2-5_health_literacy
TRANSCRIPT

Health Literacy and Hearing HealthcareBarbara E. Weinstein, Ph.D.Jennifer Gilligan, B.A.Samantha Morgan, B.ADeborah von Hapsburg, Ph.D.

Lecture Goals
Goal 1: To define health literacy and introduce how low health literacy is linked to patient outcomes
Goal 2: To examine how health literacy impacts patient behaviors such as:
• self management,• behavior change and internal motivation• self efficacy
Goal 3: To introduce methods clinicians can use to assess health literacy across multimodal domains
Goal 4: To learn the importance of using appropriate health literate patient materials, including counseling and decision aids, across multimodal domains for diverse populations

How often do you need to have
someone help you when you read instructions,
pamphlets or other materials provided by your doctor or
pharmacy?
Always
Often
Sometimes
Rarely
Never
Modified from:http://champ-program.org/static/SILS_Tool.pdf
Single Item Literacy Screener (SILS)

Class Activity
1. Reflect on a time in which you visited a physician or healthcare provider and your diagnosis, test results, or treatment plan was discussed in unfamiliar terms.
2. What factors contributed to you not understanding what the health professional communicated?
3. How did that make you feel? And why?

Ethnography/Re-Enactment

IOM (2004)
Oral Literacy: listening and speaking skillsPrint Literacy: reading and writing abilitiesNumeracy: competency when working with numerical values Cultural and conceptual knowledge: familiarity with the social and conceptual constructs of a given context
Literacy and Its Components
Literacy
Cultural and Conceptual Knowledge
Listening Speaking Writing Reading Numeracy
Oral Literacy Print Literacy
Contexts

→ The global literacy rate has been estimated at 84%
Countries in which Literacy rates are
below 50%
Regions in which average Literacy rates
are above 90%
Afghanistan Benin Burkina Faso Central African Republic Chad Côte d’Ivoire Ethiopia Guinea Haiti Liberia Mali Mauritania Niger Sierra Leone
Central and Eastern EuropeCentral Asia
East AsiaThe Pacific
Latin AmericaThe Caribbean
What Does Literacy Look Like Globally?
UNESCO (2014)

Health Literacy is:The degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions
A Prescription to End Confusion
US Department of Health and Human Services (2000)
What Is Health Literacy?

I need a cochlear WHAT?
Content and Context
Content and context each have an impact on health literacyDifferent health contexts require different knowledge bases• A patient with above-average health literacy may have
poor health literacy skills when confronted with a new health context that contains novel content.
• A new patient, regardless of low literacy risk factors, should be counseled using plain language and material consistent with low health literacy levels, as the contect and context of the situation may be novel.
McCaffery et al. (2012)I need a cochlear WHAT?

Health and Literacy
Literacy impacts:• Health knowledge• Health status• Access to health services• Health outcomes• Variety of Stakeholders: patient, providers, governments,
manufacturers of medical equipment, society, etc.
Several socioeconomic factors impact health status:• Income level• Occupation• Education• Housing• Access to medical care
Poor health literacy is a stronger predictor of a person's health than age, income, employment status, education level, and race
Schillinger (2002)
• Navigate the healthcare system, including locating providers and services and filling out forms
• Share personal and health information with providers
• Engage in self-care and chronic disease management
• Adopt health-promoting behaviors, such as not smoking and eating a healthy diet
• Act on health-related news and announcements
• Adopt preventative measures
•
Health Literacy Affects People’s Ability To:

Australia: • 60% of adults were below Level 3 health literacy skills• The percentage of individuals with low health literacy skills increased with age.
Canada: • 60% do not have the necessary skills to manage their health adequately.
United States:• >43% of adults have literacy levels below what they need to understand even
basic written health information • 33 % of older patients have limited health literacy
Europe• 47% of Europeans have limited health literacy• Limited health literacy varies from country to country (ex: Limited HL =
29% for Netherlands and 62% for Bulgaria)
Health Literacy Across the Globe
World Health Organization

Low Health Literacy: At-Risk Populations
Income level,
Occupation, Housing
Literacy
Access to
medical care
Health
status
Health knowled
ge
Access to
health service
s
Factors placing people at risk for low health literacy:• Speech, language, hearing, vision disorders• Cognitive or mental disorders• Non-native speakers• Elderly• Ethnic minority• Poverty• Homelessness
IOM (2004)
Audiologists face a special challenge:• Many patients have an existing or underlying
communication disorder• Many patients also belong to one or more risk categories

