2 prof james bently differentiating high and low grade
TRANSCRIPT

COLPOSCOPY OF CIN; DIFFERENTIATING HIGH GRADE FROM LOW GRADE LESIONS
James Bentley , Professor Department of Obstetrics and Gynecology, Dalhousie University, Halifax NS, Canada

Normal
CIN 1
CIN 2
CIN 3
Cancer

Progression/Regression of CIN
Regress Persist Progress
to CIS
Progress
to
invasion
Months to
CIS from
baseline
CIN 1 57% 32% 11% 1% 58
CIN 2 43% 35% 22% 5% 38
CIN 3 32% <56% - >12% 12
Oster AG. Int J Gynecol Pathol 1993;12:86Richart RM, Barron BA. A follow-up study of patients with cervical dysplasia. Am J Obstet Gynecol.1969;105:386–393
Resolution of CIN 1 in adolescent is 90%
CIN 3/ CIS progression to cancer in 31% of cases treated by Bx;
McCredie et al Lancet Oncology 2008 9(5) 425-34

ASCUS
LSIL
Images downloaded from http://nih.techriver.net/bethesdaTable.php

Results: hc2 +ve
Pap smear history Number of cases Hybrid Capture 2 +ve 1
95% Confidenceintervals
ASCUS/ASCUS 87 58 (67%) 56% to 76%
ASCUS/LSIL 33 23 (74%) 52% to 82%
LSIL/ASCUS 19 18 (95%) 73% to 100%
LSIL/LSIL 21 15 (71%) 49% to 86%
All cases 160 114 (72%) 64% to 78%
1 note 10 specimens had insufficient sample
•No significant difference between groups for hc2
Triage using repeat ASCUS or LSIL pap smears; is there any difference between categories? Bentley et al IFCPC
2008

Results: CIN2 + on Bx
Pap smear history Number of cases CIN 2 or greater 95% CI
ASCUS/ASCUS 87 23 (26%) 18% to 37%
ASCUS/LSIL 33 7 (21%) 10% to 38%
LSIL/ASCUS 19 2 (10.5%) 1.7% to 32%
LSIL/LSIL 21 3 (14%) 4% to 35%
All cases 160 35 (22%) 16% to 29%
•No significant difference between groups for histology
Triage using repeat ASCUS or LSIL pap smears; is there any difference between categories? Bentley et al IFCPC
2008

CIN2 and 3 after low grade cytology ALTS trial:
Progression to CIN2 or 3 in 13% of women referred for the evaluation of LSIL or ASCUS HPV +ve smear
NS Data:
2 ASCUS, 2 LSIL, or combination
HR HPV +ve 72 %
CIN2 or > 22%

ASC-H
Images downloaded from http://nih.techriver.net/bethesdaTable.php

CIN2 or > after ASC-H
Significant pathology seen in the majority of cases
Barreth et al.:
CIN2 or > in 70% of cases
2.9% invasive disease
1.7% AIS

HSIL

CIN2 or > after HSIL
Wright ASCCP:
CIN2 or > 53%-66% with Biopsy
90% if policy of immediate colposcopy

AGC cytology
Pathology finding1
CIN 1 7%
CIN 2 or 3 36%
Adenocarcinoma in situ 20%
Cervical Cancer 9%
Endometrial Pathology 29%
1Daniel A Int.J.Gynaecol.Obstet 2005; 91(3)238-2422 Wright T Emerging Issues on HPV infections 2006 p140-146
Cytology2 Any high-grade lesion
High grade glandular
AGC-NOS 9-14% 0-15%
AGC-N 27-96% 10-93%

ASC-H
Colposcopy
No CIN
Manage as per SCC guidelines
CIN1 or >
Colposcopy, cytology, at 6 months x 2 (HPV
testing at 6 or 12 months ideally)
Return to screening protocol
CIN 1 or >
No CIN
HPV +ve follow in colposcopy clinic

HSIL
Colposcopy(Bx, +/- ECC)
No CIN 2, 3
Manage as per SCC guidelines
CIN 2 or greater
SatisfactoryColposcopy
UnsatisfactoryColposcopy
Observe with
Colposcopy and cytology
Q 6/12 x2*
Return to screening protocol
Diagnostic Excision procedure
* Consider HPV testing
Cytology/histology review
disagreeagree

