laboratories. Respiratory infections Tuberculosis Nine cases of tuberculosis were diagnosed in 2007, five of which derived from outside Iceland. Late in 2007, a patient from Lithuania was diagnosed with multi-drug resistant tuberculosis. Multi-drug resis-tant TB is a serious problem in many states of the former Soviet Union, particularly the Baltic Coun-tries. As citizens of these countries do not require residence and employment permits in Iceland they do not have to submit the health certificates re-quired for such permits. The primary health care services and hospitals in Iceland therefore have to be on the alert for TB infections in individuals com-ing from these countries who seek medical assis-tance because of respiratory symptoms.
Meningococcal disease Four individuals were diagnosed with confirmed meningococcal infection in Iceland in 2007, the same number of cases as in 2006. These four indi-viduals included a three-year old child with menin-gococcal C disease, who had not been vaccinated against the disease, and three individuals with meningococcal B disease. There were no deaths in Iceland resulting from meningococcal infection in 2007.
Since the Men C vaccination was started in 2002 no vaccinated individual has been diagnosed with Men C disease.
Enteric infections Enterohemorrhagic E. Coli (EHEC) A total of 12 people were diagnosed with entero-
hemorrhagic E. coli in 2007. Straintyping revealed that all the individuals were infected with the same strain, indicating a common origin of the infection. A comparison of Icelandic and Dutch bacterial strains showed that the same strain was causing infections in both countries. Packed iceberg salad from the Netherlands came under suspicion, but attempts to trace the infection to a specific pro-ducer were unsuccessful.
Salmonellosis A total of 93 individuals were diagnosed with sal-monellosis in Iceland in 2007, which is a similar number as in previous years. Only 16 out of the 93 cases of salmonellosis were considered of domestic origin; in 64 cases the infections originated abroad while the origin of the infection in 16 cases remains uncertain.
Sexually transmitted diseases Chlamydia trachomatis A total of 1855 individuals were diagnosed with chlamydia in 2007, which represents an increase compared to the preceding year. Chlamydia cases were diagnosed in a total of 1089 women and 696 men, with information on gender lacking in 70 cases. The average age for women at the time of diagnosis was approximately 22 years, whereas the men were generally older, or around 25 years.
Gonorrhoea In 2007, the Department of Clinical Microbiology at the Landspitali University Hospital diagnosed 20 individuals with gonorrhoea, of which 14 cases were in men and 5 in women, with information on gender lacking in one case. The average age of the men diagnosed was just over 28 years and that of the women 27 years. The number of gonorrhoea cases has been increasing sharply in recent years, but the rate of increase seems to have fallen off somewhat during the past year.
Percentage of ambulatory patients with confirmed influenza symptoms and percentage of laboratory samples diagnosed as
influenza from 1 December 2007 to 8 March 2008
0
5
10
15
20
25
30
35
40
45
w 49 w 50 w51 w52 w1 w2 w3 w4 w5 w6 w7 w8 w9 w10Week of the year 2007–2008
Perc
enta
ge %
Influenza symptoms Diagnosed cases of influenza
Cases of chlamydia and gonorrhoea diagnosedin Iceland 1997–2007
0
500
1000
1500
2000
2500
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Year
Case
s of
chl
amyd
ia
05101520253035
Case
s of
gon
orrh
oea
Chlamydia Gonorrhoea

17
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
HIV and AIDS Thirteen individuals were diagnosed with HIV infec-tion in Iceland in 2007. A probable connection with intravenous drug abuse was considered to be in-volved in six of the cases. Seven of the individuals diagnosed during the year were women, making this the first time that women diagnosed with HIV infection in Iceland outnumbered the men. Bloodborne infections Infectious hepatitis An unusually large number of people was diag-nosed with hepatitis B in 2007, or 48 individuals. Approximately half of them were immigrants and eight had a confirmed history of intravenous drug abuse. The proportion of immigrants diagnosed with hepatitis B is still quite large.
Hepatitis C is by far the most common type of hepatitis in Iceland. In 2007, 95 people were diag-nosed with hepatitis C, which is a significant in-crease from the preceding years.
