11/7/2013 nursing informatics: challenges opportunities€¦ · · 2013-11-07information...
TRANSCRIPT
11/7/2013
1
Nursing Informatics:Challenges and Opportunities in the
21st Century
Thomas R. Clancy, MBA, PhD, RN, FAANClinical Professor and Assistant Dean
School of NursingThe University of Minnesota
Objectives1. Describe the emerging challenges of information
technology in health systems today.2. Review nursing informatics (NI) competencies
required of students and practicing nurses.3. Describe challenges faced by nursing programs
in providing NI education4. List opportunities to collaboratively enhance
and improve NI education to students and practicing nurses.
Over the last 50 years we have seen:• An explosion in
biomedical knowledge,• Dramatic innovations in
therapies and surgical procedures and,
• Management of conditions that were previously viewed as fatal.

11/7/2013
2
Cancer Survival Rates FDA Approved HIV Drugs
Smith, M., Saunders, R., Stuckhardt, L., and McGinnis, M. (2012). Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Institute of Medicine, National Academies Press
• Dramatic progress has been made in identifying patient safe practices.
• These five practices alone have been shown to significantly reduce medication errors and adverse outcomes at a minimum of cost.
Intervention Results
Provider order entry
81% decrease in medication errors
Pharmacist Rounding
78% reduction in preventable ADE’s
Rapid responseteams
15% decrease in cardiac arrests
Team training in labor and delivery
50% reduction in adverse outcomes
Reconciling medications upon hospital discharge
90% decrease in medication errors
Leape, L. and Berwick, D. (2005). FIVE YEARS AFTER TO ERR IS HUMAN: WHAT HAVE WE LEARNED? In the Literature, The Commonwealth Fund. 293 (19): 2384–90
• Despite this, national health expenditures as a share of gross domestic product (GDP) are currently at 17.6% and projected to rise to 20% by 2020.

11/7/2013
3
American healthcare continues to fall short on basic dimensions such as quality, cost, outcomes, and equity
Institute of Medicine (2012). Best Care at the Lowest Price. National Academies Press, Washington DC
Despite finding small improvements at the margins, it is harder to see the overall, national impact of “Too Err is Human” on patient safety.
Leape, L. and Berwick, D. (2005). FIVE YEARS AFTER TO ERR IS HUMAN: WHAT HAVE WE LEARNED? In the Literature, The Commonwealth Fund. 293 (19): 2384–90
• Over 30 years ago the IOM estimated that up to 98,000 Americans die each year from medical errors in hospitals
• Current estimates for 2013 are:– 210,000 – 440,000!
Journal of Patient Safety:
September 2013 ‐ Volume 9 ‐ Issue 3 ‐ p 122–128 Bleich, S (2005). Issue Brief in The Commonwealth Fund,1 East 75th Street,New York, NY 10021‐2692

11/7/2013
4
• Despite the progress in information technology to improve the speed and effectiveness of communication, we have seen a 2800% increase in medical errors resulting from electronic health records.
Pennsylvania Patient Safety Authority, December 2012
Decades of rapid innovation and technological improvement have created an extraordinarily complex healthcare system. So much so that healthcare often falls short of its potential.
Smith, M., Saunders, R., Stuckhardt, L., and McGinnis, M. (2012). Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Institute of Medicine, National Academies Press.
Typical chronic disease pt.
• 79 years old,
• Osteoporosis,
• Osteoarthritis,
• Type 2 diabetes,
• Hypertension,
• COPD,
Typical Patient
• See 7 doctors across 4 practices
• 27 different health providers (surgery patient)
• 19 medications per day
Smith, M., Saunders, R., Stuckhardt, L., and McGinnis, M. (2012).
Best Care at Lower Cost: The Path to Continuously Learning
Health Care in America. Institute of Medicine,
National Academies Press.

11/7/2013
5
Typical Physician
• Interacts with 229 other physicians in 117 different practices.
Typical ICU Nurse
• Manages 180 activities per patient per day!
Smith, M., Saunders, R., Stuckhardt, L., and McGinnis, M. (2012).
Best Care at Lower Cost: The Path to Continuously Learning
Health Care in America. Institute of Medicine,
National Academies Press.
Most physicians, nurses, and other health care professionals work diligently to care for their patients, but they often are contending with:
• challenges of a system that is poorly configured, for the current complexity of treatments, technologies, and clinical science.
Smith, M., Saunders, R., Stuckhardt, L., and McGinnis, M. (2012).
Best Care at Lower Cost: The Path to Continuously Learning
Health Care in America. Institute of Medicine,
National Academies Press.

