2 dr mughals rickets talk - manchester university nhs ... dr mughals rickets talk.pdf · rickets...
TRANSCRIPT

Rickets
Zulf Mughal
Consultant in Paediatric Bone Disorders
Department of Paediatric Endocriology
Royal Manchester Children's Hospital
Manchester
M13 0JH
Bone Study Day, 28th September 2012

Overview
� What is Rickets?
� Vitamin D Deficiency Rickets
� Calcium Deficiency Rickets
� Vitamin D Dependent Rickets type I & type II
� X-Linked Hypophosphataemic Rickets
What is Rickets ?

Rickets – Historical Perspective
Francis Glisson - "De Rachitide” 1650
� 19th CENTURY - Rickets rampant among the poor children living in the industrialised & polluted northern cities
� “Disappearance of Rickets” in early 20th
Century:� Cod-liver oil supplements in 1930s
� Improvement in nutrition
� Pollution control measures
� Recent resurgence of Rickets

Normal Growth Plate Rachitic Growth Plate
Apoptosis of
Hypertrophic
Chondrocytes
caused by
PHOSPHATE ions
HYPOPHOSPHATEMIA
No Apoptosis of
Hypertrophic
Chondrocytes

What is Rickets ?
Impaired Apoptosis of Terminally Differentiated Chondrocytes in the Growth Plate
Responsible for Clinical & Radiological Signs of Rickets

What is Rickets ?
Vitamin D Related Rickets
- Vitamin D Deficiency
- Impaired Hepatic 25-hydroxylation
- Impaired Renal 1α-hydroxylation of 25(OH)D
- End organ resistance to 1,25(OH)2D
Rickets due to Dietary Calcium Deficiency
Calcipaenic Rickets Phosphopaenic Rickets
Hypophosphataemic Rickets
- X-linked Dominant (PHEX gene mutation)
- Autosomal Dominant (FGF23 mutation)
- Autosomal Recessive Type 1 (DMP1mutation)
- Autosomal Recessive Type 2 (ENPP1mutation)
- With Hypercalciuria (SLC34A3 gene mutation)
- Associated with:
(a) McCune-Albright syndrome
(b) Tumour induced osteomalacia
(c) Linear nevus sebaceous syndrome
-
Raised PTH
Renal Phosphate Wastage
Hypophosphatemia
Impaired Apoptosis of Terminally Differentiated Chondrocytes in the Growth Plate
Mughal. Curr Osteoporos Rep. 2011;9(4):291-9

Calcipaenic Rickets
Vitamin D Related Rickets
� Vitamin D Deficiency Rickets
� Impaired Hepatic 25-hydroxylation
� Vitamin D Dependent Rickets Type I (Impaired Renal
1α-hydroxylation of 25(OH)D)
� Vitamin D Dependent Rickets Type II (End organ resistance to
1,25(OH)2D)
Rickets due to Dietary Calcium Deficiency

Vitamin D Deficiency Rickets

Vitamin D Deficiency in Adolescents
� Tetany & Convulsions
� Limb pains
� Lower limb & pelvic deformities
� Proximal myopathy

Biochemical Changes in Vitamin D Deficiency
Early vitamin D deficiency:
25(OH)D Ca Normal
PTH ↑ P
1,25(OH)2D ↑ ALP ↑
Severe vitamin D deficiency:
25(OH)D Ca
PTH ↑ ↑ P
1,25-(OH)2D ALP ↑ ↑
Occasionally PTH resistance: Ca P ↑, 25(OH)D
PTH ↑↑ & 1,25-(OH)2D
Archives of Disease in Childhood. 2009; 94:932-937

Radiological Changes
Rx
Vitamin D3
+
Calcium

Treatment of Vitamin D Deficiency Rickets
� Oral vitamin D2 or D3, 3000 - 6000 i.u./day for 6 to 8 weeks
� Oral calcium supplements if necessary
� Monitoring:
� Improvement in symptoms (~ 2weeks)
� ↓ in serum PTH & alkaline phosphatase
� ↑ in serum phosphate, calcium & 25(OH)vitamin D
� Radiological healing (~ 3 months)
� Improvement of bow legs or knock-knees (~ 2 years)
� Provide vitamin D supplements (~ 400 iu/day) after the rickets
has healed

Armas, L. A. G. et al. J Clin Endocrinol Metab 2004;89:5387-5391
Time course of the rise in serum 25OHD after a single oral dose of 50,000 IU of either cholecalciferol (vitamin D3) or ergocalciferol (vitamin D2) to two groups of 10 normal men each
Vitamin D3 or Vitamin D2 ?

