1 uw health depression treatment guideline update stevens s. smith, ph.d. assistant professor (chs)...
TRANSCRIPT

1
UW Health Depression Treatment UW Health Depression Treatment Guideline UpdateGuideline Update
Stevens S. Smith, Ph.D.Stevens S. Smith, Ph.D.Assistant Professor (CHS)Assistant Professor (CHS)
Department of Medicine / General Internal MedicineDepartment of Medicine / General Internal MedicineCenter for Tobacco Research and InterventionCenter for Tobacco Research and Intervention
University of Wisconsin Medical SchoolUniversity of Wisconsin Medical School
Primary Care Conference PresentationPrimary Care Conference PresentationWednesday, 28 September 2005Wednesday, 28 September 2005

2
DisclaimerDisclaimer
I have received research support (but no consulting or I have received research support (but no consulting or speaking fees) from the following companies that market speaking fees) from the following companies that market smoking cessation medications:smoking cessation medications:
• SmithKline BeechamSmithKline Beecham
• GlaxoSmithKlineGlaxoSmithKline
• Elan Corporation, plcElan Corporation, plc

3
Learning ObjectivesLearning Objectives
• Review of the revised UW Health practice guideline Review of the revised UW Health practice guideline for treating depression in adults in primary carefor treating depression in adults in primary care
• Review of diagnostic issuesReview of diagnostic issues
• Role of primary care clinicians and behavioral health Role of primary care clinicians and behavioral health specialists in the treatment of depressionspecialists in the treatment of depression
• Treatment planning for depressive disordersTreatment planning for depressive disorders

4
• 58 year-old female; single, never-married; social services worker58 year-old female; single, never-married; social services worker
• Multiple medical conditions including hypertension, diabetes, Multiple medical conditions including hypertension, diabetes, CAD, hyperlipidemia; smoker; prior tx for alcoholism; has CAD, hyperlipidemia; smoker; prior tx for alcoholism; has maintained sobriety for > 20 yearsmaintained sobriety for > 20 years
• At routine check with her primary care physician (PCP), the At routine check with her primary care physician (PCP), the patient admits that she has felt mildly depressed for several patient admits that she has felt mildly depressed for several years; she denies suicidal ideation but relates that she her main years; she denies suicidal ideation but relates that she her main symptoms are “low self-esteem,” feeling tired much of the time, symptoms are “low self-esteem,” feeling tired much of the time, and feeling hopeless about the futureand feeling hopeless about the future
• Differential diagnosis rules out obvious medical or medication Differential diagnosis rules out obvious medical or medication causes for the depression; substance abuse also ruled outcauses for the depression; substance abuse also ruled out
• What is the probable diagnosis? How should her depression be What is the probable diagnosis? How should her depression be treated?treated?
Case StudyCase Study

5
Depression in Primary CareDepression in Primary Care
• General population estimates for major depression in the U.S.General population estimates for major depression in the U.S.11 : :
- Lifetime prevalence: 16.2%- Lifetime prevalence: 16.2%- 12-month prevalence rate: 6.6%- 12-month prevalence rate: 6.6%
• Prevalence of depression in adult primary care patients tends to Prevalence of depression in adult primary care patients tends to be higher especially in the presence of chronic health problemsbe higher especially in the presence of chronic health problems22
• Depression is associated with poor self-care and poor adherence Depression is associated with poor self-care and poor adherence to medical treatmentsto medical treatments
• Second only to hypertension as the most common chronic Second only to hypertension as the most common chronic condition encountered in primary care settingscondition encountered in primary care settings
11 Kessler et al., JAMA 2003, 289:3095-3105; Kessler et al., JAMA 2003, 289:3095-3105; 22 Leon et al., Arch Fam Med 1995, 10:857-861 Leon et al., Arch Fam Med 1995, 10:857-861