11/7/2013
6
Institute of Medicine
• These problems point to the need for a transformation in how the health care enterprise generates, processes, and applies information to further patient care.
Key Imperatives
• To manage the health care system’s ever‐increasing complexity, and
• To curb ever‐escalating costs.
“Opportunities exist to address these problems—opportunities that did not exist even a decade ago:”
1. Vast computational power that is affordable and widely available;
2. Connectivity that allows information to be accessed in real time virtually anywhere;
3. Human and organizational capabilities that improve the reliability and efficiency of care processes; and
4. The recognition that effective care must be delivered by collaborations between teams of clinicians and patients, each playing a vital role in the care process.
Moores Law
• First described in 1965 by Gordon Moore, the number of transistors on integrated circuits doubles approximately every two years. – Calculations per second
– Processing speed
– Size of devices
Accessed at Wikimedia on October 27, 2013 at
http://en.wikipedia.org/wiki/File:PPTMooresLawai.jpg

11/7/2013
7
• 85% of adults own a cellphone.
• 76% own a computer
• 80% have access to the Intranet
• Mobile device growth is estimated at 30% per year.
• 10 billion users by 2020
• 86% of providers use the Intranet to gather clinical information
• The 3rd most popular use of the Intranet is looking up health information by individuals
BENEFITS of EHR
Quality, Safety & Education
• Data integrity – readable, accurate, organized and complete.
• Clinical decision support
• Care coordination, EBG’s and population mgt.
• Patient safety – Alerts, drug interactions

11/7/2013
8
ACCESS
• Simultaneous access to patient records
• Security and privacy
• Graphs, charts , trending that facilitate comparison of current and past data.
• Access to drug information, decision support tools, and literature searches, • EHR Dashboard
Accessed at AHRQ website: http://www.ahrq.gov/legacy/about/annualconf09/middleton.htmon November 4, 2014
Cost and Revenue
• Increased productivity,
• Improved billing and reimbursement rates,
• faster turnaround for accounts,
• lower medical record costs,
• Improved revenue cycle,
• enhanced regulatory, requirement compliance,
• President Bush’s goal in 2004
• Executive order established the Office of the National Coordinator for Health Information Technology (ONCHIT) as part of the Dept of Health & Human Services (HHS)
– Dr. David Brailer appointed the first National Coordinator
“… an Electronic Health Record for every American by the year 2014. By computerizing health records, we can avoid dangerous medical mistakes, reduce costs, and improve care.”
- State of the Union address,Jan. 20, 2004
Courtesy of Murphy, J. (2012) QSEN Nursing Informatics Deep Dive Workshop

11/7/2013
9
“To lower health care cost, cut medical errors, and improve care, we’ll computerize the nation’s health records in five years, saving billions of dollars in health care costs and countless lives.”
- First Weekly AddressJan. 24, 2009
• February 17, 2009 – the American Reinvestment and Recovery Act (ARRA – Stimulus Bill) is signed into law
– HITECH component of ARRA provides an incentive program to stimulate the adoption and use of HIT, especially EHR’s
– Dr. David Bluementhal appointed the new National Coordinator
• President Obama’s goal in 2009
HITECH ACTThe Health Information Technology for Economic and Clinical Health (HITECH)Act:• Provides $30 billion in
Medicare and Medicaid incentive payments
• For the meaningful use of health information technology by clinicians and hospitals,
• Estimated to yield savings of $93 billion between 2011 and 2019.
Taken from: Blumenthal, D. “Launching HITECH,” posted by the NEJM on 12‐30‐2009.
27