Prevention of Vitamin D Deficiency

Vitamin D supplementation During Pregnancy,
Lactation & Infancy
DOH
� All 0 to 6 months – 340 i.u/day or 8.5 mcg/day
(Not necessary for formula fed infants unless volume
< 500 mls/day)
� All 7 months to 5 years – 280 i.u/day or 7 mcg/day
� Adolescents at risk of vitamin D deficiency - 400 i.u/day
or 10 mcg/day
� All pregnant & lactating mothers - 400 i.u/day or 10 mcg/day

(www.healthystart.nhs.uk)
Children’s Healthy Start Vitamin drops
contain (5 drops daily):
• 233 micrograms of vitamin A
• 20 milligrams of vitamin C
• 7.5 micrograms of vitamin D3

Calcium Deficiency Rickets

Rickets Due to Calcium Deficiency
Wind-swept Abnormality due to Calcium
Deficiency Rickets – taken from a
review by Dr John Pettifor
Oginni et al Archives of Disease in Childhood. 2003;88:812-817

Severe Calcium Deficiency Rickets
16th March 2012
Age 19 months 23 months
20 12 2011 04 04 2012
Ca mmol/l 2.36 2.39
ALP iu/l 1023 1301
P mmol/l 1.01 0.79
PTH pg/ml (11-35) 192 465
25OHD2nmol/l 70.6
25OHD3nmol/l <15
• Male infant born to Somali parents
• Breast fed from birth
• Allergic to dairy, eggs & fish
• Weaned mainly on pasta, rice,
potatoes & small amount of meat
• Dalivit 0.6 mls daily
• Calcium supplements prescribed
• Presented with delayed walking
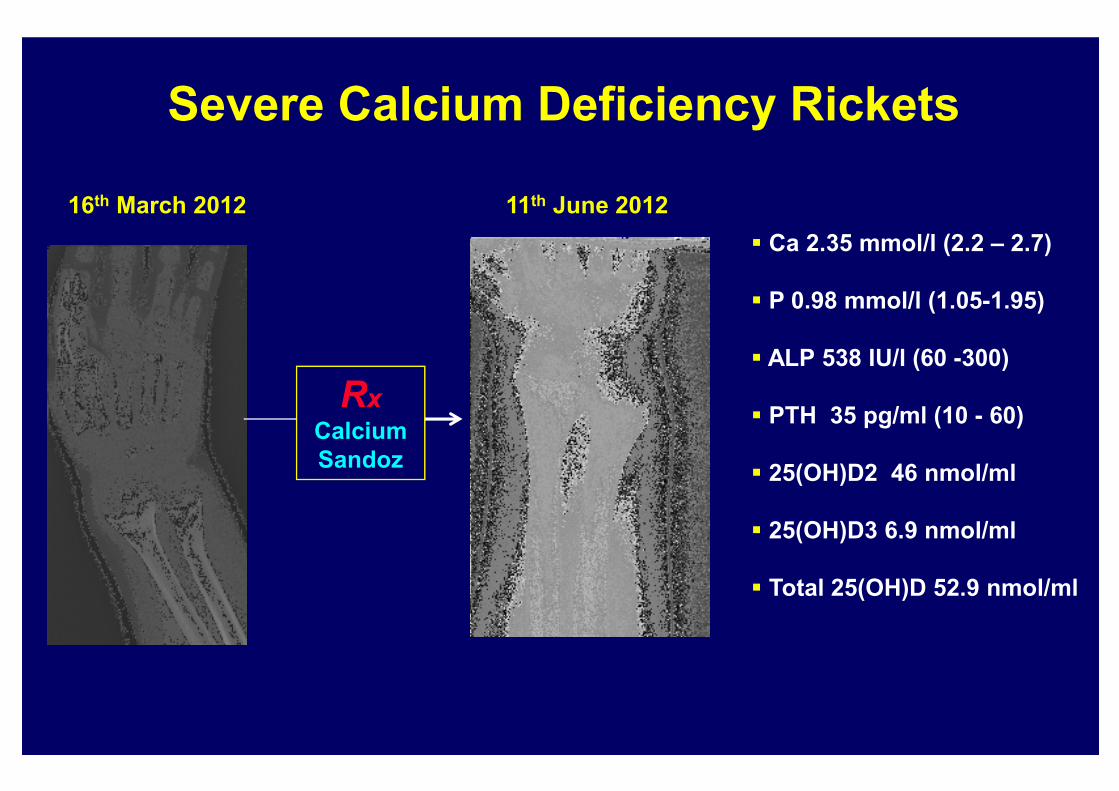
Severe Calcium Deficiency Rickets
16th March 2012 11th June 2012
� Ca 2.35 mmol/l (2.2 – 2.7)
� P 0.98 mmol/l (1.05-1.95)
� ALP 538 IU/l (60 -300)
� PTH 35 pg/ml (10 - 60)
� 25(OH)D2 46 nmol/ml
� 25(OH)D3 6.9 nmol/ml
� Total 25(OH)D 52.9 nmol/ml
Rx
Calcium
Sandoz
Vitamin D Dependent Rickets (VDDR)
Type I & Type II

VDDR Type I
� Corr Ca 2.02 mmol/l
� P 0.59 mmol/l (1.1 – 2.0)
� ALP 3636 IU/l (100 - 733)
� PTH 1087 pg/ml (10 - 60)
� 25(OH)D 31 ng/ml
� 1,25(OH)2D < 10 pg/ml (20 - 50)
September 2005 - 16 month old child with severe Rickets
Known inactivating
mutations in
the CYP27B1 gene

Vitamin D Dependent Rickets Type I & Type II
VDDR Type I
� Physiological doses of calcitriol (1,25(OH)2D) or alphacalcidiol
VDDR Type II
� Pharmacological doses of calcitriol or alphacalcidiol
(e.g. 3-6 mcg/day)
+
Oral calcium – 2 to 3 grams/day
� Long-term treatment calcium infusions (especially patients
with alopecia )