6
Depression in Primary CareDepression in Primary Care
• Primary care physicians are the gatekeepers of medical care Primary care physicians are the gatekeepers of medical care including depressionincluding depression
• Primary care physicians (PCPs) outnumber psychiatrists 7 to 1; Primary care physicians (PCPs) outnumber psychiatrists 7 to 1; PCPs prescribe the majority of antidepressantsPCPs prescribe the majority of antidepressants
• Outcomes for depression treatment of primary care patients do Outcomes for depression treatment of primary care patients do not differ for psychiatrists and primary care physiciansnot differ for psychiatrists and primary care physicians11
• Primary care physicians are increasingly prescribing Primary care physicians are increasingly prescribing antidepressants: in 1989, 2.6% of clinic visits versus 7.1% of antidepressants: in 1989, 2.6% of clinic visits versus 7.1% of visits in 2000 (National Ambulatory Medical Care Surveyvisits in 2000 (National Ambulatory Medical Care Survey22))
11 Simon et al., Arch Gen Psychiatry 2001, 58:395-401. Simon et al., Arch Gen Psychiatry 2001, 58:395-401.22 Pirraglia et al., Primary Care Companion J Clin Psychiatry 2003, 5:153-157. Pirraglia et al., Primary Care Companion J Clin Psychiatry 2003, 5:153-157.
7
UW Health: Treating Depression In Adults in UW Health: Treating Depression In Adults in Primary Care (2004)Primary Care (2004)
• Update of the 2002 Depression Treatment GuidelineUpdate of the 2002 Depression Treatment Guideline
• Addresses identification and treatment of Major Depressive Addresses identification and treatment of Major Depressive Disorder (also mentions Dysthymia and Adjustment Disorder with Disorder (also mentions Dysthymia and Adjustment Disorder with Depressed Mood with few details)Depressed Mood with few details)
• Role of Primary Care ClinicianRole of Primary Care Clinician
• When to refer patients to Behavioral Health SpecialistWhen to refer patients to Behavioral Health Specialist
• Includes decision trees, medication tools, quick reference guideIncludes decision trees, medication tools, quick reference guide

8
The UW Health Depression WorkgroupThe UW Health Depression Workgroup

9
Depression Guideline SectionsDepression Guideline Sections
1.1. Suspect depressionSuspect depression
2.2. Interview for key symptoms of depressionInterview for key symptoms of depression
3.3. Involve Behavioral Health Involve Behavioral Health
4.4. Consider co-morbid disordersConsider co-morbid disorders
5.5. Treatment planTreatment plan
6.6. Section on post-partum depressionSection on post-partum depression
7.7. Useful tables on concurrent conditions, medication side Useful tables on concurrent conditions, medication side effects, drug interactions, and dosage ranges + formulary effects, drug interactions, and dosage ranges + formulary infoinfo
8.8. Treatment monitoring flow-sheetsTreatment monitoring flow-sheets

10
Steps 1 & 2: Suspect & Diagnose Depression Steps 1 & 2: Suspect & Diagnose Depression

11
DSM-IV Disorders with DepressionDSM-IV Disorders with Depression
1.1. Major Depressive Disorder (Mild, Moderate, Severe)Major Depressive Disorder (Mild, Moderate, Severe)
2.2. Dysthymia Dysthymia
3.3. Adjustment Disorder with Depressed Mood Adjustment Disorder with Depressed Mood
4.4. Depressive Disorder Not Otherwise SpecifiedDepressive Disorder Not Otherwise Specified
5.5. Mood Disorder Due to a Medical ConditionMood Disorder Due to a Medical Condition
6.6. Substance-Induced Mood DisorderSubstance-Induced Mood Disorder
7.7. Seasonal Affective DisorderSeasonal Affective Disorder
8.8. Post-Partum DepressionPost-Partum Depression
9.9. Others including Bipolar Disorder, CyclothymiaOthers including Bipolar Disorder, Cyclothymia

12
Guideline Step 1: Suspect DepressionGuideline Step 1: Suspect Depression
1.1. Physical complaints – insomnia, fatigue, changes in Physical complaints – insomnia, fatigue, changes in appetite and/or weightappetite and/or weight
2.2. Functional impairments (work, relationships)Functional impairments (work, relationships)
3.3. Risk factors: personal or family hx of depression, female, Risk factors: personal or family hx of depression, female, socially isolated, multiple medical problems, post-partumsocially isolated, multiple medical problems, post-partum
4.4. Ask screening questions:Ask screening questions:
““During the past two weeks, have you felt down, During the past two weeks, have you felt down, depressed or hopeless?”depressed or hopeless?”
““During the past two weeks, have you felt little interest or During the past two weeks, have you felt little interest or pleasure in doing things?”pleasure in doing things?”