11/7/2013
10
Stage 2 MUACO’s
“Stage 3 MU”PCMH
3‐Part Aim
Registries to manage patient populations
Team based care, case management
Enhanced access and continuity
Privacy & security protections
Care coordination
Privacy & security protections
Patient centered care coordination
Improved population health
Registries for disease
management
Evidenced based medicine
Patient self management
Privacy & security protections
Care coordination
Structured data utilized
Data utilized to improve delivery and outcomes
Data utilized to improve delivery and outcomes
Patient informed
Patient engaged, community resources
Stage 1 MU
Privacy & security protections
Basic EHR functionality, structured data
Utilize technology
Access to information
Transform health care
Meaningful Use as a Building Block
Source: CMS EHR Incentive Program Data as of 7/31/2012
$22 $16 $26 $31
$109 $80
$116
$276
$236
$387
$607
$836
$563
$619
$659
$619
$583
$428
$384
Cumulative Total$6,597
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
$0
$100
$200
$300
$400
$500
$600
$700
$800
$900
Cumulative Amount Paid (Millions)
Amount Paid per M
onth (Millions)
Payments to All Eligible Professionals and Hospitals Under the Medicare or Medicaid EHR Incentive Programs
• Projections are for 90 percent of providers to have access to a fully operational electronic health records by 2019, up from 34‐35 percent in 2011.

11/7/2013
11
Competency in Health Information Technology (HIT) is critical for nursing:
• Largest number of health care providers in the US.
• 19.6% of all healthcare workers or over 3 million nurses.
• 1988 ‐ Nursing Informatics: Where Caring and Technology Meet (Ball, Hannah, Newbold, and Douglas).
• 1981‐ International Medical Informatics Association –Nursing Working Group
• 1982 – Computers in Nursing (1st journal)• 1984 – Council on Computer Applications in Nursing (ANA) and National Forum on Computers in Health Care (NLN).
• 1988 – 1st master’s program, U of Maryland.• 1992 – ANA specialty recognition, nursing informatics• 1995 – Standards of Practice, nursing informatics
NURSING INFORMATICS
The goal of Nursing informatics (NI) is to improve the health of populations, communities, families, and individuals by optimizing information management and communication.
Nelson, R. and Staggers, N. (2013). Health Informatics: An Interprofessional Approach. Elsevier, St. Louis.

11/7/2013
12
NURSING INFORMATICSThe design and use of informatics solutions and technology to support all areas of nursing;• Direct provision of care, • Establishing effective
administrative systems, • Designing useful decision
support systems • Managing and delivering
educational experiences, • Supporting lifelong learning,
and supporting nursing research.
Nelson, R. and Staggers, N. (2013). Health Informatics: An Interprofessional Approach. Elsevier, St. Louis.
INTERPROFESSIONAL• American Medical
Informatics Association (AMIA)
• Healthcare Information and Management and Systems Society (HIMSS)
• American Health Information Management Association (AHIMA)
• College of Healthcare Information Management Executives
NURSING• Alliance for Nursing
Informatics (ANI)• American Nursing
Informatics Association (ANIA)
COMPETENCIES IN NI• ANA – Scope and Standards of
Practicehttp://www.nursingworld.org/HomepageCategory/NursingInsider/Archive_1/2008NI/Jan08NI/RevisedNursingInformaticsPracticeScopeandStandardsofPractice.aspx• AACN ‐ American Association of
Colleges of Nursing Essentials for BSN, Masters and Doctoral students
http://www.aacn.nche.edu/education‐resources/essential‐series• TIGER – Technology Informatics
Guiding Educational Reformhttp://www.tigersummit.com/About_Us.html
11/7/2013
13
• Demonstrate skills in using patient care technologies, information systems, and communication devices that support safe nursing practice.
• Apply safeguards and decision making support tools embedded in patient care technologies and information systems to support a safe practice environment for both patients and healthcare workers.
• Use telecommunication technologies to assist in effective communication in a variety of healthcare settings.

11/7/2013
14
• Understand the use of CIS systems to document interventions related to achieving nurse sensitive outcomes.
• Use standardized terminology in a care environment that reflects nursing’s unique contribution to patient outcomes.
• Evaluate data from all relevant sources, including technology, to inform the delivery of care.

11/7/2013
15
• Recognize the role of information technology in improving patient care outcomes and creating a safe care environment.
• Uphold ethical standards related to data security, regulatory requirements, confidentiality, and clients’ right to privacy.
• Apply patient care technologies as appropriate to address the needs of a diverse patient population.
http://news.brown.edu/pressreleases/2012/05/braingate2

11/7/2013
16
• Recognize that redesign of workflow and care processes should precede implementation of care technology to facilitate nursing practice.
• Participate in evaluation of information systems in practice settings through policy and procedure development.
2006 National League for Nursing Survey• Five hundred deans and
1,557 faculty• Only 50 to 60 percent of
respondents said that informatics was integrated into the curriculum.
• Clinical experience with information systems was provided during clinical experiences.

