2-hour functional exams printassessmtrehabmsdisorders.s3.amazonaws.com/ppt slides.pdf · of...
TRANSCRIPT

8/20/13
1
Functional Assessment, Rehab, and Taping of Musculoskeletal Disorders
Barton N. Bishop, DPT, SCS, CKTI, CSCS Chief Clinical Officer
Sport and Spine Rehab Kaizenovation Lifestyle
Functional vs. Structural
• Structural faults treated with functional treatment
Functional vs. Structural
• Need to treat the deficit appropriately"• Functional faults require functional treatment"• Structural faults require structural treatment

8/20/13
2
Structural Deficits
• Joint dysfunction"• Malalignment"• Fractures
Functional Deficits
• Poor posture"• Inhibition of a muscle"
• Phasic Chain"• Muscle over facilitated"
• Tonic Chain"• Inability to do sport, skill, leisure, ADLs"
Treatment Paradigm
Structural Exam
Structural Treatment
Functional Exam
Functional Treatment

8/20/13
3
Janda’s Muscle Imbalance Syndromes
Treatment Paradigms
• The traditional, structural approach tends to be more “extrinsic” : Treat what we can see""• The functional approach takes a more “intrinsic” perspective to treat what we can’t see
Things we can’t see
• Proprioception"• Motor programs"• Chain Reactions"• Muscle Imbalances

8/20/13
4
Proprioception
• Joint mechanoreceptors"• Capsules & ligaments"
"• Muscular receptors"
• Gamma motor neuron & muscle spindle"
• Cutaneous receptors"• Pressure, temperature,
vibration
Structure vs. Function
• Proprioception"• Hilton’s Law : a nerve that
innervates a joint also tends to innervate the muscles that move the joint, as well as skin and fascia
37
Structure vs. Function
• Hilton’s Law example"• Musculocutaneous nerve
supplies elbow joint with pain and proprioception fibers. It also supplies biceps, brachioradialis, and skin.
38

8/20/13
5
The musculoskeletal & central nervous systems function as one unit:
The SENSORIMOTOR SYSTEM
Any lesion within the system is reflected by adaptive changes elsewhere in the system
Sensorimotor System
SENSORY INPUT"Visual"Vestibular"Proprioceptive"Exteroceptive
MOTOR OUTPUT"Muscle Facilitation"Muscle Inhibition
CNS PROCESSING CNS
PNS
Chain Reactions
• Muscular Chains"• Slings : continuous connections
through muscle, fascia, and bone"• Synergists & Antagonists interconnected
in closed tensegrity system"• Integral links for movement"
41

8/20/13
6
Chain Reactions • Neurological Chains"
• Upper Quarter Co-Activation (Janda)"• Tonic Chain"
• flexion, internal rotation, adduction, pronation""
• Phasic Chain"• extension, external rotation, abduction, "supination
function: prehension, reaching, grasping
Chain Reactions • Lower Quarter Co-Activation (Janda)"
• Tonic chain"• ankle PF & INV, hip flexion, internal rotation & adduction""
• Phasic chain"• ankle DF & EV, hip external rotation & abduction
function: creeping, crawling, gait
Upper Quarter Chains
Tonic Chain ! Phasic Chain
• pectoralis major"• upper trapezius"• levator scapula"• masseter/lat.
pterygoid"• SCM"• Scalenes"• suboccipitals"• UE flexors
• serratus anterior"• rhomboids"• middle/lower
trapezius"• deep neck flexors"• upper limb
extensors

8/20/13
7
Lower Quarter Chains
gastroc-soleus"tibialis posterior"hip adductors"hamstrings"rectus femoris"iliopsosas"TFL"piriformis"thoracolumbar extensors"quadratus lumborum"
peroneals"tibialis anterior"Vastus medialis/lateralis"gluteus medius/minimus"gluteus maximus"Transverse abdominus"
Tonic Chain Phasic Chain
Muscle imbalance is a systematic and predictable response of the motor system
Changes in the system will be reflected by adaptive responses within the system
Tonic muscles are prone to tightness
Phasic muscles are prone to weakness
Tonics are Too Tight
Phasics Fail to Fire

8/20/13
8
Flexors (Tonic)Prone to tightness / shortness
o gastroc-soleus"o tibialis posterior"o hip adductors"o hamstrings"o rectus femoris"o iliopsosas"o TFL"o piriformis"o thoracolumbar
extensor "
o quadratus lumborum"o pectoralis major"o upper trapezius"o levator scapula"o masseter/lat pterygoid"o SCM"o Scalenes"o suboccipitals"o UE flexors
Extensors (Phasic)Prone to weakness / lengthening
• peroneals"• tibialis anterior"• vastus medialis/
lateralis"• gluteus medius/
minimus"• gluteus maximus"• transverse abdominus
• serratus anterior"• rhomboids"• middle/lower
trapezius"• deep neck flexors"• upper limb
extensors
Muscle Imbalance & Joint Pathology