Person unaware of audiology services; unable to locate a provider
• Unable to effectively report/describe symptoms and psychosocial impact of hearing loss
• Can not take care of hearing aid; poor self advocacy for hearing loss
• Difficulty implementing aural rehabilitation; poor use of strategies for communication and coping
• Mislead by advertising; misunderstanding of expectations and prognoses
• May not use hearing protective devices
Low Health Literacy: Implications for Hearing Health

Discussion Point
1. Having identified risk factors/red flags of low health literacy, which of these characteristics are well represented within your patient population?

Discussion Point
2. What characteristics might older adults with hearing impairment have that put them at risk for low health literacy abilities; or older deaf adults?

Of 125 hospitalized patients…
Williams et al. (2002)
13% of patients
understood the word
‘terminal’
18% of patients
understood the word
‘malignant’
22% of patients
understood the word‘nerve’33% of
patients understood the word‘orally’
98% of patients
understood the word‘vomit’
Medical Vocabulary Knowledge

• 40-80% of medical information received is forgotten immediately
• ~50% of the information retained is incorrect
Sources: Kessels (2003); Anderson et al. (1979); Dewalt et al. (2010)
It is essential to check and confirm patient understanding across oral, printed and web-based sources of information.
Patients remember and understand less than half of what is explained to them by clinicians.
Recall, Comprehension & Health Literacy

Ethnography: What Did Kathleen’s Mother Understand?

“It is neither just, nor fair, to expect a patient to make appropriate health decisions and safely manage his/her care without first understanding the information needed to do so.”
AMA (2007)
Health Literacy: The Right to Understand

• What is the predicted health literacy of patients receiving audiological services?
• Are there significant differences present in the level of language used by patients and the average level of reading among U.S. adults?
• Are there significant differences present between the level of language used by audiologists and patients?
• Are there significant differences present in the level of patient education materials (i.e. hearing aid instruction guide) and the level of language used by audiologists?
• Are there patient demographic variables present that are good predictors of the language used by audiologists?
Impact of Health Literacy on Patient Understanding & Counseling in Audiology
Nair & Cienkowski (2010)

• 3 experienced audiologists from the university clinic• 12 adult hearing impaired participants
• Each participated in a hearing aid orientation appointment. The dialogues were videotaped and transcribed.• Some were given printed educational materials (Hearing aid
guides).
• Transcribed dialog was analysed using the Flesch-Kincaid grade level formula (FKGL) • The formula translates writing samples into a U.S. grade level
equivalent; theoretically, specifying the education level generally required to understand the sample. For example, a score of 5.3 would indicate that the writing sample should be understood by an average fifth grade student.
MethodsNair & Cienkowski (2010)
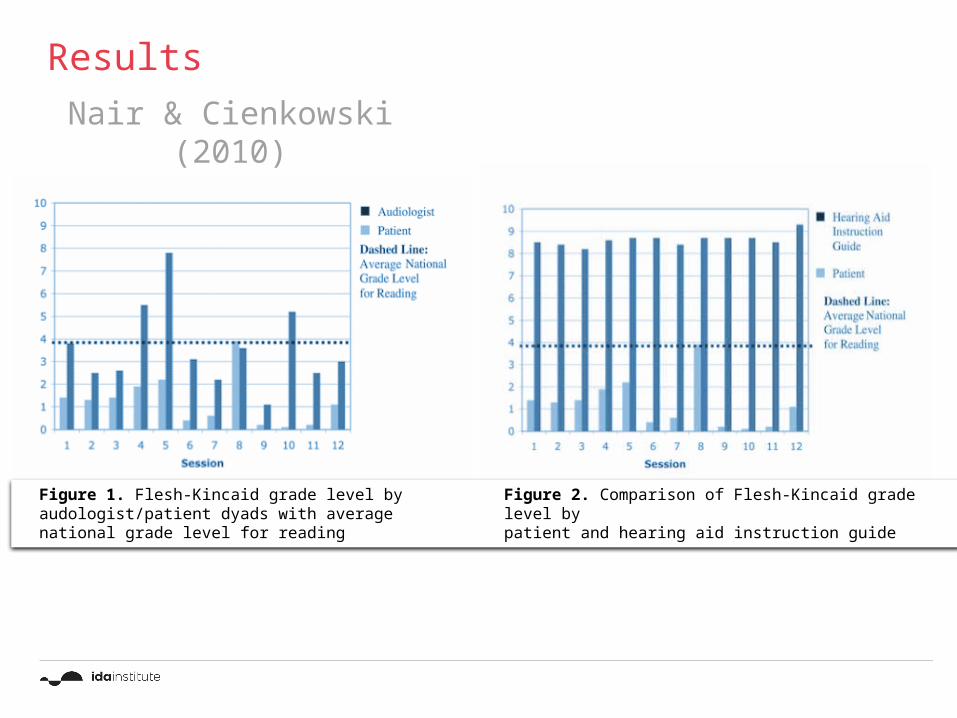
Results
Figure 1. Flesh-Kincaid grade level by audologist/patient dyads with average national grade level for reading
Figure 2. Comparison of Flesh-Kincaid grade level bypatient and hearing aid instruction guide
Nair & Cienkowski (2010)