Colposcopic Approach
Examine whole lower genital tract
Use acetic acid liberally
Beware the small lesion
Take >1 biopsy
Liberal use of ECC
Always do ECC with unsatisfactory colposcopy

High grade features: Snow white epithelium

Low grade colposcopic features: colour
The acetowhite reaction is slower in onset and more transient than high grade lesions
Semi-transparent
Snow-white colour
Gray-white colour higher grade

Low grade: colour

Low grade Colposcopic features: size / position
Peripheral lesions
Often smaller

Low grade Colposcopic features: size / position

Low grade Colposcopic features: margins
Feathered
Geographic
Flat with indistinct margins
Satellite lesions

Colposcopic features: margins

Low grade Colposcopic features: margins

Low grade Colposcopic features: margins

Colposcopic features: iodine staining

Colposcopic features: iodine staining

Colposcopic features: iodine staining

Colposcopic features: iodine staining
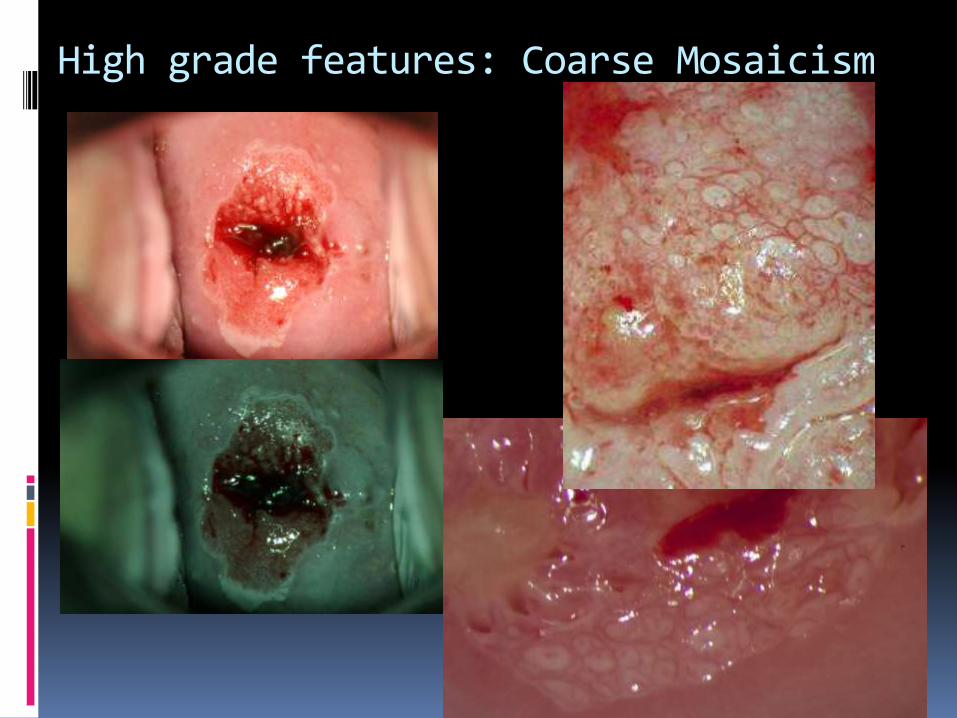
High grade features: Coarse Mosaicism