8/20/13
9
Joint Dysfunction
Unbalanced"
Forces
Abnormal Joint"Biomechanics
Abnormal"movement "pattern
Altered"
motor program
Vicious Cycle of Muscle Imbalance
Structural v. Functional Pathology
• “Dysfunction” (Lund et al, 1991)"• Characteristic of several types of musculoskeletal pain"• Neurophysiological model, based on afferent input"• Muscle Imbalance"
• Agonists become inhibited"• Antagonists become facilitated"
• Normal protective adaptation; NOT the cause of pain
Typical muscle response to joint dysfunction is similar to spastic muscles
in structural CNS lesions
Usually develops with muscle inhibition in other muscles, resulting in a muscle imbalance.

8/20/13
10
Presence of Janda’s Crossed Syndromes indicates the
presence of CNS-mediated muscle imbalance
Requires treatment of the Sensorimotor System
Janda’s Upper Crossed Syndrome
WEAK"Cervical "Flexors
TIGHT"Pectorals
TIGHT"Suboccipitals"UpTrap/Levator
WEAK"Rhomboid"Lower Trap
Janda’s Lower Crossed Syndrome
WEAK"Abdominals
TIGHT"Hip Flexors
TIGHT"Thoraco-lumbar"Extensors
WEAK"Gluteus Max

8/20/13
11
Janda’s Layer Syndrome
• Combination of both upper and lower crossed syndromes"
• Marked impairment of the motor regulation"
• Sign of poorer prognosis due to longstanding dysfunction
Functional Exam, Rehab, Treatment Cervico-Thoracic
Mouth Opening Screen"Instruc(ons
Patient seated or standing comfortably. Patient to open the mouth as wide as possible. Watch the upper cervical spine
Clinical Ra(onale Shows overactivity of suboccipitals
Failure Exercise Recommenda(ons Pain or inability to open at least 3 fingers wide. Viewing from side, look for any anterior translation of the occiput = suboccipital over activity
Thoracic extension to position c-spine in neutral shutting off suboccipitals; Upright Head Nod; dynamic cervical isometrics – extension
8/20/13
12
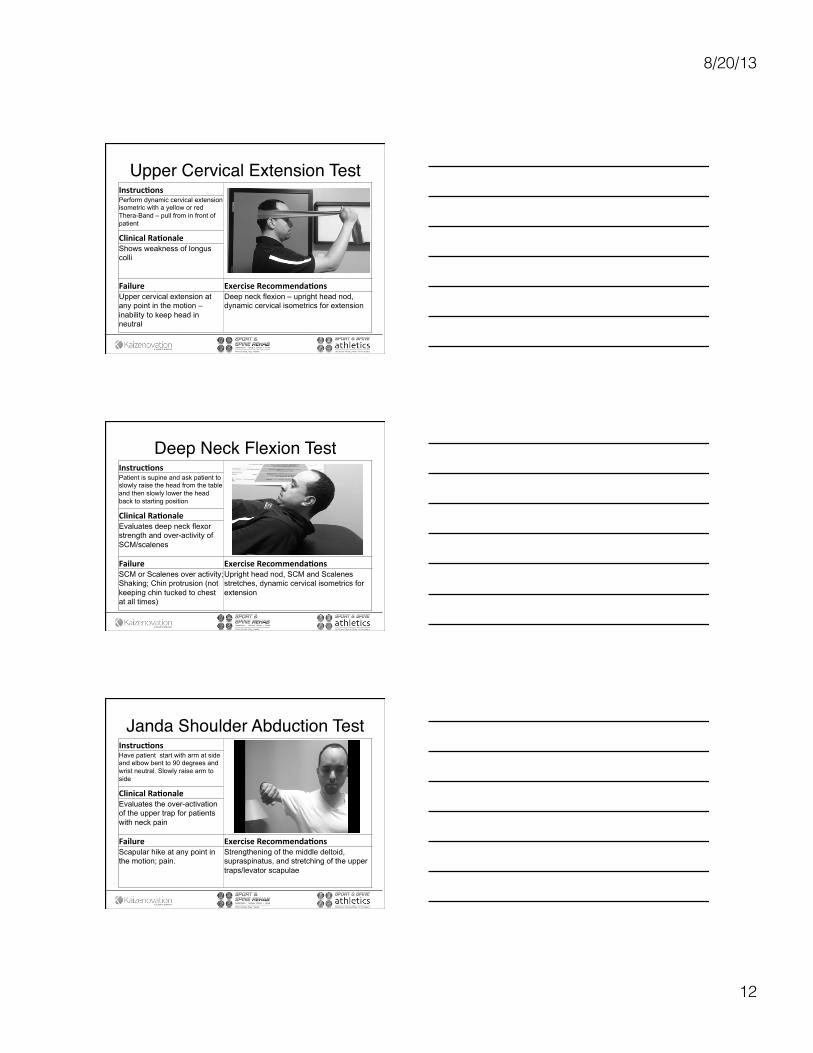
Upper Cervical Extension Test"Instruc(ons
Perform dynamic cervical extension isometric with a yellow or red Thera-Band – pull from in front of patient
Clinical Ra(onale Shows weakness of longus colli
Failure Exercise Recommenda(ons Upper cervical extension at any point in the motion – inability to keep head in neutral
Deep neck flexion – upright head nod, dynamic cervical isometrics for extension
Deep Neck Flexion Test"Instruc(ons
Patient is supine and ask patient to slowly raise the head from the table and then slowly lower the head back to starting position
Clinical Ra(onale Evaluates deep neck flexor strength and over-activity of SCM/scalenes
Failure Exercise Recommenda(ons SCM or Scalenes over activity; Shaking; Chin protrusion (not keeping chin tucked to chest at all times)
Upright head nod, SCM and Scalenes stretches, dynamic cervical isometrics for extension
Janda Shoulder Abduction Test"Instruc(ons
Have patient start with arm at side and elbow bent to 90 degrees and wrist neutral. Slowly raise arm to side
Clinical Ra(onale Evaluates the over-activation of the upper trap for patients with neck pain
Failure Exercise Recommenda(ons Scapular hike at any point in the motion; pain.
Strengthening of the middle deltoid, supraspinatus, and stretching of the upper traps/levator scapulae

