130 temporal changes and regional variation in prostate cancer imaging in a nation-wide,...
TRANSCRIPT
and $271,459 for cabazitaxel. The total cost of administering the 5-drugregimen with Sipuleucel-T was $349,767 and $234,425 for the 4-drugregimen without Sipuleucel-T.
CONCLUSIONS: Our analysis reflects a best-case scenario inwhich a patient receiving multiple treatments for mCRPC attains themaximum survival benefit. Based on the available survival data andcurrent costs of treatment, only docetaxel is close to the standard ICERthreshold of $100,000 per LYS. Future research should focus ondocumenting the survival and quality of life associated with the sequen-tial use of these therapies in addition to the economic burden, which ourstudy suggests could be substantial.
Source of Funding: None
Cost-effectiveness analysis of the current treatment paradigm for mCRPC withand without sipuleucel-T.
TreatmentCost[$](C)
Effect[LYS](E)
IncrementalCost [$]
(I”C)
IncrementalEffect [LYS]
(I”E)
ICER [$/LYS] (I”C/
I”E)CEA With Sip-T
Placebo(Sip-T Trial) $38,456 1.81
Sipuleucel-T $144,582 2.15 $106,126 0.34$310,613
(dominated)
Sip-T�Docetaxel $165,071 2.35 $20,488 0.2$102,442
(dominated)
Sip-T� Doc�Abiraterone $227,083 2.68 $188,626 0.87 $217,645
Sip-T�Doc�Abir�Enzalutamide $295,474 2.98 $68,392 0.31 $221,811
Sip-T�Doc�Abir�Enzal�Cabazitaxel $349,767 3.18 $54,292 0.2 $271,460
CEA w/o Sip-T
Placebo(DocetaxelTrial) $29,241 1.38
Docetaxel $49,729 1.58 $20,488 0.2 $102,442
Doc�Abiraterone $111,741 1.9 $62,012 0.325 $190,806
Doc�Abir�Enzalutamide $180,133 2.22 $68,392 0.31 $221,812
Doc�Abir�Enzal�Cabazitaxel $234,425 2.41 $54,292 0.2 $271,460
129EMERGENCY DEPARTMENT REVISITS FOR KIDNEY STONES:FREQUENCY AND VARIATION
Charles Scales, Jr.*, Jonathan Bergman, Christopher Saigal,Mark Litwin, Los Angeles, CA
INTRODUCTION AND OBJECTIVES: Hospital readmissionsand emergency department (ED) revisits are an important focus forimproving quality and reducing costs of healthcare delivery. Patientswith symptomatic kidney stones frequently seek ED care, yet little isknown about quality of patient care in this context, or the frequency ofrevisits for symptomatic kidney stones. Our objective was to measurethe frequency of ED revisits for patients with kidney stones, and identifypatient and facility characteristics associated with an increased risk ofED revisits.
METHODS: We used the California State Emergency Depart-ment Database to identify individuals with an ED visit for a kidney stonein 2008 and 2009. This dataset captures all ED visits in the state ofCalifornia, and permits tracking of patients across encounters andbetween hospitals in a de-identified fashion. The primary outcome wasthe occurrence of a second ED visit for kidney stones within 30 days ofthe initial visit. Using a generalized estimating equation approach witha logit link function to account for clustering at the individual hospitallevel, we identified patient and facility level factors associated with EDrevisits. As a secondary outcome, factors associated with the numberof ED revisits for an individual were identified using a zero-inflatednegative binomial regression, again adjusted for clustering.
RESULTS: The cohort comprised 128,612 persons who had aninitial ED visit for a kidney stone in 2008-2009. Among these, 11,960(9.3%) had a second visit for a kidney stone within 30 days of the initialvisit. The number of repeat visits within 30 days ranged from 0-8. Onmultivariable analysis, several patient level characteristics were asso-ciated with ED revisits. Black (OR 0.80, 95%CI 0.72-0.90, p�0.001)and Hispanic (OR 0.89, 95% CI 0.84 ? 0.94, p�0.001) were less likelythan white patients to revisit the ED. Similarly, females were less likelythan males to revisit the ED (OR 0.88, 95% CI 0.84-0.92, p�0.001). EDrevisits were most common among those with Medicaid, and amongthose patients living in rural areas. Similar results were found when thesecondary outcome of number of revisits was analyzed.