13
Guideline Step 2: Interview for Key Guideline Step 2: Interview for Key Symptoms of Major DepressionSymptoms of Major Depression
1.1. For DSM-IV diagnosis of Major Depressive Disorder, For DSM-IV diagnosis of Major Depressive Disorder, patient must have at least 5 of 9 symptoms including patient must have at least 5 of 9 symptoms including either depressed mood or anhedonia (loss of either depressed mood or anhedonia (loss of interest/pleasure)interest/pleasure)
2.2. Symptoms must have been present for at least 2 weeksSymptoms must have been present for at least 2 weeks

14
Guideline Step 2: Interview for Key Guideline Step 2: Interview for Key Symptoms of DysthymiaSymptoms of Dysthymia
• Chronic depressed mood for most of the days, for more days Chronic depressed mood for most of the days, for more days than not, for at least 2 yearsthan not, for at least 2 years
• Must not have gone for more than 2 months without experiencing Must not have gone for more than 2 months without experiencing two or more of the following symptoms: two or more of the following symptoms:
- poor appetite or overeating - poor appetite or overeating - insomnia or hypersomnia - insomnia or hypersomnia - low energy or fatigue - low energy or fatigue - low self-esteem - low self-esteem - poor concentration or difficulty making decisions - poor concentration or difficulty making decisions - feelings of hopelessness - feelings of hopelessness
• Significant distress or functional impairmentSignificant distress or functional impairment

15
Guideline Step 2: Interview for Key Guideline Step 2: Interview for Key Symptoms of Adjustment Disorder With Depressed MoodSymptoms of Adjustment Disorder With Depressed Mood
• Development of emotional or behavioral symptoms in response Development of emotional or behavioral symptoms in response to an identifiable stressor occurring within 3 months of the onset to an identifiable stressor occurring within 3 months of the onset of the stressorof the stressor
• Marked distress beyond expected response to stressor or significant functional impairment
• Not bereavement
• Symptoms do not persist > 6 months after stressor ends

16
Guideline Step 3: Consider Referral to Behavioral Guideline Step 3: Consider Referral to Behavioral Health Specialist (BHS)Health Specialist (BHS)
1.1. Same day consultation with or evaluation by psychiatrist:Same day consultation with or evaluation by psychiatrist:
- suicidality with safety concerns; assaultiveness or homicidal - suicidality with safety concerns; assaultiveness or homicidal intentions; psychosis; severe functional impairmentintentions; psychosis; severe functional impairment
2.2. Consider non-emergent/non-urgent referral to BHS:Consider non-emergent/non-urgent referral to BHS:
- psychiatric co-morbidity (e.g., OCD, eating disorders)- psychiatric co-morbidity (e.g., OCD, eating disorders)- suicidal thoughts or angry with others (no clear plan)- suicidal thoughts or angry with others (no clear plan)- alcohol or substance abuse (special referral to AODA tx)- alcohol or substance abuse (special referral to AODA tx)- psychotic depression (refer to psychiatry)- psychotic depression (refer to psychiatry)- pregnancy (refer to psychiatry)- pregnancy (refer to psychiatry)- diagnostic uncertainty- diagnostic uncertainty- poor response to antidepressant (refer to psychiatry)- poor response to antidepressant (refer to psychiatry)

17
Relative Degree of Involvement of PCPs Relative Degree of Involvement of PCPs and Behavioral Health Specialists (BHS)and Behavioral Health Specialists (BHS)
NoneNone SubthresholdSubthreshold SimpleSimple ComplexComplex SevereSevere
PCPPCP
BHS in BHS in Specialty Specialty SettingsSettings
Type of Problem/DisorderType of Problem/Disorder
BHS inBHS inPrimary CarePrimary Care
SettingsSettings
PCPPCP