11/7/2013
17
SCHOOL OF NURSING FACULTY SURVEY – 28 Nursing Schools – 2013
• 94.7 % did not provide course content regarding theories of nursing informatics and key terms.
• 53.3% did not provide content on how to use data gathered through the Electronic Health Record (EHR) to improve patient care.
• 70.8% did not provide content on how to monitor and analyze data on nurse sensitive quality indicators through electronic dashboards and other tools.
• 40% did not provide content on the application and benefits of EHR’s in enabling the use of evidence based practices (For example: developing evidence based care plans and executing electronic order sets, using standardized nursing languages, decision support, links to resources or other)
SCHOOL OF NURSING FACULTY SURVEY – 28 Nursing Schools – 2013
• 40% did not provide content on how the EHR can be used as a bridge for interdisciplinary learning (for example: the integration of information systems for nursing, pharmacy, lab, radiology, medicine and other).
• 83% did not require students to demonstrate use of a mobile device(smart phone, iPad, laptop) to access real time information.
• 50% did not provide content on consumer informatics in a course (For example: shared medical records, consumer health websites, virtual office visits and other)
• 68% did not engage with clinical sites/partners to discuss developing/enhancing nursing informatics curriculum, provide feedback on demands and priorities of each organization, hospital/regional advisory councils, etc.
• Only 9% of nurse informaticists are employed in academic institutions.
• Of the 3,179 total nursing programs in the US only 317 (10% of total) have either a certificate program or advanced degree in nursing informatics.
Workplace Percent
Hospital 48%
Health System 20%
Academic Setting 9%
Vendor Organization 10%
Consulting Firm 5%
Government/Military 4%
Ambulatory Setting 2%
Other 7%
Distribution of Nurse Informaticists
HIMSS Annual Survey 2011(660 Respondents)