Vaccinations The childhood vaccination programme At the beginning of 2007, a new arrangement of the immunisation programme entered into force following an open tender for the vaccines used in the programme. The principal change involved the introduction of a pertussis booster vaccination at 14 years of age and the use of new brands of vaccines from different manufacturers. From 1 January 2007, the following procedure has been in effect (see table).
Tender for vaccines against the annual influenza In 2007, the Icelandic government decided to offer every individual from the age of 60, together with individuals belonging to specific risk groups, a vac-cination against influenza, free of charge. A con-
tract with a term of four years was signed with the manufacturers on the purchase of 60,000 doses of influenza vaccines. It is hoped that this effort will make it possible to increase the coverage of vacci-nations in these groups.
Purchase of influenza pandemic vaccine In May 2007, the Minister of Health signed a con-tract with GlaxoSmithKline securing an option for 300,000 doses of vaccine for Iceland in the event of pandemic influenza. The term of the contract is three years, with the possibility of an extension of two years.
Purchase of vaccine against the H5N1 influenza strain In October 2007, the Chief Epidemiologist signed a contract with GlaxoSmithKline on the purchase of 10,000 doses of the so called pre-pandemic vaccine (H5N1), making the vaccine available in Iceland in the event of detection of the H5N1 strain of the virus.
Vaccination coverage in Iceland In recent years the coverage of vaccinations has been estimated on the basis of sales figures of the relevant vaccines. The estimated coverage of the primary vaccination against diphtheria, tetanus, pertussis, HIB and polio is over 95% and the cover-age of the vaccination against mumps, measles and rubella 90–95%.
Centralised Vaccination Registry On 1 March 2007, a contract was signed with TM Software – Health care (eMR hugbúnaður hf) on a centralised vaccination data base for the Chief Epi-demiologist following a successful pilot project on the electronic transfer of vaccination data that was completed in 2005. In the course of the year 2007, most health care facilities were connected to the data base and the connection of all the facilities is expected to be concluded in 2008.
Age Contents Name Producer
3, 5, 12 months DTaP, Hib, IPV Infanrix Polio Hib GSK
6, 8 months MCC NeisVac-C Baxter
18 mon., 12 yrs MMR Priorix GSK
5 years dTaP Boostrix GSK
14 years dTaP, IPV Boostrix Polio (ein sprauta) GSK
18
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
Communicable disease measures by the authorities Monitoring applicants for residence permits in Iceland The Chief Epidemiologist processed health certifi-cates with regard to temporary work or residence permits, as the general procedure has been since 2005. The number of such certificates in 2007 was 257, which represents a significant reduction com-pared to previous years. Emergency inventory Antivirals, antibacterials, necessary medica-tions, vaccines and drips The Chief Epidemiologist supervises the emergency inventory in Iceland. Measures against an influenza pandemic focus on ensuring adequate supplies of antivirals, vaccines, antibiotics and drips. In 2007, 104,000 doses of influenza medications were avail-able in Iceland, including 82,000 doses of osel-tamivir (Tamiflu®) and 22,000 doses of zanamivir (Relenza®). The target is to increase the supplies to 150,000 treatment doses.
Turnover supplies for 12 months’ average use of drips are available in Iceland.
Protective equipment In 2006, the Chief Epidemiologist, acting for the government, launched a tender for personal protec-tive equipment following the decision to stock cen-tralised national supplies for use in the event of an epidemic. The protective equipment comprises sev-eral kinds of particulate respirators, safety goggles, protective gowns and aprons, overalls and gloves for single use, the latter being added to the inven-tory in 2007. The Chief Epidemiologist supervises the safeguarding of the inventory and controls its allocation.
During the year the Chief Epidemiologist, together with other organisations, sponsored courses in the use of protective equipment. Four full-day courses were held, designed primarily for veterinarians, employees of poultry farms, the police and labora-tory personnel.