Low grade Colposcopic features: vessels
Ill defined areas of fine punctation or mosaicism
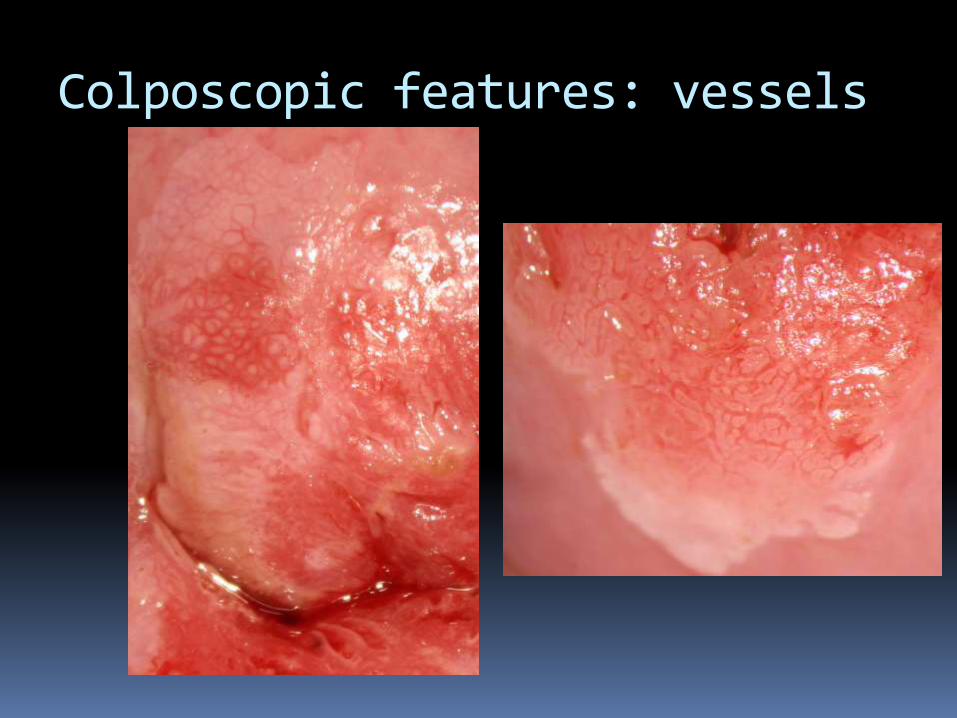
Colposcopic features: vessels
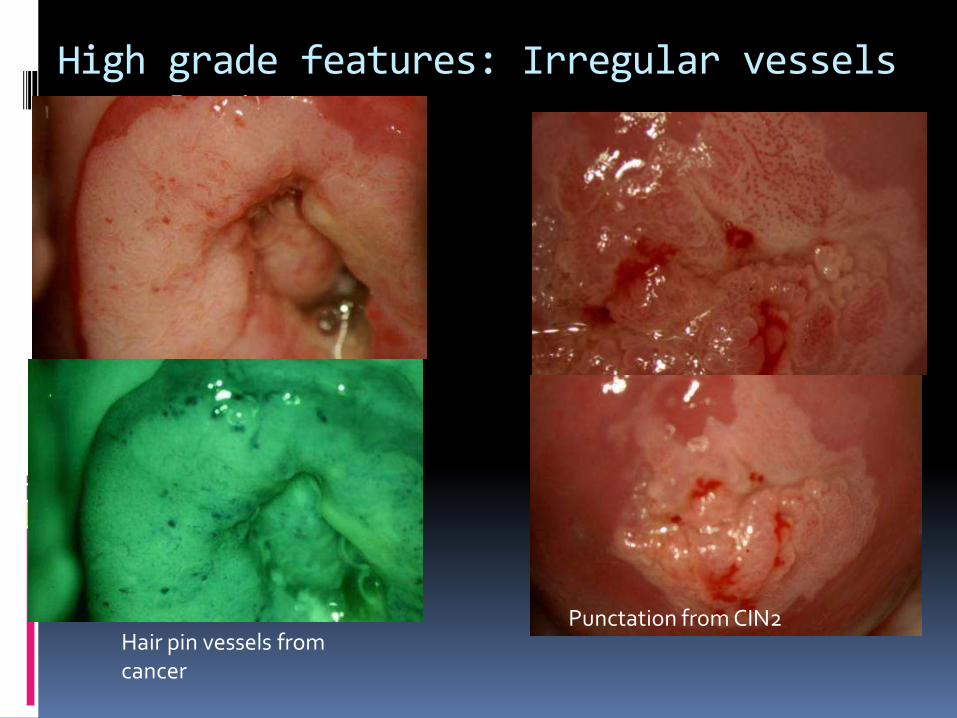
High grade features: Irregular vessels vascularity
Hair pin vessels from cancer
Punctation from CIN2

