10/4/2011 dr. kevin harris & dr. gail deyle....dr. kevin harris & dr. gail deyle. 10/4/2011...
TRANSCRIPT
Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
1
Not Every
Acromioclavicular Joint
Needs Excision
OMPT Interventions for AC
Joint Dysfunction
Kevin D. Harris, PT, DPT, DSc, OCS, FAAOMPT
Gail D. Deyle, PT, DPT, DSc, OCS, FAAOMPT
Consensus opinion
“Physical therapy, unfortunately,
has little to offer because
therapeutic exercise and range of
motion play only a minor
role….Iontophoresis or
phonophoresis may offer some
relief and is relatively benign.”
Buttaci et al 2004
“We may try an injection or
2, but you’ll need to have
surgery sooner or later”
Agenda
• Background & prevalence
• Anatomy & Biomechanics
• Clinical presentation
• Management pathways
– PT
– Injections
– Distal Clavicle Excision
• OMPT Approach
• Our ACJ trial
• Manual Therapy & Clinical Applications
• …here’s what we did and why we did it…
• Hands-on Lab time
• Clinical Reasoning: Case reports
• Conclusion
• Questions

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
2
Current Practice
Pattern?
Introduction
• 12 month prevalence of shoulder pain*
– 30.3%
– Second only to low back pain
• Acromioclavicular (AC) joint disease
present in 31% of all shoulder pain
patients**
*Picavet and Schouten 2003; **Ostor, Richards et al. 2005
Natural History
of A-C Separation
Over 48% of patients
sustaining a grade I or II
separation have
symptomatic AC joints 6
years after their injury
Mouhsine, Garofalo et al. 2003
Anatomy & Biomechanics

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
3
AC Joint
• Plane synovial
joint
• Joint surfaces
considered
incongruent
– Acromion concave
& distal clavicle
convex
– Can be vice-versa
Renfree et al 2003
Bony Stability of AC
Joint
Passive Stability of
AC Joint
Bontempo et al 2010
Dynamic Stability

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
4
Coronal Image
Simovitch et al 2009
Normal Anatomy Of The
AC Joint On MRI
Alyas et al 2008
Clinical Anatomy
Angle of AC Joint
Simovitch et al 2009

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
5
Various AC Joint
Configurations
Bisbinas et al 2006; Pichler et al 2009
Pain Referral
Pattern
Gerber et al 1998
Bone Scan

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
6
Pathoanatomy
Osteoarthritis
Etiopathogenesis
• OA is initiated by a mechanical insult to
the joint.
• OA is a manifestation of attempts to
heal the joint and ameliorate the
abnormal biomechanics.
• The osteoarthritis process may cause
joint pain but often is successful,
leading to a stable, painless joint.
Brandt et al 2008
Osteoarthritis
Radiology of OA
• Radiographic changes of OA are
extremely common in the population.
• Many people who have severe
radiographic changes of OA are
asymptomatic.
• Radiographic progression of OA
usually is slow and may cease
completely for many years.
Brandt et al 2008
Common Anatomical
Changes in OA Joints
• Synovitis
• Thickening/fibrosis of joint
capsule
• Degradation of articular
cartilage
• Subchondral sclerosis, cysts
• Osteophytes
• Degradation of disk when
applicable Brandt et al 2008

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
7
What Leads To
Pathoanatomy?
Taft et al 1987;
Mouhsine et al 2003
~ ½ have symptomatic
AC joint 6 years later
Altered Mechanics
Chronic grade 1 tear in a 32-year-old male
Old grade 2–3 injury in a 30-year-old male

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
8
Incidentally found chronic grade 3 injury in a 45-year-old male
Degeneration of the ACJ in a 41-year-old female
Spectrum
Normal Mild
Spectrum
Moderate Severe

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
9
? Biomechanics
AC Joint
Biomechanics Basics
• Function of the joint
– To allow the scapula additional
range or rotation on the thorax
– Transmission of forces
• Intra-articular motion not well
understood due to varied joint
morphologies
– Studies inconsistent in identifying
movements and axes of motion

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
10
Levangie & Norkin 2005
Posterior tipping Anterior tipping

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
11
Literature Update
• Pioneer work done by Inman et al
in 1944
• Data on normal shoulder motion
for both raising and lowering the
arm and for different planes of
elevation are sparse
Literature Update
• Previous studies have primarily relied
on either sensors attached to the skin
or testing in multiple static positions
• Accuracy limited by the use of static
testing or by motion artifact between
the skin and the underlying bones –
particularly for scapular and
clavicular motions, which were
difficult to record with surface
sensors
• 14 shoulders of 7
asymptomatic volunteers
with an average age of 23.6
yrs
• Seated, vertically open MR
• 7 (static) positions of
abduction from 0 to 180
deg.