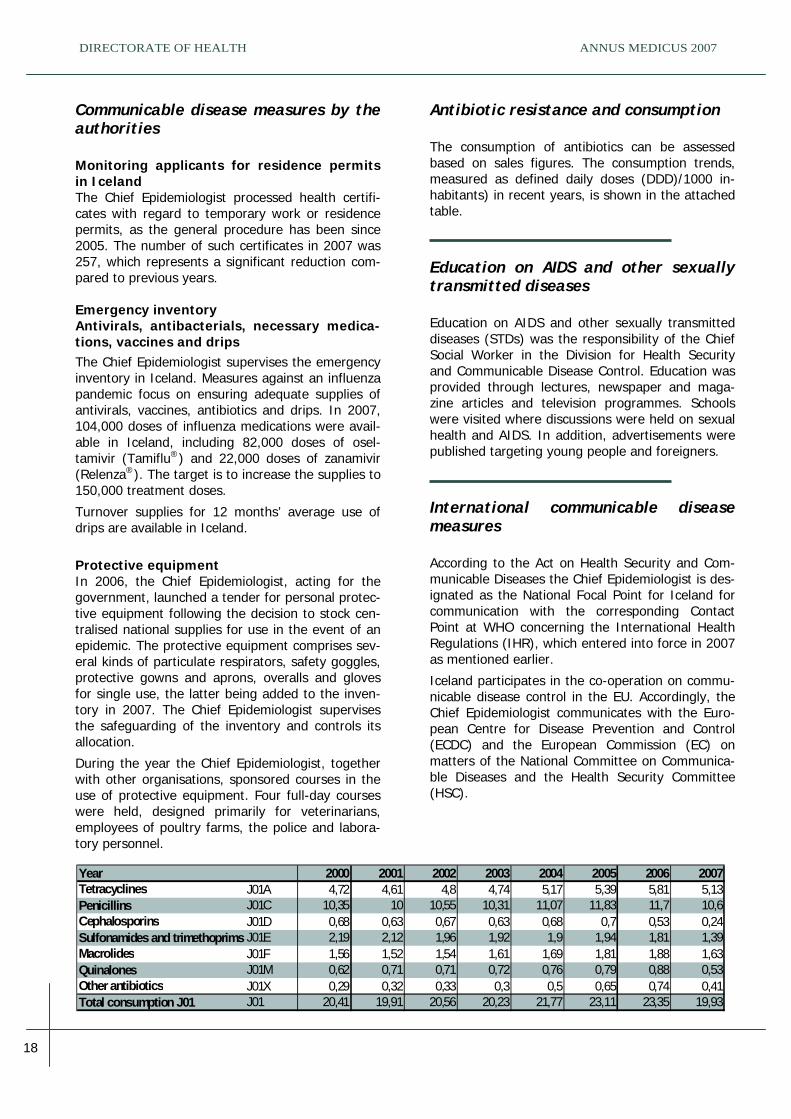
Antibiotic resistance and consumption The consumption of antibiotics can be assessed based on sales figures. The consumption trends, measured as defined daily doses (DDD)/1000 in-habitants) in recent years, is shown in the attached table. Education on AIDS and other sexually transmitted diseases Education on AIDS and other sexually transmitted diseases (STDs) was the responsibility of the Chief Social Worker in the Division for Health Security and Communicable Disease Control. Education was provided through lectures, newspaper and maga-zine articles and television programmes. Schools were visited where discussions were held on sexual health and AIDS. In addition, advertisements were published targeting young people and foreigners.
International communicable disease measures According to the Act on Health Security and Com-municable Diseases the Chief Epidemiologist is des-ignated as the National Focal Point for Iceland for communication with the corresponding Contact Point at WHO concerning the International Health Regulations (IHR), which entered into force in 2007 as mentioned earlier.
Iceland participates in the co-operation on commu-nicable disease control in the EU. Accordingly, the Chief Epidemiologist communicates with the Euro-pean Centre for Disease Prevention and Control (ECDC) and the European Commission (EC) on matters of the National Committee on Communica-ble Diseases and the Health Security Committee (HSC).