High grade features: Thick keratosis
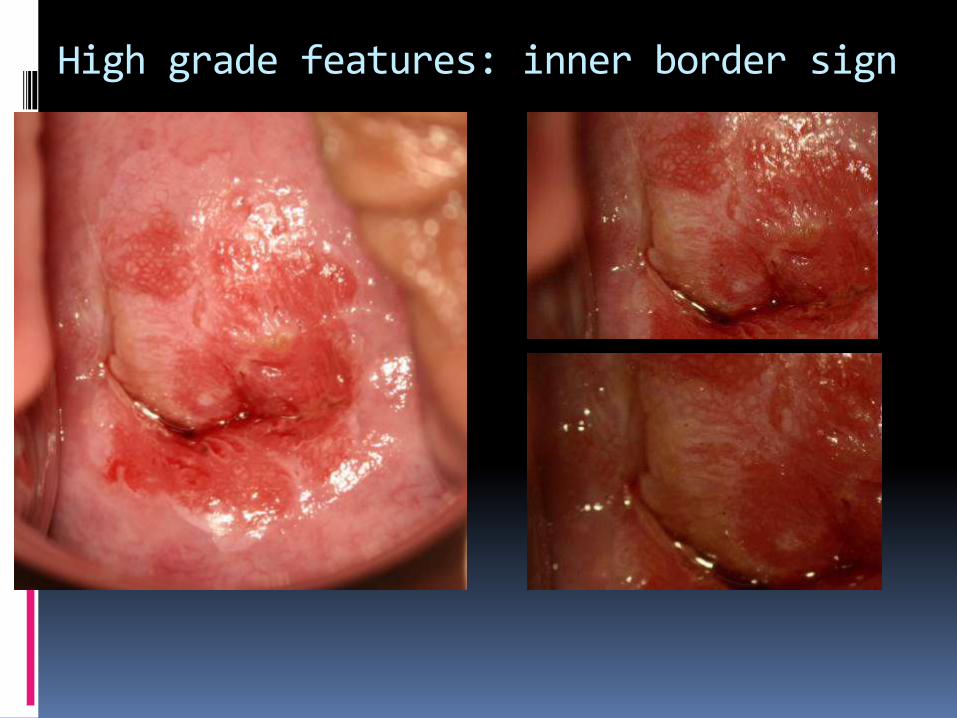
High grade features: inner border sign