Caposecco, Hickson & Meyer, 2012Caposecco, Hickson and Meyer (2012) investigated the suitability of hearing aid user guides for older adults. Rationale encompassed the following:• Research shows that easy-to-read materials are preferred by all
readers regardless of literacy level, with benefits including improved comprehension and shorter reading time (Davis et al, 1996).
• Well designed health-care materials that the reader is able to understand enhance self-efficacy (Doak et al, 1996). Self-efficacy refers to an individual’s belief that they have the ability to perform the skills needed to be successful at a particular behaviour (Bandura, 1997).
• Several readability formulae were utilized to determine mean reading grade level
• The Suitability Assessment of Materials (SAM) (Doak et al, 1996) instrument was used to assess the content and design of each user guide.
• 36 hearing aid user guides from 9 manufacturers were examined
Hearing Aid User Guides: Suitability for Older Adults

• 36 hearing aid user guides from 9 manufacturers
• Mean reading level was grade 9.6
• Too complex
Hearing Aid User Guides: Suitability for Older AdultsCaposecco, Hickson & Meyer, 2012

User guides not optimal
Major weaknesses based on the SAM analysis:
1.Inclusion of too many models in each user guide
2.Frequent use of uncommon vocabulary
3.Small text size and graphics
4.Excessive technical jargon
5.Problems with layout
6.No interactive stimulation
7.No option for visually impaired people
Caposecco, Hickson & Meyer, 2012
Results

• 69% of printed hearing aid user guides deemed “unsuitable”
• 90% were identified as using “excessive technical jargon” and “uncommon vocabulary”
• 33% did not include basic hearing aid functionality overviews
• 100% of the guides were printed in inappropriately small font sizes
Literature provided is NOT written at appropriate health literacy levels. As clinicians, we must provide our patients with clear, concise, informative literature presented at a level they can easily comprehend.
Health Literacy & Patient Instructional Brochures
Nair & Cienkowski (2010)

There is a great deal of scope for improvement. Poorly designed user guides may impact on HA self-efficacy, outcomes, and success
Caposecco, Hickson & Meyer, 2012Suggestions

Poor understanding of information costs time, money and frustration• Needing to make additional appointments for
clarification of hearing aid function.Poor understanding can lead negative outcomes• E.g. failure to use the hearing aid at allPoor understanding can affect self esteem• Psychological consequences of untreated hearing loss
can be far-reachingPoor understanding can negatively impact overall
health• A hearing impaired person without some form of
amplification will not thrive in group or individual conversational settings: social isolation and depression may occur
Poor understanding in the healthcare setting can lead to misunderstanding• Overall health outcomes could be negatively affected
Implications

Plain Language: Clear Communication
Everyone benefits from clear communication
Clear communication is essential to ensure patients receive plain, unbiased and culturally appropriate information that will equip them to understand their condition and make educated choices about treatment.
Information must be in accessible format and presented in a range of modalities.