Year 2000 2001 2002 2003 2004 2005 2006 2007Tetracyclines J01A 4,72 4,61 4,8 4,74 5,17 5,39 5,81 5,13Penicillins J01C 10,35 10 10,55 10,31 11,07 11,83 11,7 10,6Cephalosporins J01D 0,68 0,63 0,67 0,63 0,68 0,7 0,53 0,24Sulfonamides and trimethoprims J01E 2,19 2,12 1,96 1,92 1,9 1,94 1,81 1,39Macrolides J01F 1,56 1,52 1,54 1,61 1,69 1,81 1,88 1,63Quinalones J01M 0,62 0,71 0,71 0,72 0,76 0,79 0,88 0,53Other antibiotics J01X 0,29 0,32 0,33 0,3 0,5 0,65 0,74 0,41Total consumption J01 J01 20,41 19,91 20,56 20,23 21,77 23,11 23,35 19,93

19
One of the main functions of the Medical Director of Health is to collect and process data on health and health services which are necessary for man-agement, monitoring, policy making, research and planning. The new Medical Director of Health Act No. 41/2007 provides clearly for the Medical Direc-tor’s function to organise and maintain national registers on health, diseases, accidents, prescrip-tions, births, and the work and performance of the health services. According to the Act, health care providers are required to provide the Medical Direc-tor of Health with the information needed to main-tain the health registers. The Medical Director of Health is also required to maintain a register of operators of health services, who therefore need to notify the Medical Director of any changes in their operation. Accordingly, the register was in preparation at the Directorate of Health during 2007. This project will be completed in the first half of 2008.
Health registers and their processing Register of admissions to hospitals In 2007, hospital data on admissions in 2005 were processed. Statistics for the years 1999–2005 were published on the web site of the Directorate of Health. Waiting lists for hospitals A summary was prepared of waiting lists for se-lected procedures in hospitals in June and October 2007, showing the number of individuals waiting at each time and the proportion of these same indi-viduals waiting over 3 months. Statistics on the number of procedures carried out were also pub-lished.
Register on preadmission nursing home assessment (PNHA) Management and monitoring of the PNHA register was transferred from the Ministry of Health to the Directorate of Health and a dedicated project man-ager was engaged at the beginning of 2007. Vari-ous statistics can be retrieved from the register, including the number of individuals on the waiting list for residence in nursing homes at each time. At mid-year 2007, the Directorate of Health also took over access control to the PNHA register. Contact register of the primary health care services The Directorate of Health collects data on the con-tacts of individuals with health care centres accord-ing to recommendations on minimum data re-cording. Among other things, the register provides information on the date of contact, type (consultations, visits, telephone calls or other), age of patient, reason for contact, diagnosis and resolu-tion. In 2006 a total of 242,000 individuals sought the services of primary health care centres, of which 35% visited the centres five or more times. The number of contacts with primary health care cen-tres in 2006 was around 1,350,000, or 4.4 per cap-ita, and including telephone calls the total number was around 1,850,000.
I V. H E A L T H S TA T I S T I C S
Contacts withhealth care centres in 2006
0
10000
20000
30000
40000
50000
60000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15+*
Number of cont act s
Number of individuals

20
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
Self-employed specialist physicians’ contact register In 2007, the Medical Director of Health decided, pursuant to the Medical Director of Health Act, to begin collecting certain data on registered contacts of patients with specialist physicians at their clinics. The gathering of this data by the Medical Director of Health is based on the minimum data recording requirements that specialist physicians must fulfill, as described in the Medical Director of Health’s rec-ommendations on minimum recording of contacts in primary health care centres and by self-employed specialist physicians.
In the autumn of 2007, the Medical Director of Health had obtained confirmed information that 307 physicians were self-employed in their own establishments, of which 65 operated at two differ-ent establishments and 12 at three different estab-lishments.
The Icelandic Accident Registry The Icelandic Accident Registry is a data bank con-taining information on accidents that happen in Iceland. The Directorate of Health is responsible for its daily administration. The objective of the Ice-landic Accident Registry is to collect in one place information on accidents throughout Iceland and co-ordinate their registration.