High grade features: ridge sign

High grade features: papillary lesion; sharp border

CIN3
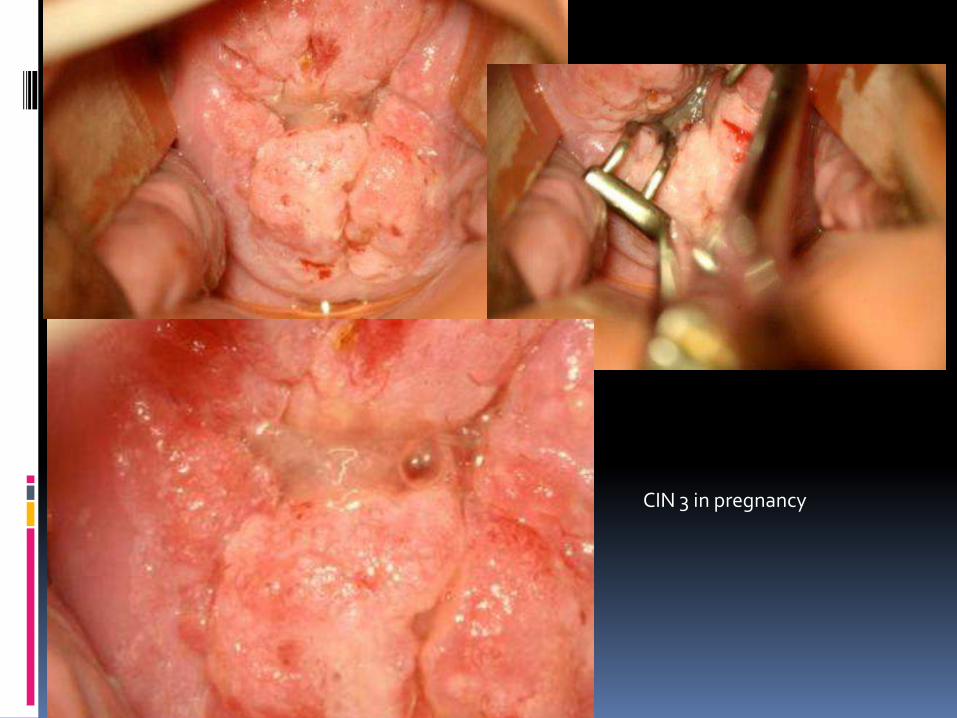
CIN 3 in pregnancy

Colposcopic mimics of CIN 1

CIN 2Photo courtesy of Dr L Geldenhuys
Histology of CIN 2
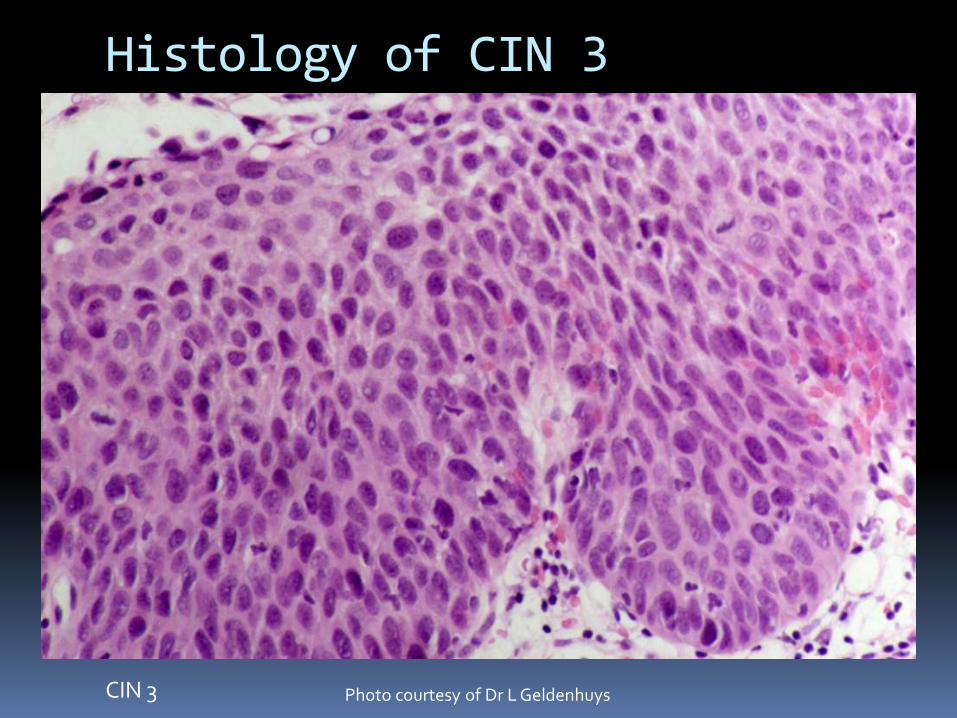
CIN 3 Photo courtesy of Dr L Geldenhuys
Histology of CIN 3

CIN 1 on Biopsy or ECC
Satisfactory Colposcopy
Observe with
Colposcopy and cytology
Q 6/12 x2
Return to screening protocol
Unsatisfactory Colposcopy
Observe with Colposcopy
and cytologyat 24 months2
Treatment1
1 consider ablative therapy for persistent CIN12 if cytology persists continue FU in colposcopy
Colposcopy and cytology -ve
CIN persists or progresses
Observe with Colposcopy
and cytology12 months
persistent
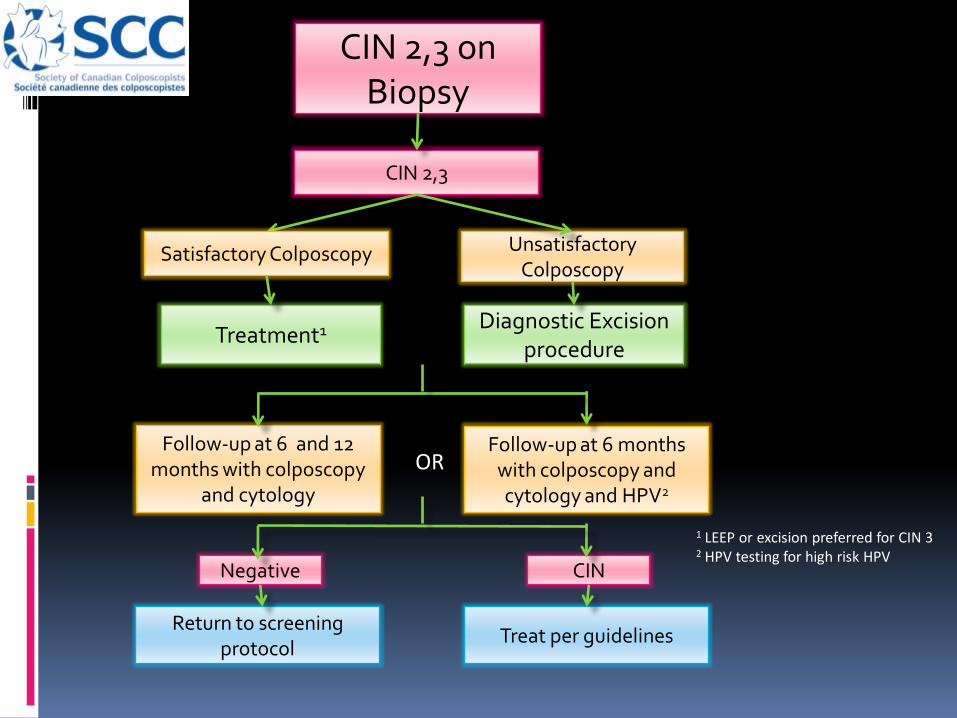
CIN 2,3 on Biopsy
Return to screening protocol
Diagnostic Excision procedure
CIN 2,3
Treatment1
Satisfactory Colposcopy Unsatisfactory Colposcopy
Follow-up at 6 and 12 months with colposcopy
and cytology
Follow-up at 6 months with colposcopy and cytology and HPV2
OR
Treat per guidelines
CIN Negative
1 LEEP or excision preferred for CIN 32 HPV testing for high risk HPV