8/20/13
13
Thoracic Extension Screen"Instruc(ons
Stand against wall with heels 1-2 inches away from wall; raise arms up (lats) or elbows at 90 degrees (Pecs)
Clinical Ra(onale Evaluates thoracic extension which lack of puts the upper cervical spine in extension and the lower c-spine in flexion
Failure Exercise Recommenda(ons Inability to flatten TL junction without losing wall contact; Note where tension occurs when performing; Pain
W-Vs, Wall Angels, Standing Jacks, Lat Stretches
Push Up Screen"Instruc(ons
In push up position, on toes or knees, lower and rise up, then shift from side to side and shift superolaterally
Clinical Ra(onale Evaluates the activation of the serratus anterior and lower and middle traps
Failure Exercise Recommenda(ons Scapula wings (unilateral more significant); Inability to perform
Depends on failure – medial border: serratus ant and mid trap exercises; inferior angle: lower trap vector, scap/sagittal flex-bar oscillation
90/90 ER With and Without Retraction"Instruc(ons
Have patient stand naturally, abduct arm to 90 degrees and externally rotate. Measure range. Redo motion after doing scapular retraction
Clinical Ra(onale Have patient stand naturally, abduct arm to 90 degrees and externally rotate. Measure range. Redo motion after doing scapular retraction
Failure Exercise Recommenda(ons Range should be more than 85 degrees with retrac6on. Without retrac6on it should be at least 90 degrees of external rota6on
Scap stab strengthening – lower trap vector, rows, serratus progression, Y-I-T. External rotation, sword. ER stretching

8/20/13
14
Functional Examinations and Appropriate Rehabilitation Exercises Low Back/Lower Quarter
Overhead Deep Squat Test"Instruc(ons
Have patient hold bar over head, feet shoulder width, toes straight and squat down keeping bar over head and heels on ground
Clinical Ra(onale Evaluates hip, ankle, and thoracic spine mobility as well as core strength
Failure Exercise Recommenda(ons Pain, Inability to break horizontal with thighs, weight shift, or bar comes forward. Knee valgus during any part
Depends on Failure: Core strengthening, hip mobility, ankle dorsiflexion mobility, glute med/max strengthening, thoracic extension mobility
Single Leg Squat"Instruc(ons
Have patient stand on one leg and perform a squat. Have them do repeatedly. Stand on 6-8 inch stepand touch the heel of other foot to floor
Clinical Ra(onale Evaluates activation of the gluteus medius, maximus, quadriceps, and soleus length
Failure Exercise Recommenda(ons Knee pain, valgus of knee, excessive foot pronation, trendelenburg, body lean, Heel lifts
Clams, fire hydrants, step down, running man, bowler’s squat, single leg stance activities, soleus stretching