Parties submitting data In the second half of 2007, there were 12 parties who submitted data to the Icelandic Accident Reg-istry. At the beginning of the year the National Commissioner of the Icelandic Police began a full registration together with all the primary health care centres pertaining to the Health Institute of East Iceland, a total of 12 establishments.
The enactment of the Medical Director of Health Act has strengthened the foundations of the Ice-landic Accident Registry by placing it under the re-sponsibility of the Medical Director of Health. Previ-ously, health care facilities were free to choose whether they participated in submitting data to the Accident Registry. The target has been set that by mid-2008 all the primary health care centres in Ice-land should be submitting data into the Accident Registry.
Processing Statistics from the Icelandic Accident Registry were published regularly on the web site of the Director-ate of Health, as in previous years, in addition to a
weekly publication of the number of accidents. In 2007, a total of 38,956 accidents were entered into the Accident Registry.
Toward the end of 2007, the Directorate of Health, in co-operation with the Public Health Institute of Iceland, began preparations for a study of home and leisure accidents, school accidents and sports accidents in 2005.
Induced Abortion and Sterilisation Registry A total of 893 induced abortions were performed in Iceland in 2006. The Directorate of Health also col-lects data on sterilisations pursuant to Act No. 25/1975. A total of 519 sterilisations were per-formed in 2006, 313 on men and 206 on women.
Registers of opt-outs Pursuant to legislation dating from 1998 the Direc-torate of Health is in charge of the registration of opt-outs from the Health Sector Database. By the close of 2007, just over 20,400 had opted out of the database, 50 of whom have withdrawn their opt-out. Opt-outs from biobanks are also registered at the Directorate of Health. At the close of 2007, a total of 222 opt-outs had been registered. Registries of health care professions The Directorate of Health has in the past few years been developing electronic registries on various health care professionals and has currently com-piled registries of physicians, dentists, nurses and midwives. Certain data from these registries are accessible on the website of the Directorate of Health, where they are regularly updated. The reg-istries are useful, for example, for the registration
Induced abortions per 1000 women 15 –44 years 1961–2006 . Five - year average
0
2
4
6
8
10
12
14
16
1961-1965
1966-1970
1971-1975
1976-1980
1981-1985
1986-1990
1991-1995
1996-2000
2001-2005
2006

21
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
of health care facilities, monitoring, planning and statistical analysis, e.g. for international databases.
By the end of 2007, a total of 1845 physicians and 355 dentists had been issued a licence to practise in Iceland. At the same time 3738 nurses and 395 midwives had been granted a licence to practise. However, these numbers do not indicate how many people were actively employed in each profession in Iceland during the year.
Talnabrunnur, a newsletter in Icelandic on health statistics On 25 October 2007, the first issue of a new monthly newsletter in Icelandic on health statistics was published by the Directorate of Health under the name Talnabrunnur. The newsletter is intended to supplement the statistics already issued by the Directorate, primarily on the Directorate’s web site, but also in printed versions.
Cartography Two maps were developed by the Directorate of Health and published on its web site in 2007. The maps show, on the one hand, the division of the country into health districts and, on the other hand, into communicable disease control districts, in both cases based on new laws and regulations which entered into force during the year.
Classification systems The international classifications of the World Health Organisation (WHO) are the common language of the health services for the registration of health data. The Medical Director of Health is responsible for the supervision of classification systems in Ice-land.
In 2007, work has been in progress on preparations of a new presentation of classification systems on the web site of the Directorate of Health and the first update of the NOMESCO Classification of Surgi-cal Procedures (NCSP) was launched.
An update of the NANDA nursing diagnosis code was concluded during the year and updates of other classification systems were prepared, all of which require extensive consultation with medical professionals, both physicians and nurses.
An application was submitted for permission to use the International Classification for Primary Care (ICPC) throughout Iceland, as this system is obliga-tory for registration of reasons for visits of individu-als to the primary health care services. Maintaining classification systems involves considerable transla-tion work. The biggest project of the year was a complete translation of the International Classifica-tion of Functioning, Disability and Health (ICF). Surveys In early May 2007, the Ministry of Health entrusted the Directorate of Health with the conduct of a sur-vey evaluating the circumstances and opinions of the elderly on the waiting list for admission to nurs-ing homes in Fjarðabyggð in eastern Iceland. A similar survey had been performed at the request of the Ministry in the preceding year among elderly people both in Reykjavík and the neighbouring town of Hafnarfjörður.