Plain Language: Oral

• Use a size 14 font or larger• Leave adequate white space• Use jargon-free language• Use a grade reading level of 5 or below• Use concrete and familiar words• Emphasize key points in headings• Chunk related information• Use bulleted lists• Use simple tenses (present is best)• Use short sentences with active voice• Use relevant and simple
diagrams/graphics• Caption the graphics
•
Plainlanguage.gov (2015)
Plain Language: Printed
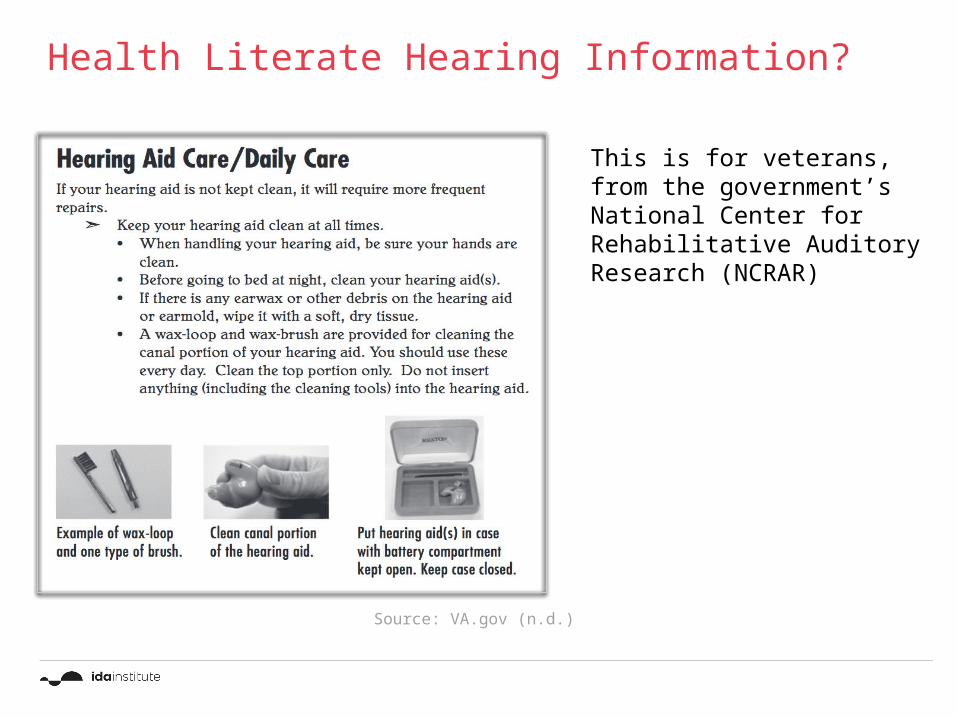
This is for veterans, from the government’s National Center for Rehabilitative Auditory Research (NCRAR)
Health Literate Hearing Information?
Source: VA.gov (n.d.)

What Does Health Literate Patient Information Look Like?

• All of the preceding information from oral and written plain language, plus:
• Organize content and simplify navigation• Label links clearly• Include printer-friendly tools and resources• Incorporate audio and visual features• Use bold colors with contrast; avoid dark
backgrounds• Make sure the “back button” works• Use linear information paths•
U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion (2010)
Plain Language: Web-Based

This is for professiona
ls who serve older adults on
health and aging issues.
Health Literate Hearing Information?
Health.gov (2015)

Health Literate Hearing Information?
This is for the general
public
ASHA. org (2015)

• Improves analytical skills • Empowers decision making• Enhances ability to apply that knowledge in one’s life• Increases understanding of risks and benefits of treatment• Facilitates the interpretation of test results • Fosters skills necessary to manage a condition and prevent
it from getting worse• Promotes self efficacy• Garners readiness
Benefits of Optimizing Health Literacy

Summary
Limited Health Literacy
Poor Motivation
Poor Compliance
Poor Health-Related Decision Making
Poorer Overall Health Outcomes

Reflection Moment
1. How did this lesson inspire you to think of new ways to approach patient counseling?
2. What are some ways you can adapt your own clinical routines right now, to ensure better patient understanding?

Homework
Please rate the clinical materials you use in your clinic in term of readability (see associated handout) and improve upon them by making them more health literate.
Judge the health literacy of the information in terms of its• readability, • content and • design Develop health literate information about hearing loss or hearing aids for a patient in one of the video re-enactments.