CONCLUSIONS: ED revisit rates for kidney stones vary bynon-clinical factors such as sex, race and payer. This variation mayrepresent an opportunity to optimize quality of ED care and, by reduc-ing revisit rates, decrease costs for kidney stone management in theUnited States. Future efforts should include identification of clinicaldrivers of ED revisits with targeted interventions to improve patient careand reduce preventable ED revisits.
Source of Funding: Robert Wood Johnson Foundation/ USDepartment of Veterans Affairs Clinical Scholars Program
130TEMPORAL CHANGES AND REGIONAL VARIATION INPROSTATE CANCER IMAGING IN A NATION-WIDE,POPULATION-BASED COHORT FOLLOWING AN EFFORT TODISCOURAGE INAPPROPRIATE USE
Danil Makarov*, Stacy Loeb, David Ulmert, New York, NY;Linda Drevin, Uppsala, Sweden; Mats Lambe, Stockholm, Sweden;Par Stattin, Umeaº, Sweden
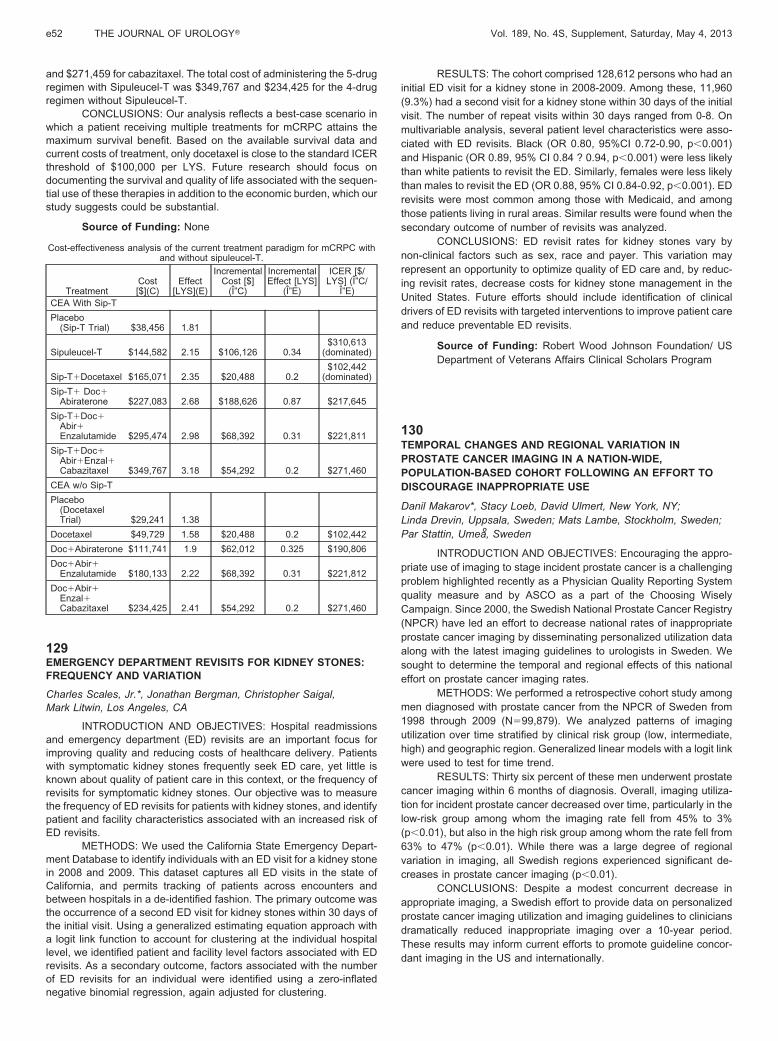
INTRODUCTION AND OBJECTIVES: Encouraging the appro-priate use of imaging to stage incident prostate cancer is a challengingproblem highlighted recently as a Physician Quality Reporting Systemquality measure and by ASCO as a part of the Choosing WiselyCampaign. Since 2000, the Swedish National Prostate Cancer Registry(NPCR) have led an effort to decrease national rates of inappropriateprostate cancer imaging by disseminating personalized utilization dataalong with the latest imaging guidelines to urologists in Sweden. Wesought to determine the temporal and regional effects of this nationaleffort on prostate cancer imaging rates.