As previously mentioned a study was performed on the health, wellbeing and welfare of Icelanders from 18–79 years of age. The participants are 10,000 people, randomly chosen. The study was conducted by the Public Health Institute of Iceland in co-operation with other parties.
22
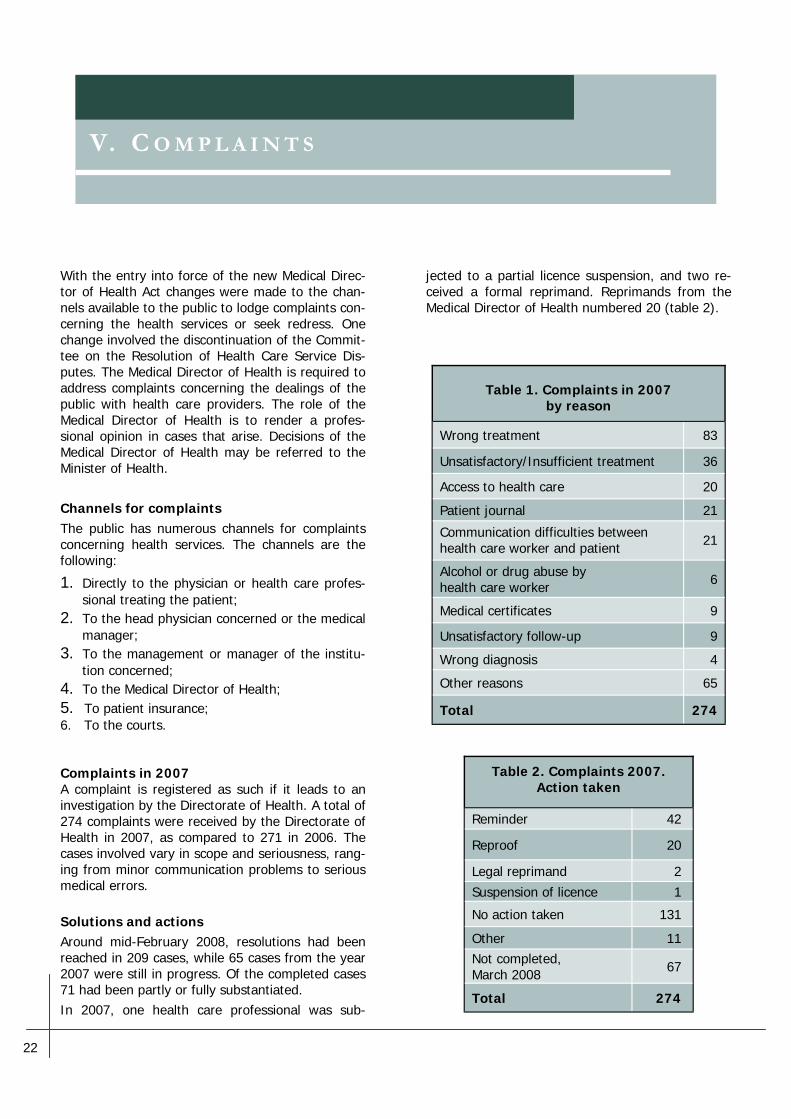
jected to a partial licence suspension, and two re-ceived a formal reprimand. Reprimands from the Medical Director of Health numbered 20 (table 2).