18
Guideline Step 4: Consider Co-Morbid DisordersGuideline Step 4: Consider Co-Morbid Disorders
1.1. Is depression secondary to a medical condition?Is depression secondary to a medical condition?
2.2. Is depression secondary to medication?Is depression secondary to medication?
3.3. Is depression secondary to alcoholism or substance use?Is depression secondary to alcoholism or substance use?
4.4. Are there other psychiatric disorders that may be masked Are there other psychiatric disorders that may be masked by depression such as anxiety, OCD, phobias, or eating by depression such as anxiety, OCD, phobias, or eating disorders?disorders?
5.5. Is the patient experiencing normal bereavement (lasting Is the patient experiencing normal bereavement (lasting up to 2 months)?up to 2 months)?
19
Guideline Step 5: Treatment PlanGuideline Step 5: Treatment Plan
1.1. Objectives of treatment:Objectives of treatment:
- Reduction and elimination of depressive signs and symptoms- Reduction and elimination of depressive signs and symptoms- Restoration of premorbid functioning- Restoration of premorbid functioning- Relapse prevention- Relapse prevention
2. 2. Modes of treatment: Modes of treatment:
- psychotherapy alone - psychotherapy alone - medication- medication- medication and psychotherapy- medication and psychotherapy- ECT- ECT
3. 3. Patient educationPatient education
- medication compliance- medication compliance- nature and course of depression- nature and course of depression- importance of follow-up appointments- importance of follow-up appointments
20
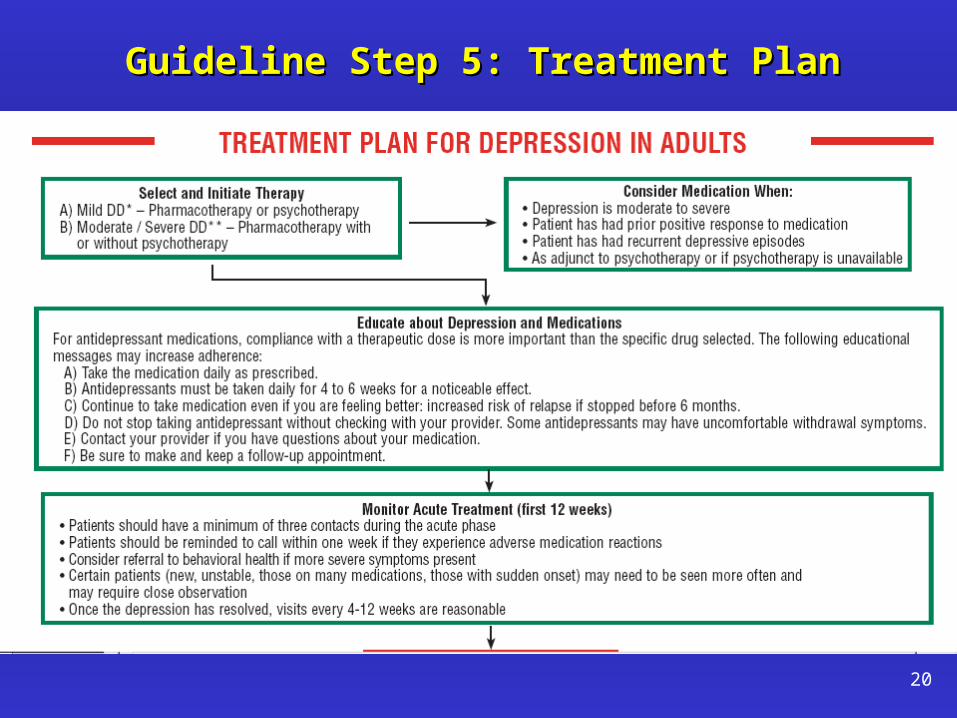
Guideline Step 5: Treatment PlanGuideline Step 5: Treatment Plan
21
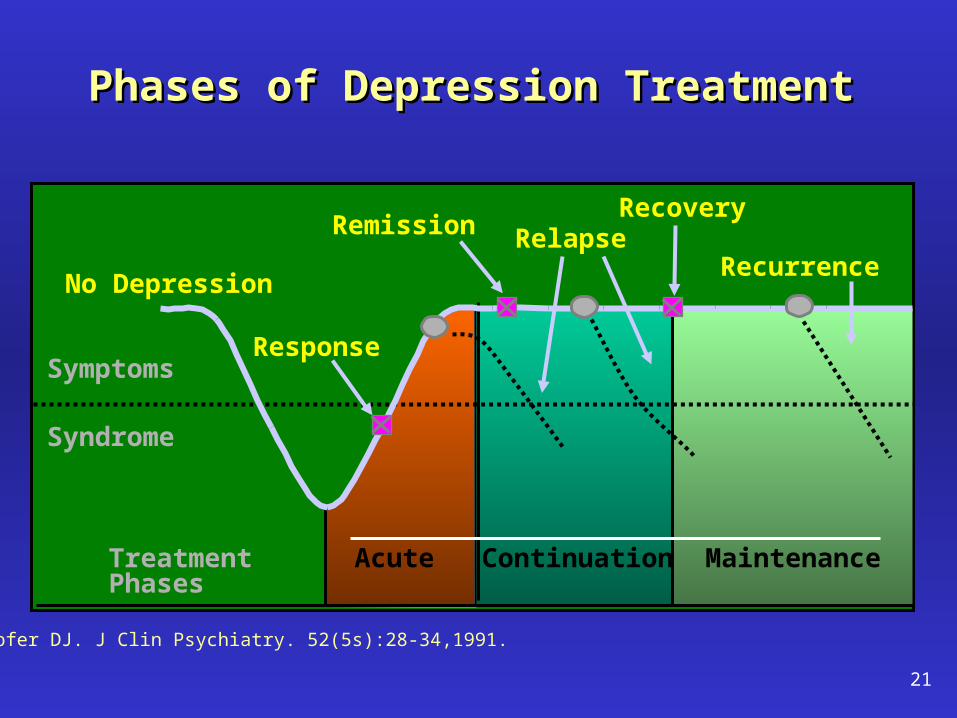
Phases of Depression TreatmentPhases of Depression Treatment
Kupfer DJ. J Clin Psychiatry. 52(5s):28-34,1991.
Treatment Phases
RelapseRecurrence
Recovery
Acute Continuation Maintenance
Syndrome
Symptoms
Remission
Response
No Depression