METHODS: We performed a retrospective cohort study amongmen diagnosed with prostate cancer from the NPCR of Sweden from1998 through 2009 (N�99,879). We analyzed patterns of imagingutilization over time stratified by clinical risk group (low, intermediate,high) and geographic region. Generalized linear models with a logit linkwere used to test for time trend.
RESULTS: Thirty six percent of these men underwent prostatecancer imaging within 6 months of diagnosis. Overall, imaging utiliza-tion for incident prostate cancer decreased over time, particularly in thelow-risk group among whom the imaging rate fell from 45% to 3%(p�0.01), but also in the high risk group among whom the rate fell from63% to 47% (p�0.01). While there was a large degree of regionalvariation in imaging, all Swedish regions experienced significant de-creases in prostate cancer imaging (p�0.01).
CONCLUSIONS: Despite a modest concurrent decrease inappropriate imaging, a Swedish effort to provide data on personalizedprostate cancer imaging utilization and imaging guidelines to cliniciansdramatically reduced inappropriate imaging over a 10-year period.These results may inform current efforts to promote guideline concor-dant imaging in the US and internationally.
e52 THE JOURNAL OF UROLOGY� Vol. 189, No. 4S, Supplement, Saturday, May 4, 2013
Source of Funding: The Swedish Research Council 825-2008-5910 and The Swedish Cancer Foundation 11 0471,Västerbotten county council and Lions Cancer ResearchFoundation at Umeaº University. SL and DM are supported bythe United States Department of Veterans Affairs, HealthServices Research and Development Service and the LouisFeil Charitable Lead Trust.
131AN ANALYSIS OF ACADEMIC DIFFUSION OF SURGICALINNOVATIONS IN UROLOGY
Sriram Rangarajan*, Kerrin Palazzi, David Chang,J. Kellogg Parsons, La Jolla, CA
INTRODUCTION AND OBJECTIVES: Diffusion is the processby which innovations spread through social constructs. The diffusion ofsurgical innovations in the urological literature, and its association withdiffusion of innovations into urological practice, has not been described.We analyzed the academic diffusion patterns of three major surgicalinnovations – minimally-invasive radical prostatectomy (MIRP), ne-phrectomy, and partial nephrectomy ? in the academic literature andcompared them with corresponding practice diffusion patterns.
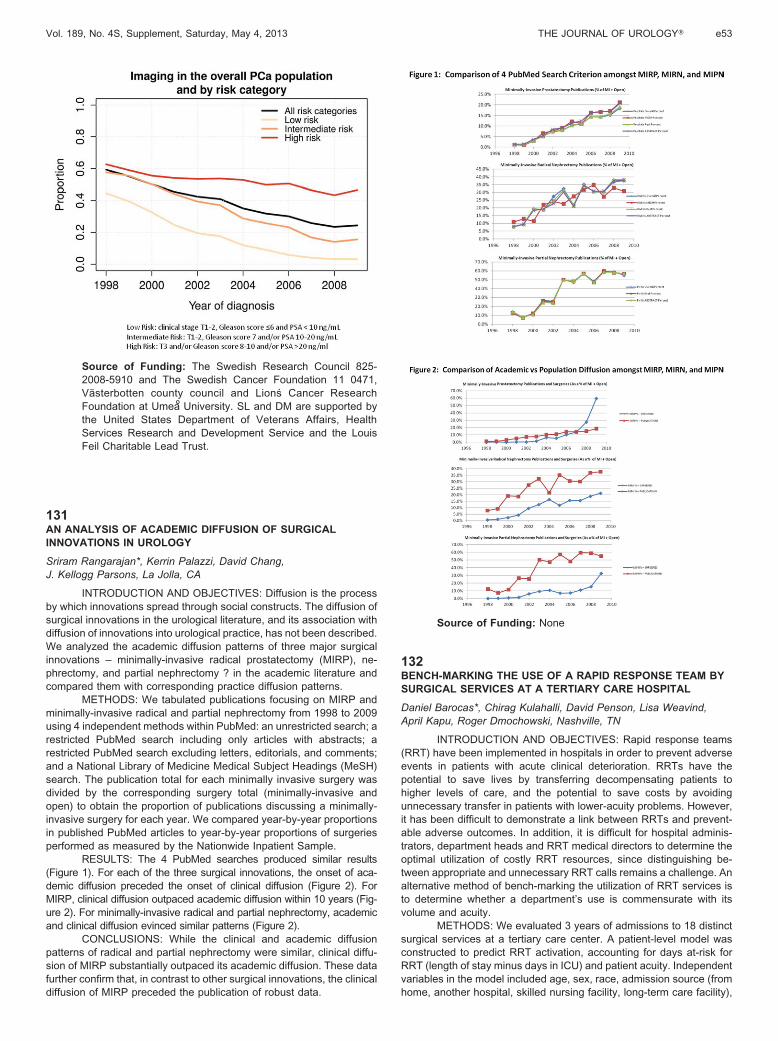