With the entry into force of the new Medical Direc-tor of Health Act changes were made to the chan-nels available to the public to lodge complaints con-cerning the health services or seek redress. One change involved the discontinuation of the Commit-tee on the Resolution of Health Care Service Dis-putes. The Medical Director of Health is required to address complaints concerning the dealings of the public with health care providers. The role of the Medical Director of Health is to render a profes-sional opinion in cases that arise. Decisions of the Medical Director of Health may be referred to the Minister of Health. Channels for complaints The public has numerous channels for complaints concerning health services. The channels are the following:
1. Directly to the physician or health care profes-sional treating the patient;
2. To the head physician concerned or the medical manager;
3. To the management or manager of the institu-tion concerned;
4. To the Medical Director of Health; 5. To patient insurance; 6. To the courts. Complaints in 2007 A complaint is registered as such if it leads to an investigation by the Directorate of Health. A total of 274 complaints were received by the Directorate of Health in 2007, as compared to 271 in 2006. The cases involved vary in scope and seriousness, rang-ing from minor communication problems to serious medical errors. Solutions and actions Around mid-February 2008, resolutions had been reached in 209 cases, while 65 cases from the year 2007 were still in progress. Of the completed cases 71 had been partly or fully substantiated. In 2007, one health care professional was sub-
V. C O M P L A I N T S
Table 2. Complaints 2007. Action taken
Reminder 42
Reproof 20
Legal reprimand 2 Suspension of licence 1
No action taken 131
Other 11 Not completed, March 2008 67
Total 274
Table 1. Complaints in 2007 by reason
Wrong treatment 83
Unsatisfactory/Insufficient treatment 36
Access to health care 20
Patient journal 21
Communication difficulties between health care worker and patient 21
Alcohol or drug abuse by health care worker 6
Medical certificates 9
Unsatisfactory follow-up 9
Wrong diagnosis 4
Other reasons 65
Total 274

23
The Directorate of Health is responsible for policy-making and advising the health authorities on pub-lic health, e.g. as regards primary health care and prevention. The Directorate has developed guide-lines in this respect in co-operation with primary health care professionals and the Icelandic universi-ties. In addition, the Directorate co-operates with the Public Health Institute of Iceland in matters concerning first-stage prevention and health pro-motion. The Medical Director of Health sits on the National Public Health Committee.
Collaboration projects on prevention and public health Primary health services for infants and toddlers In recent years the Directorate of Health has been revising a manual on primary health services for infants and toddlers, on which considerable time was spent in 2007. It is clear that changes will be made in the key age examinations, substituting examinations at two and a half years and four years of age for the previous examinations at three and a half and five years of age. Child obesity A seminar on child obesity, prevention and treat-ment was held in June 2007, and subsequently an advisory board was appointed to submit proposals on measures to be taken by the health services. The advisory board started working immediately and proposals are expected in the spring of 2008. Education on sexual maturity During the year the Directorate co-operated with the Centre for Child Health Services on the produc-tion of literature on sexual maturity for the School Health Service. This work is part of the preparation of an education project intended to serve as a co-ordinated basis for the School Health Service’s ef-fort to educate students and parents on health and health care.
Healthy advice At the beginning of 2007, the decision was made for the Directorate of Health to stop providing ma-terial to the awareness and information campaign, which has been known as Healthy advice. The cam-paign was started in February 2002. The material gathered during the five years of the campaign is preserved on the Directorate’s web site, where it will remain for the time being.
Suicide prevention – the Icelandic Alliance Against Depression The Icelandic Alliance Against Depression, a pro-gramme devoted to preventive measures, has been operated since 2002 with the aim of reducing the rate of suicide in Iceland, increasing the skills and knowledge of professionals concerning depression and suicide, and raising the awareness of the gen-eral public on depression and suicidal behaviour with the objective of reducing prejudice.
In 2007, a decision was made to focus the effort to a greater extent on children and adolescents. Preparations were begun in co-operation with rep-resentatives from several organisations to launch a web site designed to increase access to education on the psychological welfare of children and their families.
Education Education and training for professionals mostly took the form of courses of study designed for the health care districts of Iceland. The basic courses of the Icelandic Alliance on Depression continued to be provided to physicians, nurses, psychologists, social workers, ministers of the church and the po-lice, in addition to educational and vocational coun-sellors and teachers.
