1st case conference of the year sheryl kho, m.d. pgy 3 july 22, 2009
TRANSCRIPT

1st Case Conference of the Year
Sheryl Kho, M.D.
PGY 3
July 22, 2009

Chief Complaint
17 yo AA boy
“I can’t move my face.”

History of Present Illness
6 days PTA- Woke up unable to move R side of face
No fever, rash, HA, constitutional sxs, trauma
Went to ED- Dx: Bell’s PalsyRx: Acyclovir + Prednisone

History of Present Illness
3 days PTA- persistent facial paralysis with pins and needle sensation
+ HA-frontal, +photophobia, +phonophobia
+vomiting+pain in R ear
+hyperacusis+tingling sensation on his
tongue

Past Surgical Hx
S/p I&D Pilonidal abscess- 2 wks ago
Rx: Augmentin x 7 days

Past Medical Hx
Varicella @ 5yoOccasional cold sores on upper lipIUTDPPD negative- 1 year ago

Adolescent Hx (HEADSSS)
Lived in the BronxNo travelDenies tick bites, animal exposureJunior in HS, worked as a lifeguard
during summerDenies sexual activityDenies use of illicit drugs or alcohol

Physical Exam
VS: T 38.2C, HR 110bpm, RR 20/min, BP 127/75, SaO2 100%
AAO, c/o frontal HAHEENT: NCAT, PERRLA, +crusted lesion in R ear canal,
TM intact B/L, +2 crusted sores on R upper lip, MMM, clear OP, supple neck, no Brudzinski, no Kernig,+nuchal rigidity
Lungs: CTA B/L, no WRR, no retractionsHeart: RRR, normal S1/S2, no mrg
Physical Exam
Abd: +BS, soft, NT, ND, no HSMExt: FROMx4, no cyanosis, no edema, 2+pulses, good
cap refillNeuro: AAO, unable to close R eye, +drooping R side of
face with flattening of ipsilateral nasolabial fold, unable to wrinkle R side of forehead, unable to puff out R cheek, +asymmetric smile

Differential Diagnosis? Infectious
AOM, COM, cholesteatoma Meningitis Bell’s Palsy Lyme Disease Viral Syndrome Mumps Herpes zoster oticus
Neuro/CNS Mass/Tumor ie. Acoustic neuroma,
glomus tumor,facial ner neuroma Stroke Bleed
Others Vertigo Trigeminal Neuralgia TMJ Disorders Dental Pain Persistent Idiopathic Facial Pain
Toxins Tetanus
Iatrogenic Surgical Embolization Nerve block
Idiopathic Autoimmune syndrome Myasthenia gravis Multiple sclerosis Sarcoidosis Amyloidosis
Systemic DM Alcoholic neuropathy Hyperthyroidism Pregnancy
Trauma Birth trauma Temporal bone fracture Facial trauma
Diagnostic Workup?
CBC, BCxCMPCSF, CSF CxLyme titersCT scanWound Cx

Diagnostic Workup
CBC- 4.4>13<172,000 N65 L19 M16CMP- normal TP: 7.5 Alb: 4UA-normalCT Brain- negativeLyme titers negative IgM, IgG

Diagnostic Workup
Lumbar PunctureClear CSFWBC: 32, L91, RBC: 25CSF protein 45, CSF glucose 47Gm stain: no organisms, no cellsCSF culture pendingCSF PCR HSV negativeCSF Viral Cx negative

Management
Started on Ceftriaxone and AcyclovirPrednisone taperHA and neck stiffness resolved w/in 24hrCTX d/c’d once CSF cx negative

Further Diagnostic Workup
VZV cultured from R ear canal lesionsHIV ELISA: positiveCD4 count: 28 AIDSHIV Viral load: 414,555

Further Management
IV Acyclovir continuedPrednisone PO x 7 daysBactrim and Zithromax- prophylaxis for M.
avium, Pneumocystis jiroveciEfavirenz, Emtricitabine and Tenofovir
started 6 wks after acute illness

What happened later?
6 months after start HAARTViral load: undetectableCD4 count: 220Continues with sensitivity to sound and R facial
paralysis

Ramsay Hunt Syndrome
Ramsay Hunt Syndrome
1907: described by James Ramsay Hunt“Geniculate neuralgia”, “nervus
intermedius neuralgia”Facial paralysisInner ear dysfunctionPeriauricular painHerpetiform vesicles of the pinna (herpes
zoster oticus)
Ramsay Hunt Syndrome
Primary infection with VZV (HHV 3)Latent in the geniculate ganglion of CN VIIVZV reactivation, zoster: decline in cell
mediated immunity ie. HIV