8/20/13
15
Step Down Test"Instruc(ons
Stand on 6-8 inch step. Step down and touch the heel of the other foot to the floor
Clinical Ra(onale Evaluates activation of the foot instrinsic musculature
Failure Exercise Recommenda(ons Pain, Heel raises up, Valgus knee load, Trendelenburg
Soleus stretch, glute med strengthening, quadriceps/VMO strengthening
Forward Lunge Screen"Instruc(ons
Patient performs forward lunge
Clinical Ra(onale Evaluates activation of the gluteus medius, quadriceps, and hip mobility
Failure Exercise Recommenda(ons Valgus knee load, excessive knee flexion (knee anterior to ankle), knee pain, inability to maintain upright trunk
Depends on failure – glute med/max strengthening, core stabilization, quadriceps strengthening
Single Leg Stance Test"Instruc(ons
Stand on one leg, look straight ahead, opposite leg ideally at hip height and not touching stance leg. Get balance with eyes open, then close eyes
Clinical Ra(onale Evaluates balance, core stability, and glute medius stability
Failure Exercise Recommenda(ons Trendelenburg (loss of height), gain of height, inability to maintain balance for minimum of 15 seconds
Depends on failure – glute strengthening, core, or balance training

8/20/13
16
Lat Length Test"Instruc(ons
Patient stands with back against wall with feet forward. Raise arms up to touch thumbs to walls. Move supine to table and repeat if unable to perform. Then flex knees to chest.
Clinical Ra(onale Evaluates lat dorsi length as well as thoracic extension and diaphragm weakness
Failure Exercise Recommenda(ons Pain, inability to touch walls with thumbs with head to sacrum touching wall
Lat stretch, thoracic extension exercises, diaphragmatic breathing exercises/retraining
Thoracic Rotation Test"Instruc(ons
Hold bar in front of body and rotate to each direction while sitting. Then Hold bar behind back through arms and rotate again
Clinical Ra(onale Evaluates the mobility of the thoracic spine in rotation
Failure Exercise Recommenda(ons Pain. <50 degrees rotation with bar in front, <45 degrees with bar behind, loss of >20 degrees from front to back
Thoracic rotation strengthening (if active insufficiency); Assisted thoracic rotation; Scapular stabilizer exercises
Vleeming’s Active and Resistive SLR Test"Instruc(ons
Have patient lift one leg 20 cm off table keeping it straight. Switch sides. Then perform again and provide resistance. Finally, do again after asking patient to brace.
Clinical Ra(onale Evaluates core stability via activation of the transverse abdominus or obliques
Failure Exercise Recommenda(ons Pain or pelvis rotates in any part of the motion on either side. Unilateral failure is more significant.
Ab Bracing; New Abs; Multi-Planar Vertical Stabilization; Abdominal activation via posterior weight shift with band (all depends on patient’s ability to stabilize after activation