V I . P U B L I C H E A L T H A N D P R I M A R Y C A R E

24
ANNUS MEDICUS 2007 DIRECTORATE OF HEALTH
Train the Trainers is a training programme intended for professionals for the purpose of disseminating specialised knowledge to the extent possible to the grassroots, and to this end all the participants re-ceived a CD with the material from the courses for use in their work. A total of ten Train the Trainers courses were held, most of them with cross-curricular participation, and a substantial multiplica-tion effect is anticipated. Psychologists at the psychiatric unit of the Landspi-tali University Hospital (LUH) have developed and designed a course called Cognitive Behavioural Therapy for Depression. The initial courses were intended for primary health care physicians, but in 2007 three courses were also held for other profes-sionals. Support for families based on the Beardslee model. In collaboration with the psychiatric unit of LUH, a one-year course was launched for the purpose of training employees of the psychiatric division to employ systematic support measures for children living in circumstances where one or both parents suffer from mental disorders. The same parties or-ganised a cross-curricular Nordic seminar in Reyk-holt in western Iceland in May with the participa-tion of 70 individuals, of which 45 were from the other Nordic countries. Courses in co-operation with the Red Cross, the Bishop’s Office and other parties continued to be held. Seven two-day courses of this kind were held during the year with the participation of 800 indi-viduals. Following the courses support groups have been founded in many parts of the country.
For the purpose of educating the general public, articles from members of the advisory board were published in newspapers and magazines and mem-bers have also appeared on radio and television programmes to discuss mental health issues. Fi-nally, lectures were held at conferences and sym-posiums, both in Iceland and abroad, on depres-sion, suicide and other mental disorders in addition to addiction disorders. International co-operation The Icelandic Alliance Against Depression is a founding member of the European Alliance Against Depression (EAAD), of which 16 European nations are members. The Alliance has received a grant from the European Union for the prevention of de-pression. During the year, the Icelandic Alliance Against De-pression participated in a Nordic collaboration pro-ject designed to enhance the services available to parents with mental disorders and their children, based on the previously mentioned Beardslee model. Grants At the close of 2007, Alcan in Iceland provided a handsome grant from its community fund to the Icelandic Alliance Against Depression, which was used primarily to cover the cost of projects under-taken in the course of the year. SPRON Savings Bank also supported the effort.
25
In 2007, as in recent years, the Directorate of Health published several reports and pamphlets, as well as circulars and clinical guidelines. As men-tioned earlier, the Directorate launched the publica-tion of a new newsletter in Icelandic on health sta-tistics, Talnabrunnur. The Directorate’s publications are currently issued primarily on the web site, but some literature is also published in printed form, mostly pamphlets.
Reports and other publications in 2007 1. The Quality Policy of the Health Authorities to
the Year 2010. Published in collaboration with the Ministry of Health and Social Security, both in print and on the Internet.
2. Antibiotic Consumption and Resistance in Iceland in 2005.
3. Annual Report of the Directorate of Health 2006. 4. Annus Medicus 2006. Extract from the Annual
Report of the Directorate of Health 2006.
5. Guidelines on the Choice of Birth Environment. 6. Report of the Working Group on Threats to
Health Care Professionals 7. Indications for the Use of Multi-detector Com-
puted Tomographs of the Coronary Arteries. 8. Procedures for the Assessment and Treatment of
Attention-Deficit Hyperactivity Disorder (ADHD). A collection of clinical guidelines and proce-dures, primarily intended for professionals.
Pamphlets 1. Information on the Childhood Vaccination
Programme for Parents and Family Members. 2. Overview of the Childhood Vaccination Pro-
gramme in Iceland from 1 January 2007.
An update from an older educational pamphlet published in connection with changes in the or-ganisation of the childhood vaccination programme, which took effect on 1 January 2007. 3. Folate for Women of Childbearing Potential. Newsletters 1. Farsóttafréttir. The third year of Farsóttafréttir,
a newsletter in Icelandic on communicable dis-ease, was published monthly on the Directorate’s web site in 2007.
2. EPI–ICE. The English version of Farsóttafréttir. 3. Talnabrunnur – the Directorate’s newsletter in
Icelandic on health statistics. The first issue of Talnabrunnur, a monthly newsletter, was pub-lished in October.
V I I . P U B L I C A T I O N S