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
12
Internal
Rotation
Posterior
Tipping
Many prior studies have evaluated
shoulder motion, yet no 3-D
analysis comparing the combined
clavicular, scapular, and humeral
motion during arm elevation has
been done
Methods
• 12 a-
symptomatic
• 29.3 yrs +/-
6.8 yrs
Methods
• 3 motions
– Flexion
– Scapular plane abd.
– Humerothoracic abd.
• 2 repetitions each
• Full active ROM
• Measured motion of
the scapula relative
to thorax & scapula
relative to clavicle

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
13
Results
Average of 8 degrees
Results
Average of 11 degrees
Results
Average of 19 degrees
AC Joint Findings
• Posterior tilting was the
predominant AC joint motion
• Posterior tilting was > 90% AC
joint motion

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
14
Conclusion
Overall shoulder motion
consists of substantial angular
rotations at each of the four
shoulder joints, enabling the
multiple-joint interaction
required to elevate the arm
overhead
Biomechanics
Literature Summary
Author Static
or
Dynami
c
Method Interna
l
Rotatio
n
Upward
Rotatio
n
Posteri
or
Tipping
Sahara Static 3D - Open
MRI
15.6 21.5 22.2
Ludewig Dynamic 3D –
Transcor
tical pin
8 11 19
Pathomechanics
Pathomechanics
• Few high-quality studies exist on normal
biomechanics of shoulder motions
• No pathomechanics data on AC joint
• Methodological flaws in most studies of
biomechanics of shoulder pain patients
– Diagnostic standards
– Lack of agreement in findings
– Small n’s

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
15
Pathomechanics
• Excess clavicular elevation is a
consistent finding in patients with
shoulder pain
• The predominant rotation of the scapula
relative to the clavicle was posterior
tilting
• Reductions in posterior tilting of the
scapula on the thorax have been
associated with shoulder impingement
“When in doubt, examine
the patient…” (Jack McBride, MD)
• We have a rough idea of how the AC
joint should move both theoretically
and clinically (patient’s “good” side)
• Your manual examination will lead you
to the relevant pathomechanics of
your patient
• Degenerated and/or arthritic joints
don’t move well, neither do painful
joints
Anatomy & Biomechanics
Summary
Anatomy Summary
• AC joint morphology is highly
variable
• Synovial joint, susceptible to
osteoarthritis
• Radiologic findings do not
predict pain or function
• Degeneration is expected with age

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
16
Biomechanics
Summary
• Internal/external rotation,
upward/downward rotation, and
anterior/posterior tipping
motions occur at AC joint
• These motions are critical for
overall arm elevation
• Posterior tilting was the
predominant AC joint motion
Management Pathways
Nonoperative
Management
• Rest, activity modification, oral
analgesics, non-steroidal anti-
inflammatory medications, and ice
• Absence of evidence
Rios and Mazzocca 2008; Hossain, Jacobs et al. 2008;
Buttaci, Stitik et al. 2004; Burbank, Stevenson et al. 2008
P T ?
No specific reports in the
literature of physical
rehabilitation or non-invasive
treatment for patients with
primary non-acute AC joint
pathology

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
17
Buttaci et al 2004
“Physical therapy, unfortunately,
has little to offer because
therapeutic exercise and range of
motion play only a minor
role….Iontophoresis or
phonophoresis may offer some
relief and is relatively benign.”
Corticosteroid
Injections
• Relief
– 2 hours to 3
months
• Not definitive
treatment
• 3 Prospective cohorts
• 72 - 81% failed to achieve lasting
benefit
Corticosteroid
Injections
Hossain et al 2008, Jacob & Sallay 1997, van Riet et al 2011

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
18
Distal Clavicle Excision
Evidence
Operative
Management
• Mumford technique reported
prior to World War II
• No trials to ever define the role
of the procedure relative to
other interventions or natural
history
Operative
Management
• 3 Level II or III Trials comparing
surgical approaches
• Complications reported in up to 64%
of cases
– Infection
– H.O.
– Joint instability
– Suprascapular neuropathy
– Distal clavicle fracture
– Anesthesia
• Long-term results of DCE
• 1 in 3 had poor outcome
• Advised against DCE for patients
with higher functional demands