Pathophysiology of RHS
Geniculate ganglion of CN VIIPetrous portion of the temporal bone lies
the ear apparatus (inner ear)CNVII courses through the inner and
middle earInflammation causes facial paresis,
vertigo, otalgia, hyperacusis

Anatomy of the Facial Nerve

Anatomy of the Facial Nerve

Anatomy of the Facial Nerve

Epidemiology of RHS
RareComplete recovery rate <50%Self limitingMorbidity: facial weakness

History Taking
Pain deep in the earVertigoTinnitusFacial paresis
Rash, blisters, herpetic lesions

Physical Examination
PainPeripheral facial nerve paralysis with
herpetic lesionsAnt 2/3 of tongueSoft palateext auditory canalPinna
Ipsilateral hearing loss, balance problemsNeuro exam

Physical Examination

Diagnostic Workup
CBC with differentialESRSerum electrolytesViral Studies
Serologic testsVZV PCR on tear samplesViral cxs
Imaging studiesMRI, CT scan
AudiometryCSF studies (controversial)

RHS in HIV Patients
Normal children: 0.74/1000>70% in HIV, CA 7-20x greater risk than children with
leukemiaRecurrence: 53% (1.7-5%)Persistence of skin lesions: 14%

Bell’s PalsyIdiopathic facial paralysis (IFP)Virally mediated, exact mechanism unknownAffects CN VIIReactivation of HSV60-75% of acute facial palsiesSudden paresis of facial muscles on one side,
absence of CNS dse <48hrs20-30 pxs/100,000Paresis in the morning, worsens thru the day
Otalgia, facial pain, hyperacusis, decreased tears, NO SKIN LESIONS
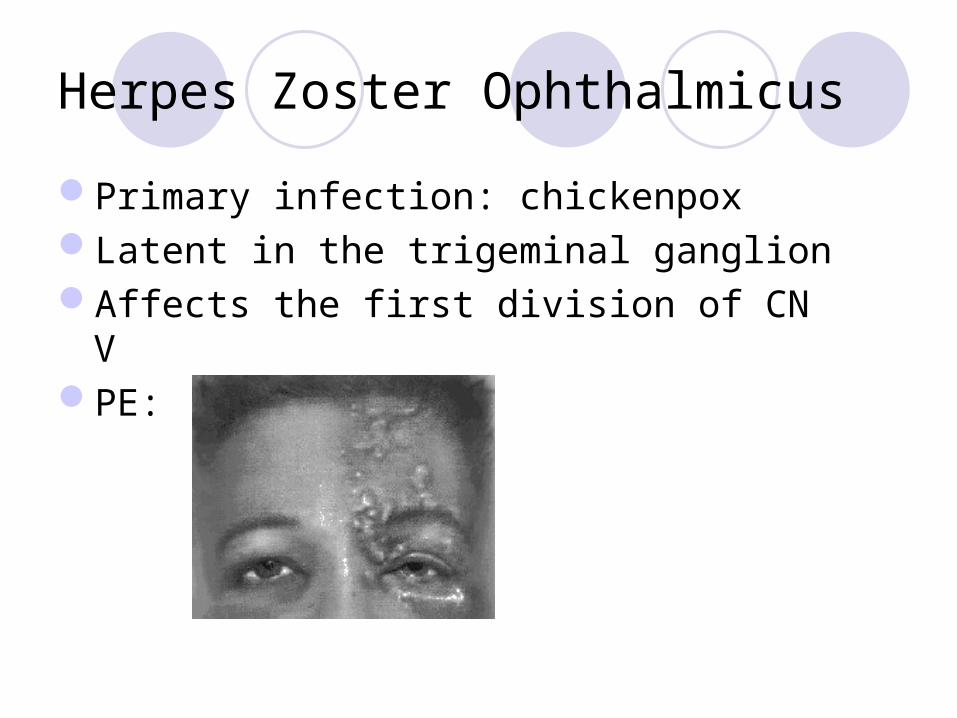
Herpes Zoster Ophthalmicus
Primary infection: chickenpoxLatent in the trigeminal ganglionAffects the first division of CN VPE:

Treatment of RHS
Acyclovir + prednisoneRemains controversial

Thank you…