11/7/2013
18
SCHOOL OF NURSING FACULTY SURVEY – 28 Nursing Schools – 2013
• Confusion on what nursing informatics is.
• NI is a new field and faculty must find ways to integrate the content into an already full schedule of courses.
• To meet the accreditation requirements for NI many Schools rely on a clinical site’s EHR.
• It is difficult for faculty to learn the specialized field of informatics given their current demands.
Training Program Type Percent
Masters/PhD (Informatics Specialty) 23%
Bachelors (Informatics Courses) 2%
Certificate (ANCC, CPHIMS, Other) 15%
On the Job Training (courses, workshops, e-learning & other) 15%
None 32%
Distribution of Training for Nurse Informaticists by Program TypeHIMSS Annual Survey 2011
(660 Respondents)
Content and teaching methods needed by nurse educators for nursing informatics is:
• Scattered among numerous websites
• Aimed primarily at professional development of working informatics professionals.
11/7/2013
19
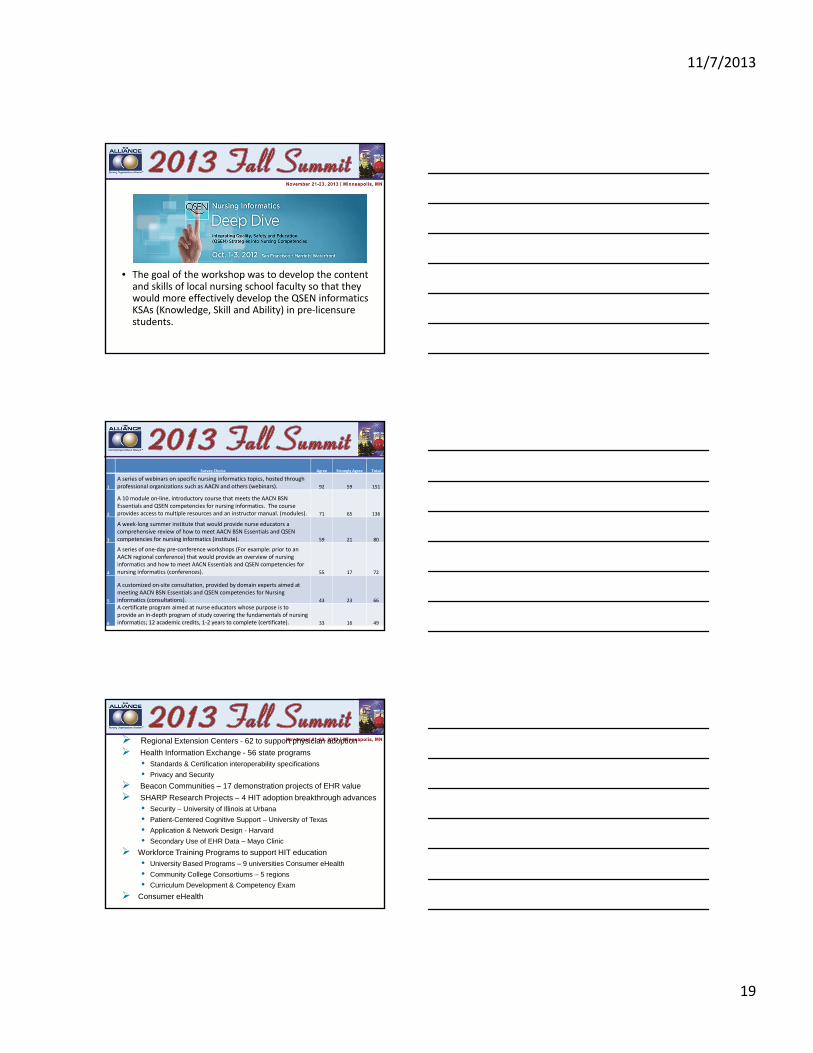
• The goal of the workshop was to develop the content and skills of local nursing school faculty so that they would more effectively develop the QSEN informatics KSAs (Knowledge, Skill and Ability) in pre‐licensure students.
Survey Choice Agree Strongly Agree Total
1
A series of webinars on specific nursing informatics topics, hosted through professional organizations such as AACN and others (webinars). 92 59 151
2
A 10 module on‐line, introductory course that meets the AACN BSN Essentials and QSEN competencies for nursing informatics. The course provides access to multiple resources and an instructor manual. (modules). 71 65 136
3
A week‐long summer institute that would provide nurse educators a comprehensive review of how to meet AACN BSN Essentials and QSEN competencies for nursing informatics (institute). 59 21 80
4
A series of one‐day pre‐conference workshops (For example: prior to an AACN regional conference) that would provide an overview of nursing informatics and how to meet AACN Essentials and QSEN competencies for nursing informatics (conferences). 55 17 72
5
A customized on‐site consultation, provided by domain experts aimed at meeting AACN BSN Essentials and QSEN competencies for Nursing informatics (consultations). 43 23 66
6
A certificate program aimed at nurse educators whose purpose is to provide an in‐depth program of study covering the fundamentals of nursing informatics; 12 academic credits, 1‐2 years to complete (certificate). 33 16 49
Regional Extension Centers - 62 to support physician adoption
Health Information Exchange - 56 state programs
• Standards & Certification interoperability specifications
• Privacy and Security
Beacon Communities – 17 demonstration projects of EHR value
SHARP Research Projects – 4 HIT adoption breakthrough advances
• Security – University of Illinois at Urbana
• Patient-Centered Cognitive Support – University of Texas
• Application & Network Design - Harvard
• Secondary Use of EHR Data – Mayo Clinic
Workforce Training Programs to support HIT education
• University Based Programs – 9 universities Consumer eHealth
• Community College Consortiums – 5 regions
• Curriculum Development & Competency Exam
Consumer eHealth
11/7/2013
20
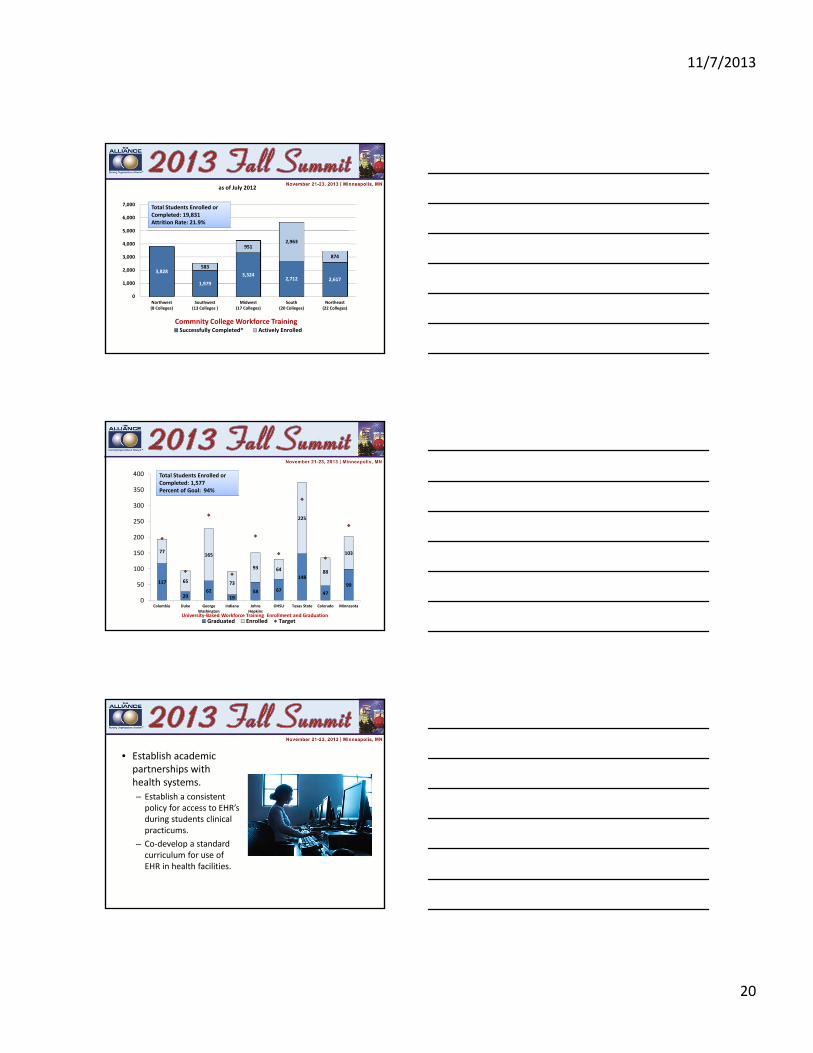
Commnity College Workforce Training Enrollment and Graduation
3,828
1,979
3,3242,712 2,617
583
9512,963
874
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
Northwest(8 Colleges)
Southwest(13 Colleges )
Midwest(17 Colleges)
South(20 Colleges)
Northeast(22 Colleges)
as of July 2012
Successfully Completed* Actively Enrolled
Total Students Enrolled or Completed: 19,831Attrition Rate: 21.9%
117
2962
1958 67
148
47
99
77
65
165
73
93 64
225
88
103
0
50
100
150
200
250
300
350
400
Columbia Duke GeorgeWashington
Indiana JohnsHopkins
OHSU Texas State Colorado Minnesota
Graduated Enrolled TargetUniversity‐Based Workforce Training Enrollment and Graduation
Total Students Enrolled or Completed: 1,577Percent of Goal: 94%
• Establish academic partnerships with health systems.
– Establish a consistent policy for access to EHR’s during students clinical practicums.
– Co‐develop a standard curriculum for use of EHR in health facilities.