METHODS: We tabulated publications focusing on MIRP andminimally-invasive radical and partial nephrectomy from 1998 to 2009using 4 independent methods within PubMed: an unrestricted search; arestricted PubMed search including only articles with abstracts; arestricted PubMed search excluding letters, editorials, and comments;and a National Library of Medicine Medical Subject Headings (MeSH)search. The publication total for each minimally invasive surgery wasdivided by the corresponding surgery total (minimally-invasive andopen) to obtain the proportion of publications discussing a minimally-invasive surgery for each year. We compared year-by-year proportionsin published PubMed articles to year-by-year proportions of surgeriesperformed as measured by the Nationwide Inpatient Sample.
RESULTS: The 4 PubMed searches produced similar results(Figure 1). For each of the three surgical innovations, the onset of aca-demic diffusion preceded the onset of clinical diffusion (Figure 2). ForMIRP, clinical diffusion outpaced academic diffusion within 10 years (Fig-ure 2). For minimally-invasive radical and partial nephrectomy, academicand clinical diffusion evinced similar patterns (Figure 2).
CONCLUSIONS: While the clinical and academic diffusionpatterns of radical and partial nephrectomy were similar, clinical diffu-sion of MIRP substantially outpaced its academic diffusion. These datafurther confirm that, in contrast to other surgical innovations, the clinicaldiffusion of MIRP preceded the publication of robust data.
Source of Funding: None
132BENCH-MARKING THE USE OF A RAPID RESPONSE TEAM BYSURGICAL SERVICES AT A TERTIARY CARE HOSPITAL
Daniel Barocas*, Chirag Kulahalli, David Penson, Lisa Weavind,April Kapu, Roger Dmochowski, Nashville, TN
INTRODUCTION AND OBJECTIVES: Rapid response teams(RRT) have been implemented in hospitals in order to prevent adverseevents in patients with acute clinical deterioration. RRTs have thepotential to save lives by transferring decompensating patients tohigher levels of care, and the potential to save costs by avoidingunnecessary transfer in patients with lower-acuity problems. However,it has been difficult to demonstrate a link between RRTs and prevent-able adverse outcomes. In addition, it is difficult for hospital adminis-trators, department heads and RRT medical directors to determine theoptimal utilization of costly RRT resources, since distinguishing be-tween appropriate and unnecessary RRT calls remains a challenge. Analternative method of bench-marking the utilization of RRT services isto determine whether a department’s use is commensurate with itsvolume and acuity.
METHODS: We evaluated 3 years of admissions to 18 distinctsurgical services at a tertiary care center. A patient-level model wasconstructed to predict RRT activation, accounting for days at-risk forRRT (length of stay minus days in ICU) and patient acuity. Independentvariables in the model included age, sex, race, admission source (fromhome, another hospital, skilled nursing facility, long-term care facility),
Vol. 189, No. 4S, Supplement, Saturday, May 4, 2013 THE JOURNAL OF UROLOGY� e53