22
1. 1. Acute phaseAcute phase - first 12 weeks of treatment: - first 12 weeks of treatment:
- Patient should be seen a minimum of 3 times (at least once with - Patient should be seen a minimum of 3 times (at least once with prescriber)prescriber)
- After resolution of depression, patient can be seen about every - After resolution of depression, patient can be seen about every 4-12 weeks4-12 weeks
2.2. Continuation phaseContinuation phase – next 6-9 months – next 6-9 months
- Patient should remain on medication for at least 6 months after - Patient should remain on medication for at least 6 months after resolution of symptomsresolution of symptoms
- Patient must be symptom-free for 6-9 months before - Patient must be symptom-free for 6-9 months before discontinuing medication/treatmentdiscontinuing medication/treatment
3.3. Maintenance phaseMaintenance phase – 1 year to lifetime (if needed) – 1 year to lifetime (if needed)
Guideline Step 5: Treatment PlanGuideline Step 5: Treatment Plan

23

24
• Primary care physician referred the patient to a psychologist for Primary care physician referred the patient to a psychologist for evaluation and treatmentevaluation and treatment
• Psychiatric Diagnoses:Psychiatric Diagnoses: Dysthymic DisorderDysthymic DisorderTobacco Use DisorderTobacco Use Disorder
• Treatment:Treatment: Initial medication – fluoxetineInitial medication – fluoxetinePsychotherapyPsychotherapyMedication changed to bupropion XL after 2 Medication changed to bupropion XL after 2
yearsyears
• Patient is continuing in treatment (medication and psychotherapy)Patient is continuing in treatment (medication and psychotherapy)
Case StudyCase Study
25
Depression Guideline Sections RevisitedDepression Guideline Sections Revisited
1.1. Suspect depressionSuspect depression
2.2. Interview for key symptoms of depressionInterview for key symptoms of depression
3.3. Involve Behavioral Health Involve Behavioral Health
4.4. Consider co-morbid disordersConsider co-morbid disorders
5.5. Treatment planTreatment plan
6.6. Section on post-partum depressionSection on post-partum depression
7.7. Useful tables on concurrent conditions, medication side Useful tables on concurrent conditions, medication side effects, drug interactions, and dosage ranges + formulary effects, drug interactions, and dosage ranges + formulary infoinfo
8.8. Treatment monitoring flow-sheetsTreatment monitoring flow-sheets