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
19
OMPT Approach
…ok, so wiggle the AC
joint & manip the T-spine
right??
Orthopaedic Manual
Physical Therapist (OMPT)
Approach
• Clinical reasoning
• Comprehensive patient examination
– Interview
– Manual examination
• Treatment tailored to the
examination findings for the
individual patient
Deyle, Henderson et al. 2000; Deyle, Allison et al. 2005; Walker,
Boyles et al. 2008; Whitman et al. 2006 Deyle, Henderson et al. 2000; Deyle, Allison et al. 2005;
Walker, Boyles et al. 2008; Whitman et al. 2006
Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
20
OMPT approach trials
• Shoulder Impingement
• Bang & Deyle 2000
• Mechanical Neck Pain
• Walker et al 2009
• Hip Osteoarthritis
• Hoeksma 2004
• Knee Osteoarthritis
• Deyle et al 2000
• Deyle et al 2005
• Lumbar Stenosis
• Whitman et al 2006
Basis for OMPT
Approach
• Chronic AC joint pain may be similar in nature
to other persistent musculoskeletal
conditions
• Other conditions respond well to OMPT
approach in high-quality RCTs
• Supporting evidence at level of systematic
review for impingement syndrome of the
shoulder
Deyle, Henderson et al. 2000; Hoeksma, Dekker et al. 2004; Deyle, Allison et al.
2005; Walker et al 2008; Whitman et al. 2006; Ho 2009
Our Study
Purpose
To observe the short and long term
changes using an OMPT approach for
primary non-acute AC joint pain
In Press, JOSPT, 2012.

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
21
Study Design
• Prospective single cohort
• Outcomes measured at baseline, 4
weeks & 6 months
In Press, JOSPT, 2012.
Inclusion Criteria
> 50% pain reduction within
10 minutes from an AC joint
injection with anesthetic
only within previous 30 days
In Press, JOSPT,
2012. In Press, JOSPT, 2012.
Exclusion Criteria
• Past history of AC joint
surgery
• AC joint ligamentous
injury (separation) within
last 12 months
• Corticosteroid injection
in this joint in last 6
months
• Neurological deficit
• Fracture or infection of
shoulder girdle bones
• Past history of
neoplastic growth in
shoulder girdle
• Inability to commit for at
least five follow-up
appointments within one
month of initial
evaluation and/or
failure to comply with
prescribed plan of care
• Any standard
contraindications to
manual therapy such as
connective tissue
disorders, rheumatoid
arthritis, osteoporosis
etc.
In Press, JOSPT, 2012.
Intervention
OMPT approach
• Typical 30 minute appointments
• Manual therapy with reinforcing ROM
activities
• Strengthening after 4 weeks
• 6 sessions
– 2x/week
– 3 weeks
In Press, JOSPT, 2012.

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
22
Commonly Used AC Joint
Mobilizations
Anterior to
Posterior
Glide
Superior to
Inferior Glide
In Press, JOSPT, 2012.
Results
Characteristics of the Cohort
Baseline Demographics*
Patients 13
Gender (M/F) 11/2
Mean age in years ± SD 41.1 (± 9.6)
Median symptom duration
(months) 6
Dominant side affected 6
Normal x-rays per radiologist 4
Taking medication for shoulder 5
* Values expressed as frequency count, except
where otherwise indicated
In Press, JOSPT, 2012.
SPADI Scores
• Mean values with error bars representing SD
• Lower values represent less pain and disability
• *p<0.001; Clinically important change = 10
In Press, JOSPT, 2012.
ASES Scores
• Mean values with error bars representing SD
• Higher values represent less pain and disability
• *p<0.001; Clinically important change = 6.4
In Press, JOSPT, 2012.

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
23
Discussion
First trial showing a
potential benefit of non-
invasive treatment of
primary AC joint pain
In Press, JOSPT, 2012.
Discussion
Convincingly positive and clinically
meaningful improvement in shoulder
pain and function:
– SPADI and ASES
– After 6.5 visits utilizing a pragmatic
clinical approach
In Press, JOSPT, 2012.
Clinical Context
Baseline 6 WK *
4 WK**
24 Months*
6 Months**
Optimal
Surgical
Procedure
62 88* 95*
Present
Cohort 59 87** 92**
ASES values
Charron et al 2007
In Press, JOSPT, 2012.
Conclusion
• Statistically significant and clinically
meaningful improvements in shoulder
pain and disability were observed in a
prospective cohort with AC joint pain
following a trial of an OMPT approach
• First reported instance of a
positive outcome with non-invasive
treatment of primary AC joint pain
In Press, JOSPT, 2012.