8/20/13
17
Janda Hip Extension Test"Instruc(ons
Patient prone on table, keeps leg straight and extends hip. Palpate hamstrings, glute max, and contralateral lumbar paraspinals
Clinical Ra(onale Evaluates activation of the glute max, paraspinals, and hamstrings
Failure Exercise Recommenda(ons Delay of glute max and excessive firing of lumbar paraspinals and/or hamstrings; early anterior pelvic tilt
Glute max strengthening – 4-way hip, glute squeezes, running man, squats
Janda Hip Abduction Test"Instruc(ons
Patient sidelying on table. Expose waist and have patient abduct leg. Watch for the belt line to stay in place
Clinical Ra(onale Evaluates activation of the gluteu medius to create hip abduction
Failure Exercise Recommenda(ons Belt line moving toward ribs (activation of QL), external rotation of toes or flexion of hip
Glute med strengthening – 4-way hip, clams, monster walk, running man, bowler’s squat
Single Leg Bridge Test"Instruc(ons
Patient supine on floor (not table if possible) and performs a bridge (arms on chest or up). In bridge, one leg is kicked straight. Hold this position for 10 seconds
Clinical Ra(onale Evaluates glute max activation over hamstring and lumbar paraspinals
Failure Exercise Recommenda(ons Pelvis drops to ground, hamstring cramps, pelvis rotates, lower back pain, can’t hold for 20 seconds
Glute max activation – bridges, glute sets, 4-way hip, hip hinging running man, bowler’s squat
8/20/13
18
Vele’s Reflex"Instruc(ons
Patient standing in bare feet and they fall forward until they start to fall. Ask the patient to catch his/herself. Watch the toes for gripping into the ground.
Clinical Ra(onale Evaluates activation of the foot instrinsic musculature
Failure Exercise Recommenda(ons Delayed firing of the foot intrinsics (unilateral is worse)
Ski jumpers, Janda short foot, rolling towel, marble pick up, brushing sole of foot with a comb
Common Glute Exercises
MSSE 2013 TRAC Preceedings 2013
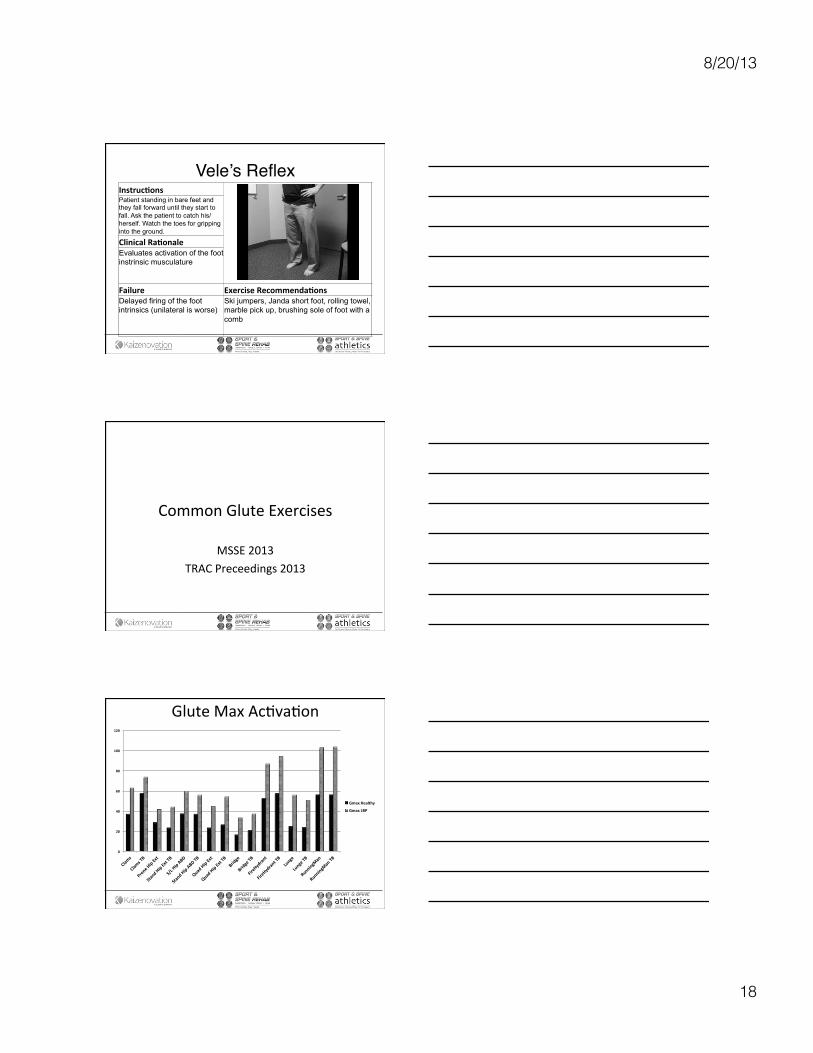
Glute Max Ac6va6on
0
20
40
60
80
100
120
Clams
Clams TB
Prone Hip Ext
Stand Hip Ext TB
S/L Hip ABD
Stand Hip ABD TB
Quad Hip Ext
Quad Hip Ext TB
Bridge
Bridge TB
FireHydrant
FireHydrant TB
Lunge
Lunge TB
RunningMan
RunningMan TB
Gmax Healthy
Gmax LBP

8/20/13
19
Glute Med Ac6va6on
0
10
20
30
40
50
60
Clams
Clams TB
Prone Hip Ext
Stand Hip Ext TB
S/L Hip ABD
Stand Hip ABD TB
Quad Hip Ext
Quad Hip Ext TB
Bridge
Bridge TB
FireHydrant
FireHydrant TB
Lunge
Lunge TB
RunningMan
RunningMan TB
Gmed Healthy
Gmed LBP
Fire Hydrants
Clams

8/20/13
20
Running Man
Principles of Propriocep6ve Taping
• Not all tapes are the same • Tape the area that you exercise/massage • Tape for the pain AND the cause of the pain • Think globally, act locally (and globally)
Taping to Inhibit Internal Rotators

8/20/13
21
Taping to Facilitate Posterior Cuff
Taping to Facilitate Posterior Cuff
Taping to Facilitate Lower Traps