11/7/2013
21
• Establish academic partnerships with commercial information technology vendors:
– Co‐develop academic versions of EHR’s
– Case studies
– Teaching methods
Establish regular reviews with academic institutions to review;• Existing curriculum• New trends in IT
– Consumer informatics & pt. engagement
– eMobile health– Big data– Robotics– Virtual health– Computer simulation and
serious gameshttp://www.ohsu.edu/xd/education/schools/school‐of‐medicine/departments/clinical‐
departments/family‐medicine/pcfdi/training/
Consumer Informatics and Patient Engagement
• Personal health records
• Portals
• eHealth literacy
• Patient engagement

11/7/2013
22
eMobile Health• Caregiver Alerts
• Voice Prompts
• Floor Sensors
• Safety Features
• Smart Beds
• Video Monitors
• Vital Sign Monitoring
• Medical Condition Monitoring
Robotics
Big Data
• Virtual Experiments
• Standardized Nursing Languages
• Knowledge discovery and data mining
• Data Visualization• http://healthpopuli.com/2013/04/08/the‐value‐of‐big‐
data‐in‐health‐care‐450‐billion

11/7/2013
23
Serious Games
• Problem solving
• Meaningful goals
• Possibility spaces
• Feedback and information
• Empowerment and reward
Thank You!
Thomas R. Clancy