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
24
Manual Therapy &
Clinical Applications
When Is The AC Joint
Clinically Relevant?
• Primary AC joint
• Non-specific shoulder pain
– Sub-acromial impingement syndrome
Common AC Joint
Impairments
• Flexion
• Horizontal adduction (flexion)
Flexion Impairments
• Proposed mechanism
– Scapular posterior tipping > upward
rotation occur during flexion
– This requires superior/inferior >
medial/lateral AC joint translation
• Indications
– *AC Joint pain or limitation with
flexion
– Impaired caudal glide

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
25
Posterior
tipping
Anterior
tipping
>
Intervention for
Flexion Impairment
• Possible mobilizations for AC
joint posterior tipping
Caudal Glide
Progression
Arm at side Arm in
abduction
Prone, arm
flexed
Loaded
position
Impairments
with caudal
glide commonly
found with
difficulty in
elevating arm
Progression of
forces
Caudal Glides
Grades I - V
• Patient position
• Supine, arm at side, minimal GHJ
extension
• Therapist position
• Place the tips of both thumbs on
the superior surface of the
clavicle adjacent to the ACJ;
spread fingers out for stability
• Position forearms in line with the
caudal movement at the ACJ
• Mobilization technique
• Graded oscillatory mobilization is
applied by your arms, acting
through stable thumbs
• May span the joint or be proximal
to joint along distal clavicle
• May alter angle to a more medially
directed force

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
26
Alternate Technique
for ACJ Caudal Glides
• Lay “dummy
thumb” along
distal clavicle
• Apply caudally-
directed force
through
opposite
pisiform
Caudal Glides in
Abduction
• Patient position
• Supine, arm abducted, minimal
GHJ extension
• Therapist position
• Place the tips of both thumbs on
the superior surface of the
clavicle adjacent to the ACJ;
spread fingers out for stability
• Position forearms in line with the
caudal movement at the ACJ
• Mobilization technique
• Graded oscillatory mobilization
is applied by your arms, acting
through stable thumbs
• May span the joint or be proximal
to joint along distal clavicle
• May alter angle to a more
medially directed force
Caudal Glides in
Prone Flexion
• Patient position
– Prone; upper extremity
flexed overhead with
forearm resting on chair
• Therapist position
– Standing at patient’s head
– Thumbs on distal clavicle,
fingers splayed out for
stability
• Mobilization Technique
– Apply caudally directed
mobilization
Caudal Glides in
Prone Flexion
• Patient position
– Prone; upper extremity
flexed overhead with
forearm resting on chair
• Therapist position
– Standing at patient’s head
– Thumbs on distal clavicle,
fingers splayed out for
stability
• Mobilization Technique
– Apply caudally directed
mobilization

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
27
Caudal Glides in
Loaded Position
• Patient position
– Prone on elbows
• Therapist position
– Standing
– thumbs on distal
clavicle
• Mobilization
Technique
– caudal
Caudal Glides in
Loaded Position
• Patient position
– Prone
– Arm abducted and off
plinth
– Hand in contact with
surface
• Therapist position
– Standing
– Thumbs on distal
clavicle
• Mobilization
Technique
– Caudal glide
Horizontal Flexion
Impairments
• Proposed mechanism
– Scapular protraction occurs as the
arm crosses the body
– This requires AC joint internal
rotation
• Indications
– *AC Joint pain or motion impairment
with horizontal flexion
– Impaired A-P movement

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
28
Intervention for
Horizontal Flexion
Impairment
Possible mobilizations for AC joint IR/ER
Anterior to Posterior
Glide Progression
Arm at side Seated
Seated, IR bias
Seated, flexed,
horizontally
adducted
Impairments
with AP glide
commonly
found with
difficulty in
horizontal
adduction or
internal
rotation
Progression of
forces
AP Glides in supine
Grades III/IV
• Patient position: Supine
• Therapist position
• Place the tips of both thumbs on the
anterior surface of the clavicle
adjacent to the ACJ; spread fingers
out for stability
• Position forearms in line with the
posterior movement at the ACJ
• Mobilization technique
• Graded oscillatory mobilization is
applied by your body and arms, acting
through stable thumbs
• Pad of your outer thumb should feel
the joint motion (feel for the
stationary acromion process)
• Variations: use the pisiform to apply
posterior mobilization or use AC
shear test technique
AP Mobilization in
sitting Grades III/IV