CIN 2,3 on Biopsy in women < 25 yrs old
CIN 2
Return to screening protocol
Diagnostic Excision procedure
CIN 3
Observe with Colposcopy
and cytologyQ 6/12 x2 yrs
Treatment
Satisfactory ColposcopyUnsatisfactory
Colposcopy
CIN persists or progresses
CIN Resolves

CIN 3 with AIS (on final LEEP)

HSIL pap: colposcopic view after acetic acid
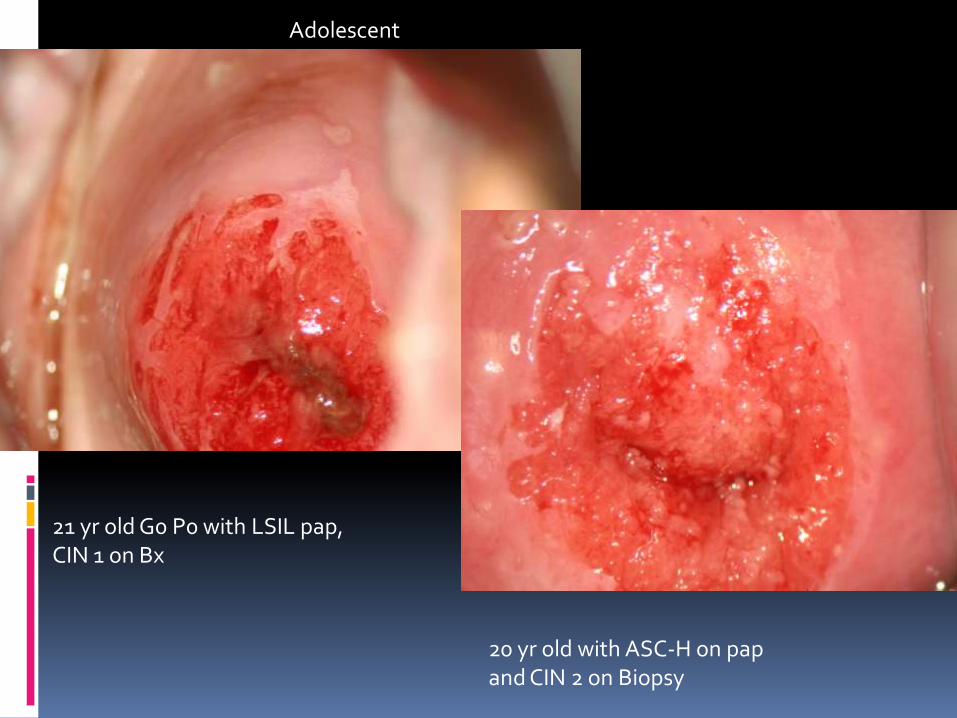
21 yr old G0 P0 with LSIL pap, CIN 1 on Bx
20 yr old with ASC-H on pap and CIN 2 on Biopsy
Adolescent

Conclusion
CIN 1 does not warrant therapy as most will resolve spontaneously
CIN 3 and CIN 2 are recognised cervical cancer precursors
They can be identified following both high grade and low grade cytology
The colposcopic features should allow differentiation between CIN 1 and CIN 2/3