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
29
AP Mobilization in
sitting Grades III/IV
• Patient position: seated
• Therapist position
– Standing perpendicular
to shoulder
– Apply one hand along
distal clavicle
– Apply other hand across
posterior acromion
• Mobilization Technique
– Apply graded A-P
mobilization
AP Mobilization Grades
III/IV for IR Rotation Bias
• Same as previous
technique except pre-
position patient in IR
• Progress position,
grade, and/or dosage
as tolerated
AP Mobilization in flexion
Grades III/IV for Horizontal
Adduction Bias
• Patient position
– Seated or standing
– Forearm resting on stable
surface (plinth, cabinet
etc.)
• Therapist position
– Perpendicular to shoulder
– A-P hand position
• Mobilization Technique
– Apply graded A-P
mobilization
Other Commonly Used ACJ
Mobilizations
Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
30
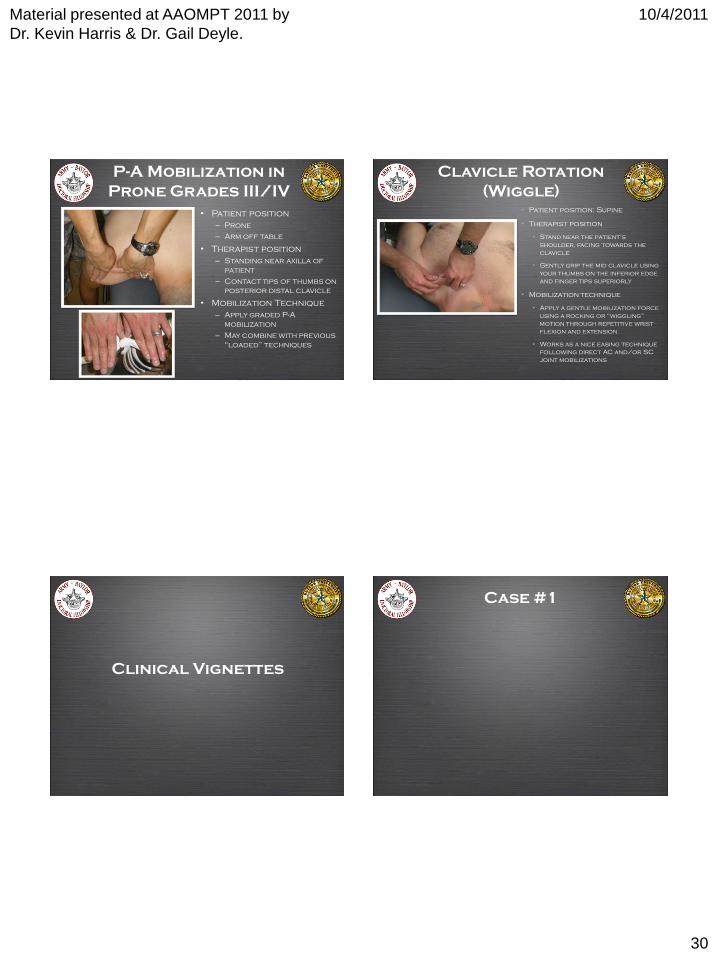
P-A Mobilization in
Prone Grades III/IV
• Patient position
– Prone
– Arm off table
• Therapist position
– Standing near axilla of
patient
– Contact tips of thumbs on
posterior distal clavicle
• Mobilization Technique
– Apply graded P-A
mobilization
– May combine with previous
“loaded” techniques
• Patient position: Supine
• Therapist position
• Stand near the patient’s
shoulder, facing towards the
clavicle
• Gently grip the mid clavicle using
your thumbs on the inferior edge
and finger tips superiorly
• Mobilization technique
• Apply a gentle mobilization force
using a rocking or “wiggling”
motion through repetitive wrist
flexion and extension
• Works as a nice easing technique
following direct AC and/or SC
joint mobilizations
Clavicle Rotation
(Wiggle)
Clinical Vignettes
Case #1

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
31
Case #1
Subjective Examination
Case #1
Objective Examination
Case #1
Treatment
Case #1
Follow-up Visit

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
32
Case #2 Case #2
Subjective Examination
Case #2
Objective Examination
Case #2
Treatment

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
33
Case #2
Follow-up Visit
Summary
• AC Joint is an important, but often
under-appreciated joint
• There’s more movement at the AC
joint than many clinicians
remember
• Role of DCE to be determined
• Evidence for impairment-based
Manual Therapist approach
Conclusion
• AC Joint is a vital link in shoulder
movement
• We have very specific targeted
interventions to treat this joint
• The more precise and direct we
can be, the larger we can expect
our effect size to be
Questions?

Material presented at AAOMPT 2011 by
Dr. Kevin Harris & Dr. Gail Deyle.
10/4/2011
34